Upload
landyyun-rahmawan-s
View
220
Download
0
Embed Size (px)
Citation preview
8/12/2019 New Advances
1/14
Review
New advances in molecular mechanisms and the prevention of adriamycintoxicity by antioxidant nutrients
Sergio Granados-Principal a, Jos L. Quiles b, Cesar L. Ramirez-Tortosa c, Pedro Sanchez-Rovira d,MCarmen Ramirez-Tortosa a,*
a Department of Biochemistry and Molecular Biology II, Institute of Nutrition and Food Technology Jos Mataix Verd, University of Granada, Granada, Spainb Department of Physiology, Institute of Nutrition and Food Technology Jos Mataix Verd, University of Granada, Granada, Spainc Department of Pathology, Complejo Hospitalario de Jan, Jan, Spaind Department of Oncology, Complejo Hospitalario de Jan, Jan, Spain
a r t i c l e i n f o
Article history:
Received 30 October 2009
Accepted 6 April 2010
Keywords:
Doxorubicin
Antioxidants
Toxicity
Chemoprevention
a b s t r a c t
Anthracyclines (doxorubicin, daunorubicin, epirubicin, and idarubicin) are currently the most effective
group of anti-neoplastic drugs used in clinical practice. Of these, doxorubicin (also called adriamycin)
is a key chemotherapeutic agent in cancer treatment, although its use is limited as a consequence of
the chronic and acute toxicity associated with this drug. The molecular mechanisms of doxorubicin
account for both the anti-cancer and the toxic side effects. Many antioxidants have been assayed, with
positive or negative results, to prevent the toxicity of doxorubicin. The present review has two main
goals: (1) to report the latest findings regarding the molecular mechanisms of doxorubicin toxicity; (2)
to update our understanding of the role of natural antioxidants in preventive therapy against doxorubi-
cin-induced toxicity. This review provides new evidence for the chemoprevention of doxorubicin toxicity,
making use of natural antioxidants in particular vitamin E, vitamin C, coenzyme Q, carotenoids, vitamin
A, flavonoids, polyphenol, resveratrol, antioxidant from virgin olive oil and selenium and offers new
insights into the molecular mechanisms of doxorubicin toxicity with respect to DNA damage, free radi-
cals and other parameters.2010 Elsevier Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1426
2. Adriamycin: molecular mechanisms and toxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1426
2.1. DNA damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1426
2.2. Mechanisms related to free radicals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1428
2.3. Other mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1428
3. Natural antioxidants: advances in the prevention of adriamycin toxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1429
3.1. Vitamin E. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1429
3.2. Vitamin C. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14313.3. Carotenoids and vitamin A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1431
3.4. Coenzyme Q. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1431
3.5. Flavonoids, polyphenols, and other natural antioxidants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1432
3.6. Antioxidant compounds from virgin olive oil . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1433
3.7. Selenium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1434
0278-6915/$ - see front matter 2010 Elsevier Ltd. All rights reserved.doi:10.1016/j.fct.2010.04.007
Abbreviations: AP-1, activator protein-1; Ca2+, calcium; CBR1, carbonyl reductase1; CDK, cyclin dependentkinase; CoQ, Coenzyme Q; DOX, doxorubicin; ERK, extracellular
signal-regulated kinase; H2O2, hydrogen peroxide; HO, hydroxyl radical; iNOS, inducible nitric oxide synthase; IU, international units; LDL, low density lipoprotein; MMP,
matrix metalloproteinase; monoHER, 7-monohydroxyethylrutoside; MPT, mitochondrial permeability transition; NF-jB, nuclear factor kappa B; NOX, NAD(P)H oxidase;O2, superoxide radical; ONOO, peroxynitrite; P-gp, P-glycoprotein; RNS, reactive nitrogen species; ROS, reactive oxygen species; TNF, tumour necrosis factor; TOP2,
topoisomerase II.
* Corresponding author. Address: Instituto de Nutricin y Tecnologa de Alimentos Jos Mataix Verd, Universidad de Granada, Centro de Investigacin Biomdica,
Parque Tecnolgico de Ciencias de la Salud, Avenida del Conocimiento s/n, 18071 Granada, Spain. Tel.: +34 958241000x20316; fax: +34 958819132.
E-mail address: [email protected](MCarmen Ramirez-Tortosa).
Food and Chemical Toxicology 48 (2010) 14251438
Contents lists available at ScienceDirect
Food and Chemical Toxicology
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / f o o d c h e m t o x
8/12/2019 New Advances
2/14
4. Summary and conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1435
Conflict of Interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1435
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1435
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1435
1. Introduction
Chemotherapy is based on the systemic use of drugs with cyto-
toxic activity against cells presenting high proliferation rates, in
the hope of slowing or halting the progression of the primary or
distal tumour (metastasis). The main problem posed by these
drugs is that they target not only the tumour, but also other cells,
thus causing the same damage to both abnormal and normal cells.
Therefore, they are normally only used for treating patients who
fail to respond to other measures or who are not suitable candi-
dates for surgery or primary radiotherapy (Sausville and Longo,
2009).
The cell cycle has been targeted for many years, using various
approaches, such as CDK inhibitors. These inhibitors trigger cell cy-
cle arrest and could induce apoptosis, as occurs with flavonoids.Phase nonspecific agents such as anthracyclines can damage DNA
at any phase but especially at the G2/M phase, before cell division
(Sausville and Longo, 2009).
Chemotherapeutic agents can be grouped into three general
categories: those that influence DNA, microtubules, and those with
effects at the molecular level. On the basis of the mode of action,
these agents can be classified into: (a) DNAdrug direct interaction
(forming DNA covalent adducts) or alkylating agents (cyclophos-
phamide, cysplatin, etc.); (b) anti-neoplastic antibiotics and
topoisomerase poisons (actinomycin D or anthracyclines like doxo-
rubicin, daunorubicin or epirubicin); (c) antimetabolites or DNA
function indirect effectors (5-fluorouracil, metotrexate, etc.); (d)
mitotic spindle inhibitors or anti-mitotic agents (vincristine, vin-
blastine, or taxanes like paclitaxel, docetaxel, etc.); (e) agents tar-geting molecules (bexarotene, which selectively activates retinoid
receptors, or lapatinib, which inhibits HER2 and EGFR) (Li et al.,
2008; Sausville and Longo, 2009).
In contrast to other types of epithelial origin malignant tu-
mours, some cancers, such as breast cancer, respond to various
chemotherapeutic substances, such as anthracyclines, taxanes,
antimetabolites and alkylating agents (Sausville and Longo,
2009). The most effective chemotherapy regimens are those con-
taining anthracyclines, and their efficiency is greater when tamox-
ifen is administered after chemotherapy (Early Breast Cancer
Trialists Collaborative Group, 2005).
Taking into account the above, this review focuses on adriamy-
cin toxicity, molecular mechanisms and preventive therapy, aim-
ing to identify the role of certain antioxidants in preventing thetoxic side effects of this drug.
2. Adriamycin: molecular mechanisms and toxicity
Adriamycin, also called doxorubicin (DOX), is an antibiotic
anthracycline that was isolated from a pigment of Streptomyces
peacetius in the early 1960s but which is now chemically synthes-
ised. Having been employed for more than 30 years in the battle
against cancer, DOX is essential in treating breast and oesophageal
carcinomas, solid tumours in childhood, osteosarcomas, Kaposis
sarcoma, soft tissue sarcomas, and Hodgkin and non-Hodgkin lym-
phomas (Minotti et al., 2004; Quiles et al., 2006).
Anthracyclines (doxorubicin, daunorubicin, epirubicin, and ida-
rubicin) are the most effective anti-neoplastic family in currentclinical practice. Specifically, DOX is a key chemotherapeutic drug
for cancer treatment, although its use is limited by the chronic andacute toxic side effects it produces (Quiles et al., 2006). Acute side
effects related to intravenous injection of DOX appear within min-
utes after infusion, including nausea, vomiting, myelosuppression
and arrhythmia. On the other hand, chronic effects may develop
several weeks or even months after the recurrent administration
of the drug, provoking heart, liver, brain or kidney injury. Since
cardiomyocytes, as well as neurons, are post-mitotic cells, the vast
majority of the damage is irreversible, and unalterably affects
cardiac and brain functions. Furthermore, heart repercussions are
even more prevalent because of this organs greater sensitivity to
damage induced by free radicals, given the high oxidative
metabolism of the heart and its lower level of antioxidant defences.
Adriamycin-related cardiotoxicity may cause dose-dependent car-
diomyopathy and congestive heart failure; moreover, persistentchanges of cognitive function (memory and concentration loss
and difficulty of performing multiple tasks) may occur (Chen
et al., 2007; Quiles et al., 2006).
Dosage-dependent chronic cardiomyopathy associated with
DOX administration generates marked hypotension, tachycardia,
cardiac dilatation and ventricular failure. At the serum level, in-
creased glutamate oxalacetic transaminase, lactate dehydrogenase,
and creatinine phosphokinase enzyme activities have been noted.
At the ultrastructural level, myofibril loss, mitochondrial swelling,
cytoplasmatic vacuolization, and an increased number of lyso-
somes have been reported (Bertinchant et al., 2003; Quiles et al.,
2002). Toxicity associated with DOX therapy in the brain is due
to the indirect action of the drug, because it is not able to cross
the bloodbrain barrier. DOX raises circulating levels of tumournecrosis factor (TNF)-a, which can cross this barrier, reachingand activating glial cells to initiate the local production of TNFaand raise its circulating levels. This TNFa induces the local gener-ation of reactive nitrogen species (RNS) through nitric oxide syn-
thase induction, and therefore intensifies the oxidative stress
responsible for brain injury (Chen et al., 2007).
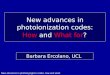
Molecular mechanisms of DOX account for both its anti-cancer
and its toxic effects (in the heart, brain, kidney, etc.). DOX acts at
two fundamental levels: altering DNA and producing free radicals;
in this respect, too, other mechanisms have been studied ( Fig. 1).
