Embed Size (px)
Citation preview

New Advances in Breast Cancer Radiotherapy
By Julie A. Bradley, MD, Michael Rutenberg, MD, PhD, Ray Mailhot, MD, MPH, and
Nancy P. Mendenhall, MD
University of Florida Department of Radiation Oncology, Jacksonville, Florida
Address correspondence to:
Julie A Bradley, MD University of Florida Health Proton Therapy Institute 2015 North Jefferson St. Jacksonville, FL 32206 Telephone: (904) 588-1800; Fax: (904) 588-1300 [email protected]
Abstract
Radiation therapy has undergone immense growth in knowledge, technology, and precision.
Treatments for breast cancer have evolved from sole reliance on bony anatomy and clinical set-
up to detailed dose measurements to organ substructures. Imaging techniques have evolved from
2-dimensional (2D) to 3-dimensional (3D) with the standardized use of computed tomography
simulation and target delineation. Advances in technology with intensity-modulated radiotherapy
and volumetric modulated arc therapy have increased high-dose conformality and low-dose
normal-tissue exposure. Proton therapy is emerging as a modality that can minimize the
compromises between target coverage and avoidance of organs at risk. Although not yet in
clinical use, a significant step in precision radiotherapy is on the horizon: the use of genomics,
which may allow tailored radiation doses based on the genetic make-up of the tumor and
patient-specific factors conferring radiosensitivity or radioresistance.

Introduction
The benefit of radiation therapy in the treatment of breast cancer has been well-established.
While a multitude of radiation techniques can be used to treat breast cancer, all are directed by
the simultaneous goals of covering the target and avoiding organs at risk (OARs). While various
studies have shown improvements in local-regional control, disease-free survival, and overall
survival with the use of radiation therapy for breast cancer, toxicity to the nearby normal tissue
can detract from the therapeutic ratio. Even with significant improvements in systemic therapy in
recent years, modern studies continue to show a benefit to radiotherapy. Reduction in target
volume with partial breast irradiation and cardiac-sparing techniques, such as deep-inspiration
breath hold and prone positioning, have contributed to show improvement in the therapeutic
ratio.
In one study, randomization to irradiation of the whole breast and regional lymphatics compared
to whole-breast irradiation alone resulted in improved 10-year disease-free survival (DFS) (82
percent vs. 77 percent, respectively; p=0.01).1 A similar study comprised of 44 percent high-risk
node-negative patients and 24 percent mastectomy patients also showed a 3 percent improvement
in 10-year DFS with the addition of supraclavicular (SCV) and internal mammary node (IMN)
irradiation compared to irradiation to the breast or chest wall alone (72.1 percent vs. 69.1
percent; p=0.04).2
Target and normal tissue delineation (contouring)

Historically, radiation was delivered based on bony anatomy as seen on x-rays or fluoroscopy.
Using computed tomography (CT) to direct the location of the radiation therapy portals was
initiated in the 1990s. By the early 2000s, CT-based treatment planning was routinely used, with
CT scanners becoming available within most radiation oncology departments in the United
States. The transition from 2D to 3D imaging allowed for the ability to define 3D targets. Targets
(gross disease or areas at risk for microscopic disease) and adjacent tissues, such as OARs, are
delineated on the CT imaging using various treatment planning systems. While contouring has
been implemented for different diseases at different rates, contouring has had a slow rate of
adoption in breast cancer. In fact, the first Radiation Therapy Oncology Group (RTOG) protocol
that required contouring in treatment of the whole breast opened in 2011.3
Delineation on CT allows the dose to a structure (such as a target or OAR) to be determined,
including the minimum dose, the maximum dose, and the amount of dose to a certain volume.4
Goals for target coverage and limits for OARs are used to guide treatment planning. In an
iterative process, if target coverage is suboptimal or the OAR dose is exceeded, the dosimetrist
changes the plan design to find a better solution. Without contours, the dose distribution can be
visually assessed, but dose-volume relationships cannot be determined.5,6
With the transition to contour-based planning, it was recognized among experts that variation
existed in the definitions of the targets and OARs.7 In an attempt to standardize these structure
definitions more than five years ago, the RTOG published an online contouring atlas based
primarily on muscle and bony anatomy.8 Since that time, several investigators have assessed the
comprehensiveness of this contouring atlas. Brown et al reported that in 39 percent of patients,
disease in the supraclavicular region occurred outside of the volume suggested by the RTOG
atlas.9 Jethwa et al reported that 22 percent of disease fell outside of the recommended internal

