Embed Size (px)
Citation preview

GESITRA 1
New antifungal strategies
Patricia Muñoz, MD. Ph.D. ([email protected])
Hospital General Universitario Gregorio Marañón
Universidad Complutense de Madrid
Monday, March 2nd 2015 10-10:30
New and upcoming antifungals
Index
1. Present way of using antifungals
Present way of using antifungals
Culture based
Targeted prophylaxis
Empirical/Preemptive therapy based on local epidemiology, risk factors, and clinical scores such as the ‘Candida score’
More common problems
Too much
Empirical therapy in ICU (2/182 treated pts had candidemia) González, Crit Care 2012
Colonization (UTI, RT) Aitken, Ann Pharmacother 2014
Combination therapy or excessive prophylaxis Muñoz, Clin
Transplant 2012
No adjustment to Microbiology results (29-39%) Shah. JAC
2011; Baddley Diagn Microbiol Infect Dis 2004
Too little, too late
Therapy in candidemia first 48h: 7% Bassetti CMI 2013; Aitken, Ann
Pharmacother 2014
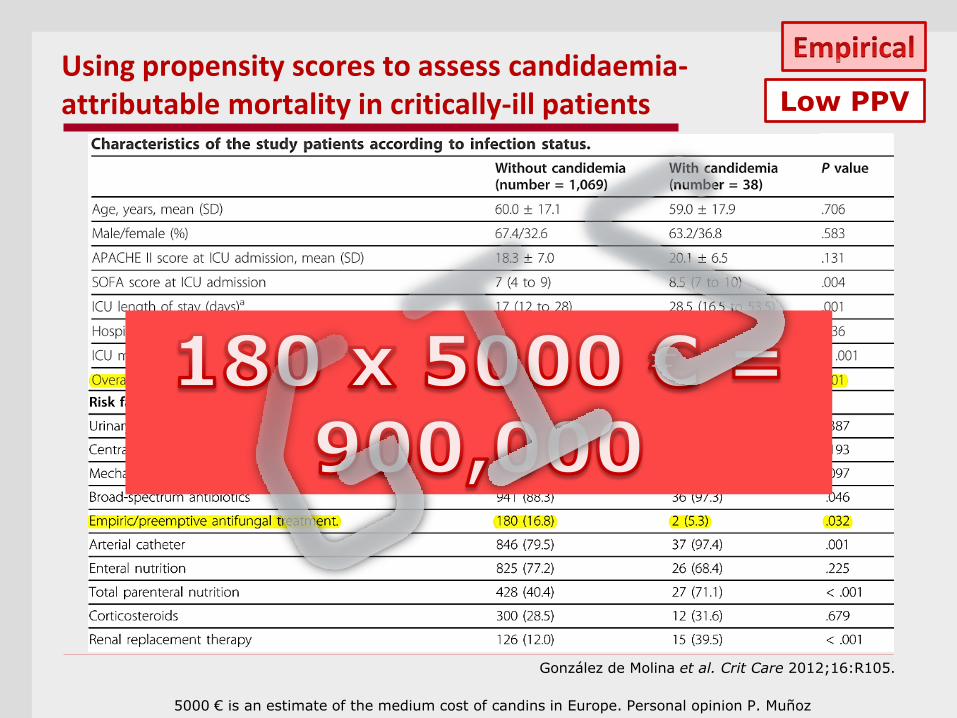
Using propensity scores to assess candidaemia- attributable mortality in critically-ill patients
González de Molina et al. Crit Care 2012;16:R105.
Low PPV
5000 € is an estimate of the medium cost of candins in Europe. Personal opinion P. Muñoz
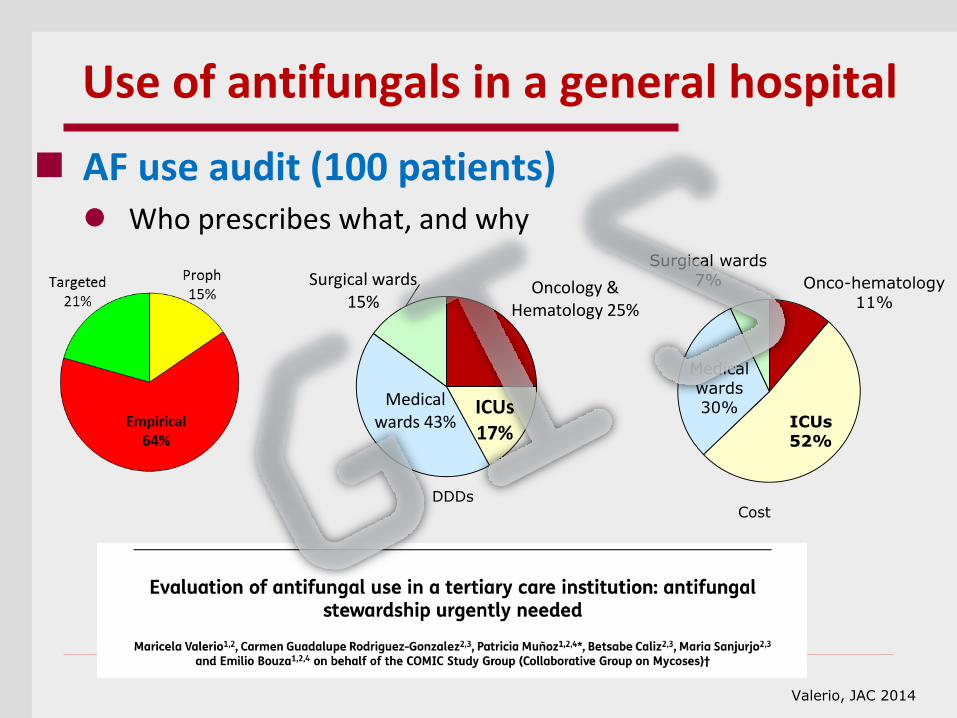
AF use audit (100 patients) Who prescribes what, and why
Onco-hematology
11%
ICUs 52%
Medical
