Embed Size (px)
Citation preview

Neurologic Disorders Neurologic Disorders
By: David R Telles, DDSBy: David R Telles, DDSDiplomate of the American Board of Diplomate of the American Board of
Oral and Maxillofacial SurgeryOral and Maxillofacial Surgery

INTRODUCTION INTRODUCTION - Epilepsy- Epilepsy
Epilepsy is a term that describes a group of disorders Epilepsy is a term that describes a group of disorders characterized by chronic, recurrent, paroxysmal changes in characterized by chronic, recurrent, paroxysmal changes in neurologic function (seizures) that are caused by abnormal neurologic function (seizures) that are caused by abnormal and spontaneous changes in the brain.and spontaneous changes in the brain.
Seizures may be either convulsive (i.e., accompanied by Seizures may be either convulsive (i.e., accompanied by motor manifestations) or manifested by other changes in motor manifestations) or manifested by other changes in neurologic function (i.e., sensory, cognitive, emotional).neurologic function (i.e., sensory, cognitive, emotional).
The classification of epilepsy commonly accepted was The classification of epilepsy commonly accepted was developed by the International League Against Epilepsy. This developed by the International League Against Epilepsy. This classification is based on clinical behavior and classification is based on clinical behavior and electroencephalographic changes.electroencephalographic changes.

INTRODUCTIONINTRODUCTIONClassification of Epileptic SeizuresClassification of Epileptic Seizures Partial (focal, focal)Partial (focal, focal)
Simple partial seizuresSimple partial seizures Complex partial seizuresComplex partial seizures Partial seizures evolving to generalized tonic-clonic convulsionsPartial seizures evolving to generalized tonic-clonic convulsions
Generalized (convulsive or nonconvulsive)Generalized (convulsive or nonconvulsive) Absence seizures (petit mal)Absence seizures (petit mal) Atypical absence seizuresAtypical absence seizures Myclonic seizuresMyclonic seizures Clonic seizuresClonic seizures Tonic-clonic seizures (grand mal)Tonic-clonic seizures (grand mal) Tonic seizuresTonic seizures Atonic seizuresAtonic seizures Unclassified epileptic seizuresUnclassified epileptic seizures

INTRODUCTIONINTRODUCTION
Partial seizures are subdivided as Partial seizures are subdivided as simplesimple when when consciousness is preserved and consciousness is preserved and complexcomplex when when consciousness is impaired.consciousness is impaired.
Generalized seizures are more global in scope and Generalized seizures are more global in scope and manifestation. They involve an altered consciousness state manifestation. They involve an altered consciousness state and frequently abnormal motor activity.and frequently abnormal motor activity.

INCIDENCE AND INCIDENCE AND PREVALENCEPREVALENCE
It is estimated that 10% of the population will have at least It is estimated that 10% of the population will have at least one epileptic seizure in a lifetime, and that the overall one epileptic seizure in a lifetime, and that the overall incidence rate is 0.5%incidence rate is 0.5%
Seizures are most common during childhood, with as many Seizures are most common during childhood, with as many as 4% of children having at least one seizure during the first as 4% of children having at least one seizure during the first 15 years of life. Fortunately, most children outgrow the 15 years of life. Fortunately, most children outgrow the disorder.disorder.

ETIOLOGYETIOLOGY
The etiology of epilepsy is known in many cases. Common The etiology of epilepsy is known in many cases. Common causes include head trauma, developmental abnormalities, causes include head trauma, developmental abnormalities, intracranial neoplasm, hypoglycemia, drug withdrawal, and intracranial neoplasm, hypoglycemia, drug withdrawal, and febrile illness.febrile illness.
Many patients, however, have epilepsy for which there is no Many patients, however, have epilepsy for which there is no known cause. This is termed known cause. This is termed idiopathic epilepsy.idiopathic epilepsy.
Although the underlying cause of idiopathic generalized Although the underlying cause of idiopathic generalized epilepsy is unknown, seizures can sometimes be evoked by a epilepsy is unknown, seizures can sometimes be evoked by a specific stimulus. Approximately 1 out of 15 patients report specific stimulus. Approximately 1 out of 15 patients report that seizures follow exposure to a specific circumstance – that seizures follow exposure to a specific circumstance – such as flickering lights, monotonous sounds, music, or a such as flickering lights, monotonous sounds, music, or a loud noise.loud noise.
PATHOPHYSIOLOGYPATHOPHYSIOLOGY
The basic event underlying an epileptic seizure is an The basic event underlying an epileptic seizure is an excessive focal neuronal discharge that spreads to thalamic excessive focal neuronal discharge that spreads to thalamic and brainstem nuclei. The cause of this abnormal electrical and brainstem nuclei. The cause of this abnormal electrical activity is not precisely known, although a number of theories activity is not precisely known, although a number of theories have been proposed as explanations.have been proposed as explanations.
These include altered neuronal membrane potentials, altered These include altered neuronal membrane potentials, altered synaptic transmission, diminution of inhibitory neurons, synaptic transmission, diminution of inhibitory neurons, increased neuronal excitability, and decreased electrical increased neuronal excitability, and decreased electrical threshold for epileptic activity.threshold for epileptic activity.