mammary node volume.10 A 3- to 4-cm expansion beyond the RTOG axillary nodal volume in
the anterior and cranial directions for the level I (low) axilla was recommended by Gentile et
al.11 A revised atlas by NRG Oncology (the cooperative group that replaced RTOG) is in
development. Other contouring atlases were developed after the seminal RTOG atlas. The
Danish atlas was based on expert consensus and the use of vessel location as well as muscle and
bone anatomy.12 The PROCAB/ESTRO (PROject on CAncer of the Breast/European Society of
Radiation Oncology) guidelines are vessel-based and centered around a 5-mm margin on the
veins in the regional lymphatic regions.13
While these atlases provide guidelines, they are not meant to prohibit adjustments to each
individual case. Particularly for those who present with node positive disease, fusion of the
imaging at diagnosis (including positron emission tomography (PET) and magnetic resonance
imaging (MRI) to the CT simulation images) can ensure that the area that previously harbored
gross disease is fully covered with sufficient dose to eradicate any microscopic residual disease
(Figure 1A). Early referral to radiation oncology allows assessment of the disease at
presentation, which may alter the radiation fields. Once the disease has regressed with systemic
therapy, or been excised with surgery, the opportunity for the radiation oncologist to tailor the
radiation fields based on initial disease presentation has passed (Figure 1B). Surgical clips to
demarcate the lumpectomy bed allow the boost volume to be accurately defined. Surgical clip
demarcation is important in all breast-conserving cases, but is absolutely critical in oncoplastic
reconstructions and for external-beam partial-breast irradiation.
Advanced delivery techniques

With 2D or 3D treatment planning, contouring contributes to a high-quality plan, yet it is not a
required step in the treatment planning process. A plan can be created in the absence of contours
and reviewed based solely on isodose distributions. However, for more advanced treatment
planning, such as step-and-shoot intensity-modulated radiation therapy (IMRT), arc therapy, or
proton therapy, a treatment plan cannot be generated without contours as dose is prescribed to a
delineated volume rather than a point. With these planning techniques, the high dose achieves
tighter conformality around the target volume. Therefore, the target delineation is a critical step
in the treatment planning process upon which all of the subsequent steps hinge. Prioritization of
target coverage and OAR goals may be necessary and may depend on the clinical situation.
Treatment plan evaluation includes a review of the radiation dose distribution achieved by a
particular plan, which designates field size and shaping, number and angle of fields, weighting of
fields (how much dose is delivered through a given field), and technique. The robustness, or
reliability, of the treatment plan must be considered. Factors such as treatment delivery time,
respiratory motion, potential change in anatomy, such as variation in seroma size, are assessed.
Other variables, like thorax shape, proximity of the heart to the chest wall, breast size and shape,
presence of expanders, and implants, can impact radiotherapy dosimetry and contribute to
decisions about the optimal radiation modality.14,15 In women with left-sided breast cancers, the
proximity of the left anterior descending artery and left ventricle to the chest wall can present a
challenge, particularly if the IMNs are treated.16,17
3D conformal photon radiation therapy (3DCRT) remains a common form of treatment for breast
cancer. This technique is robust in that modest changes in breast size or shape or changes in
seroma are unlikely to affect the dosimetry (Figure 2). While the high dose may not be as
conformal as IMRT or arc techniques, the low dose tends to be more confined compared to these

approaches. A common beam arrangement consists of parallel-opposed photon tangent fields to
treat the breast or chest wall, IMNs, and low axilla, matched to an anterior photon field that treats
the high axilla and SCV nodes. Smaller fields may be inserted within a larger field or dose-
absorbing wedges may be placed in the beam path, particularly in tangential fields, to modulate
or improve dose homogeneity. Electrons may be used to treat superficial targets, such as a thin
chest wall or some lumpectomy cavities. With 3DCRT, a dosimetrist selects the beam angles and
evaluates the dose distribution to maximize target coverage and OAR constraint goals in an
iterative fashion.
IMRT uses multiple beams (typically 5 to 7) to achieve conformality of the high dose
distribution to the target volume. Unlike 3DCRT, with IMRT, the target coverage and OAR
constraint goals are entered into the treatment planning system, and the system selects beam
angles and shapes. Volumetric modulated arc radiotherapy (VMAT) is a type of IMRT that also
achieves high dose conformality with faster delivery time.18 While IMRT uses multiple
independent beam angles, VMAT delivers radiation continuously in an arc as the gantry rotates
around the patient. Multiple parameters can be adjusted during this dynamic delivery, such as
field shape and orientation, dose rate, and rate of gantry rotation.19 These techniques yield high-
dose conformality, but often expose larger volumes of normal tissue to low-dose radiation
compared to the 3DCRT technique (Figure 3); for example, there may be an increase in the
volume of heart receiving 5 Gy,18 a parameter associated with an increasing risk of cardiac
disease. One dosimetric study predicted an increased risk of contralateral breast cancer with the
use of IMRT compared to conventional 3D technique, but not with VMAT.20 In a dosimetric
study comparing VMAT and conventional 3DCRT, VMAT achieved high dose conformity and
lower mean heart doses, but the dose to the contralateral breast and/or lung increased.21 Five