wards 30%
Surgical wards
7%
Cost
Use of antifungals in a general hospital
Valerio, JAC 2014
Oncology & Hematology 25%
ICUs 17%
Medical wards 43%
Surgical wards 15%
DDDs
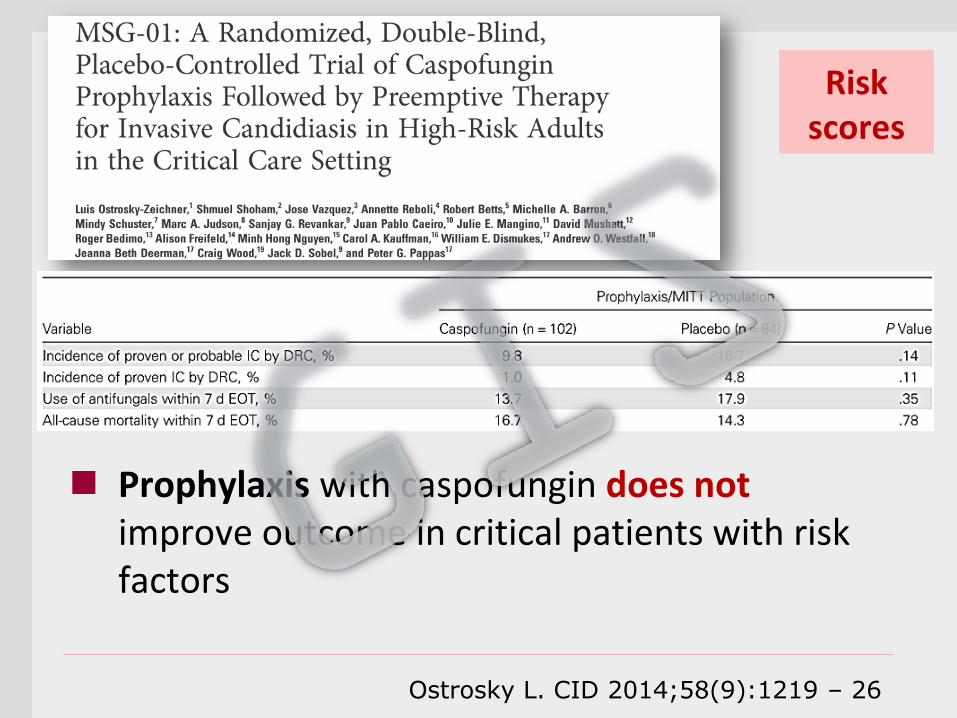
Risk scores
Prophylaxis with caspofungin does not improve outcome in critical patients with risk factors
Ostrosky L. CID 2014;58(9):1219 – 26
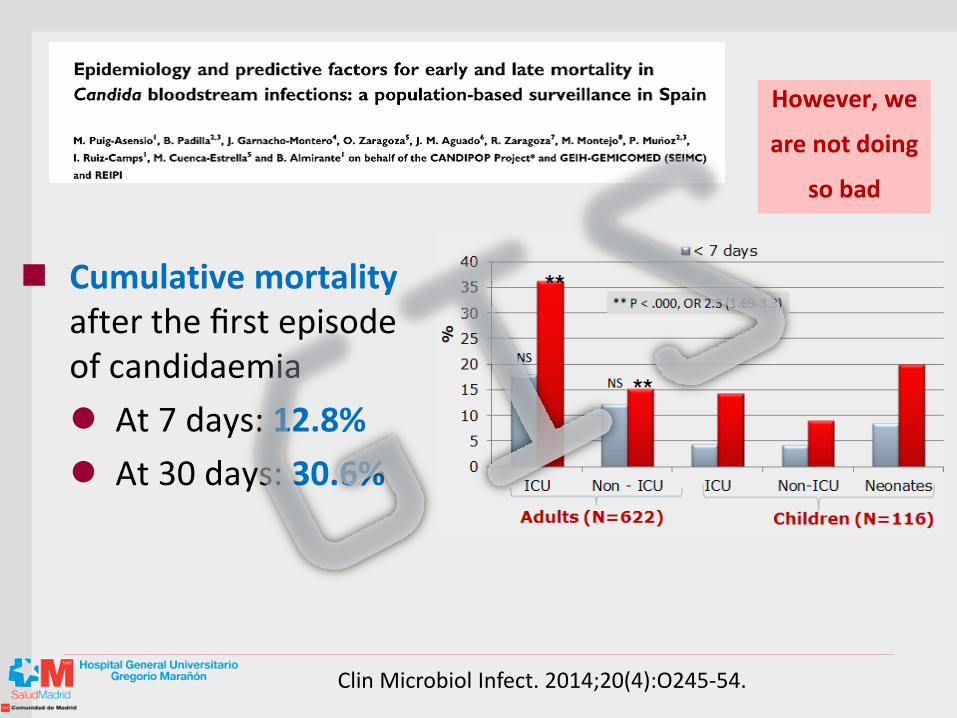
However, we
are not doing
so bad
Cumulative mortality after the first episode of candidaemia
At 7 days: 12.8%
At 30 days: 30.6%
Clin Microbiol Infect. 2014;20(4):O245-54.
Benchmarking. What is a normal AF use?
How many DDDs/ 1,000 patient-days is normal to expend?
Published data: 40 to 296
In our center, a tertiary hospital with very active transplant, oncology and HIV programs, a recent survey showed that
- 65.1 DDDs per 1000 patient-days
- 13% were considered unnecessary
Mondain, 2013; Cook, 2004; Standiford, 2012; Apisarnthanarak, 2010; Lopez-Medrano, 2013; Valerio, 2014
Ideas to take home
Both culture based and risk factor-based approaches have very low sensitivity, increase cost and risk of resistance emergence. However, candidemia mortality has been significantly reduced
Index
1. Present way of using antifungals
2. Stewardship programs
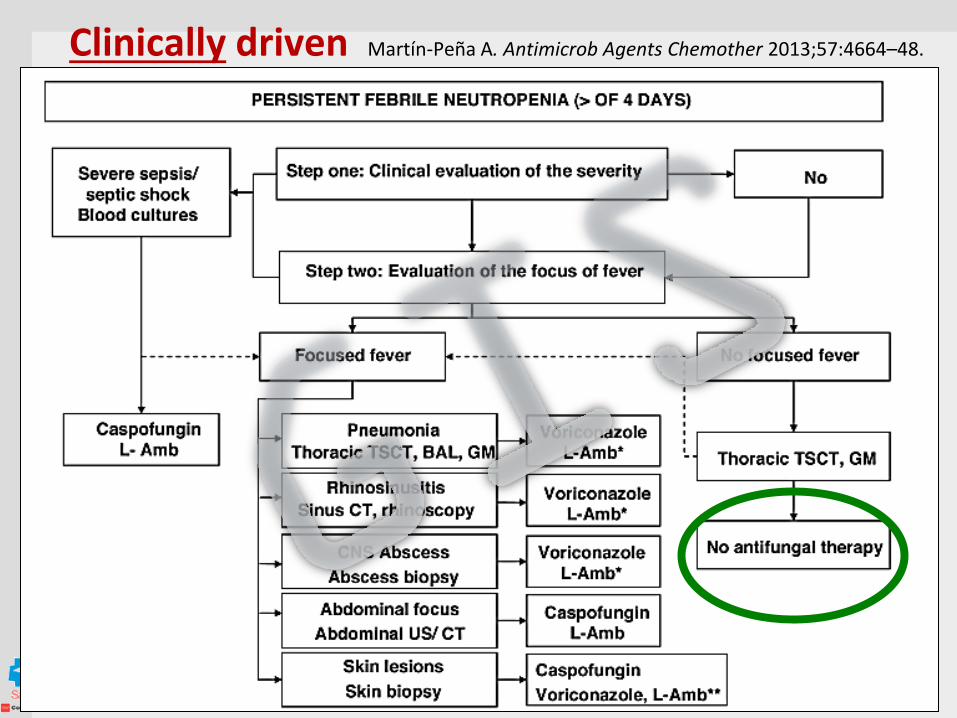
Clinically driven Martín-Peña A. Antimicrob Agents Chemother 2013;57:4664–48.
