Embed Size (px)
Citation preview

Neurophysiology of Atypical Parkinsonism 409
409
From: Current Clinical Neurology: Atypical Parkinsonian DisordersEdited by: I. Litvan © Humana Press Inc., Totowa, NJ
24Role of Electrophysiology in Diagnosis and Research
in Atypical Parkinsonian Disorders
Josep Valls-Solé
INTRODUCTION
Correct clinical diagnosis of patients with parkinsonism is not always possible in spite of thecontinuous effort in defining diagnostic criteria (1). Parkinsonism, defined as the combination ofbradykinesia and rigidity (2), may be a predominant clinical feature of several diseases, includingidiopathic Parkinson’s disease (IPD) and several other entities commonly known as “Parkinson-plus”syndromes or atypical parkinsonian disorders (APDs). In these entities, parkinsonism is accompa-nied by other clinical signs, or red flags (3), that should warn the physician of the existence of adegenerative disorder. Even though rather specific clinical patterns have been described in patientswith APDs, such as predominantly autonomic failure, cerebellar, or pyramidal dysfunction, in mul-tiple system atrophy (MSA), axial rigidity, ocular motility disorders, and falls early in the course ofthe disease, in progressive supranuclear palsy (PSP), myoclonus and asymmetrical higher corticallimb dysfunction, in corticobasal degeneration (CBD), and fluctuating cognitive deficits, visual hal-lucinations, and REM sleep behavior disorder, in diffuse Lewy-body disease (LBD), these signs arenot always evident or they may pass unrecognized by nonspecialized neurologists. In some condi-tions, such as for instance CBD, similar clinical expressions may be common to different pathologies(4), and the same disease may encompass diverse clinical presentations (5). In others, such as MSAwith parkinsonian features (MSA-P), patients may behave like IPD until death (6), making it almostimpossible to establish a clinical separation between the two diseases. Nowadays, the definite clini-cal diagnosis still resides in the pathological postmortem examination (1,7,8).
When in doubt, the clinician may seek help in laboratory exams. Unfortunately, however, there arenot yet laboratory methods that can supply a diagnosis of certainty for APDs. Although single photonemission computer tomography (SPECT) and positron emission tomography (PET) have shownpostsynaptic dopaminergic deficits in APDs (9), these tests are not yet capable of differentiatingbetween the various degenerative syndromes featuring parkinsonism. Though electrophysiologicalstudies do not usually provide the diagnosis, they can be of great help in the recognition of patho-physiological mechanisms underlying the presentation of some symptoms and signs. In parkinsonism,pallidal hyperactivity might be responsible for reduced activation of thalamocortical projections, andfor an abnormal control of brainstem circuits (10–12). The situation might be slightly different inAPDs, in which the basal ganglia pathology is accompanied by neuronal loss and atrophy in manynuclei of the brainstem and cerebellum, and dysfunctions might be present in various circuits. It is

410 Valls-Solé
therefore logical that, although some clinical neurophysiological manifestations are common to bothtypes of disorders, there are a few specific and distinctive features of each syndrome that may beclinically useful.
Neurophysiological studies are suited to demonstrate, document, and quantify clinical observa-tions. They are not expensive, and mainly noninvasive. They may occasionally bring information onneurological functions that is not obtainable with other means. One such example is, for instance, themeasure of excitability in neuronal structures or circuits. In this chapter, we describe the neurophysi-ological observations made in patients with the principal disorders grouped under the term APDs,and discuss how the results compare between different patient groups.
NEUROPHYSIOLOGICAL CORRELATE OF PARKINSONISM
Patients with APDs usually present with the main clinical signs characteristic of parkinsonism,i.e., bradykinesia and rigidity. Although clinicians identify bradykinesia and rigidity with no need forneurophysiological recordings, these are convenient for quantitation of the dysfunction. Bradykine-sia and, specially, rigidity are present with varying degree and localization in patients with parkin-sonism. They may not be observed at all in patients at early stages of the cerebellar variant of multiplesystem atrophy (MSA-C), though they will eventually appear during the course of the disease.
Hypokinesia and BradykinesiaHypokinesia and bradykinesia are abnormalities of movement, and the best way to quantify them
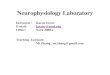
is with the use of reaction time task paradigms. Akinesia is defined as a delay in movement initiation,whereas bradykinesia is defined as the slowness of movement execution (13). There are many studieson reaction time in patients with IPD, but considerably less in APDs. Reaction time can be studiedusing different methods, ranging from the execution of a task (14,15), the release of a switch or alever (16,17), the onset of limb displacement (18,19), or the onset of electromyogram (EMG) activity(20,21). In paradigms of simple reaction time (SRT), the subject knows all details about the requestedmotor performance before the imperative signal is delivered. In paradigms of choice reaction time(CRT), subjects have to process some of the information contained in the imperative signal itself.When measuring SRT as the onset of EMG activity in wrist extensors in patients with IPD, PSP, andMSA, Valldeoriola et al. (22) found a significantly larger delay of reaction time in patients with PSPin comparison to the other groups of patients (Fig. 1). This is in fitting with previously reportedresults of an investigation of reaction time to progressively complex tasks in PSP patients (23). Theseauthors found an increased central processing time in patients with PSP compared with both IPD andcontrol subjects. PSP patients might have degraded cognition, with a delay in stimulus identificationand categorization processes (24).
The mechanisms underlying hypokinesia can be studied using EMG analysis of reaction timetasks. Hallett and Khoshbin (10) found that IPD patients were unable to appropriately scale the sizeof the first agonist burst to the requirements of a ballistic movement. They proposed that such defectrepresented a physiological mechanism of bradykinesia. It is likely that the increased pallidal inhibi-tion of thalamocortical excitatory connections accounts for such an abnormal “energization” of themotor cortex. A proper study of the triphasic pattern in patients with APDs has not been done so far.However, in a small group of PSP patients, Molinuevo et al. (25) observed abnormalities of thetriphasic pattern that were similar to those observed in IPD patients.
RigidityRigidity in patients with parkinsonism manifests as a difficulty of complete muscle relaxation,
with often permanent tonic background EMG activity (11). Several neurophysiological tests havebeen used to assess rigidity, although direct clinico-neurophysiological correlations have proven moredifficult than with bradykinesia. Rigidity has been considered to be the cause of some neurophysi-

Neurophysiology of Atypical Parkinsonism 411
ological findings in IPD, such as an increased size of the F wave (26), increased size of long loopreflex responses to stretch (27) or to electrical stimuli (28–30), abnormalities in the silent periodinduced by transcranial magnetic stimulation (31,32), reduced reciprocal inhibition (33,34), andreduced autogenic (Ib) inhibition of the soleus H reflex (35). However, none of those tests is spe-cific for rigidity, which continues to be assessed by clinical evaluation of the resistance to passivemovements.
Like with bradykinesia, most tests directed to the evaluation of rigidity have been proven inpatients with IPD, and more scarcely in patients with APDs. However, it is not unreasonable toadmit that when and where rigidity is present, patients with APDs would present similar abnormali-ties as those described for IPD. Direct surface electrophysiological recording of a muscle in rigidpatients in resting conditions may be enough to notice that there is increased muscle activity withrespect to normal subjects. Electrophysiological evidence for that can be found when testing therelaxation time after a sustained contraction (36). The stretch reflex, which is the most paradigmaticelectrophysiological test for limb rigidity, has not been properly tested in patients with APDs. Inthese patients, rigidity often predominates in axial muscles and is very mild in limb muscles, makingit more difficult for neurophysiological evaluation. The shortening reaction (37–40) is a relativelypoorly studied long latency reflex that occurs in the muscle shortened during a passive movement. Itsfrequent presence in patients with IPD could reflect the difficulties of these patients in modulatingsensory signals generated by either joint afferents (38), tendon organ afferents (39), or both. Unfortu-nately, however, there have not been recent studies on such an interesting phenomenon.
The pathophysiology of rigidity may be related to abnormalities in propriospinal reflexes. In theirstudy of IPD patients, Delwaide et al. (35) postulate that reduced autogenic inhibition mediated by Ibinterneurons would be a neurophysiological correlate of rigidity. Interestingly, however, in the solestudy published so far on spinal physiological mechanisms in APD patients, Fine et al. (41) reportedincreased Ib inhibition in patients with PSP. The observation of such an opposite behavior betweenIPD and PSP patients might be useful for differential diagnosis but points to the fact that neurophysi-
Fig. 1. Histograms of the mean and 1 standard deviation of simple reaction time values (expressed in ms)for EMG activity, onset of movement and task execution in healthy volunteers, and in patients with IPD,PSP, and MSA.