randomized trials comparing IMRT to 2D or 3DCRT22,23,24,25,26 have shown a reduction in acute
radiation dermatitis with the use of IMRT.27
Protons differ from photons in that they are particles rather than energy, they have mass, and
they travel only a finite distance. With proton therapy, the depth of penetration into tissue can be
controlled, thus there is no exit radiation dose beyond the tumor target. In addition, less dose is
deposited along the entrance path compared to photons. Protons deposit most of the dose at the
end of their path in a sharp peak of energy deposition called the Bragg peak (Figure 4).
Therefore, with protons, most of the dose is deposited in the target compared to outside of the
target with photons (regardless of photon technique, be it 3DCRT, IMRT, or VMAT).
In the use of proton therapy for breast cancer, anterior en face beams are aimed directly at the
target in the direction of respiratory motion, rather than tangentially, minimizing the risk of loss
of target coverage during respiration and improving the robustness of the proton plan. The en
face beam orientation also allows for a choice of treatment with arms akimbo rather than
overhead, which may increase patient comfort during treatment delivery. The abrupt dose fall-off
permits coverage of all target areas, including the internal mammary nodes, while simultaneously
achieving little or no dose to the heart (Figure 3). A median mean heart dose of < 1 Gy, even
with IMN treatment, has been consistently achieved in multiple studies of proton therapy for
breast cancer.28,29,30,31,32 The dose can be modulated to maximize radiation avoidance to cardiac
substructures, such as the coronary arteries. Proton therapy for unilateral breast cancer typically
eliminates the dose to the contralateral lung. In the setting of regional lymphatic irradiation, the
volume of ipsilateral lung receiving 5 Gy and 20 Gy is often decreased by 50 percent compared
to 3D conformal photon therapy treatment.30,32 Compared to IMRT, proton therapy also delivers
significantly less low-dose radiation (V5, V10) to the lung with reduced or similar moderate-to-

high-dose radiation (V20, V40).28,29 Of all currently available techniques, proton therapy yields
the lowest overall integral dose (dose to non-targeted tissue).32 With the decreased integral dose
and lung dose as well as elimination of contralateral breast/chest wall dose, proton therapy may
decrease the rate of second malignancy.33
Proton therapy can be delivered with passive-scattering (double-scattering or uniform scanning)
or with scanning (intensity-modulated proton therapy [IMPT]) techniques. The skin dose can be
higher with proton therapy compared to photon techniques, increasing the risk of radiation
dermatitis. With IMPT, modulation can be used to decrease the dose to skin, but passive-
scattering does not allow for this.34
While all aspects of breast cancer radiotherapy operate within guidelines, each step in the
process is individualized depending on patient needs, including positioning (supine or prone;
with protons, arms up or akimbo), target delineation (adjusted based on review of initial imaging;
decision on which nodal volumes are at high enough risk to warrant treatment; partial or whole
breast treatment), and modality (photon vs. electron vs. proton; 3DCRT vs. IMRT vs. VMAT
with photons; double scattering vs. scanning proton therapy). In addition, the prescription dose is
largely empirical, based on historical studies, with minimal variation between patients. These
treatment planning decisions are made after evaluating patient and disease characteristics, but
rarely on genomics.
Genomics
Data continues to emerge on the association between recurrence score and local-regional failure.
If validated in ongoing prospective studies, the recurrence score may become an important tool