2.1. DNA damage
Anthracyclines, such as DOX, are known as topoisomerase II(TOP2) poisons. DOX can block the synthesis of DNA by intercalat-
ing into the DNA strand; moreover, it inhibits TOP2. This enzyme
modifies DNA topology without altering the structure and se-
quence of deoxynucleotides, causing transient double strand DNA
breaks and then modulating DNA supercoiling. Thus, a suitable
state of DNA is achieved for different cell cycle phases and tran-
scriptional activity (Quiles et al., 2002, 2006). To provoke this
DNA injury, DOX must cross into the cancer cell cytoplasm by sim-
ple diffusion and become bound to the 20S proteosomal subunit,
forming a complex that translocates into the nucleus, where the
complex is dissociated and DOX binds to DNA. Moreover, DOX is
able to bind toTOP2, stabilizing an intermediate reaction in which
the DNA strands are cut and covalently linked to tyrosine residues
ofTOP2, creating a ternary complex DOXDNATOP2 that disturbsthe DNA structure and impedes its synthesis (Minotti et al., 2004).
1426 S. Granados-Principal et al. / Food and Chemical Toxicology 48 (2010) 14251438
8/12/2019 New Advances
3/14
DOX is known to be most effective when cells are rapidly prolifer-
ating and expressing high levels ofTOP2. Nevertheless, after treat-
ment with adriamycin, TOP2 undergoes down-regulation. It has
been postulated that such down-regulation may be a major cause
of subsequent chemo-resistance. It is now known that this down-
regulation ofTOP2provoked by DOX is due to the repressive effect
of the transcriptional activator Sp3, while the transcriptional acti-
vator Sp1 is reduced during the cell cycle arrest (Williams et al.,
2007).
It is widely accepted that DNA damage is an early importantevent that takes place in doxorubicin-induced cardiac myocyte
death, where the activation and accumulation of p53 and mito-
chondrial dysfunction are prominent mediators (LEcuyer et al.,
2006). In addition, DOX-mediated p53 activation reportedly leads
to apoptosis (Quiles et al., 2002). It is possible that this effect on
DNA may be related to signalling events of growth arrest and
p53activation; in fact, this activation leads to apoptosis depending
on the tumour and competent p53 status. In this case, proficient
and deficient cells suffer similar rates of damage, becausep53defi-
cient cells have more TOP2 (expressed in the S phase of the cell cy-
cle), and so there are more DNA intercalations. While present in
p53 proficient cells, this tumour suppressor blocks the ligase
capacity of TOP2 and augments the irreversible breakage of DNA
strands. Such genetic disturbances, together with the activationof tumour suppressor p53, and other additional mechanisms, are
responsible for the apoptosis induced by adriamycin. Among those
additional mechanisms, DOX can trigger apoptosis by producing
ceramide (which prompts apoptosis by activating p53 or other
downstream pathways such asJNK), the degradation of Akt by ser-
ine threonine proteases, the mitochondrial release of cytochrome c,
increased FasL (death receptor Fas/CD95 ligand) mRNA production
(Minotti et al., 2004; Ozben, 2007; Quiles et al., 2002, 2006), and a
greater production of free radicals (Chen et al., 2007). It has re-
cently been discovered that DOX-promoted DNA damage triggers
the accumulation of p53 protein in cardiomyocytes through theprior induction of the ATM kinase (Yoshida et al., 2009). The latter
authors also reported p53-dependent cardiomyocyte apoptosis
during chronic cardiotoxicity in p53 heterozygous knockout mice
(Yoshida et al., 2009). Acute DOX-led cardiotoxicity is mediated
by the inhibitory effect of p53 on mTOR (mammalian target of rap-
amycin) activity, an independent effect of cardiomyocyte apoptosis
in transgenic mice (Zhu et al., 2009). Further information is avail-
able on the DOX-induced apoptosis in cardiomyocytes, since we
are now aware of the functional link between extracellular sig-
nal-regulated kinases (ERKs) and p53. This signalling pathway is
closely associated with a lower expression of Bcl-2, increases in
Bax, the activation of caspase-3, poly(ADP-ribose) polymerase
cleavage, and a collapse of mitochondria membrane potential
leading to cardiac cell apoptosis (Liu et al., 2008). The down-mod-ulation of the anti-apoptotic heme oxygenase-1 by DOX was re-
Fig. 1. Molecular mechanisms of doxorubicin toxicity. The main events are: (1) DNA damage, (2) production of free radicals and (3) other mechanisms.
S. Granados-Principal et al./ Food and Chemical Toxicology 48 (2010) 14251438 1427
8/12/2019 New Advances
4/14
cently considered as a ROS-independent cardiomyocyte apoptosis
triggered by exposure to low doses of the drug (Bernuzzi et al.,
2009).
The generation of DNA adducts is another genotoxic mechanism
of DOX, and free radicals originated by DOX are deeply involved.
These radicals promote lipid peroxidation and therefore malondi-
aldehyde production, which reacts with exocyclic amino groups
of deoxyguanosine, deoxyadenosine and deoxycytidine to formalkylated adducts. Furthermore, several types of oxidative injury
in nitrogen bases such as 4,6-diamino-5-formamido-pyrimidine
(FapyAde) or 5-(hydroxymethyl)uracil (5-OH-MeUra) have been
demonstrated. These oxidative adducts are highly mutagenic prod-
ucts that block DNA replication and augment the reading error fre-
quency by DNA polymerase. Moreover, DOX can produce
complexes with formaldehyde through NAD(P)H oxydoreductase
systems and transition metals. Such complexes form covalent links
with DNA and, depending on the intercalation region, can also form
more or less stable intercalations or more stable DNA cross links
(Minotti et al., 2004). A consequence that is probably related to
these cross links is the impossibility of helicase enzymes separat-
ing the DNA strands and interfering with its unwinding, but this ef-
fect might also be due to the direct action of DOX on helicases
(Minotti et al., 2004; Quiles et al., 2002, 2006).
2.2. Mechanisms related to free radicals
The production of free radicals and oxidative stress is closely in-
volved with DOX action, regarding both anti-tumour and toxic ef-
fects. There are four different modes of free radical production by
adriamycin:
(1) Production of semiquinone: DOX is transformed into a semi-
quinone free radical through electron reduction by various
NAD(P)H-dependent reductases in the complex I of the elec-
tron transport chain (cytochrome P-450 reductase). This
semiquinone reacts with molecular oxygen to produce the
superoxide radical (O2
) and it converts DOX into quinone.This quinonesemiquinone cycle generates large amounts of
O2, which subsequently give rise to ROS and RNS species
such as hydrogen peroxide (H2O2), hydroxyl radical (HO)
or peroxynitrite (ONOO) (Chen et al., 2007; Quiles et al.,
2006).
(2) Activation of NAD(P)H oxidases (NOXs): DOX activates NOXs,
which give rise to free radicals that participate in activating
the apoptotic pathway in cardiac cells (Gilleron et al., 2009).
NOX activation may generate ONOO through the mitochon-
drial production of ROS as O2 and the reaction with nitric
oxide (Kimura et al., 2005). ONOO also activates matrix
metalloproteinases (MMPs); these proteases have been
implicated as a major mechanism of the peroxynitrite-
dependent cardiotoxicity of DOX (Bai et al., 2004).(3) Non-enzymatic mechanism: DOX interferes with non-enzy-
matic metabolic reactions in which iron is involved, and
leads to ROS production. Thus, the DOX semiquinone, O2,
and H2O2, can promote the release of iron from ferritin and
cytoplasmic aconitase, thus altering iron metabolism. Subse-
quently, iron can react with DOX and subsequently produce
HO (Chen et al., 2007; Minotti et al., 2004).
(4) Products from the metabolism of DOX: this metabolism leads
to ROS production. On the one hand, the side chain carbonyl
group of the carbon 13 in DOX is converted into a hydroxyl
group by aldoketo reductases, giving rise to a secondary
alcohol (doxorubicinol), which can release iron from cyto-
plasmic aconitase, disturbing the iron metabolism and,
therefore, causing oxidative stress. On the other hand, itcan be metabolised into a lipophilic aglycone capable of dif-
fusing through the mitochondrial membrane and accumu-
lating within it. This aglycone is the starting point for
several reactions that release electrons, producing ROS and
disturbing the functional integrity of the respiratory chain
(Chen et al., 2007).
All the oxidative mechanisms described above are triggered by
DOX to induce cancer cell death and toxic effects in cardiac myo-cytes. Moreover, it is important to take into account that the heart
is very rich in mitochondria. DOX has the ability to modify the
chemical composition, structure and function of biological mem-
branes, mainly at the mitochondrial level, fundamentally due to
the peroxidation generated by DOX (Huertas et al., 1991a,b,
1992). It has been reported that phospholipid peroxidation in-
duced by DOX can cause an exchange of mitochondrial and micro-
somal cholesterol with exogenous pools (Huertas et al., 1992). The
mitochondria contain a phospholipid, cardiolipin, in their inner
membrane, and DOX has a high affinity for this cardiolipin, which
results in the accumulation of adriamycin inside cardiac cells
(Quiles et al., 2002, 2006). This effect may be enhanced by a highly
unsaturated diet, producing a cardiolipin that is very rich in highly
peroxidisable unsaturated fatty acids (Huertas et al., 1991b).Ber-
thiaume and Wallace (2007b) reported a gene expression profile
in the heart of male rats treated with 6 weekly injections of
2 mg/kg DOX followed by a 5-week drug free period. Several path-
ways are closely related to mitochondria, including glycolysis and
fatty acid metabolism, which supports the hypothesis that these
organelles are key targets in DOX toxicity. The same authors
(Berthiaume and Wallace, 2007a) also reviewed the importance
of the mitochondrion in DOX cardiotoxicity, this being an impor-
tant target of this chemotherapeutic drug, which induces ROS pro-
duction due to the adriamycin redox cycling at complex I of the
electron transport chain. This oxidative damage can impair both
short and long term mitochondrial functioning, causing reduced
energy production, oxidation of the mitochondrial DNA and loss
of mitochondrial membrane potential by generating mitochondrial
permeability transition (MPT) pores. It has been suggested that theadenine nucleotide translocator may be the principal component
of those MPT pores, and the concentration of this protein has been
shown to diminish after DOX administration, thus aggravating
mitochondrial dysfunction (Oliveira and Wallace, 2006). In addi-
tion to these events, a decrease in other mitochondrial components
such as coenzyme Q (CoQ) has been reported, as a consequence of
the oxidative stress associated with the administration of DOX
(Huertas et al., 1991a).
2.3. Other mechanisms
Treatment with DOX also causes various disturbances related to
cardiotoxicity, as occurs with alterations in calcium (Ca2+) metab-olism. Such alterations include an increase in intracellular Ca2+,
accumulating in the ventricular myocardium, and even in the
mitochondria, producing transport anomalies in cardiac tissue
and in the Ca2+ release function of the sarcoplasmic reticulum by
affecting the ionic channels (Quiles et al., 2006). Changes in Ca2+
by DOX are also exerted at the muscle response level. It has been
reported that these disturbances in Ca2+ upset the balance in the
response of myotubes and thus disrupt skeletal muscle relaxation
and restrict contraction (van Norren et al., 2009).