412 Valls-Solé
ological observations might only be one manifestation of dysfunctional mechanisms. Further studiesare required to find out the mechanisms by which the Ib interneurons are modulated in a differentdirection in PSP and IPD, and what is the exact role of this dysfunction in the generation of rigidity.
NEUROPHYSIOLOGICAL TESTS IN THE ASSESSMENT OF ATYPICALPARKINSONIAN DISORDERS
Some neurophysiological features are specific or distinctive of patients with APDs. However, thisdoes not mean that the electrophysiological findings hold the key for the diagnosis, since sensitivityand specificity of the tests has not been properly examined yet. The most relevant of these observa-tions are described below, where they are grouped according to the neurophysiological method ortechnique in which the observation is based.
Brainstem ReflexesThe brainstem is a crucial structure for integration of reflexes and functions related to motor con-
trol. These structures receive modulatory inputs from more rostral centers, including the basal gan-glia. There are many nuclei and circuits of interest in the brainstem for neurophysiological studies.However, it is still difficult to assign the results of some neurophysiological observations to specificbrainstem centers or circuits. Therefore, most data gathered from the study of the brainstem in patientswith APDs have the value of an empirical finding, and the exact anatomical/pathological correlation inhumans is mainly based on hypothesis and theoretical knowledge from animal experiments.
Table 1 summarizes the observations made in patients with parkinsonism regarding facial move-ments and brainstem reflexes. Although many brainstem circuits are dysfunctional in patients withAPDs, the examination of brainstem reflexes and functions yields more interesting results in patientswith PSP than in any other form of parkinsonism.
Eye and Eyelid MovementsSome of the most striking features differentiating PSP from other disorders presenting with par-
kinsonism regard facial expression and gaze disturbances (42). A list of abnormalities reported so farregarding eye or eyelid movements in these patients is shown in Table 2. The resting blink rate, of 24per minute in normal controls, was found to be reduced in most patients with parkinsonism (43), butsignificantly more so in patients with PSP, whose mean blinking frequency can be reduced to as littleas 4 blinks per minute. Blinking rate may be an expression of the level of dopamine activity.
Clinical evidence of eye movement abnormalities is not always present in the initial phases of thedisease (42). If the possibility of PSP is suspected on the basis of some other clinical features, record-ing of eye movements by electro-oculography might be of some help. Surface electrodes are placedin the upper, lower, nasal, and temporal edges of the orbit and the subject is requested to makehorizontal and vertical eye movements (44). Electro-oculogram recordings may show characteristicabnormalities in patients with PSP (45), including slowness of vertical eye movements, absent Bell’sphenomenon, and square wave jerks (Fig. 2). In the study reported by Vidailhet and coworkers, 9 outof 10 patients with PSP had vertical-gaze paralysis with preserved reflex eye movements. Vidailhetet al. (46) also showed slowness of horizontal eye movement and microsaccades that would help indistinguishing patients with PSP from those with other parkinsonisms. Some eye movement abnor-malities are already apparent at simple inspection. A PSP patient exhibiting slowness of saccades andlimitation of vertical eye movement with preserved oculo-cephalic reflexes is shown in video segment 1.
Reflex Responses of the Orbicularis OculiIn contrast to the reduced frequency of spontaneous blinking, reflex responses of the orbicularis
oculi to trigeminal nerve inputs are of normal latency (47). The normality of reflex responses totrigeminal nerve stimuli is in contrast to the absence or significant reduction of the responses toauditory inputs (48). Whether the response of the orbicularis oculi to loud auditory stimulus is part of

Neurophysiology of Atypical Parkinsonism 413
Table 1Characteristics of Some Brainstem Reflexes and Functions in Patients With Parkinsonism
Test IPD PSP MSA CBD
Spontaneous Reduced Extremely Reduced Enhanced Normalblinking frequency Normal Reduced
Excitability recovery Enhanced Enhanced Enhanced Normalcurve (paired pulses)
Blinking to loud auditory Normal Reduced Normal or Increased Normalstimuli
Blinking to median nerve Normal Reduced or Absent Normal Normalstimuli
Auditory prepulse Reduced Reduced ? ?inhibition
Somatosensory prepulse Normal Reduced ? ?inhibition
IPD, idiopathic Parkinson’s disease; PSP, progressive supranuclear palsy; MSA, multiple system atrophy(strionigral degeneration); CBD, corticobasal degeneration; ?, data unknown.
Table 2Eye and Eyelid Movement Abnormalities Observed in Patients With PSP
Reduced spontaneous blinking (43)Blepharospasm (42)Supranuclear palsy of eyelid opening (45)Supranuclear palsy of eyelid closing (42)Reduced voluntary suppression of vestibular ocular reflex (VOR) (42)Eyelid retraction (Cowper’s sign) (42)Square-wave jerks (46)Absent eyelid responses to acoustic stimuli (48)Absent eyelid responses to median nerve stimuli (47)
the generalized startle reaction or is an auditory blink reflex with separate physiological characteris-tics is still a matter of debate (49,50). In any case, the reduction of orbicularis oculi responses toauditory stimuli is indeed an important observation of some clinical utility in the differential diagno-sis of APDs.
The palmomental reflex is usually elicited by scratching the volar aspect of the thenar eminence orthe thumb. This leads to a reflex movement of the chin that is considered abnormal when it showsreduced habituation (51). Electromyographic recording of facial muscle responses during elicitationof the palmomental reflex permits the quantitation of the responses (52). The facial reflex response isnot limited to the mentalis muscle but is usually accompanied by an ipsilateral eyelid movement thatcan be apparent with simple inspection and readily demonstrated with surface electromyographicrecording (Fig. 3A). Interestingly, in patients with PSP, contraction of eyelid muscles is not presenteven when the mentalis response is evident (see the second part of video segment 1 on accompanyingDVD). In a protocolized study of facial reflexes in patients with parkinsonism, Valls-Solé et al. (47)analyzed the responses elicited simultaneously in the mentalis and orbicularis oculi muscles bymedian nerve electrical stimulation. The study included patients with IPD, PSP, MSA, CBD, andhealthy volunteers. Responses in the mentalis muscle were found in most patients and in 2 out of 10normal subjects. In all of them, whenever there were responses in the mentalis muscle, there were

414 Valls-Solé
Fig. 2. Electro-oculogram in a healthy subject (A) and in a patient with PSP (B) during fixation to an object(upper traces) and voluntary saccades (lower traces). Note the presence of small eye movements during fixa-tion, and of a slow and staircase eyeball displacement during the saccadic movement.
Fig. 3. Facial reflex responses to median nerve stimulation in a patient with IPD (A), and in a patient withPSP (B). Note the absence of orbicularis oculi response in the patient with PSP even though the mentalis muscleresponse (lower traces) is similar in both patients.
also responses in the orbicularis oculi muscle. The exception were the patients with PSP, who had noorbicularis oculi responses even if the responses of the mentalis muscle were not different from thoseobserved in the other groups of patients (Fig. 3B). This abnormality probably reflects the activationof two different circuits by the median nerve afferent volley. The mentalis response could be con-veyed through the cortico-nuclear tract, since this tract innervates predominantly lower facial moto-neurons (53), and a transcortical loop has been suggested because of the contiguity between thumband chin areas in the brain sensorimotor region (52,54). The selective damage of the pontine reticular

Neurophysiology of Atypical Parkinsonism 415
formation in patients with PSP would be responsible for the absence of the orbicularis oculi response.Enhancement of mentalis response may occur because of disinhibition of thalamo-cortical connec-tions from their striatal control (54).
One of the earliest contributions of electromyography to the assessment of central nervous system(CNS) abnormalities in patients with parkinsonism was made by Kimura in 1973 (55). Kimura dem-onstrated in these patients the existence of an abnormal decrease of habituation of the blink reflex topaired supraorbital nerve electrical stimuli. The fact that the abnormalities occurred in the R2 but notin the R1 component of the blink reflex suggested that the disturbance lies in the interneurons ratherthan in the motoneurons. Since then, many authors have studied the blink reflex excitability recoverycurve to paired stimuli, by dividing the size of the response to the test stimulus by that of the responseto the conditioning stimulus. This sign has been reported not only in parkinsonism, but in many otherdisorders as well (56,57). It is therefore of little use for differential diagnosis between degenerativedisorders. In clinical practice, the assessment of enhanced trigemino-facial reflex excitability may beof interest for documenting the existence of an abnormal function of brainstem interneurons in patientsin whom clinical assessment is dubious or at early stages of their disease. We found similar interneu-ronal brainstem excitability enhancement in IPD, PSP, and MSA patients (47). Figure 4 shows theproposed circuit of basal ganglia control of trigemino-facial reflex excitability, according to Bassoand Evinger (58) and Basso et al. (59), and the dysfunction likely occurring in parkinsonism.
Other Facial ReflexesNeurophysiological abnormalities have been reported in other brainstem reflexes in parkinsonism,
although they have not been investigated specifically in APDs (60–62). It has been shown that thesecond inhibitory period of the masseteric exteroceptive inhibitory reflex has an enhanced excitabil-ity recovery cycle, similar to that of the blink reflex in patients with IPD. The same excitabilityrecovery abnormalities have been reported in parkinsonism and dystonia (60).
The Startle Reaction and the Startle-Induced Modulation of Reaction TimeThe startle reaction in experimentation animals is known to be generated in the nucleus reticularis
pontis caudalis (nRPC), which activates the reticulospinal tract inducing muscle responses in facialand spinal motoneurons (63). In humans, the startle reaction is also thought to originate in corre-sponding nuclei of the brainstem, and spread caudally and rostrally to limb and facial muscles.
Abnormalities in the startle reaction can be related to enhancement or reduction of the responsesize. One example of abnormal startle response enhancement is hyperkeplexia (64), whereas anabnormal startle response reduction takes place in patients with PSP (48). The decrease of thestartle reaction in PSP patients should not be surprising, since neuronal loss in these patients involvesspecifically the cholinergic neurons of the lower pontine reticular formation, where the startle reac-tion is generated. Neuronal loss has been reported in the pedunculo-pontine tegmental nucleus andthe nucleus reticularis pontis caudalis (65–67). In the study carried out by Vidailhet et al. (48), theresponse was absent in three out of eight patients, and it was small and delayed in the other fivepatients. The same finding was later replicated by Valldeoriola et al. (22), who carried out a compara-tive study of PSP and other APDs.
Whereas response enhancement is easy to identify because of reactions of larger size and decreasedhabituation, assessment of an abnormal reduction of the response may be more difficult because of thefact that the response habituates easily in healthy subjects (49). For this reason, the observationsmade in experiments in which the startling stimulus was applied together with the imperative signalin the context of a reaction time task paradigm should be helpful for clinical purposes. Using suchmethods, Valls-Solé and coworkers (68–70) made a few interesting observations in healthy subjects:
1. The startling stimulus applied together with the imperative signal of a reaction time task induces a signifi-cant acceleration in the execution of the intended movement. The ballistic movement is executed withoutany distortion but at a significantly faster speed (70).

