Embed Size (px)
Citation preview

NEUROTRANSMITTERRESOURCE GUIDE
Science + Insight
doctorsdata.com

www.doctorsdata.com
Table of Contents
Sample Report
Sample Report ...........................................................................................................................................................................
Analyte Considerations
Phenylethylamine (B-phenylethylamine or PEA) .................................................................................................Tyrosine ..........................................................................................................................................................................................Tyramine ........................................................................................................................................................................................Dopamine .....................................................................................................................................................................................3, 4-Dihydroxyphenylacetic Acid (DOPAC) ...............................................................................................................3-Methoxytyramine (3-MT) ...............................................................................................................................................Norepinephrine .........................................................................................................................................................................Normetanephrine ....................................................................................................................................................................Epinephrine .................................................................................................................................................................................Metanephrine .............................................................................................................................................................................Norepinephrine/Epinephrine Ratio ..............................................................................................................................Tryptamine ...................................................................................................................................................................................Serotonin .......................................................................................................................................................................................5-Hydroxyindolacetic Acid (5-HIAA) .............................................................................................................................Glutamate .....................................................................................................................................................................................Gamma-aminobutyrate ......................................................................................................................................................Glycine ............................................................................................................................................................................................Histamine ......................................................................................................................................................................................Taurine ............................................................................................................................................................................................Creatinine ......................................................................................................................................................................................
Neurotransmitter Pathways
Neurotransmitter Pathways ..............................................................................................................................................
Treatment Considerations
Treatment Considerations ..................................................................................................................................................
References
References .....................................................................................................................................................................................
1
1346791011131416171820222325262829
30
31
37
Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 1
www.doctorsdata.com
Analyte Considerations
Phenylethylamine (PEA) LOW
Summary from report:
Low phenethylamine (PEA) may be associated with depression, attention deficits and hyperactivity(ADHD), Parkinson’s disease and bipolar disorder. Phenylalanine is the precursor amino acid to PEA, andvitamin B6 is a required co-factor in the conversion to this primary trace amine. Use of Reserpine can resultin depletion of PEA.
Sample Report
Order:SAMPLE REPORT Page: 2 of 3
Low dopamine may be associated with anxiety/depression, difficulty concentrating, decreased libido and obesity, and may be associated withincreased addiction and other stimulation seeking activities. Failure to regenerate tetrahydrobiopterin [BH4], an essential cofactor for dopaminesynthesis, may decrease dopamine levels, and could be reflected in urine. BH4 regeneration may be supported by folates, vitamin B3, C,molybdenum and zinc. Additionally, production of dopamine requires vitamin D, iron and vitamin B6. L-tyrosine, L-theanine and Mucuna pruriensmay influence dopamine signaling.DOPAC levels may be low simply if dopamine levels are low. DOPAC is the primary metabolite of dopamine formed by MAO activity. Alternativelylow levels of DOPAC may be associated with medications such as adrenergic antagonists, monoamine or norepinephrine reuptake inhibitors.Low DOPAC levels may also indicate low activity of MAO-A. Vitamins B2, B3, B6, and iron are required for optimal dopamine metabolism.Although a low level of urinary DOPAC is absolutely not diagnostic, low DOPAC levels in cerebral spinal fluid have been associated withParkinson’s disease.Elevated epinephrine may be associated with stress response and contributory to anxiety, agitation, irritability, insomnia and hypertension.Epinephrine levels may be elevated in patients in association with exercise prior to the urine collection. Metabolism of epinephrine requiresvitamins B2, B3, SAMe, magnesium, and iron. L-theanine may modulate epinephrine effects.Low serotonin may contribute to mood concerns including anxiety, OCD, depression, anger and a sense of discontentment. Low serotonin mayalso be associated with poor sleep quality and appetite changes, as well as chronic fatigue, rheumatoid arthritis, and over-all lassitude. Failure toregenerate tetrahydrobiopterin [BH4], an essential cofactor for serotonin synthesis, may decrease serotonin levels, and could be reflected inurine. BH4 regeneration may be supported by folates, vitamin B3, C, molybdenum and zinc. Additionally, production of serotonin requires vitaminD, iron and vitamin B6. Tryptophan is the essential precursor of serotonin. 5-HTP may increase serotonin, and L-theanine may affect serotoninfunction.Low 5-HIAA may be associated with mood concerns including depression and anxiety, sleep changes, and poor concentration. Low 5-HIAA maybe associated with low precursor serotonin, or compromised metabolism of serotonin by MAO-A. Some medications, including aspirin, MAO-inhibitors, levodopa, and tricyclic antidepressants may decrease 5-HIAA levels. MAO may be inhibited by cigarette smoke. Vitamins B2, B3, B6,magnesium and iron are required for optimal serotonin metabolism. If MAO-A enzyme function is inhibited, serotonin may be elevated and 5-HIAA will be low.Upper range glutamate may contribute to anxiety, poor concentration, attention deficits and hyperactive tendencies as well as poor sleep andnighttime awakening. Glutamate may be increased in association with hypoglycemia, Alzheimer’s, ALS and chronic compromised blood flow tothe brain. Possible sources of increased glutamate include MSG, yeast extract and other hidden sources of free glutamic acid. L-theanine maymodulate elevated glutamate levels and attenuate glutamate signaling, and taurine may provide protection from excitotoxicity andneuroinflammation.Low range GABA may be associated with anxiety, poor impulse control, depression, pain and decreased sleep quality. Low GABA may be seenin individuals deficient in vitamin B6. L-theanine, GABA and glutamine may positively affect functional GABA activity, and phenibut exerts GABA-like effects (experimental models).Considerations to address the demonstrated imbalances beyond the identified co-factors and amino acid precursors may include dosageadjustments if indicated, as well as nervine and adaptogenic herbs, methylation support, vitamin D, and gastrointestinal health optimization.
Analyzed by DOCTOR’S DATA, INC. • 3755 Illinois Avenue, St. Charles, IL 60174-2420 USA • LAB DIR: Erlo Roth, MD • CLIA ID: 14D0646470
Order:SAMPLE REPORT
Client #:12345Doctor:Sample DoctorDoctor's Data, Inc.3755 Illinois Ave.St. Charles, IL 60174
Patient:Sample PatientAge:35Sex:FemaleBody Mass Index (BMI):20.0
Sample Collection Date/TimeDate Collected 01/21/2020Wake Up Time 07:30Collection Period 1st morning voidDate Received 01/22/2020Date Reported 01/23/2020
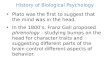
Notes:Results are creatinine corrected to account for urine dilution variations. Creatinine is not meant to be used as an indicator of renal function.RI= Reference Interval, L (blue)= Low (below RI), WRI (green)= Within RI (optimal), WRI (yellow)= Within RI (not optimal), H (red)= High (above RI)
Urinary neurotransmitter levels provide an overall assessment of the body's ability to make and break down neurotransmitters and arerepresentative of whole body levels. Neurotransmitters are secreted all through the body, in neurons of both the central and peripheral nervoussystems. The enzymes, cofactors and precursors in neurotransmitter metabolism in general are the same in the periphery and in the centralnervous system. Therefore, alterations in urinary neurotransmitter levels assessed in urine provide important clinical information, and may beassociated with many symptoms including cognitive and mood concerns, diminished drive, fatigue and sleep difficulties, cravings, addictions andpain.Low phenethylamine (PEA) may be associated with depression, attention deficits and hyperactivity (ADHD), Parkinson’s disease and bipolardisorder. Phenylalanine is the precursor amino acid to PEA, and vitamin B6 is a required co-factor in the conversion to this primary trace amine.Use of Reserpine can result in depletion of PEA.
Neurotransmitter Comments:
Analyte Result Unit per Creatinine L WRI H Reference Interval
5-Hydroxyindoleacetic acid (5-HIAA) 1985 µg/g 2000 – 8000
3,4-Dihydroxyphenylacetic acid (DOPAC) 380 µg/g 390 – 1500
3-Methoxytyramine (3-MT) 125 nmol/g 90 – 210
Normetanephrine 200 µg/g 85 – 300
Metanephrine 98 µg/g 45 – 119
Tryptamine 0.5 µmol/g 0.20 – 0.90
Tyrosine 45 µmol/g 32 – 80
Taurine 560 µmol/g 320 – 1000
Tyramine 3.0 µmol/g 2.0 – 4.0
Serotonin 26 µg/g 60 – 125
Dopamine 120 µg/g 125 – 250
Norepinephrine 45 µg/g 22 – 50
Epinephrine 9 µg/g 1.6 – 8.3
Norepinephrine / Epinephrine ratio 5 < 13
Glutamate 35 nmol/g 12.0 – 45.0
Gamma-aminobutyrate (GABA) 2.1 nmol/g 2.0 – 5.6
Glycine 2000 nmol/g 450 – 2200
Histamine 32 µg/g 14 – 44
Phenethylamine (PEA) 31 nmol/g 32 – 84
Creatinine 120 mg/dL 30 – 225
Analyzed by DOCTOR’S DATA, INC. • 3755 Illinois Avenue, St. Charles, IL 60174-2420 USA • LAB DIR: Erlo Roth, MD • CLIA ID: 14D0646470Methodology: LCMS QQQ,Creatinine by Jaffe Reaction
Comprehensive Neurotransmitter

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 2
www.doctorsdata.com
Expanded information:
The level of phenylethylamine (B-phenylethylamine or PEA) is lower than expected in this sample. PEA is considered a trace amine neuromodulator; it modifies the effects of neurotransmitter signals on cells or receptors. Trace amines may be found in both the central and peripheral nervous systems – there are trace amine receptors in vascular and renal tissues. Trace amines and their metabolites are excreted through the kidney into the urine.
Low PEA levels have been associated with Parkinson’s disease, depression, attention deficit hyperactivity disorder (ADHD) and autism. Trace amines may play a role in the activation or regulation of immune responses. PEA may alter a cell’s response to dopamine and norepinephrine. PEA may have endocrine effects and inhibit prolactin secretion. Levels of PEA are not associated with neuronal responses to serotonin, GABA or glutamate. PEA is derived from the amino acid phenylalanine. Low levels of phenylalanine may contribute to low PEA levels. Phenylalanine levels may be depleted by stress. PEA synthesis requires vitamin B6. PEA excretion may be influenced by diurnal rhythms; larger amounts are excreted during the late evening and early morning hours.
Phenylethylamine (PEA) HIGH
Summary from report:
Elevated phenethylamine (PEA) may contribute to anxiety, with very high levels having amphetamine-like effects. Elevations in PEA may occur due to supplementation, use of monoamine oxidase inhibitors orantipsychotic medications, high protein diets, and production by protein-fermenting gut microbes. PEA and other trace amines are found in fermented foods (wine, cheese, chocolate, etc.). Elevated PEA levels may be associated with higher cortisol levels.
Expanded information:
The level of Phenylethylamine (B- phenylethylamine or PEA) is higher than expected in this sample. PEA is considered a trace amine neuromodulator; it modifies the effect of a neurotransmitter signal on a cell or receptor. Trace amines may be found in both the central and peripheral nervous systems – there are trace amine receptors in vascular and renal tissues. Trace amines and their metabolites are excreted through the kidney into the urine.
The interaction of trace amines and trace amine-associated receptors (TAARs) in the brain may play a role in psychiatric and neurological disease processes. Elevated PEA has been associated with schizophrenia. Experiments in humans and animals have associated PEA elevations with stress or anxiety. Very high levels may have amphetamine-like effects and may induce seizures (animal studies). Patients with hypertension or bone disease may also have elevated PEA levels. Elevations in PEA levels have been reported during the use of monoamine oxidase inhibitors (MAOIs) or antipsychotic medications. PEA may alter a cell’s response to dopamine and norepinephrine. PEA may have endocrine effects and inhibit prolactin secretion. Animal studies indicate that PEA may increase glucocorticoid levels and PEA

