Embed Size (px)
Citation preview
Neurophysiological Basis of Movement
World VI:Motor Disorders

Sites of Damage in Nerve and Muscle
Site Disorder
Neuron cell body ALS (Lou Gehrig’s disease)Root Cervical or lumbar radiculopathyAxon Axonal neuropathyDemyelination Guillain-Barré syndromeNeuromuscular synapse Myasthenia gravisMuscle Muscular dystrophy
Lecture 30: Peripheral Muscularand Neurological Disorders
Muscular Dystrophies
Genetic diseases: progressive weakness and degeneration of skeletal muscles
Duchenne and Becker dystrophy—1 in 3,500 to 5,000 births
Mostly males are affected
Mutation of a gene responsible for dystrophin, a protein involved in maintaining integrity of muscle fibers
Clinical symptoms at 2 to 6 years; all muscles are affected
Late to walk; waddling, unsteady gait
Respirator dependence by the age of 20
Muscular Dystrophies:Duchenne Dystrophy
Similar to Duchenne dystrophy; mutation of a gene responsible for dystrophin
Clinical symptoms appear at adolescence
Slower disease progression; longer life expectancy
Muscular Dystrophies:Becker Dystrophy

Most common adult form of muscular dystrophy
Myotonia: prolonged episode of muscle activity after its voluntary contraction
Commonly in finger and facial muscles
High-stepping, floppy-footed gait
Long face; drooping eyelids
Muscular Dystrophies:Myotonic Dystrophy
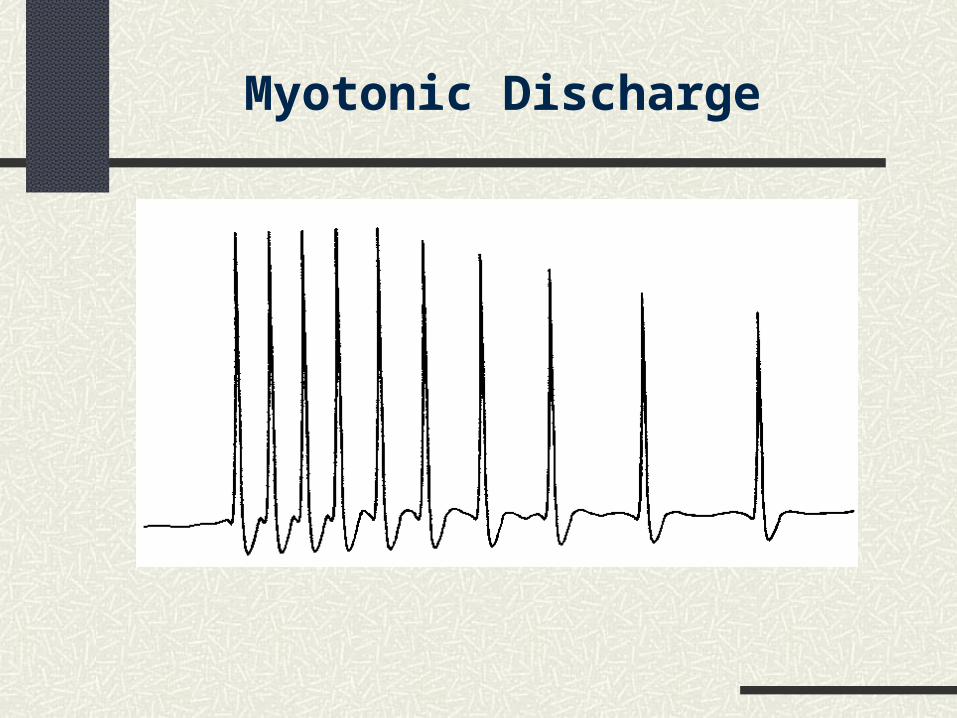
Myotonic Discharge

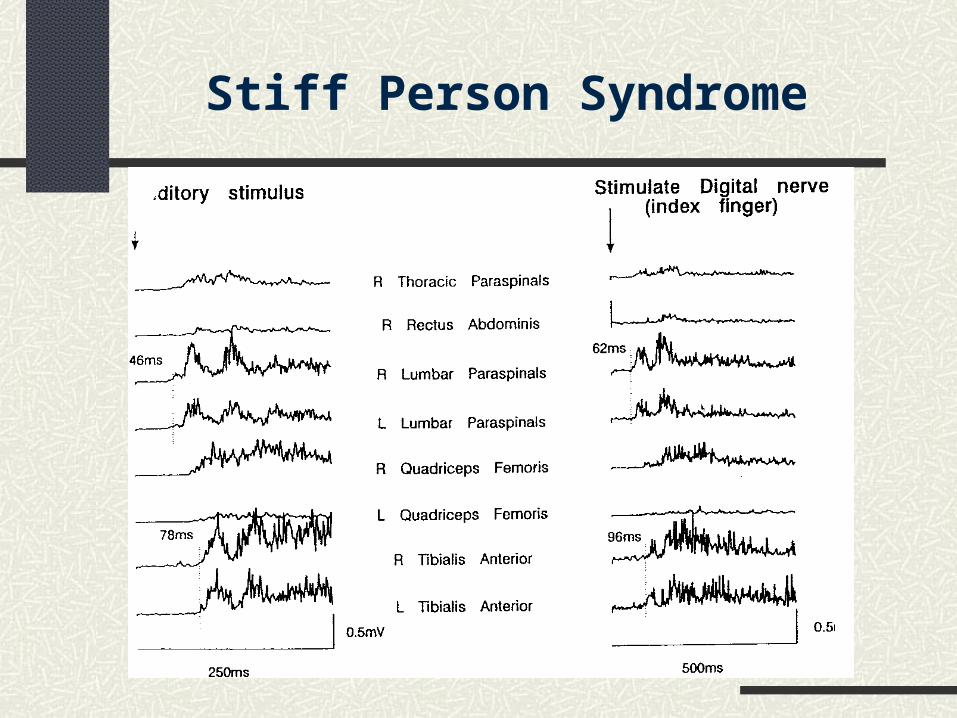
Stiff Person Syndrome
Excessive motoneuron excitation
Starts at 30 to 60 years of age
Leads to boardlike rigidity of trunk muscles
Stiff Person Syndrome

Continuous Muscle FiberActivity Syndromes
