Embed Size (px)
Citation preview

Neuroimaging Studies of Mood Disorders
Wayne C. Drevets
Neuroimaging studies of major depression have identifiedneurophysiologic abnormalities in multiple areas of theorbital and medial prefrontal cortex, the amygdala, andrelated parts of the striatum and thalamus. Some of theseabnormalities appear mood state–dependent and are lo-cated in regions where cerebral blood flow increasesduring normal and other pathologic emotional states.These neurophysiologic differences between depressivesand control subjects may thus implicate areas wherephysiologic activity changes to mediate or respond to theemotional, behavioral, and cognitive manifestations ofmajor depressive episodes. Other abnormalities persistfollowing symptom remission, and are found in orbital andmedial prefrontal cortex areas where postmortem studiesdemonstrate reductions in cortex volume and histopatho-logic changes in primary mood disorders. These areasappear to modulate emotional behavior and stress re-sponses, based upon evidence from brain mapping, lesionanalysis, and electrophysiologic studies of humans and/orexperimental animals. Dysfunction involving these regionsis thus hypothesized to play a role in the pathogenesis ofdepressive symptoms. Taken together, these findings im-plicate interconnected neural circuits in which pathologicpatterns of neurotransmission may result in the emotional,motivational, cognitive, and behavioral manifestations ofprimary and secondary affective disorders.Biol Psychi-atry 2000;48:813–829 ©2000 Society of BiologicalPsychiatry
Key Words: Positron emission tomography (PET), mag-netic resonance imaging (MRI), major depression, pre-frontal cortex, anterior cingulate, amygdala
Introduction
Neuroimaging technology provides unprecedented op-portunities for elucidating the anatomic correlates of
affective disease. Functional imaging tools such aspositron emission tomography (PET), single photon emis-sion computed tomography, and functional magnetic res-onance imaging (fMRI) have enabled in vivo character-
ization of neurophysiologic and/or receptor pharmacologiccorrelates of normal and pathologic emotional states,treatment response and resistance, and chronic or recurrentillness. Structural MRI allows assessment of neuromor-phology and neuromorphometry in primary mood disor-ders, and localization of pathology in major depressiveepisodes (MDEs) arising secondary to cerebral lesions. Invivo neuroimaging data are beginning to guide postmor-tem studies of mood disorders by delimiting areas wheregray matter volume is abnormal and characterizing theclinical conditions under which such abnormalities areevident. Future studies will combine neuroimaging andgenetic approaches to facilitate investigations of geno-types that may underlie the vulnerability to mood disor-ders or to specific neuroimaging abnormalities. This arti-cle reviews the psychiatric imaging literature andintegrates its major findings with data from electrophysi-ologic and lesion analysis studies to develop hypothesesregarding the neural substrates of major depression.
Neuroimaging Approaches to Understandingthe Functional Anatomy of Depression
A constellation of cerebral blood flow (CBF) and glucosemetabolic abnormalities are found in limbic and prefrontalcortex (PFC) structures by PET studies of major depres-sive disorder (MDD). Some abnormalities reverse duringsymptom remission and likely reflect areas where physi-ologic activity changes to mediate or respond to theemotional, behavioral, and cognitive manifestations ofMDEs. Others persist despite symptom remission, andhave in some cases been linked to anatomic differencesbetween depressives and control subjects.
The interpretation of neurophysiologic differences be-tween depressives and control subjects is complex. Be-cause neural activity, CBF, and glucose metabolism arecoupled, physiologic images can dynamically reflect thefunctional anatomic correlates of cognitive, emotional, orbehavioral processes as changes in regional CBF ormetabolism during mental activity. These changes com-prise summations of the chemical and hemodynamicprocesses involved in neural activity, which is dominatedby the energy utilization associated with terminal fieldsynaptic transmission (DiRocco et al 1989; Magistretti etal 1995; Raichle 1987). When CBF or glucose metabolism
From the Departments of Psychiatry and Radiology, University of Pittsburgh,Pittsburgh, Pennsylvania.
Address reprint requests to Wayne C. Drevets, M.D., University of PittsburghMedical Center, PET Facility Room B-938 PUH, 200 Lothrop Street, Pitts-burgh PA 15213.
Received February 16, 2000; revised June 19, 2000; accepted August 8, 2000.
© 2000 Society of Biological Psychiatry 0006-3223/00/$20.00PII S0006-3223(00)01020-9

images acquired during performance of a neuropsycho-logic task are compared with images obtained in the samesubject during a control condition, regional increases inCBF or metabolism generally signify increasing afferentsynaptic transmission from local or distal structures in theexperimental condition, relative to the control condition,while reductions in these parameters reflect decreasingafferent transmission (DiRocco et al 1989; Raichle 1987).Differences in regional CBF or metabolism between de-pressives and control subjects may thus reflect changes inneurotransmission associated with depressive symptoms;however, CBF and metabolism are also affected bychanges in neurotransmitter/neuroreceptor function, neu-ropathologic alterations in the number of cells and synap-tic contacts, and disease processes affecting cerebrovascu-lar or thyroid function (Chimowitz et al 1992; Drevets et
al 1999b; Fazekas 1989; Wooten and Collins 1981). Sincesuch factors may be abnormal in some mood-disorderedsubtypes, interpreting differences between depressives andcontrol subjects requires thoughtful research design andinformation obtained using complementary approaches.
Critical Assessment of the Psychiatric ImagingLiterature
The literature is in disagreement regarding the specificlocations and the direction of neurophysiologic abnormal-ities in MDD. Critical review of design and data analysisresolves some inconsistencies across studies. Design is-sues that relate to technical aspects of image acquisitionare discussed elsewhere (Drevets and Botteron 1997;Raichle 1987). Issues involving subject selection and
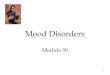
Figure 1. (A) Areas of abnormally increased cerebral blood flow (CBF) in familial major depressive disorder (MDD) shown in animage oft values, produced by a voxel-by-voxel computation of the unpairedt statistic to compare CBF between depressed and controlsamples (Drevets et al 1992). The positivet values in this sagittal section at 17 mm left of midline (x5 217) show areas of increasedCBF in depressives relative to control subjects in the amygdala and medial orbital cortex. Abnormal activity in these regions in MDDwas confirmed using higher resolution, glucose metabolic measures in other studies. Anterior is to the left. (Modified from Price et al1996.)(B) Coronal (31 mm anterior to the anterior commissure, or y5 31) and sagittal (3 mm left of midline, or x5 23) sectionsshowing negative voxelt values where glucose metabolism isdecreasedin depressives relative to control subjects (Drevets et al 1997).The reduction in activity in this region appeared to be accounted for by a corresponding reduction in cortex volume. Although noneof these subjects were involved in the study that generated thet image shown inA, the mean metabolism in this independent set ofdepressives was also abnormallyincreasedin the amygdala and orbital cortex. Anterior is to the left. (Reproduced with permission fromDrevets et al 1997.)(C) Sagittalt image section 41 mm left of midline (x5 241) shows an area of increased CBF in depressivesrelative to healthy control subjects in the left ventrolateral PFC (VLPFC), lateral orbital cortex, and anterior insula (Drevets et al 1992).(Reproduced with permission from Drevets et al 1999b.)(D) Coronalt image section 19 mm caudal to the anterior commissure (i.e.,y 5 219) showing the area corresponding to increased CBF in the left medial thalamus of depressives relative to control subjects(Drevets et al 1992, 1995b). (Reproduced with permission from Drevets and Todd 1997.)