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 3
www.doctorsdata.com
has been shown to stimulate acetylcholine release. Levels of PEA are not associated with neuron responses to serotonin, GABA or glutamate. Monoamine oxidase inhibitor (MAOI) medications may increase trace amine levels without affecting levels of other neurotransmitters. Trace amines may play a role in the activation or regulation of immune responses. PEA excretion may be influenced by diurnal rhythms; larger amounts are excreted during the late evening and early morning hours. Exercise, high protein diets or supplements may also increase PEA levels. High levels of the phenylalanine may result in high PEA levels.
Trace amines may be generated in the gastrointestinal tract by protein-fermenting gut bacteria after a protein-rich meal, and they may be found in a variety of foods as the result of food spoilage or deliberate fermentation. Dietary trace amines are usually metabolized quickly by MAO enzymes. PEA is primarily oxidized by MAO-B which may require selenium.
Tyrosine LOW
Summary from report:
Tyrosine is the non-essential amino acid precursor for dopamine, norepinephrine and epinephrine. Tyrosine is derived from essential phenylalanine. Low tyrosine levels may increase irritability, and affect mood, mental performance, energy levels, body temperature and thyroid function. Low levels of the precursor amino acid phenylalanine may result in low levels of tyrosine and phenylethylamine (PEA). Chronic tyrosine deficiency may decrease catecholamine levels. An elevated phenylalanine, but low tyrosine level may indicate either inherited phenylketonuria (rare) or a lack of iron and/or tetrahydrobiopterin (BH4). BH4 regeneration may be supported by folates, vitamins B3 and C, molybdenum and zinc. Selenium deficiency may increase the conversion of tyrosine to L-DOPA (dopamine precursor).
Expanded information:
The level of tyrosine in this sample is lower than expected. Tyrosine, a non-essential amino acid, is the precursor for the catecholamine neurotransmitters dopamine, epinephrine and norepinephrine. Tyrosine is also a precursor for thyroid hormone.
Tyrosine is s synthesized in the liver from dietary phenylalanine, an essential amino acid, using a tetrahydropiopterin (BH4) as a cofactor. The proportion of tyrosine in systemic circulation is controlled by the enzymes in liver and kidney. Brain tyrosine levels mediate the rate of synthesis for the catecholamine neurotransmitters. Elevated glucocorticoid, insulin, glucagon, or tryptophan levels may induce the liver enzyme tyrosine aminotransferase, which may then, decreases tyrosine levels. Low levels of the phenylalanine precursor may contribute to low tyrosine levels.
Human studies of short-term dietary tyrosine depletion indicate that low tyrosine levels may increase prolactin levels and may lower mood and energy levels. Low tyrosine levels may impair aspects of spatial recognition memory, mental performance and increase irritability scores during psychological challenge testing. Tyrosine depletion has been reported to worsen clinical ratings for manic symptoms in patients. Low tyrosine levels have been associated with decreased body temperature and thyroid function.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 4
www.doctorsdata.com
Tyrosine HIGH
Summary from report:
Tyrosine is the non-essential amino acid precursor for dopamine, norepinephrine and epinephrine. Increased tyrosine may exacerbate migraine headaches and hyperthyroid conditions. Elevated tyrosine levels may occur due to supplementation (phenylalanine or tyrosine), heritable enzyme defects, or liver disease. Tyrosine hydroxylase converts tyrosine into the dopamine precursor L-DOPA; BH4, Vitamin D and iron are cofactors for that enzymatic activity.
Expanded information:
The level of tyrosine in this sample is higher than expected. Tyrosine is the precursor for the catecholamine neurotransmitters dopamine, epinephrine and norepinephrine. Brain tyrosine levels control the rate of synthesis for the catecholamine neurotransmitters. Tyrosine is also a precursor for thyroid hormone.
Elevated plasma tyrosine levels may result in seizures or developmental delays. Migraine headaches and hyperthyroid conditions may be exacerbated by elevated tyrosine levels. Tyrosine may interfere with medications such as MAO inhibitors, thyroid hormone replacement and L-dopa replacement. Human studies indicate that tyrosine supplementation may improve cognition and performance under stressful conditions.
Tyrosine is also synthesized in the liver from dietary phenylalanine, an essential amino acid. The proportion of dietary tyrosine that enters systemic circulation is controlled by the enzyme tyrosine aminotransferase (TAT) in liver and kidney. TAT requires vitamin B6 and alpha-ketoglutarate as cofactors. Oxidative stress has been shown to lower TAT activity (in vitro). Tyrosine levels may be elevated due to heritable enzyme defects (tyrosinemia), liver disease, or supplementation.
Tyramine LOW
Summary from report:
Tyramine is a trace amine derived directly from tyrosine by a B6-dependent enzyme. Decreased tyramine levels may be associated with depression. Low levels of tyramine may result if the level of the precursor amino acid tyrosine is low. B6 deficiency may decrease trace amine levels, but increase tyrosine. Tyramine is metabolized by MAO; its activity may be increased by oxidative stress. Antioxidants (selenium, pycnogenol, curcumin, berberine), and Vitamin B12 may normalize MAO activity levels.
Expanded information: The level of tyramine is lower than expected in this sample. Tyramine is derived from the essential amino acid phenylalanine. Tyramine and the other trace amines are found at low levels in the brain. Trace amines are not considered neurotransmitters; they are believed to act as neuromodulators. Evidence indicates that tyramine may alter neuronal responsiveness, neuron active transport mechanisms and vesicle dynamics. Low levels of the precursor amino acid phenylalanine or its metabolite tyrosine, may contribute to low tyramine levels. Reserpine may deplete CNS levels of trace amines. Trace amines and their metabolites are excreted through the kidney into the urine.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 5
www.doctorsdata.com
Multiple studies demonstrate that loss of neurons in specific brain areas or loss of specific types of neurons may result in decreased trace amine levels. Low tyramine levels or deficient trace amine functions may be associated with some depressive disorders. Tyramine has been shown to inhibit the responses of gamma-aminobutyric acid (GABA) receptors (in vitro).
Aromatic L-amino acid decarboxylase (AADC) is the rate-limiting enzyme in tyramine synthesis. Altered AADC activity may alter trace amine levels which may affect dopamine signaling. Loss of specialized dopamine neurons containing AADC have been associated with some forms of schizophrenia. Trace amines are metabolized by monoamine oxidase (MAO A/B).
Tyramine HIGH
Summary from report:
Tyramine is a trace amine derived directly from tyrosine by a B6-dependent enzyme. Elevated levels of tyrosine may increase tyramine levels, especially when metabolism to dopamine is compromised. Trace amines (tryptamine, tyramine, PEA) may have stimulant effects at high levels. Foodstuffs such as hard cheeses and red wines contain large amounts of tyramine. If tyramine is high, but dopamine is low, the enzymes of dopamine synthesis (folates, vitamins B3, D, zinc, molybdenum, iron cofactors) may be inhibited. Tyramine is normally metabolized by MAO; low enzyme activity may increase tyramine levels. Vitamin B2 may increase the activity of MAO enzymes.
Expanded information:
Tyramine is higher than expected in this sample. Tyramine is derived from the essential amino acid phenylalanine. Tyramine, and the other trace amines are found at low levels in the brain. Trace amines are not considered neurotransmitters; they are believed to act as neuromodulators. Evidence indicates that tyramine may alter neuronal responsiveness, neuron active transport mechanisms and vesicle dynamics. Trace amines and their metabolites are excreted through the kidney into the urine.
Both the function of trace amine–associated receptors (TAARs) and the level of trace amines are thought to contribute to altered brain activity Elevated levels of tyramine have been associated with some forms of schizophrenia. Elevated levels of a tryamine metabolite, octopamine, have been associated with migraine and cluster headaches. Tyramine has been shown to inhibit the responses of gamma-aminobutyric acid (GABA) receptors in vitro. Studies in vitro, and in vivo indicate that tyramine may inhibit prolactin secretion.
Trace amines may be generated in the gastrointestinal tract by protein-fermenting gut bacteria after a protein-rich meal, and they may be found in a variety of foods as the result of food spoilage or deliberate fermentation. Trace amines are commonly obtained from the diet in chocolate, aged cheeses and red wine. Dietary trace amines are usually metabolized quickly by MAO enzymes. Elevated levels of trace amines may occur due to phenylketonuria, exposure to ergot fungi or the use of MAO inhibitors.
Aromatic L-amino acid decarboxylase (AADC) is the rate-limiting enzyme in tyramine synthesis. Increased AADC activity increases trace amine levels, without affecting levels of monoamine neurotransmitters. Trace amines are metabolized by monoamine oxidase (MAO A/B).

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 6
www.doctorsdata.com
Dopamine LOW
Summary from report:
Low dopamine may be associated with anxiety/depression, difficulty concentrating, decreased libido and obesity, and may be associated with increased addiction and other stimulation seeking activities. Failure to regenerate tetrahydrobiopterin [BH4], an essential cofactor for dopamine synthesis, may decrease dopamine levels, and could be reflected in urine. BH4 regeneration may be supported by folates, vitamin B3, C, molybdenum and zinc. Additionally, production of dopamine requires vitamin D, iron and vitaminB6. L-tyrosine, L-theanine and Mucuna pruriens may influence dopamine signaling.
Expanded information:
The level of dopamine is lower than expected in this sample. Dopamine is a catecholamine neurotransmitter and hormone. Almost half of the dopamine synthesized in the body is found in the gastrointestinal tract (GIT). Decreased dopamine production or signaling in the CNS has been associated with attention deficit hyperactivity disorder (ADHD), mood disorders, sexual dysfunction, and obesity. Oxidative stress and mitochondrial dysfunction are common causes of neurodegeneration. The loss of dopamine-producing neurons is associated with neurodegenerative disorders such as Parkinson’s disease, and may result in motor symptoms such as rigidity, tremor or bradykinesia (slow movement). Manganese excess may also produce Parkinson’s-like symptoms.
Synthesis of dopamine in the CNS requires tetrahydrobiopterin, iron and vitamin B6. The availability of precursor amino acids phenylalanine or tyrosine may affect dopamine levels; however, some studies indicate that tyrosine supplements may decrease renal dopamine excretion. Dopamine is metabolized by monoamine oxidase (MAO) and catechol-O methyl transferase (COMT). Evidence indicates that most urinary excretion of dopamine may reflect renal conversion of the precursor 3, 4-dihydroxyphenylalanine (DOPA) to dopamine. Renal excretion of dopamine may decrease in cases of heart failure. Metyrosine therapy may decrease dopamine levels.
Dopamine HIGH
Summary from report:
Elevated dopamine may be associated with increased worry, distrust of others and decreased ability to interact socially and is often found in patients with attention deficits and hyperactivity. Medications thatmay increase dopamine levels include L-dopa, methyldopa, select antidepressants and some ADD/ADHD medications. L-theanine may modulate catecholamine effects. Metabolism requires vitamins B2, B3, SAMe,magnesium, and iron, while conversion to norepinephrine requires vitamin C, copper and vitamin B3.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 7
www.doctorsdata.com
Expanded information:
The level of dopamine is higher than expected in this sample. Dopamine is a catecholamine hormone and neurotransmitter. Almost half of the dopamine synthesized in the body is found in the gastrointestinal tract (GIT).
Elevated dopamine levels may affect behavior and have been associated with Obsessive-Compulsive Disorder, impulsivity, addictive behavior, schizophrenia, manic states and other psychiatric disorders. Research continues to determine if elevated dopamine or impaired dopamine receptors are the causative factor. Ongoing research indicates that dopamine synthesis may be increased in cases of post-streptococcal autoimmune encephalitis. Marked dopamine elevations in children have also been associated with rare physiologic conditions such as neuroblastoma, Costello syndrome, leukemia, pheochromocytoma, Menke’s disease and rhabdomyosarcoma of the bladder. Elevated urinary dopamine in adults has been associated with drug effects and physiologic conditions including pheochromocytoma, carcinoid tumor and pregnancy. Medications, including L-dopa, methyldopa, clozapine, antidepressants and metoclopramide, may elevate dopamine levels.
Dopamine is metabolized by monoamine oxidase (MAO) and catechol-O methyl transferase (COMT). Sulfotransferase (SULT) 1A3 metabolizes dopamine by a different process, sulfate conjugation.
3,4-dihydroxyphenyl acetic acid (DOPAC) LOW
Summary from report:
DOPAC levels may be low simply if dopamine levels are low. DOPAC is the primary metabolite of dopamine formed by MAO activity. Alternatively low levels of DOPAC may be associated with medications such as adrenergic antagonists, monoamine or norepinephrine reuptake inhibitors. Low DOPAC levels mayalso indicate low activity of MAO-A. Vitamins B2, B3, B6, and iron are required for optimal dopamine metabolism. Although a low level of urinary DOPAC is absolutely not diagnostic, low DOPAC levels in cerebral spinal fluid have been associated with Parkinson’s disease.
Expanded information:
The level of 3,4-dihydroxyphenyl acetic acid (DOPAC) is lower than expected in this sample. DOPAC is the major intermediary metabolite of dopamine. Research indicates that approximately one-third of newly synthesized dopamine is immediately processed to DOPAC, which is then secreted into the extracellular space between neurons. Evidence indicates that some sympathetic neurons may produce DOPAC, andthat DOPAC may be synthesized in both the central and peripheral nervous systems.
Evidence indicates that fasting and impedance of stimulation of the sympathetic nervous system decreased plasma DOPAC levels. In vitro studies indicate that exposure to high levels of manganese decrease DOPAC levels; manganese excess is associated with Parkinson’s-like symptoms. DOPAC levels may be decreased in patients with paroxysmal atrial fibrillation, pure autonomic failure,