The toxin blocks postsynaptic inhibition at the spinal level.
EMG bursts can be stopped by neuromuscular or peripheral nerve block.
Discharges are attenuated during sleep and under general or spinal anesthesia.
Tetanus (induced by tetanus toxin):
Excessive motoneuron excitation Coactivation of agonist–antagonist muscles Proximal muscles are particularly involved
Stiff person syndrome:
Continuous activity of single muscle fibers Seen at rest and on the background of vol. activation Defect probably in the motor axon terminals
Neuromyotonia:
Continuous Muscle FiberActivity Syndromes
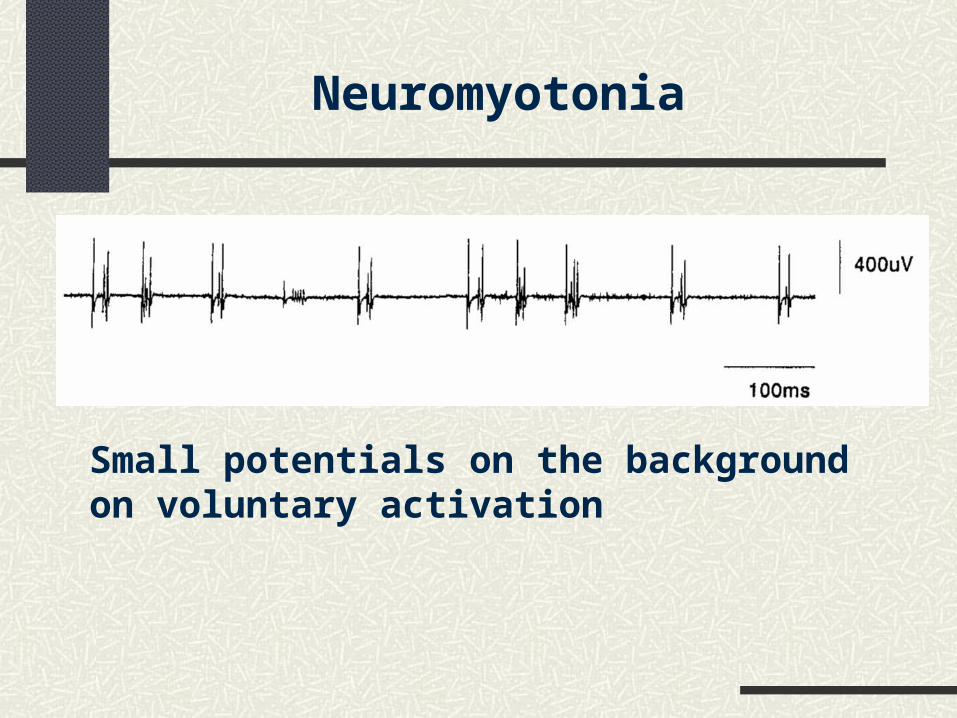
Neuromyotonia
Small potentials on the background on voluntary activation
Myasthenia Gravis
– fatigue, exhaustion, muscle atrophy
– any muscle(s) can be affected, but especially eye, face, lip, tongue, throat, neck, and limb muscles
– ocular signs (eyelid droop; inability to open one eye)
– facial weakness (stiffness of the face; difficulties with chewing, swallowing, laughing, and speech [dysarthria])
– may lead to ventilatory insufficiency and death
Disorder of transmission at the neuromuscular synapse
Clinical signs:
3 to 4 new cases per million annually
Prevalence: 60 cases per million
Can start at any age
Women are affected 2:1 over men
Death rate in the 1930s was 40%; death rate in the 1970s–1980s was 7%
Myasthenia Gravis: Epidemiology
Autoimmune process (the body produced antibodies to ACh receptors)
Reduction of ACh receptors
Reduction of postsynaptic potentials
Myasthenia Gravis: Physiology
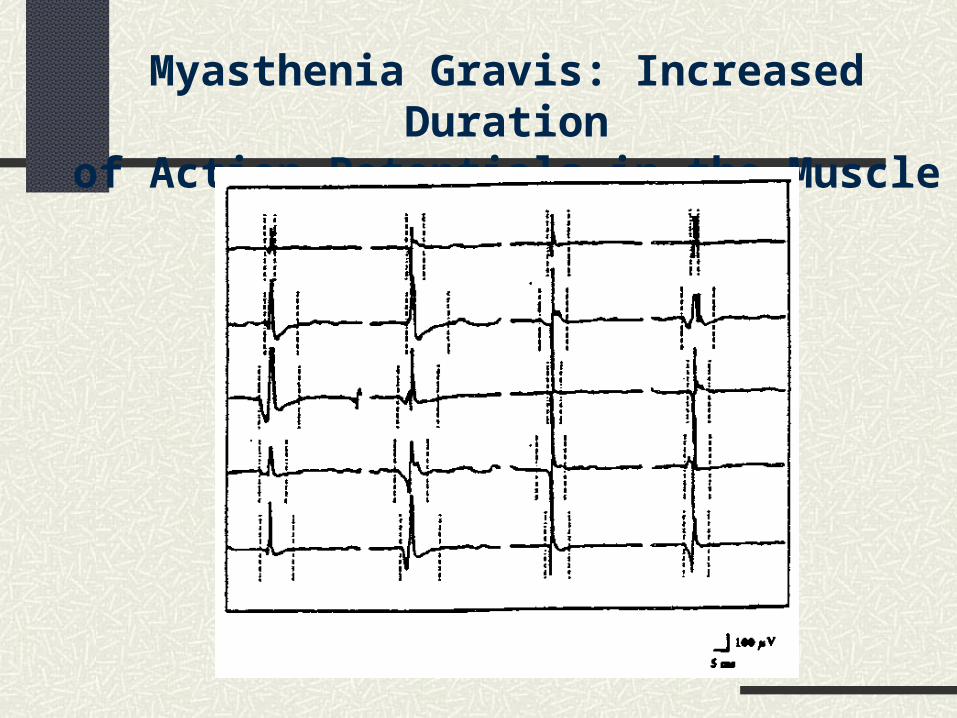
Myasthenia Gravis: Increased Durationof Action Potentials in the Muscle