in selecting patients with favorable biology for whom radiation therapy may afford minimal
benefit versus those with unfavorable biology for whom radiation therapy may have a significant
impact. An analysis of combined retrospective data from NSABP B14 and B20 evaluated women
with node-negative, ER-positive breast cancer. Even for these luminal breast cancers, recurrence
score correlated with local-regional recurrence, and this association persisted regardless of the
type of systemic therapy administered. From this data set, subgroups that would benefit from
radiation can be identified.35 In an analysis of women with node-positive breast cancer enrolled
on the NSABP B28 trial, recurrence score again correlated with local-regional failure,
contributing prognostic information beyond the traditional clinical factors such as the number of
involved lymph nodes.36
Routine testing for individual tumor sensitivity to radiotherapy appears to be on the horizon.
Investigators who underwent an in-vitro study of 16 breast cancer cell lines found that, after
exposure to 2 Gy, the surviving fraction ranged from 17 percent to 77 percent.37 A 51-gene
radiosensitivity signature was then developed, which predicted local-regional failure better than
traditional clinical factors, with a sensitivity of 84 percent and a negative predictive value of 89
percent.37 In 2015, Torres-Roca et al identified radioresistant and radiosensitive populations in a
cohort of over 300 patients treated with adjuvant radiotherapy by combining the radiosensitivity
index and molecular subtype. The triple-negative, radioresistant group had a higher risk of local-
regional failure than the triple-negative, radiosensitive group, whose local-regional failure rates
were comparable to those with luminal breast cancers. A luminal, radioresistant cohort was also
identified. One year later, Scott et al combined a genomic radiosensitivity index and the
radiobiologic linear quadratic model to create the genomic-adjusted radiation dose model. Such a
model may allow prospective trials to test and validate these promising genomic assays along a

sliding scale of radiation dose, from omission of radiation to dose de-escalation to dose
escalation. Late radiation toxicity may also be influenced by genomics.38,39 Knowledge of patient
susceptibility to radiation injury of healthy tissue could triage patients towards a certain radiation
modality or delivery technique. Those most sensitive to radiation damage may benefit most from
advanced, maximal organ-sparing techniques, such as proton therapy. An expert panel convened
at the National Institutes of Health in 2016 to review the current status of genomically guided
radiotherapy and outline the journey ahead to move from the lab to the bedside with
individualized, precision radiotherapy.40
Conclusion
The optimal radiation technique to treat breast cancer may vary with the treatment volume,
patient anatomy, and laterality of the breast cancer. However, the initial step of accurate target
and OAR delineation is essential to high-quality radiotherapy regardless of delivery technique.
Current challenges include reducing radiation exposure to normal, non-targeted tissues
(especially the heart and lung) while improving the coverage of critical breast cancer targets,
such as regional nodes. Compared to conventional 3DCRT, the use of IMRT and VMAT
improve conformality of the high dose to the target regions but at the expense of exposing a
greater volume of uninvolved adjacent tissue (contralateral breast and lung) to low radiation
doses. Proton therapy improves target coverage, achieves conformality of the high-dose volume
to the target, and significantly reduces both OAR and integral doses. Advanced radiation
techniques may further enhance the therapeutic ratio through increased target coverage and/or
reduction of critical organ exposure and allow for dose escalation, intensification, or
hypofractionation to further improve outcomes. Genomic analysis for tumor and healthy tissue
radiosensitivity appears to be a key step in the forward progress of precision radiotherapy,

allowing for tailoring of radiation dose and modality. Significant improvements in patient
outcomes are anticipated with these novel techniques, but a minimum of 10 years of follow-up
will be necessary to confirm expectations.
References
1. Whelan TJ, Olivotto IA, Parulekar WR, et al. Regional nodal irradiation in early-stage
breast cancer. N Engl J Med. 2015 Jul 23;373(4):307-16.
2. Poortmans PM, Collette S, Kirkove C, et al. Internal mammary and medial
supraclavicular irradiation in breast cancer. N Engl J Med. 2015 Jul 23;373(4):317-27.
3. Vicini FA, Radiation Therapy Oncology Group. RTOG 1005: A phase III trial of
accelerated whole breast irradiation with hypofractionation plus concurrent boost versus standard
whole breast irradiation plus sequential boost for early-stage breast cancer. 2014 Jul 31.
4. Pereira GC, Traughber M, Muzic RF, Jr. The role of imaging in radiation therapy
planning: past, present, and future. BioMed Res Int. 2014;2014:231090.
5. Bentel G, Marks LB, Hardenbergh P, et al. Variability of the location of internal
mammary vessels and glandular breast tissue in breast cancer patients undergoing routine CT-
based treatment planning. Int J Radiat Oncol Biol Phys. 1999 Jul 15;44(5):1017-25.
6. Saito AI, Vargas C, Morris CG, et al. Differences between current and historical breast
cancer axillary lymph node irradiation based on arm position: implications for radiation
oncologists. Am J Clin Oncol. 2009 Aug;32(4):381-6.