814 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

image analysis that are particularly relevant to the inter-pretation of imaging studies of depression are addressedhere.
Image analysis techniques differ widely in their sensi-tivity for detecting the relatively subtle abnormalitiesextant in mood disorders. Region of interest (ROI) ap-proaches involving coregistration of high resolution PETand anatomic MRI images have the greatest sensitivity fordetecting abnormalities when an affected region can bedelimited in MRI scans; however, ROI placement mayundersample or dilute focal abnormalities of radiotraceruptake when anatomic boundaries are unknown.
To address this type II error source, omnibus imageanalysis strategies are used to survey brain images voxelby voxel (e.g., Figure 1; Drevets et al 1992; Friston et al1991). Primary images are spatially transformed into astandardized stereotaxic space so that tomographic datacan be averaged across subjects. Since current spatialtransformation algorithms do not precisely align the vari-able, complex three-dimensional structure of images fromdifferent brains, images are blurred before analysis to
minimize the impact of misalignment error (Poline et al1997); however, the loss of spatial resolution from blur-ring and the error in overlaying brain structure acrosssubjects decrease sensitivity for detecting abnormalities insmall structures (e.g., amygdala, subgenual PFC) or areascharacterized by high anatomic variability (e.g., orbitalcortex). Voxel-by-voxel analyses may also increase type Ierror because they require thousands of statistical compar-isons, and thep values obtained in published studies ofMDD have generally not been appropriately corrected formultiple comparisons (Poline et al 1997). Nevertheless,when constrained by appropriate statistical considerationsand followed by replication using targeted, MRI-based,ROI analyses in independent samples, approaches involv-ing omnibus statistical mapping techniques prove invalu-able for delineating abnormalities in MDD (e.g., Drevetset al 1992, 1995c, 1997).
The sensitivity for identifying abnormalities is alsoaffected by sample size, medication effects, and biologicalheterogeneity. Antidepressant and antianxiety treatmentsreportedly decrease CBF and metabolism in frontal, pari-
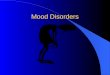
Figure 2. Anatomic circuits implicated by neuroimaging and neuropathologic studies of familial mood disorders. The regional abnormalitiessummarized are specifically hypothesized to contribute to the genesis of pathologic emotional behavior. Regions in red have neuromorpho-metric and/or histopathologic abnormalities in primary major depressive disorder and/or bipolar disorder (BD; see text). Regions in yellowhave not been microscopically examined in mood disorders, but are areas where structural abnormalities aresuspectedbased upon the findingof third ventricle enlargement in children and adults with BD. Open arrows to the right of each region indicate the direction of abnormalitiesin cerebral blood flow (CBF) and metabolism reported in depressives relative to control subjects (? indicates where experimental data awaitreplication). Parenthetical open arrows indicate the direction of metabolic abnormalities after correcting the positron emission tomography(PET) measures for partial volume effects of reduced gray matter volume [(?) indicates where decreased gray matter is suspected as theexplanation for reductions in CBF and metabolism, but partial volume-corrected PET results have not been reported]. Solid lines indicatemajoranatomic connections between structures (e.g., weak projections, such as that from the orbital cortex back to the subiculum [Carmichaeland Price 1995], are not included), with closed arrowheads indicating the direction of the projecting axons (reciprocal connections havearrowheads at both line ends). Affected prefrontal cortex (PFC) areas include the ventrolateral and orbital PFCs (ORB/VLPFC), the anterior(agranular) insula (A.INS), the anterior cingulate gyrus ventral and anterior to the genu of the corpus callosum (subgenual PFC [SGPFC] andpregenual anterior cingulate [PAC], respectively), and the dorsomedial/dorsal anterolateral PFC (DM/DALPFC). The parts of the striatumunder consideration are the ventromedial caudate and nucleus accumbens, which particularly project to the ventral pallidum (Nauta andDomesick 1984). BNST, bed nucleus of the stria terminalis; VTA, ventral tegmental area; LC, locus coeruleus; NTS, nucleus tractussolitarius; PAG, periaqueductal gray.
Neuroimaging Studies of Mood Disorders 815BIOL PSYCHIATRY2000;48:813–829

etal, and temporal lobe regions, and studies includingimages from subjects taking such agents usually fail todetect the areas of hypermetabolism identified in unmedi-cated depressives, and instead report areas of reduced CBFor metabolism not evident in unmedicated samples (for areview, see Drevets et al 1999b). Moreover, MDD andbipolar disorder (BD) likely encompass groups of disor-ders that are heterogenous with respect to etiology andpathophysiology, and “enrichment” of samples for thelikelihood of having psychobiological markers appearsnecessary to replicate some imaging findings.
In some studies, biological variability was reduced byselecting subjects with familial mood disorders. Subjectswith primary, familial MDD (i.e., familial pure depressivedisease [FPDD]) were previously shown to be more likelyto have abnormalities of hypothalamic–pituitary–adrenal(HPA) axis function, platelet [3H]imipramine binding, andsleep electroencephalography relative to MDD subjectswho either lacked mood-disordered relatives or had alco-holic relatives (Kupfer et al 1992; Lewis et al 1983; Lewisand McChesney 1985; Winokur 1982). Depressed sampleswith familial MDD or BD have also been more likely toshow elevated CBF/metabolism in the amygdala, orbitalcortex, and medial thalamus and decreased metabolismand cortex volume in the subgenual PFC than nonfamilialcases or cases with secondary depressive syndromes (Dre-vets et al 1992, 1995c, 1999b; Hirayasu et al 1999;Kegeles et al 1999; O¨ ngur et al 1998). Studies usingalternative means for selecting enriched MDD samples,such as melancholic subtype criteria or responsiveness tosleep deprivation or phototherapy, have also found ele-vated metabolism in the amygdala and orbital cortexduring MDEs (Cohen et al 1992; Ebert et al 1991;Nofzinger et al 1999; Wu et al 1992).
The mood-disordered subtype for which a distinct set ofneuroimaging abnormalities has been best characterized iscomprised of elderly depressives with a late age at illnessonset. Depressives with onset of first MDE after age;55are more likely than both age-matched, healthy controlsubjects and age-matched depressives with an earlier ageof onset to have large “patches” of MR signal hyperinten-sity (in T2-weighted images) in the periventricular anddeep white matter and lacunae in the cortex and striatum(Drevets et al 1999b; Krishnan et al 1993). Tissue acquiredpostmortem from brain areas showing patches of MRsignal hyperintensity reveals arteriosclerosis, gliosis,white matter necrosis, and axon loss in the affected areas,but not in the surrounding tissue where the MRI signalappears normal (Awad et al 1986; Chimowitz et al 1992).Functional imaging studies confirm that CBF is decreasedin areas where white matter hyperintensities are evident inMR images (Chimowitz et al 1992; Fazekas 1989). Late-onset depressives also commonly have widened cortical
sulci, ventricular enlargement, and reduced frontal lobeand basal ganglia volumes, which are thought to reflecttissue atrophy secondary to ischemia (for a review, seeDrevets et al 1999b). Because cerebrovascular diseasealters CBF, radiotracer delivery, and relationships betweenneuronal activity, CBF, metabolism, and oxygen extrac-tion (Derdeyn et al 1998), the functional imaging corre-lates of late-onset MDD profoundly differ from those ofdepressives with early or midlife illness onset (Drevets etal 1999b). Nevertheless, most imaging studies of MDDthat included elderly subjects failed to distinguish orexclude such subjects, confounding interpretation of theirresults.