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
A curious feature is that no specific type of brain lesion is A curious feature is that no specific type of brain lesion is absolutely correlated with epileptic seizures. absolutely correlated with epileptic seizures.
In other words. The same lesion in the same location of the In other words. The same lesion in the same location of the brain may be epileptogenic in one patient but not in another.brain may be epileptogenic in one patient but not in another.
In fact, in many cases there is no identifiable lesion at all, In fact, in many cases there is no identifiable lesion at all, which seems to suggest a biochemical abnormality.which seems to suggest a biochemical abnormality.

COMPLICATIONSCOMPLICATIONS
Approximately 60% to 80% of patients with epilepsy will Approximately 60% to 80% of patients with epilepsy will achieve complete control over their seizures; the remainder achieve complete control over their seizures; the remainder will achieve only partial or poor control.will achieve only partial or poor control.
The most serious acute complication of epilepsy is the The most serious acute complication of epilepsy is the occurrence of repeated seizures over a short time without a occurrence of repeated seizures over a short time without a recovery period. This is called recovery period. This is called status epilepticusstatus epilepticus, and it , and it constitutes a medical emergency.constitutes a medical emergency.
Patients may become seriously hypoxic and acidotic during Patients may become seriously hypoxic and acidotic during this event and suffer permanent brain damage or death.this event and suffer permanent brain damage or death.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS
The clinical manifestations of The clinical manifestations of generalized tonic-clonic generalized tonic-clonic convulsions (grand mal seizure) convulsions (grand mal seizure) are classic.are classic.
An aura (a momentary sensory An aura (a momentary sensory alteration that produces an alteration that produces an unusual smell or visual unusual smell or visual disturbance) precedes the disturbance) precedes the convulsion in one third of patients.convulsion in one third of patients.
After the aura warning, the patient After the aura warning, the patient emits a sudden cry (caused by emits a sudden cry (caused by spasm of the diaphragmatic spasm of the diaphragmatic muscles) and immediately loses muscles) and immediately loses consciousness.consciousness.

SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS
The tonic phase consists of The tonic phase consists of generalized muscle rigidity, pupil generalized muscle rigidity, pupil dilation, eyes rolling upward or to dilation, eyes rolling upward or to the side, and loss of the side, and loss of consciousness. Breathing may consciousness. Breathing may stop due to spasm of respiratory stop due to spasm of respiratory muscles.muscles.
This is followed by clonic activity This is followed by clonic activity that consists of uncoordinated that consists of uncoordinated beating movements of the limbs beating movements of the limbs and head, forcible jaw closing, and and head, forcible jaw closing, and head rocking.head rocking.

SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS
Incontinence of the urine or feces may occur.Incontinence of the urine or feces may occur.
After a few minutes, movement ceases, muscles relax, and a After a few minutes, movement ceases, muscles relax, and a gradual return to consciousness occurs that is accompanied gradual return to consciousness occurs that is accompanied by stupor, headache, confusion and depression.by stupor, headache, confusion and depression.
Several hours of rest and/or sleep may be needed to fully Several hours of rest and/or sleep may be needed to fully regain cognitive and physical abilities.regain cognitive and physical abilities.
LABORATORY FINDINGSLABORATORY FINDINGS
Seizures produce characteristic spike and wave patterns on Seizures produce characteristic spike and wave patterns on an electroencephalogram (EEG).an electroencephalogram (EEG).
Even during intervals between seizures, many epileptic Even during intervals between seizures, many epileptic patients will often demonstrate an abnormal EEG.patients will often demonstrate an abnormal EEG.
The diagnosis then is established based on the history of The diagnosis then is established based on the history of seizures and the EEG.seizures and the EEG.
Other diagnostic procedures useful to rule out other causes Other diagnostic procedures useful to rule out other causes of seizures include CAT scans, lumbar puncture, serum of seizures include CAT scans, lumbar puncture, serum chemistry profiles, and toxicology screening.chemistry profiles, and toxicology screening.

DENTAL MANAGEMENTDENTAL MANAGEMENT
1)1) Identification of patient by historyIdentification of patient by historya)a) Type of seizureType of seizure
b)b) Age at time of onsetAge at time of onset
c)c) Cause of seizures (if known)Cause of seizures (if known)
d)d) MedicationsMedications
e)e) Frequency of physician visits (name and phone number)Frequency of physician visits (name and phone number)
f)f) Degree of seizure controlDegree of seizure control
g)g) Frequency of seizuresFrequency of seizures
h)h) Date of last seizureDate of last seizure
i)i) Known precipitating factorsKnown precipitating factors
j)j) History of seizure-related injuriesHistory of seizure-related injuries