7. Li XA, Tai A, Arthur DW, et al. Variability of target and normal structure delineation for
breast cancer radiotherapy: an RTOG Multi-Institutional and Multiobserver Study. Int J Radiat
Oncol Biol Phys. 2009 Mar 1;73(3):944-51.
8. White J, Tai A, Arthur D, et al. Breast cancer atlas for radiation therapy planning:
consensus definitions [Internet]. 2017 [cited 2017 May 7]. Available from:
https://www.rtog.org/LinkClick.aspx?fileticket=vzJFhPaBipE=
9. Brown LC, Diehn FE, Boughey JC, et al. Delineation of supraclavicular target volumes
in breast cancer radiation therapy. Int J Radiat Oncol Biol Phys. 2015 Jul 1;92(3):642-9.
10. Jethwa KR, Kahila MM, Hunt KN, et al. Delineation of internal mammary nodal target
volumes in breast cancer radiation therapy. Int J Radiat Oncol Biol Phys. 2017 Mar
15;97(4):762-9.
11. Gentile MS, Usman AA, Neuschler EI, et al. Contouring guidelines for the axillary
lymph nodes for the delivery of radiation therapy in breast cancer: evaluation of the RTOG
breast cancer atlas. Int J Radiat Oncol Biol Phys. 2015 Oct 1;93(2):257-65.
12. Nielsen MH, Berg M, Pedersen AN, et al. Delineation of target volumes and organs at
risk in adjuvant radiotherapy of early breast cancer: national guidelines and contouring atlas by
the Danish Breast Cancer Cooperative Group. Acta Oncol. 2013 May;52(4):703-10.
13. Verhoeven K, Weltens C, Remouchamps V, et al. Vessel based delineation guidelines for
the elective lymph node regions in breast cancer radiation therapy - PROCAB guidelines.
Radiother Oncol. 2015 Jan;114(1):11-6.
14. Guan H, Dong YL, Ding LJ, et al. Morphological factors and cardiac doses in whole
breast radiation for left-sided breast cancer. Asian Pac J Cancer Prev. 2015;16(7):2889-94.

15. Kubasov IV. [The potassium ion yield from the frog muscle studied using a contact ion-
selective electrode]. Fiziol Zh SSSR Im I M Sechenova. 1990 Nov;76(11):1550-6.
16. Sardar P, Kundu A, Chatterjee S, et al. Long-term cardiovascular mortality after
radiotherapy for breast cancer: a systematic review and meta-analysis. Clin Cardiol. 2017
Feb;40(2):73-81.
17. Henson KE, McGale P, Taylor C, et al. Radiation-related mortality from heart disease
and lung cancer more than 20 years after radiotherapy for breast cancer. Br J Cancer. 2013 Jan
15;108(1):179-82.
18. Popescu CC, Olivotto IA, Beckham WA, et al. Volumetric modulated arc therapy
improves dosimetry and reduces treatment time compared to conventional intensity-modulated
radiotherapy for locoregional radiotherapy of left-sided breast cancer and internal mammary
nodes. Int J Radiat Oncol Biol Phys. 2010 Jan 01;76(1):287-95.
19. Webb S. Volumetric-modulated arc therapy: its role in radiation therapy [Internet].
Medical Physics Web; 2009 Jun 25 [cited 2017 May 7]. Available from:
http://medicalphysicsweb.org/cws/article/opinion/39542.
20. Johansen S, Cozzi L, Olsen DR. A planning comparison of dose patterns in organs at risk
and predicted risk for radiation induced malignancy in the contralateral breast following
radiation therapy of primary breast using conventional, IMRT and volumetric modulated arc
treatment techniques. Acta Oncol. 2009;48(4):495-503.
21. Boman E, Rossi M, Haltamo M, et al. A new split arc VMAT technique for lymph node
positive breast cancer. Phys Med. 2016 Oct 28.