The MRI and clinical correlates of late-onset depressionsuggest this mood-disordered subgroup develops MDEssecondary to cerebrovascular disease (Krishnan et al1993). The regions most commonly affected by whitematter hyperintensities or lacunae in late-onset MDD arealso the regions where infarction increases the risk fordeveloping MDEs following stroke—namely, the leftfrontal lobe and striatum (for reviews, see Drevets et al1999b; Starkstein and Robinson 1989). These regionscontain neuropathologic abnormalities in familial MDDand BD subjects studied early in life, as well, which are ofa distinct, idiopathic nature (see below). Thus, dysfunctioninvolving an overlapping set of brain structures mayconfer vulnerability to MDEs in both early- and late-onsetmood disorders.
Functional Anatomic Correlates of MajorDepression
The Subgenual Anterior Cingulate Cortex
The anterior cingulate cortex situated anterior and ventralto the genu of the corpus callosum (termedpregenualandsubgenual,respectively) has been implicated by numerousstudies of MDD and BD (for reviews, see Drevets 1999;Drevets and Raichle 1998). In the subgenual PFC, CBFand metabolism are decreased in unipolar and bipolardepressives relative to healthy control subjects (Figure 1B;Buchsbaum et al 1997; Drevets et al 1997; Kegeles et al1999). This abnormality appears to be accounted for by aleft-lateralized, volumetric reduction of the correspondingcortex, initially demonstrated by MRI-based morphomet-ric measures (Drevets et al 1997; Hirayasu et al 1999) andlater by postmortem neuropathologic studies of familialBD and MDD (Ongur et al 1998). This reduction involume exists early in the illness in familial BD (Hirayasuet al 1999) and MDD (Botteron et al 1999), but appears tofollow illness onset, based upon preliminary evidence intwins discordant for MDD (Botteron et al 1999).
Although baseline CBF and metabolism appear abnor-mally decreased in PET images during MDEs, computer
816 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

simulations that correct PET data for the partial volumeeffect of reduced gray matter volume conclude the “actu-al” metabolic activity in the remaining subgenual PFCtissue is increased in depressives relative to controlsubjects (Figure 2; Drevets 1999). This hypothesis appearscompatible with findings that effective antidepressant drug(AD) treatments result in adecreasein metabolic activityin this region in MDD (Buchsbaum et al 1997; Drevets1999; Mayberg et al 1999). Computer simulations ofposttreatmentimages find that actual (partial volumecorrected) metabolism decreases to normative levels dur-ing effective treatment (Drevets 2000). This mood statedependency of subgenual PFC metabolism would appearconsistent with PET studies showing that flow increases inthe subgenual PFC of healthy, nondepressed humansduring experimentally induced sadness (Damasio et al1998; George et al 1995; Mayberg et al 1999).
Although effective treatment with selective serotoninreuptake inhibitor (SSRI) ADs did not alter the subgenualPFC volume in MDD (Drevets et al 1997), this cortex wassignificantly larger in BD subjects chronically medicatedwith lithium or divalproex than in BD subjects who wereunmedicated or were medicated with other agents (W.C.Drevets et al, unpublished data). Chronic administration ofthese mood stabilizers markedly increases levels of theneuroprotective protein Bcl-2 in the frontal cortex, stria-tum, and hippocampus of experimental animals (Manji etal 1999). Bcl-2 administration increases neurite sproutingand protects against glutamate-mediated excitoxicity, rais-ing the possibility that this difference in subgenual PFCvolume reflects a neuroprotective/neurotrophic effect ofmood-stabilizing medications (Manji et al 1999 [thisreference also considers alternative explanations for lithi-um’s effects on cortical volume, however]).
Postmortem assessment of the subgenual PFC (agranu-lar cortex on the prelimbic anterior cingulate gyrus [part ofBrodmann’s area (BA) 24]) demonstrated this abnormalreduction in gray matter was associated with areductioninglia, no equivalent loss of neurons, and increased neuronaldensity in MDD and BD relative to healthy and schizo-phrenic control samples (O¨ ngur et al 1998). These findingssuggest the volumetric abnormality in the subgenual PFCmay specifically reflect a reduction of neuropil, the fibrouslayers comprised of dendrites and axons that occupy mostof the cortex volume (McEwen 1999). Glia are dividingcells that support neurons and synaptic transmission, sothe reduction in glia may conceivably occur secondary tothe reduction of synapses expected from a reduction inneuropil (Magistretti et al 1995; McEwen 1999). Never-theless, because glia maintain potassium homeostasis,transport glutamate andg-aminobutyric acid (GABA)from the extracellular fluid, and provide trophic factorsand energy substrates to neurons, glial hypofunction may
also disturb synaptic transmission within the affectedcortex (Azmitia 1999; Magistretti et al 1995).
The subgenual PFC has extensive reciprocal connec-tions with the orbital cortex, hypothalamus, amygdala,accumbens, ventral tegmental area (VTA), substantianigra, raphe, locus coeruleus, periaqueductal gray (PAG),and nucleus tractus solitarius (Figure 2; Carmichael andPrice 1995; Leichnetz and Astruc 1976). Humans withlesions that include the subgenual PFC show abnormalautonomic responses to emotionally provocative stimuli,inability to experience emotion related to concepts thatordinarily evoke emotion, and inability to use informationregarding the likelihood of punishment and reward inguiding social behavior (Damasio et al 1990). In rats,bilateral orright-lateralized lesions of the prelimbic (theapparent homologue of the primate subgenual PFC) andinfralimbic corticesattenuatesympathetic autonomic re-sponses, stress-induced corticosterone secretion, and gas-tric stress pathology during restraint stress or exposure tofear-conditioned stimuli (Frysztak and Neafsey 1994;Morgan and LeDoux 1995; Sullivan and Gratton 1999). Incontrast,left-sided lesions of this areaincreasesympa-thetic autonomic arousal and corticosterone responses torestraint stress (Sullivan and Gratton 1999). Althoughthese latter data await replication, they suggest the hypoth-esis that the right subgenual PFC facilitates expression ofvisceral responses during emotional processing, whereasthe left subgenual PFC modulates such responses (Sulli-van and Gratton 1999). This hypothesis is noteworthy inlight of the left-lateralized nature of the volumetric reduc-tion of the subgenual PFC in MDD and BD, and of PETdata showing thatright subgenual PFC metabolism corre-lates positively with depression severity in MDD (rated bythe Hamilton Depression Rating Scale [HDRS];r 5 .76,p , .01; Drevets 2000). It is thus conceivable thatdysfunction of the left subgenual PFC contributes to thealtered neuroendocrine and autonomic function in depres-sion (Carney et al 1988; Dioro et al 1993; Holsboer 1995;Veith et al 1994).
