Embed Size (px)
Citation preview

NEUROSCIENCE, TRAUMA &
RELATIONSHIP Tanager Place Conference
May 2018
Randall R. Lyle, Ph.D.
Mount Mercy University

“Changes in the organization
of brain function, emotional
regulation, and long-term
memory are mediated by
alterations in neural structure.
These structural changes are
due to the activation or
deactivation of genes encoding
information for protein
synthesis. Experience, gene
expression, mental activity,
behavior, and continued
interactions with the
environment (experience) are
tightly linked in a
transactional set of processes.
Such is the recursive nature of
development and the way in
which nature and nurture,
genes and experience, are
inextricably part of the same
process. (Dan Siegel)

MEMORY IMPLICIT, EXPLICIT, NARRATIVE

ATTACHMENT
Implicit Memory
No thought/All Emotion
Develops as the brain develops
therefore not accessible to
thought
Created by
attachment/distorted by failure
to attach

Attachment establishes an interpersonal relationship that helps the immature
brain use the mature functions of the parent’s brain to organize its own
processes.

The emotional transactions of secure
attachment involve a parent’s
emotionally sensitive responses to a
child’s signals, which can serve to
amplify the child’s positive emotional
states and to modulate negative
states. In particular, the aid parents
can give in reducing uncomfortable
emotions, such as fear, anxiety, or
sadness, enables children to be
soothed and gives them a haven of
safety when they are upset. Repeated
experiences become encoded in
implicit memory as expectations and
then as mental models or schemata of
attachment.



PLASTICITY
Old idea: The best you could
ever be at birth/downhill from
then on.
New idea: Never stops
changing/change can be good
or ill depending…

“Resilience is the dynamic
process through which an
individual can adaptively
overcome a stressful and/or
traumatic event(s), while
maintaining relatively normal
physical and psychological
function over time.” C. Osorio et
al
“It is important to mention that
resilience is not conceptualized
as the absence of a diagnosable
psychiatric condition but rather
a constructive adaptation to
adversity and traumatic
experience.”
“The neural mechanisms that
underlie resilience to stress are
extremely complex, involving
the interaction of neurobiologic,
genetic, and epigenetic
components, together with the
environment.”
“It should be noted that
active coping strategies,
humor, hardiness, and
extraversion can promote
resilience through fostering
feelings of mastery,
commitment, and competence
as well as the ability to help
others through bonding.”

Studies that evaluated
parental neglect and abusive
behavior toward children
during the early weeks of life
found: fewer stress
management skills, lower self-
independence, and higher
levels of anxiety and stress.
Statistically, the more
stressful and/or adverse
experiences someone
encounters in childhood, the
higher his or her risk of
developing cognitive,
emotional, and psychiatric
problems in adulthood.

CORE NEED SURVIVAL ADAPTATION STRATEGY USED TO PROTECT THE ATTACHMENT RELATIONSHIP
Connection Foreclosing connection Disconnect from body and social engagement
Children give up their very sense of existence, disconnect, and attempt to become invisible
Attunement Foreclosing the awareness and expression of personal needs
Children give up their own needs in order to focus on the needs of others, particularly the needs of the parents
Trust Foreclosing trust and healthy interdependence
Children give up their authenticity in order to be who the parents want them to be: best friend, sports star, confidante, etc.
Autonomy Foreclosing authentic expression, responding with what they think is expected of them
Children give up direct expressions of independence in order not to feel abandoned or crushed
Love-Sexuality Foreclosing love and heart connection Foreclosing sexuality Foreclosing integration of love with sexuality
Children try to avoid rejection by perfecting themselves, hoping that they can win love through looks or performance
Heller & LaPierre 2012

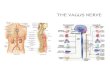
Stephen Porges’ Poly Vagal Model

Neuroception is a term coined by Stephen Porges to describe
how neural circuits distinguish whether a situation is safe,
threatening, or dangerous. It is an ongoing process through
which our autonomic nervous system evaluates information
from our senses about our environment and the state of our
body.
Neuroception takes place in the deep parts of the brain,
beyond our conscious awareness. It can be likened to a good
watchdog that is always on guard, allowing us to focus on
things other than survival, or to sleep soundly, and rousing
us only when intrusions could compromise our survival.
Based on neuroception, well-defined neural circuits are
activated to support the state of social engagement and
friendly behaviors when we are safe; the defensive strategies
of fight or flight when we are threatened; and shutdown
when we are in serious danger.

Descartes—I think therefore I
am. The so-called Cartesian
error was to separate the brain
from the body. Mind—
thinking, became the highest
accomplishment of the human.
Soma/body—has been
relegated to the domain of
allopathic medicine and the
closed interventions of
medication or surgery.
The polyvagal theory regarding
the function of the vagus
systems encourages us to
reunite the two and remember
that we are one.
Somatic Treatment
You cannot heal trauma by
words alone!

Interoception:
The perception of internal (endogenous)
sensations that contribute to our subjective
experience of body state.
Or
The only thing determining whether
something is interoceptive is whether it
contributes to the subjective perception of
body state.