416 Valls-Solé
Fig. 4. Basal ganglia control of trigemino-facial reflex excitability. The basal ganglia modulate the excit-ability of the blink reflex through the output signals arising from the globus pallidus pars interna (GPi) and thesubstantia nigra pars reticulata (SNr). According to Basso et al. (58) and Basso and Evinger (59), the GPi/SNrcomplex sends inhibitory inputs to the superior colliculus (SC), which is excitatory for the nucleus raphe magnus(nRM). This, in turn, inhibits the trigeminal neurons of the spinal nucleus. In PD, there is increased GPi/SNrinhibition of the SC which, as a consequence, reduces its excitatory inputs to the nRM. The less active nRMinduces less inhibition of the spinal trigeminal nucleus, which becomes dis-inhibited (hyperexcitable). As withbradykinesia, it is difficult to know whether the same mechanisms apply to APDs. I, inhibitory; E, excitatory ofstimulus.
2. The response to the startling stimulus is enhanced. The same startling stimulus that would give rise to arelatively small and inconsistent response when given alone induce a significantly larger response when isapplied during motor preparation (68).
3. Habituation of the response to the startling stimulus is significantly reduced. In a study in which auditorystimuli were applied at the same rate in different experimental conditions, Valls-Solé et al. (69) found thathabituation of the response to the startling stimulus was reduced in facial and cervical muscles whensubjects were engaged in preparation for a ballistic reaction.
Clinical application of the collision between a startle reaction and the voluntary activity in a reac-tion time task paradigm (the StartReact effect) was reported by Valldeoriola et al. (22). These authorsfound that patients with PSP not only had absent startle reaction but they were also not able to accel-erate their voluntary reaction when the startling stimulus was applied together with the imperativesignal.
In contrast to patients with PSP, patients with MSA have normal auditory startle reaction in facialand cervical muscles (71). Furthermore, when the responses of cranial and limb muscles are analyzedtogether, MSA patients had enhanced probability of a response, shortened onset latency, and enlargedresponse magnitude compared to normal controls (72,73). In the only analysis of the startle response inpatients with LBD, Kofler et al. (73) reported fewer and abnormally delayed ASR of low amplitude andshort duration in extremity muscles in comparison to healthy controls. Two more details of the studiesof Kofler and coworkers (72,73) are relevant for the discussion of the contribution of the startlereaction to the differential diagnosis of APD patients. One is the fact that three patients with MSAhad no response to the startle reaction, indicating that absence of the startle reaction is not a featureexclusive to PSP patients (48). A particularly high density of oligodendroglial cytoplasmatic inclu-

Neurophysiology of Atypical Parkinsonism 417
sions in the brainstem area responsible for the generation of the reticulospinal tract was assumed tobe the cause of absent startle response in those MSA patients. Another observation made by Kofleret al. (72) was the existence of subtle differences in the characteristics of the response betweenMSA-P and MSA-C patients. Whereas MSA-P patients had a higher startle probability and a largerarea and shorter latency of the motor response, patients with MSA-C had less habituation. Differ-ences between the two groups in the inhibitory effect of the cerebellum over the motor cortex may beresponsible for such neurophysiological observation (72).
Prepulse InhibitionA weak stimulus preceding by about 100 ms the startling stimulus has an effect of inhibition upon
the startle reaction (prepulse inhibition). The prepulse stimulus may be of the same or a differentsensory modality as the stimulus inducing the startle (50). In the blink reflex, an auditory prepulsecauses enhancement of the R1 and depression of the R2 to electrical supraorbital nerve stimuli (74).In a study of prepulse inhibition in patients with IPD, Nakashima et al. (75) found that auditoryprepulse stimuli induced an abnormally reduced inhibition of the R2 response of the blink reflex, andLozza et al. (76) reported an abnormally reduced blink reflex inhibition after index finger stimula-tion. However, some patients with IPD have an abnormal auditory prepulse inhibition and a normalsomatosensory prepulse inhibition (77). The different behavior of auditory and somatosensoryprepulse stimuli in IPD patients could be owing to differences in the prepulse effectiveness of thesame vs different sensory modality, differences in the arrival time of prepulse inputs to the brainstemcenters, or to selective impairment of reticular formation neurons activated by auditory inputs. Patientswith PSP have also absent or significantly reduced prepulse inhibition to both auditory and somatosen-sory prepulses (Fig. 5), revealing an even more striking dysfunction of the prepulse circuit in PSPcompared to IPD. No data are available so far regarding prepulse inhibition in MSA patients.
Spinal ReflexesA variety of tests determining the excitability of propriospinal interneurons (78,79) have been
applied to patients with IPD, demonstrating reduced reciprocal (33,34) and autogenetic (Ib) inhibi-tion (35), possibly related to the clinical expression of rigidity. These exams have not been done inpatients with APDs, except for a single study of autogenetic inhibition (Ib inhibition) in patients withPSP (41). In such a study, the authors showed enhancement of the inhibition, the exact opposite ofwhat was reported in patients with IPD. The explanation why opposite results have been found inthese two groups of patients is, up to now, not clear.
Audiospinal facilitation is known as the effect of an auditory stimulus on spinal reflexes, specifi-cally the soleus H reflex. The methods for audiospinal facilitation were developed by Rossignol andJones (80) and Delwaide et al. (81). The stimulus to the posterior tibial nerve to induce the H reflex isapplied between 0 and 110 ms after a loud acoustic stimulus. Healthy subjects have H reflex facilita-tion beginning at intervals between 60 and 80 ms, and lasting until the intervals of 100 or 110 ms.However, audiospinal facilitation is abnormally reduced in patients with IPD (12,81). Our own pre-liminary observations in patients with the clinical diagnosis of probable PSP is that they exhibit thesame abnormality (82).
Surface EMG Recording of Abnormal MovementsThe recording of abnormal movements by means of surface EMG recording yields interesting
information for the analysis of tremor, such as in patients with IPD (82). Tremor has also been reportedin up to 74% of MSA patients (83). However, this figure included several types of tremor, with only afew patients exhibiting the resting tremor typical of IPD, and a large proportion of unclassifiablehands and finger “jerky” tremors, such as those shown in video segment 2. Electrophysiologicalstudies of these latter movements have shown that their characteristics are closer to myoclonus thanto tremor (84). A piezoelectric accelerometer was used to record finger movements and analyze the

418 Valls-Solé
Fig. 5. Prepulse inhibition of the blink reflex in a healthy volunteer and in a patient with PSP. The traces ofthe upper row show the responses to a stimulus to the supraorbital nerve applied at the vertical line. Ipsilateralrecordings (ipsi) show R1 and R2 responses whereas contralateral recordings show only the R2. The traces ofthe lower row show the responses to the same stimulus when a prepulse is applied 100 ms before (arrows).(A) Normal auditory prepulse inhibition in a healthy volunteer; (B) Absent auditory prepulse inhibition in apatient with PSP. (C) Absent somatosensory prepulse inhibition in the same patient.
frequency spectrum of the signal through fast Fourier transformation. This procedure showed thatmovements of MSA patients were rather non-rhythmic in comparison to those of patients with otherforms of tremor (Fig. 6). Salazar et al. (84) suggested the term minipolymyoclonus to be used todescribe these small amplitude, irregular, jerklike abnormal movements. Other forms of myoclonushave been also reported in a few MSA patients (30,85), which might have their origin in a reducedinhibition of the strio-palido-thalamo-cortical circuit (86). Table 3 shows a list of disorders in whichactivity defined as minipolymyoclonus has been encountered, together with some of the most rel-evant neurophysiological findings.
Myoclonus is also an apparent feature in patients with CBD (87), in whom they are thought to beof cortical origin in spite of lacking neurophysiological evidence. The expected findings of corticalmyoclonus, such as giant somatosensory evoked potentials and jerk-locked EEG potentials, are incon-sistent in CBD. The cortical response is occasionally absent, which is attributed to the marked frontopa-rietal cortical atrophy and neuronal degeneration characteristic of these patients (88,89). Corticalatrophy of inhibitory neurons could lead to the enhanced (disinhibited) motor cortex excitability.
The “C” wave, or focal reflex myoclonus (90), is a response seen in forearm muscles after electri-cal stimulation of ipsilateral cutaneous nerves of the hand. This response is thought to be mediated byfast-conducting afferent and efferent pathways and might have a latency as short as 43.1+/–3.2 ms(87). In some patients, focal reflex myoclonus might be elicited by stimuli of an intensity belowperception threshold, which suggests a direct connection from the thalamic nuclei to the motor cortex(91). The “C” response should not be mistaken for the long latency excitatory response of the cutaneo-muscular reflexes (92,93). The cutaneo-muscular reflex can be elicited during a sustained tonic vol-untary contraction of the forearm muscles. The long latency excitatory component of thecutaneo-muscular reflex is abnormally enhanced in patients with IPD or MSA (30). However, thelatency of such a response is longer than that of the “C” reflex.