The cardiomyopathy created after chronic administration of
DOX displays a down-regulation of the calcium/calmodulin-depen-
dent protein kinase II mRNA. This is correlated with cardiac func-
tion depletion, the reduced expression of sarcomeric proteins,
and greater tissue injury (Little et al., 2009). The use of adenosineA3agonists restores Ca
2+ homeostasis and prevents mitochondrial
1428 S. Granados-Principal et al. / Food and Chemical Toxicology 48 (2010) 14251438
8/12/2019 New Advances
5/14
damage that can occur as a result of Ca2+ overload being able to re-
verse the cardiac toxicity (Emanuelov et al., 2009).
Another possible mechanism of DOX toxicity is related to alter-
ations in the metabolism of prostaglandins (Quiles et al., 2006).
The endocannabinoid system has recently been reported to
have a putative role in DOX-induced cardiotoxicity, since the use
of cannabinoid-1-receptor antagonists can reverse the cardiode-
pressive effects of endocannabinoids (Mukhopadhyay et al.,2007). As stated above, MMPs are involved in the mechanism of
the peroxynitrite-dependent cardiotoxicity of DOX (Bai et al.,
2004). Mukhopadhyay et al. (2009) recently demonstrated in-
creases in matrix MMP-2 and MMP-9 gene expression in the cardiac
cells of mice.
Overall, DOX-induced cardiotoxicity has been attributed to sev-
eral events that are probably linked to elevated ROS and risk of oxi-
dative injury. Such effects include mitochondrial dysfunction,
disruption of the sarcoplasmic reticulum function, the direct inhi-
bition of key transporters involved in ion homeostasis, apoptotic
cell loss, and alterations in cellular iron and calcium metabolism
(Berthiaume and Wallace, 2007a). At the brain level, Cardoso
et al. (2008) have reported with respect to experiments on rats that
DOX treatment (2 mg/kg) increases the susceptibility of brain
mitochondria to Ca2+-induced permeability transition pore open-
ing and oxidative stress, predisposing brain cells to degeneration
and death.
3. Natural antioxidants: advances in the prevention of
adriamycin toxicity
This therapy consists in the use of substances or strategies to
protect against or prevent the toxic effects of adriamycin. There
are several ways to achieve this, for example by optimising the
dosage pattern (Chen et al., 2007). Nonetheless, the goal is a diffi-
cult one because even doses of doxorubicin lower than a cumula-
tive dosage of 450550 mg/m2, through continuous infusion, canelevate the risk of cardiotoxicity (Verma et al., 2008). Another
strategy to reduce cardiac toxicity involves the synthesis and use
of DOX analogues with equivalent activity but less toxicity. All
these procedures are intended to reduce levels of DOX-induced
free radicals. In this sense, dexrazoxane is able to chelate the free
iron ions released by DOX, thereby diminishing reactions involving
adriamycin and iron to produce ROS (Chen et al., 2007; Della Torre
et al., 1999a,b; Minotti et al., 2004; Xiang et al., 2009).
Because of their clinical and social relevance, we focus on the
use of various compounds derived from the human diet that have
been demonstrated to protect against adriamycin toxicity, mainly
through their high antioxidant capacity. There is some controversy
surrounding the use of antioxidants either combined with DOX or
previously administered, to prevent the toxic effects of adriamycin.It has been postulated that different antioxidant compounds can
diminish the anti-tumour activity of DOX, by eliminating the oxi-
dative component connected with the toxic and anti-neoplastic ac-
tions, and thus protecting from the side effects but reducing the
efficacy of the drug. Nevertheless, a growing number of authors be-
lieve that drugs such as anthracyclines can exert an effect by addi-
tional forms of oxidative stress. Therefore, these antioxidants
would not diminish the efficacy of DOX, but rather they would pre-
vent some of its toxic side effects. Such claims need to be clarified,
because there are antioxidant compounds that act in synergy with
DOX activity and also weaken its toxicity (Ozben, 2007).
The present review is exclusively focused on the antioxidants
that are derived from the diet, such as vitamin E, vitamin C, carote-
noids, vitamin A, coenzyme Q, flavonoids, antioxidant componentsof virgin olive oil, and selenium. The antagonistic effects of these
antioxidant compounds on the toxicity induced by DOX are sum-
marised inTable 1.
3.1. Vitamin E
Vitamin E has a high antioxidant capacity and plays a funda-
mental biologic role, especially in protecting cells and tissues from
oxidative damage, and membrane lipid and lipoprotein peroxida-tion (Quiles et al., 2002, 2006). In general, preclinical studies in ro-
dents have shown that oral vitamin E tends to increase anti-
tumour actions and protects against the toxic effects of DOX
(Quiles et al., 2006); nevertheless, it has been reported that both
vitamins E and C can increase the expression of P-glycoprotein
(P-gp) and ofhypoxia inducible factor-1alpha in Nox-1overexpress-
ing prostate tumour cells (Wartenberg et al., 2005). Therefore,
these vitamins might fortify resistance to chemotherapy, although
this proposal needs to be more extensively studied. As a beneficial
agent, vitamin E has been found to lengthen the life span of labo-
ratory animals and to diminish the weight loss provoked by che-
motherapy. Moreover, this antioxidant can protect from both
acute and chronic cardiotoxicity caused by DOX, and it increases
antioxidant capacity in the heart (Quiles et al., 2006). With the
aim of testing the cardioprotective effect of vitamin E in doxorubi-
cin-induced acute cardiotoxicity in rats, Puri et al. (2005) pre-
treated them with a high dose of vitamin E intraperitoneally
followed by DOX. The results show that vitamin E pre-treatment
prevents the electrocardiographic changes caused by doxorubicin;
moreover, it helps to lower the levels of creatine phosphokinase
and lactate dehydrogenase raised by DOX. As seen above, adriamy-
cin can provoke mitochondrial permeability transition pores, thus
causing a loss of mitochondrial membrane potential (Berthiaume
and Wallace, 2007a). In this sense, it has been reported that dietary
vitamin E decreases doxorubicin-induced oxidative stress in rats
and enriches cardiac mitochondrial membranes witha-tocopherol,but it cannot prevent the mitochondrial dysfunction caused by
chemotherapeutics (Berthiaume et al., 2005). It seems that the dos-
age and treatment schedule of vitamin E are important if it is to ex-ert a preventive role. Thus, Bjelogrlic et al. (2005) found no
inhibition of DOX-induced acute cardiotoxicity in mice after a sin-
gle dose of oral vitamin E (100 IU/kg). On the other hand, chronic
supplementation with vitamins E and C (400 IU/kg/day and
250 mg/kg/day, respectively) for 30 days in rats reversed the
changes in alanine aminotransferase, lactate dehydrogenase, urea
and creatinine caused by DOX administration, enhancing the sur-
vival rates of the rats (Santos et al., 2007).
At high doses (>90 mg/kg), vitamin E also reduces lipid peroxi-
dation and chromosomal aberrations, the best results being ob-
tained with a dose of 100 mg/kg per body weight in rat bone
marrow cells. It has also been reported that this antioxidant allevi-
ates DOX-induced nephrotoxicity and has positive effects against
skin ulcerations by weakening ulcer aggressiveness and accelerat-ing skin regeneration. In sharp contrast, clinical studies suggest
that vitamin E does not protect against chronic cardiotoxicity in-
duced by DOX, and provides only slight protection against acute
cardiotoxicity (Conklin, 2000; Quiles et al., 2002, 2006). Little evi-
dence has been published in the last five years on the preventive
role of vitamin E against DOX-induced nephrotoxicity. It has been
reported that the intraperitoneal administration of combined vita-
min E and N-acetyl-cysteine (50 mg/kg) 1 day before doxorubicin
counteracts the damage caused by DOX in the rat kidney. Such
combined preventive therapy depresses lipid peroxidation, pre-
vents necrosis caused by DOX, and maintains the activities of the
enzymes superoxide dismutase, catalase, glutathione peroxidase,
glutathione reductase, glucose-6-phosphate dehydrogenase and
glutathione-S-transferase (Kalaiselvi et al., 2005). A surprisingstudy reported that vitamin E (1lg/ml) could make embryonic
S. Granados-Principal et al./ Food and Chemical Toxicology 48 (2010) 14251438 1429
8/12/2019 New Advances
6/14
kidney cells more sensitive to genotoxic insults from doxorubicin
by preventing the p53 unfolded isoform. The authors speculatedthat this effect could result from vitamin E reversing the ROS pro-
duction induced by pre-treatment with b-amyloid peptide (Uberti
et al., 2007). In terms of the liver, a study using rats showed thatintraperitoneal vitamin E (100 mg/kg/day) for eight days inhibits
Table 1
Effects of antioxidants on toxicity induced by DOX.
Compound Effects against the action of DOX Organs protected
against DOX toxicity
Effects over
chemo-resistance
Therapeutic
efficacy of DOX
Vitamin E
Decreases ROS Heart Increased Affected?
Lipid peroxidation Liver
Chromosomal aberrations Kidney
Skin ulcerations SkinSerum markers of toxicity
Prevents ECG changes
Increases Skin regeneration
HIF-1aP-gp
Vitamin C
Decreases ROS Heart (weak) Increased Not affected or decreased?
Lipid peroxidation Liver (weak)
Increases P-gp
Carotenoids:b-carotene, lycopene
Decreases ROS Heart unknown Increased (b-carotene)
Lipid peroxidation Kidney
Normalizes the histopathology, and the serum
and tissue markers of toxicity
Vitamin A
Decreases ROS Heart unknown Not affected
Lipid peroxidation Kidney
Chromosomal aberrations Liver
Bone marrow
Brain
Coenzyme Q
Decreases ROS Heart unknown Not affected
Lipid peroxidation
Protects the MTC
Flavonoids: monoHER, catechines, quercetin, ginestein
Iron chelators Heart Reduced Increased
Decreases ROS Liver
Lipid oxidation
Apoptosis of myocytesEfflux pumps
Increases Accumulation of DOX inside the cells
Garlic
Decreases ROS Heart Reduced Increased
Myocardial TNFaP-gp
Polyphenols: curcumin, resveratrol
Decreases ROS Heart Reduced Increased
Lipid oxidation Liver
Protection of membranes Kidney
Efflux pumps
Increases Accumulation of DOX inside the cells
Antioxidant enzymes
Oleuropein from olive oil
Decreases ROS Heart unknown unknown
Lipid and protein oxidation
Serum markers of toxicity
Vacuolisation in myocytes
Restores the distressed energy metabolic
pathways
Selenium
Decreases ROS Heart unknown Increased
Liver (weak)
Increases Antioxidant enzymes Kidney (weak)
Abbreviations:DOX: doxorubicin; ECG: electrocardiogram; HIF-1a: hypoxia inducible factor-1alpha; monoHER: 7-monohydroxyethylrutoside; MTC: mitochondrial transportchain;P-gp:P-glycoprotein; ROS: reactive oxygen species; TNFa: tumour necrosis factor alpha.
