Embed Size (px)
Citation preview
Journal of Neurology, Neurosurgery, and Psychiatry, 1980, 43, 63-67
Neurophysiological assessment of alpha pattern comaJ A OBESO, MI IRAGUI, JF MARTI-MASSO, E MARAVI, JM TEIJEIRA,N CARRERA, AND J TEIJEIRA
From the division of Neurology, Residencia Sanitaria, San Sebastian, and the Department of Clinical Neuro-physiology and division ofNeurology, Residencia Sanitaria, Pamplona, Spain
S U M M A R Y Somatosensory evoked potentials, blink reflexes, andH wave reflexes, were recorded onseveral days from three patients with alph pattern coma. Coma was secondary to cardiac arrest in twocases and to brainstem infarction in one. Results are compatible with damage to the brainstemreticular formation with sparing of thalamo-cortical circuits as the main physiopathological charac-teristic of alpha pattern coma. This condition should not be regarded as a discrete entity whenestablishing the prognosis of patients in coma, since they only differ from other patients in coma fromthe point view of the EEG record.
Comatose patients whose electroencephalographicactivity is predominantly of alpha frequency havebeen the subject of several reports over the lastfew years. Early publications correlated brain-stem lesions, particularly in the pons, with theappearance of this type of EEG tracing,`4 andonly recently have there been reports of alphapattern coma in patients after cardiopulmonaryarrest.57 The general opinion is that alphapattern coma has an extremely bad prognosis, butrecent evidence indicates that the chance ofsurvival is no lower in comatose patients withEEG rhythm of alpha frequency than in thosein coma associated with slow EEG waves.8Whether the alpha pattern represents a patho-
logical rhythm or retained normal activity hasnot been elucidated. In the present paper wedescribe a detailed electrophysiological study ofthree patients with alpha pattern coma, and theneuropathological data from one of them.
Case reports
CASE 1A 72 year old woman was admitted to hospitalbecause she was dysarthric and complained ofunsteady gait. By the time she reached hospitalshe was in coma and her pupils were myotic butreactive to light. Horizontal oculocephalic move-
Address for reprint requests: Dr JA Abeso, Augusto Linares 4,Torrelavega, Santander, Spain.
Accepted 27 June 1979
ments were normally present, but vertical move-ments could not be elicited. Corneal reflexes werepresent bilaterally. Her extremities were diffuselyrigid, and plantar responses were extensor. Fivedays later the patient showed spontaneousdecerebrate motor posture on both sides of herbody. Oculocephalic and oculovestibular reflexeswere no longer present; breathing was spon-taneous. On the thirteenth day in hospital hertemperature rose to 41°C, with a respiratoryinfection. Breathing became irregular and mech-anical respiration was needed. Three days latershe died. The brain necropsy revealed thrombosisof the basilar artery with infarction involving theentire rostral two-thirds of the basis pontisbilaterally, with scattered ischaemic lesions in thetegmentum (fig 1). The infarct also involvedboth sides of the cerebellum.
CASE 2
A 55 year old man had a sustained period ofcardiac arrest during a traffic accident, afterwhich he remained unconscious. On admission,pupils were in mid position and reactive to light.His extremities were diffusely rigid, and a rightextensor plantar response was noted. Cornealreflexes were depressed but present on both sides.Oculocephalic movements were normal; breath-ing was regular. Two days later, a right lobarpneumonia became an important hazard, and thepatient died four days after the cardiac arrest.Data from necropsy could not be obtained.
63
Protected by copyright.
on 3 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.43.1.63 on 1 January 1980. D
ownloaded from

64 J A Obeso, M I Iragui, J F Marti-Masso, E Maravi, J M Teijeira, N Carrera, and J Teijeira
Fig. 1 Myelin sheath stain of a transverse section through the rostralpart of the pons in case 1. Extensive infarction ofthe basispontis is observed, with scattered lesions appearing on the tegmentum.
CASE 3
This 48 year old man suffered a cardiac infarc-tion and secondary cardiac arrest while comingto the hospital. On admission he was in coma,pupils were myotic, oculocephalic and cornealreflexes were normal bilaterally, and lower limbswere slightly hypotonic but tendon jerk reflexescould be elicited easily. An extensor plantarresponse was noted on the right. Breathing wasnormal. The ECG showed signs of acute anteriormyocardial infarction. On the following days thepupils were clearly reactive to light, but no othersign of recovery was observed. Eight days afteradmission, he had a new and irreversible cardiacarrest. Necropsy was not performed.