Neurophysiology of Atypical Parkinsonism 419
Fig. 6. Surface EMG recording from wrist extensors (A), accelerometric recording of finger movements(B), and FastFourier analysis of the movement recording (C) in a patient with MSA and minipolymyoclonus.See the absence of a dominant frequency peak.
Table 3Disorders Featuring Minipolymyoclonus
Disorder Dominant Clinical Sign EMG Bursts EEG “C” wave
Motoneuron disease Fasciculation atrophy Asynchronous (1–20 Hz) Not described Not described
Polyneuropathy Absent tendon jerks Slow and asynchronous Not described Not describedSevere sensory deficit
Alzheimer’s disease Dementia Multifocal Slow waves PresentEpileptiform
activityNegative
frontal wave
Myoclonic epilepsy Seizures Synchronized or irregular Slow negative Presentfrontal wave
Syringomyelia Weakness. Spasticity Asynchronous and Not described Not describedSensory deficit irregular
MSA-P Rigid-akinetic syndrome Synchronous (1–12 Hz) Normal Present
Autonomic Reflexes and FunctionsAutonomic nervous system dysfunction is the key to the diagnosis in patients with MSA who
present with parkinsonism or cerebellar syndromes (3), and is presently a required criterion for thediagnosis of probable MSA (94). Clinically relevant autonomic dysfunctions in these patients areorthostatic hypotension, urinary and fecal incontinence, erectile dysfunction in males, sudomotordisregulation, and abnormalities in respiratory control during sleep. Autonomic dysfunction, i.e.,urinary incontinence (97%) and constipation (83%), has also been reported in patients with LBD (95).

420 Valls-Solé
Orthostatic hypotension may result from the inability to increase sympathetic activity when stand-ing. This can be shown as an abnormal regulation of baroreflex responses to different stimuli (96).Using readily available electrophysiological equipment, it is also possible to monitor heartbeat fre-quency. Recording the R-R interval variation by means of the signal trigger and the delay line unit ofan electromyograph shows graphically the reduced adaptation of the heart beat rate to a posturalchange or to the Valsalva maneuver (77). The main drawback of this test is that patients with severebradykinesia might be unable to perform adequately the maneuvers, and reduced R-R interval varia-tion could actually be owing to insufficient stimulation. One of the possibilities to test R-R intervalvariation using methods that do not require the patient’s cooperation is based on the fact that thestartle response is normal in MSA patients (71,72), and on the observation that a startle acceleratesheartbeat frequency in normal subjects (97). In a group of six MSA patients, a startling acousticstimulus induced the normal motor component of the startle reaction but a significantly smaller changeof the R-R interval in comparison to healthy volunteeers (98).
The sympathetic sudomotor skin response, or SSR (99), may reveal dysfunctions in the autonomiccontrol of sudomotor reflexes. Loss of sympathetic neurons of the intermediolateral column mightexplain the finding of frequently abnormal SSRs in patients with MSA (100). Other tests of sudomo-tor function, such as the evaluation of the amount of sweat production to direct gland stimulationwith intradermal methacholine, have also demonstrated a decreased sweat response in patients withMSA (101).
Sleep disorders are frequent in patients with MSA and in those with LBD. Some of these disordersmight be related to autonomic dysfunction. In the study of Plazzi et al. (102), 35 out of 39 patientswith MSA had REM sleep behavior disorders. These preceded the diagnosis in 44% of the cases.Polysomnographic studies revealed subclinical obstructive sleep apnea in 6 patients, laryngeal stri-dor in 8 patients, and periodic leg movements during sleep in 10 patients. Laryngeal stridor, owing tovocal cord abductor paralysis during sleep, is probably caused by selective denervation atrophy ofthe cricoarytenoid muscle resulting from selective loss of neurons in the nucleus ambiguous (103),and may lead to chocking and death in advanced stages of MSA. This can be prevented with tracheo-stomy (104) or with continuous positive air pressure (105). REM sleep behavior disorder has alsobeen considered a sign heralding LBD (106) and, in a more recent study, it is considered as a possiblehallmark of a synucleinopathy in the setting of a cognitive dementia or parkinsonism (107).
Needle EMG Recording of the Sphincter MusclesIn MSA patients, manifestations of autonomic dysfunctions such as erectile impotence are usually
accompanied by increased urinary frequency and urgency, leading soon to incontinence, associatedwith large residual urine volumes (108). The severity of urinary symptoms is one main red flag thatshould warn the neurologist of the possibility that the parkinsonian patient thought to have IPD isactually facing the diagnosis of probable MSA (3). Urinary incontinence in MSA patients might bebecause of autonomic dysfunction, loss of pontine control of micturition, striatal sphincter denerva-tion, or a combination of them all. Striatal sphincter denervation is attributed to the selective loss ofmotoneurons in the nucleus of Onuff at the S2-S3 medullary segments. Needle electromyographyof the external anal sphincter, therefore, is considered an important neurophysiological test in theassessment of patients with parkinsonism, as most patients with MSA show denervation-reinnerva-tion signs (109,110). We and others have confirmed that anal sphincter denervation is prominent inpatients with MSA, although similar types of abnormalities have been found in a large proportion ofpatients with PSP as well as in some patients with IPD (111,112). Therefore, the utility of anal orvesical sphincter needle EMG in the diagnosis of MSA is still under debate (113,114). Chronic con-stipation, local trauma related to delivery, and other pudendal nerve long-standing lesions may giverise also to sphincter denervation (115,116), which may diminish the validity of the sign as a truemarker of motoneuronal loss. In the consensus statement for the diagnosis of MSA (94), sphincterEMG abnormalities are considered as a supportive laboratory finding.

Neurophysiology of Atypical Parkinsonism 421
Transcranial Magnetic Stimulation
There are not many studies published on the use of transcranial magnetic stimulation (TMS) inpatients with APDs in comparison to the large body of literature published in patients with IPD.However, finding an abnormality in central conduction time in a patient with parkinsonism should beconsidered as a red flag to warn of the likely existence of a degenerative disorder different from IPD.Central motor conduction time has been found slightly delayed in a number of patients with MSA, inboth the parkinsonian (117) and cerebellar variants (118).
Many other cortical and subcortical functional measures can be determined with single-pulse TMS,including resting and active threshold, stimulus-response curves, silent period duration, or corticalmaps, but only a few studies of this kind have been carried out in patients with APDs. Most of themhave been performed in patients with CBD, a disorder featuring clinical signs of asymmetrical sen-sorimotor cortex involvement. Recording from muscles of the more affected side, Lu et al. (119)reported shortened TMS-induced silent period, and Strafella et al. (120) reported enhanced facilita-tion and reduced inhibition of MEPs modulated by digital nerve stimulation. These findings are likelyreflecting motor cortical excitability enhancement.
Patients with CBD exhibit lack of voluntary control of limb movements (video segment 3), or“alien-hand” syndrome, which suggests a cortical dysfunction (121,122). In normal subjects, unilat-eral TMS, applied with the figure of “8” coil, induces hand muscle responses restricted to the con-tralateral side. However, in 6 out of 10 patients with CBD, Valls-Solé et al. (123) found bilateralresponses to focal, unilateral, TMS applied to the side contralateral to the alien hand (Fig. 7). Ipsilat-eral responses were delayed with respect to the contralateral ones by a mean of 7.7 ± 2.2 ms, a timeallowing for conduction through the corpus callosum. Such abnormality was not found in any of 10normal subjects, 8 patients with Alzheimer’s disease, or 6 patients with IPD presenting with pre-dominantly unilateral rigidity. This finding points again to an enhanced motor cortex excitability inthe hemisphere contralateral to the alien hand, which may be unable to inhibit transcallosal excitatoryinputs from the other hemisphere.
Paired-pulse TMS has been also used in the study of corticospinal tract functions in patients withAPD. Intrahemispheric cortico-cortical inhibition was found abnormally reduced in patients with MSA-P, but not in patients with MSA-C (124). It has also been abnormal in the study of patients with CBD(125,126), suggesting the possibility of its clinical utility in the early phases of the disease (126).
TMS is an important tool not only for the assessment of cortical motor function but also for theanalysis of the modulatory effects that descending pathways might have on segmental reflexes.Using methods similar to those proposed by Delwaide and collaborators with auditory stimuli (81),we examined the effects of TMS on the soleus H reflex in normal subjects and in patients withparkinsonism. In healthy volunteers, TMS induced early (5–30 ms) and late (60–100 ms) phases ofsignificant facilitation of the soleus H reflex (127). The second phase is absent or significantlyreduced in about 50% of patients with IPD (82), and in all eight patients with PSP examined so far(unpublished results).
Evoked PotentialsThe early components of the somatosensory evoked potentials in patients with IPD are normal,
except for the N30 recorded at the frontal lobe, which shows reduced amplitude (128). According toRossini and collaborators, the reduced amplitude of the N30 might be owing to an abnormal sen-sorimotor integration (129). A different kind of abnormality has been reported in patients with PSP.In these patients, Kofler and collaborators (130) reported an enhancement of the amplitude of theearly components of the somatosensory evoked potentials, which was considered to be the conse-quence of cortical disinhibition. More recently, Miwa and Mizuno (131) confirmed the finding andproposed that the observation of enlarged somatosensory evoked potentials can be useful in the dif-ferentiation of PSP patients from other patients with movement disorders.