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 8
www.doctorsdata.com
tetrahydrobiopterin (BH4) deficiency, or patients with chronic suppression of the activity of the sympathetic nervous system. Rat studies indicate that DOPAC levels may decrease with prolonged or chronic stress. Metyrosine therapy which decreases the activity of tyrosine hydroxylase will decrease levels of dopamine and may result in low DOPAC levels.
Dopamine is metabolized by monoamine oxidase (MAO) and aldehyde dehydrogenase to DOPAC. MAO and noradrenalin reuptake inhibitors may decrease plasma DOPAC levels.
3,4-dihydroxyphenyl acetic acid (DOPAC) HIGH
Summary from report:
DOPAC may be high if dopamine is also high. Ask about use of L-DOPA. DOPAC is the primary metaboliteof dopamine formed by MAO activity. MAO-A activity may increase due to oxidative stress. An elevated DOPAC level can indicate increased dopamine breakdown, leading to increased levels of free radicals. The oxidative stress can affect neurotransmitter pathways. Antioxidants (selenium, pycnogenol, curcumin, berberine), and Vitamin B12 may ameliorate heightened MAO activity. DOPAC may also be high with acute stress or the use of reserpine or other dopamine reuptake inhibitors. Low activity of COMT may also increase DOPAC (and decrease 3MT). Check 3MT for that pattern. SAMe and Mg are essential for normal methylation and COMT activity. The Plasma Methylation Profile might be considered to evaluatemethylation issues.
Expanded information:
The level of 3,4-dihydroxyphenyl acetic acid (DOPAC) is higher than expected in this sample. DOPAC is the major intermediary metabolite of dopamine. Research indicates that approximately one-third of newly synthesized dopamine is immediately processed to DOPAC, which is then secreted into the extracellular space between neurons. Evidence indicates that some sympathetic neurons may produce DOPAC, and that DOPAC may be synthesized in both the central and peripheral nervous systems.
Elevated DOPAC may occur with dopamine beta-hydroxylase (DBH) deficiency, which results in failure to convert dopamine to norepinephrine, and leads to elevated plasma DOPAC levels. DPH requires copper and ascorbate (Vitamin C) as co-factors. Animal studies indicate that DOPAC levels will increase during acute stressors, but may decrease with prolonged or chronic stress. Increases in L-3,4dihydroxyphenylalanine (L-DOPA) and dopamine occur after feeding and they enter the bloodstream as either DOPAC or dopamine sulfate (animal studies). Administration of reserpine or similar compounds has been shown to increase plasma DOPAC levels in animals. Forskolin also increases plasma DOPAC levels in animals. Catachol-O-methyl transferase (COMT) enzyme deficiencies increase DOPAC.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 9
www.doctorsdata.com
3-Methoxytyramine (3-MT) LOW
Summary from report:
3-MT is formed by direct metabolism of dopamine by COMT. 3-MT may be low if dopamine is low. Lowlevels of 3-MT may affect attention, cognition and sleep. Inhibition of COMT (e.g. lead) and/or low-activitygenetic variations in COMT may be associated with low levels of 3-MT. S-adenosylhomocysteine (SAH) and oxidative stress may inhibit COMT and essential methylation in general. The Plasma Methylation Profilemight be considered (SAM:SAH). High activity of MAO may decrease 3-MT and increase DOPAC. MAOactivity may increase due to oxidative stress. Antioxidants (selenium, pycnogenol, curcumin, berberine), and Vitamin B12 may normalize MAO activity. Vitamins C, B2, B3, SAMe, magnesium, copper and iron arerequired for optimal dopamine metabolism.
Expanded information:
The level of 3-methoxytyramine (3-MT) is lower than expected in this sample. 3-MT is the primary extracellular metabolite of dopamine released from neurons. Dopamine is methylated by catechol-O-methyltransferase (COMT) to 3-MT. Experimental inhibition of COMT reduces levels of 3-MT. COMT activity requires S-adenosyl-L-methionine (SAM) and magnesium. As COMT is the rate-limiting enzyme, single nucleotide polymorphisms (SNPs) or mutations that affect COMT enzyme activity may affect levelsof 3-MT.
Metyrosine therapy which decreases the activity of tyrosine hydroxylase (TH) will decrease dopamine levels, which may reduce 3MT levels. TH activity may also be down-regulated by high levels of catecholamines, oxidative stress, nitrosative stress and thiolation (reactions with sulfur amino acids).
3-Methoxytyramine (3-MT) HIGHSummary from report:
3-MT may be increased if dopamine is high; rule out use of L-DOPA. 3-MT is formed by direct metabolismof dopamine by COMT. Very high levels of 3-MT may have stimulatory effects. 3-MT levels may increaseduring acute stress. Herbicides, such as paraquat, have been shown to increase 3-MT levels in animals.Consumption of foods rich in catecholamines (bananas, pineapple, walnuts) may acutely increaseurinary levels of 3-MT. Deficiency or inhibition of MAO may increase 3-MT levels. MAO may be inhibitedby cigarette smoke or medications such as monoamine oxidase inhibitors. Vitamins C, B2, B3, SAMe,magnesium, copper and iron are required for optimal dopamine metabolism. Note: Markedly elevated levels of 3-MT may be associated with dopamine-secreting pheochromocytomasand paragangliomas. In some paraganglioma cases, only 3-MT is elevated. Plasma levels should always beused to confirm results if catecholamine-producing tumors are suspected.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 10
www.doctorsdata.com
Expanded information:
The level of 3-methoxytyramine (3-MT) is higher than expected in this sample. 3-MT is the primaryextracelluar metabolite of dopamine. Dopamine is methylated by catechol-O-methyltransferase (COMT) to make 3-MT. 3-MT is metabolized by monoamine oxidase and aldehyde dehydrogenase. If dopamine levels are also elevated, symptoms of anxiety or hyperactivity may be present. In mice increased levels of 3-MT have been shown to induce behavioral changes, and the changes were associated with 3-MT binding to the trace amine associated receptor 1 (TAAR1). However, this has not been confirmed in human studies. Experimental effects of increasing 3-MT include tremor, repetitive behaviors, hyperactivity and/or hypoactivity (animal studies).
3-Methoxytyramine levels may increase during acute stressors (animal studies). Inhibition of monoamine oxidase (MAO) may elevate both 3-MT and normetanephrine levels. Herbicides have been shown to elevate levels in animal studies. Elevations of 3-MT have also been associated with paraganglioma, pheochromocytoma, brain and carcinoid tumors.
Norepinephrine LOW
Summary from report:
Low norepinephrine may be associated with depression and mood changes as well as fatigue, difficultyconcentrating, decreased ability to stay focused on tasks and diminished sense of personal/professional drive. Norepinephrine is converted from dopamine requiring vitamin C, copper and B3, and L-tyrosine is an amino acid precursor. L-theanine and Mucuna pruriens may modulate norepinephrine effects.
Expanded information:
The level of norepinephrine is lower than expected in this sample. Norepinephrine is a catecholamine hormone and neurotransmitter secreted by the adrenal gland. It is the principal neurotransmitter in sympathetic nerve endings. Norepinephrine may help regulate vigilant attention, cognition and sleep. Studies indicate that the brain contributes at most 20% of circulating norepinephrine levels.
Low levels of norepinephrine may be associated with conditions such as orthostatic hypotension, dopamine beta-hydroxylase (DBH) enzyme deficiency and Menke’s disease. Alpha-2 agonistic pharmaceuticals decrease sympathetic nerve outflow and norepinephrine levels. Metyrosine therapy may decrease norepinephrine levels. Surgical sympathectomy or medical conditions that disrupt autonomic nerve functions may also decrease norepinephrine levels. Low levels of precursor amino acids phenylalanine or tyrosine, or low levels of the precursor neurotransmitter dopamine may result in low norepinephrine levels.
The synthesis of norepinephrine from dopamine requires Vitamin C and copper. About half of all norepinephrine is produced in the gastrointestinal tract, pancreas and spleen. Most of the norepinephrine produced by these mesenteric organs is removed from portal vein blood by the liver and converted to vanillylmandelic acid (VMA) for excretion.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 11
www.doctorsdata.com
Norepinephrine HIGH
Summary from report:
Elevated norepinephrine may be associated with stress response / sympathetic stimulation and contributory to anxiety, agitation, irritability, insomnia and lack of mental focus. Metabolism of norepinephrine requires vitamins B2, B3, SAMe, magnesium and iron, while conversion to epinephrine requires adequate cortisol and SAMe. L-theanine may modulate catecholamine effects. Some antidepressant medications may influence norepinephrine levels.
Expanded information:
The level of norepinephrine is higher than expected in this sample. Norepinephrine is a catecholamine hormone and neurotransmitter secreted by the adrenal gland. It is the principal neurotransmitter in sympathetic nerve endings. Norepinephrine may help regulate attention, cognition and sleep. Studies indicate that the brain contributes at most 20% to circulating norepinephrine levels.
Elevated levels of urinary norepinephrine and cortisol have been associated with anxiety. Profuse sweating and heat intolerance may occur with elevated norepinephrine levels. Elevated norepinephrine may result in nausea or vomiting. Elevations in norepinephrine levels may be seen in patients with depression, and with depressive symptoms in patients with cardiac disease. Impaired norepinephrine re-uptake has also been associated with heart palpitations, Congestive Heart Failure and Postural Tachycardia Syndrome. Mutations in the norepinephrine transporter (NET) may alter function and increase norepinephrine levels. Patients with NET mutations have excessive increases in heart rate and plasma concentrations of norepinephrine when standing.
Phenylethanolamine N-methyltransferase (PNMT) enzyme insufficiency may elevate norepinephrine and decrease epinephrine levels. Beta-adrenoceptor agonists increase norepinephrine release into plasma. Serious illness, physical activity or stress may temporarily increase catecholamine levels.
Norepinephrine is metabolized by monoamine oxidase (MAO) and catechol-O-methyltransferase. If MAO is inhibited by medication or enzyme function is compromised, dietary tyramine is able to reach the sympathetic nerve terminals, and paroxysmal hypertension may result from norepinephrine release. Resulting elevations in blood pressure may result in throbbing headaches.
Normetanephrine LOW
Summary from report:
Normetanephrine may simply be low if precursor norepinephrine is low. Alternatively, normetanephrinemay be low due to compromised COMT activity. Vitamins B2, B3, SAMe, magnesium and iron supportthe COMT enzyme; normal methylation by methyl donor SAM is required for COMT activity. The PlasmaMethylation Profile might be considered to evaluate the methylation index (SAM:SAH). Medications that may lower norepinephrine and normetanephrine include antihypertensives, serotonin reuptake inhibitors, and lithium carbonate.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 12
www.doctorsdata.com
Expanded information:
Normetanephrine is lower than expected in this sample. Normetanephrine is the 3-methoxy metabolite of norepinephrine. Clinically, normetanephrine provides an index of norepinephrine released due to sympathetic nerve activity. Between 25-40% of circulating normetanephrine is derived from catecholamine metabolism in the adrenal medulla.
Normetanephrine inhibits low affinity, high capacity biogenic amine transporters such as the plasma membrane monoamine transporter (PMAT), which is highly expressed in the brain. PMAT function has been associated with monoamine-related neuropsychiatric disorders, including attention deficit hyperactivity disorder (ADHD), depression, anxiety, addiction, narcolepsy, fatigue, obesity, eating disorder, other mood disorders, schizophrenia, bipolar disorder and Parkinson’s disease. Research continues to define these associations.
Low norepinephrine levels are typically associated with low normetanephrine levels. Acquired or inherited deficiencies in catechol-O-methyl transferase (COMT) may result in low normetanephrine levels. COMT function requires S-adenosyl-L-methionine (SAM) and magnesium. Inherited conditions such as dopamine beta-hydroxylase (DBH) deficiency and Menkes disease may also decrease norepinephrine and normetanephrine levels. Enzyme function may also be affected by single nucleotide polymorphisms (SNPs). Metyrosine therapy may decrease normetanephrine levels.
Plasma concentrations of total normetanephrine (free plus conjugated metanephrine) largely reflect conjugated gastrointestinal metanephrine). Total urinary normetanephrine is more clinically relevant and is reported by Doctor’s Data.
Normetanephrine HIGH
Summary from report:
Normetanephrine is the primary metabolite of norepinephrine; levels may be high if norepinephrine isalso high. High urinary normetanephrine levels may be associated with obstructive sleep apnea. If themetabolism of norepinephrine by MAO is suppressed, or the conversion of norepinephrine to epinephrineis impaired, consider insufficient cortisol. In that case more norepinephrine may be metabolized by COMT, increasing normetanephrine levels. Vitamins B2, B3, SAMe, magnesium and iron are required for optimal norepinephrine metabolism. Note: Markedly elevated normetanephrine levels may be associated with additional pathology (i.e. pheochromocytoma). Further workup is a consideration, depending on the clinical presentation and other relevant laboratory results.
Expanded information:
Normetanephrine is higher than expected in this sample. Normetanephrine is the 3-methoxy metabolite of norepinephrine. Clinically, normetanephrine provides an index of norepinephrine released due to sympathetic nerve activity. The metabolites are usually present in the urine in small fluctuating amounts and may be increased during and shortly after stress exposures. Between 25-40% of circulating

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 13
www.doctorsdata.com
normetanephrine is derived from catecholamine metabolism in the adrenal medulla.
Elevated normetanephrine and metanephrine has been associated with sleep apnea in hypertensive men.Epinephrine and metanephrine may be elevated by:
• Drugs that stimulate nicotinic, angiotensin II, or glucagon receptors• Anesthetics such as cocaine, lidocaine or halothane• Stressors posing global metabolic threats, such as acute glucose deprivation, emotional distress, and
hemorrhagic hypotension• Withdrawal from substances of abuse
Elevated levels of normetanephrine may occur if sulfotransferase (SULT) or PhenylethanolamineN-methyltransferase (PNMT) enzymatic activity is insufficient. Pheochromocytomas and other neural crest tumors may secrete catecholamines, metanephrine and normetanephrine. Urine tests may not always detect an intermittently secreting tumor, and urine tests are considered confirmatory for plasma results.
Plasma concentrations of total normetanephrine (free plus conjugated metanephrine) largely reflect conjugated gastrointestinal metanephrine). Total urinary normetanephrine is more clinically relevant and is reported by Doctor’s Data.
Epinephrine LOW
Summary from report:
Low epinephrine may be associated with depression and mood changes as well as fatigue, difficulty concentrating, decreased ability to stay focused on tasks and diminished sense of personal/professional drive. Conversion of epinephrine from norepinephrine requires SAMe and adequate cortisol., L-tyrosine is an amino acid precursor. L-theanine and Mucuna pruriens may influence epinephrine signaling.
Expanded information and references:
The level of epinephrine is lower than expected in this sample. Epinephrine is a catecholamine neurotransmitter and hormone synthesized in the adrenal medulla; small amounts are synthesized in the Central Nervous System (CNS) and the vagus nerve. Evidence indicates that epinephrine has neurotransmitter-like functions in the CNS that may affect the regulation of blood pressure, respiration, and pituitary hormone secretion.
Conditions that may be associated with low epinephrine levels include Addison’s disease, diabetic nephropathy, congenital 21- hydroxylase deficiency and autonomic failure syndromes. Drugs that can decrease catecholamine levels include clonidine, disulfiram, guanethidine, monoamine oxidase inhibitors (MAOIs), salicylates and Metyrosine therapy. Low levels of precursor norepinephrine may result in low epinephrine levels.
Phenylethanolamine N-methyltransferase (PNMT) methylates norepinephrine to form epinephrine, using S-adenosyl-L-methionine (SAM) as the methyl donor. Individual production and response to epinephrine levels may be influenced in part by genetic polymorphisms (SNPs) in the PNMT enzyme.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 14
www.doctorsdata.com
Epinephrine HIGH
Summary from report:
Elevated epinephrine may be associated with stress response and contributory to anxiety, agitation, irritability, insomnia and hypertension. Epinephrine levels may be elevated in patients in association with exercise prior to the urine collection. Metabolism of epinephrine requires vitamins B2, B3, SAMe, magnesium, and iron. L-theanine may modulate epinephrine effects.
Expanded information:
Levels of epinephrine are higher than expected in this sample. Epinephrine is a catecholamine neurotransmitter synthesized in the adrenal medulla; small amounts are synthesized in the Central Nervous System (CNS) and by the vagus nerve. Larger amounts of epinephrine may be secreted during acute stress (fight or flight response). Evidence indicates that epinephrine has neurotransmitter-like functions in the CNS that may affect the regulation of blood pressure, respiration, and pituitary hormone secretion.
Epinephrine elevations have been documented in strenuous exercise, panic attacks and some cases of essential hypertension. Postural tachycardia syndrome (POTS) patients may have elevated plasma epinephrine at rest. Drugs that stimulate nicotinic, angiotensin II, or glucagon receptors also increase plasma epinephrine levels. Serious illness and stress may cause moderate to large temporary increases in catecholamine levels.
Phenylethanolamine N-methyltransferase (PNMT) methylates norepinephrine to form epinephrine, using S-adenosyl-L-methionine (SAM) as a cofactor. PNMT expression may be up-regulated by exercise or glucocorticoid exposure. Catecholamine clearance from the blood may require several passes through the hepatic circulation. Epinephrine is primarily metabolized by the Phase II detoxification enzyme catechol-O-methyltransferase (COMT) in the liver, and lesser amounts may be metabolized by monoamine oxidase (MAO). COMT function requires SAM and magnesium. COMT function may also be affected by single nucleotide polymorphisms (SNPs).
Metanephrine LOW
Summary from report:
Metanephrine may simply be low if epinephrine is low because metanephrine is a direct metaboliteof epinephrine. Inhibition of the PNMT enzyme may decrease epinephrine and metanephrine levels,but increase norepinephrine. Vitamins B2, B3, SAMe, magnesium and iron support the COMT enzyme. Methylation is required for the formation of epinephrine (PNMT; phenylethanolamine N-methyltransferase).Further, methylation by COMT is required for conversion of epinephrine to metanephrine.Hypomethylation may be a causal factor for the pattern of low levels of epinephrine and metanephrineand disproportionate levels of norepinephrine. In such a case evaluation of the plasma methylation statusmay be directly addressed with the Plasma Methylation Profile.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 15
www.doctorsdata.com
Expanded information:
Metanephrine is lower than expected in this sample. Metanephrine is a metabolite of epinephrine. Clinically, metanephrine levels provide an indication of adrenal medulla metabolism of epinephrine prior to its release into circulation. The metabolites are usually present in the urine in low and fluctuating levels. Decreases in epinephrine levels will also decrease metanephrine levels. Pure autonomic failure syndromes decrease adrenomedullar function and may decrease epinephrine and metanephrine levels. Metyrosine therapy may lower both epinephrine and metanephrine levels. There is scant literature describing the symptoms of pure epinephrine and/or metanephrine insufficiency. However, conditions that may be associated with low epinephrine levels include Addison’s disease, diabetic nephropathy and autonomic failure syndromes.
Approximately 93% of circulating metanephrine is derived from catecholamine metabolism through the enzyme catechol-O methyl transferase (COMT) in the adrenal medulla. In the normal population, plasma normetanephrine levels are low. Acquired or inherited deficiencies in COMT may result in low metanephrine levels. COMT activity requires S-adenosyl-L-methionine (SAM) and magnesium, and may be suppressed by single nucleotide polymorphisms (SNPs). Phenylethanolamine N-methyltransferase (PNMT) deficiency or 21-dehydroxylase deficiency may decrease epinephrine and metanephrine levels.
Plasma concentrations of total metanephrine (free plus conjugated metanephrine) largely reflect conjugated gastrointestinal metanephrine). Total urinary metanephrine is more clinically relevant and is reported by Doctor’s Data.
Metanephrine HIGH
Summary from report:
Metanephrine is a primary metabolite of epinephrine formed by COMT activity. Elevated levels of epinephrine may increase metanephrine levels. Metanephrine may be elevated in anxiety disorders,bipolar disorders, hyperthyroidism and some autoimmune conditions. Individuals with obstructive sleepapnea have higher urinary metanephrine and normetanephrine levels. If MAO-A activity is inhibited, more epinephrine will be metabolized by COMT, increasing metanephrine levels. Vitamins B2, B3, SAMe, magnesium and iron are required for optimal epinephrine metabolism. Note: Markedly elevated levels of metanephrine may be associated with additional pathology (i.e. pheochromocytoma). Further workup is a consideration, depending on the clinical presentation and otherrelevant laboratory results.
Expanded information:
Metanephrine is higher than expected in this sample. Metanephrine is a metabolite of epinephrine. The metabolites are usually present in the urine in small fluctuating amounts and may be higher

