Embed Size (px)
Citation preview

38ournal ofNeurology, Neurosurgery, and Psychiatry 1994;57:348-352
The neck-tongue syndrome
RichardW Orrell, C David Marsden
AbstractThe neck-tongue syndrome, consisting ofpain in the neck and altered sensation inthe ipsilateral half of the tongue aggra-
vated by neck movement, has beenattributed to damage to lingual afferentfibres travelling in the hypoglossal nerve
to the C2 spinal roots. The lingual affer-ents in the hypoglossal nerve are thoughtto be proprioceptive. Two further cases
of the neck-tongue syndrome are
described, the spectrum of its clinicalmanifestations is explored, and the phe-nomenon of lingual pseudoathetosis isillustrated as a result of the presumedlingual deafferentation.
(7 Neurol Neurosurg Psychiatry 1994;57:348-352)
UniversityDepartment ofClinical Neurology,The NationalHospital, QueenSquare, LondonWClN 3BG, UKRW OrrellC D MarsdenCorrespondence to:Dr RW Orrell.Received 14 April 1993and in final revised form14 June 1993.Accepted 21 June 1993
Lance and Anthony' described four patients,aged 8 to 14 years at onset, with a brief (sec-onds to a minute) sharp pain on one side ofthe upper neck or occiput on sudden rotationof the neck, followed immediately by tran-sient (seconds to minutes) ipsilateral numb-ness of the tongue. Two of these cases hadcongenital anomalies of the upper cervicalspine on radiography. Cyriax2 had previouslynoted a similar syndrome in two patients, one
of whom was a 45-year-old woman withattacks of severe pain at the occiput and leftside of the neck and numbness of the tongueand back of the palate, precipitated by turn-ing her head sharply to the right. The otherpatient had a cervical disc lesion and a sensa-
tion of pins and needles felt in the tongueonly.
Lance and Anthony' concluded that thepain was due to irritation of the second (andthird) cervical root, which is vulnerable tocompression in its course between the atlasand axis during neck rotation. They explainedthe unilateral numbness of the tongue on thebasis of afferent impulses (notably, propriocep-tive) travelling from the lingual nerve via thehypoglossal nerve to the second cervical root.
Bogduk3 clarified the anatomical basis forthe syndrome by cadaveric dissection,demonstrating that the C2 ganglion andspinal nerve lie dorsal to the lateral atlantoax-ial joint; the joint is innervated by the C2ventral ramus. He proposed that the pain was
due to temporary abnormal subluxation ofthe lateral atlantoaxial joint on rotation of thehead. This strains the joint capsule, andthereby causes pain in the suboccipital
region. He attributed the unilateral numbnessof the tongue (and of the skin behind the ear)to compression of the C2 ventral ramus bymovement or subluxation of the lateralatlantoaxial joint. He suggested that theabnormal sensation on compression of pro-prioceptive afferents from the tongue is simi-lar to the altered sensation or numbnessrecognised in Bell's palsy, despite intacttrigeminal sensation, due to compression ofproprioceptive fibres in the facial nerve.
Since these original descriptions of theneck-tongue syndrome, a few other caseshave been described. Lance4 briefly mentionsa further four patients in whom the syndromestarted in late childhood or adolescence.Elisevich et all reported a 53-year-old womanwith assimilation of the atlas to the occiputpresenting with neck pain and ipsilateralparaesthesiae of the tongue on head turning,in whom the symptoms became persistentand incapacitating. At operation, the C2spinal. nerves were found to be compressed bya protuberant atlantoaxial joint. Resection ofthe superficial parts of the C2 spinal nervesled to partial relief.Webb et a16 described three cases with ipsi-
lateral neck pain and tongue numbness pre-cipitated by neck movement, first developingsymptoms at ages of 10 to 61 years. Degen-erative changes of the anterior atlantoaxialjoint were present in two of the cases.Restriction of neck movement, including useof a surgical collar in two of the cases, con-trolled the symptoms.