22. Donovan E, Bleakley N, Denholm E, et al. Randomised trial of standard 2D radiotherapy
(RT) versus intensity modulated radiotherapy (IMRT) in patients prescribed breast radiotherapy.
Radiother Oncol. 2007 Mar;82(3):254-64.
23. Mulliez T, Veldeman L, van Greveling A, et al. Hypofractionated whole breast
irradiation for patients with large breasts: a randomized trial comparing prone and supine
positions. Radiother Oncol. 2013 Aug;108(2):203-8.
24. Barnett GC, Wilkinson JS, Moody AM, et al. The Cambridge Breast Intensity-modulated
Radiotherapy Trial: patient- and treatment-related factors that influence late toxicity. Clin Oncol
(R Coll Radiol). 2011 Dec;23(10):662-73.
25. Livi L, Meattini I, Marrazzo L, et al. Accelerated partial breast irradiation using intensity-
modulated radiotherapy versus whole breast irradiation: 5-year survival analysis of a phase 3
randomised controlled trial. Eur J Cancer. 2015 Mar;51(4):451-63.
26. Pignol JP, Truong P, Rakovitch E, et al. Ten years results of the Canadian breast intensity
modulated radiation therapy (IMRT) randomized controlled trial. Radiother Oncol. 2016
Dec;121(3):414-9.
27. Buwenge M, Cammelli S, Ammendolia I, et al. Intensity modulated radiation therapy for
breast cancer: current perspectives. Breast Cancer (Dove Med Press). 2017 Mar 6;9:121-6.
28. Ares C, Khan S, Macartain AM, et al. Postoperative proton radiotherapy for localized and
locoregional breast cancer: potential for clinically relevant improvements? Int J Radiat Oncol
Biol Phys. 2010 Mar 1;76(3):685-97.
29. Xu N, Ho MW, Li Z, et al. Can proton therapy improve the therapeutic ratio in breast
cancer patients at risk for nodal disease? Am J Clin Oncol. 2014 Dec;37(6):568-74.

30. MacDonald SM, Patel SA, Hickey S, et al. Proton therapy for breast cancer after
mastectomy: early outcomes of a prospective clinical trial. Int J Radiat Oncol Biol Phys. 2013
Jul 1;86(3):484-90.
31. Cuaron JJ, Chon B, Tsai H, et al. Early toxicity in patients treated with postoperative
proton therapy for locally advanced breast cancer. Int J Radiat Oncol Biol Phys. 2015 Jun
1;92(2):284-91.
32. Bradley JA, Dagan R, Ho MWet al. Initial Report of a Prospective Dosimetric and
Clinical Feasibility Trial Demonstrates the Potential of Protons to Increase the Therapeutic Ratio
in Breast Cancer Compared With Photons. Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):411-
21.
33. Manem VSK, Dhawan A. Modelling recurrence and second cancer risks induced by
proton therapy. Math Med Biol. 2017 Jul 4.
34. Tommasino F, Durante M, D'Avino V, et al. Model-based approach for quantitative
estimates of skin, heart, and lung toxicity risk for left-side photon and proton irradiation after
breast-conserving surgery. Acta Oncol. 2017 May;56(5):730-6.
35. Mamounas EP, Tang G, Fisher B, et al. Association between the 21-gene recurrence
score assay and risk of locoregional recurrence in node-negative, estrogen receptor-positive
breast cancer: results from NSABP B-14 and NSABP B-20. J Clin Oncol. 2010 Apr
1;28(10):1677-83.
36. Mamounas EP, Liu Q, Paik S, et al. 21-gene recurrence score and locoregional recurrence
in node-positive/ER-positive breast cancer treated with chemo-endocrine therapy. J Natl Cancer
Inst. 2017 Jan 25;109(4).

37. Speers C, Zhao S, Liu M, et al. Development and validation of a novel radiosensitivity
signature in human breast cancer. Clin Cancer Res. 2015 Aug 15;21(16):3667-77.
38. Popanda O, Marquardt JU, Chang-Claude J, et al. Genetic variation in normal tissue
toxicity induced by ionizing radiation. Mutat Res. 2009 Jul 10;667(1-2):58-69.
39. Chang-Claude J, Ambrosone CB, Lilla C, et al. Genetic polymorphisms in DNA repair
and damage response genes and late normal tissue complications of radiotherapy for breast
cancer. Br J Cancer. 2009 May 19;100(10):1680-6.
40. Hall WA, Bergom C, Thompson RF, et al. Precision oncology and genomically guided
radiation therapy: a report from the American Society for Radiation Oncology/American
Association of Physicists in Medicine/National Cancer Institute Precision Medicine Conference.
Int J Radiat Oncol Biol Phys. 2017 Jun 9.