422 Valls-Solé
Fig. 7. Recordings from bilateral thenar muscles to focal, unilateral, transcranial magnetic stimulation (TMS)in a healthy control subject (A), and in a patient with CBD (B). Upper traces result from left-hemisphere TMS,and lower traces from right-hemisphere TMS. Note the presence of a delayed ipsilateral MEP in the patient.
The premotor evoked potentials are abnormal in patients with IPD, likely reflecting a disturbancein preparation of the motor act. Deecke et al. (132) showed that there was a delay and reduction of thebereitschaftpotential, and abnormalities in event-related potentials have been also published. How-ever, there are no studies of the premotor potentials in patients with APDs.
NEUROPHYSIOLOGICAL TESTS MOST USEFULFOR DIFFERENTIAL DIAGNOSIS IN PATIENTS WITH APD
There is no single clinical neurophysiology test that can be used to distinguish with certitudebetween patients with APD at an individual level. This situation of clinical neurophysiology is com-mon to many other conditions. In practicing clinical neurophysiology, the examiner is constantlylooking for data that can bring more cues to confirm or refute an hypothesis made on the basis ofclinical exam. The selection of tests useful for differential diagnosis in patients with APD can only beorientative or suggestive, but conclusive. One of the roles of those whose work is devoted to clinicalneurophysiology should be to search for new methods and technical improvements to bring furtherunderstanding on pathophysiological mechanisms of the disease process.
From the author’s point of view, the neurophysiological tests that better characterize parkinsonismand, specifically, the APDs, are listed in Table 4. Performance of ballistic movements within a reac-tion time task paradigm is useful to test the mechanisms of motor preparation and execution, eventhough very much should still be learned on the physiology of motor preparation for the test to pro-vide its full potential of information. Brainstem and spinal reflexes have to be conveniently modu-lated by the descending motor commands for them to be integrated in the subject’s normal motorbehavior. Although many tests have given interesting information on the abnormal brainstem andspinal reflex modulation in patients with parkinsonism, a good clinical correlate of these abnormali-ties is still pending. The evaluation of autonomic reflexes and the sphincter EMG provides informa-tion on specific abnormalities that can be predominant in certain groups of patients. They reflect theinvolvement of specific groups of neurons, well correlated with pathologic findings. However, theyare not useful for the diagnosis on an individual patient basis since similar abnormalities can be

Neurophysiology of Atypical Parkinsonism 423
present in other groups of patients. TMS, short latency evoked potentials, and event-related poten-tials, are all offering many possibilities for the study of motor and sensory pathways as well as brainsensorimotor integration and high level processing of information. Although many studies have beencarried out in patients with parkinsonism, very few reports on APDs have been published so far. Alarge amount of research is under way regarding the physiological mechanisms of TMS and event-related potentials. Many of them are already available for clinical application and more will be in thenear future, allowing for better characterization of the abnormalities involving sensory and motorfunctions of patients with APDs.
FURTHER RESEARCH IN NEUROPHYSIOLOGY OF APD
There is a large amount of possibilities for research in neurophysiology of parkinsonism and ofmovement disorders in general. Neurophysiology offers the advantage of a good temporal resolutionof events and should bring further understanding of what is wrong in the CNS that leads to motordsyfunction. The research in clinical neurophysiology will probably continue until the pathophysi-ological mechanisms of the diseases are well understood. However, meaningful information can onlybe obtained if a careful neurological examination is followed by an imaginative albeit meticulousneurophysiological study. Undoubtedly, the most rewarding situation would be the one in whichneurologists and clinical neurophysiologists join their efforts. Relevant and interesting informationderived from neurophysiological studies should stir up the interest of clinicians, whereas challengingquestions arising from clinical exams should stimulate the imagination of the clinical neurophysiolo-gist in devising new techniques for more careful documentation of the signs.
Although the cooperation between clinical and neurophysiological experts is the first conditionfor the development of future lines of research, the second one is the development of better methodsfor clinical diagnosis of the diseases. Neurophysiology would be able to provide accurate informa-tion on the pathophysiology of movement disorders only if the diagnostic uncertainty is reduced tonegligible levels. A thorough neurophysiological characterization of patients with APDs, appropri-ately classifed into well-differentiated groups, would certainly bring information that may be usefulin the future to improve the diagnostic accuracy but, most of all, the pathophysiology of the diseases.
Suggestions for future research lines are listed in Table 5. Some of them are based on clinicalfeatures that should be the focuss of neurophysiological studies. However, some techniques may be
Table 4Selection of Neurophysiological Findings Allowing for Characterization of Specific DisordersPresenting With Parkinsonism
Disorder Results of Neurophysiological Tests
IPD Mild delay of reaction time in performance of ballistic movementsReduced prepulse inhibition of the blink reflex to auditory stimuli, with normal prepulse
inhibition to somatosensory stimuliRegular alternating tremor at rest
PSP Absent startle reaction to auditory stimuliAbsent orbicularis oculi response to a median nerve electrical stimulus eliciting a response
in the mentalis muscleReduced prepulse inhibition of the blink reflex to both auditory and somatosensory stimuli
MSA Signs of denervation-reinnervation in sphincter musclesSigns of autonomic dysfunctionMinipolymyoclonus
CBD Spontaneous and reflex myoclonusAsymmetry in cortical maps of representation of hand muscles
LBD REM sleep behavior disorder

424 Valls-Solé
Table 5Lines of Future Research in Neurophysiology of APD
Clinical Feature Research Lines
Motor systems Documentation of bradykinesia when performing natural tasksMethods for enhancing energization of the motor tractReadiness and premotor potentialsRelationship between mental processes and motor actionsRole of external cues and rhythms on movement performanceDysfunction of subcortical motor pathwaysSource of rest and action tremor oscillations
Sensory systems Multilevel sensorimotor integrationLong latency and event-related evoked potentialsIntersensory facilitation vs collision between sensory stimuli
Spinal cord reflexes Alpha motoneuronal excitabilityThe role of propriospinal inhibitory circuits in rigidity
Brainstem physiology Relationship between basal ganglia and brainstem nucleiRecording pedunculopontine tegmental nucleus functionsPhysiology of automatic movementsSpontaneous and reflex blinks
Cortical stimulation Modulation of cortical responses with sensory inputsIpsilateral effects of TMSRepetitive transcranial magnetic stimulation
able to demonstrate features of the disease that point to the dysfunction of certain nervous systemcenters or structures. Among those techniques, TMS and event-related potentials are probably themost promising ones. Since their implantation, TMS and especially repetitive TMS (rTMS) haveopened a large avenue of research in parkinsonism and other movement disorders. They will cer-tainly bring more possibilities for neurophysiological interventions in the near future, including thera-peutic actions. It has been demonstrated that the introduction of a variable amount of electrical currentin brain tissues by applying rTMS of different intensities and frequencies induces excitability changesthat can in turn be measured by conventional TMS or other methods (133). Since 1994 (134), rTMShas been used as a therapy in patients with IPD. Although there has been contradictory observationsup to the most recently published papers (135,136), researchers will certainly keep trying until thetechnique finds its position among the armamentarium of neurophysiological interventions in patientswith APDs. Recording event-related brain potentials should provide information on structures that maybe dysfunctional in parkinsonism. Cognitive negative variation has been reported to be improvedafter subthalamic nucleus stimulation (137), indicating the sensitivity of the test to basal ganglia–cortical loop function. A variety of other neurophysiological techniques could be in the list of sug-gestions for future studies. The reader may find helpful information regarding many of thoseprocedures in the specialized literature. However, apart from knowing technical details, the researcherinterested in neurophysiology of parkinsonism should exercise imagination to find new ways to dem-onstrate specific features of the disease.
LEGENDS FOR THE VIDEO SEGMENTS
Video segment 1. Two patients with PSP featuring slow and limited voluntary eye movements.The second patient shows responses of the lower facial muscles, but not of the periocular muscles, toa scratch stimulus to the thenar eminence.
Video segment 2. Two patients with MSA-P showing minipolymyoclonus. Note the irregularmovements, sometimes limited to one finger