1430 S. Granados-Principal et al. / Food and Chemical Toxicology 48 (2010) 14251438
8/12/2019 New Advances
7/14
the general toxic and hepatotoxic effects of DOX (Gokcimen et al.,
2007). Similar results were previously obtained by other authors,
who reported that both intravenous vitamin E (200 IU/kg/week)
and intraperitoneal catechin (200 mg/kg/week) for 6 weeks signif-
icantly reduced doxorubicin-induced hepatotoxicity in rats, by
decreasing malondialdehyde, glutathione peroxidase and catalase
activities (Kalender et al., 2005).
In this context, the vast majority of studies have focused on theeffects of vitamin E against DOX-induced cardiotoxicity, although
several have examined other toxic effects. Thus, topical vitamin E
was tested against DOX-induced oral mucositis in paediatric oncol-
ogy. To this end, 2 ml of vitamin E (800 mg ofDL-a-tocopheryl ace-tate diluted with corn oil) was orally administered 24 h after
doxorubicin administration, once daily for 2 weeks. The results ob-
tained show that topical vitamin E does not reduce mucositis in
children receiving doxorubicin as chemotherapy, and the authors
concluded that it should not be used in the clinical context for this
purpose (Sung et al., 2007).Branda et al. (2006)found no mitigat-
ing effect on DOX-induced leucopoenia by dietary vitamin E, either
at low (50 mg/kg) or high (750 mg/kg) doses in rats. Such lack of
effect of vitamin E did not occur with other chemotherapeutic-in-
duced leucopoenia drugs such as docetaxel or cyclophosphamide,
but in the latter case the effect of dietary vitamin E appears to be
dose-dependent.
3.2. Vitamin C
Vitamin C (ascorbic acid) is an effective water soluble antioxi-
dant against lipid peroxidation, scavenging ROS in the aqueous
fraction before these molecules can give rise to lipid oxidation
(Conklin, 2000). An intervention review by van Dalen et al.
(2008) showed that none of the individual studies carried out dem-
onstrated a cardioprotective effect by vitamin C combined with
vitamin E, mainly administered by oral supplementation. Preclini-
cal studies have provoked some controversy about the effects of
vitamin C on the anti-tumour activity of DOX; nevertheless, the
overall view is that ascorbic acid does not increase the anti-neo-plastic action of adriamycin. However, it can lengthen the life span
of laboratory animals and reduce the toxic effects of DOX. This con-
troversy is probably due to the pro-oxidant effect of vitamin C at
high doses (Conklin, 2000; Quiles et al., 2002, 2006). Despite the
controversy, vitamin C is commonly used to compare the protec-
tive activity of other compounds against the toxic effects of DOX.
These kinds of studies still find vitamin C to be a weak protector
against cardiotoxicity and hepatotoxicity in orally supplemented
rats (100 mg/kg/week for 3 weeks) (Injac et al., 2009), H9c2 cardio-
myocytes (Choi et al., 2007; Chularojmontri et al., 2005; Kim et al.,
2006), cardiac myocytes of adult rats (Wold et al., 2005) and in
myocytes of neonate rats (Yamanaka et al., 2003). AlthoughWatt-
anapitayakul et al. (2005) reported that ascorbic acid registers
modest activity in protection against doxorubicin-induced cyto-toxicity by screening several herbal antioxidants in H9c2 cardio-
myocytes, there are several indications that the use of vitamin C
to prevent the toxic effects of DOX may not be an effective choice.
In this sense, a recently published article on mice with lymphoma
cell-derived xenogeneic tumours shows that ascorbic acid
(250 mg/kg dehydroascorbic acid by tail vein) significantly reduced
the therapeutic efficacy of several anti-neoplastic drugs (doxorubi-
cin, cisplatin, vincristine, methotrexate and imatinib). Vitamin C
caused a dose-dependent decrease in apoptosis in cells treated
with anti-tumour drugs, an effect not caused by vitamin C reten-
tion modulated by chemotherapeutics, the antioxidant activity of
ascorbic acid, or the up-regulation of P-gp (Heaney et al., 2008).
This conclusion is corroborated by the fact that vitamin C (at a final
concentration of 10 mmol/l) can decrease the accumulation ofadriamycin in human ovarian carcinoma cells 3AO exposed to
ultrasounds (Yu et al., 2003). Wartenberg et al. (2005)reported
that ascorbic acid raised the expression ofP-gp, a multidrug resis-
tance transporter, in Nox-1 overexpressing prostate tumour cells.
3.3. Carotenoids and vitamin A
Carotenoids such as b-carotene can reduce the lipid peroxida-
tion associated with DOX and augment the anti-tumour effect ofthis drug (Conklin, 2004). Oral supplementation with lycopene
(5 mg/kg/day for 7 weeks), the carotenoid presenting the most
powerful antioxidant activity, has demonstrated a cardioprotective
effect at the myocyte level in rats treated with DOX (4 mg/kg)
intraperitoneally by weeks 3, 4, 5 and 6, but it fails to prevent adri-
amycin-induced cardiac dysfunction (Anjos Ferreira et al., 2007).
Moreover, it has been reported that a tomato oleoresin supplement
containing lycopene (95%), all-trans-b-carotene (5%), and 13-cis-b-
carotene (1%), reduces cardiomyocyte oxidative DNA damage
caused by doxorubicin in rats (Ferreira et al., 2007a). The same
authors reported that DOX maintains levels of lycopene in the
myocardial tissue of rats, and at the same time it raises the antiox-
idant capacity of this tissue. This suggests DOX has an antioxidant
more than a pro-oxidant effect (Ferreira et al., 2007b). The protec-
tion exerted by lycopene against DOX-induced heart and kidney
damage was studied by Yilmaz et al. (2006). Lycopene (4 mg/kg)
was orally administered for 10 days before DOX injection (10 mg/
kg) (pre-treatment group) and for 2 days before and 3 days after
the administration of adriamycin (post-treatment group). The re-
sults show that the lycopene group had higher levels of malondial-
dehyde and lower levels of glutathione, with normalized catalase
activity in heart and kidney tissues. This group also presented nor-
malized levels of plasmatic creatinine and urea, and a normal his-
topathology in heart and kidney tissues. Similar results were
reported for mice receiving intraperitoneal tomato extract (1.2
and 2.4 g/kg) and lycopene (1.7 and 3.5 mg/kg) and a single intra-
peritoneal injection (15 mg/kg) of DOX. Lycopene prevented the in-
crease of serum creatine kinase and ameliorated cardiac cell injury
(Karimi et al., 2005). The benefits derived from lycopene have alsobeen studied at other levels. Thus, it has been reported that pre-
treatment with intraperitoneal lycopene (4 mg/kg) significantly re-
stored malondialdehyde and lowered glutathione levels, and also
reversed the histopathology in rats treated with DOX (10 mg/kg)
(Atessahin et al., 2006). A review of this question has shown that
vitamin A (retinol and some retinol metabolites) also significantly
reduces this lipid oxidation, providing good results in the heart,
brain membranes, liver microsomes and kidney, but it does not
facilitate the anti-tumour action of adriamycin in mice (3.3 mg/
kg of retinol palmitate by intraperitoneal injection) (Quiles et al.,
2006). Vitamin A also has a protective dose-dependent effect
against the chromosomal aberrations induced by doxorubicin in
rat bone marrow cells, 15lg/kg being the most effective dose,
whereas 30lg/kg was found to be clastogenic (Glka et al., 2004).
3.4. Coenzyme Q
Coenzyme Q (CoQ), or ubiquinone, plays a critical role in the
mitochondrial respiratory chain, acting as a redox link between fla-
voproteins andcytochromes, being an essentialcomponent in extra-
mitochondrial redox chains. Its concentration in blood and tissues
depends on biologic requirements, endogenous biosynthesis, and
ofcourse thedietaryintake(Quiles et al., 2002). Due to thehighpres-
ence of CoQin themitochondria, its concentration reflects thecellu-
larcontent of mitochondriaamong differenttissues, being greater in
the heart than in the liver (fivefold more), kidney, pancreas, spleen
(10-fold more), and skeletal muscle (5% more) (Conklin, 2005).
Adriamycin induces cardiotoxicity by lipid peroxidation in cardiacmyocytes, reduces the content of CoQ10 in mitochondrial
S. Granados-Principal et al./ Food and Chemical Toxicology 48 (2010) 14251438 1431
8/12/2019 New Advances
8/14
membranes, and inhibitsthe mitochondrial biosynthesis of CoQ10 as
well as respiratory chain CoQ10-dependent enzymes(Conklin, 2000,
2004). Similar effects have been found in rats where the plasma and
mitochondria levels of CoQ10and CoQ9, respectively, were sharply
decreased by the oxidative stress generated by DOX (Huertas et al.,
1991a). Thus, preclinical studies have shown that both supplemen-
tation and treatment with CoQ10 prior to DOX administration de-
creases lipid oxidation and heart toxicity without interfering withthe anti-tumour activity of DOX. Clinical studies have also shown
oral CoQ10 to have a protective effect against the chronic cardiotox-
icity induced by adriamycin (Conklin, 2005; Quiles et al., 2006).
