Embed Size (px)
Citation preview

San Antonio Breast Cancer Symposium San Antonio Breast Cancer Symposium 2007 Highlights – Radiotherapy2007 Highlights – Radiotherapy
Kathleen C. Horst, M.D.Kathleen C. Horst, M.D.
Assistant ProfessorAssistant ProfessorDepartment of Radiation OncologyDepartment of Radiation Oncology
Stanford UniversityStanford University

Post-lumpectomy XRTTechniqueFractionationPartial Breast Irradiation
Post-mastectomy XRT
Nodal XRT

The Cambridge Breast Intensity Modulated Radiotherapy (IMRT) Trial: Dosimetry Results
Abstract # 4086 Coles, et al.
1089 patients with breast cancer treated with BCT
Standard treatment plan
< 2 cm3 of breast tissue > 107% > 2 cm3 of breast tissue > 107%
Non-randomized Randomized
Standard RT IMRT

317/1089 (29%) had acceptable homogeneity with standard 2D radiotherapy.
IMRT significantly reduced both “hot spots” and “cold spots”.
The Cambridge Breast Intensity Modulated Radiotherapy (IMRT) Trial: Dosimetry Results
Abstract # 4086 Coles, et al.




Prospective trial of individual optimal positioning (prone vs supine) for whole breast radiotherapy: results of 224 patients
Abstract # 4082 Formenti, et al.

Prospective trial of individual optimal positioning (prone vs supine) for whole breast radiotherapy: results of 224 patients
Abstract # 4082 Formenti, et al.
CONCLUSIONS:Prone enables best sparing of heart and lung in most patients (204/224)Most patients best treated supine (17/20) had left-sided lesions
When prone, heart is displaced anteriorly 5-19 mm (Duke)May limit utility of prone technique

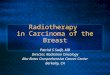
Node-NegativePost BCS
1234 patients
Accelerated Hypofractionated Whole Breast Irradiation (AHWBI)
42.5 Gy/16 fractions622 patients
Standard Whole Breast Irradiation (SWBI)
50 Gy/25 fractions612 patients
Stratification: Age Size Systemic tx Center
Recruitment April ’93- Sept ’96
R
Radiotherapy Fractionation SchedulesRadiotherapy Fractionation SchedulesAbstract #21 Whelan, et al.
Long-term results of a randomized trial of accelerated hypofractionated whole breast irradiation following breast conserving surgery in women with node negative breast cancer

SWBI AHWBI n=612 n=622 n (%) n (%)
Age < 50 yrs 148 (24) 157 (25)Tumor size ≥ 2 cm 203 (33) 190 (31)ER negative 157 (26) 165 (26)Tumor grade high 116 (21) 117 (20)Tamoxifen 266 (41) 265 (41)Chemotherapy 72 (11) 75 (11)
BASELINE CHARACTERISTICS

LOCAL RECURRENCE
SWBI AHWBI
5 years 3.2% 2.8%10 years 6.7% 6.2%
No difference in Overall Survival
Whelan T, et al. J Natl Cancer Inst. 94(15):1143-50, 2002. Whelan T, et al. Abstract #21. SABCS 2007.
Radiotherapy Fractionation SchedulesRadiotherapy Fractionation SchedulesAbstract #21 Whelan, et al.

SWBI AHWBI
Age (y) < 50 10.7 7.5 ≥ 50 5.4 5.8
Tumor < 2 cm 6.1 5.4Size (cm) ≥ 2 cm 7.8 8.0
Systemic yes 5.9 6.5Therapy no 7.4 5.8
Local Recurrence Rates at 10 years

Baseline 3 yr 5 yr 10 yr
SWBI 83% (604) 77% (496) 79% (423) 71% (216)
AHWBI 84% (616) 77% (518) 78% (448) 70% (235)
Cosmetic Outcome by Time and Treatment
% excellent or good (# evaluable)

3 yr 5 yr 10 yr
SkinSWBI 2% 3% 8% AHWBI 2% 3% 9%
Subcutaneous tissueSWBI 5% 6% 11% AHWBI 4% 5% 12%
% Grades 2-3
RTOG/EORTC Late Radiation Morbidity by Time and Treatment

SWBI AHWBI (n=612) (n=622)
Cancer related 13.2% (81) 13.7% (85)
Non-cancer related 7.4% (45) 5.9% (37)
Total 20.6% (126) 19.6% (122)
Cause of Death

Accelerated Hypofractionated Whole Breast Irradiation:
• Demonstrated excellent local control
• Was not associated with long-term morbidity
• Skin and soft tissue toxicity• Breast Cosmesis• Non-cancer deaths
CONCLUSIONS