Neurophysiology of Atypical Parkinsonism 425
Video segment 3. Two patients with corticobasal degeneration. The first patient shows some fea-tures of alien limb. The second patient had asymmetrical upper limb appraxia.
REFERENCES1. Litvan I, Bhatia KP, Burn DJ, et al. SIC Task force appraisal of clinical diagnostic criteria for Parkinsonian disorders.
Mov Disord 2003;18:467–486.2. Jankovic J, Rajput AH, McDermott MP, Perl DP. The evolution of diagnosis in early Parkinson’s disease. Arch Neurol
2000;57:369–372.3. Quinn N. Multiple system atrophy—the nature of the beast. J Neurol Neursurg Psychiatry 1989;Suppl:78–89.4. Boeve BF, Maraganore DM, Parisi JE, et al. Pathologic heterogeneity in clinically diagnosed corticobasal ganglionic
degeneration. Neurology 1999;53:795–800.5. Bergeron C, Pollanen MS, Weyer L, Black SE, Lang AE. Unusual clinical presentations of cortical basal ganglionic
degeneration. Ann Neurol 1996;40:893–900.6. Hughes AJ, Colosimo C, Kleedorfer B, Daniel SE, Lees AJ. The dopaminergic response in multiple system atrophy.
J Neurol Neurosurg Psychiatry 1992;55:1009–1013.7. Poewe W, Wenning G. The differential diagnosis of Parkinson’s disease. Eur J Neurol 2002;9(Suppl 3):23–30.8. Dickson DW, Bergeron C, Chin SS, et al. Office of rare diseases neuropathologic criteria for corticobasal degeneration.
Exp Neurol 2002;61:935–946.9. Brooks DJ, Ibáñez V, Sawle GV, et al. Striatal D2 receptor status in patients with parkinson’s disease, striatonigral
degeneration, and progressive supranuclear palsy, measured with IIC-raclopride and positron emission tomography.Ann Neurol 1992;31:184–192.
10. Hallett M, Khoshbin SA. A physiological mechanism of bradykinesia. Brain 1980;103:301–314.11. Berardelli A, Sabra AF, Hallett M. Physiological mechanisms of rigidity in Parkinson’s disease. J Neurol Neurosurg
Psychiatry 1983;46:45–83.12. Delwaide P, Pepin JL, DePasqua V, Maertens de Noordhout A. Projections from the basal ganglia to tegmentum: a
subcortical route for explaining the pathophysiology of Parkinson’s disease signs? J Neurol 2000;247(Suppl 2):75–81.13. Hallett M. Clinical neurophysiology of akinesia. Rev Neurol 1990;146:585-590.14. Rafal RD, Posner MI, Walker JA, Friedrich FJ. Cognition and the basal ganglia. Separating mental and motor compo-
nents of performance in Parkinson’s disease. Brain 1984;107:1083–1094.15. Bloxham CA, Dick DJ, Moore M. Reaction times and attention in Parkinson’s disease. J Neurol Neurosurg Psychiatry
1987;50:1178–1183.16. Daum I, Quinn N. Reaction times and visuospatial processing in Parkinson’s disease. J Clin Exp Neuropsychol
1991;13:972–982.17. Godaux E, Koulischer D, Jacquy J. Parkinsonian bradykinesia is due to depression in the rate of rise of muscle activity.
Ann Neurol 1992;31:93–100.18. Evarts EV, Teravainen H, Calne DB. Reaction time in Parkinson’s disease. Brain 1981;104:167–186.19. Pullman SL, Watts RL, Juncos JL, Chase TN, Sanes JN. Dopaminergic effects on simple and choice reaction time
performance in Parkinson’s disease. Neurology 1988;38:249–254.20. Berardelli A, Dick JPR, Rothwell JC, Day BL, Marsden CD. Scaling of the size of the first agonist EMG burst during
rapid wrist movements in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 1986;49:1273–1279.21. Pascual-Leone A, Valls-Solé J, Brasil-Neto JP, Cohen LG, Hallett M. Akinesia in Parkinson’s disease. I. Shortening of
simple reaction time with focal, single pulse transcranial magnetic stimulation. Neurology 1994;44:884–891.22. Valldeoriola F, Valls-Solé J, Tolosa E, Ventura PJ, Nobbe FA, Martí MJ. The effects of a startling acoustic stimulus on
reaction time in patients with different parkinsonian syndromes. Neurology 1998;51:1315–1320.23. Dubois B, Pillon B, Legault F, Agid Y, Lhermitte F. Slowing of cognitive processing in progressive supranuclear palsy.
A comparison with Parkinson’s disease. Arch Neurol 1988;45:1194–1199.24. Johnson R Jr, Litvan I, Grafman J. Progressive supranuclear palsy: altered sensory processing leads to degraded cogni-
tion. Neurology 1991;41:1257–1262.25. Molinuevo JL, Valls-Solé J, Valldeoriola F. The effect of transcranial magnetic stimulation on reaction time in progres-
sive supranuclear palsy. Clinical Neurophysiology 2000;111:2008–2013.26. Abbruzzese G, Vische M, Ratto S, Abbruzzese M, Favale E. Assessment of motor neuron excitability in parkinsonian
rigidity by the F wave. J Neurol 1985;232:246–249.27. Rothwell JC, Obeso JA, Traub MM, Marsden CD. The behavior of the long latency stretch reflex in patients with
Parkinson’s disease. J Neurol Neurosurg Psychiatry 1983;46:35–44.28. Deuschl G, Lucking CH. Physiology and clinical applications of hand muscle reflexes. Electroenceph Clin Neurophysiol
1990;Suppl 41:84–101.29. Fuhr P, Zeffiro T, Hallett M. Cutaneous reflexes in Parkinson’s disease. Muscle Nerve 1992;15:733–739.30. Chen R, Ashby P, Lang AE. Stimulus-sensitive myoclonus in akinetic rigid syndromes. Brain 1992;115:1875–1888.

426 Valls-Solé
31. Cantello R, Gianelli M, Bettucci D, Civardi C, De Angelis MS, Mutani R. Parkinson’s disease rigidity: magnetic MEPsin a small hand muscle. Neurology 1991;41:1449–1456.
32. Valls-Solé J, Pascual-Leone A, Brasil-Neto JP, McShane L, Hallett M. Abnormal facilitation of the response totranscranial magnetic stimulation in patients with Parkinson’s disease. Neurology 1994;44:735–741.
33. Bathien N, Rondot P. Reciprocal continuous inhibition in rigidity of parkinsonism J Neurol Neurosurg Psychiatry1977;40:20–24.
34. Lelli S, Panizza M, Hallett M. Spinal cord inhibitory mechanisms in Parkinson’s disease. Neurology 1991;41:553–55635. Delwaide P, Pepin JL, Maertens de Noordhout A. Short latency autogenic inhibition in patients with parkinsonian
rigidity. Ann Neurol 1991;30:83–89.36. Grasso M, Mazzini L, Schieppati M. Muscle relaxation in Parkinson’s disease: a reaction time study. Mov Disord
1996;11:411–420.37. Angel RW, Lewitt PA. Unloading and shortening reactions in Parkinson’s disease. J Neurol Neurosurg Psych
1978;41:919–923.38. Bathien N, Toma S, Rondot P. Étude de la réaction de raccourcissement présente chez l’homme dans diverses affec-
tions neurologiques. Electroenceph Clin Neurophys 1981;51:156–164.39. Berardelli A, Hallett M. Shortening reaction of human tibialis anterior. Neurology 1984;34:242–246.40. Diener C, Scholz E, Guschlbauer B, Dichgans J. Increased shortening reaction in Parkinson’s disease reflects a diffi-
culty in modulating long loop reflexes. Mov Disord 1987;2:31–36.41. Fine EJ, Hallett M, Litvan I, Tresser N, Katz D. Dysfunction of Ib (autogenic) spinal inhibition in patients with progres-
sive supranuclear palsy. Mov Disord 1998;13:668–672.42. Golbe LI, Davis PH, Lepore FE. Eyelid movement abnormalities in progressive supranuclear palsy. Mov Disord
1989;4:297–302.43. Karson CN, Burns S, LeWitt P, Foster NL, Newman RP. Blink rates and disorders of movement. Neurology
1984;34:677–678.44. Heide W, Koenig E, Trillenberg P, Kömpf D, Zee DS. Electrooculography: technical standards and applications.
Electroenceph Clin Neurophysiol 1999;(Suppl 52):223–240.45. Chu FC, Reingold DB, Cogan DG, Williams AC. The eye movement disorders of progressive supranuclear palsy.
Ophthalmology 1979;86:422–428.46. Vidailhet M, Rivaud S, Gouider-Khouja N, et al. Eye movements in parkinsonian syndromes. Ann Neurol 1994;35:
420–426.47. Valls-Solé J, Valldeoriola F, Tolosa E, Martí MJ. Distinctive abnormalities of facial reflexes in patients with progres-
sive supranuclear palsy. Brain 1997;120:1877–1883.48. Vidailhet M, Rothwell JC, Thompson PD, Lees AJ, Marsden CD. The auditory startle response in the Steele–
Richardson–Olszewsky syndrome and Parkinson’s disease. Brain 1991;115:1181–1192.49. Brown P, Rothwell JC, Thompson PD, Day BL, Marsden CD. New observations on the normal auditory startle reflex in
man. Brain 1991;114:1891–1902.50. Valls-Solé J, Valldeoriola F, Molinuervo JL, Cossu G, Nobbe F. Prepulse modulation of the startle reaction and the
blink reflex in normal human subjects. Exp Brain Res 1999;129:49–56.51. Heilman KM. Exploring the enigmas of frontal lobe dysfunction. Geriatrics 1976;31:81–87.52. Dehen H, Bathien N, Cambier J. The palmo-mental reflex. An electrophysiological study. Eur Neurol 1975;13:395–404.53. Jenny AB, Saper CB. Organization of the facial nucleus and corticofacial projection in the monkey: a reconsideration
of the upper motor neuron facial palsy. Neurology 1987;37:930–939.54. Maertens de Noordhout A, Delwaide PJ. The palmomental reflex in Parkinson’s disease. Comparisons with normal
subjects and clinical relevance. Arch Neurol 1988;45:425–427.55. Kimura J. Disorders of interneurons in parkinsonism. The orbicularis oculi reflex to paired stimuli. Brain 1973;96:87–96.56. Smith SJ, Lees AJ. Abnormalities of the blink reflex in Gilles de la Tourette syndrome. J Neurol Neurosurg Psychiatry
1989;52:895–898.57. Eekhof JL, Aramideh M, Bour LJ, Hilgevoord AA, Speelman HD, Ongerboer de Visser BW. Blink reflex recovery
curves in blepharospasm, torticollis spasmodica, and hemifacial spasm. Muscle Nerve 1996;19:10–1558. Basso MA, Powers AS, Evinger C. An explanation for reflex blink hyperexcitability in Parkinson’s disease. I. Superior
colliculus. J Neurosci 1996;16:7308–7317.59. Basso MA, Evinger C. An explanation for reflex blink hyperexcitability in Parkinson’s disease. II Nucleus raphe
magnus. J Neurosci 1996;16:7318–7330.60. Cruccu G, Pauletti G, Agostino R, Berardelli A, Manfredi M. Masseter inhibitory reflex in movement disorders.
Huntington’s chorea, Parkinson’s disease, dystonia, and unilateral masticatory spasm. Electroenceph Clin Neurophysiol1991;81:24–30.
61. Alfonsi E, Nappi G, Pacchetti C, et al. Changes in motoneuron excitability of masseter muscle following exteroceptivestimuli in Parkinson’s disease. Electroencephalogr Clin Neurophysiol 1993;89:29–34
62. Deuschl G, Goddemeier C. Spontaneous and reflex activity of facial muscles in dystonia, Parkinson’s disease, and innormal subjects. J Neurol Neurosurg Psychiatry 1998;64:320–324.