The subgenual PFC may also participate in evaluatingthe reward-related significance of stimuli. The subgenualPFC sends efferent projections to the VTA and substantianigra and receives dense dopaminergic innervation fromthe VTA (Leichnetz and Astruc 1976; Price 1999). In rats,electrical or glutamatergic stimulation of medial PFCareas that include the prelimbic cortex elicits burst firingpatterns from dopamine cells in the VTA and increasesdopamine release in the accumbens (for a review, seeDrevets 1999). Because these phasic, burst firing patternsof dopamine neurons are thought to encode informationregarding stimuli that predict reward and deviations be-tween such predictions and the actual occurrence ofreward (Schultz 1997), subgenual PFC dysfunction may
Neuroimaging Studies of Mood Disorders 817BIOL PSYCHIATRY2000;48:813–829

conceivably contribute to disturbances of hedonic percep-tion and motivated behavior in mood disorders. In thisregard, the magnitude of abnormal metabolic activity inthe subgenual PFC may relate to switches between depres-sion and mania, as, even in the presence of reducedvolume, apparent subgenual PFC activity appears abnor-mally increased in small samples of manic subjects (e.g.,Drevets et al 1997).
The Pregenual Anterior Cingulate Cortex
The psychiatric imaging literature is less consistent withrespect to the pregenual anterior cingulate cortex. Thisregion consistently shows elevated CBF during variousemotional conditions elicited in healthy or anxiety-disor-dered humans (for a review, see Drevets and Raichle1998). Electrical stimulation of this region elicits fear,panic, or a sense of foreboding in humans, and vocaliza-tion in experimental animals (for a review, see Price et al1996).
Most imaging studies find that CBF and metabolism areincreased in this area during MDEs (for a review, seeDrevets 1999); however, Mayberg et al (1997) reportedthat, although metabolism in this area was abnormallyincreased in depressives who subsequently showed a goodresponse to ADs, metabolism was abnormally decreased indepressives who later had poor or incomplete treatmentresponses. In contrast, other groups found inverse corre-lations between basal metabolism and subsequent antide-pressant response in MDD, with lower baseline pregenualanterior cingulate metabolism predicting superior respon-siveness to ADs (Brody et al 1999; Ketter et al 1999). Theeffects of treatment on pregenual anterior cingulate CBFand metabolism have also differed across studies, withactivity decreasing in some but increasing in others inposttreatment scans, relative to pretreatment scans (for areview, see Drevets 1999). The extent to which thesediscrepancies are explained by differential effects in sub-regions of this area remains unclear.
The Orbital and Anterior Insular Cortices
In the left and right posterior orbital cortices, the leftventrolateral PFC (VLPFC), and the anterior (agranular)insula, CBF and metabolism are abnormallyincreasedinunmedicated subjects with primary MDD (Figure 1, A andC; e.g., Baxter et al 1987, Table 3; Biver et al 1994; Cohenet al 1992; Drevets et al 1992, 1995c; Ebert et al 1991).Flow and metabolism also increase in the these areasduring experimentally induced sadness and anxiety inhealthy subjects and during induced anxiety and obses-sional states in subjects with obsessive–compulsive, post-traumatic stress, simple phobic, and panic disorders (for areview, see Drevets and Raichle 1998). The elevation of
physiologic activity in these areas during MDEs appearsmood state dependent, as a variety of effective, somaticantidepressant therapies result in decreases in CBF andmetabolism in the remitted phase of MDD relative to thedepressed phase (e.g., Brody et al 1999; Drevets 1999;Drevets et al 1992; Mayberg et al 1999; Nobler et al 1994).
A complex relationship exists between depression se-verity and metabolic activity in the orbital cortex andVLPFC. Although CBF and metabolism are elevated inthese areas in the depressed phase of MDD relative to theremitted phase, these measures correlate inversely withratings of depression severity and depressive ideation(Drevets et al 1992, 1995c). Compatible with these data,although metabolic activity is abnormally increased inthese areas in outpatient, treatment-responsive, unipolarand bipolar depressives, more severely ill or treatment-refractory BD samples and inpatient MDD samples haveshown mean CBF and metabolic values that either did notsignificantly differ or were decreased relative to controlsamples (Drevets et al 1997; Ketter et al 1999; Mayberg etal 1997). Similarly, PET studies of depression secondaryto Parkinson’s disease, cerebrovascular disease, or com-plex partial seizures have shown that flow is eitherunchanged or abnormally decreased in these conditionsrelative to nondepressed control subjects with the sameneurologic conditions (Bromfield et al 1992; Lesser et al1994; Mayberg et al 1990; Ring et al 1994). Elevatedorbital activity is, therefore, not essential to the productionof depressive symptoms.
Instead, these relationships between orbital metabolismand depression severity are consistent with evidence fromimaging, lesion analysis, and electrophysiologic studiesthat the posterior orbital cortex participates in modulatingbehavioral, visceral, and cognitive responses associatedwith defensive, fear, and reward-directed behavior asreinforcement contingencies change. Posterior orbital cor-tex CBF increases in subjects with obsessive–compulsivedisorder or animal phobias during exposure to phobicstimuli and in healthy subjects during induced sadness(Drevets et al 1995b; Rauch et al 1994; Schneider et al1995). In each of these cases,DCBF in the posteriororbital cortex correlates inversely with concomitantchanges in obsessive thinking, anxiety, and sadness, re-spectively. In animal phobic subjects, serial PET imagesacquired during repeated exposures to phobic stimulirevealed that the orbital CBF was unchanged during initialexposures when the fear response was greatest, but assubjects habituated to the stimuli during subsequent expo-sures, posterior orbital CBF progressively increased, andthe DCBF was inversely correlated with changes in anxi-ety ratings and heart rate (Drevets et al 1995b).
Nearly one half of pyramidal cells in the orbital cortexalter their firing rates during the delay period between
818 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

stimulus and response, and the patterns of posttrial activ-ity, which relate to the presence or absence of reward,suggest these cells play a role in extinguishing unrein-forced responses to appetitive and aversive stimuli (Rolls1995). This role may be partly mediated by interactionswith the amygdala and other limbic structures (Mogensonet al 1993; Price et al 1996). The orbital cortex andamygdala send direct projections to each other and over-lapping projections to the striatum, hypothalamus, andPAG through which they modulate each other’s transmis-sion (Figure 2; Carmichael and Price 1995; Mogenson etal 1993; Price 1999). Such interactions are evidenced byfindings that defensive behaviors and cardiovascular re-sponses evoked by electrical stimulation of the amygdalaare attenuated or ablated by concomitant stimulation oforbital cortex sites, which when stimulated alone produceno autonomic changes (Timms 1977). Compatible with thehypothesis that orbital cortex activity modulates amyg-dalar function during MDEs, glucose metabolisms in theorbital cortex and amygdala are inversely correlated indepressed humans (Drevets 2000).
Although tumors and cerebrovascular lesions involv-ing the frontal lobe increase the risk for developingMDEs, the specific PFC regions where dysfunctionconfers this risk have not been established (Mayeux1982; Starkstein and Robinson 1989). Humans withlesions of the orbital cortex show impaired performanceon tasks requiring application of information related toreward or punishment, exhibit difficulty shifting intel-lectual strategies in response to changing demands, andperseverate in strategies that become inappropriate(Bechara et al 1998; Rolls 1995). Lesion analysisstudies in monkeys and functional imaging studies inhumans show that the lateral orbital cortex/VLPFC inparticular is involved when responses to stimuli requirethe suppression of previously rewarded responses (El-liott et al 2000; Iversen and Mishkin 1970).