Provides a significant portion
of the information we use to
form our experience of self
and our view of the self in
relation to others. It provides
a large portion of the self-
communication we use to
assess whether or not we are
safe or unsafe and whether an
external event or person is
pleasurable, exciting, or
threatening.
Interoception can be easily
influenced, including by
something as simple as our
mood when we are asked to rate
our pain levels: positive emotion
increases our tolerance for pain,
and negative emotion decreases
it.
Is meant to inform us in a predictive
assessment of our internal and
external environments, but it can
mislead us if this system developed
without congruent context and
feedback, in which case, our markers
for perception and meaning making
may be overly sensitive or tuned to
signals that don’t provide reliable
information.
Information gathered tend to
be experienced as factual, not
evaluative, because it comes
from what many of us call
“inner knowing” or gut feeling.


Treatment Strategies:
1. Understand the impact early trauma has, so that we can assess
their needs in the necessary context. Symptoms related to all
aspects of the self should be taken into account: psychological,
emotional, physiological, social, and spiritual.
2. Assess the client’s capacity for regulation, perception of safety, and
assessment of affiliated somatic symptoms. It is important to assess
where the client falls in his/her preexisting capacity for self-
regulation.
3. Regulation, regulation, regulation. Attention to supporting the
client’s capacity for regulation will always be a part of any
interventions when working with developmental trauma. This may
take months or even years.
4. Pay attention to defensive accommodations and the false coping
skills.
5. Support more accurate interoception. More accurate interoception is
a critical element in the client’s ability to notice their increasing
capacity for regulation, to access a felt sense of safety, to notice co-
regulation, and to more accurately notice internal experiences—and
report those to the clinician.

6. Change the narrative. This often happens simultaneously with the
previous two steps. Sometimes clients will need coaching to perceive the
differences in how they attend to their experiences, and the ways in
which various aspects of their narrative are changing.
7. Remain focused on regulation. As the work progresses, there is often
a stage when it’s time to return attention more fully to regulation.
Because the client has greater access to their ventral parasympathetic
physiology, is more able to track their internal experiences, and has a
more developed sense of safety, their capacity for regulation has often
grown to the point that returning to this focus can help consolidate the
gains made.
8. Work with more specific symptoms.

Neuromodulation:
These are techniques associated with computer (device) biological
connections enabling the individual to gain knowledge and control
of autonomic regulation or other means of changing brain function.
Neurofeedback
Peripheral biofeedback
HRV (Heart Rate Variability Training)
Pemf training
PirHeg (Passive Infrared Hemoencephalography)
tDCS (Transcranial Direct Current Stimulation)
EMDR
Mindfulness

Touch

“Failure of the holding environment is experienced as failure of
the self. Infants who experience early trauma of any kind
experience the early environmental failure as if there were
something wrong with them. Later cognitions such as ‘There is
something basically wrong with me’ or ‘I am bad’ are built upon
the early somatic sensation ‘I feel bad.’”
“When children split off
significant aggressive
impulses, they see only two
possibilities: to identify as
good but powerless—acting
in—or as bad but powerful—
acting out.”
“Designated issues, whether or
not they have a basis in physical
reality, come to dominate a
person’s life, covering the deeper
distress and masking the
underlying core disconnection.”
Heller & LaPierre 2012.

Interventions such as Theraplay
where touch is often used as a
means of facilitating attachment,
connection, and security are
increasingly understood to be
essential elements of resolving and
regulating the individuals ability to
heal.

The Somatic Experiencing® method is a body-oriented approach to
the healing of trauma and other stress disorders. It is the life’s
work of Dr. Peter A. Levine, resulting from his multidisciplinary
study of stress physiology, psychology, ethology, biology,
neuroscience, indigenous healing practices, and medical biophysics,
together with over 45 years of successful clinical application. The
SE approach releases traumatic shock, which is key to
transforming PTSD and the wounds of emotional and early
developmental attachment trauma.
Offers a framework to assess where a person is “stuck” in the fight,
flight or freeze responses and provides clinical tools to resolve
these fixated physiological states. It provides effective skills
appropriate to a variety of healing professions including mental
health, medicine, physical and occupational therapies, bodywork,
addiction treatment, first response, education, and others.

Implicit memory, the
roots of our existence,
resides in the body.
Romania taught us that
if you feed and clean
them but don’t hold
them they will die.
Resiliency without the
body is not resiliency.
We cannot self-regulate
if we are not in touch
with our bodies.

Take aways:
In order to develop resiliency there must be struggle.
The struggle must be accompanied by support
(physical as well as emotional), compassion (suffering
with), mentoring (education of mind, body and spirit).
The silent child (adult), the yelling child (adult), the
hitting child (adult) are likely to all be asking for the
same thing.
The caregiver (healer, therapist, counselor, etc.)
probably cannot give what they do not have.

Will you see me? touch me? feel me? know me? hold me? love me?



The best treatment of all is happiness and love and joy!

Nurturing Resilience: Helping Clients Move Forward frpom
Developmental Trauma. Kain & Terrell 2018, North Atlantic
Books
Accessing the Healing Power of the Vagus Nerve: Self-Help
Exercises for Anxiety, Depression, Trauma, and Autism.
Rosenberg. 2017. North Atlantic Books.
Healing Developmental Trauma: How Early Trauma Affects
Self-Regulation, Self-Image, and the Capacity for Relationship.
Heller & LaPierre. 2012. North Atlantic Books.