ACh-esterase inhibitors (neostigmine, distigmine)
Thymectomy to suppress autoimmune processes
Plasmapheresis to remove autoimmune antibodies
Side effects with any treatment
Myasthenia Gravis: Treatment
Peripheral Neuropathies:Mononeuropathies
Slowed conduction in a single nerve Reduced amplitude of motor and/or sensory potentials Signs of denervation Carpal tunnel syndrome: entrapment of the median nerve
at the wrist Ulnar nerve can be entrapped near the elbow Brachial plexus lesions: mostly seen in muscles innervated
by median and ulnar nerves Peroneal: peroneal pressure palsy Tibial: tarsal tunnel syndrome Sciatic
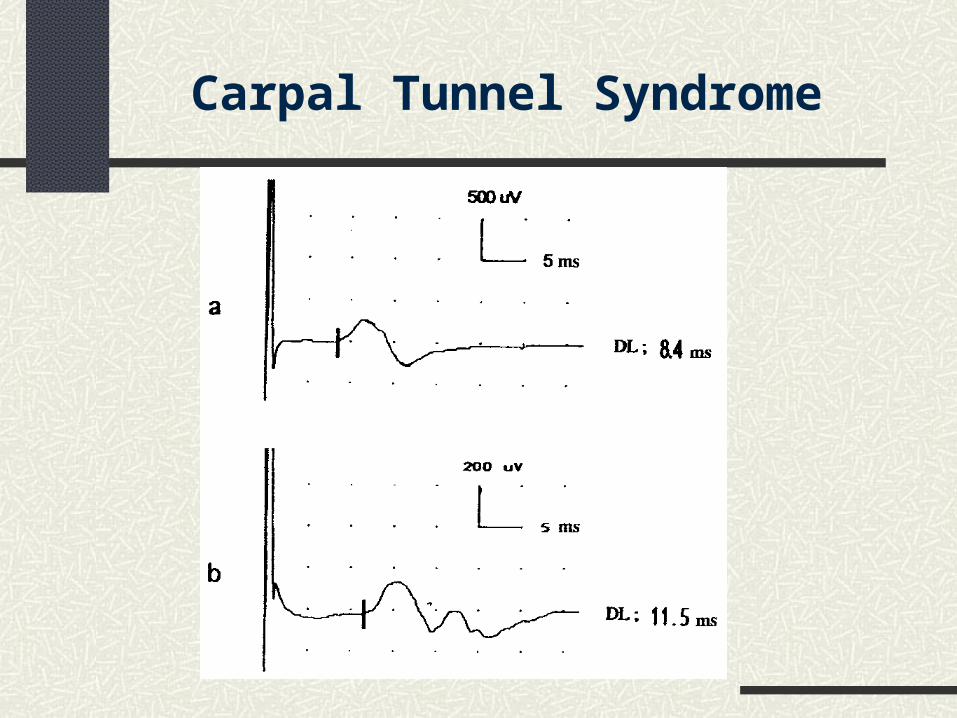
Carpal Tunnel Syndrome
Diabetes mellitus
Polyarteritis nodosa (connective tissue disorder, vasculitis)
Leprosy
Peripheral Neuropathies:Multiple Mononeuropathies
Diabetes (Diabetes Mellitus):Impaired Ability to Metabolize Glucose
Total number of cases in the U.S.: 16 million
Yearly increase: 650,000 new cases
Long-term complications:
– Peripheral sensory neuropathy
– Peripheral motor neuropathy
– Loss of autonomic nerve function
– Atrophy of peripheral tissues
Diabetes
Clinically apparent peripheral nerve damage occurs: In 25% of patients after 10 years
In 50% of patients after 20 years
Consequences: Loss of balance and coordination
Increased probability of falls, fractures, bruises, etc.
Lower during vibration of Achilles tendon
Higher during vibration of hamstrings
Effects of muscle vibration on posture:
Reorganization of postural control: switch to alternative sources of information
Diabetes
