Embed Size (px)
DESCRIPTION
act as ghostwriter for the neurosurgeons on this newsletter, interviewing physicians then conducting medical research and writing. Audience is primary care physicians and other referring medical personnel.
Citation preview
Vol. 2, No. 4 n Fall 2011
INSIDE
2 New research into migraines
4 Treating movement disorders with deep brain stimulation
5 Briefs
:: Littleton Hospital among nation’s best
:: Upcoming CME program
6 Meet our physicians
�� continued on Page 2
�� continued on Page 3
Neurostimulation: Offering hope for intractable chronic headachesBy Mariel Szapiel, MDNeurosurgeonSouth Denver Neurosurgery
Chronic daily headaches affect about 5% of Americans and account for a significant portion of primary care, neurology, and pain clinician patient
load. Fortunately, most headache patients respond to acute and preventive medications. In about 1% of patients, however, the headaches (typically migraine or cluster) remain resistant to medication, even the big gun of BOTOX®. (Jasper and Hayek 2008)
It might be time to consider peripheral neurostimulation for these patients. The actual procedure is relatively simple. A neurosurgeon places an electrode
under the skin in the suboccipital region. The electrode delivers mild electrical pulses to the occipital nerves that project to the trigeminocervical complex,
which is implicated in migraine and cluster headaches. The idea is that those electrical pulses will “break” the feedback loop of pain.
Neuromodulation comes of ageMariel Szapiel, MD, is the featured author of this issue of Neuroscience News. Dr. Szapiel recently joined South Denver Neurosurgery after completing a six-year specialized residency in neurosurgery at The Ohio State University Medical Center. Following her neurosurgery residency, Dr. Szapiel completed a one-year fellowship in functional neurosurgery under Ali R. Rezai, MD.
Dr. Szapiel grew up in Puerto Rico. She earned a bachelor’s degree in industrial microbiology and her medical degree at the University of Puerto Rico. She is fluent in Spanish and English.
Dr. Szapiel has concentrated her training and research in stereotactic and functional neurosurgery, including the emerging use of deep brain stimulation for a number of conditions, including Parkinson’s disease, essential tremor, Tourette’s syndrome, and mental health conditions such as obsessive-compulsive disorder and intractable depression.
Q What is functional neurosurgery, and why have you chosen to specialize in this area?
Functional neurosurgery, or neuromodulation, focuses on surgical interventions for chronic conditions involving abnormal brain activity. What’s new and exciting is that we can now treat a patient and then continue to adjust or modify the treatment as needed if symptoms change. Much of what neurosurgeons do happens once and you’re done. The beauty
Dr. Mariel Szapiel
Phot
o: h
EADA
ChE:
©iS
toCk
Phot
o.Co
m/ F
EvEr
PitC
hED
2 Neuroscience News | Fall 2011
Neurostimulation from page 1
The procedure has been evaluated in patients with occipital neuralgia, migraine, transformed migraine, chronic daily headaches, cervicogenic headaches, and cluster headaches. (Schwedt 2009) A review of 13 articles (controlled and observational studies) on nerve stimulation conducted in 150 patients who had intractable, frequent, and intense headaches for more than six months concluded an “overwhelmingly positive” response.(Jasper and Hayek 2008)
Fish originsThe concept dates back centuries, when early physicians inserted a bioelectric fish to short-circuit neural pathways related to pain (they didn’t know about the pathways, of course, just that the fish worked).
But the use of an electrical current for pain and other neurological conditions really came into its own in the 1970s and 1980s – with the use of vagal nerve stimulation for intractable epilepsy and deep brain stimulation for intractable pain. (Jenkins B, Tepper SJ; 2011)
Occipital nerve stimulation, the most common type of peripheral neurostimulation used for chronic headaches, was first tried in 1977. However, research into the procedure didn’t take off until 1999. That’s when the first report of its use to successfully treat occipital
neuralgia was published. (Weiner R, Reed K; 1999).
With occipital nerve stimulation, neurosurgeons implant the electrode on the occipital nerves in the suboccipital area. Most patients receive continuous stimulation from the probe, although intermittent stimulation is sometimes used. (Jenkins B, Tepper SJ; 2011) They get a remote control to adjust the intensity of the pulses.