Neurophysiological procedure
The EEG was recorded with an eight channelportable aapparatus. Spin electrodes of 7 mm
diameter were used for recording of both theEEG and somatosensory evoked potentials(SEPs). They were placed according to the 10-20system.9 All patients were stimulated by handclaps, light flashes, and pinching of the extremi-ties. Electroencephalograms were recorded everytwo or three days, thus case 1 had eight tracingat daily intervals. Case 2 had only three record-ings, and case 3 had five EEGs. Somatosensoryevoked potentials were elicited by median nervestimulation at the wrist, using a stimulus ampli-tude of 10% above the motor threshold for theopponens pollicis muscle. The stimulation ratewas 0-5 per second. The active electrode wasplaced 20 mm behind C3 and C4, while thereference electrode was on the midfrontal region(F.). One set of tests consisted of 256 responses,repeated two or three times. Analysis time was200 ms, and the amplifiers had a flat frequencyresponse from 2 to 1000 Hz and a high frequency
Protected by copyright.
on 3 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.43.1.63 on 1 January 1980. D
ownloaded from
Neurophysiological assessment of alpha pattern coma
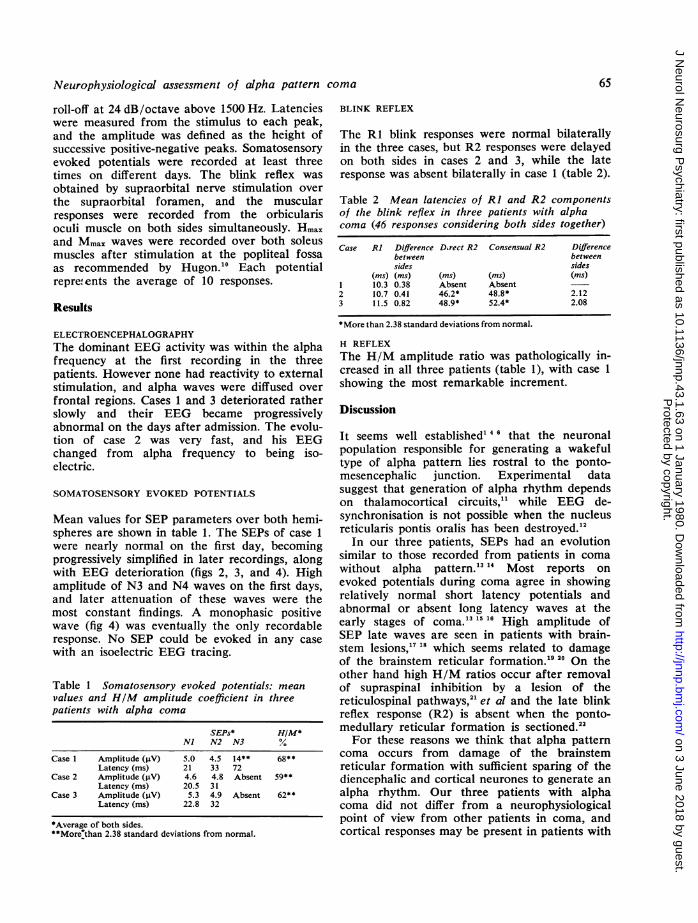
roll-off at 24 dB/octave above 1500 Hz. Latencieswere measured from the stimulus to each peak,and the amplitude was defined as the height ofsuccessive positive-negative peaks. Somatosensoryevoked potentials were recorded at least threetimes on different days. The blink reflex wasobtained by supraorbital nerve stimulation over
the supraorbital foramen, and the muscularresponses were recorded from the orbicularisoculi muscle on both sides simultaneously. Hmaxand Mmax waves were recorded over both soleusmuscles after stimulation at the popliteal fossaas recommended by Hugon.'0 Each potentialrepre. ents the average of 10 responses.
Results
ELECTROENCEPHALOGRAPHYThe dominant EEG activity was within the alphafrequency at the first recording in the threepatients. However none had reactivity to externalstimulation, and alpha waves were diffused overfrontal regions. Cases 1 and 3 deteriorated ratherslowly and their EEG became progressivelyabnormal on the days after admission. The evolu-tion of case 2 was very fast, and his EEGchanged from alpha frequency to being iso-electric.
SOMATOSENSORY EVOKED POTENTIALS
Mean values for SEP parameters over both hemi-spheres are shown in table 1. The SEPs of case 1
were nearly normal on the first day, becomingprogressively simplified in later recordings, alongwith EEG deterioration (figs 2, 3, and 4). Highamplitude of N3 and N4 waves on the first days,and later attenuation of these waves were themost constant findings. A monophasic positivewave (fig 4) was eventually the only recordableresponse. No SEP could be evoked in any case
with an isoelectric EEG tracing.