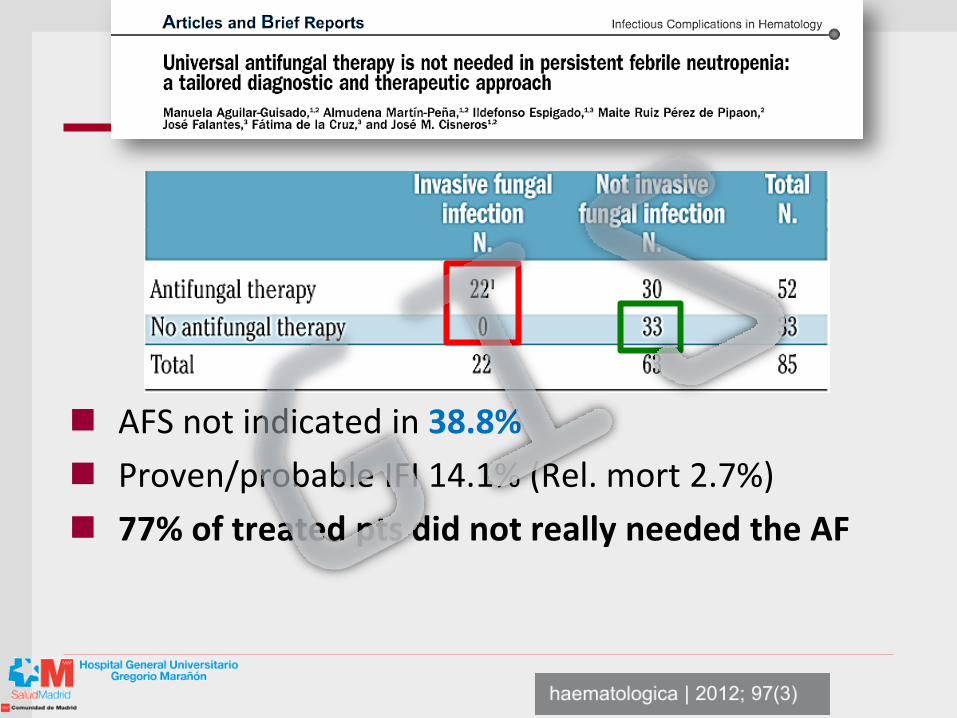
AFS not indicated in 38.8%
Proven/probable IFI 14.1% (Rel. mort 2.7%)
77% of treated pts did not really needed the AF
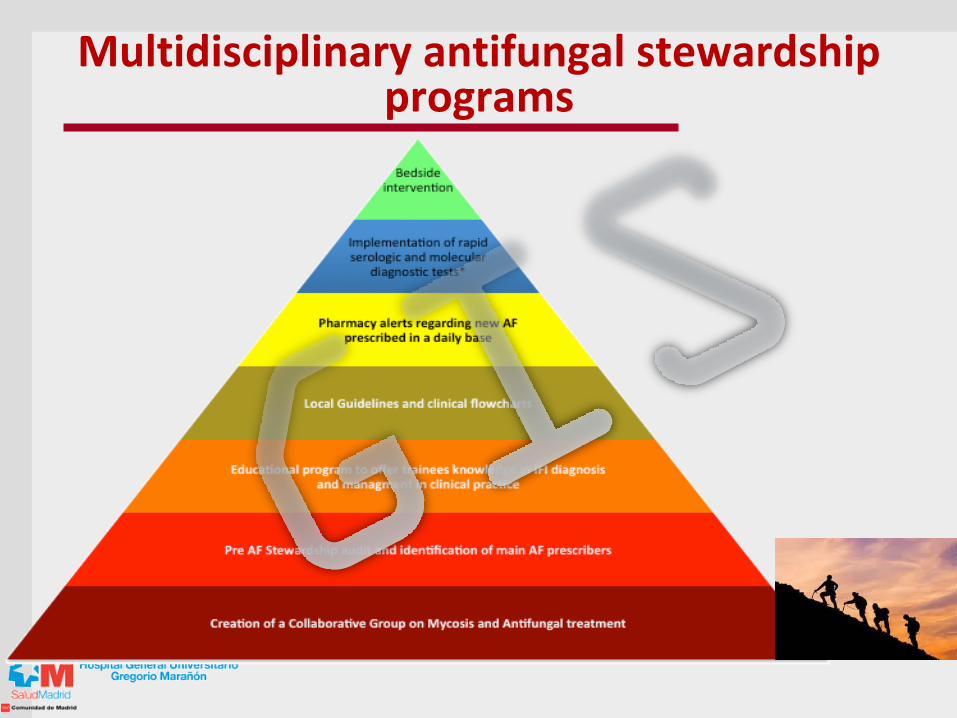
Multidisciplinary antifungal stewardship programs
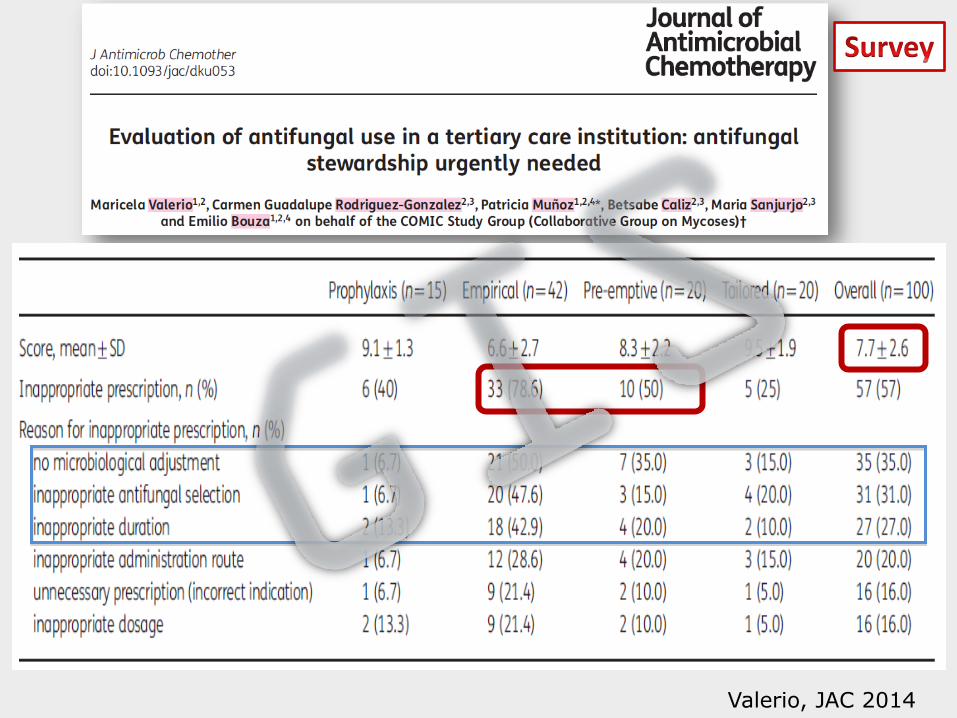
Valerio, JAC 2014
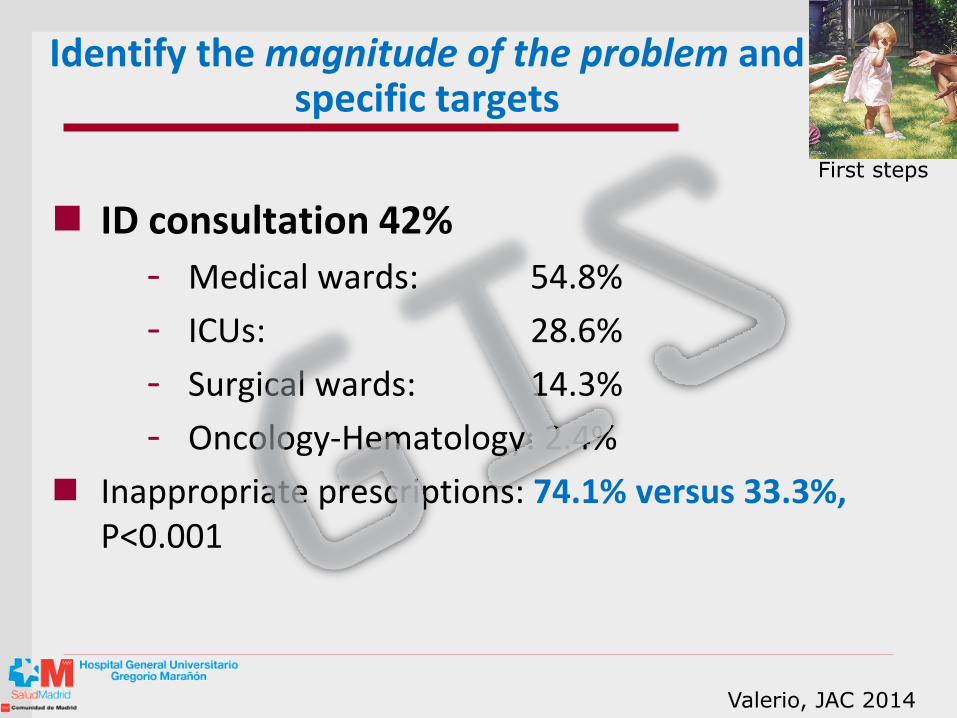
Identify the magnitude of the problem and specific targets
ID consultation 42%
- Medical wards: 54.8%
- ICUs: 28.6%
- Surgical wards: 14.3%
- Oncology-Hematology: 2.4%
Inappropriate prescriptions: 74.1% versus 33.3%, P<0.001
Valerio, JAC 2014
First steps
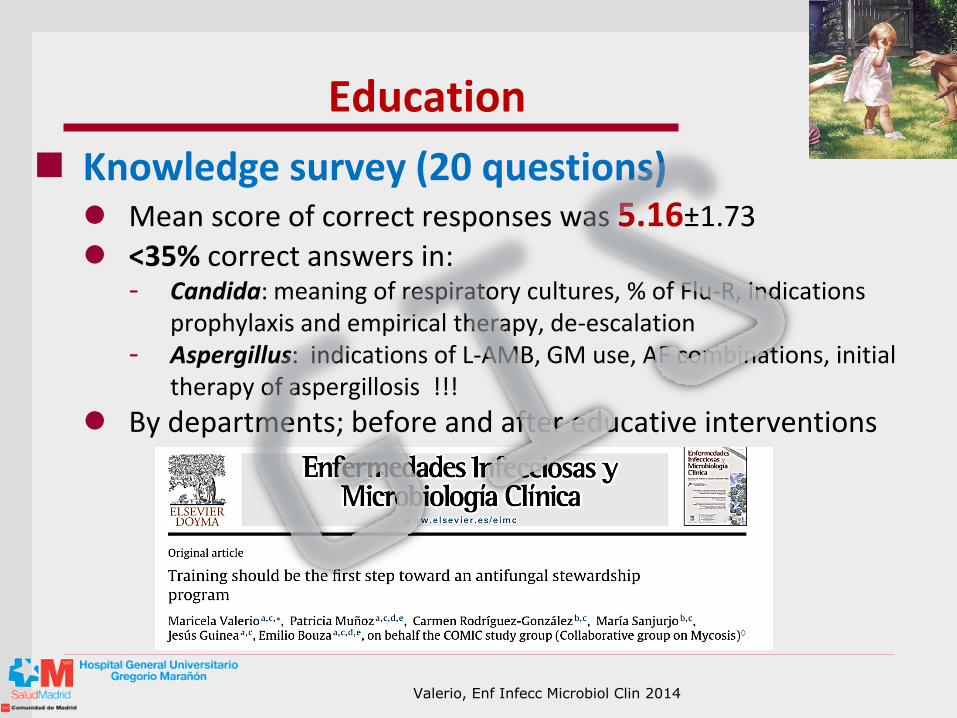
Education
Knowledge survey (20 questions) Mean score of correct responses was 5.16±1.73 <35% correct answers in:
- Candida: meaning of respiratory cultures, % of Flu-R, indications prophylaxis and empirical therapy, de-escalation
- Aspergillus: indications of L-AMB, GM use, AF combinations, initial therapy of aspergillosis !!!
By departments; before and after educative interventions
Valerio, Enf Infecc Microbiol Clin 2014
Education
Initiate educational activities
General and particular sessions Use the results of the previous surveys Involve members of the AFS team
Produce your own local guidelines
General or for specific departments Local epidemiology, diagnostic criteria, indications, dose
adjustments Members contact telephones Intranet and/or pocket leaflets
First steps
Multidisciplinary
Pharmacy department AF alerts, prescription tools, interactions, advice
Cost: Monitor DDDs or PDDDs. Overall and at unit level
Price negotiation !!!