Physicians believe the implant works by stimulating large nerve fibers, which have an inhibitory effect on the small-diameter nociceptive fibers that transmit pain signals. (Schwedt 2009) In addition, the stimulation affects the entire central nervous system, impacting other parts of the trigeminal nerve pathway that are implicated in these headaches.
Minimal riskThe first results of randomized, placebo-controlled studies are just being published (see accompanying box), but numerous case reports have been published in the past decade showing significant benefit with low associated risks. The primary safety concerns are lead displacement (21% overall, higher with certain leads), battery failure (less common with rechargeable batteries), and infection (4.6%).(Jasper and Hayek 2008)
Latest researchOccipital nerve stimulation has been used for more than 10 years to treat intractable chronic headaches. However, only more recently have quality, randomized, double-blind clinical trials been published.
In September, European authorities approved the Genesis neurostimulation system from St. Jude Medical to treat intractable chronic migraines. The system, used in the United States in spinal cord stimulation for chronic back, limb, and trunk pain, is the first such device to be approved specifically for headache pain.
The approval was based on a randomized, double-blind, placebo-controlled study in 157 patients with serious, recurring migraines. After 12 weeks, patients receiving the device reported seven fewer headache days a month as measured by the MIDAS questionnaire, compared to one fewer headache a month in the control group. Patients also had a 41% improvement in overall disability, compared with a 13% improvement in the control group.
After one year, 65% of patients who received the device reported excellent or good pain relief; 68% said their quality of life had improved; and 67% were satisfied or very satisfied with the results.
Results of the study were presented at the International Headache Congress in June 2011 and will be published in early 2012. The company is still evaluating its options in the U.S., where the Food and Drug Administration requested data demonstrating a higher migraine control rate.
Another manufacturer-sponsored trial, the Occipital Nerve Stimulation for the Treatment of Intractable Migraine (ONSTIM) was designed to evaluate Medtronic’s Synergy IPG for chronic migraines. Preliminary efficacy and safety data on 66 of 75 patients in the treatment group published earlier this year found that 39% of patients responded to adjustable stimulation, 6% to preset stimulation, and none to medical management. The primary adverse effects were lead migration or dislodgement, and incision-site complications. (Saper J, Dodick DW, et al; 2011)
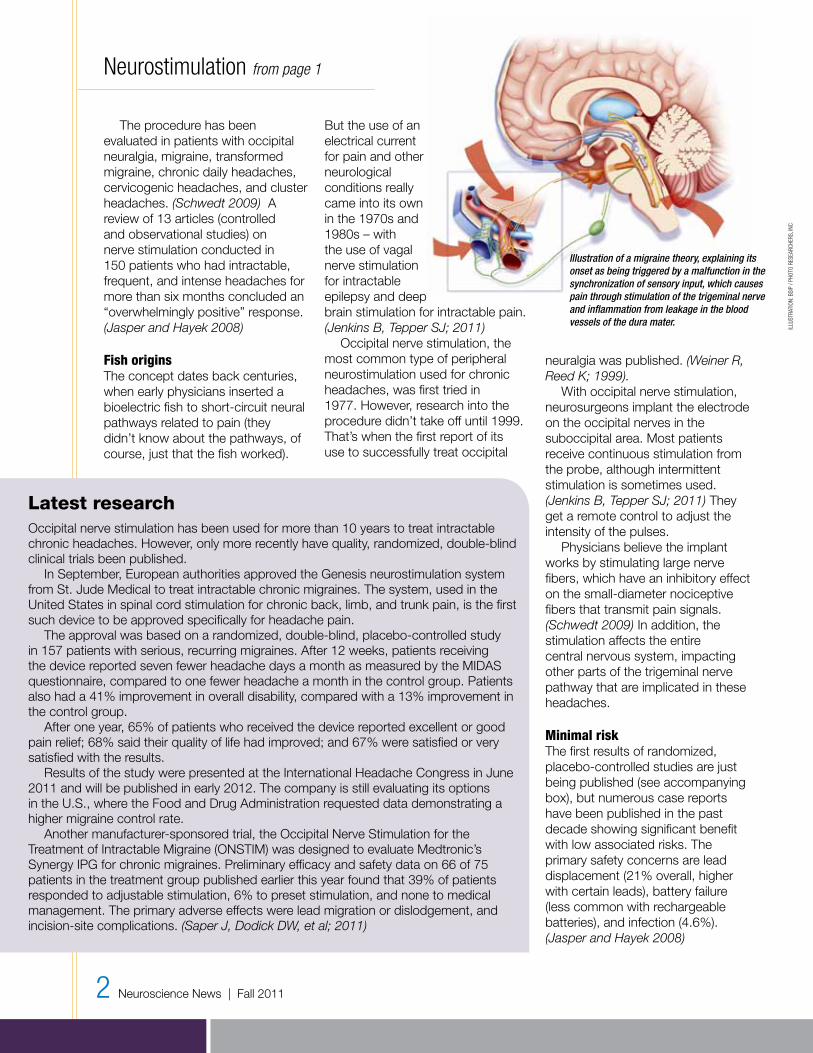
Illustration of a migraine theory, explaining its onset as being triggered by a malfunction in the synchronization of sensory input, which causespain through stimulation of the trigeminal nerve and inflammation from leakage in the blood vessels of the dura mater.