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 16
www.doctorsdata.com
during and shortly after stressful experiences. Metanephrine may be elevated in a non-fasting patient. Approximately 93% of circulating Metanephrine is derived from catecholamine metabolism in the adrenal medulla.
Metanephrine may be elevated in anxiety or bipolar disorders. Physical conditions, including congestive heart failure, porphyria, hyperthyroid and some autoimmune conditions may present with elevated metanephrine. High levels of metanephrine and normetanephrine have been associated with sleep apnea in hypertensive men. Pheochromocytoma and other neural crest tumors may secrete catecholamines and their metabolites, including metanephrine, though urine tests may not always detect an intermittently secreting tumor. Epinephrine and Metanephrine may be elevated by pharmaceuticals:
• Drugs that stimulate nicotinic, angiotensin II, or glucagon receptors• Anesthetics such as cocaine, lidocaine or halothane• Monoamine oxidase (MAO) inhibitors• Stimulants, including caffeine• Withdrawal from substances of abuse
Metanephrine is metabolized by monoamine oxidase (MAO). MAO enzymatic activity may be affected by single nucleotide polymorphisms (SNPs). Metanephrine levels may elevate if sulfotransferase (SULT) enzymatic activity is insufficient.
Plasma concentrations of total metanephrine (free plus conjugated metanephrine) largely reflect conjugated gastrointestinal metanephrine). Total urinary metanephrine is more clinically relevant and is reported by Doctor’s Data.
N/E Ratio
Summary from report:
Elevated N/E ratio is consistent with poor conversion of norepinephrine to epinephrine. This conversion is driven by the phenylethanolamine N-methyltransferase (PNMT) enzyme that requires SAMe, magnesium and cortisol (adequate HPA axis function) as cofactors. Suggest interpretation in context of cortisol levels/HPA axis function, with subsequent optimization of HPA axis function when clinically warranted.
Expanded information:
Elevated N/E ratio may be consistent with poor conversion of norepinephrine to epinephrine. This conversion is driven by the phenylethanolamine N-methyltransferase (PNMT) enzyme that requires SAMe, magnesium and cortisol (adequate HPA axis function) as cofactors. Consider the actual levels of both neurotransmitters, and interpret in the ratio in context of cortisol levels/HPA axis function. Optimization of HPA axis function may be clinically warranted.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 17
www.doctorsdata.com
Tryptamine LOW
Summary from report:
Tryptamine is a trace amine derived directly from tryptophan by a B6-dependent enzyme. Decreasedtryptamine levels may be associated with depression. Low range levels of tryptamine may simply beassociated with insufficient intake/assimilation of the essential amino acid tryptophan. Low range levels of tryptamine, but high levels of tryptophan, may suggest a vitamin B6 deficiency. Tryptamine is metabolized by MAO; its activity may be increased by oxidative stress. Antioxidants (selenium, pycnogenol, curcumin, berberine), and Vitamin B12 may normalize MAO activity levels.
Expanded information:
The level of tryptamine is lower than expected in this sample. Tryptamine is derived from the essential amino acid tryptophan. Tryptamine levels may affect arterial resistance (vasoconstriction) and serotonin signaling.
Low tryptamine levels or deficient trace amine functions may be associated with some depressive disorders. Low plasma tryptamine levels have been associated with chronic migraine and chronic tension headaches. Tryptamine may act as a neuromodulater for serotonin signaling; serotonin affects mood, sleep and appetite. Urinary tryptamine levels seem to correlate with symptom severity in schizophrenia. Tryptamine levels may affect arterial resistance (vasoconstriction) and serotonin signaling. Methylated tryptamines may also play a role in the development of schizophrenia.
Aromatic L-amino acid decarboxylase (AADC) is the rate-limiting enzyme in the conversion of tryptophan to tryptamine. Altered AADC activity may affect trace amine levels without affecting the levels of monoamine neurotransmitters (catecholamines, histamine, serotonin, etc.). Reserpine decreases AADC activity and trace amine levels.
Tryptamine HIGH
Summary from report:
Tryptamine is a trace amine derived directly from tryptophan by a B6-dependent enzyme. Trace amines(tryptamine, tyramine, PEA) may have stimulant effects at high levels. Tryptophan supplementationmay increase tryptamine levels, especially when conversion of tryptophan to 5-HTP and serotonin iscompromised by nutrient insufficiencies (BH4, iron, B6, D). Such might be the case if tryptamine is high,but serotonin is low. Tryptamine is normally metabolized by MAO; low enzyme activity may increasetryptamine levels. Vitamin B2 may increase the expression of MAO enzymes.
Expanded information:
Tryptamine is higher than expected in this sample. Tryptamine is derived from the essential amino acid tryptophan. Tryptamine levels may affect artery resistance (vasoconstriction) and serotonin signaling.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 18
www.doctorsdata.com
Elevated levels of tryptamine have been associated with some forms of schizophrenia; urinary tryptamine levels seem to correlate with symptom severity. Methylated tryptamines may also play a role in the development of schizophrenia. Elevated methylated tryptamine levels may contribute to acute schizophrenia episodes. Methylated tryptamines, such as N,N- dimethyltryptamine (DMT), are produced within the body, and may have hallucinogenic effects when present at high levels. Methylated tryptamines are naturally occurring in plants and have been taken orally for psychedelic effects.
Trace amines may be generated in the gastrointestinal tract by protein-fermenting gut bacteria after a protein-rich meal. They may also be found in a variety of foods as the result of food spoilage or deliberate fermentation. Dietary trace amines are usually metabolized quickly by MAO enzymes. Elevated levels of trace amines may occur in association with phenylketonuria, ergot fungi exposure or the use of MAO inhibitors.
Aromatic L-amino acid decarboxylase (AADC) activity is the rate-limiting enzyme in conversion of tryptophan to tryptamine. Increased AADC activity increases trace amine levels without affecting levels of monoamine neurotransmitters (catecholamines, histamine, serotonin, etc.). Tryptamine is metabolized by monoamine oxidase (MAO) in glial cells and neurons.
Serotonin (5-hydroxytryptamine) LOW
Summary from report:
Low serotonin may contribute to mood concerns including anxiety, OCD, depression, anger and a sense of discontentment. Low serotonin may also be associated with poor sleep quality and appetite changes, as well as chronic fatigue, rheumatoid arthritis, and over-all lassitude. Failure to regenerate tetrahydrobiopterin [BH4], an essential cofactor for serotonin synthesis, may decrease serotonin levels, and could be reflected in urine. BH4 regeneration may be supported by folates, vitamin B3, C, molybdenum and zinc. Additionally, production of serotonin requires vitamin D, iron and vitamin B6. Tryptophan is the essential precursor of serotonin. 5-HTP may increase serotonin, and L-theanine may affect serotonin function.
Expanded information:
The level of serotonin in this sample is lower than expected. Serotonin signaling in the central nervous system (CNS) may influence mood, appetite, sleep, memory and learning, homeostasis, and sexual behaviors. There are a great many serotonin receptors with different affinities, expression and function. Decreased serotonin levels have been associated with obsessive-compulsive disorder (OCD), anger, insomnia, and depression. Some eating disorders and migraine headaches may also be related to low serotonin levels. Low urinary serotonin levels during pregnancy have been associated with increased risk of premature birth. In the peripheral nervous system, low levels of serotonin may affect gastrointestinal motility (constipation), and possibly bone mass. Low serotonin levels have been associated with irritable bowel syndrome. Cyprohepatadine is an anthistamine that decreases serotonin levels.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 19
www.doctorsdata.com
Studies indicate that serotonin depletion is more likely to affect mood in those with a family history of mood disorders. Mutations or single nucleotide polymorphisms (SNPs) in specific enzymes may affect serotonin synthesis or degradation. Several SNPs have been identified and linked to depression; research continues in this area.
Serotonin is unable to cross the blood-brain barrier and must be synthesized in the peripheral and central nervous system. Tetrahydrobiopterin, iron and Vitamin B6 are required cofactors for serotonin synthesis. The gastrointestinal (GI) tract produces about 80% of the body’s serotonin. During the “first pass” through hepatic circulation monoamine oxidase (MAO) metabolizes 30-80% of GI-derived serotonin to 5-hydroxyindoleacetic acid (5-HIAA). Serotonin may also be converted to 5-HIAA in the lungs. Urine and plasma levels of serotonin may vary with the intake of certain foods rich in serotonin, and medications that alter serotonin levels.
Serotonin HIGH
Summary from report:
Elevated serotonin may be associated with symptoms of, increased anxiety, agitation and diarrhea (IBS-like symptoms). Serotonin levels may be increased by low protein or high-carbohydrate meals, insulin, and tryptophan or 5-HTP supplementation. Many mood altering medications, including SSRIs and SNRIs, may influence serotonin levels. L-theanine may affect serotonin function. Note: Significantly elevated serotonin levels may be associated with additional pathology (i.e. carcinoid tumor). Suggest further work up depending on the clinical picture.
Expanded information:
The level of serotonin in this sample is higher than expected. Serotonin signaling in the central nervous system (CNS) may influence mood, appetite, sleep, memory and learning, homeostasis, and sexual behaviors. Altered levels of urinary or plasma serotonin are thought to play a role in many disorders including anxiety, depression, obsessive compulsive disorder and phobias. Elevated plasma serotonin and platelet serotonin levels are a common finding in autistic patients, and may contribute to psychiatric disorders such as schizophrenia. There are a great many serotonin receptors with different affinities, expression and function.
The main diseases that may be associated with elevated levels of serotonin are neuroectodermal tumors, in particular carcinoid tumors arising from gastrointestinal (GI) enterochromaffin cells. Only about 10% of mid-gut carcinoids produce enough serotonin to cause symptoms. Symptoms of serotonin excess (Serotonin Syndrome), are wide-ranging. A triad of symptoms including altered mental status (usually anxiety), neuromuscular hyperactivity or hyperreflexia, and autonomic instability, is suspicious for serotonin excess. Exogenous estrogens have been shown to raise both serotonin and 5-HIAA levels in post-menopausal women. Serotonin levels may be increased by exercise, increased daylight (or daylight equivalent) exposure, low-protein or high-carbohydrate meals, insulin, or by Tryptophan or 5-hydroxytryptophan

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 20
www.doctorsdata.com
(5-HTP) supplements. Some studies indicate that therapeutic massage may also elevate serotonin levels. The herbs St. John’s wort and ginseng may elevate serotonin levels.
Medications that may increase serotonin include:
• serotonin reuptake inhibitors (SSRIs)• monoamine oxidase inhibitors (MAOIs)• antidepressants: bupropion, trazodone• migraine medications• pain medications• lithium• dextromethorphan (cough suppressant)• anti-emetics
The gastrointestinal tract produces about 80% of the body’s serotonin. During the “first pass” through hepatic circulation, monoamine oxidase A (MAO-A) metabolizes 30-80% of GI serotonin to 5-hydroxyindoleacetic acid (5-HIAA). Serotonin metabolism requires selenium, magnesium and vitamin B3 as cofactors. Mutations, or single nucleotide polymorphisms (SNPs), in MAO-A may affect serotonin degradation. SNPS or mutations in serotonin receptors may affect responses to serotonin.
5-hydroxyindol acetic acid (5-HIAA) LOW
Summary from report:
Low 5-HIAA may be associated with mood concerns including depression and anxiety, sleep changes,and poor concentration. Low 5-HIAA may be associated with low precursor serotonin, or compromisedmetabolism of serotonin by MAO-A. Some medications, including aspirin, MAO-inhibitors, levodopa, andtricyclic antidepressants may decrease 5-HIAA levels. MAO may be inhibited by cigarette smoke. VitaminsB2, B3, B6, magnesium and iron are required for optimal serotonin metabolism. If MAO-A enzyme functionis inhibited, serotonin may be elevated and 5-HIAA will be low.
Expanded information:
The level of 5-hydroxyindoleacetic acid (5-HIAA) is lower than expected in this sample. Clinically, urinary 5-HIAA is an indicator of serotonin synthesis and metabolism. Serotonin is metabolized by monoamine oxidase A (MAOA) into 5-HIAA; about 1% of the tryptophan metabolized in the body is converted to 5-HIAA.
Studies have demonstrated an association between low serotonin or 5-HIAA levels and aggression; most of these studies have focused on males. Low 5-HIAA levels (cerebrospinal fluid) may be associated with depression and advanced Parkinson’s disease. Mutations or single nucleotide polymorphisms (SNPs) in specific enzymes may affect serotonin synthesis. Low levels of the precursor amino acid L-tryptophan may decrease serotonin and 5-HIAA levels.
Serotonin does not cross the blood-brain barrier and must be synthesized in the peripheral and central nervous systems. Tetrahydrobiopterin, iron and vitamin B6 are required cofactors for serotonin synthesis.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 21
www.doctorsdata.com
The gastrointestinal tract produces about 80% of the body’s serotonin. During the “first pass” through hepatic circulation, MAO-A in the liver metabolizes 30-80% of GI serotonin to 5-hydroxyindoleacetic acid (5-HIAA). Serotonin may also be converted to 5-HIAA in the lungs. Medications that may decrease 5-HIAA include aspirin, ethyl alcohol, imipramine, levodopa, MAO inhibitors, heparin, isoniazid, methyldopa, and tricyclic antidepressants.
5-hydroxyindol acetic acid (5-HIAA) HIGH
Summary from report:
Clinically the urine levels 5-HIAA provide an indicator of serotonin synthesis, and serotonin metabolismby MAO-A. Elevated levels of 5-HIAA may simply be associated with high serotonin; consider if patientsupplements with tryptophan and/or 5-HTP. Some medications as well as dietary consumption of foodsrich in serotonin (plantain, pineapple, banana, kiwi fruit, plums, tomatoes, walnuts and hickory nuts) mayelevate levels of 5-HIAA. It is recommended to avoid these foods for 3 days prior to sample collection.Excessive 5-HIAA has been found in some patients with celiac disease, metabolic syndrome, andchronic renal insufficiency. MAO-A activity may increase due to oxidative stress. Antioxidants (selenium,pycnogenol, curcumin, berberine), and Vitamin B12 may help normalize MAO activity.
Note: Markedly elevated 5-HIAA coupled with significantly elevated serotonin may be associated with additional pathology (i.e. carcinoid tumor). Further workup is a consideration, depending on the clinicalpresentation and other relevant laboratory test results.
Expanded information:
The level of 5-hydroxyindoleacetic acid (5-HIAA) is higher than expected in this sample. Serotonin is metabolized by monoamine oxidase A (MAOA) to 5-HIAA; about 1% of the tryptophan metabolized in the body is converted into 5-HIAA. The gastrointestinal tract produces about 80% of the body’s serotonin. During the “first pass” through hepatic circulation, MAO-A in the liver metabolizes 30-80% of GI serotonin to 5-hydroxyindoleacetic acid (5-HIAA). Serotonin may also be converted to 5-HIAA in the lungs. Serotonin metabolism requires selenium, magnesium and vitamin B3.
Non-fasted samples may have elevated levels of 5-HIAA. Elevated 5-HIAA has been associated with Celiac disease and chronic renal insufficiency. Carcinoid tumors arising from gastrointestinal enterochromaffin cells may be associated with measurable increases in serotonin and 5-HIAA.
Exogenous estrogens have been shown to elevate both serotonin and 5-HIAA levels in post-menopausal women. Tryptophan or 5-hydroxytryptophan (5-HTP) supplements may elevate 5-HIAA levels. Foods known to elevate serotonin may confound interpretation of results for 5-HIAA and, should be avoided prior to sample collection. Diagnosis of carcinoid tumor requires evaluation of multiple biomarkers in

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 22
www.doctorsdata.com
plasma and urine. The herbs St John’s wort and ginseng may elevate serotonin levels. Medications that may increase serotonin include:
• serotonin reuptake inhibitors (SSRIs)• monoamine oxidase inhibitors (MAOIs)• antidepressants: bupropion, trazodone• migraine medications• pain medications
The use of these medications may occasionally result in serotonin excess. Symptoms of serotonin excess (Serotonin Syndrome), are wide-ranging. A triad of symptoms including altered mental status (usually anxiety), neuromuscular hyperactivity or hyperreflexia, and autonomic instability, raises suspicious for serotonin excess.
Serotonin levels may be increased by exercise, increased daylight (or daylight equivalent) exposure, low-protein or high-carbohydrate meals, insulin or caffeine. Some studies indicate that therapeutic massage may also elevate serotonin levels.
Glutamate LOW
Summary from report:
Low glutamate may be associated with depression, increased addictive tendencies including food seeking behaviors, and can contribute to mental fatigue and diminished mental stimulation. L-glutamine is a precursor amino acid.
Expanded information:
The level of glutamate is lower than expected in this sample. Glutamate is a non-essential amino acid that acts as an excitatory neurotransmitter for metabolic signaling pathways. Glutamate signaling affects neuron maturation, plasticity and higher cognitive functions.
Decreased Glutamate signaling may contribute to apoptosis (death) of immature neurons. Reduced glutamate signaling has also been associated with elevations in dopamine which may contribute to symptoms of schizophrenia. Glutamate signaling may occur through a variety of Glutamate receptors. N-methyl-D-aspartate (NMDA) receptor signals are the most complex, as the receptor requires both glutamate and glycine to function. Research continues into associations between glutamate signaling and cognitive disorders.
In the central nervous system (CNS), glutamate is recognized as the primary excitatory neurotransmitter and the glutamate signaling system is involved in fast synaptic transmission between neurons. The blood-brain barrier prevents the passage of glutamate. Astroglial cells are the primary source of glutamate in the CNS. Enteric glial cells may be important in glutamate signaling within the gut as neurotransmitter receptors and glial cells respond to dietary L-glutamate and monosodium glutamate (MSG).