Expert Pharm: advice to prescribing physicians or daily audit of agreed on protocols
Clinical Microbiology Rapid turnover of lab results (streamlining) Help clinicians with Dx investigations TDM Innovative diagnostic tools: help to stop empirical therapy,
start early antifungals, streamlining
ID physicians
Bedside intervention Prescribing etiquette: health-care models,
perceived loss of autonomy, local leaders in charge
Die of success: when program works, your collaborators will get better work offers (happened in ID and Pharmacy) - Have someone learning the role simultaneously
Always play safe: Prestige of the AFS
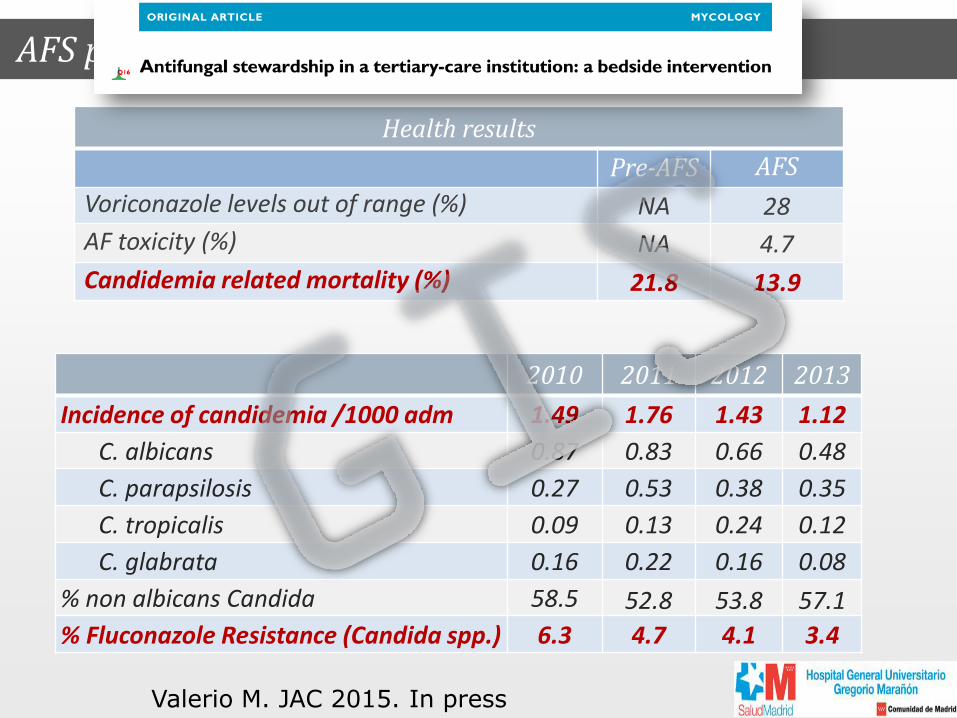
AFS program: Clinical and Microbiological results
Health results
Pre-AFS AFS
Voriconazole levels out of range (%) NA 28
AF toxicity (%) NA 4.7
Candidemia related mortality (%) 21.8 13.9
2010 2011 2012 2013
Incidence of candidemia /1000 adm 1.49 1.76 1.43 1.12
C. albicans 0.87 0.83 0.66 0.48
C. parapsilosis 0.27 0.53 0.38 0.35
C. tropicalis 0.09 0.13 0.24 0.12
C. glabrata 0.16 0.22 0.16 0.08
% non albicans Candida 58.5 52.8 53.8 57.1
% Fluconazole Resistance (Candida spp.) 6.3 4.7 4.1 3.4
Valerio M. JAC 2015. In press
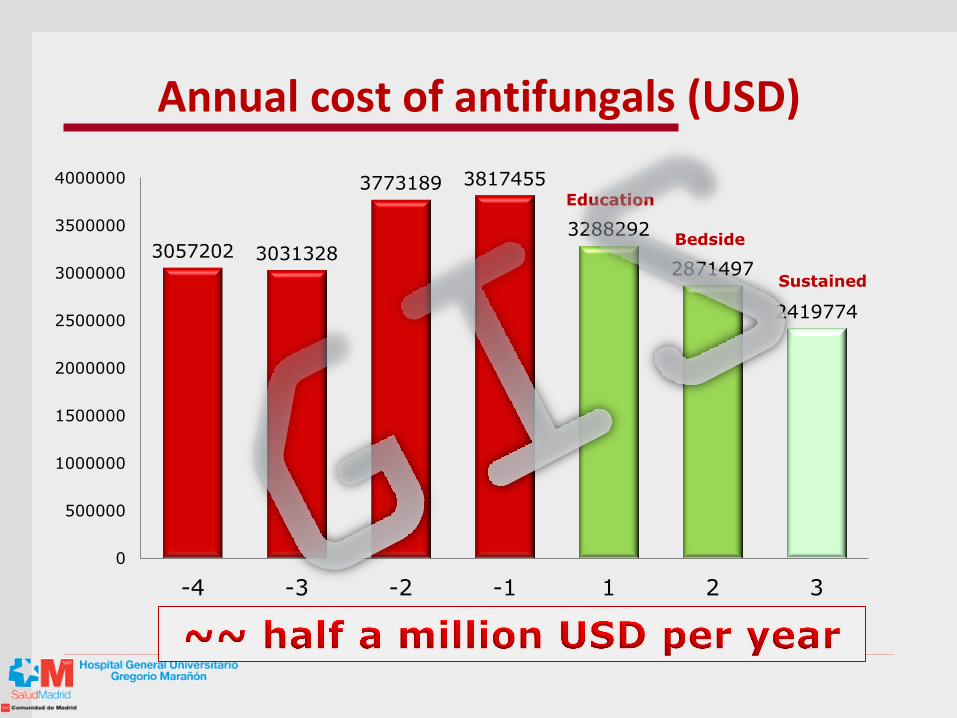
Annual cost of antifungals (USD)
3057202 3031328
3773189 3817455
3288292
2871497
2419774
0
500000
1000000
1500000
2000000
2500000
3000000
3500000
4000000
-4 -3 -2 -1 1 2 3
Education
Bedside
Sustained
Ideas to take home
Multidisciplinary antifungal stewardship programs performed by dedicated experts are effective, but require great effort and long-term maintained dedication
Index