Bryant et al. (2007)reviewed the evidence on the clinical and cost-
effectiveness of cardioprotection against anthracycline-induced
toxiceffects,and found justone studyreporting the cardioprotective
effect of CoQ10(100 mg by oral administration twice daily) on pae-
diatric patients affected by acute lymphoblastic leukaemia or non-
Hodgkinslymphoma,treatedwith adriamycin (250 mg/m2) (Iarussi
et al., 1994). More recently, it has been shown that intraperitoneal
mitoquinone, a triphenylphosphonium-conjugated analogue of
CoQ, either alone (5 mg/kg) or combined (5 mg/kg, twice a week)
with DOX (2.5 mg/kg per week) for 12 weeks in rats, provides car-
dioprotection through a novel mechanism, involving cardiac resto-
ration by the expression ofcytochrome c oxidase subunits IIandVa,
together withthe electronparamagnetic resonancesignal, thussup-
porting the ideathat mitoquinone amelioratesDOX-inducedcardio-
toxicity (Chandran et al., 2009).
3.5. Flavonoids, polyphenols, and other natural antioxidants
Flavonoids are characterised by high antioxidant power, and
have been considered potential protectors against the chronic car-
diotoxicity associated with DOX (Quiles et al., 2002). This protec-
tive effect of flavonoids is closely related to their antioxidant,
iron chelating (Kaiserov et al., 2007) and carbonyl reductase 1
(CBR1)-inhibitory properties (Carlquist et al., 2008). The proposed
mechanism involving iron chelating and antioxidant activities in-
volves two steps: (1) iron is chelated by the flavonoid; (2) ROS pro-duction is quickly scavenged by flavonoids at the place of
generation; such a concept has been termed site-specific scaveng-
ing (Kaiserov et al., 2007). The semisynthetic flavonoid 7-mono-
hydroxyethylrutoside (monoHER) has been extensively studied as
a good cardioprotective compound, both in preclinical (intraperito-
neally administered in mice) (Abou El Hassan et al., 2003a; Bast
et al., 2007b; Bruynzeel et al., 2007d; De Celle et al., 2004) and in
clinical trials (Bruynzeel et al., 2007c; Willems et al., 2006) after
intravenous injection. This flavonoid inhibits negative cardiac ef-
fects in a dose-dependent manner, in accordance with the essential
properties of all flavonoids, i.e. their iron chelating and antioxidant
characteristics. MonoHER reduces lipid peroxidation, the produc-
tion of superoxide anion radical, ferricytochrome creduction, and
oxygen consumption by DOX; it also protects against the negativeionotropic effects of DOX (Bast et al., 2007a; Quiles et al., 2002) and
guards against inflammation by preventing the DOX-mediated
overexpression ofVCAMand E-selectinin neutrophils (Abou El Has-
san et al., 2003c). Recent findings show that the anti-inflammatory
action of monoHER is related to the reduction of N-e-(carboxy-
methyl)-lysine, the accumulation of which is promoted by DOX
during cardiotoxicity (Bruynzeel et al., 2007a). This dose-depen-
dent cardioprotective effect exerted by monoHER does not affect
the anti-tumour capacity of adriamycin (van Acker et al., 1997),
even without interfering with the pharmacokinetics or metabolism
of DOX (Abou El Hassan et al., 2003b). More recently, it has been
determined that monoHER (1 mM) suppresses DOX-induced apop-
tosis in neonatal rat cardiac myocytes, as well as in human endo-
thelial cells, and the ovarian cancer cell lines A2780 and OVCAR-3, this being a caspase-dependent and -independent effect (Bruyn-
zeel et al., 2007b). Finally, monoHER also inhibits the activity of
CBR1 V88 and CBR1 I88 proteins, encoded by polymorphic CBR1
V88 in a concentration-dependent manner (Gonzalez-Covarrubias
et al., 2008).
Other flavonoids, such as catechins, have cardioprotective prop-
erties at low doses, exhibiting an iron chelating activity. These cat-
echins also have beneficial properties for the liver, and Kalender
et al. (2005)reported that catechin (200 mg/kg/week for 6 weeksby intraperitoneal injection) depressed malondialdehyde,
glutathione peroxidase and catalase activities in rats against doxo-
rubicin-induced hepatotoxicity. Two fundamental biochemical
mechanisms of flavonoids can increase the anti-tumour capacity
of DOX when they are administered jointly: (1) the inhibition of
the intracellular metabolism of the drug; (2) the blocking of intra-
cellular drug eliminating mechanisms. In previous in vitro studies,
it has been shown that green tea polyphenols such as caffeine, and
catechins such as epigallocatechin gallate or epigallocatechin can
enhance DOX-induced anti-tumour activity and increase DOX con-
centration in tumours by inhibiting its efflux (Mei et al., 2004;
Quiles et al., 2002). This reversal effect of the multidrug resistance
of green tea polyphenols, and of ()-epigallocatechin gallate in
particular, has been extensively studied, and it is clear that such
compounds can modulate the function of P-gp (Mei et al., 2004,
2003; Wei et al., 2003; Zhang et al., 2004), an effect that is partially
achieved by the regulation of DOX-induced intracellular ROS (Mei
et al., 2005). With respect to the protective effect against DOX-
associated toxicity, Dudka et al. (2005) tested the action of ()-
epigallocatechin gallate, quercetin and resveratrol on the activity
of NADPH-cytochrome P-450 reductase in the human heart, liver
and lungs. The results show that dietary ()-epigallocatechin gal-
late and quercetin may increase the activity of the P-450 reductase
during doxorubicin therapy implying an increased risk of toxicity
while resveratrol has no significant effect.
Quercetin, in addition to its high antioxidant capacity, can inhi-
bit TOP2 and intercalate into DNA strands, thereby boosting the
anti-tumour effect of DOX (Snyder and Gillies, 2002). Quercetin
also inhibits several protein kinases and increases the concentra-tion of adriamycin inside chemotherapy resistant cancer cells, by
blocking efflux pump proteins such as the P-gp and ABCG2 proteins
(Eckford and Sharom, 2009). Moreover, quercetin enormously im-
proves the therapeutic index of DOX in breast cancer cells and in
mice with breast cancer (100 mg/kg by oral gavage for 3 weeks).
The mechanism seems to be related to its inhibitory effect on hy-
poxia inducible factor-1alphain both tumour and normal cells (Du
et al., 2009). It has been reported that quercetin protects rat heart
microsomes and mitochondria against iron-dependent doxorubi-
cin-induced lipid peroxidation (Psotov et al., 2002, 2004). This
cardioprotective effect has been corroborated by Vclavkov
et al. (2008), who reported that quercetin is a potent inhibitor of
DOX-induced toxicity, significantly inhibiting the formation of
doxorubicinol in human liver cytosolic fractions.Oral garlic supplementation decreases the oxidative stress pro-
voked by chronic administration of DOX, and protects against free
radicals, improving the clinical efficacy of adriamycin (Quiles et al.,
2002). Moreover, chronic garlic administration (250 and 500 mg/
kg daily, orally, for 30 days) has been shown to prevent acute adri-
amycin-induced cardiotoxicity and decreases myocardial TNFaexpression (Mukherjee et al., 2003). The garlic-derived volatile
organosulphur compound diallyl sulphide has been shown to be
a non-toxic, selective and highly potent modulator ofP-gp in hu-
man K562 leukaemia cells and in the rodent liver (Arora et al.,
2004).
Other compounds, such as genistein, a soy isoflavone with high
antioxidant capacity, can increase cellular antioxidant status by
scavenging ROS and augmenting the activity of antioxidantenzymes like glutathione peroxidase, glutathione reductase or
1432 S. Granados-Principal et al. / Food and Chemical Toxicology 48 (2010) 14251438
8/12/2019 New Advances
9/14
superoxide dismutase. Genistein is also an inhibitor of TOP2, inhib-
iting the binding of ATP to its binding site on the enzyme (Conklin,
2000); furthermore, it is a competitive inhibitor of tyrosine ki-
nases, inhibiting growth factor b signalling pathways, and also
exerting antiproliferative effects in cells and putative anti-cancer
effects, possibly through the induction of apoptosis. Thus, genistein
can be considered a TOP2-specific clastogen (Lynch et al., 2003). Fi-
nally, this isoflavone can enhance the accumulation of doxorubicinin cancer cells, and makes MDA-MB-231 cells more sensitive to
doxorubicin, probably via increasedGRP78(glucose-regulated pro-
tein 78) expression, while having no effects on MCF-7 cells (Lim
et al., 2006).