Fortin and Biller7 described a 57-year-oldwoman with repeated episodes of numbnessof the posterior right half of the tongue andright posterolateral oropharynx, an ipsilateral"ear pressure", and a sharp aching pain radi-ating along the border of the trapezius to theacromioclavicular joint. At the same time shenoticed a pressure sensation in the occiputand paraesthesiae in the fourth and fifth fin-gers of the right hand. The episodes lastedone minute, and she herself noted no clearprecipitant, but they were precipitated byextreme lateral rotation of the neck. Theregion of the atlantoaxial joint was normalradiologically. They also described a 29-year-old man, with previous head injury and lowerthoracic vertebral compression fracture after amotorcycle accident, who complained ofmainly right, but sometimes left sided (neverboth sides simultaneously), hemiglossal andfacial paraethesiae, sharp occipital pain shoot-ing to the periorbital area, dysarthria, nasal
348 on 8 S
eptember 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.3.348 on 1 M
arch 1994. Dow
nloaded from

The neck-tongue syndrome
congestion, sialorrhoea, and paraesthesiae inthe ulnar distribution of the upper limb. Thesymptoms in both patients were relieved byuse of a surgical collar.
Bertoft and Westerberg8 reported a furthersix patients with a complete syndrome, andthree with an incomplete syndrome, whichthey define as having characteristic attacks,but lacking the paroxysmal numbness of thetongue. We have not included these cases ofan incomplete syndrome in the present dis-cussion, but two of the patients with a com-plete syndrome had radiological evidence ofarthritis of the lateral atlantoaxial joints, andin one the symptoms were abolished aftersurgical atlantoaxial fusion.
Cassidy et a19 described three patients withthe neck-tongue syndrome, who were suc-cessfully treated with rotational manipulationof the cervical spine. Terrett et al'° describedeight cases of the neck-tongue syndrome,which were treated with spinal manipulativetherapy. They also referred to an additional54-year-old woman with headaches, who,after cervical manipulation, developed leftsided tongue numbness, persisting for twoyears, together with an intermittentdysarthria. Hankey" described a moreclassical neck-tongue syndrome in, a 14-year-old girl with recurrent episodes of unilateralupper nuchal pain radiating to the ipsilateralside of the tongue on ipsilateral rotation ofthe neck.Noda and Umezaki"2 described a 35-year-
old woman with paroxysmal episodes, lastingup to one minute, of numbness of the leftneck and occiput, with simultaneous numb-ness of the left half of the tongue, precededby tonic spasm of the left arm. They suggestthis is a component of a spinal tonic seizurerelated to an upper cervical inflammatorymyelopathy involving the dorsal funiculus,proximal to the C2 and C3 dorsal root gan-glia, and hence a spinal neck-tongue syn-drome.
In total, 36 cases of this syndrome havebeen previously described in the literature,some very briefly,48 although Bogduk13 com-ments that on discussion with other neurolo-gists and neurosurgeons it seems that thesyndrome is not rare. Accordingly wedescribe two further cases of the syndrome,due in one case to atlantoaxial osteoarthritis,and in the other to a traumatic fracture anddisplacement of the occipital condyle. A strik-ing feature was dysarthria and, in the secondcase, pseudoathetosis of the tongue.
PatientsCASE 1A 51-year-old woman complained of a pro-gressive stiffness and pain in the neck for sixyears. Three years previously she had noticedthat the pain was exacerbated by movementof the neck to a critical position, with the chindown and to the right. She was aware of agrating sensation in the neck, and the painappeared to be deep to the angle of the jawon the left, radiating to the occiput. These
exacerbations were associated with a tinglingsensation of the left side of the tongue, and asensation of the tongue being pulled into theback of the throat on the left, causing a feel-ing of choking, with difficulty speaking.