1. Present way of using antifungals
2. Stewardship programs
3. Biomarkers
Biomarkers
BDG (Associates of Cape Cod Incorporated, USA)
Not Candida-specific and many false positives
Promising tool for the diagnosis of IC (pooled S of 76.8% and Sp of 85.3%) CID 2011; 52: 750
CAGTA (Vircell, Granada, Spain)
Less mortality in treated ICU patients with increasing CAGTA values BMC Infect Dis 2011; 11: 60
Platelia Candida
Lack reproducibility and indeterminate results
Biomarker-driven approach in hematology
• GM EIA, PCR + High resolution CT scan
• No empirical antifungal therapy in patients receiving adequate prophylaxis (TDM)
• Negative GM + PCR: exclude IA
Sensitivity: 98.1%, NPV: 99.6%
• Neither PCR nor GM EIA can be used alone to diagnose IA: PPV <31.7%
Barnes R et al. J Infect 2013;67:206–14.
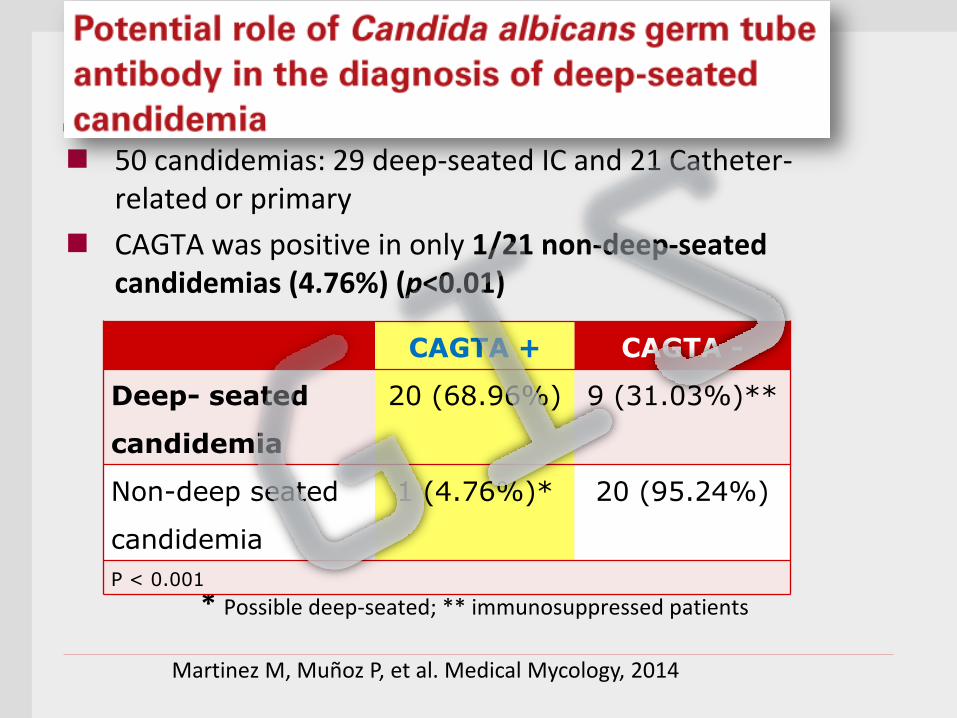
CAGTA may help differentiate CR-candidemia
50 candidemias: 29 deep-seated IC and 21 Catheter-related or primary
CAGTA was positive in only 1/21 non-deep-seated candidemias (4.76%) (p<0.01)
* Possible deep-seated; ** immunosuppressed patients
CAGTA + CAGTA -
Deep- seated
candidemia
20 (68.96%) 9 (31.03%)**
Non-deep seated
candidemia
1 (4.76%)* 20 (95.24%)
P < 0.001
Martinez M, Muñoz P, et al. Medical Mycology, 2014
Value of combining biomarkers at different cut-offs to rule out IC
31 candidemias (Candida albicans 40%, C. tropicalis 20%, C. parapsilosis 18%, C. glabrata 12%, other 10%) and 50 bacteremias
CAGTA, mannan antigens (MN), anti-mannan antibodies (AMN), and (1→3)-β-D-glucan (BDG)
Manufacturer’s and alternative cut-offs to improve the accuracy of the tests