iLLU
StrA
tioN
: BSi
P / P
hoto
rES
EArC
hErS
, iNC

of neuromodulation is that we are able to help patients who have run out of options. We may not be able to cure them, but we can provide them with improved quality of life. That’s a very satisfying part of the job.
Q Can you give us an example of this?
You can really see this with patients with essential tremor. As their tremors worsen, they withdraw from society because they are embarrassed. We’re not talking about a shaky hand. These patients can’t hold a glass without spilling the contents, and they are often unable to take care of themselves. Brushing their teeth is a challenge – forget about shaving themselves, too dangerous. They become socially inhibited, eventually refusing to leave their homes. At work, they try to hide their tremors and end up withdrawing there as well.
Q What is your patient care philosophy?
It’s very important to build a team-oriented approach with each patient and his or her physicians. Our surgery provides only a part of the patient’s recovery. I partner with the patient’s neurologist, psychologist or psychiatrist,
neurophysiologist, and other physicians to create an integrated approach to care. I also need cooperation from the patient and the family. The treatment begins with surgical intervention. Following surgery, rehabilitation can further improve on the initial benefits of surgery. I am very honest and realistic with patients. I won’t promise something if it’s not reasonable.
Q What emerging developments in neuroscience excite you?
Until now, the stimulation of the nervous system has focused mainly on electrical stimulation from a one-sided perspective. That is, us controlling the stimulation in its entirety. In the future, technology will hopefully allow us to detect where and how the abnormal functioning in the brain is taking place and adjust itself according to the needs of that individual at the time. Stimulation hopefully will not only be achieved through pure electrical means but also at the biochemical level by altering specific levels of neurotransmitters in the brain.
Developments in brain-machine interface also are very exciting. This technology allows a patient with a spinal cord injury to move items – such as a mechanical arm – using his brain. The brain electrodes being developed for these technologies eventually can serve in other systems where brain feedback is needed to adjust stimulation.
To help increase the likelihood of benefit, the neurosurgeons at South Denver Neurosurgery require patients to undergo a one-week “trial” run with an external device. We want to make sure that they will experience at least some improvement before implanting the device. Even then, their pain may not be completely resolved. But given the severe disability these chronic headaches cause, we believe that the benefit of any improvement in pain and/or reduction in medication use outweighs the relatively rare
occurrence of serious complications from the procedure.
ReferencesJasper, J.F., and Hayek, S.M. 2008. Implanted occipital nerve stimulators. Pain Physician 11 (2): 187-197.
Jenkins B, Tepper SJ. Neurostimulation for primary headache disorders: part 2, review of central neurostimulators for primary headache, overall therapeutic efficacy, safety, cost, patient selection, and future research in headache neuromodulation. Headache. 2011.
Magis D, Gerardy PY, Remacle JM, et al. Sustained effectiveness of occipital nerve stimulation in drug-resistant chronic cluster headache. Headache. 2011;51(8):1191-1201.
Matharu MS, Bartsch T, Ward N, et al. Central neuromodulation in chronic migraine patients with suboccipital stimulators: A PET study. Brain. 2004;127(Pt 1):220-230.
Popeney CA, Alo KM. Peripheral neurostimulation for the treatment of chronic, disabling transformed migraine. Headache. 2003;43(4):369-375.
Saper JR, Dodick DW, Silberstein SD, et al. Occipital nerve stimulation for the treatment of intractable chronic migraine headache: ONSTIM feasibility study. Cephalalgia. 2011;31(3):271-285.