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 23
www.doctorsdata.com
Glutamate HIGH
Summary from report:
Elevated glutamate may contribute to anxiety, poor concentration, attention deficits and hyperactive tendencies as well as poor sleep and nighttime awakening. Glutamate may be increased in association with hypoglycemia, Alzheimer’s, ALS and chronic compromised blood flow to the brain. Possible sources of increased glutamate include MSG, yeast extract and other hidden sources of free glutamic acid. L-theaninemay modulate elevated glutamate levels and attenuate glutamate signaling, and taurine may provide protection from excitotoxicity and neuroinflammation.
Expanded information:
Glutamate is a non-essential amino acid that acts as an excitatory neurotransmitter for metabolic signaling pathways. Glutamate signaling affects neuronal maturation, plasticity and higher cognitive functions. Excess glutamate signaling, and its effects, has been termed “excitotoxicity” and is considered a contributing factor in the neurodegeneration seen in Huntington’s disease, Alzheimer’s disease, amyotrophic lateral sclerosis (ALS), multiple sclerosis, stroke and fibromyalgia. Animal studies indicate that acute stressors may cause transient elevations in extracellular glutamate. Glutamate signaling may occur through a variety of glutamate receptors. N-methyl-D-aspartate (NMDA) receptor signals are the most complex, requiring both glutamate and glycine to function.
The blood-brain barrier prevents the passage of glutamate. Astroglial cells are the primary source of glutamate in the CNS. Any glutamate released into the synapse is cleared by excitatory amino acid transporters (EAAT) found on the astroglia. EEATs, unless damaged or defective, keep extracellular glutamate levels low and insufficient for glutamate receptor signaling. EAAT functions are inhibited by oxidative stress. Extracellular glutamate may alter activity by binding with extra-synaptic high affinity glutamate receptors. Extracellular glutamate levels may also accumulate due to defects in the glutamate-glutamine cycle which removes ammonia from the CNS.
Enteric glial cells in the gastrointestinal tract may be important in glutamate signaling within the gut as neurotransmitter receptors and glial cells respond to dietary L-glutamate and monosodium glutamate (MSG). Gastrointestinal microbes may also affect glutamate levels.
Gamma Aminobutyric Acid (GABA) LOW
Summary from report:
Low GABA may be associated with anxiety, poor impulse control, major depression, pain, and decreasedsleep quality. Low GABA may be seen in individuals deficient in vitamin B6. L-theanine, GABA, andglutamine may positively affect functional GABA activity, and phenibut exerts GABA-like effects(experimental models).

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 24
www.doctorsdata.com
Expanded information:
The level of Gamma-aminobutyric acid (GABA) is lower than expected in this sample. GABA functions as an inhibitory neurotransmitter in the central nervous system (CNS). GABA acts in opposition to glutamate, the primary excitatory neurotransmitter.
Studies demonstrate decreased GABA levels in animal models of depression, and clinical studies report low plasma and cerebrospinal fluid GABA in patients with mood disorder. GABA deficiency may also play a role in psychiatric disorders such as anxiety, depression, pain, panic, or mania. GABA deficiency has also been associated with neurological disorders such as Huntington’s chorea, Parkinson’s and Alzheimer’s disease. GABA deficiency has not been directly associated with epilepsy, but disorders of GABA receptors have. Altered GABA signaling has been associated with neurodevelopmental disorders such as autism, Fragile X, Down’s syndrome, schizophrenia, Tourette’s syndrome and neurofibromatosis. Low plasma GABA levels have also been associated with premenstrual dysphoric disorder.
GABA synthesis requires a pyridoxal-5’-phosphate (vitamin B6). Single nucleotide polymorphisms (SNPs) or mutations in GABA synthesis or transport may affect GABA levels. Mutations or SNPs in GABA receptors may exacerbate the effects of low GABA levels.
Peripherally, GABA regulates gastrointestinal motility, intestinal secretion and electrolyte transport via the enteric nervous system. In vitro studies indicate that GABA may inhibit nitric oxide synthesis in gut neurons. The gastrointestinal (GI) microbiome may affect levels of glutamate and GABA as some GI bacteria are known to synthesize GABA and other neuro-active molecules.
Gamma Aminobutyric Acid (GABA) HIGH
Summary from report:
Elevated GABA may contribute to difficulty concentrating, diminished memory, dampened mood and decreased cognitive processing as well as fatigue, decreased exercise endurance, sleepiness and aninability to feel alert. Elevated GABA levels may be compensatory in the presence of elevated excitatoryneurotransmitters, and may result with gabapentin use. L-theanine may modulate the effects of elevatedGABA levels. Elevated GABA levels may be associated with bacterial overgrowth (i.e. urinary tract infectionor gastrointestinal dysbiosis).
Expanded information:
The level of Gamma-aminobutyric acid (GABA) is higher than expected in this sample. GABA functions as an inhibitory neurotransmitter in the central nervous system (CNS). GABA acts in opposition to glutamate, the primary excitatory neurotransmitter. Elevated GABA levels may have sedative, hypnotic or muscle-relaxing effects, depending on which GABA receptors are stimulated.
GABA may be elevated during bacterial urinary tract infections and, occasionally due to gastrointestinal infections (dysbiosis). GABA may be produced or metabolized by gastrointestinal bacteria (Lactobacilli and Bifdobacteria).

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 25
www.doctorsdata.com
Elevated plasma levels of GABA have been associated with symptom severity in autistic patients. Recently, infection with the parasite Toxoplasma gondii has been associated with elevated extracellular GABA levels; such infections are known to decrease fear responses and reaction times in animals and humans. Urinary GABA levels may be elevated due to malignancies of the ovary. GABA-transaminase deficiency, succinic semialdehyde dehydrogenase (SSADH) deficiency and homocarnosinosis are rare genetic disorders of GABA metabolism that may elevate GABA levels; all present early in life with a variety of neurological symptoms. These disorders usually require cerebro-spinal fluid sampling for diagnosis. GABA supplementation may also elevate urinary GABA levels. GABA may be elevated due to vitamin B-6 deficiency.
Single nucleotide polymorphisms (SNPs) or mutations in GABA transport or metabolism may also affect GABA levels. Mutations or SNPs in GABA receptors may further alter responses to GABA levels.
Glycine LOW
Summary from report:
Low levels of glycine may contribute to REM Sleep Behavior Disorder, and sleep disorders in general can be associated with poor cognitive function and memory. Low levels of glycine may also contribute to symptoms in some patients with schizophrenia. Vitamin B6, L-theanine and glycine may improve symptoms in some individuals. The primary reason for low levels of glycine is low activity of serine hydroxy methyltransferase (SHMT) that requires B6 and magnesium as cofactors.
Expanded information:
The level of glycine is lower than expected in this sample. Glycine is a non-essential amino acid that acts as a neurotransmitter in the central nervous system (CNS). Glycine is inhibitory when bound to glycine receptors in the spinal cord, brain or retina, and is considered inhibitory in the CNS. The presence of glycine transporters on glial cells suggests that glycine may also have neuromodulatory effects. Low levels of glycine may to contribute to impaired sleep and mental function.
Low glycine levels may contribute to symptoms in some subsets of patients with obsessive-compulsive disorder or schizophrenia. Genetic variation in the glycine receptor may contribute to seizure disorders, and genetic variation in the N-methyl-D-aspartate (NDMA) receptor may affect neuron excitability and plasticity. Mutations of glycine receptor subunits have been associated with hereditary hyperekplexia (startle disease). Glycine is an essential ligand with glutamate for NDMA receptor excitatory signaling.
Glycine synthesis in the cell cytoplasm requires B6. Glycine is a required precursor for glutathione (GSH) synthesis. The GSH tripeptide is not transported across the blood brain barrier and must be synthesized in nerve cells. Low levels of GSH may result in oxidative stress in neurons. Low urinary glycine may occur due to impaired renal clearance or toxicant exposure.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 26
www.doctorsdata.com
Glycine HIGH
Summary from report:
Glycine is a non-essential amino acid that acts as an inhibitory neurotransmitter in the central nervous system. Elevated glycine levels may be associated with compromised cognitive processing. Elevated levels may be seen with glycine supplementation. Glycine may be given in conjunction with pharmaceutical agents when supporting schizophrenia or psychosis. Lipoic acid may enhance glycine break down. Break down of glycine requires vitamin B6 and tetrahydrofolate as cofactors. Note: High levels of glycine may interact with clozapine and decrease its clinical efficacy.
Expanded information:
The level of glycine is higher than expected in this sample. Glycine is a non-essential amino acid that acts as a neurotransmitter in the central nervous system (CNS). Glycine is inhibitory when bound to glycine receptors in the spinal cord, brain or retina, and is considered inhibitory in the CNS. The presence of glycine transporters on glial cells suggests that glycine may also have neuromodulatory effects. Glycine is an essential ligand with glutamate for N-methyl-D-aspartate (NDMA) receptor excitatory signaling.
Animal studies indicate that elevated glycine levels may severely impair energy use in the CNS. Genetic defects may result in glycine encephalopathy. Elevated levels of glycine in the CNS may result in intellectual disability, poor muscle tone, chorea, and respiratory or feeding difficulties (infants). This condition is characterized by non-ketotic hyperglycinemia (NHK) and elevated urinary glycine. Most cases are diagnosed during infancy, although occasionally a patient will have a milder, atypical form of NHK with onset from late infancy to adulthood. Genetic variation in the glycine receptor may contribute to seizure disorders, and may also affect neuronal excitability and plasticity.
Mutations of glycine receptor subunits have been associated with hereditary hyperekplexia (startle disease). Glycine supplements may be used in conjunction with pharmaceutical supports for schizophrenia or psychosis, and may result in elevated urinary glycine.
The glycine cleavage complex (GCC) metabolizes glycine and is comprised of four different proteins. GCC requires vitamin B6 and tetrahydrofolate as cofactors. Alternately, glycine may be converted to serine by serine hydroxymethyltransferase, which also requires vitamin B6. High levels of glycine may interact with clozapine and decrease the drug’s effect.
Histamine LOW
Summary from report:
Low histamine may affect digestion and appetite control, learning, memory, and mood, and may result in drowsiness. Histamine has been noted to modulate neurotransmitter release from neurons. Histamine levels may be supported by consumption of high-protein foods and whole grains, as well as L-histidine supplementation. Vitamin B6 is a cofactor for histamine synthesis.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 27
www.doctorsdata.com
Expanded information:
The level of histamine in this sample is lower than expected. Histamine is one of the most important neurotransmitters to stimulate and maintain arousal in the central nervous system (CNS). Histamine-aceytlcholine signal interactions influence wakefulness (arousal), circadian rhythms, appetite control, learning, memory and emotion.
The essential amino acid histidine is converted to histamine. Histamine synthesis may be influenced by oxidative stress, glucocorticoids and gastrin. Vitamin B-6 deficiency may impair histamine synthesis. Two rare genetic disorders, histidine ammonia-lyase deficiency or histidine decarboxylase deficiency, may prevent the conversion of histidine to histamine. Sedatives such as ethanol, tetrahydrocannabinol , barbiturates and benzodiazepines may also decrease histamine levels.
Alterations in CNS histamine levels may contribute to age-related neurodegenerative diseases such as Parkinson’s disease and Alzheimer’s disease. Low levels of histamine in the CNS may also contribute to Tourette’s syndrome, narcolepsy and other hypersomnia disorders. Histamine levels in the CNS may be reduced by nicotinic and serotonergic signaling.
Histamine HIGH
Summary from report:
Elevated histamine may be associated with allergy-like symptoms, gastro-intestinal concerns, skin itch/inflammation (pruritis), increased wakefulness and insomnia, and has been demonstrated in gastrointestinal blastocystis infections. Levels may be elevated due to use of histamine-releasing medications, consumption of allergenic and sulfite-rich foods and/or histamine-rich foods, dysbiotic bacterial production in the intestine and zinc deficiency. High urine (and blood) histamine levels have been associated with cluster and cyclic headaches. Break down of histamine requires SAMe and copper.
Expanded information:
The level of histamine is higher than expected in this sample. Histamine is one of the most important neurotransmitters to stimulate and maintain arousal in the central nervous system (CNS). Histamine-aceytlcholine signal interactions influence wakefulness (arousal), circadian rhythms, appetite control, learning, memory and emotion. The essential amino acid histidine is converted to histamine.Alterations in histamine levels in the CNS may contribute to age-related neurodegenerative diseases such as Parkinson’s disease and Alzheimer’s disease. Increased populations of CNS mast cells and increased histamine levels have been associated with Multiple Sclerosis, and increased levels of histamine metabolites have been found in the cerebrospinal fluid of schizophrenic patients. Approximately one percent of the population is histamine intolerant due to reduced diamine oxidase (DAO) activity. Elevated plasma histamine and DAO deficiency have been associated with inflammatory bowel disease (IBD), allergic enteropathy, colorectal cancers, and food allergy. Patients with allergies or mastocytosis may have higher plasma histamine levels. Certain bacteria in the gastrointestinal microbiome may synthesize histamine, and some patients with gastric carcinoids may have elevated histamine levels. Animal studies indicate that morphine, clozapine, olanzapine, methylphenidate, atomoxetine and other pharmaceuticals may increase histamine release and turnover in the CNS.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 28
www.doctorsdata.com
Histamine is a mediator of allergic Type I hypersensitivity reactions. Histamine released during allergic reactions may result in itching, flushing, hives, vomiting, syncope, anaphylaxis or shock.
Taurine (2-aminoethane- sulfonic acid) LOW
Summary from report:
Taurine is an essential amino acid that may have an inhibitory effect on the firing rate of neurons in the CNS. Decreased CNS taurine synthesis has been reported in individuals with autoimmune and neurodegenerative diseases, including rheumatoid arthritis, Parkinson’s disease, Alzheimer’s disease, and motor neuron diseases such as amyotrophic lateral sclerosis (ALS). Cells with low taurine levels may not retain magnesium or other minerals. Naïve vegetarians or individuals with digestion or malabsorption disorders may have low range taurine levels. Taurine does not cross the blood brain barrier (BBB) easily and must be synthesized within the CNS, which requires a functional methylation pathway. Taurine synthesis requires cysteine, vitamin B6, iron, and molybdenum.
Expanded information:
The level of taurine in this patient is lower than expected. Taurine acts as a neuromodulator and exerts an inhibitory effect on the firing rate of neurons in the central nervous system (CNS)in vitro . Taurine has been shown in human and animal studies to have mild anti-convulsion effects. Taurine promotes neural development in both the embryonic brain and the adult brain.
Decreased taurine synthesis has been reported in individuals with autoimmune and neurodegenerative diseases, including rheumatoid arthritis, Parkinson’s disease, Alzheimer’s disease, and motor neuron disease. Low taurine levels may contribute to heart muscle disease (cardiomyopathy), kidney disease, pancreatic beta cell malfunction, and the loss of retinal photoreceptors. Taurine in nerve cells inhibits glutamate-induced calcium influx and protects against glutamate-induced exicitotoxicity. Taurine supplements have been used to treat seizure disorders, autism and attention deficit-hyperactivity disorder (ADHD).
Taurine levels may be low due to dietary insufficiency or enzyme deficiencies. Taurine synthesis requires B6 and the precursor amino acid cysteine. Taurine synthesis may be important in the CNS. Taurine is excreted via urine and bile. The amount of taurine excreted daily is affected by various factors including genetics, age, gender, diet, renal function and medical conditions. A low urinary taurine due to a renal clearance disorder may occasionally mask an elevated plasma taurine level.
Taurine (2-aminoethane- sulfonic acid) HIGH
Summary from report:
Taurine is an essential amino acid that may have inhibitory effects on CNS neurons. High urinary levels of taurine may be associated with stress reactions, depression, autism and psychosis. Symptoms may include apathy, sleep changes, irritability, recklessness, poor concentration, aches and pains, or social withdrawal. Patients with Cushing’s syndrome (high cortisol) may have elevated urinary taurine levels. Urinary taurine levels may be high with acute or chronic kidney damage, inherited kidney disorders, liver inflammation,