Neurophysiology of Atypical Parkinsonism 427
63. Davis M, Gendelman DS, Tischler MD, Gendelman PM. A primary acoustic startle circuit: lesion and stimulationstudies. J Neurosci 1982;2:791–805.
64. Brown P, Rothwell JC, Thompson PD, Britton TC, Day BL, Marsden CD. The hyperekplexias and their relationship tothe normal startle reflex. Brain 1991;114:1903–1928.
65. Zweig RM, Whitehouse PJ, Casanova MF, Walker LC, Jankel WR, Price DL. Loss of pedunculopontine neurons inprogressive supranuclear palsy. Ann Neurol 1987;22:18–25.
66. Malessa S, Hirsch EC, Cervera P, et al. Progressive supranuclear palsy: loss of cholinergic acetyltransferase-likeimmunoreactive neurons in the pontine reticular formation. Neurology 1991;41:1593–1597.
67. Juncos JL, Hirsch EC, Malessa S, Duyckaerts C, Hersh LB, Agid Y. Mesencephalic cholinergic nuclei in progressivesupranuclear palsy. Neurology 1991;41:25–30.
68. Valls-Solé J, Solé A, Valldeoriola F, Muñoz E, González LE, Tolosa ES. Reaction time and acoustic startle. NeurosciLett 1995;195:97–100
69. Valls-Solé J, Valldeoriola F, Tolosa E, Nobbe F. Habituation of the startle reaction is reduced during preparation forexecution of a motor taskin normal human subjects. Brain Res 1997;751:155–159.
70. Valls-Solé J, Rothwell JC, Goulart F, Cossu G, Muñoz JE. Patterned ballistic movements triggered by a startle inhealthy humans. J Physiol 1999;516:931–938.
71. Valldeoriola F, Valls-Solé J, Toloa E, Nobbe FA, Muñoz JE, Martí MJ. The acoustic startle response is normal inpatients with multiple system atrophy. Mov Disord 1997;12:697–700.
72. Kofler M, Müller J, Seppi K, Wenning GK. Exaggerated auditory startle responses in multiple system atrophy: a com-parative study of parkinson and cerebellar subtypes. Clin Neurophysiol 2003;114:541–547.
73. Kofler M, Müller J, Wenning G, et al. The auditory startle reaction in parkinsonian syndromes. Mov Disord 2001;16:62–71.
74. Ison JR, Sanes JN, Foss JA, Pinckney LA. Facilitation and inhibition of the human startle blink reflexes by stimulusanticipation. Behav Neurosci 1990;104:418–429.
75. Nakashima K, Shimoyama R, Yokoyama Y, Takahashi K. Auditory effects on the electrically elicited blink reflex inpatients with Parkinson’s disease. Electroenceph Clin Neurophysiol 1993;89:108–112.
76. Lozza A, Pepin JL, Rapisarda G, Moglia A, Delwaide PJ. Functional changes of brainstem reflexes in Parkinson’sdisease. Conditioning of the blink reflex R2 component by paired and index finger stimulation. J Neural Transm1997;104:679–687.
77. Valls-Solé J. Neurophysiological characterization of parkinsonian syndromes. Neurophysiol Clin 2000;30:352–367.78. Pierrot-Deseilligny E, Mazières L. Circuits réflexes de la moelle epinière chez l’homme. Rev Neurol 1984;140(Part
I):605–61479. Pierrot-Deseilligny E, Mazières L. Circuits réflexes de la moelle epinière chez l’homme. Rev Neurol 1984;140(Part
II):681–694.80. Rossignol S, Jones GM. Audio-spinal influence in man studied by the H-reflex and its possible role on rhythmic move-
ments synchronized to sound. Electroenceph Clin Neurophysiol 1976;41:83–92.81. Delwaide P, Pepin JL, Maertens de Noordhout A. The audiospinal reaction in Parkinsonian patients reflects functional
changes in reticular nuclei. Ann Neurol 1993;33:63–6982. Valls-Solé J, Valldeoriola F. Neurophysiological correlate of clinical signs in Parkinson’s disease. Clinical Neuro-
physiology 2002;113:792–805.83. Wenning GK, Ben Shlomo Y, Magalhaes M, Daniel SE, Quinn NP. Clinical features and natural history of multiple
system atrophy. An analysis of 100 cases. Brain 1994;117:835–845.84. Salazar G, Valls-Solé J, Martí MJ, Chang H, Tolosa ES. Postural and action myoclonus in patients with parkinsonian
type multiple system atrophy. Mov Disord 2000;15:77–83.85. Gouider-Khouja N, Vidailhet M, Bonnet AM, Pichon J, Agid Y. “Pure” striatonigral degeneration and Parkinson’s
disease: a comparative clinical study. Mov Disord 1995;10:288–294.86. Patel S, Slater P. Analysis of the brain regions involved in myoclonus produced by intracerebral picrotoxin. Neuro-
science 1987;20:687–693.87. Thompson PD, Day BL, Rothwell JC, Brown P, Britton TC, Marsden CD. The myoclonus in corticobasal degeneration.
Evidence for two forms of cortical reflex myoclonus. Brain 1994;117:1197–1208.88. Gibb WRG, Luthert PJ, Marsden CD. Corticobasal degeneration Brain 1989;112:1171–1192.89. Brunt ERP, vanWeerden TW, Pruim J, Lakke JWPF. Unique myoclonic pattern in corticobasal degeneration. Mov
Disord 1995;10:132–142.90. Sutton GG, Mayer RF. Focal reflex myoclonus. J Neurol Neurosurg Psychiatry 1974;37:207–217.91. Mauguière F, Desmedt JE, Courjon J. Astereognosis and dissociated loss of frontal or parietal components of soma-
tosensory evoked potentials in hemispheric lesions: detailed correlations with clinical signs and computerized tomo-graphic scanning. Brain 1983;106:271–311.
92. Caccia MR, McComas AJ, Upton ARM, Blogg T. Cutaneous reflexes in small muscles of the hand. J Neurol NeursurgPsychiatry 1973;36:960–977.