Schwedt TJ. Neurostimulation for primary headache disorders. Current Neurology and Neuroscience Reports. 2009;9(2):101-107.
Weiner R, Reed K. Peripheral neurostimulation for control of intractable occipital neuralgia. Neuromodulation. 1999; 2:217-221.
fast facts
Occipital nerve stimulationBest for: Patients with chronic occipital neuralgia, migraine and cluster headaches resistant to conventional pharmacologic therapy (including BOTOX®); the headaches should cause significant disability.
Pre-procedure workup: Includes a psychological evaluation to determine if the patient is a suitable candidate. If accepted, a “trial” is conducted with external stimulation for one week. If that is successful, the patient returns for permanent placement.
The procedure: The surgery is performed on a same-day, outpatient basis. The trial procedure is done under conscious sedation. The permanent implantation requires general anesthesia. Postsurgical discomfort is minimal and treated with oral pain medications.
Risks of procedure: The primary risks are immediate or later infection; lead migration or breakage; need for battery replacement; and paresthesias, or tingling, at the implantation site.
Other key points:• Not effective in every
patient• May not completely
eradicate all headaches, but should significantly reduce frequency and severity in properly selected candidates
• May take several months to reach maximum efficacy in cluster headache patients
Mariel Szapiel from page 1
iLLU
StrA
tioN
: BSi
P / P
hoto
rES
EArC
hErS
, iNC

By Mariel Szapiel, MDNeurosurgeonSouth Denver Neurosurgery
Essential tremor (ET) is considered by many to be the most prevalent adult-onset movement disorder, followed by Parkinson’s disease and primary dystonia. Both ET and dystonia are often unrecognized or misdiagnosed. Once identified, they’re likely to be managed by primary care clinicians and neurologists. (Louis and Ferreira 2010; Lyons and Pahwa 2008)
Both conditions have a significant impact on a patient’s quality of life. In the case of ET, worsening symptoms can significantly affect a patient’s quality of life, interfering with social activities, work, and lifestyle needs, including brushing teeth, shaving, and eating. As this occurs, many patients withdraw, which can result in depression and negatively impact health, particularly in older adults who are the most likely to be affected by ET.
While there are several medications available for ET, including beta-blockers, anticonvulsants, benzodiazepines, and BOTOX® injections, about half of patients prove resistant to medical treatment, and approximately 10% suffer from severe disability. (Zhang, Bhatia and Oh 2010; Blomstedt, Sandvik and Tisch 2010)
Dystonias cause intense, involuntary muscle spasms that lead to abnormal twisting and postures. These, in turn, can cause severe disability and pain. Medical treatment options for dystonias are limited. (Speelman, Contarino, Schuuman et al. 2010)
Deep brain stimulation (DBS) surgery is a reasonable option in ET and dystonia patients who have exhausted all conservative and medical treatment alternatives, and their condition is causing a significant negative impact on quality of life.
Long-term results The results of DBS for patients with essential tremor are excellent. One study found up to 80.1% improvement in tremor and 69% improvement in handwriting, with benefits still present up to seven years after implantation. In other reports, the improvements have ranged from 40% in overall tremor to 87% in upper extremity tremor. (Zhang, Bhatia and Oh 2010)
Another published report of 31 electrodes implanted in the left posterior subthalamic area in 21 patients found the best results occurred in the hands and arms, with a 95% improvement in the contralateral arm and 87% improvement in the hand seen at one year. The main side effect was some mild, temporary dysphasia in eight patients. There is also a risk of patient tolerance to the stimulation over time. (Blomstedt, Sandvik and Tisch 2010)
One of the few published reports of the long-term (mean five years) effects of DBS for 18 patients ages 18 to 78 with
primary dystonia found a mean improvement in the Burke-Fahn-Marsden (BFM) score used to assess generalized dystonia of 39% at three months, 42.5% at 12 months, and 46.8% at the long-term follow-up. Patients with focal/segmental dystonia demonstrated a mean reduction in the Tsui score of 36.8%, 65.1%, and 59.8%, for the same time periods. Two patients had a local infection, and one patient experienced an electrode dislocation and a broken extension cable. (Mehrkens, Botzel et al. 2009)
Overall, in the hands of an experienced neurosurgeon and with the appropriate patient preparation and postsurgical management, DBS can safely provide significant reductions in patients’ symptoms and improvements in their quality of life.