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 29
www.doctorsdata.com
or gastrointestinal dysbiotic bacterial or yeast over growth. Oral supplementation may raise taurine levels; taurine is an ingredient in many “energy drinks”. High taurine levels may compete with glycine N-methyl-D-aspartate receptors (NMDR). Chronically high taurine excretion may deplete intracellular magnesium and calcium.
Expanded information:
The level of taurine in this sample is higher than expected. Taurine acts as a neuromodulator and exerts, in vitro, an inhibitory effect on the firing rate of neurons in the central nervous system (CNS). Taurine has been shown in human and animal studies to have mild anti-convulsive effects. Taurine promotes neural development in both the embryonic brain and the adult brain.
High plasma taurine may be associated with stress reactions, depression and psychosis. Patients with Cushing’s disease may have elevated urinary taurine levels, but low plasma levels. Patients with autism may have elevated urine taurine, glycine and alanine with low glutamate. Elevated urinary taurine levels may result from inherited renal defects, liver disease, heart disease or radiation injury. Gastrointestinal dybiosis with associated excess beta-alanine can cause taurine wasting in the urine (high). Oral supplementation may raise urinary taurine levels. Taurine is an ingredient in many“energy drinks” and taurine supplements are used by some athletes. Taurine is excreted via urine and bile. A renal wasting condition may result in elevated urine taurine with a low plasma taurine level. The amount of taurine excreted daily is affected by various factors including genetics, age, gender, diet, renal function and medical conditions.
Creatinine
Expanded information:
The urinary creatinine concentration (CC) presented in this report represents the actual creatinine concentration in the specimen that was submitted. Under normal conditions, the rate of excretion of creatinine is quite constant and highly correlated with lean body mass (muscle). However, the CC can vary significantly as a function of urine volume. An unusually high CC most likely indicates poor hydration of the patient at the time of the urine collection. A very low CC most likely indicates unusually high fluid consumption, or perhaps the influence of diuretics. If the urine specimen is very dilute (extremely low CC), the accuracy of the neurotransmitter analysis may be compromised due to analytical detection limits. It is emphasized that the CC in this specimen should not be utilized to assess renal function or glomerular filtration. For that purpose, one should perform a bona fide creatinine clearance test.
For a given age and gender, intra-individual variability in daily creatinine excretion can vary by as much as two-fold. Therefore, to more accurately assess neurotransmitter status using a random collection, the reported values for each analyte are expressed per gram “normalized” creatinine.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 30
www.doctorsdata.com
KEYMAO = monoamine oxidaseCofactors for MAO: B2, B3, P5P, Fe, MgCOMT = catechol-o-methyl-transferaseCofactors for COMT: SAMe, MgP5P = (pyridoxal-5-phosphate) activated form of vitamin B6BH4 = (tetrahydrobiopterin)Endogenous levels can be supported with SAMe, vitamin B3, C, Mo, ZnMTHF = (methyltetrahydrofolate) active form of folate. SAMe = endogenous levels can be supported with Mg, MTHF, and methylcobalamin supplementation.
Cofactors = Enzymes =
Neurotransmitter PathwaysNT
L-Dopa
Dopamine
Norepinephrine
Epinephrine
P5PIronBH4
Vitamin D
P5P
P5P
SAMeCortisol
phenylethanolamine N-methyltransferase
dopamineB-hydroxylase
aromatic amino acid decarboxylase
tyrosine hydroxylase
tyrosine decarboxylase
tryptophan decarboxylase
MAO
Vitamin CCopper
B3
Phenylalanine
Phenethylamine (PEA)
MAO
P5P
P5P, Fe, BH4aromatic amino acid decarboxylase
Phenylalanine hydroxylase
MAO
COMT
COMT
COMT
Normetanephrine
Metanephrine
DOPAC
3-MT
Tyrosine TyramineTryptophan
5-Hydroxytryptophan(5-HTP)
Serotonin
Acetylserotonin
Melatonin
P5P
SAMehydroxyindole-0-methyltransferase
B2B3
Iron
N-acetyltransferase
5-HIAA
MAO
aromatic amino acid decarboxylase
tryptophan hydroxylase
P5PIronBH4
Vitamin D
MAO
TryptamineP5P
Serine GlycineSAMeP5PMg
P5P
serine hydroxymethyltransferase
glycinedecarboxylase
CO2NH3
“glycine cleavage system”
Cysteine TaurineP5P, Fe, Mo, SAMe
Glutamine
glutaminaseglutaminesynthetase
Glutamate
GABA
glutamatedecarboxylase (GAD)
P5PTaurine
(P5P)
Glutamic Acidalpha-ketoglutarate
glutamatedehydrogenase (B3)
aminotransferase
Note: aminotransferase aka transaminase
Histidine
metabolites
metabolites
HistamineP5P
HistidineDecarboxylase
Diamine oxidaseP5P, Copper, Iron, B12, vitamin C
Histamine
methyltransferase
SAMe
Neurotransmitter Pathways

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 31
www.doctorsdata.com
Treatment Considerations
LOW PEA HIGH PEA
• DL/LPhenylalanine: 250-4000 mg
• PEA 100 - 500 mg
• Probiotics
• Cofactor (to support metabolism and conver-sion)
1. P5P: 10-50 mg
• Dietary adjustments (decrease protein and fer-mented foods)
• Probiotics
• Support MAO for metabolism
LOW TYROSINE HIGH TYROSINE
• DL/L-Phenylalanine: 250-4,000 mg
• Tyrosine: 500-2500 mg
• Iron, SAMe, Vitamins B3, C, D
LOW TYRAMINE HIGH TYRAMINE
• P5P: 10-50 mg • If tyramine is high, but dopamine is low, the en-zymes of dopamine synthesis (cofactors: SAMe, vitamins B3, D, zinc, molybdenum, iron) may be inhibited.
• Support MAO for metabolism
LOW DOPAMINE HIGH DOPAMINE
• N-acetyl L-tyrosine 250-1,500 mg
• Rhodiola (Rhodiola rosea) root extract (4% Rosav-ins, 1%Salidroside) 100-300 mg
• Mucuna pruriens 200-800 mg
• L-theanine 100-500 mg bid
• Co-factors
1. Vitamin D: 1,000-10,000 IU
2. Iron: 25-50 mg
3. P5P: 10-50 mg
4. BH4
a) Vitamin B3: 50 mg
b) Vitamin C: 1000-3000 mg
c) SAMe: 100-500 mg
d) Molybdenum: 250-500 mcg
e) Zinc: 15-30 mg
• L-theanine 100-500 mg bid
• Rhodiola (Rhodiola rosea) root extract (4% Rosav-ins, 1%Salidroside) 1,000-2,000 mg
• Co-factors (to support MAO/COMT)
1. Vitamin B2: 50 mg
2. Vitamin B3: 100 mg
3. Iron: 25-50 mg
4. SAMe: 100-500 mg
• Co-factors (if norepi low or low range)
1. Vitamin C: 1,000-3,000 mg
2. Copper: 0.5-1 mg
3. Vitamin B3: 50 mg
DISCLAIMER: All information given about health conditions, treatments, products and dosages are not intended to be a substitute for professional medical advice, diagnosis or treatment.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 32
www.doctorsdata.com
LOW DOPAC HIGH DOPAC
• Support MAO enzyme
• If dopamine levels are low, support dopamine secretion
• Support COMT enzyme
• Antioxidants
• i.e., Selenium, pycnogenol, curcumin, ber-berine and vitamin B12
• St. John’s Wort 300 mg tid
• Adrenal support
LOW 3-MT HIGH 3-MT
• Support COMT enzyme
• Antioxidants
• i.e., Selenium, pycnogenol, curcumin, berberine and vitamin B12
• If dopamine levels are low, support dopamine secretion
• Support MAO enzyme
LOW NOREPINEPHRINE HIGH NOREPINEPHRINE
• N-acetyl L-tyrosine 250-1,500 mg
• Rhodiola (Rhodiola rosea) root extract (4% Rosavins, 1%Salidroside) 100-300 mg
• Mucuna pruriens 200-800 mg
• L-theanine 100-500 mg bid
• Co-factors
1. Vitamin C: 1,000-3,000 mg
2. Copper: 0.5-1 mg
3. Vitamin B3: 50 mg
4. P5P: 10-50 mg
• L-theanine 100-500 mg bid
• Rhodiola (Rhodiola rosea) root extract (4% Rosav-ins, 1%Salidroside) 1,000-2,000 mg
• Co-factors (to support MAO/COMT)
1. Vitamin B2: 50 mg
2. Vitamin B3: 100 mg
3. Iron: 25-50 mg
4. SAMe: 100-500 mg
• Co-factors (if epi low)
1. Vitamin C: 1,000-3,000 mg
2. SAMe: 100-500 mg
3. Adrenal support
LOW NORMETANEPHRINE HIGH NORMETANEPHRINE
• Support COMT enzyme
• If norepinephrine levels are low, support nor-epinephrine secretion
• Support MAO enzyme

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 33
www.doctorsdata.com
LOW EPINEPHRINE HIGH EPINEPHRINE
• N-acetyl L-tyrosine 250-1,500 mg
• Rhodiola (Rhodiola rosea) root extract (4% Rosavins, 1%Salidroside) 100-300 mg
• Mucuna pruriens 200-800 mg
• L-theanine 100-500 mg bid
• Co-factors
1. Vitamin C: 1,000-3,000 mg
2. SAMe: 100-500 mg
3. Magnesium: 150-500 mg
4. P5P: 10-50 mg
5. Adrenal support
• L-theanine 100-500 mg bid
• Rhodiola (Rhodiola rosea) root extract (4% Rosav-ins, 1%Salidroside) 1,000-2,000 mg
• Co-factors (to support MAO/COMT)
1. Vitamin B2: 50 mg
2. Vitamin B3: 100 mg
3. Iron: 25-50 mg
4. SAMe: 100-500 mg
LOW METANEPHRINE HIGH METANEPHRINE
• Support COMT enzyme
• If epinephrine levels are low, support epineph-rine secretion
• Support MAO enzyme
ELEVATED N/E RATIO
• SAMe 100-500 mg
• Magnesium 150-500 mg
• Adrenal support
LOW TRYPTAMINE HIGH TRYPTAMINE
• P5P: 10-50 mg • If tryptamine is high, but serotonin is low, the enzymes of serotonin synthesis (cofactors: SAMe, vitamins B3, D, zinc, molybdenum, iron) may be inhibited.
• Support MAO for metabolism

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 34
www.doctorsdata.com
LOW SEROTONIN HIGH SEROTONIN
• Tryptophan 500-2,000 mg
• Rhodiola (Rhodiola rosea) root extract (4% Rosav-ins, 1%Salidroside) 100-300 mg
• 5 HTP 50-600 mg
• L-theanine 100-500 mg bid
• Co-factors
1. Vitamin D: 1,000-10,000 IU
2. Iron: 25-50 mg
3. P5P: 10-50 mg
4. BH4
a) Vitamin B3: 50 mg
b) Vitamin C: 1000-3000 mg
c) SAMe: 100-500 mg
d) Molybdenum: 250-500 mcg
e) Zinc: 15-30 mg
• L-theanine 100-500 mg bid
• Rhodiola (Rhodiola rosea) root extract (4% Rosav-ins, 1%Salidroside) 1,000-2,000 mg
• Co-factors (to support metabolism and conver-sion)
1. Vitamin B2: 50 mg
2. Vitamin B3: 100 mg
3. Iron: 25-50 mg
4. SAMe: 100-500 mg
LOW 5-HIAA HIGH 5-HIAA
• Support MAO enzyme
• If serotonin levels are low, support serotonin secretion
• Antioxidants
• i.e., Selenium, pycnogenol, curcumin, ber-berine and vitamin B12
• St. John’s Wort 300 mg tid
• Adrenal support
LOW GLUTAMATE HIGH GLUTAMATE
• L-glutamine 1,000-3,000 mg • L-theanine 100-500 mg bid
• Taurine 500-1,500 mg
• N-acetyl cysteine 600 mg bid-tid
• Cofactors (to support metabolism and conversion)
1. Vitamin B3: 100 mg
2. P5P: 10-50 mg
3. Magnesium: 150-500 mg (reduces gluta-mate toxicity)

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 35
www.doctorsdata.com
LOW GABA HIGH GABA
• L-theanine 100-500 mg bid
• GABA 500-2,000 mg qd
• Taurine 500-1,500 mg
• Glutamine 1,000-3,000 mg
• Co-factors
1. P5P: 10-50 mg
• L-theanine 100-500 mg bid
LOW GLYCINE HIGH GLYCINE
• Glycine 500-6,000 mg bid
• L-theanine 100-500 mg bid
• Cofactors (to support metabolism and conver-sion)
1. P5P: 10-50 mg
2. Magnesium 150-500 mg
• Alpha lipoic acid 200-1,200 mg
• Cofactors (to support metabolism and conver-sion)
1. P5P: 10-50 mg
2. SAMe 100-500 mg
LOW HISTAMINE HIGH HISTAMINE
• Histidine 500-1000 mg
• Cofactors (to support metabolism and conver-sion)
1. P5P: 10-50 mg
2. SAMe 100-500 mg
• Avoid histamine rich foods
• Diamine oxidase 10,000-20,000 HDU no longer than 15 min before each histamine rich meal
• Anti-inflammatory compounds (quercetin, cur-cumin, botswellia, flavonoids)
• MSM 1,000-3,000 mg
• Cofactors (to support metabolism and conversion)
1. SAMe 100-500 mg
2. Vitamin B2: 50 mg
3. Copper: 0.5-1 mg
4. P5P: 10-50 mg
LOW TAURINE HIGH TAURINE
• Taurine 500-2,000 mg
• Cysteine 500-1,500 mg
• Co-factors
1. P5P: 10-50 mg
2. Iron: 25-50 mg
3. Molybdenum: 250-500 mcg
• Antioxidants
• Probiotics