Neurological examination was normal, andin particular touch and pin prick sensation onboth sides of the tongue was preserved. Thetongue and palate appeared normal, with nor-mal movement. Cervical spine movement wasseverely limited due to pain.A cervical spine radiograph showed degen-
erative changes in the mid and lower cervicalspine, with rotation at the atlantoaxial joint,but no horizontal subluxation. A cervicalspine CT scan with the head turned to theright and left showed no structural lesion orabnormal movement. Rotatory movementwas equal to the right and left, with no dislo-cation of the lateral atlantoaxial joint. Therotation was about 40 degrees on each side, alittle more than usually seen, but probablynot pathological. A radioisotope bone scan,however, revealed increased uptake in the leftatlantoaxial joint, attributed to osteoarthritis.Injection of a local anaesthetic and steroidinto this joint led to brief relief of the pain.
CASE 2A 32-year-old woman accidentally fell down affight of 12 stairs at night, hitting the rightfrontoparietal region of her head against atable. This caused a scalp laceration but noloss of consciousness or immediately appar-ent neurological deficit. The next day sheawoke with a continuous right sided occipitalheadache and neck pain exacerbated byattempts at neck movement. She had slurringof speech, continuous altered sensation of thetongue and pharynx on the right with a feel-ing of the tongue moving to the left, and diffi-culty manipulating food in the mouth.On examination she had tenderness over
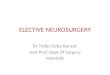
the upper cervical spine, and neck move-ments were severely restricted by pain. Thetongue was rotated anticlockwise in themouth, with consequent appearance ofdecreased bulk of the left side of the tongue(fig A). On forward protrusion of the tonguethere was equal bulk of the two sides, butgreat difficulty in maintaining a sustainedsteady forward position, the tongue movinginvoluntarily to right and left (fig B). Therewere no visible fasciculations. There was fullmovement of the tongue to the left (fig C)despite partial denervation of the right half ofthe tongue demonstrated by EMG. Tongueprotrusion to the right was incomplete andpoorly sustained although no weakness of theleft half of the tongue could be detected(fig D). On fibreoptic endoscopy the base ofthe tongue was more posterior than usual,and partially obstructing the larynx. She hada mild lingual dysarthria. Sensation of thetongue and pharynx to touch, taste, and pinprick was normal. Neurological examinationwas otherwise normal.
Cervical spine radiography was normal. Anupper cervical CT scan was normal, but a CTscan of the skull base showed a fracture of the
349
on 8 Septem
ber 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.3.348 on 1 March 1994. D
ownloaded from

Orrell, Marsden... .sS _ii wss ? ;,A >,t,_¢ ......... ........................ . o vS ..' .... _" _ '.F ti .. Sa .. _ _ . ''._ ........... ..tw' . .,. ' . ' ..... :_sx >, ., ., ,, .m AF , Dst z J tW' Ei T. '' ; i
J. .;S4Rp jl_ ._, uSSel-.E#s. jjfi r.-... _,8., . ... J , ,. _ Z ,:':' jr ,j':
ffi .... '' ,S.,
< s er iS i£ fisl.'S i .: '''0., ... o'' . '>. -" +'i_i i+ K.- ;. |F .............. . W%,,.
.. _ ?5'. '.A / .............................................. . - .... : 1 ':>:' ' ..C .S v j D ... '' :.Movement of the tongue in case 2; postures A,B,C, andD as described in the text.
right occipital condyle, with slight medial dis-placement of the fragment just distal to theright hypoglossal canal.
DiscussionThe clinical spectrum of the neck-tongue syn-drome, including age at presentation,chronicity, and disablement, has broadenedsince the original description. The twopatients we describe had a feeling of abnor-mal posturing or movement of the tongue asa significant feature of their symptomatology.In case 2 the positioning of the tongue wasclearly abnormal and she was unable to main-tain a sustained normal posture of the tonguein the absence of any specific weakness. Inparticular there was no weakness of tonguemovement to the left, which would beaffected by motor denervation of the rightside of the tongue. We propose that this is aresult of proprioceptive deafferentation of thetongue, with the clinical sign of lingualpseudoathetosis. This is similar to pseudo-athetosis as previously described in thelimbs.14 Pseudoathetoid movements of thetongue seem particularly complex in theabsence of any restriction of direction ofmovement imposed by a joint. The associateddysarthria has features of both impaired lin-gual control and pharyngeal obstruction asmanifestations of lingual pseudoathetosis pre-dominantly of the tip and base respectively.