Candida biomarkers in patients with candidemia and bacteremia
M. Carmen Martínez-Jiménez 1,2 ;Patricia Muñoz* 1,2,3,4 Maricela Valerio 1,2 Roberto Alonso 1,2 Carmen Martos 1 Jesús Guinea 1,2,3 Emilio Bouza 1,2,3,4
1 Clinical Microbiology and Infectious Disease Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain. 2 Instituto de Investigación Sanitaria del Hospital Gregorio Marañón, Madrid, Spain. 3 CIBER Enfermedades Respiratorias-CIBERES (CB06/06/0058), Madrid, Spain. 4 Medicine Department, School of Medicine, Universidad Complutense de Madrid, Madrid, Spain
Martinez M. JAC 2015 in press
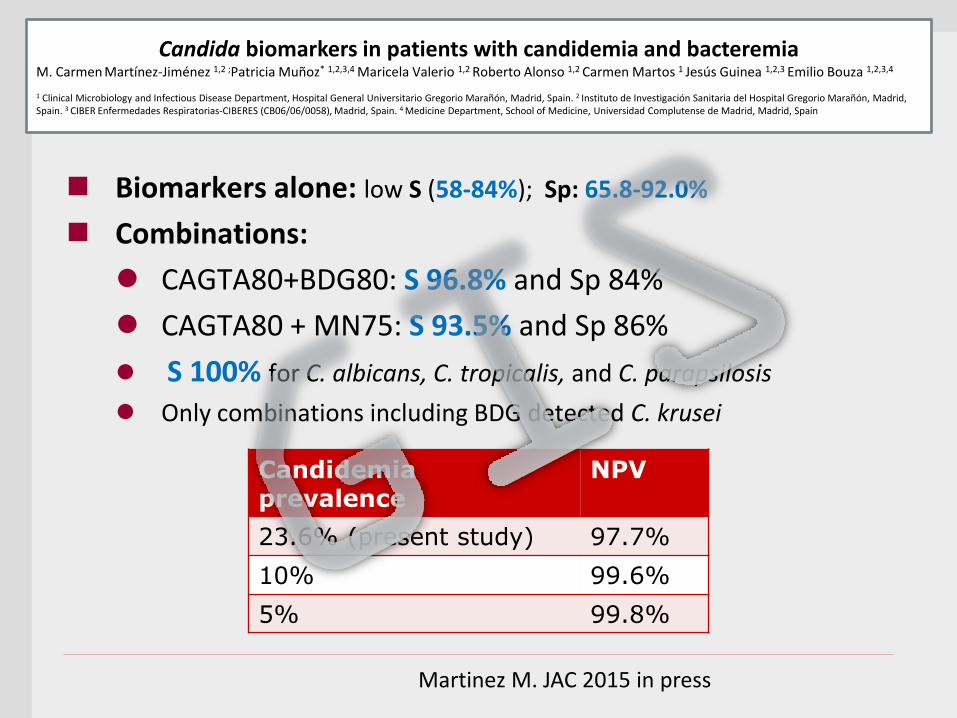
Biomarkers alone: low S (58-84%); Sp: 65.8-92.0%
Combinations:
CAGTA80+BDG80: S 96.8% and Sp 84%
CAGTA80 + MN75: S 93.5% and Sp 86%
S 100% for C. albicans, C. tropicalis, and C. parapsilosis
Only combinations including BDG detected C. krusei
Candida biomarkers in patients with candidemia and bacteremia
M. Carmen Martínez-Jiménez 1,2 ;Patricia Muñoz* 1,2,3,4 Maricela Valerio 1,2 Roberto Alonso 1,2 Carmen Martos 1 Jesús Guinea 1,2,3 Emilio Bouza 1,2,3,4
1 Clinical Microbiology and Infectious Disease Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain. 2 Instituto de Investigación Sanitaria del Hospital Gregorio Marañón, Madrid, Spain. 3 CIBER Enfermedades Respiratorias-CIBERES (CB06/06/0058), Madrid, Spain. 4 Medicine Department, School of Medicine, Universidad Complutense de Madrid, Madrid, Spain
Martinez M. JAC 2015 in press
Candidemia prevalence
NPV
23.6% (present study) 97.7%
10% 99.6%
5% 99.8%
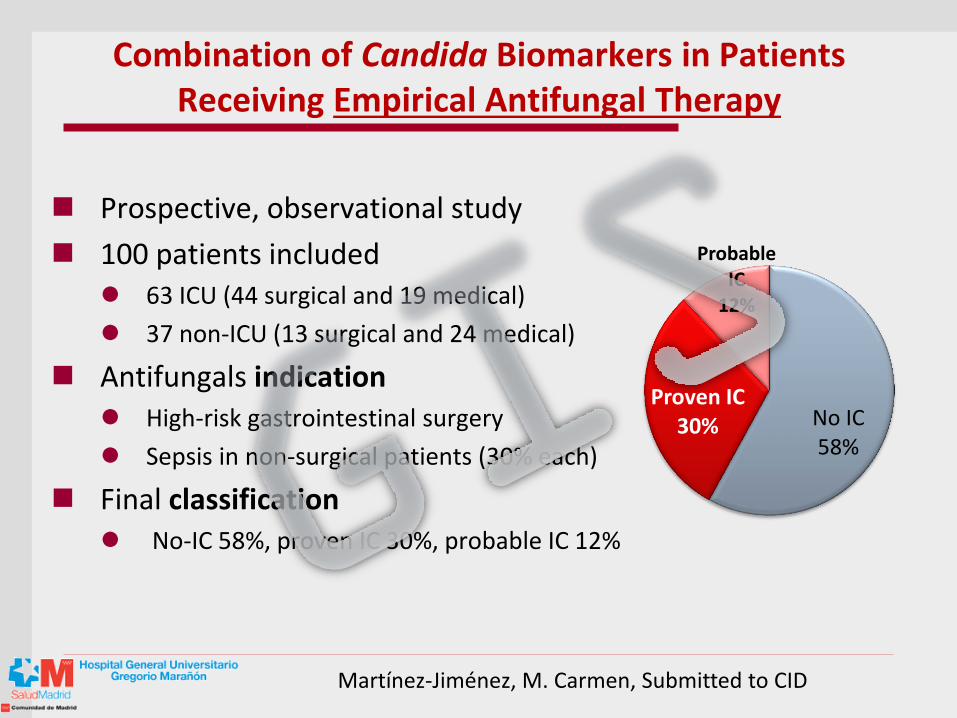