During MDEs orbital cortex activation may reflectendogenous attempts to attenuate emotional expression orinterrupt perseverative patterns of aversive, nonrewardingthought and emotion. Nevertheless, evidence that neuro-pathologic changes exist in the orbital cortex in primarymood disorders raises the possibility that impairment ofthese orbital functions predisposes to MDEs. Postmortemstudies of MDD and BD report abnormal reductions ofgray matter, glia, and neuronal size, but no decrement inneuronal number, in the posterior orbital cortex andVLPFC (Bowen et al 1989; Rajkowska et al 1997, 1999).Like the histopathologic changes found in the subgenualPFC, these data are most consistent with a reduction inneuropil. If such abnormalities are associated with dis-turbed synaptic interactions between the orbital cortex andamygdala, striatum, hypothalamus, or PAG, then orbital
dysfunction may conceivably contribute to the develop-ment of excessive emotional responses to stressors andruminative ideation.
The abnormalities of serotonergic and catecholaminer-gic neurotransmitter function reported in mood disorderssuggest other mechanisms by which orbital activity maybe impaired in depression. In healthy subjects serotonin(5-HT) depletion (via tryptophan-free diet) produced per-formance deficits on decision-making tasks involvingrisk/reward probabilities that were similar to those seen insubjects with orbital cortex lesions (Rogers et al 1999).Moreover, depressive relapse occurring in remitted MDDsubjects scanned during serotonin depletion was associ-ated with reductions in metabolism in the orbital cortexand VLPFC (Bremner et al 1997 [the area termedmiddlefrontal by Bremner is part of the VLPFC area describedherein]; Smith et al 1999). Finally, orbital cortex metab-olism is decreased in depressed subjects with Parkinson’sdisease, relative to nondepressed subjects, suggesting thatdopamine depletion may impair orbital cortex function(Mayberg et al 1990; Ring et al 1994).
The effects of antidepressant treatment on neurophysi-ologic activity in the orbital cortex and VLPFC arenoteworthy in this regard. The highly replicated findingthat CBF and metabolism decrease in the orbital/insularcortex and VLPFC during effective AD treatment mayindicate that this cortex can “relax,” as such treatmentsdirectly inhibit pathologic activity in limbic structuressuch as the amygdala (for a review, see Drevets 1999). Incontrast, nonpharmacologic treatments such as cognitivebehavioral therapy and repetitive transcranial magneticstimulation reportedlyincreasemetabolism in the VLPFCand posterior orbital cortex, respectively (Brody et al1999; Teneback et al 1999), suggesting the hypothesis thattheir therapeutic mechanisms depend upon enhancing thefunction of PFC mechanisms for attenuating emotionalexpression.
The Dorsomedial/Dorsal Anterolateral PrefrontalCortex
Other PFC regions where dysfunction may impair theability to modulate emotional responses in mood disordersinclude the dorsomedial PFC (DMPFC; vicinity of dorsalBA 32 and rostral BA 9) and dorsal anterolateral PFC(DALPFC; approximately rostral BA 9). Several PETstudies of MDD found abnormally decreased CBF andmetabolism in these areas, which normalized during ef-fective AD therapy in some studies but not others (Baxteret al 1989; Drevets et al 1999b). Ring et al (1994) showedthat CBF is also reduced in the DMPFC in depressedpatients with Parkinson’s disease, as compared with non-depressed Parkinson’s patients. In postmortem studies of
Neuroimaging Studies of Mood Disorders 819BIOL PSYCHIATRY2000;48:813–829

MDD, Rajkowska et al (1999) observed abnormal reduc-tions in the density and size of neurons and glia in thesupra- and infragranular layers of the DALPFC (rostralBA 9), a finding that may relate to the reduction inmetabolic activity in this area in MDD.
In brain mapping studies of healthy humans, CBF in theDMPFC increases during performance of tasks that elicitemotional responses or require emotional evaluations(Dolan et al 1996; Drevets et al 1994; Reiman et al 1997).In healthy humans imaged during anticipation of anelectrical shock, the relationship betweenDCBF andemotion ratings suggested that while this region activatedduring anxiety it exerted a modulatory influence onemotional expression, such that the change in anxietyratings and heart rate correlated inversely withDCBF(Drevets et al 1994). In rats, lesions of the area thatappears homologous with the human DMPFC result inexaggerated heart rate responses to fear-conditioned stim-uli, and electrical and chemical stimulation of these sitesattenuates defensive behavior and cardiovascular re-sponses evoked by amygdala stimulation (for a review, seeFrysztak and Neafsey 1994). The DMPFC sends efferentprojections to the PAG through which it may modulatecardiovascular responses associated with emotional be-havior or stress (Price 1999). If the histopathologicchanges found in this area in MDD by Rajkowska et al(1999) are associated with functional impairment, theymay conceivably contribute to the pathologic stress re-sponses and elevated resting heart rate seen in MDD.
Dorsolateral PFC and Dorsal Anterior CingulateCortex
Abnormal reductions of CBF and metabolism have alsobeen reported in MDD in areas of the lateral and dorso-lateral PFC (L/DLPFC) and the dorsal anterior cingulatecortex situated posterior to the areas described in thepreceding section (for reviews, see Drevets et al 1999b;Drevets and Raichle 1998). These abnormalities appearmood state dependent, reversing during symptom remis-sion (Bench et al 1995; Mayberg et al 1999). Initial studiesassessing neuromorphometry or histology have not foundabnormalities in these areas in MDD or BD (Bowen et al1989; Drevets et al 1997; Rajkowska et al 1997).
Human PET and fMRI studies show that hemodynamicresponses in the anterior cingulate cortex dorsal andposterior to the genu of the corpus callosum consistentlyincrease during tasks requiring discriminative attentionand selection for action (for a review, see Drevets andRaichle 1998). Attentional demand, target frequency,and/or frequency of being incited to action modulate themagnitude ofDCBF in this region (for a review, seeDrevets and Raichle 1998). In contrast, CBF isdecreased
in this area in healthy subjects during experimentallyinduced anxiety and depressed subjects with MDD, rela-tive to control conditions (Bench et al 1992; Drevets andRaichle 1998). Moreover, the normal activation of thisregion during a verbal fluency task was attenuated duringthe depressed mood associated with acute tryptophandepletion (Smith et al 1999).
Multiple L/DLPFC areas activate when verbal or visuo-spatial information is maintained in working memory andprocessed in some way (for a review, see Drevets andRaichle 1998). In the vicinity of these areas, CBF andmetabolism are reportedly decreased in the depressedphase of MDD, as compared with the remitted phase, indepressives relative to healthy control subjects, and duringexperimentally induced sadness in healthy subjects (Benchet al 1992; Biver et al 1994; Mayberg et al 1999). TheseDLPFC areas do not appear activated during emotionalprocessing, and lesions of this region do not impairperformance on tasks involving the application of infor-mation related to reward or punishment (e.g., Bechara et al1998). In one left DLPFC area, Dolan et al (1993) reportedthat the reduction in CBF correlated with impoverishmentof speech (thought to reflect slowed cognitive processing)in MDD and schizophrenia, although this finding awaitsreplication.