Proprioception in the tongue has beenstudied in animals and humans,"5 with con-troversy initially concerning whether thetongue musculature has proprioception. As ageneralisation, it seems that muscle spindlesare not found in the tongue of mammals,except in moles, primates, and humans.16Muscle spindles have been demonstrated his-tologically in the human tongue.'7 18 Theafferent pathways seem to be in the hypoglos-sal nerve,'6 19 which is otherwise thought of asbeing a purely motor nerve.
Lingual pseudoathetosis is suggested in
previous descriptions of neck-tongue syn-drome. A 15-year-old boy had a right occipi-tal pain and numbness of the right side of thetongue on sudden neck rotation, and a feelingthat the tongue was twisted sideways in hismouth.' The symptoms lasted a few secondsonly. A 29-year-old man had ipsilateral occip-ital pain and tingling in his tongue, withdysarthria and nasal congestion, precipitatedby neck movement.7 A 60-year-old man, withsymptoms since the age of 10 years, hadexperienced a sensation of his tongue beingtwisted sideways in the mouth during anattack, "as though the whole tongue is cleav-ing to the roof of the mouth".4 A 19-year-oldwoman with pain in the left side of the neckon sudden head turning also noticed devia-tion of her tongue to the right for 10 seconds,with anarthria.4 A 33-year-old womandescribed paralysis of her tongue for aboutfive seconds on sharp rotation of the neck.'0 A19-year-old woman described her tongue asseeming to take up all the room in her mouth,having a mind of its own, being uncontrol-lable, and resulting in dysarthria.'0 A 46-year-old man experienced the symptoms of theneck-tongue syndrome, his tongue beingnumb and rigid, with dysarthria.10 A 26-year-old woman experienced the neck-tongue syn-drome, with an inability to move hertongue.'0 In these cases the dysarthria, as incase 2, may be related to proprioceptive deaf-ferentation rather than a primary motordeficit.A 53-year-old woman had pain in the right
side of her neck and tingling of the ipsilateralside of her tongue, initially intermittent butthen constant. This was aggravated by headturning and talking, and when severe the painradiated to the back of her head or right armand caused mild dysphagia related to a feelingof muscle spasm in the throat.5 A 34-year-oldman complained of intermittent left sidedneck pain radiating to the occiput, with ipsi-lateral aching and numbers of the tongue.The symptoms were precipitated by rapid
350
on 8 Septem
ber 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.3.348 on 1 March 1994. D
ownloaded from

The neck-tongue syndrome
neck flexion and rotation to either side whenbreathing during competitive free-style swim-ming. Occasionally the symptoms were sointense and associated with a choking sensa-tion that he had to stop swimming during arace. (He had experienced the same symp-toms while swimming between the ages of 10and 22 years).6Most reported cases have had transient
symptoms and signs, but in case 2 these wereconstant, enabling the tongue posture andmovement to be observed. The tongueseemed to be drawn back in the mouth, com-patible with the symptom described in case 1,and possibly explaining the muscle spasm inthe throat of the 53-year-old woman5 and 34-year-old swimmer.6Of the cases of the neck-tongue syndrome
previously described, four involved abnormal-ities at the atlantoaxial joints, two fusion ofthe atlas to the occiput, and another a minorabnormality of the occipital condylarprocesses. A cervical disc lesion was noted inanother. In the other cases no clear pathologyof the upper cervical joints was noted(although in one an intrinsic myelopathy wassuggested). In case 1 the structural abnormal-ity was osteoarthritis at the left atlantoaxialjoint demonstrated by radioisotope bonescan. Irregular loss of the left lateralatlantoaxial joint space with reactive sclerosisand osteophytic lipping was noted in a 36-year-old man,6 and moderate degenerativechanges at the anterior atlantoaxial joint in a65-year-old woman.6