Table 1 Somatosensory evoked potentials: mean
values and HIM amplitude coefficient in threepatients with alpha coma
SEPs* HIM*Ni N2 N3 %
Case 1 Amplitude (pV) 5.0 4.5 14** 68**Latency (ms) 21 33 72
Case 2 Amplitude (j±V) 4.6 4.8 Absent 59**Latency (ms) 20.5 31
Case 3 Amplitude (gV) 5.3 4.9 Absent 62**Latency (ms) 22.8 32
*Average of both sides."*More7than 2.38 standard deviations from normal.
BLINK REFLEX
The RI blink responses were normal bilaterallyin the three cases, but R2 responses were delayedon both sides in cases 2 and 3, while the lateresponse was absent bilaterally in case 1 (table 2).
Table 2 Mean latencies of RI and R2 componentsof the blink reflex in three patients with alphacoma (46 responses considering both sides together)
Case RI Difference D.rect R2 Consensual R2 Differencebetween betweensides sides
(ms) (ms) (ms) (ms) (ms)1 10.3 0.38 Absent Absent2 10.7 0.41 46.2* 48.8* 2.123 11.5 0.82 48.9* 52.4* 2.08
*More than 2.38 standard deviations from normal.
H REFLEXThe H/M amplitude ratio was pathologically in-creased in all three patients (table 1), with case 1showing the most remarkable increment.
Discussion
It seems well established' 46 that the neuronalpopulation responsible for generating a wakefultype of alpha pattern lies rostral to the ponto-mesencephalic junction. Experimental datasuggest that generation of alpha rhythm dependson thalamocortical circuits," while EEG de-synchronisation is not possible when the nucleusreticularis pontis oralis has been destroyed.'2
In our three patients, SEPs had an evolutionsimilar to those recorded from patients in comawithout alpha pattern.'3 '4 Most reports onevoked potentials during coma agree in showingrelatively normal short latency potentials andabnormal or absent long latency waves at theearly stages of coma.'3 ..1 High amplitude ofSEP late waves are seen in patients with brain-stem lesions,'7 '8 which seems related to damageof the brainstem reticular formation.'9 ao On theother hand high H/M ratios occur after removalof supraspinal inhibition by a lesion of thereticulospinal pathways,2' et al and the late blinkreflex response (R2) is absent when the ponto-medullary reticular formation is sectioned.22For these reasons we think that alpha pattern
coma occurs from damage of the brainstemreticular formation with sufficient sparing of thediencephalic and cortical neurones to generate analpha rhythm. Our three patients with alphacoma did not differ from a neurophysiologicalpoint of view from other patients in coma, andcortical responses may be present in patients with
65
Protected by copyright.
on 3 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.43.1.63 on 1 January 1980. D
ownloaded from

66 J A Obeso, M I Iragui, J F Marti-Masso, E Maravi, J M Teijeira, N Carrera, and J Teijeira
30 6 77Fp- F3
F3- C3
P3-0 -ils 50jV
FP2 F -
C47 P4
P4- O2
6 7 77Fy T3
F501 _
,5- 50VF1 T4
T4 T6
T6F2
Ff02
Fig 2 EEG and SEPs of case Itwo days after admission. Alpharhythm and SEPs of normallatencies and high amplitude ofN3 wave were recorded.
Fig 3 The same record on case Ion the sixth hospital day. The EEGis slower and SEPs have lost theirlate waves.
14 7 77
F7-A1
Ts-A1 V
Oi-Al,F-A2A2
Fig 4 Marked EEG slowing alongwith a simple positive wave inboth SEPs at the final stage of lifein case 1.
alpha coma when the afferent pathways arespared, as in case 1 (fig 1). The failure of theEEG to desynchronise in most reported casesmay be related to a lesion of the nucleus reticul-aris pontis oralis, but further neuropathologicaldata from patients with alpha coma of metabolicorigin are needed to establish such a correlation.Alpha coma does not invariably portend a poorprognosis, and indeed the chance of survival orresidual disability is the same as in other in-dividuals in coma.8 Thus alpha coma should
be only considered as a dissociation betweenconsciousness and the EEG, because both pheno-mena are partially independent. Detailed neuro-physiological studies along with clinical data maybe useful in the evolution of patients with alphapattern coma, overcoming the absolute limitationof EEG recording.
We would like to thank Mrs M Martin fortechnical assistance.
30 6 77
6 7 77
5,uV 2oms
+fu
14 7 77
5MV 20ms
+
fp _ _ t_
0 -A22
Protected by copyright.
on 3 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.43.1.63 on 1 January 1980. D
ownloaded from

Neurophysiological assessment of alpha pattern coma
References
1 Loeb C, Poggio G. Electroencephalograms in a
case with ponto-mesencephalic hemorrhage.Electroencephalogr Clin Neurophysiol 1953; 5:295-6.