Interpreting reversible decreases in CBF and metabo-lism found during MDEs in areas that have not beenimplicated in emotional processing requires an under-standing of the regulation of neurophysiologic activityacross anatomic systems. Brain mapping studies showthat, whereas CBF increases in brain regions putativelyactivated to perform an experimental task, CBF concom-itantly decreasesin some other neural systems that appearnonessentialto task performance (Drevets and Raichle1998). Such “deactivated” areas are thought to reflectattention-related processes in which signal processing isenhanced via suppression of neural transmission convey-ing competing, unattended information (for a review, seeDrevets et al 1995a).
The clearest examples of these phenomena involvepatterns of reduced CBF seen during expectation ofsomatosensory stimuli, in which CBF decreases in thehuman first somatosensory cortex (SI) and second somato-sensory cortex located outside the cortical representationof the skin area targeted by the expected stimulus, but doesnot change in the somatosensory cortex representing theskin locus of the awaited stimulation (Drevets et al 1995a).These results concur with electrophysiologic evidence ofsuppression, or “gating,” of sensory input to SI corticalneurons when the cutaneous receptive field of the recordedcell is not engaged during tactile discrimination behaviorand preserved to fields where behaviorally significantsomatosensory stimuli are expected (for a review, see
820 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

Drevets et al 1995a). The reduced afferent synaptic trans-mission into the portions of the SI representing unattendedskin sites presumably accounts for the reduction in CBF inthese areas in PET images (DiRocco et al 1989; Drevets etal 1995a). Similar interactions appear to occur acrosssensory modalities (for a review, see Drevets and Raichle1998), as exemplified by findings that CBF decreases inthe primary auditory cortex, auditory association cortex,somatosensory cortex, and posterior cingulate and midcin-gulate cortices as subjects process complex visual stimuli(Haxby et al 1994).
Areas specialized for emotional versus higher cognitivefunctions may also engage in such cross-modal relation-ships. In the amygdala, posterior orbital cortex, andventromedial PFC sites where CBF increases during emo-tion-related tasks, flowdecreasesduring performance ofattentionallydemanding, cognitive tasks (Drevets andRaichle 1998; Shulman et al 1997). Conversely, in dorsalanterior cingulate and DLPFC areas where flow increaseswhile attentionally demanding cognitive tasks are per-formed, CBF decreasesduring some emotional states(Drevets and Raichle 1998; Mayberg et al 1999).
These reciprocal patterns of neural activity hold intrigu-ing implications for interactions between emotion andcognition (Drevets and Raichle 1998). The reduction ofCBF in dorsal anterior cingulate and DLPFC areas spe-cialized for verbal, attentional, visuospatial, and mne-monic processing during depression may reflect a suppres-sion of afferent activity to those regions as dysphoricemotions or thoughts are processed. This suppression mayrelate to the subtle impairments of attention, memory, and
visuospatial function that accompany MDEs (Drevets andRaichle 1998).
The Amygdala
Resting CBF and glucose metabolism are abnormallyelevated in the amygdala in depressives with FPDD, typeII BD or nonpsychotic, type I BD (Figures 1 and 3;Drevets et al 1992, 1995b; Wu et al 1992). In contrast, thisabnormality is not evident in more severe, psychotic, typeI BD subjects (Drevets 1995), and the extent to which thisseverity-based difference between BD samples may reflectdifferential magnitudes of partial volume effects associ-ated with abnormalities of amygdala structure in BDremains unclear (Bowley et al, in press; Pearlson et al1997). Abnormalities of resting amygdalar CBF/metabo-lism have also not been found in MDD samples meetingWinokur (1982) criteria for depression spectrum disease(Drevets et al 1995c), obsessive–compulsive disorder,panic disorder, phobic disorders, or schizophrenia, sug-gesting this abnormality may be specific to some primarymood disorder subtypes (for a review, see Drevets andBotteron 1997).
In FPDD the magnitude of this abnormality as measuredby PET is about 5% to 7% (Figure 3). When corrected forspatial resolution effects, this difference would reflect anincrease in the actual CBF and metabolism of about50–70% (Drevets et al 1992; Links et al 1996). Thesemagnitudes are in the physiologic range, as CBF increases;50% in the rat amygdala during exposure to fear-
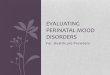
Figure 3. Mean physiologic activity (6SEM) in the left amygdala in midlife de-pressed subjects relative to age-, gender-,and handedness-matched healthy controlsubjects. The results of three consecutivestudies obtained using different positronemission tomography (PET) cameras indifferent laboratories in independent sub-ject samples are summarized (subject andPET scanner characteristics are describedin Drevets et al 1992, 1997, 1999a; 2D and3D, image acquisition modes). In eachstudy normalized CBF or metabolism wasincreased 6% to 8% in the depressivesversus the control subjects (quantitativewhole brain cerebral blood flow [CBF] andmetabolism did not significantly differ be-tween groups in these studies). rCBF/gCBF, regional-to-global CBF ratio; rMR-glu/gMRglu, ratio of regional-to-globalmetabolic rates for glucose; CON, healthycontrol subjects; FPDD, familial pure de-pressive disease (Winokur 1997); BD-D,depressed phase of bipolar disorder.
Neuroimaging Studies of Mood Disorders 821BIOL PSYCHIATRY2000;48:813–829

conditioned stimuli as measured by tissue autoradiography(LeDoux et al 1983).
Amygdalar CBF and metabolism correlate positivelywith depression severity (Abercrombie et al 1996; Drevetset al 1992, 1995b). During AD treatment that both inducesand maintains symptom remission, amygdala metabolismdecreases to normative levels, compatible with preclinicalevidence that chronic AD administration has inhibitoryeffects on amygdala function (for a review, see Drevets1999). Nevertheless, CBF and metabolism in the leftamygdala appear abnormally increased (although to alesser extent) during the unmedicated, remitted phase ofFPDD (Drevets et al 1992), and AD-medicated, remittedMDD subjects who relapse in response to serotonindepletion (via tryptophan-free diet) have higher amygdalametabolism before depletion than those who do not relapse(Bremner et al 1997). Abnormal amygdala activity maythus relate to both the severity of MDEs and the suscep-tibility to MDE recurrence. The extent to which theserelationships reflect differentiable components (e.g., re-lated to involvement of distinct amygdalar nuclei) remainsunclear due to the limited spatial resolution of PET.
The positive correlation between amygdala metabolismand depression severity rated by HDRS scores may reflectthe amygdala’s role in organizing multiple aspects ofemotional/stress responses (Davis 1992). In humans, elec-trical stimulation of the amygdala can produce anxiety,fear, dysphoria, recollection of emotionally provocativeevents, and increased cortisol secretion (for a review, seeDrevets 1999). Moreover, an excessive amygdalar driveon the PAG (LeDoux 1996) may conceivably contribute todepressive signs such as inactivity, panic attacks, andreduced pain sensitivity, since in experimental animalsstimulation of ventrolateral PAG produces social with-drawal, behavioral quiescence, and hypoalgesia, whereasstimulation of lateral PAG produces defensive behaviors,sympathetic autonomic arousal, and hypoalgesia (for areview, see Price 1999). Excessive efferent amygdalatransmission to the lateral hypothalamus and locus coer-uleus could also potentially contribute to the elevatedsympathetic tone, behavioral arousal, and insomnia seen inMDD (Carney et al 1988; Davis 1992; Veith et al 1994).In addition, activation of the amygdalar projections to theventral striatum arrests goal-directed behavior in experi-mental animals (Mogenson et al 1993), suggesting apossible neural mechanism for the cessation of motivatedor reward-directed behavior during MDEs.