Another possible example of the conditionwas described by Lees et al20 as "paroxysmalhemiglossal twisting". These authors reportedtwo patients, and tentatively suggested dysto-nia or tonic seizure as the cause. The firstcase was a 61-year-old woman who, onreview of the original records, described a tin-gling sensation at the back of the tongue onthe left, the tongue then deviated to the right,and she was unable to move her tongue to theleft, associated with dysarthria. On otheroccasions the tongue twisted from side toside, and she had bitten the left side of hertongue several times. Touch sensation of thetongue was normal during an episode. Shehad repeated episodes, lasting for about oneminute, which were infrequent, with no clearprecipitating neck movement, but appearedto be related to exercise. The attacks could beassociated with discomfort down the left sideof the neck and behind the left ear. A cervicalspine radiograph showed no abnormality ofthe upper cervical region, and CT scan of theatlantoaxial joint was normal. Except for theabsence of precipitation by neck movement,this case has features in common with theneck-tongue syndrome, and the abnormaltwisting of the tongue may be a lingualpseudoathetosis due to lingual proprioceptivedeafferentation, with associated C2 pain.(The second patient had brief spontaneousattacks of tongue twisting and dysarthriawithout pain or paraesthesiae).
In case 1, the site of deafferentation isassumed to be in the neck, related to the
atlantoaxial joint. In case 2, the site of deaf-ferentation is uncertain, and could be at theatlantoaxial joint related to the fall and twist-ing of the neck, related to the displacedoccipital condyle and abnormal atlanto-occipital joint, or in the hypoglossal nerveafter exit from the hypoglossal canal relatedto the displaced bone fragment. Previousabnormalities of the atlanto-occipital jointwere described in a 26-year-old man withanteromedial bosses of bone on the condylarprocesses of the occiput representing a minoranomaly of the occipital assimilation.' Thespinous processes of the atlas were fused tothe adjoining occipital bones in a 15-year-oldgirl,' and assimilation of the atlas to theocciput was noted in a 53-year-old woman.5Thus of the 38 cases now described,
pathology of the occipitoatlantoaxial jointshas been noted in 10.The onset of symptoms in case 2 was
clearly related to trauma, as were 10 previouscases. A 29-year-old man had a motorcycleaccident, with head and thoracic spine injury,two years before developing the neck-tonguesyndrome.7 A 26-year-old man was hit in themidfrontal region by a child's swing, with lac-eration of the forehead. Shortly afterwards hedeveloped numbness and weakness of theright hand lasting for several days. Ever sincehe has had transient symptoms of numbnessof the right side of the tongue and rightfourth and fifth fingers, and right sided neckpain, lasting a few seconds only, on suddenrotation of the neck.' A 36-year-old man acci-dentally jarred his neck, and subsequently,whenever jolted unexpectedly, experiencedhigh cervical pain radiating to the left side ofhis tongue "like the aftermath of a dentalanaesthetic".6 A 28-year-old woman devel-oped the neck-tongue syndrome the day aftera whiplash injury, which persisted for oneyear, but resolved with spinal manipulation.9Other cases associated with trauma includefour after a motor vehicle collision, and onedeveloping eight years after a water skiingaccident.10The transient relief of the symptoms in
case 1 by injection of local anaesthetic andsteroid into the lateral atlantoaxial joint issupportive of the symptoms being related tothis joint, and raises the possibility of treat-ment by permanent cervical fusion.Previously reported surgery with bilateralresection of C2 spinal nerves with their dorsaland ventral rami, initially relieved the symp-toms, but after one week there was a recur-rence of mild tingling sensations in thetongue when the patient was tired. The neckpain also recurred, but less severely thanbefore the operation. The authors suggestedthat the recurrence of tongue symptomscould be explained by facilitation of residualproprioceptive fibres in the adjacent unin-jured spinal roots. In another patient, surgicalatlantoaxial fusion abolished the symptoms.8Other patients have had their symptomsrelieved by spinal manipulation.910 Symptomshave been improved by preventing the precip-itative neck movement with a surgical collar,
351 on 8 S
eptember 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.3.348 on 1 M
arch 1994. Dow
nloaded from

Onrell, Marsden
but the benefit is not necessarily permanent,and with no long term follow up of this syn-drome the natural history is unclear.