JCO. 25:18S (June 20 Supplement), 2007: LBA518
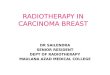
T1-3, N0-1Post BCS
Recruitment 1999-2002
Radiotherapy Fractionation SchedulesRadiotherapy Fractionation SchedulesASCO 2007 Dewar, et al.
Hypofractionation for early breast cancer: First results of the UK standardisation of breast radiotherapy (START) trials
START A2236 patients
50 Gy/25 fractions/5 weeks
41.6 Gy/13 fractions/5 weeks
39 Gy/13 fractions/5 weeks
START B2215 patients 40 Gy/15 fractions/3 weeks
50 Gy/25 fractions/5 weeks

Radiotherapy Fractionation SchedulesRadiotherapy Fractionation Schedules
RATIONALE
Tumor response (i.e., local control) thought to be as sensitive to fraction size as late adverse effects
Radiation fraction sizes > 2.0 Gy may have advantages in breast cancer treatment1
Goals: test the benefit of fraction sizes > 2.0 Gy in terms of locoregional controllate normal tissue responses
1Owen R et al. Lancet Oncol 7:467-71, 2006.

Radiotherapy Fractionation SchedulesRadiotherapy Fractionation SchedulesASCO 2007 Dewar, et al.
Hypofractionation for early breast cancer: First results of the UK standardisation of breast radiotherapy (START) trials
Median follow up = 5.1 yrs Median follow up = 6.0 yrs

Radiotherapy Fractionation SchedulesRadiotherapy Fractionation SchedulesASCO 2007 Dewar, et al.
Hypofractionation for early breast cancer: First results of the UK standardisation of breast radiotherapy (START) trials

Are patients with T1-2 breast cancer with 1-3 +LN suitable candidates for partial breast radiotherapy trial enrollment?
Abstract # 4089 Truong, et al.

Are patients with T1-2 breast cancer with 1-3 +LN suitable candidates for partial breast radiotherapy trial enrollment?
Abstract # 4089 Truong, et al.
5688 women
pT1-2, 0-3 N+ breast ca
Treated with BCT (1989-1999)
N0 (n=4433) vs 1-3 N+ (n=1255)
Median follow up = 8.6 yrs

Are patients with T1-2 breast cancer with 1-3 +LN suitable candidates for partial breast radiotherapy trial enrollment?
Abstract # 4089 Truong, et al.

Are patients with T1-2 breast cancer with 1-3 +LN suitable candidates for partial breast radiotherapy trial enrollment?
Abstract # 4089 Truong, et al.
CONCLUSIONS:
Patients with 1-3 N+ have high risks of regional nodal relapse ~10-15% despite standard whole breast XRT and systemic therapy, particularly
young agegrade III histologyER- disease>20% positive nodes
Such patients should receive standard whole breast XRT and are not ideal candidates for PBI trial enrollment

Update of the Phase II MammoSite Brachytherapy Trial for DCISAbstract # 4079 Streeter, et al.

NSABP B39/RTOG 0413 Interstitial/intracavitary brachytherapy, 3DCRT
European Institute of Oncology Intraoperative electrons
TARGIT Intrabeam – photoelectron 50 kV photons
RAPID Canadian External Beam
Ongoing Trials in Partial Breast Irradiation
Other Intraoperative techniques Stanford University of North Carolina MSKCC (Intraoperative HAM applicator)
Protons MGH
Permanent radioactive seed University of Toronto, Canada
Other Intracavitary applicators Cianna Medical SenoRx North American Scientific Xoft

Identification of Patients for Post-Mastectomy Radiotherapy using the Cambridge Index
Abstract # 4093 Wilson, et al.
Index designed to help identify intermediate and low risk patients who might be at higher risk of local recurrence after mastectomy.
Applied since 1999. Retrospective review of patients from 2000-2003

Low level of LR in both the Low and Intermediate risk groups confirms that appropriate patients in the Intermediate risk group are receiving PMRT
Identification of Patients for Post-Mastectomy Radiotherapy using the Cambridge Index
Abstract # 4093 Wilson, et al.
Intermediate risk Score < 3 (n=21)
Low riskScore < 3 (n=131)
Chest Wall XRT n=198 (55%)
No XRT n=159 (45%)
High risk (n=125)
Intermediate risk Score > 3 (n=63)
Low riskScore > 3 (n=17)

Increased use of regional radiotherapy is associated with improved outcome in a population based cohort of women with
breast cancer and 1-3 positive nodesAbstract # 4076 Wai, et al.

EORTC 10925LN+ or any medial/central lesionBreast Only vs Breast + Upper IM/Medial SCV
NCIC MA.20LN+ and high risk LN-Breast Only vs Breast + Upper IM, high axilla, SCV
Ongoing Trials in Regional Nodal RT in Breast Conservation Therapy

Post-operative radiotherapy does not adversely affect the outcome of autologous free abdominal flap breast
reconstructionAbstract # 4084 Chatterjee, et al.
• No significant difference by objective mammometry in the volume of reconstructed breast compared with contralateral breast
• No significant difference in fibrosis and thickening in the reconstructed breast
• Postoperative XRT does not adversely affect the outcome of immediate DIEP reconstruction following mastectomy