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 36
www.doctorsdata.com
Metabolism Support• MAO enzyme supported by
• Vitamin B2: 50 mg (ideally riboflavin 5 phosphate)
• Vitamin B3: 100 mg
• Iron: 25-50 mg
• COMT enzyme supported by
• SAMe: 100-500 mg
• Mg: 150-500 mg
• MTHF: 400-5,000 mcg
• Methylcobalamin: 1,000-5,000 mcg
Clinical Pearls: General Treatment Considerations• Because of their importance as co-factors, consider generalized support in the form of methylated B
vitamins and Mg for every patient with an imbalance.
• Fish oil (EPA/DHA) is neuromodulatory, and exhibits antidepressant effects.
• SAMe: endogenous levels can be supported with Mg, MTHF and methylcobalamin
• Mg: 150-500 mg
• MTHF: 400-5,000 mcg
• Methylcobalamin: 1,000-5,000 mcg
• L-theanine
• Best given BID as it has a short ½ life
• Acts as a GABA agonist. Neuroinhibitory and parasympathetic
• Antagonistic effects on glutamate receptors
• Acts to optimize serotonin, dopamine and GABA levels, promoting overall neurotransmitter balance
• Magnesium and vitamin C can be given to bowel tolerance
• Iron best given as citrate or bisglycinate.
• Adaptogenic herbs treat both the adrenal cortex and the medulla, and therefore can modulate cortisol, dopamine, norepinephrine and epinephrine levels.
• Cytokines associated with inflammation can influence neurotransmitter secretion. Identifying and addressing inflammation is an essential compnent of any treatment plan.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 37
www.doctorsdata.com
References
PhenylethylamineBerry, MD. (2004), Mammalian central nervous system trace amines. Pharmacologic amphetamines, physiologic neuromodulators. Journal of Neurochemistry vol. 90 (2) p. 257-71.
Husebye, ES; Boe, AS; Rorsman, F; et al. (2000,) Inhibition of aromatic L-amino acid decarboxylase activity by human autoantibodies. Clinical and Experimental Immunology vol. 120 (3) p. 420-3.
Kusaga, A. (2002), Decreased beta-phenylethylamine in urine of children with attention deficit hyperactivity disorder and autistic disorder. Brain and Development vol. 34 (3) p. 243-8.
Licata, AA; Radfar, N; Bartter, FC; et al. (1978), The urinary excretion of phosphoethanolamine in diseases other than hypophosphatasia. The American Journal of Medicine vol. 64 (1) p. 133-138.
Narang, D; et al. (2011), Trace amines and their relevance to psychiatry and neurology: A brief overview. Bulletin of Clinical Psychopharmacology vol. 21:73-79.
Zucchi, R; Chiellini, G; Scanlan, TS; et al. (2006), Trace amine-associated receptors and their ligands. British Journal of Pharmacology vol. 149 (8) p. 967-78.
Tyrosine
Cansev, M; Wurtman, RJ. (2007) Chapter 4: Aromatic Amino Acids in the Brain. Handbook of Neurochemistry and Molecular Neurobiology, Springer U.S.
Fernstrom, JD. (2000), Can nutrient supplements modify brain function? Am J Clin Nutr vol. 71 (6) p. 1669S-1673.
Fernstrom, JD; Fernstrom, MH. (2007), Tyrosine, phenylalanine, and catecholamine synthesis and function in the Brain. J. Nutr. vol. 137 (6) p. 1539S-1547.
Leyton, M; Young, SN; Pihl, RO; et al. (2000), Effects on mood of acute phenylalanine/tyrosine depletion in healthy women American College of Neuropsychopharmacology vol. 22 (1) p. 52-63.
Tyramine
Berry, MD. (2007), The potential of trace amines and their receptors for treating neurological and psychiatric diseases. Reviews on Recent Clinical Trials vol. 2 p. 3-19.
Berry, MD. (2004), Mammalian central nervous system trace amines. Pharmacologic amphetamines, physiologic neuromodulators. Journal of Neurochemistry vol. 90 (2) p. 257–71.
Goldstein, DS. (2008), Genotype and vascular phenotype linked by catecholamine systems. Circulation vol. 117 (4) p. 458-61.
Narang, D; Tomlinson, S; Holt, A; et al. (2011), Trace amines and their relevance to psychiatry and neurology: a brief overview. Bulletin of Clinical Psychopharmacology vol. 21 (1) p. 73-79.
Dopamine
Buttarelli, FR; Fanciulli, A; Pellicano, C; et al. (2011) The dopaminergic system in peripheral blood lymphocytes: from physiology to pharmacology and potential applications to neuropsychiatric disorders. Current Neuropharmacology vol. 9 (2) p. 278-88.
Davidson, D. (2005) Elevated urinary dopamine in adults and children. Annals of clinical biochemistry vol. 42 (Pt 3) p. 200-7.
Eisenhofer, G; Kopin, IJ; Goldstein, DS. (2004) Catecholamine Metabolism: A Contemporary View with Implications for Physiology and Medicine. Pharmacol. Rev. vol. 56 (3) p. 331-349.
Ferreira, A; Bettencourt, P; Pestana, M; et al. (2001) Heart failure, aging, and renal synthesis of dopamine, American Journal of Kidney Diseases vol. 38 (3) p. 502-509.
Glavin, GB; Szabo, S. (1990) Dopamine in gastrointestinal disease. Digestive Diseases and Sciences vol. 35 (9) p. 1153-1161.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 38
www.doctorsdata.com
Hahn, RG MD; Knox, LM PhD; Formann,TA. (2005) Evaluation of Post streptococcal Illness.Am Fam Physician. vol. 15;71(10) p.1949-1954.
Meiser, J; Weindl, D; Hiller, K. (2013) Complexity of dopamine metabolism. Cell Communication and Signaling : CCS vol. 11 (1) p. 34.
Rasheed, N; Alghasham, A. (2012) Central dopaminergic system and its implications in stress-mediated neurological disorders and gastric ulcers: short review. Advances in Pharmacological Sciences vol. 2012 p. 182671.
Sistrunk, SC; Ross, MK; Filipov, NM. (2007) Direct effects of manganese compounds on dopamine and its metabolite Dopac: an in vitro study. Environmental Toxicology and Pharmacology vol. 23 (3) p. 286-96.
Trachte, GJ; Uncini, T; Hinz, M. (2009) Both stimulatory and inhibitory effects of dietary 5-hydroxytryptophan and tyrosine are found on urinary excretion of serotonin and dopamine in a large human population. Neuropsychiatric disease and treatment vol. 5 p. 227-35.
Zhang, Y; Cuevas, S; Asico, LD; et al. (2012) Deficient dopamine D2 receptor function causes renal inflammation independently of high blood pressure. PloS one vol. 7 (6) p. e38745
3,4-dihydroxyphenyl acetic acid (DOPAC)
Desai, Vl; Kaler, SG. (2008) Role of copper in human neurological disorders. American Journal of Clinical Nutrition vol. 88 (3) p. 855S-858.
Eldrup, E; Richter, EA. (2000) DOPA, dopamine, and DOPAC concentrations in the rat gastrointestinal tract decrease during fasting. Am J Physiol Endocrinol Metab vol. 279 (4) p. E815-822.
Eldrup, E. (2004) Significance and origin of DOPA, DOPAC, and dopamine-sulphate in plasma, tissues and cerebrospinal fluid. Danish Medical Bulletin - No. 1. February 2004. Vol. 51 Pages 34-62.
Goldstein, DS; Eisenhofer, G; Kopin, IJ. (2003) Sources and Significance of Plasma Levels of Catechols and Their Metabolites in Humans. J. Pharmacol. Exp. Ther. vol. 305 (3) p. 800-811.
Sistrunk, SC; Ross, MK; Filipov, NM. (2007) Environmental toxicology and pharmacology vol. 23 (3) p. 286-96.
Wallace, LJ; Traeger, JS. (2012) Dopac distribution and regulation in striatal dopaminergic varicosities and extracellular space. Synapse (New York, N.Y.) vol. 66 (2) p. 160-73
Zhou, W; Gallagher, A; Hong, D-P; et al. (2009) At low concentrations, 3,4-dihydroxyphenylacetic acid (DOPAC) binds non-
covalently to alpha-synuclein and prevents its fibrillation. Journal of Molecular Biology vol. 388 (3) p. 597-610.
3-Methoxytyramine (3-MT)
Alachkar, A; Brotchie, JM; Jones, OT. (2010) Binding of dopamine and 3-methoxytyramine as l-DOPA metabolites to human a2-adrenergic and dopaminergic receptors. Neuroscience Research vol. 67 (3) p. 245-249
Antkiewicz-Michaluk, L; Ossowska, K; Romanska, I; et al. (2008) 3-Methoxytyramine, an extraneuronal dopamine metabolite plays a physiological role in the brain as an inhibitory regulator of catecholaminergic activity. European Journal of Pharmacology vol. 599 (1) p. 32-35.
Cabib, S.; Puglisi-Allegra, S. (1996) Different effects of repeated stressful experiences on mesocortical and mesolimbic dopamine metabolism. Neuroscience vol. 73 (2) p. 375-380.
Eisenhofer, G; Lenders, JWM; Timmers, H; et al. (2011) Measurements of plasma methoxytyramine, normetanephrine, and metanephrine as discriminators of different hereditary forms of pheochromocytoma. Clin. Chem. vol. 57 (3) p. 411-420
Ossowska, K; Wardas, J; Kuter, K; et al. Influence of paraquat on dopaminergic transporter in the rat brain. Pharmacological Reports vol. 57 (3) p. 330-5.
Sotnikova TD; Beaulieu J-M; Espinoza S; et al. (2010) The Dopamine Metabolite 3-Methoxytyramine Is a Neuromodulator. PLoS ONE 5(10): e13452. doi:10.1371/journal.pone.0013452.
Young, WF. (2006) Paragangliomas: Clinical overview. Annals of the New York Academy of Sciences vol. 1073 p. 21-9