Combination of Candida Biomarkers in Patients Receiving Empirical Antifungal Therapy
Prospective, observational study
100 patients included 63 ICU (44 surgical and 19 medical)
37 non-ICU (13 surgical and 24 medical)
Antifungals indication High-risk gastrointestinal surgery
Sepsis in non-surgical patients (30% each)
Final classification No-IC 58%, proven IC 30%, probable IC 12%
Martínez-Jiménez, M. Carmen, Submitted to CID
No IC 58%
Proven IC 30%
Probable IC
12%
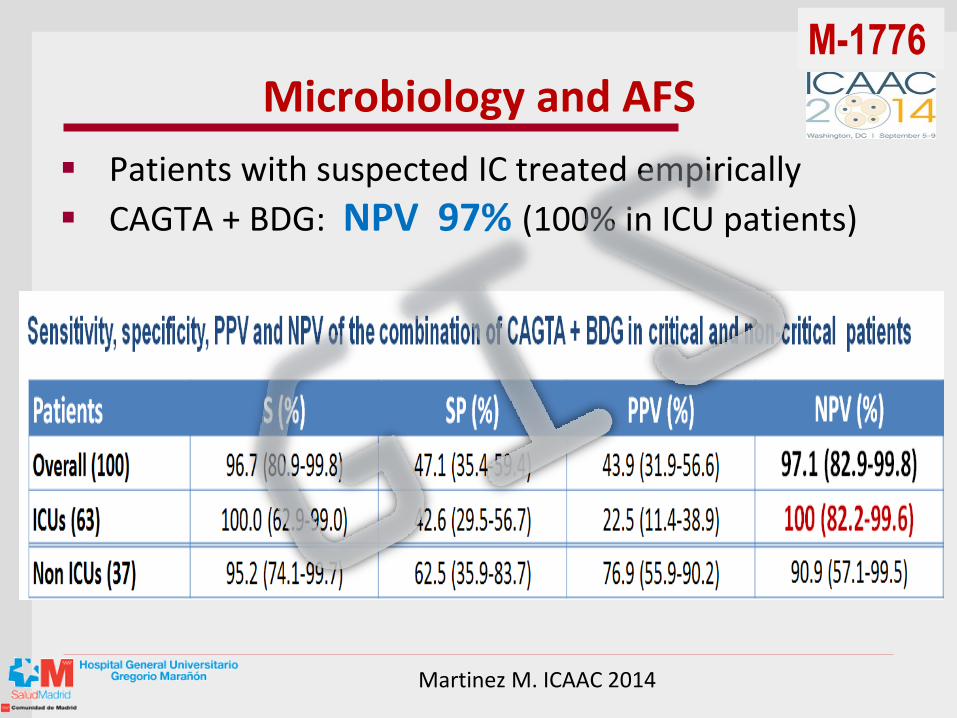
Microbiology and AFS
Patients with suspected IC treated empirically
CAGTA + BDG: NPV 97% (100% in ICU patients)
M-1776
Martinez M. ICAAC 2014
Ideas to take home
Candida biomarkers may help in the identification of CR-candidemia (CAGTA) and in the reduction of the duration of empirical therapy.
The behavior of the biomarkers in non-candidemic forms of IC needs more research.
Index
1. Present way of using antifungals
2. Stewardship programs
3. Candida biomarkers
4. New diagnostic methods
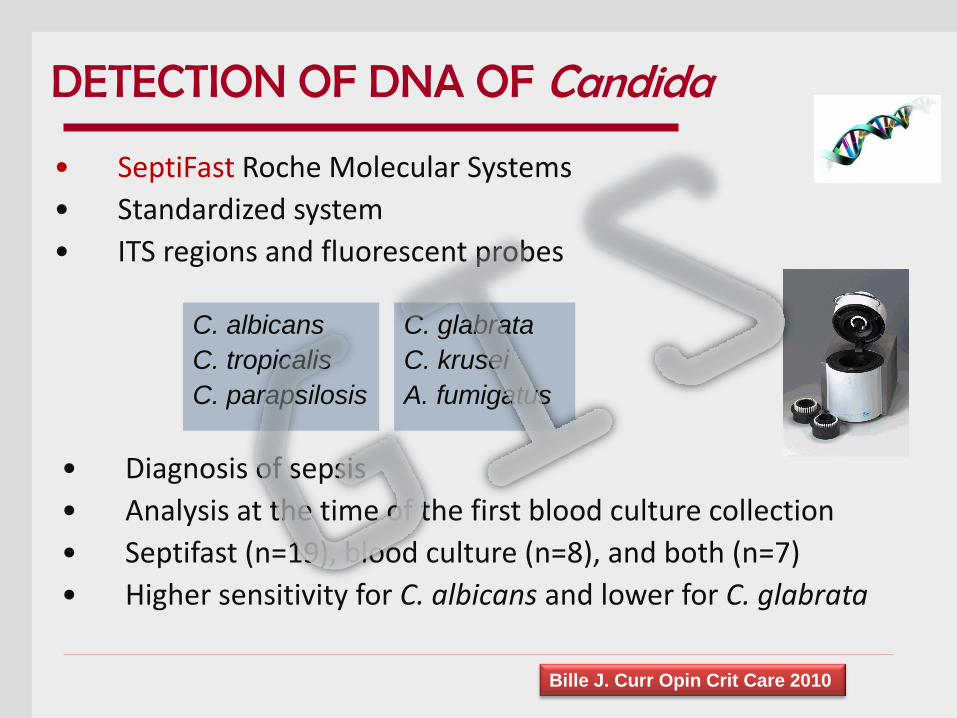
• SeptiFast Roche Molecular Systems
• Standardized system
• ITS regions and fluorescent probes
C. albicans
C. tropicalis
C. parapsilosis
C. glabrata
C. krusei
A. fumigatus
• Diagnosis of sepsis
• Analysis at the time of the first blood culture collection
• Septifast (n=19), blood culture (n=8), and both (n=7)
• Higher sensitivity for C. albicans and lower for C. glabrata
Bille J. Curr Opin Crit Care 2010
DETECTION OF DNA OF Candida
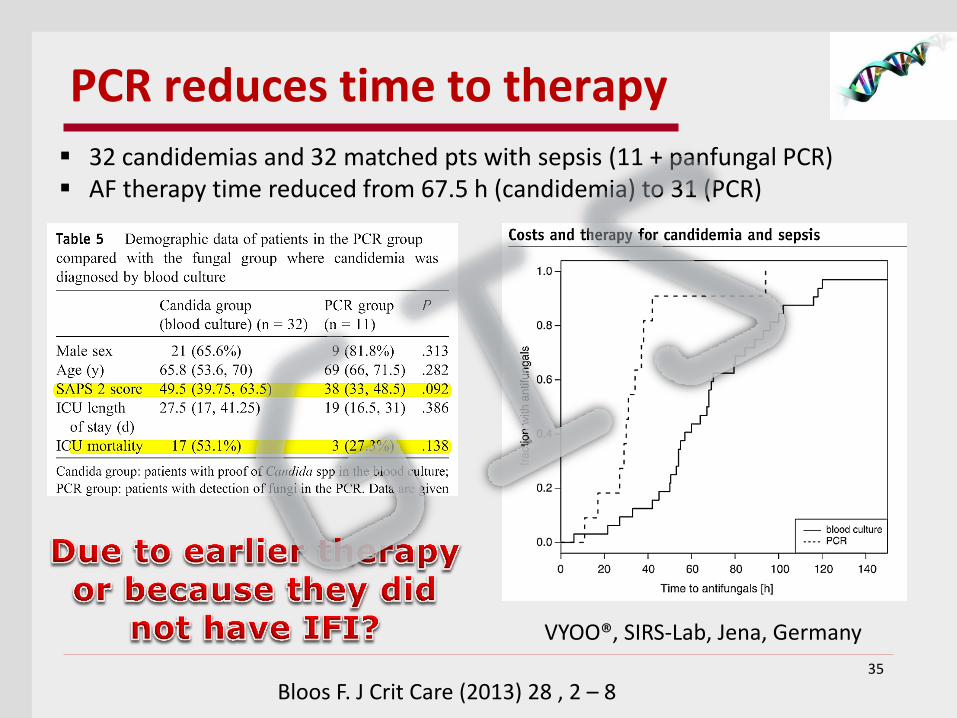
PCR reduces time to therapy
35
Bloos F. J Crit Care (2013) 28 , 2 – 8