ReferencesBlomstedt P, Sandvik U, Tisch S. Deep brain stimulation in the posterior subthalamic area in the treatment of essential tremor. Movement Disorders 2010;25(10):1350-1356.
Louis ED, Ferreira JJ. How common is the most common adult movement disorder? Update on the worldwide prevalence of essential tremor. Movement Disorders 2010;25(5):534-541.
Lyons KE, Pahwa R. Deep brain stimulation and tremor. Neurotherapeutics. 2008;5(2):331-338.
Mehrkens JH, Botzel K, Steude U, et al. Long-term efficacy and safety of chronic globuspallidusinternus stimulation in different types of primary dystonia. Stereotactic and Functional Neurosurgery. 2009;87(1):8-17.
Speelman JD, Contarino MF, Schuurman PR, et al. Deep brain stimulation for dystonia: Patient selection and outcomes. European Journal of Neurology 2010; 17 (Suppl 1) 102-106.
Zhang K, Bhatia S, Oh MY, et al. Long-term results of thalamic deep brain stimulation for essential tremor. Journal of Neurosurgery 2010;112(6):1271-1276.
SouthDenverNeurosurgery.org | Neuroscience News 4
Deep brain stimulation for essential tremor and dystonia
fast facts
Deep brain stimulation for essential tremor and dystonia Best for: Patients with essential tremor and primary dystonia who are resistant to existing treatment.
Pre-procedure workup: We use a combination of CT and MRI scanning to preplan the surgery to ensure we operate around blood vessels.
The procedure: The surgery is performed in a three-step approach and requires an inpatient stay as well as pre- and postsurgical outpatient procedures.
Risks of procedure: The primary risks are local infection and mechanical issues with the implant; a rare risk is hemorrhagic stroke. Physicians at South Denver Neurosurgery have experienced no hemorrhagic strokes in more than 100 DBS patients over the past three years.
This lateral x-ray demonstrates two deep electrodes (blue lines) extending through frontal burr holes and extending into the cerebral hemispheres bilaterally for the treatment of movement disorders.
imAg
E Co
UrtE
Sy o
F m
EDiC
AL B
oDy
SCAN
S / P
hoto
rES
EArC
hErS
, iNC

5 Neuroscience News | Fall 2011
briefs
Littleton hospital named among nation’s bestHealthGrades, an independent hospital quality rating agency, has named Littleton Adventist Hospital one of America’s top 100 hospitals for coronary intervention procedures. The hospital was ranked No. 1 in Colorado in this category.
Littleton Hospital was specifically recognized for the following national achievements::: Recipient of the HealthGrades
Coronary Intervention Excellence Award for two years in a row (2011-2012)
:: Ranked among the top 5% in the nation for coronary interventional procedures in 2012
Littleton Hospital’s cardiac services provide comprehensive services from diagnosis to treatment of cardiovascular disease. The hospital’s team of cardiologists,
cardiac surgeons, and specially trained
cardiac care teams is dedicated to achieving the best outcomes possible for patients.
Littleton Hospital also received the Gold
Plus Recognition from the American Heart Association for the highest possible “Get With The Guidelines” achievement recognition for Stroke and Heart Failure. Littleton Hospital’s average door-to-balloon time for 2010 was 56 minutes, 34 minutes faster than the national average.
Littleton Hospital’s comprehen-sive cardiac services include:
:: cardiac alert program :: cardiac observation unit :: cardiac testing :: cardiovascular
catheterization lab :: nationally accredited chest
pain center
Five-star stroke careHealthGrades also awarded Littleton Hospital a five-star rating for treatment of stroke and rated the hospital one of America’s 100 Best for Pulmonary Care. Littleton Hospital’s Stroke Center was awarded the Gold Plus Performance Achievement Award from the American Stroke Association. This award recognizes achievement in using evidence-based guidelines to provide the best possible care to patients through the association’s “Get With The Guidelines” program.
Target stroke honor rollLittleton Hospital’s stroke program also was named on the Target Stroke Honor Roll by the American Heart Association/American Stroke Association. The criteria for Target
Stroke is to give IV TPA within 60 minutes more than 50% of the time (minimum of six patients treated). Collaboration between EMS, the emergency department, neurologists, CT, radiologists, and
pharmacy made this recognition possible.
Joint Commission accreditation
Littleton Hospital was among the first providers in
Colorado to be designated a Primary Stroke Center by the Joint Commission.