The amygdala also facilitates stress-related cortico-tropin-releasing hormone (CRH) release via bothintrinsic CRH-containing neurons and bisynaptic (doubleGABAergic) anatomic projections to the paraventricularnucleus of the hypothalamus (Herman and Cullinan 1997).These data thus suggest a pathway through which exces-
sive amygdala activity may contribute to the abnormalelevation of CRH secretion in MDD, which has beenthought to be partly mediated by increased limbic drive(for a review, see Holsboer 1995). Corticotropin-releasinghormone administration is reported to induce appetitesuppression, decreased sexual behavior, sleep disturbance,and anxiety in rats, suggesting another mechanism bywhich amygdalar hyperactivity may yield depressivesymptoms (Musselman and Nemeroff 1993).
Finally, amygdala dysfunction may conceivably alterthe interpretation of social or emotionally valenced stimuliin mood disorders. Neuroimaging, electrophysiologic, andlesion analysis studies demonstrate that the amygdala isinvolved in the acquisition and expression of emotional/arousing memories (e.g., aversive conditioning; Canli et al2000; LeDoux 1996; Phelps and Anderson 1997). Forexample, single-trial fMRI studies show that the humanamygdala activates during initial exposures to fear-condi-tioned stimuli, but becomes deactivated during repeatedexposures to the same stimulus (Bu¨chel et al 1998; LaBaret al 1998). The amygdala is also involved in interpretingthe emotional significance of social cues. In humans,blood flow increases in the amygdala as subjects viewfaces expressing fear or sadness (Blair et al 1999; Morriset al 1996), and amygdala lesions impair the ability torecognize fear or sadness in facial expression (Adolphs etal 1994; Anderson and Phelps 1997) and fear and anger inspoken language (Scott et al 1997). Preliminary studiesemploying such neuropsychologic tasks in depressed hu-mans suggest that the pattern of hemodynamic responsesto facially expressed emotion is altered in primary mooddisorders (Casey et al 2000; Drevets 1999).
The preliminary finding that amygdala metabolismremains abnormally increased in MDD during sleep ar-gues that it is unlikely that the abnormal elevation inresting metabolism is simply accounted for by a height-ened response to the stressful stimuli related to scanning.Nofzinger et al (1999) reported that, although amygdalametabolism is increased in depressives relative to controlsubjects during wakefulness, the normal increase in me-tabolism that occurs during rapid eye movement sleep isalso greater in depressives than in control subjects.
Abnormalities in the Striatum and Other BrainAreas
The amygdala and the orbital, ventrolateral, and subgenualPFCs share extensive anatomic connections with themediodorsal nucleus of the thalamus (MD) and the ventralstriatum (Price et al 1996). In the left medial thalamus,CBF and metabolism are abnormally increased in de-pressed MDD and BD samples (Figure 1D; Drevets et al1992, 1995b). In contrast, CBF and metabolism are
822 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

abnormally decreased in the caudate in MDD (Baxter et al1985; Drevets et al 1992). The volumes of the caudatehead and ventral striatum appear abnormally decreased inMRI and postmortem studies of MDD (Baumann et al1999; Krishnan et al 1992). The partial volume effectsassociated with this abnormality may thus contribute to theCBF and metabolic reductions in the caudate in MDD.Nevertheless, depressive relapse during acute tryptophandepletion results in a corresponding reduction in caudateblood flow relative to baseline, suggesting that dynamicaspects of caudate function are also involved in mooddisorders (Smith et al 1999).
Regional CBF and metabolic abnormalities in otherstructures have been less consistently replicated. Abnor-mally increased CBF has been reported in the posteriorcingulate cortex and medial cerebellum in MDD (Bench etal 1992; Buchsbaum et al 1997). Medial cerebellar CBFalso increases during experimentally induced anxiety orsadness in healthy or anxiety-disordered subjects (forreviews, see Drevets and Botteron 1997; George et al1995). Some studies report reduced CBF and metabolismin sensory association areas in the lateral temporal andinferior parietal areas in MDEs (e.g., Biver et al 1994;Cohen et al 1992; Drevets et al 1992). Deactivation ofthese areas during MDE may reflect phenomena like thosediscussed above for the L/DLPFC (Drevets and Raichle1998).
Anatomic Circuits Implicated in MDD
The abnormalities of function and structure in mooddisorders implicate limbic–thalamic–cortical (LTC) cir-cuits, involving the amygdala, medial thalamus, and or-bital and medial PFCs, and limbic–cortical–striatal–palli-dal–thalamic (LCSPT) circuits, involving the componentsof the LTC circuit along with related parts of the striatumand pallidum (Figure 2; Drevets et al 1992). The amygdalaand PFC are interconnected by excitatory projections witheach other and with the MD (Carmichael and Price 1995;Price et al 1996). Through these connections the amygdalais in a position to directly activate the PFC and tomodulate the reciprocal interaction between the PFC andMD (Drevets et al 1992).
Pathologically increased amygdala activity could alsoproduce abnormal activity in the PFC and MD through thestriatum and pallidum. The amygdala and PFC sendexcitatory projections to overlapping parts of the ventro-medial caudate and nucleus accumbens (Carmichael andPrice 1995; Price et al 1996). This part of the striatumsends an inhibitory projection to the ventral pallidum,which in turn sends GABAergic, inhibitory fibers to theMD (Graybiel 1990; Kuroda and Price 1991). Because thepallidal neurons have relatively high spontaneous firing
rates (DeLong 1972), activity in the amygdala or PFC thatactivates the striatum and in turn inhibits the ventralpallidum may release the MD from an inhibitory pallidalinfluence.
The putative functions of the orbital and medial PFCs inmodulating emotional and stress responses discussedabove could potentially be impaired by dysfunction arisingwithin these PFC regions themselves or within theirefferent terminal projection fields in the striatum. Consis-tent with this hypothesis, lesions involving either the PFCor the striatum (e.g., strokes or tumors) and degenerativediseases affecting the striatum (e.g., Parkinson’s andHuntington’s diseases) are associated with higher rates ofsecondary major depression than similarly debilitatingconditions that spare these regions (Folstein et al 1991;Mayeux 1982; Starkstein and Robinson 1989). Becausethese conditions disturb the LCSPT and LTC circuitry indifferent ways, imbalances within these circuits, ratherthan overall increased or decreased synaptic activity in aparticular structure, may increase the risk for developingMDEs (Drevets et al 1992). It is nevertheless noteworthythat surgical lesions that interrupt projections from theorbital cortex into the striatum do not result in depressionif the amygdalar projections into the striatum or anteriorcingulate are also severed, as would occur during neuro-surgical interventions for intractable depression (e.g., sub-caudate tractotomy, prefrontal/limbic leukectomy; Ballan-tine et al 1987; Corsellis and Jack 1973; Knight 1965;Nauta 1973; Newcombe 1975). Therefore, neural mecha-nisms of depression may more specifically require dys-function of the orbitomedial PFC and/or other brainsystems that results in disinhibition of the amygdala andother limbic structures involved in mediating emotionalresponses.