Consequence of Diabetes:Atrophy of Peripheral Tissues
Is it a consequence of inadequate blood supply?
Is it a consequence of abnormal pressure distribution with foci of high pressure?
Studies by the group of Peter Cavanagh
VIF
VIF
VIF
VIF
Diabetes
May be associated with demyelinating neuropathies
Guillain-Barré syndrome: reduced recruitment; conduction block; may result in permanent axonal loss
Chronic inflammatory demyelinating polyneuropathy: common recovery, but nerve conduction velocity may remain slow
Peripheral Neuropathies:Polyneuropathies

– Amyotrophic lateral sclerosis (Lou Gehrig’s disease)
– Poliomyelitis (enterovirus destroying anterior horn cells; EMGs show chronic denervation; may lead to weakness and pain—a postpolyo syndrome)
Axonal neuropathies (mostly of toxic origin)
Neuronal degenerations:
Peripheral Neuropathies:Polyneuropathies
ALS
20,000 Americans have ALS (one in 15,000). 5,000 people in the United States are diagnosed with
ALS each year. Men are affected more often than women. ALS most commonly strikes people between 40 and
60 years of age. About 5 to 10 percent of all ALS cases are inherited. About 20 percent of all familial cases result from a
specific genetic defect: mutation of superoxide dismutase 1 (SOD1).
The earliest symptoms may include twitching, cramping, or stiffness of muscles; muscle weakness affecting an arm or a leg; slurred and nasal speech; or difficulty chewing or swallowing.
Patients have increasing problems with moving, swallowing (dysphagia), and speaking or forming words (dysarthria).
Patients have tight and stiff muscles (spasticity) and exaggerated reflexes (hyperreflexia).
ALS