Curcumin, the main component of the curry spice turmeric, is a
phenolic compound with a high antioxidant effect at several levels:
it prevents the oxidation of low density lipoprotein (LDL) and poly-
unsaturated fatty acids, and the lipid peroxidation of biological
membranes, and affects intracellular systems closely associated
with oxidative processes, such as nuclear factor kappa B (NF-jB),transcription factor, inducible nitric oxide synthase (iNOS), thiore-
doxin, nuclear factor (erythroid-derived 2)-like 2, heme oxygen-
ase-1, hypoxia inducible factor-1, or heat shock protein 70
(Ramirez-Tortosa et al., 2009; Quiles et al., 1998). Curcumin also
induces several antioxidant enzymes, such as glutathioneS-trans-
ferase, NAD(P)H:quinone oxidoreductase 1, glutathione reductase,
glutathione peroxidase, and catalase (Calabrese et al., 2008; Quiles
et al., 2006). This high antioxidant capacity enables oral curcumin
to play a protective role against adriamycin-induced nephrotoxi-
city and cardiotoxicity (Quiles et al., 2006), by three fundamental
mechanisms: (1) inhibiting lipid peroxidation by scavenging free
radicals; (2) raising glutathione levels; (3) stabilizing cardiac cell
membranes (Wongcharoen and Phrommintikul, 2009). A recent re-
port showed that curcumin, administered as an oral turmeric ex-
tract in rats, ameliorated the harmful effects of adriamycin in the
heart and liver, and also blocked nephrotoxicity. With respect to
plasma, turmeric extract effectively inhibited increases in choles-
terol, lactate dehydrogenase and creatine kinase (Mohamad et al.,
2009). Curcumin can also fortify the anti-tumour action of DOXby several mechanisms, one of which consists in raising the intra-
cellular concentration of this chemotherapeutic agent. This mech-
anism is the result of curcumin being a potent modulator of efflux
pump ABCG2 protein (Chearwae et al., 2006) as well as P-gp (Ange-
lini et al., 2008) probably because of the inhibition of the PI3K/Akt/
NF-jB pathway (Choi et al., 2008). Curcumin also sensitizes gliomacells to DOX, among others, by inhibiting the AP-1 (activator pro-
tein-1) and NF-jB transcription factors (Dhandapani et al., 2007).Resveratrol, a non-flavonoid polyphenolic compound, is a
powerful antioxidant found predominantly in peanuts, grapes,
cranberries, turmeric, hops, mulberries, etc., with anti-cancer (neu-
roblastoma, lymphoblastic leukaemia, multiple myeloma, breast,
colorectal and prostate cancer), anti-inflammatory and antioxidant
properties (Udenigwe et al., 2008), although it can exhibit a pro-oxidant capacity under certain experimental conditions (Athar
et al., 2009). Resveratrol exerts its anti-cancer activity at different
levels, affecting cell growth, angiogenesis, invasion, metastasis and
inflammation by targeting tumour suppressors (p53 andRb), cell
cycle mediators (cyclins, CDKs or CDK inhibitors), transcription
factors (NF-jB, AP-1, or c-Jun), or regulators of the apoptotic andsurvival signalling pathways (Bax, Bak, Noxa, TRAIL, survivin, Akt,
Bcl-2, among others) (Athar et al., 2009). The protective role of this
polyphenolic compound against DOX cardiotoxicity is being
studied. It is known that pre-treatment with resveratrol and subse-
quent treatment with doxorubicin in H9c2 cardiomyocytes pro-
tects against the toxicity generated by DOX and can decrease the
intracellular accumulation of ROS induced by xanthine oxidase/
xanthine (Cao and Li, 2004). This protective effect of resveratrolagainst DOX-promoted cardiac toxicity has also been studied in
neonatal rat ventricular myocytes, in which it increases cell viabil-
ity; in addition, it improves electrocardiogram results in mice
(Rezk et al., 2006).Tatlidede et al. (2009)showed that resveratrol
(10 mg/kg was administered intraperitoneally for a total of
7 weeks), in combination with adriamycin (20 mg/kg), markedly
ameliorates the severity of cardiac dysfunction by preventing the
oxidative stress provoked by DOX toxicity in rats. A possible action
mechanism was reported by Danz et al. (2009), who studied theprotective role of resveratrol against DOX-induced cell death in
primary cardiomyocytes. This elegant study shows that resveratrol
protects against DOX-induced mitochondrial depolarization and
cardiomyocyte death by inhibiting ROS production, probably
through the up-regulation of manganese superoxide antioxidant
activity, together with maintenance of mitochondrial function
and the Sirt1 pathway. Sirt1 is a NAD+-dependent class III histone
deacetylase, the overexpression of which protects the heart from
oxidative stress through the up-regulation of antioxidants (Alcen-
dor et al., 2007). More recently, it has been discovered that intra-
peritoneal resveratrol (10 mg/kg) also reverses the vascular
dysfunction caused by DOX in the rat thoracic aorta. The putative
mechanism of this effect could be related to the overexpression
of eNOS (endothelial nitric oxide synthase) and iNOS (Olukman
et al., 2009). Finally, it is important to mention that, apart from
its protective effect, resveratrol also improves the effectiveness of
adriamycin (Rezk et al., 2006) and encourages sensitization to
apoptosis induced by doxorubicin and other chemotherapeutics
in sensitive and multidrug resistant (P-gp positive) promyelocytic
leukaemia HL60 cells (Duraj et al., 2006).
3.6. Antioxidant compounds from virgin olive oil
In comparison with Northern Europe or other Western coun-
tries, Mediterranean countries register a lower rate of mortality
from cardiovascular disease and cancer, attributed at least partly
to the so-called Mediterranean diet (Knoops et al., 2004; Tricho-
poulou et al., 2003). The healthy effects of olive oil consumption
have traditionally been ascribed to its high oleic acid content.However, there is growing evidence that components of olive oil
other than oleic acid could be related to its healthy properties.
The basis for this hypothesis is the presence of minor bioactive
compounds, fundamentally phenols with a strong antioxidant
capacity, such as hydroxytyrosol and oleuropein (Prez-Jimnez
et al., 2007; Aguilera et al., 2003, 2004), and other antioxidants
such as vitamin E (Quiles et al., 2002).
A previous review has highlighted the importance of olive oil in
counteracting the toxic effects exerted by adriamycin. Thus, virgin
olive oil as dietary fat (8 g/100 g of diet) can reduce the damage
caused by DOX in the mitochondria and in liver microsomes
(Mataix et al., 2006; Quiles et al., 2002). Following the idea that
antioxidant compounds from virgin olive oil are beneficial, two
studies were performed in our laboratory using dietary olive oillacking the antioxidant fraction but supplemented with vitamin E
(Quiles et al., 1999a,b). The results obtained show that supplemen-
tation with this antioxidant, up to the normal levels found in virgin
olive oil, greatly improves the response of this edible oil against
adriamycin toxicity in rats. As stated above, other antioxidants,
too, provide virgin olive oil with major healthy properties, and
oleuropein is currently being studied in this sense.
Oleuropein, a hydrophilic phenolic compound belonging to the
secoiridoid family, is found in high concentrations in olives, olive
oil, and the leaves and small branches of the olive tree (Japn-Lujan
and Luque de Castro, 2007). This secoiridoid is the bitter principle
of olive oil, and during ripening and storage, it undergoes hydroly-
sis and yields oleuropein aglycone, elenolic acid and several simple
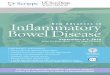
phenols (such as hydroxytyrosol), which build up the well-knowncomplex taste of olive oil (Visioli et al., 2006) (Fig. 2). Both oleurop-
S. Granados-Principal et al./ Food and Chemical Toxicology 48 (2010) 14251438 1433
8/12/2019 New Advances
10/14
ein and hydroxytyrosol present a catechol group that gives these
phenolic compounds a high antioxidant capacity through the for-
mation of intramolecular hydrogen bonds. This antioxidative prop-
erty is even more potent than that exerted by other antioxidants
such as vitamin E, dimethylsulfoxide (DMSO) and butylated
hydroxytoluene. It has been shown that oleuropein and hydroxyty-
rosol can efficiently scavenge free radicals and inhibit LDL oxida-
tionin vitro
(Owen et al., 2000; Visioli et al., 2002). In addition totheir antioxidant effect, both oleuropein and hydroxytyrosol
(orally administered) have demonstrated an antidiabetic activity,
with a hypoglycaemic effect in alloxan diabetic rats (Jemai et al.,
2009) and rabbits (Al-Azzawie and Alhamdani, 2006), and oleurop-
ein could also prevent or slow down the progression of type II dia-
betes (Rigacci et al., 2009). Both oleuropein and hydroxytyrosol
also inhibit lipid and protein oxidation in human plasma (Roche
et al., 2009), and present antiviral activity against hepatitis B (Zhao
et al., 2009) and viral haemorrhagic septicaemia virus (Micol et al.,
2005). Moreover, they are small molecule HIV-1 fusion and integr-
ase inhibitors, interacting with the protein envelope gp41
(Lee-Huang et al., 2007a,b). Oleuropein also interacts with b-amy-
loid peptide, and is a putative inhibitor of the formation of the
neurotoxic b-amyloid peptide assembly associated with
Alzheimers disease. Therefore, oleuropein might profitably be
used against this disease (Benaki et al., 2009). Furthermore, it
inhibits platelet aggregation (Zbidi et al., 2009), acts as an antipar-
asitic agent againstToxoplasma gondii(Jiang et al., 2008), and as an
anti-inflammatory agent (Giamarellos-Bourboulis et al., 2006;
Miles et al., 2005; Puel et al., 2006).
Dietary virgin olive oil, being rich in antioxidants such as phe-
nolic compounds, has been considered an effective protector agent
against cancer (colon, breast or skin), ageing, or cardiovascular dis-
ease (Owen et al., 2000). As an important component in this edible
oil, oleuropein also exhibits an effect against breast cancer. This
phenolic compound has been studied to test its ability to inhibit
the proliferation of breast cancer cells (Han et al., 2009; Menendez
et al., 2007, 2008, 2009), or human urinary bladder carcinoma or
endothelial cells (Goulas et al., 2009). Oleuropein has protectiveproperties against cardiovascular disease, protecting low density
lipoproteins from oxidation (Visioli and Galli, 1994), enhancing ni-
tric oxide production by macrophages (Visioli et al., 1998), inhibit-
ing endothelial activation (Carluccio et al., 2003) through the
down-regulation of adhesion molecules involved in early athero-
genesis (DellAgli et al., 2006), decreasing lipaemia (Jemai et al.,
2008), and preventing the oxidative myocardial injury induced
by ischemia/reperfusion (Manna et al., 2004).
With respect to the protective properties of oleuropein against
doxorubicin-induced cardiotoxicity,Andreadou et al. (2007) have
shown that this secoiridoid, intraperitoneally administered (100
and 200 mg/kg) for 5 or 3 consecutive days, respectively, startingeither 2 days before or on the day of DOX administration, prevents
the acute cardiotoxicity caused by intraperitoneal DOX (20 mg/kg)
in rats. In this study, oleuropein significantly reduced the serum
levels of creatine phosphokinase, creatine phosphokinase-MB, lac-
tate dehydrogenase, aspartate aminotransferase and alanine ami-
notransferase. Moreover, in heart tissue, it not only decreased the
concentrations of lipid peroxidation products (conjugated dienes
and malondialdehyde), protein carbonyls and nitrotyrosine, and
lowered cytoplasmic vacuolisation in cardiomyocytes, but also
boosted the induction of iNOS.
This cardioprotective effect of oleuropein has been supported in
another, more recent, study with the same experimental protocol
and doses of oleuropein and DOX (Andreadou et al., 2009). A nucle-
ar magnetic resonance-based metabolomic approach was used to
analyse acute DOX-induced cardiotoxicity, and found acetate and
succinate to be novel biomarkers applicable to the disturbance of
metabolic energy pathways. Oleuropein at both doses removed
the succinate and acetate accumulation in heart tissue, which indi-
cates that this antioxidant restores distressed energy metabolic
pathways during DOX-associated cardiac toxicity.
3.7. Selenium
In addition to the above mentioned antioxidants, micronutri-
ents such as selenium also present major biological and
antioxidant properties. Selenium has been widely studied for its
anti-cancer effects and the cardioprotective role played against
DOX toxicity. Concerning the former, it has been reported that
selenium induces apoptosis and decreases DNA synthesis, in sev-eral tumour cell lines (breast, colon, prostate, lung, small intestine
and liver) (Vadgama et al., 2000). It also induces massive apoptosis
in a DOX resistant cell line (derived from human small cell lung
carcinoma) in a caspase-3 independent manner (Jnsson-Videster
Fig. 2. Hydrolysis of oleuropein during olive ripening and storage.