Since the initial description by Lance andAnthony' of patients aged 15 to 26 years,with an onset age of eight to 15 years, it hasbecome apparent that the same syndromemay present up to at least the age of 61 years,and may present as transient symptoms whichmay persist, may resolve and relapse, or maybecome permanent and present as a perma-nent deficit. In a significant proportion thereis pathology at the atlantoaxial and atlanto-occipital joints, and in some cases the syn-drome may result from trauma.
We thank Professor A E Harding for permission to includedetails of the patient under her care.
1 Lance JW, Anthony M. Neck-tongue syndrome on sud-den turning of the head. J7 Neurol Neurosurg Psychiatry1980;43:97-101.
2 Cyriax J. Textbook of orthopaedic medicine. 4th ed. Vol 1.London: Cassell, 1962:158.
3 Bogduk N. An anatomical basis for the neck-tongue syn-drome. J Neurol Neurosurg Psychiatry 198 1;44:202-8.
4 Lance JW. Unusual syndromes in neurological practice.MedJAust 1984;140:409-16.
5 Elisevich K, Stratford J, Bray G, Finlayson M. Neck-tongue syndrome: operative management. J NeurolNeurosurg Psychiatry 1984;47:407-9.
6 Webb J, March L, Tyndall A. The neck-tongue syndrome:occurrence with cervical arthritis as well as normals.J Rheumatol 1984;11:530-3.
7 Fortin CJ, Biller J. Neck-tongue syndrome. Headache1985;25:255-8.
8 Bertoft ES, Westerberg CE. Further observations onthe neck-tongue syndrome. Cephalgia 1985;5(suppl 3):312-3.
9 Cassidy JD, Diakow PRP, De Korompay VL, Munkacsi I,Yong-Hing K. Treatment of neck-tongue syndrome byspinal manipulation: a report of three cases. The PainClinic 1986;1:41-6.
10 Terrett AGJ. Neck-tongue syndrome and spinal manipu-lative therapy. In: Vernon H, ed. Upper cervical syn-drome: chiropractic diagnosis and treatment. Baltimore:WiHiams and Wilkins, 1988:223-9.
11 Hankey GJ. "Neck-tongue" syndrome on sudden neckrotation. AustNZJ Med 1988;18:181.
12 Noda SN, Umezaki H. Spinal neck-tongue syndrome.J Neurol Neurosurg Psychiatry 1984;47:75 1.
13 Bogduk N. Neck-tongue syndrome. Med,JAust 1980;2:4.14 Liversedge LA. Involuntary movements. In: Vinken PJ,
Bruyn GW, eds. Handbook of clinical neurology. Vol 1.Amsterdam: North-Holland, 1969:277-292.
15 Tier GA, Rees RT, Rood JP. The sensory nerve supply tothe tongue: a clinical reappraisal. Br Dent Jf 1984;157:354-7.
16 Kubota K, Narita N, Takada K, et al. Origin of lingualproprioceptive afferents in Japanese monkey, M fuscatafuscata. Studied by HRP-labelling technique. Anat Anz1988;166: 141-8.
17 Cooper S. Muscle spindles in the intrinsic muscles of thehuman tongue. J Physiol (Lond) 1953;122:193-202.
18 Kubota K, Negishi T, Masegi T. Topological distributionof muscle spindles in the human tongue and its signifi-cance in proprioception. Bull Tokyo Med Dent Univ1975;22:235-42.
19 Adatia AK, Gehring EN. Proprioceptive innervation ofthe tongue. JAnat 1971;110:215-20.
20 Lees AJ, Blau JN, Schon F. Paroxysmal hemiglossal twist-ing. Lancet 1986;ii:812-3.
352
on 8 Septem
ber 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.3.348 on 1 March 1994. D
ownloaded from