This title reflects the depth of
commitment to the program and patients. Littleton Hospital focuses on innovation and integration of best practices, professional expertise, emerging technology and the healing power of compassion.
Treatment of Stroke
Five-Star R ated
2012
CME: Deep brain stimulationSouth Denver Neurosurgery, in conjunction with Littleton Adventist Hospital, will be holding a continuing medical education program in May 2012 on Neuromodulation for Movement Disorder Patients. This accredited CME program is targeted at primary care physicians, neurologists, geriatricians, physiatrists, and any other providers who care for patients with chronic movement disorder diseases.
Neurosurgeons David Vansickle, MD, PhD, and Mariel Szapiel, MD, will present this program. Their discussion will include: Advancements in neuromodulation for movement disorders An in-depth review of deep brain stimulation:
+ The latest research into long-term efficacy
+ Patient selection criteria
+ Reducing risk, including techniques to reduce hemorraghic stroke, lead breakage, and postsurgical infections
Look for more information, including date and location, in the next issue of Neuroscience News or email [email protected] to receive an electronic invitation.
MAY

Meet our physicians
PRSRT STDU.S. Postage
PAIDDenver, CO
Permit No. 1818
7780 S. Broadway, Suite 350
Littleton, CO 80122
About usSouth Denver Neurosurgery provides state-of-the-art diagnostic and treatment programs for a wide range of brain and spinal disorders. We partner with our patients and their physician teams to make individualized decisions and treatment plans. Our physicians are some of the most experienced in the Rocky Mountain region, offering the latest, most up-to-date procedures and treatment options to patients.
Physicians desiring a consult, please call: 303.734.8650
Locations:Littleton Adventist Hospital CampusArapahoe Medical Plaza III7780 S. Broadway, Suite 350Littleton, CO 80122
Porter Adventist Hospital CampusHarvard Park Medical Plaza 950 E. Harvard Ave., Suite 570Denver, CO 80210
Castle Rock Adventist Health Campus1189 S. Perry St., Suite 230 Castle Rock, CO 80104
South Denver Neurosurgery303.734.8650 (phone)303.734.8653 (fax)SouthDenverNeurosurgery.org
Centura Health complies with the Civil Rights Act of 1964 and Section 504 of the Rehabilitation Act of 1973, and no person shall be excluded from participation in, be denied benefits of, or otherwise be subjected to discrimination in the provision of any care or service on the grounds of race, religion, color, sex, national origin, sexual preference, ancestry, age, familial status, disability, or handicap.
Ben Guiot, MD Neurosurgeon, board-certified by the American Board of Neurological Surgeons and the Royal College of Physicians and Surgeons of Canada. Specializing in all aspects of spine care, including::: Minimally invasive
spine surgery:: Spinal deformity
correction:: Reconstruction
of complex spinal disorders
Christopher Nichols, MDNeurologist, specializing in stroke and vascular neurology and endo-vascular neurosurgery, including evaluation and treatment of::: Brain aneurysms:: Arteriovenous
malformations:: Dural arteriovenous
fistulas:: Acute stroke
and intracerebral hemorrhage
:: Cervical and intracranial arterial disease
:: Cerebral vasculopathy:: Cerebral venous
thrombosis
J. Adair Prall, MDNeurosurgeon, specializing in::: Trigeminal neuralgia:: Spinal disorders:: Neuro-oncology:: Minimally invasive
and motion-preserving spine surgery
:: Stereotactic radiosurgery (Gamma Knife® and CyberKnife®)
David VanSickle, MD, PhDNeurosurgeon, PhD in bioengineering, specializing in::: Deep brain stimulation
(DBS) for Parkinson’s and essential tremor
:: Epilepsy surgery:: Neuro-oncology:: Spinal cord stimulator
implantation for pain:: Transsphenoidal surgery
(pituitary surgery):: Minimally invasive and
motion-preserving spine surgery
:: Stereotactic radiosurgery (Gamma Knife® and CyberKnife®)
Mariel Szapiel, MDNeurosurgeon, specializing in neuromodulation for chronic diseases, including::: Essential tremor:: Dystonia:: Parkinson’s disease:: Tourette’s syndrome:: Obsessive-compulsive
disorder and other mood disorders
:: Chronic intractable headaches
Welcome





