1434 S. Granados-Principal et al. / Food and Chemical Toxicology 48 (2010) 14251438
8/12/2019 New Advances
11/14
et al., 2004), sensitizes MCF-7 breast cancer cells to DOX-induced
apoptosis by repressing adriamycin-induced Akt activation
(Li et al., 2007b), and induces the Fas death pathway in cooperation
with DOX in MCF-7 cells (Li et al., 2007a). More recently,Tan et al.
(2009)reported that selenium nanoparticles are capable of induc-
ing apoptosis in human hepatic cancer cells Bel7402, and that the
combination of DOX and selenium nanoparticles provides higher
inhibition efficiencies. The cardioprotective effects of seleniumagainst DOX toxicity were reviewed earlier (Quiles et al., 2002),
and it was found that selenium oral supplementation fortifies the
antioxidant defences of cardiac cells and diminishes the heart in-
jury caused by DOX in animals. Recent studies support this idea;
thus,Danesi et al. (2006)reported that a moderate dietary supple-
mentation of selenium (0.1 mg/kg) increases the total antioxidant
activity and glutathione concentration as well as glutathione
peroxidase and catalase activities in the rat heart. Such increases
in endogenous antioxidants lead to reduced ROS production. In a
mouse model of combined therapy (doxorubicin, vincristine and
prednisolone) the administration of selenium decreased catalase
activity, but did not significantly lower xanthine oxidase activity
(Popovic et al., 2007). Weak protective activity of selenium has also
been reported against the nephrotoxicity (Bulucu et al., 2008) and
hepatotoxicity (Bulucu et al., 2009) induced by DOX in rats.
Finally, a recent study shows that a commercial mixture of vita-
mins (C, E and b-carotene) and minerals (copper, selenium and
zinc) administered to Drosophila melanogaster larvae treated with
DOX, was not genotoxic and it also protected against the genotoxic
effects of chemotherapeutic agents (Costa and Nepomuceno,
2006).
4. Summary and conclusions
Adriamycin is one of the most commonly used and effective
drugs against several types of cancer, including breast carcinoma.
Nonetheless, doxorubicin-associated toxicity is a severe problem
in its use in humans, this toxicity occurring mainly in the heart,
kidney and liver. In addition, it provokes DNA alterations and pro-
duces free radicals. Many natural compounds with antioxidant
properties, such as vitamins E, C and A, carotenoids, coenzyme Q,
flavonoids, polyphenols, virgin olive oil compounds, resveratrol
and selenium, have been proposed as promising means of prevent-
ing or reducing such toxic effects, without decreasing the anti-tu-
mour action of adriamycin. Since much of the evidence derives
from in vitrostudies on cell preparations or from laboratory animal
studies, more clinical studies are needed to test the ability of these
compounds to act as chemopreventive agents or to reverse the dis-
turbances provoked by adriamycin. Moreover, the anti-tumour ac-
tion of natural compounds combined with anthracyclines or other
chemotherapeutic drugs should be studied more thoroughly at the
clinical level. It is necessary to establish the appropriate concentra-
tion, dosage and treatment schedule of antioxidants, not only as
dietary supplements, but also probably to be administered as che-
motherapeutic drugs to intensify the anti-tumour action of adria-
mycin, and at the same time to diminish its toxicity.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Acknowledgements
This study was partlyfunded by theExcelentsima Diputacin de
Jan, the CEAS Foundation (30.C0.244500) and Junta de Andaluca
(PI-0210/2007). We thank the Spanish Ministry of Science and Inno-vation (AP2005-144) andthe University of Granada for the personal
support of Dr. S. Granados-Principal. The authors thank Mr. Glenn
Harding for his extensive editing of the manuscript.
References
Abou El Hassan, M.A., Heijn, M., Rabelink, M.J., van der Vijgh, W.J., Bast, A., Hoeben,R.C., 2003a. The protective effect of cardiac gene transfer of CuZn-sod in
comparison with the cardioprotector monohydroxyethylrutoside againstdoxorubicin-induced cardiotoxicity in cultured cells. Cancer Gene Ther. 10,270277.
Abou El Hassan, M.A., Kedde, M.A., Zwiers, U.T., Bast, A., van der Vijgh, W.J., 2003b.The cardioprotector monoHER does not interfere with the pharmacokinetics orthe metabolism of the cardiotoxic agent doxorubicin in mice. CancerChemother. Pharmacol. 51, 306310.
Abou El Hassan, M.A., Verheul, H.M., Jorna, A.S., Schalkwijk, C., van Bezu, J., van derVijgh, W.J., Bast, A., 2003c. The new cardioprotector monohydroxyethylrutosideprotects against doxorubicin-induced inflammatory effects in vitro. Brit. J.Cancer 89, 357362.
Aguilera, C.M., Mesa, M.D., Ramirez-Tortosa, M.C., Nestares, M.T., Ros, E., Gil, A.,2004. Sunflower oil does not protect against LDL oxidation as virgin olive oildoes in patients with peripheral vascular disease. Clin. Nutr. 23, 673681.
Aguilera, C.M., Mesa, M.D., Ramrez-Tortosa, M.C., Quiles, J.L., Gil, A., 2003. Virginolive and fish oils enhance the hepatic antioxidant defence system inatherosclerotic rabbits. Clin. Nutr. 22, 379384.
Al-Azzawie, H.F., Alhamdani, M.S., 2006. Hypoglycemic and antioxidant effect ofoleuropein in alloxan-diabetic rabbits. Life Sci. 78, 13711377.
Alcendor, R.R., Gao, S., Zhai, P., Zablocki, D., Holle, E., Yu, X., Tian, B., Wagner, T.,Vatner, S.F., Sadoshima, J., 2007. Sirt1 regulates aging and resistance tooxidative stress in the heart. Circ. Res. 100, 15121521.
Andreadou, I., Papaefthimiou, M., Zira, A., Constantinou, M., Sigala, F., Skaltsounis,A.L., Tsantili-Kakoulidou, A., Iliodromitis, E.K., Kremastinos, D.T., Mikros, E.,2009. Metabonomic identification of novel biomarkers in doxorubicincardiotoxicity and protective effect of the natural antioxidant oleuropein.NMR Biomed. 22, 585592.
Andreadou, I., Sigala, F., Iliodromitis, E.K., Papaefthimiou, M., Sigalas, C., Aligiannis,N., Savvari, P., Gorgoulis, V., Papalabros, E., Kremastinos, D.T., 2007. Acutedoxorubicin cardiotoxicity is successfully treated with the phytochemicaloleuropein through suppression of oxidative and nitrosative stress. J. Mol.Cell. Cardiol. 42, 549558.
Angelini, A., Iezzi, M., Di Febbo, C., Di Ilio, C., Cuccurullo, F., Porreca, E., 2008.Reversal ofP-glycoprotein-mediated multidrug resistance in human sarcomaMES-SA/Dx-5 cells by nonsteroidal anti-inflammatory drugs. Oncol. Rep. 20,731735.
Anjos Ferreira, A.L., Russell, R.M., Rocha, N., Placido Ladeira, M.S., Favero Salvadori,D.M., Oliveira Nascimento, M.C., Matsui, M., Carvalho, F.A., Tang, G., Matsubara,L.S., Matsubara, B.B., 2007. Effect of lycopene on doxorubicin-inducedcardiotoxicity: an echocardiographic, histological and morphometricalassessment. Basic Clin. Pharmacol. Toxicol. 101, 1624.
Arora, A., Seth, K., Shukla, Y., 2004. Reversal ofP-glycoprotein-mediated multidrugresistance by diallyl sulfide in K562 leukemic cells and in mouse liver.Carcinogenesis 25, 941949.
Atessahin, A., Trk, G., Karahan, I., Yilmaz, S., Ceribasi, A.O., Bulmus, O., 2006.Lycopene prevents adriamycin-induced testicular toxicity in rats. Fertil. Steril.85, 12161222.
Athar, M., Back, J.H., Kopelovich, L., Bickers, D.R., Kim, A.L., 2009. Multiple moleculartargets of resveratrol: anti-carcinogenic mechanisms. Arch. Biochem. Biophys.486, 95102.
Bai, P., Mabley, J.G., Liaudet, L., Virg, L., Szab, C., Pacher, P., 2004. Matrixmetalloproteinase activation is an early event in doxorubicin-inducedcardiotoxicity. Oncol. Rep. 11, 505508.
Bast, A., Haenen, G.R., Bruynzeel, A.M., Van der Vijgh, W.J., 2007a. Protection byflavonoids against anthracycline cardiotoxicity: from chemistry to clinicaltrials. Cardiovasc. Toxicol. 7, 154159.
Bast, A., Kaiserov, H., den Hartog, G.J., Haenen, G.R., van der Vijgh, W.J., 2007b.Protectors against doxorubicin-induced cardiotoxicity: flavonoids. Cell Biol.Toxicol. 23, 3947.
Benaki, D., Stathopoulou, K., Leondiadis, L., Ferderigos, N., Pelecanou, M., Mikros, E.,2009. Detection of interactions of the beta-amyloid peptide with smallmolecules employing transferred NOEs. J. Pept. Sci. 15, 435441.
Bernuzzi, F., Recalcati, S., Alberghini, A., Cairo, G., 2009. Reactive oxygen species-independent apoptosis in doxorubicin-treated H9c2 cardiomyocytes: role forheme oxygenase-1 down-modulation. Chem. Biol. Interact. 177, 1220.
Berthiaume, J.M., Oliveira, P.J., Fariss, M.W., Wallace, K.B., 2005. Dietary vitamin Edecreases doxorubicin-induced oxidative stress without preventingmitochondrial dysfunction. Cardiovasc. Toxicol. 5, 257267.
Berthiaume, J.M., Wallace, K.B., 2007a. Adriamycin-induced oxidativemitochondrial cardiotoxicity. Cell Biol. Toxicol. 23, 1525.
Berthiaume, J.M., Wallace, K.B., 2007b. Persistent alterations to the gene expressionprofile of the heart subsequent to chronic doxorubicin treatment. Cardiovasc.Toxicol. 7, 178191.
Bertinchant, J.P., Polge, A., Juan, J.M., Oliva-Lauraire, M.C., Giuliani, I., Marty-Double,C., Burdy, J.Y., Fabbro-Peray, P., Laprade, M., Bali, J.P., Granier, C., de la Coussaye,
J.E., Dauzat, M., 2003. Evaluation of cardiac troponin I and T levels as markers ofmyocardial damage in doxorubicin-induced cardiomyopathy rats, and their
S. Granados-Principal et al./ Food and Chemical Toxicology 48 (2010) 14251438 1435
8/12/2019 New Advances
12/14
relationship with echocardiographic and histological findings. Clin. Chim. Acta329, 3951.