Figure Legend
Figure 1: (A) Tumor involving an inframammary crease warrants a generous inferior border of
the radiation field to ensure adequate coverage of tissue at risk for harboring microscopic
disease. (B) Supraclavicular nodes extending posteriorly, beyond typical contouring guideline
recommendations, highlights the need for adaptation of the guidelines to the individual patient
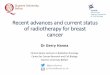
Figure 2: (A) An image from a computed tomography verification scan at fraction 10 of
radiotherapy shows a new seroma posterior to the expander at the inferior aspect (top image) that
was not present on the CT simulation images (bottom image). (B) The 3-dimensional conformal
dose distribution was not affected by the seroma development.
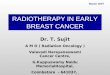
Figure 3: Comparison treatment plans for a patient with breast cancer, including (A) 3-
dimensional conformal radiotherapy, (B) intensity-modulated radiotherapy, (C) volumetric
modulated arc therapy, (D) and pencil-beam scanning with protons.
10% of the prescription dose is shown in orange, 50% in green, 90% in light blue, 95% in pink,
and 110% in dark blue.
In (A), there is a small amount of high dose to the heart but less low dose compared to (B) and
(C). In (B) and (C), there is less high dose to the ipsilateral lung but an increased volume of low
dose. In (D), both low and high doses are eliminated from the heart and lung while maintaining
95% coverage of the targets (the breast and internal mammary nodes).
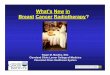
Figure 4: (A) The path of a single proton as it enters the body and deposits the vast majority of
its energy at a single point. This phenomenon is referred to as the Bragg peak. Oncologists can
manipulate the deposition depth by controlling the speed of the proton in addition to controlling
the target area, thereby reducing radiation to normal tissue. (B) A comparison of the amount of

radiation delivered with conventional photon radiation therapy versus proton therapy.
Conventional therapy is distinguished by a relatively high entrance dose and exit dose. By
contrast, proton therapy has a much lower entrance dose and no exit dose. The goal in radiation
therapy is to minimize damage to healthy tissue by minimizing the tissue exposed in the entrance
and exit doses. Borrowed with permission from UF Health Proton Therapy Institute.

Figure 1 A
Figure 1 B

Figure 2A

Figure 2B

Figure 3

Figure 4

New Advances in Breast Radiotherapy CME Test
Return by May 1, 2021 by Email to [email protected]
1. How does the RTOG contouring atlas define target nodal areas in the treatment of breast cancer?
a. 5mm margin around vessels b. bone and muscle c. based only on pre-treatment imaging d. definitions vary based on patient age and body mass index
2. The purpose of clips placed in the tumor bed at the time of surgery is to:
a. decrease the risk of infection b. minimize post-operative risk of bleeding c. improve accuracy of post-treatment mammogram surveillance d. ensure full coverage of the tumor bed with the prescribed dose of radiation
3. Evaluation by radiation oncology early in the work-up and assessment of a patient is important
because: a. radiation should be the initial step in breast cancer treatment. b. CT simulation is required prior to the start of other therapies. c. radiation dose and fields may be tailored based on clinical findings at initial diagnosis. d. the radiation modality should be determined at that time.
4. Which of the following factors does not affect plan robustness?
a. prescription dose b. respiratory motion c. treatment delivery time d. change in seroma
5. Advantages of 3D conformal radiation therapy over IMRT or VMAT include all of the following
except: a. less low dose exposure to normal tissues b. less sensitive to daily differences in patient set-up c. increased conformality of high dose d. increased robustness in the setting of breast edema
6. Which of the following modalities uses a continuous arc to deliver radiation dose?
a. 3D CRT b. IMRT c. VMAT d. Proton therapy

7. Which modality eliminates the exit dose beyond the target volume? a. 3D CRT b. IMRT c. VMAT d. Proton therapy
8. The sharp fall-off of dose at the end of the proton path is called the:
a. given dose b. Bragg peak c. beam angle d. Compton effect
9. One advantage of proton therapy compared to IMRT or VMAT is:
a. decreased dose to adjacent organs such as heart, lung and contralateral breast b. increased conformality of high dose c. decreased skin dose d. target contouring is not necessary
10. What is the sensitivity of the 51-gene radiosensitivity signature?
a. 17% b. 51% c. 77% d. 84%