VYOO®, SIRS-Lab, Jena, Germany
32 candidemias and 32 matched pts with sepsis (11 + panfungal PCR) AF therapy time reduced from 67.5 h (candidemia) to 31 (PCR)
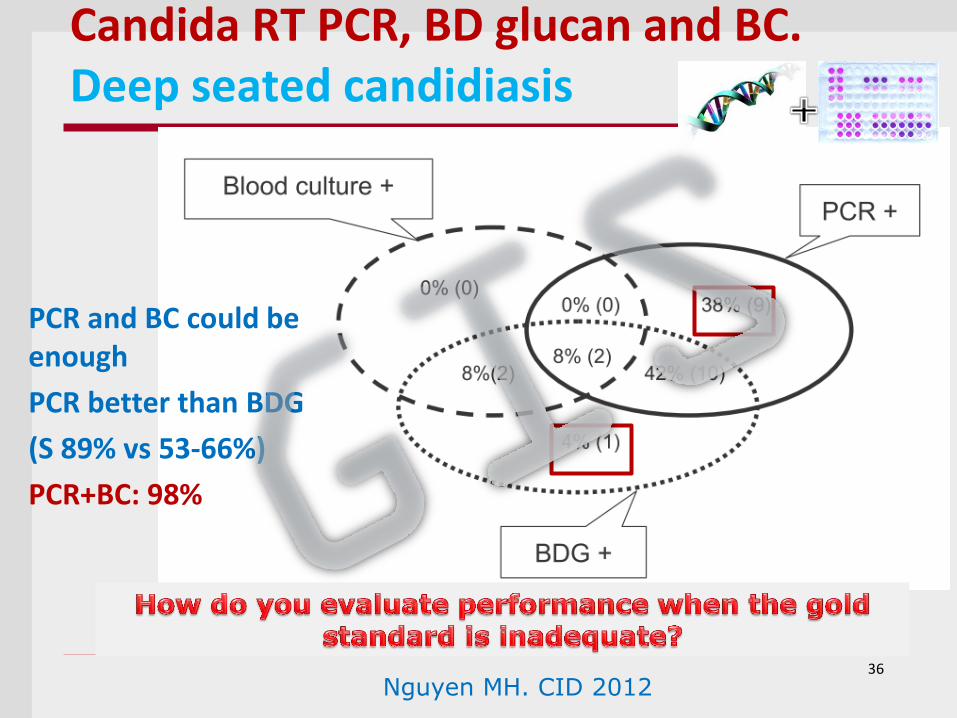
Candida RT PCR, BD glucan and BC. Deep seated candidiasis
PCR and BC could be enough
PCR better than BDG
(S 89% vs 53-66%)
PCR+BC: 98%
36
Nguyen MH. CID 2012
40 healthy controls and 63 ICU patients with suspected IC (27 later confirmed)
21 candidaemias (16 CR and 5 other sources)
6 abdominal or urological IC with BC -
Samples: 0 and +2, +7, +14 and +21 d
In house MRT-PCR for C. albicans, C. parapsilosis, C. tropicalis, C. glabrata, C. krusei and C. guilliermondii
J Antimicrob Chemother 2014; 69: 3134–3141
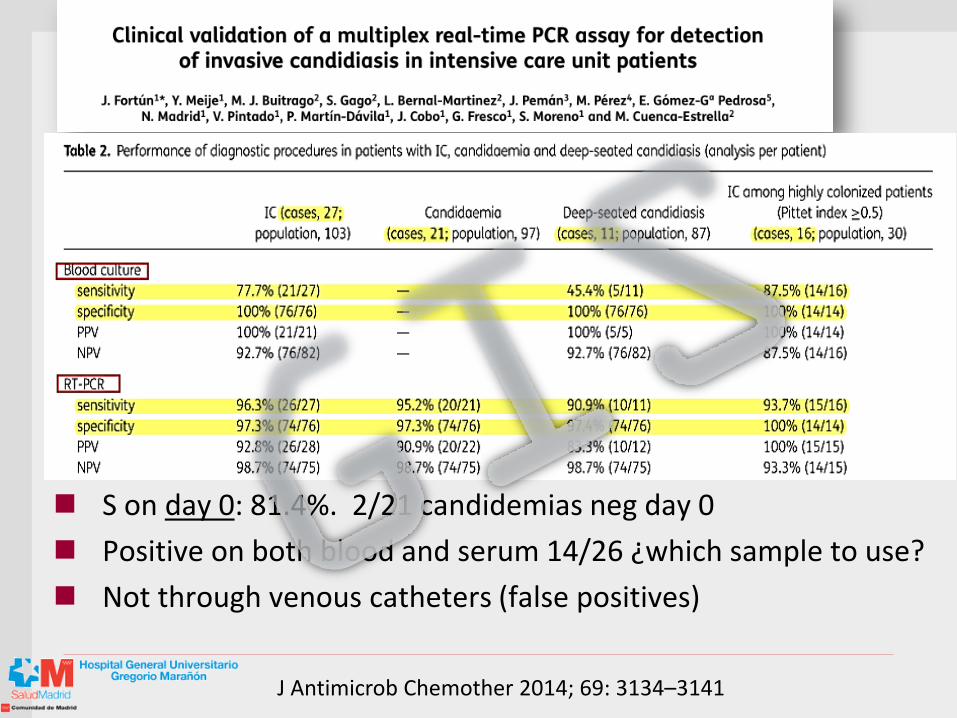
S on day 0: 81.4%. 2/21 candidemias neg day 0
Positive on both blood and serum 14/26 ¿which sample to use?
Not through venous catheters (false positives)
J Antimicrob Chemother 2014; 69: 3134–3141
T2MR is the first fully automated technology that directly analyzes whole blood specimens to identify species without the need for prior isolation of Candida species
Nanodiagnostic approach
Mylonakis E. Clin Infect Dis. 2015 Jan 12. pii: ciu959
Specificity 99.4%
Mean time to neg result:4.2 ± 0.9 hours
Sensitivity 91.1%
Mean time for detection 4.4 ± 1.0 hours
88.1% for C. krusei/C. glabrata
NPV: 99.5%-99.0% (5% and 10% prevalence)
Clin Infect Dis. 2015 Jan 12. pii: ciu959. [Epub ahead of print]
Ideas to take home
PCR and T2MRI may represents a breakthrough shift into a new era of molecular diagnostics in fungal infections. Clinical impact needs to be assessed.