2 Lundervold A, Hauge T, Loken AC. UnusualEEG in unconscious patients with brainstematrophy. Electroencephal Clin Neurophysiol1956; 8:665-70.
3 Chatrian GE, White LE, Shaw CM. EEGpattern resmbling wakefulness in unresponsivedecerebrate state following traumatic brainsteminfarct. Electroencephalog Clin Neurophysiol1964; 16:285-9.
4 Wilkus RJ, Harvey F, Ojemann LM. EEG andsensory evoked potentials. Findings in an un-responsive patient with pontine infarction.Arch Neurol 1971; 24:538-44.
5 Vignaedra V, Wilkus RJ, Copass MK, ChatrianGE. Electroencephalographic rhythms of alphafrequency in comatose patients after cardio-pulmonary arrest. Neurology (Minneap) 1974;24:582-8.
6 Westmoreland BF, Klass DW, Sharbrough FW,Reagan TJ. "Alpha coma". Electroencephalo-graphic, clinical, pathological and etiologiccorrelations. Arch Neurol 1975; 32:713-8.
7 Chokroverty S. "Alpha-like" rhythms in electro-encephalograms in coma after cardiac arrest.Neurology (Minneap) 1975; 25:655-63.
8 Sorensen K, Thomassen A, Wemnberg M. Prog-nostic significance of alpha frequency EEGrhythm in coma after cardiac arrest. J NeurolNeurosurg Psychiatry 1978; 41:840-2.
9 Jasper HH. The ten-twenty electrodes system ofthe International Federation. ElectroencephalogrClin Neurophysiol 1958; 10:371-5.
10 Hugon M. Methodology of the Hoffmann reflexin man. In: Desmedt JE, ed. New Developmentsin Electromyography and Clinical Neuro-physiology, vol 3. Basel: Karger, 1973; 277-93.
11 Andersen P, Andersson SA. Thalamic origin ofcortical rhythmic activity. In: Rimond A, ed.Handbook of Electroencephalography andClinical Neurophysiology, vol 2. Amsterdam:Elsevier, 1974; 90-118.
12 Camacho-Evangelista A, Reinoso-Suarez F.
Activating and synchronizing centers in catbrain: electroencephalograms after lesions.Science 1964; 146:268-70.
13 Greenberg RP, Becker P, Miller JD, Mayer DJ.Evaluation of brain function in severe humanhead trauma with multimodality evoked poten-tials. Part 2. Localization of brain dysfunctionand correlation with posttraumatic neurologicalconditions. J Neurosurg 1977; 47:163-77.
14 Obeso JA, Teijeira JM, Marti-Masso JF et al.Somatosensory evoked potentials: abnormalitiesin brainstem lesions. Electromyogr Clin Neuro-physiology 1979; in press.
15 Arfel G. Stimulations visuelles et silencecerebral. Electroencephalogr Clin Neurophysiol1967; 23:172-5.
16 Trojaborg W, Jorgensen EO. Evoked corticalpotentials in patients with "isoelectric" EEGs.Electroencephalogr Clin Neurophysiol 1973; 35:301-9.
17 Halliday AM. Changes in the form of cerebralevoked responses in man associated with variouslesions of the nervous system. Electroen-cephalogr Clin Neurophysiol 1967; Suppl 25:178-92.
18 Obeso JA, Marti-Masso JF, Iragui MI, TeijeiraJM, Carrera N, Teijeira J. Valor de lospotenciales evocados somatosensoriales en laevaluaci6n funcional de pacientes en coma.Med Clin (Barcelona) 1979; in press.
19 Reinoso-Suarez F. Effects of diencephalic andmesencephalic lesions upon afferent impulses inthe central sensory pathways. Electroen-cephalogr Clin Neurophysiol 1963; suppl 24:33-42.
20 Cantor FK, Ilborg F. Facilitation of photicresponses by focal lesions. ElectroencephalogrClin Neurophysiol 1973; 36:214-25.
21 Pierrot E, Bussel B, Morin C. Supra-spinalcontrol of the changes induced in H-reflex bycutaneous stimulation, as studied in normal andspastic men. In: Desmedt JE, ed. New Develop-ments in Electromyography and Clinical Neuro-physiology, vol 3. Basel: Karger, 1973; 550-55.
22 Ongerboer de Visser BW, Kuypers HGJM. Lateblink reflex changes in lateral medullary lesions.Brain 1978; 101:285-94.
67
Protected by copyright.
on 3 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.43.1.63 on 1 January 1980. D
ownloaded from