DENTAL MANAGEMENTDENTAL MANAGEMENT
2)2) Provide normal care – well controlled seizures pose no Provide normal care – well controlled seizures pose no management problemsmanagement problems
3)3) If questionable history or poorly controlled seizures, If questionable history or poorly controlled seizures, consultation with physician before dental treatment – may consultation with physician before dental treatment – may require modification of medicationsrequire modification of medications
4)4) Be alert to adverse effects of anticonvulsantsBe alert to adverse effects of anticonvulsantsa)a) DrowsinessDrowsinessb)b) Slow mentationSlow mentationc)c) DizzinessDizzinessd)d) AtaxiaAtaxiae)e) Gastrointestinal upsetGastrointestinal upsetf)f) Allergic signs (rash, erythema multiforme)Allergic signs (rash, erythema multiforme)

DENTAL MANAGEMENTDENTAL MANAGEMENT
5)5) Patients taking valproic acid (Depakene) or carbamazepine Patients taking valproic acid (Depakene) or carbamazepine (Tegetrol) may have bleeding tendencies because of (Tegetrol) may have bleeding tendencies because of platelet interference – order pretreatment bleeding time; if platelet interference – order pretreatment bleeding time; if grossly abnormal, consultation with physiciangrossly abnormal, consultation with physician
6)6) Be prepared to manage grand mal seizureBe prepared to manage grand mal seizurea)a) Consider placing a ligated mouth prop at beginning of Consider placing a ligated mouth prop at beginning of
procedureprocedureb)b) Chair back in supported supine positionChair back in supported supine position
7)7) Manage the seizureManage the seizurea)a) Clear areaClear areab)b) Turn patient to side (to avoid aspiration)Turn patient to side (to avoid aspiration)c)c) Do not attempt to use padded tongue bladeDo not attempt to use padded tongue bladed)d) Passively restrainPassively restrain

DENTAL MANAGEMENTDENTAL MANAGEMENT
8)8) After the seizureAfter the seizurea)a) Examine for traumatic injuriesExamine for traumatic injuries
b)b) Discontinue treatment, arrange for patient transportDiscontinue treatment, arrange for patient transport
In the event of status epilepticus, intravenous diazepam, In the event of status epilepticus, intravenous diazepam, 10 mg, is effective in controlling it. However, measures for 10 mg, is effective in controlling it. However, measures for respiratory support should be available because respiratory support should be available because respiratory function may be depressed postictally.respiratory function may be depressed postictally.

ORAL COMPLICATIONSORAL COMPLICATIONS
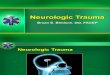
The most significant oral The most significant oral complication seen in complication seen in epileptic patients is gingival epileptic patients is gingival hyperplasia associated with hyperplasia associated with phenytoin (Dilantin).phenytoin (Dilantin).
The anterior labial surfaces The anterior labial surfaces of the maxillary and of the maxillary and mandibular gingiva are mandibular gingiva are most commonly and most commonly and severely affected.severely affected.
TREATMENT PLANNING TREATMENT PLANNING MODIFICATIONSMODIFICATIONS
Because of Dilantin-induced gingival hyperplasia, every effort must Because of Dilantin-induced gingival hyperplasia, every effort must be made to maintain a patient at an optimum level of oral hygiene. be made to maintain a patient at an optimum level of oral hygiene. This may require frequent visits for monitoring progress.This may require frequent visits for monitoring progress.
If significant hyperplasia exists, surgical reduction will be If significant hyperplasia exists, surgical reduction will be necessary; however, this must be accomplished by an increase necessary; however, this must be accomplished by an increase awareness of oral hygiene needs and a positive commitment by the awareness of oral hygiene needs and a positive commitment by the patient to maintain oral cleanliness.patient to maintain oral cleanliness.
A missing tooth or teeth should be replaced if possible to prevent A missing tooth or teeth should be replaced if possible to prevent the tongue from being caught in the edentulous space during a the tongue from being caught in the edentulous space during a seizure.seizure.
A fixed prosthesis is preferable to a removable one because a A fixed prosthesis is preferable to a removable one because a removable prosthesis is dislodged more easily. removable prosthesis is dislodged more easily.

TREATMENT PLANNING TREATMENT PLANNING MODIFICATIONSMODIFICATIONS
For fixed prosthesies, all-metal units should be considered For fixed prosthesies, all-metal units should be considered when possible to minimize the chance of fracture.when possible to minimize the chance of fracture.
When placing anterior castings, the dentist may consider When placing anterior castings, the dentist may consider using three-quarter crowns or retentive acrylic facings in lieu using three-quarter crowns or retentive acrylic facings in lieu of porcelain to facilitate repair if fracture occurs.of porcelain to facilitate repair if fracture occurs.
Removable prostheses are, nevertheless, sometimes Removable prostheses are, nevertheless, sometimes constructed for epileptic patients. Metallic palates and bases constructed for epileptic patients. Metallic palates and bases are preferable to all acrylic. If acrylic is used, it should be are preferable to all acrylic. If acrylic is used, it should be reinforced with a wire mesh.reinforced with a wire mesh.