428 Valls-Solé
93. Jenner JR, Stephens JA. Cutaneous reflex responses and their central nervous pathways studied in man. J Physiol1982;333:405-419.
94. Gilman S, Low PA, Quinn N, et al. Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci1999;163:94–98.
95. Horimoto Y, Matsumoto M, Akatsu H, et al. Autonomic dysfunctions in dementia with Lewy bodies. J Neurol2003;250:530–533.
96. Benarroch EE, Chang FLF. Central autonomic disorders. J Clin Neurophysiol 1993;10:39–50.97. Holand S, Girard A, Laude D, Meyer-Bisch C, Elghozi JL. Effects of an auditory startle stimulus on blood pressure and
heart rate in humans. J Hypertens 1999;17:1893–1897.98. Valls-Solé J, Veciana M, León L, Valldeoriola F. Effects of a startle on heart rate in patients with multiple system
atrophy. Mov Disord 2002;17:546–549.99. Shahani BW, Halperin JJ, Boulu P, Cohen J. Sympathetic skin response: a method of assessing unmyelinated axon
dysfunction in peripheral neuropathies. J Neurol Neurosurg Psychiatry 1984;47:536–542.100. Bordet R, Benhadjali J, Destee A, Hurtevent JF, Bourriez JL, Guieu JD. Sympathetic skin response and R-R interval
variability in multiple system atrophy and idiopathic Parkinson’s disease. Mov Dis 1996;11:268–272.101. Baser SM, Meer J, Polinsky RJ, Hallett M. Sudomotor function in autonomic failure. Neurology 1991;41:1564–1566.102. Plazzi G, Corsini R, Provini F, et al. REM sleep behavior disorders in multiple system atrophy. Neurology
1997;48:1094–1097.103. Bannister R, Gibson W, Michaels L, Oppenheimer DR. Laryngeal abductor paralsysis in multiple system atrophy. A
report on three necropsied cases, with observation on the laryngeal muscles and the nuclei ambigui. Brain1981;104:351–368.
104. Isozaki E, Naito A, Horiguchi S, Kawamura R, Hayashida T, Tanabe H. Early diagnosis and stage classification of vocalcord abductor paralysis in patients with multiple system atrophy. J Neurol Neurosurg Psychiatry 1996;60:399–402.
105. Iranzo A, Santamaría J, Tolosa E, et al. Continuous positive air pressure eliminates nocturnal stridor in multiple systematrophy. The Lancet 2000;356:1329–1330.
106. Turner RS. Idiopathic rapid eye movement sleep behavior disorder is a harbinger of dementia with Lewy bodies. J GeriatrPsychiatry Neurol 2002;15:195–199.
107. Boeve BF, Silber MH, Parisi JE, et al. Synucleinopathy pathology and REM sleep behavior disorder plus dementia orparkinsonism. Neurology 2003;61:40–45.
108. Kirby R, Fowler CJ, Gosling J, Bannister R. Urethro-vesical dysfunction in progressive autonomic failure with mul-tiple system atrophy. J Neurol Neurosurg Psychiatry 1986;49:554–562.
109. Sakuta M, Nakanishi T, Toyokura Y. Anal muscle electromyograms differ in amyotrophic lateral sclerosis and Shy–Drager syndrome. Neurology 1978;28:1289–1293.
110. Eardley I, Quinn NP, Fowler CJ, et al. The value of urethral sphincter electromyography in the differential diagnosis ofparkinsonism. Br J Urol 1989;64:360–362.
111. Valldeoriola F, Valls-Solé J, Tolosa ES, Martí MJ. Striated anal sphincter denervation in patients with progressivesupranuclear palsy. Mov Disord 1995;10:550–555.
112. Giladi N, Simon ES, Korczyn AD, et al. Anal sphincter EMG does not distinguish between multiple system atrophy andParkinson’s disease. Muscle Nerve 2000;23:731–734.
113. Rodi Z, Denislic M, Vodusek DB. External anal sphincter electromyography in the differential diagnosis of parkin-sonism. J Neurol Neurosurg Psychiatry 1996;60:460–461.
114. Libelius R, Johansson F. Quantitative electromyography of the external anal sphincter in Parkinson’s disease and mul-tiple system atrophy. Muscle Nerve 2000;23:1250–1256.
115. Kiff ES, Swash M. Slowed conduction in the pudendal nerves in idiopathic (neurogenic) faecal incontinence. Br J Surg1984;71:614–616.
116. Podnar S, Vodusek DB. Standardization of anal sphincter electromyography: effect of chronic constipation. MuscleNerve 2000;23:1748–1751.
117. Abbruzzese G, Marchese R, Trompetto C. Sensory and motor evoked potentials in multiple system atrophy: a compara-tive study with Parkinson’s disease. Mov Disord 1997;12:315–321.
118. Cruz Martinez A, Arpa J, Alonso M, Palomo F, Villoslada C. Transcranial magnetic stimulation in multiple system andlate onset cerebellar atrophies. Acta Neurol Scand 1995;92:218–224.
119. Lu CS, Ikeda A, Terada K, et al. Electrophysiological studies of early stage corticobasal degeneration. Mov Disord1998;13:140–146.
120. Strafella A, Ashby P, Lang AE. Reflex myoclonus in cortical-basal ganglionic degeneration involves a transcorticalpathway. Mov Disord 1997;12:360–369.
121. Goldberg G, Mayer NH, Toglia JU. Medial frontal cortex infarction and the alien hand sign. Arch Neurol 1981;38:683–686.
122. Feinberg TE, Schindler RJ, Flanagan NG, Haber LD. Two alien hand syndromes. Neurology 1992;42:19–24.

Neurophysiology of Atypical Parkinsonism 429
123. Valls-Solé J, Tolosa E, Martí MJ, et al. Examination of motor output pathways in patients with corticobasal ganglionicdegeneration using transcranial magnetic stimulation. Brain 2001;124:1131–1137.
124. Marchese R, Trompetto C, Buccolieri A, Abbruzzese G. Abnormalities of motor cortical excitability are not correlatedwith clinical features in atypical parkinsonism. Mov Disord 2000;15:1210–1214.
125. Hanajima R, Ugawa Y, Terao Y, Ogata K, Kanazawa I. Ipsilateral cortico-cortical inhibition of the motor cortex invarious neurological disorders. J Neurol Sci 1996;140:109–116.
126. Frasson E, Bertolasi L, Bertasi V, et al. Paired transcranial magnetic stimulation for the early diagnosis of corticobasalganglionic degeneration. Clin Neurophysiol 2003;114:272–278.
127. Goulart F, Valls-Solé J, Alvarez R. Posture-related modification of soleus H reflex excitability. Muscle Nerve2000;23:925–932.
128. Rossini PM, Babiloni F, Bernardi G, et al. Abnormalities of short-latency somatosensory evoked potentials in parkinso-nian patients. Electroenceph Clin Neurophysiol 1989;74:277–289.
129. Rossini PM, Filippi MM, Vernieri F. Neurophysiology of sensorimotor integration in Parkinson’s disease. Clin Neurosci1998;5:121–130.
130. Kofler M, Müller J, Reggiani L, Wenning GK. Somatosensory evoked potentials in progressive supranuclear palsy.J Neurol Sci 2000;179:85–91.
131. Miwa H, Mizuno Y. Enlargements of somatosensory-evoked potentials in progressive supranuclear palsy. Acta NeurolScand 2002;106:209–212.
132. Deecke L, Englitz HG, Kornhuber HH, Schmitt G. Cerebral potential preceding voluntary movement in patients withbilateral or unilateral Parkinson akinesia. In: Desmedt JE, ed. Progress in Clinical Neurophysiology, vol. 1. Basel:Karger, 1977:151–163.
133. Rizzo V, Siebner HR, Modugno N, et al. Shaping the excitability of human motor cortex with premotor rTMS. J Physiol2004;554:483–495.
134. Pascual-Leone A, Valls-Sole J, Brasil-Neto JP, Cammarota A, Grafman J, Hallett M. Akinesia in Parkinson’s disease.II. Effects of subthreshold repetitive transcranial motor cortex stimulation. Neurology 1994;44:892–898.
135. Ikeguchi M, Touge T, Nishiyama Y, Takeuchi H, Kuriyama S, Ohkawa M. Effects of successive repetitive transcranialmagnetic stimulation on motor performances and brain perfusion in idiopathic Parkinson’s disease. J Neurol Sci2003;209:41–46.
136. Okabe S, Ugawa Y, Kanazawa I. Effectiveness of rTMS on Parkinson’s Disease Study Group. 0.2-Hz repetitivetranscranial magnetic stimulation has no add-on effects as compared to a realistic sham stimulation in Parkinson’sdisease. Mov Disord 2003;18:382–388.
137. Gerschlager W, Alesch F, Cunnington R, et al. Bilateral subthalamic nucleus stimulation improves frontal cortex functionin Parkinson’s disease. An electrophysiological study of the contingent negative variation. Brain 1999;122:2365–2373.

![Vascular parkinsonism · Vascular parkinsonism – REVIEW future science groupfuture science group 239 20%) suffered from parkinsonism with strong evidence of CVD [23]](https://img.pdfslide.us/doc/110x75/5c12e69c09d3f208438bb500/vascular-parkinsonism-vascular-parkinsonism-review-future-science-groupfuture.jpg)