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 39
www.doctorsdata.com
Norepinephrine
Eisenhofer, G; Kopin, IJ; Goldstein, DS. (2004) Catecholamine Metabolism: A Contemporary View with Implications for Physiology and Medicine. Pharmacol. Rev. vol. 56 (3) p. 331-349.
Goldstein, DS.; Eisenhofer, G; Kopin, IJ. (2003) Sources and Significance of Plasma Levels of Catechols and Their Metabolites in Human. Journal of Pharmacol. Exp. Ther. vol. 305 (3) p. 800-811.
Kodirov, SA. (2012) The Amygdala - A Discrete Multitasking Manager. InTech. ISBN 978-953-51-0908-2.
Otte, C; Neylan, C; Pipkin, SS.; et al. (2005) Depressive Symptoms and 24-Hour Urinary Norepinephrine Excretion Levels in Patients With Coronary Disease: Findings From the Heart and Soul Study. American Journal of Psychiatry vol. 162 (11) p. 2139-2145.
Soliman, K; Sturman, S; Sarkar, PK; et al. (2010) Postural orthostatic tachycardia syndrome (POTS): a diagnostic dilemma. Br J Cardivol. 17 (1) p. 36-9.
Normetanephrine
American Association for Clinical Chemistry (2010), Urine metanephrines http://labtestsonline.org/understanding/analytes/urine-metanephrine/tab/sample/
Daubner, SC; Le, Ty; Wang, S. (2011), Tyrosine hydroxylase and regulation of dopamine synthesis. Archives of biochemistry and biophysics vol. 508 (1) p. 1-12.
Eisenhofer, G; Kopin, IJ; Goldstein, DS. (2004), Catecholamine metabolism: A contemporary view with implications for physiology and medicine. Pharmacol. Rev. vol. 56 (3) p. 331-349.
Eisenhofer, G. (2001), Free or Total Metanephrines for diagnosis of pheochromocytoma: What is the difference? Clin. Chem. vol. 47 (6) p. 988-989.
Elmasry, A; Lindberg, E; Hedner, J; et al. (2002), Obstructive sleep apnoea and urine catecholamines in hypertensive males: a population-based study. Eur. Respir. J. vol. 19 (3) p. 511-517.
Goldstein, DS. (2010), Catecholamines 101. Clinical autonomic research: Official Journal of the Clinical Autonomic Research Society vol. 20 (6) p. 331-52.
Jong, WHA; Eisenhofer, G; Post, WJ; et al. (2013), Dietary influences on plasma and urinary metanephrines: Implications for diagnosis of catecholamine-producing tumors. The Journal of clinical endocrinology and metabolism vol. 94 (8) p. 2841-9
Epinephrine
Goldstein, DS. (2010) Catecholamines 101. Clinical autonomic research: Official Journal of the Clinical Autonomic Research Society, vol. 20(6) p.331-52.
Hays, MT; Solomon,DH. (1969) Effect of epinephrine on the peripheral metabolism of thyroxine.The Journal of Clinical Investigation vol. 48 (6) p. 1114-23.
Ji, Y; Snyder, EM; Fridley, BL; et al. (2008) Human phenylethanolamine N-methyltransferase genetic polymorphisms and exercise-induced epinephrine release. Physiol Genomics vol. 33 (3) p. 323-332.
Tobin, L; Simonsen, L; Galbo, H; et al. (2012) Vascular and metabolic effects of adrenaline in adiposetissue in type 2 diabetes. Nutrition & diabetes vol. 2 p. e46.
Wu, Q; Caine, JM; Thomson, SA; et al. (2009) Time-dependent inactivation of human phenylethanolamine N-methyltransferase by 7-isothiocyanatotetrahydroisoquinoline. Bioorganic & Medicinal Chemistry Letters vol. 19 (4) p. 1071-4.
Ziegler, MG; Aung, M; Kennedy, B (1997) Sources of human urinary epinephrine. International Society of Nephrology vol. 51 (1) p. 324-327.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 40
www.doctorsdata.com
Metanephrine
Daubner, SC; Le, T; Wang, S. (2011) Tyrosine hydroxylase and regulation of dopamine synthesis. Archives of Biochemistry and Biophysics vol. 508 (1) p. 1-12.
Eisenhofer, G ; Lenders, JWM; Timmers, H; et al. (2011) Measurements of plasma methoxytyramine, normetanephrine, and metanephrine as discriminators of different hereditary forms of pheochromocytoma. Clin. Chem. vol. 57 (3) p. 411-420.
Eisenhofer, G; Kopin, IJ; Goldstein, DS. (2004) Catecholamine Metabolism: A Contemporary View with Implications for Physiology and Medicine. Pharmacol. Rev. vol. 56 (3) p. 331-349.
Eisenhofer, G. (2001) Free or Total Metanephrines for Diagnosis of Pheochromocytoma: What Is the Difference? Clin. Chem. vol. 47 (6) p. 988-989.
Elmasry, A.; Lindberg, E; Hedner, J; et al. (2002) Obstructive sleep apnea and urine catecholamines in hypertensive males: a population-based study. Eur. Respir. J. vol. 19 (3) p. 511-517.
Goldstein, DS. (2010), Catecholamines 101. Clinical autonomic research: Official Journal of the Clinical Autonomic Research Society vol. 20 (6) p. 331-52.
Goldstein, DS; Eisenhofer, G; Kopin, IJ. (2003) Sources and Significance of Plasma Levels of catechols and their metabolites in humans. J. Pharmacol. Exp. Ther. vol. 305 (3) p. 800-811.
Jong, WHA; Eisenhofer, G; Post, WJ; et al. (2013) Dietary influences on plasma and urinary metanephrines: Implications for diagnosis of catecholamine-producing tumors. The Journal of clinical endocrinology and metabolism vol. 94 (8) p. 2841-9
American Association for Clinical Chemistry (2010) Urine Metanephrines http://labtestsonline.org/understanding/analytes/urine-metanephrine/tab/sample/ metanephrine/tab/sample/
Tryptamine
Anwar, MA; Ford, WR; Broadley, KJ; et al (2012), Vasoconstrictor and vasodilator responses to tryptamine of rat-isolated perfused mesentery: comparison with tyramine and ß-phenylethylamine.British journal of pharmacology vol. 165 (7) p. 2191-202.
Berry, MD. (2007), The potential of trace amines and their receptors for treating neurological and psychiatric diseases. Reviews on Recent Clinical Trials vol.2 p. 3-19.
Berry, MD. (2004), Mammalian central nervous system trace amines. Pharmacologic amphetamines, physiologic neuromodulators. Journal of Neurochemistry vol. 90(2) p. 257–71.
Narang, D; Tomlinson, S; Holt, A; et al (2011), Trace amines and their relevance to psychiatry and neurology: a brief overview. Bulletin of Clinical Psychopharmacology vol. 21 (1) p. 73-79.
Yu, A-M; Granvil, CP; Haining, RL; et al. (2003), The relative contribution of monoamine oxidase and cytochrome P450 isozymes to the metabolic deamination of the trace amine tryptamine. J. Pharmacol. Exp. Ther. vol. 304 (2) p. 539-546.
Serotonin (5-hydroxytryptamine)
Cansev, M; Wurtman, RJ. (2007), Chapter 4: Aromatic amino acids in the brain. Handbook of Neurochemistry and Molecular Neurobiology, Springer U.S.
Field, T; Hernandez-Reif, M; Diego, M; et al. (2009), Cortisol decreases and serotonin and dopamineincrease following massage therapy. Informa UK Ltd UK.
Field, T; Diego, M; Hernandez-Reif, M; et al. (2008), Prenatal serotonin and neonatal outcome: brief repor. Infant Behavior & Development vol. 31 (2) p. 316-20.
Hannon, J; Hoyer, D. (2008), Molecular biology of 5-HT receptors. Behavioral Brain Research vol. 195 (1) p. 198-213.
Iqbal, MM. (2012) Overview of serotonin syndrome. Annals of clinical Psychiatry vol. 24(4):310-318.
Janusonis, S. (2005), Statistical distribution of blood serotonin as a predictor of early autistic brain abnormalities. Theoretical biology & medical modeling vol. 2 p. 27.
Jovanovic, H; Lundberg, J; Karlsson, P; et al. (2008), Sex differences in the serotonin 1A receptor and serotonin transporter binding in the human brain measured by PET. NeuroImage vol. 39 (3) p. 1408-19.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 41
www.doctorsdata.com
Oxenkrug, GF. (2010), Tryptophan kynurenine metabolism as a common mediator of genetic and environmental impacts in major depressive disorder: the serotonin hypothesis revisited 40 years later.The Israel Journal of Psychiatry and Related Sciences vol. 47 (1) p. 56-63.
Spiller, R. (2007), Recent advances in understanding the role of serotonin in gastrointestinal motility in functional bowel disorders: alterations in 5-HT signaling and metabolism in human disease.Neurogastroenterology and Motility vol. 19 Suppl. 2 p. 25-31.
Young, SN. (2007), How to increase serotonin in the human brain without drugs. Journal of Psychiatry & Neuroscience vol. 32 (6) p. 394-9.
5-hydroxyindol acetic acid (5-HIAA)
Cansev, M; Wurtman, RJ. (2007,) Chapter 4: Aromatic amino acids in the brain. Handbook of Neurochemistry and Molecular Neurobiology, Springer U.S.
Garg, S; Staros, EB. (2014) 5-hydroxyindol acetic acid (5-HIAA)http://emedicine.medscape.com/article/2089202-overview 2 Gastroenterology vol. 3 p. e13.
Garg, S; Staros, E. (2014) B5-hydroxyindol acetic acid (5-HIAA) http://emedicine.medscape.com/article/2089202-overview. Manocha, M; Khan, WI. (2012), Serotonin and GI disorders: an update on clinical and experimental studies. American College of Gastroenterology vol. 3 p. e13.
Moul, C; Dobson-Stone, C; Brennan, J; et al. (2013), An exploration of the serotonin system in antisocial boys with high levels of callous-unemotional traits. PloS one vol. 8 (2) p. e56619.
Spiller, R. (2007), Recent advances in understanding the role of serotonin in gastrointestinal motility in functional bowel disorders: alterations in 5-HT signaling and metabolism in human disease. Neurogastroenterology and Motility vol. 19 Suppl. 2 p. 25-31
Glutamate
Akiba, Y; Kaunitz, JD. (2009), Luminal chemo sensing and upper gastrointestinal mucosal defenses.Am J Clin Nutr vol. 90 (3) p. 826S-831
Bridges, R; Lutgen, V; Lobner, D; et al (2012), Thinking outside the cleft to understand synaptic activity: contribution of the cystine-glutamate antiporter (System xc-) to normal and pathological glutamatergic signaling. Pharmacological reviews vol. 64 (3) p. 780-802.
Bridges, RJ; Natale, NR; Patel, SA. (2012), System xc? cystine/glutamate antiporter: an update on molecular pharmacology and roles within the CNS. British Journal of Pharmacology vol. 165 (1) p. 20-34.
Burrin, DG; Stoll, B. (2009), Metabolic fate and function of dietary glutamate in the gut. Am J Clin Nutr vol. 90 (3) p. 850S-56.
Cotman, CW; Kahle, JS; Miller, SE; et al. (2000), Excitatory Amino Acid Neurotransmission.Neuropsychopharmacology – 5th Generation of Progress Lippincott, Williams, & Wilkins, Philadelphia, Pennsylvania.
Dai, Z-L; Wu, G; Zhu, W-Y. (2011), Amino acid metabolism in intestinal bacteria: links between gut ecology and host health, Frontiers in Bioscience vol.16, p.1768-86.
De Bundel, D; Schallier, A; Loyens, E et al. (2011), Loss of system xformula does not Induce oxidative stress but decreases extracellular glutamate in hippocampus and Influences spatial working memory and limbic seizure susceptibility. J. Neurosci. vol. 31 (15) p. 5792-5803.
Labow, BI; Souba, WW; Abcouwer, SF. (2001), Mechanisms governing the expression of the enzymes of glutamine metabolism- glutaminase and glutamine synthetase. J. Nutr. vol. 131 (9) p. 2467S-2474
Julio-Pieper, M; Flor, PJ; Dinan, TG; et al. (2011), Exciting times beyond the brain: metabotropic glutamate receptors in peripheral and non-neural tissues. PHARMACOLOGICAL REVIEWS Vol. 63, No. 1.Pharmacol Rev 63:35–58.
Nakamura, E; Uneyama, H; Torii, K. (2013), Gastrointestinal nutrient chemo sensing and the gut-brain axis: significance of glutamate signaling for normal digestion. Journal of Gastroenterology and Hepatology vol. 28 Suppl 4 p. 2-8.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 42
www.doctorsdata.com
Valentine, GW; Sanacora, G. (2009), Targeting glial physiology and glutamate cycling in the treatment of depression. Biochemical Pharmacology vol. 78 (5) p. 431-9.
Willard, SS; Koochekpour, S. (2013), Glutamate, Glutamate Receptors, and Downstream Signaling Pathways. Int J Biol Sci 2013; 9(9):948-959.
Gamma Aminobutyric Acid (GABA)
Alabdali, A; Al-Ayadhi, L; El-Ansary, A. (2014) Association of social and cognitive impairment and biomarkers in autism spectrum disorders. Journal of Neuroinflammation vol. 11 (1) p. 4.
Claus SP; Tsang, TM; Wang, Y; et al. (2008) Systemic multicompartmental effects of the gut microbiome on mouse metabolic phenotypes. Molecular Systems Biology vol. 4 (1) p. 219.
Davis; et al., Editors Neuropsychopharmacology: The Fifth Generation of Progress, Lippincott, Williams, & Wilkins, Philadelphia, Pennsylvania, 2002.
Gajcy, K.; Lochynski, S.; Librowski, T. (2010) A Role of GABA analogues in the treatment of neurological diseases. Current Medicinal Chemistry, vol. 17(22), p. 2338-47.
Kim, K-J; Pearl PL; Jensen K; et al. (2011) Succinic semialdehyde dehydrogenase: biochemical-molecular-clinical disease mechanisms, redox regulation, and functional significance. Antioxidants & Redox Signaling vol. 15 (3) p. 691-718.
Morgan, PT; Pace-Schott EF; Mason GF; et al. (2012), Cortical GABA levels in primary insomnia. Sleep vol. 35 (6) p. 807-14.
Neuropsychopharmacology: The Fifth Generation of Progress, Davis, et al. Lippincott, Williams, & Wilkins, Philadelphia, Pennsylvania, 2002. Fuks, JM; Arrighi, RBG; Weidner, JM; et al. (2012), GABAergic signaling is linked to a hypermigratory phenotype in dendritic cells infected by Toxoplasma gondii. PLoS pathogens vol. 8 (12) p. e1003051.
Nicholson-Guthri, CS; Guthrie, GD; Sutton, GP; et al. (2001), Urine GABA levels in ovarian cancer patients: elevated GABA in malignancy. Cancer Letters vol. 162 (1) p. 27-30.
Pearl, PL; Hartka, TR; Cabalza, JL; et al. (2006), Inherited disorders of GABA metabolism. Future Neurology vol. 1 (5) p. 631-636.
Glycine
Betz, H, Gomeza; J; Armsen, W; et al. (2006) Glycine transporters: essential regulators of synaptic transmission. Biochemical SocietyTransactions vol. 34 (Pt 1) p. 55-8.
Busanello, ENB; Moura, AP; Viegas, CM; et al. (2010), Neurochemical evidence that glycine induces bioenergetical dysfunction. Neurochemistry International vol. 56 (8) p. 948-954.
Christoffel, P; Stephanus, B; Elardus, E. (2014) A new perspective on the importance of glycine conjugation in the metabolism of aromatic acids. Drug Metab Rev. 2014; 46(3):343-61 (ISSN: 1097-9883)
Legendre, P. (2001) The glycinergic inhibitory synapse. Cellular and Molecular Life Sciences vol. 58 (5) p. 760-93.
Petrus, C; Badenhorst, S; Erasmus, E. (2014), A new perspective on the importance of glycine conjugation in the metabolism of aromatic acids. Drug Metab Rev. 2014; 46(3):343-61 (ISSN: 1097-9883)
Histamine
Blandina, P; Efoudebe, M; Cenni, G; et al. (2004), Acetylcholine, histamine, and cognition: Two sides of the same coin. Learn. Mem. vol. 11 (1) p. 1-8.
Castellan Baldan, L; Williams, KA; Gallezot, JD; et al. (2014), Histidine decarboxylase deficiency causes tourette syndrome: parallel findings in humans and mice. Neuron vol. 81 (1) p. 77-90.

Doctor’s Data, Inc. Neurotransmitter RESOURCE GUIDE 43
www.doctorsdata.com
Devaraj, S; Hemarajata, P; Versalovic, J. (2013), The human gut microbiome and body metabolism: implications for obesity and diabetes. Clin. Chem. vol. 59 (4) p. 617-28.
Fell, MJ; Katner, JS; Rasmussen, Kt; et al. (2012), Typical and atypical antipsychotic drugs increase extracellular histamine levels in the rat medial prefrontal cortex: contribution of histamine h(1) receptor blockade. Frontiers in Psychiatry vol. 3 p. 49.
Friedman, BS; Steinberg, SC; Meggs, WJ; et al. (1989), Analysis of plasma histamine levels in patients with mast cell disorders. The American Journal of Medicine vol. 87 (6) p. 649-54.
Hofstra, CL; Desai, PJ; Thurmond, RL; Fung-Leung, W-P. (2003), Histamine H4 receptor mediates chemotaxis and calcium mobilization of mast Cells. J. Pharmacol. Exp. Ther. vol. 305 (3) p. 1212-21.
Horner, WE; Johnson, DE Schmidt, AW; et al. (2007), Methylphenidate and atomoxetine increase histamine release in rat prefrontal cortex. European Journal of Pharmacology vol. 558 (1) p. 96-97.
Kimura, K; Adachi, M; Kubo, K; et al. Y. (1999), The basal plasma histamine level and eosinophil count in allergic and non-allergic patients. Fukuoka Igaku Zasshi = Hukuoka Acta Medica vol. 90 (12) p. 457-63
Maintz, L; Novak, N. (2007), Histamine and histamine intolerance. American Journal of Clinical Nutrition vol. 85 (5) p. 1185-1196.
Scammell, TE; Mochizuki, T. (2009), Is low histamine a fundamental cause of sleepiness in narcolepsy and idiopathic hypersomnia? Sleep vol. 32 (2) p. 133-4.
Schwartz, J-C; Arrang, J-M; Garbarg, M. (2002), Histamine Neuropsychopharmacology – 5th Generation of Progress Lippincott, Williams, & Wilkins, Philadelphia, Pennsylvania.
Shan, L; Swaab, DF.; Bao, A-M. (2013), Neuronal histaminergic system in aging and age-related neurodegenerative disorders. Experimental Gerontology. Volume 48 (7) p. 603–7.
Yanai, K; Tashiro, M. (2007), The physiological and pathophysiological roles of neuronal histamine: an insight from human positron emission tomography studies. Pharmacology & Therapeutics vol. 113 (1) p. 1-15.
Taurine (2-aminoethane- sulfonic acid)
Cornell Chronicle (2014), Scientists close in on taurine’s activity in the brain (Red Bull drinkers, take note) Cornell Chronicle • 312 College Ave., Ithaca, NY 14850. http://news.cornell.edu/stories/2008/02/scientists-close-taurines-activity-brain
Jerkins, AA.; Jones, DD.; Kohlhepp, EA. (1998), Cysteine sulfinic acid decarboxylase mRNA abundance decreases in rats fed a high-protein diet. J. Nutr. vol. 128 (11) p. 1890-95.
Lourenco, R. and Camilo, M.E. (2002), Taurine: a conditionally essential amino acid in humans? An overview in health and disease. Nutr. Hosp. vol. XVII (6) 262-70.
Ripps, H; Shen, W. (2012) Review: Taurine: a “very essential” amino acid. Molecular vision vol. 18 p. 2673-86.
Stipanuk, MH; Ueki, I; Dominy, J E; et al. (2009), Cysteine dioxygenase: a robust system for regulation of cellular cysteine levels. Amino Acids vol. 37 (1) p. 55-63.
Ueki, L; Stipanuk, MH. (2007), Enzymes of the taurine biosynthetic pathway are expressed in rat mammary gland. J. Nutr. vol. 137 (8) p. 1887-1894.
Wu, Jang-Yen; Prentice, Howard (2010), Role of Taurine in the Central Nervous System. Journal of Biomedical Science, 17(Suppl 1) p.S1.

3755 Illinois Avenue • St. Charles, IL 60174-2420
800.323.2784 (US AND CANADA)0871.218.0052 (UK)
+1.630.377.8139 (GLOBAL)
doctorsdata.com
Science + Insight
© 2020 Doctor’s Data, Inc. All rights reserved.