Bjelogrlic, S.K., Radic, J., Jovic, V., Radulovic, S., 2005. Activity ofD,L-alpha-tocopherol(vitamin E) against cardiotoxicity induced by doxorubicin and doxorubicin withcyclophosphamide in mice. Basic Clin. Pharmacol. Toxicol. 97, 311319.
Branda, R.F., Powden, C., Brooks, E.M., Yildirim, Z., Naud, S.J., McCormack, J.J., 2006.Vitamin E but not St. Johns wort mitigates leukopenia caused by cancerchemotherapy in rats. Transl. Res. 148, 315324.
Bruynzeel, A.M., Abou El Hassan, M.A., Schalkwijk, C., Berkhof, J., Bast, A., Niessen,H.W., van der Vijgh, W.J., 2007a. Anti-inflammatory agents and monoHER
protect against DOX-induced cardiotoxicity and accumulation of CML in mice.Brit. J. Cancer 96, 937943.
Bruynzeel, A.M., Abou El Hassan, M.A., Torun, E., Bast, A., van der Vijgh, W.J., Kruyt,F.A., 2007b. Caspase-dependent and -independent suppression of apoptosis bymonoHER in doxorubicin treated cells. Brit. J. Cancer 96, 450456.
Bruynzeel, A.M., Niessen, H.W., Bronzwaer, J.G., van der Hoeven, J.J., Berkhof, J., Bast,A., van der Vijgh, W.J., van Groeningen, C.J., 2007c. The effect ofmonohydroxyethylrutoside on doxorubicin-induced cardiotoxicity in patientstreated for metastatic cancer in a phase II study. Brit. J. Cancer 97, 10841089.
Bruynzeel, A.M., Vormer-Bonne, S., Bast, A., Niessen, H.W., van der Vijgh, W.J.,2007d. Long-term effects of 7-monohydroxyethylrutoside (monoHER) on DOX-induced cardiotoxicity in mice. Cancer Chemother. Pharmacol. 60, 509514.
Bryant, J., Picot, J., Baxter, L., Levitt, G., Sullivan, I., Clegg, A., 2007. Clinical and cost-effectiveness of cardioprotection against the toxic effects of anthracyclinesgiven to children with cancer: a systematic review. Brit. J. Cancer 96, 226230.
Bulucu, F., Ocal, R., Karadurmus, N., Sahin, M., Kenar, L., Aydin, A., Oktenli, C., Koc, B.,Inal, V., Yamanel, L., Yaman, H., 2009. Effects ofN-acetylcysteine, deferoxamineand selenium on doxorubicin-induced hepatotoxicity. Biol. Trace Elem. Res.(Epub ahead of print).
Bulucu, F., Oktenli, C., Kenar, L., Ocal, R., Koc, B., Inal, V., Yamanel, L., Yaman, H.,Sanisoglu, Y.S., Aydin, A., 2008. Efficacy of deferoxamine, N-acetylcysteine andselenium treatments in rats with adriamycin-induced nephrotic syndrome. J.Nephrol. 21, 576583.
Calabrese, V., Bates, T.E., Mancuso, C., Cornelius, C., Ventimiglia, B., Cambria, M.T., DiRenzo, L., De Lorenzo, A., Dinkova-Kostova, A.T., 2008. Curcumin and the cellularstress responsein freeradical-relateddiseases.Mol.Nutr.FoodRes. 52,10621073.
Cao, Z., Li, Y., 2004. Potent induction of cellular antioxidants and phase 2 enzymesby resveratrol in cardiomyocytes: protection against oxidative and electrophilicinjury. Eur. J. Pharmacol. 489, 3948.
Cardoso, S., Santos, R.X., Carvalho, C., Correia, S., Pereira, G.C., Pereira, S.S., Oliveira,P.J., Santos, M.S., Proena, T., Moreira, P.I., 2008. Doxorubicin increases thesusceptibility of brain mitochondria to Ca(2+)-induced permeability transitionand oxidative damage. Free Radical Biol. Med. 45, 13951402.
Carlquist, M., Frejd, T., Gorwa-Grauslund, M.F., 2008. Flavonoids as inhibitors ofhuman carbonyl reductase 1. Chem. Biol. Interact. 174, 98108.
Carluccio, M.A., Siculella, L., Ancora, M.A., Massaro, M.,Scoditti, E., Storelli, C., Visioli,F., Distante, A., De Caterina, R., 2003. Olive oil and red wine antioxidant
polyphenols inhibit endothelial activation: antiatherogenic properties ofMediterranean diet phytochemicals. Arterioscl. Thromb. Vas. Biol. 23, 622629.
Chandran, K., Aggarwal, D., Migrino, R.Q., Joseph, J., McAllister, D., Konorev, E.A.,Antholine, W.E., Zielonka, J., Srinivasan, S., Avadhani, N.G., Kalyanaraman, B.,2009. Doxorubicin inactivates myocardial cytochrome c oxidase in rats:cardioprotection by Mito-Q. Biophys. J. 96, 13881398.
Chearwae, W., Shukla, S., Limtrakul, P., Ambudkar, S.V., 2006. Modulation of thefunction of the multidrug resistance-linked ATP-binding cassette transporterABCG2 by the cancer chemopreventive agent curcumin. Mol. Cancer Ther. 5,19952006.
Chen, Y., Jungsuwadee, P., Vore, M., Butterfield, D.A., St Clair, D.K., 2007. Collateraldamage in cancer chemotherapy: oxidative stress in nontargeted tissues. Mol.Interv. 7, 147156.
Choi, B.H., Kim, C.G., Lim, Y., Shin, S.Y., Lee, Y.H., 2008. Curcumin down-regulates themultidrug-resistance mdr1b gene by inhibiting the PI3K/Akt/NF kappa Bpathway. Cancer Lett. 259, 111118.
Choi, E.H., Chang, H.J., Cho, J.Y., Chun, H.S., 2007. Cytoprotective effect ofanthocyanins against doxorubicin-induced toxicity in H9c2 cardiomyocytes inrelation to their antioxidant activities. Food Chem. Toxicol. 45, 18731881.
Chularojmontri, L., Wattanapitayakul, S.K., Herunsalee, A., Charuchongkolwongse,S., Niumsakul, S., Srichairat, S., 2005. Antioxidative and cardioprotective effectsof Phyllanthus urinaria L. on doxorubicin-induced cardiotoxicity. Biol. Pharm.Bull. 28, 11651171.
Conklin, K.A., 2000. Dietary antioxidants during cancer chemotherapy: impact onchemotherapeutic effectiveness and development of side effects. Nutr. Cancer37, 118.
Conklin, K.A., 2004. Chemotherapy-associated oxidative stress: impact onchemotherapeutic effectiveness. Integr. Cancer Ther. 3, 294300.
Conklin, K.A., 2005. Coenzyme q10 for prevention of anthracycline-inducedcardiotoxicity. Integr. Cancer Ther. 4, 110130.
Costa, W.F., Nepomuceno, J.C., 2006. Protective effects of a mixture of antioxidantvitamins and minerals on the genotoxicity of doxorubicin in somatic cells ofDrosophila melanogaster. Environ. Mol. Mutagen. 47, 1824.
Danesi, F., Malaguti, M., Nunzio, M.D., Maranesi, M., Biagi, P.L., Bordoni, A., 2006.Counteraction of adriamycin-induced oxidative damage in rat heart byselenium dietary supplementation. J. Agric. Food Chem. 54, 12031208.
Danz, E.D., Skramsted, J., Henry, N., Bennett, J.A., Keller, R.S., 2009. Resveratrol
prevents doxorubicin cardiotoxicity through mitochondrial stabilization andthe Sirt1 pathway. Free Radical Biol. Med. 46, 15891597.
De Celle, T., Heeringa, P., Strzelecka, A.E., Bast, A., Smits, J.F., Janssenm, B.J., 2004.Sustained protective effects of 7-monohydroxyethylrutoside in an in vivomodel of cardiac ischemia-reperfusion. Eur. J. Pharmacol. 494,205212.
Della Torre, P., Imondi, A.R., Bernardi, C., Podesta, A., Moneta, D., Riflettuto, M.,Mazue, G., 1999a. Cardioprotection by dexrazoxane in rats treated withdoxorubicin and paclitaxel. Cancer Chemother. Pharmacol. 44, 138142.
Della Torre, P., Mazu, G., Podest, A., Moneta, D., Sammartini, U., Imondi, A.R.,1999b. Protection against doxorubicin-induced cardiotoxicity in weanling ratsby dexrazoxane. Cancer Chemother. Pharmacol. 43, 151156.
DellAgli, M., Fagnani, R., Mitro, N., Scurati, S., Masciadri, M., Mussoni, L., Galli, G.V.,Bosisio, E., Crestani, M., De Fabiani, E., Tremoli, E., Caruso, D., 2006. Minorcomponents of olive oil modulate proatherogenic adhesion molecules involvedin endothelial activation. J. Agric. Food Chem. 54, 32593264.
Dhandapani, K.M., Mahesh, V.B., Brann, D.W., 2007. Curcumin suppresses growthand chemoresistance of human glioblastoma cells via AP-1 and NFkappaBtranscription factors. J. Neurochem. 102, 522538.
Du, G., Lin, H., Wang, M., Zhang, S., Wu, X., Lu, L., Ji, L., Yu, L., 2009. Quercetin greatlyimproved therapeutic index of doxorubicin against 4T1 breast cancer by itsopposingeffects on HIF-1alpha in tumor and normal cells. Cancer Chemother.Pharmacol. (Epub ahead of print).
Dudka, J., Jodynis-Liebert, J., Korobowicz, E., Burdan, F., Korobowicz, A., Szumilo, J.,Tokarska, E., Klepacz, R., Murias, M., 2005. Activity of NADPH-cytochrome P-450reductase of the human heart, liver and lungs in the presence of ()-epigallocatechin gallate, quercetin and resveratrol: an in vitro study. BasicClin. Pharmacol. Toxicol. 97, 7479.
Duraj, J., Bodo, J., Sulikova, M., Rauko, P., Sedlak, J., 2006. Diverse resveratrolsensitization to apoptosis induced by anticancer drugs in sensitive andresistantleukemia cells. Ne