Implications of Histopathologic Findings in theLTC and LCSPT Circuits
In primary MDD and BD, neuropathologic findings likethose described in the subgenual PFC and orbital cortex(decreased gray matter volume and glial counts, with noequivalent loss of neurons) may exist in multiple parts ofthe LTC and LCSPT circuits (Figure 2). A postmortemstudy of the amygdala found that glial cell counts, glialdensity, and glia-to-neuron ratios are abnormally de-creased in MDD (Bowley et al, in press). In the ventralstriatum, postmortem assessments showed decreased vol-ume in MDD and BD relative to control samples, althoughthe histopathologic correlates of this abnormality were notaddressed (Baumann et al 1999). Finally, the finding ofthird ventricle enlargement in adults and adolescents withBD (Drevets and Botteron 1997; Pearlson et al 1997)suggests that the thalamic and hypothalamic areas that
Neuroimaging Studies of Mood Disorders 823BIOL PSYCHIATRY2000;48:813–829

receive projections from the orbital and medial PFCs mayalso be affected (Carmichael and Price 1995). In contrast,the volumes of the whole brain, entire PFC, dorsal anteriorcingulate, somatosensory cortex, lateral temporal cortex,and other control regions have not differed betweenmidlife or early-onset MDD or BD subjects and healthycontrol subjects (e.g., Drevets et al 1997; Pearlson et al1997). Morphometric data in the hippocampus have beenless clear, as subtle reductions of hippocampal volumewere found by some but not most MRI studies of MDD orBD, and histopathologic assessments of the hippocampushave thus far been negative (for reviews, see Drevets et al1999a, 1999b).
Although the etiology and time course of the neuro-pathologic abnormalities in mood disorders are unknown,the histopathology and the apparent specificity for areasimplicated in the modulation of emotional behavior sug-gest clues regarding their pathogenesis. The finding thatthe gray matter volumetric deficit is accompanied by areduction in glia with no equivalent loss of neurons doesnot support neurodegenerative hypotheses, and insteadimplies that the neuropil volume is decreased in primarymood disorders. The neuropil volume can be modulated insome regions of the adult brain by exposure to increasedconcentrations of excitatory amino acid neurotransmittersor cortisol, and by decreased function of neurotrophins,5-HT1A receptors, estrogen receptors, and other factorsthat maintain the cytoskeleton (for reviews, see Azmitia1999; McEwen 1999). Glia are dividing cells that supportneurons and synaptic transmission (Magistretti et al 1995),so the reduction in glia may conceivably arise secondaryto a reduction of synapses associated with retraction of theneuropil.
In primary mood disorders, abnormally elevated cortisolconcentrations and reduced 5-HT1A receptor function maycomprise risk factors for developing reductions in neuropilthat could affect widespread areas of the brain (e.g.,Drevets et al 1999a; Musselman and Nemeroff 1993;Sargent et al 2000; Young et al 1993); however, thetargeted nature of the gray matter volume reductions tospecific areas of the LTC and LCSPT circuits (e.g., the leftsubgenual PFC, but not the right; Drevets et al 1997;Hirayasu et al 1999; Figure 2) suggests that glutamatergicneurotransmission also plays a role in inducing neuropilalterations in primary mood disorders (McEwen 1999).The finding that during MDEs metabolic activity is ele-vated in the LTC pathway, which is formed by predomi-nantly glutamatergic projections, suggests a potentialsource for chronic glutamate exposure (Drevets et al1992). Glutamate is predominantly removed from theextracellular fluid by astrocyte-based transporter sitessituated adjacent to synaptic clefts (Magistretti et al 1995).If the reduction of astroglia found in mood disorders
(Rajkowska 2000) impairs the efficiency of glutamatetransport, it is conceivable that glutamate concentrationsmay increase. The excitotoxic effects of elevated gluta-mate concentrations may be facilitated in affective illnessby increased release of cortisol (Sapolsky 1996).
Currently the only evidence that glutamate transportmay be insufficient in depression is that high-affinityN-methyl-D-aspartate (NMDA) glutamatergic receptorsare desensitized in the PFC of suicide victims, compatiblewith antemortem exposure to elevated glutamate concen-trations (Nowak et al 1995). Nevertheless, antidepressanttreatments may compensate for impaired glutamate trans-port, as repeated electroconvulsive shock and chronic ADadministration desensitize NMDA-glutamatergic receptorsin the rat frontal cortex (Paul et al 1994). Moreover, someanticonvulsant agents that are effective in BD reduceglutamatergic transmission (Sporn and Sachs 1997). Therecently discovered neurotrophic and neuroprotective ef-fects of chronic AD and mood-stabilizing treatments mayalso play roles in ameliorating the neuromorphometricchanges in primary mood disorders (Duman et al 1997;Manji et al 1999).
Finally, the putative effect of chronic AD treatment ofincreasing serotonin transmission, tonically activatingpostsynaptic 5-HT1A receptors, and enhancing negativefeedback inhibition of cortisol release suggests othermechanisms through which such agents may protectagainst or reverse neuropil reduction (Chaput et al 1991;Duman et al 1997; Haddjeri et al 1998; Magarinos et al1999; McEwen 1999). Stimulation of neuron-based5-HT1A receptors inhibits disassociation of the tubulinpolymers that form the dendritic cytoskeleton, and stimu-lation of astroglial-based 5-HT1A receptors induces releaseof the neurotrophic factor S100b, which promotes tubulinpolymerization and inhibits microtubule breakdown(Azmitia 1999). Conversely, administration of serotonin-depleting agents, 5-HT1A receptor antagonists, or antibod-ies to S100b all produce similar losses of dendrites,spines, and/or synapses in adult and developing animals,effects that are blocked by administration of 5-HT1A
receptor agonists or SSRIs (Azmitia 1999).The hypothesis that the abnormalities of gray matter
volume in early-onset or early to midlife mood disordersare related to dendritic reshaping is potentially consistentwith the observations that illness subgroups showing therelevant neuromorphometric changes are also the sub-groups that manifest risk factors for this process. The graymatter reductions in the subgenual PFC and the elevatedCBF and metabolism in the LTC circuit have been morelikely to be evident in primary, familial BD or MDD(Hirayasu et al 1999; O¨ ngur et al 1998) and have not beendemonstrated in subgroups with secondary depression ordepression spectrum disease. Similarly, depressive sub-
824 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

groups with FPDD or BD are reportedly more likely tohave neuroendocrine evidence of elevated limbic–HPAaxis activity (e.g., Lewis et al 1983; Winokur 1982).Finally, the 5-HT1A receptor imaging studies using PETand [carbonyl-11C]WAY-100635 (Drevets et al 1999a;Sargent et al 2000) converge with in vitro studies acquiredpostmortem (Bowen et al 1989; Lo´pez et al 1998) orantemortem (Francis et al 1989) to indicate that 5-HT1A
receptor binding is abnormally decreased in primary MDDand BD. In contrast, the 5-HT1A receptor data from suicidevictims who may have secondary mood disorders orneuropsychiatric conditions other than mood disordershave been highly variable (for a review, see Drevets et al1999b).
Directions for Future Studies
Among the questions raised by the neuroimaging andneuropathologic data is the critical problem of understand-ing cause and effect. The extent to which the abnormalitiesdiscussed above reflect primary pathophysiology thatproduces affective disease as opposed to secondary re-sponses to alterations in behavior, adaptations to chronicillness, or drug treatment remains unclear. Future neuro-imaging studies may elucidate these issues in studies ofhealthy subjects at high familial risk for developing mooddisorders and studies of the relationships between geneticmarkers and neuroimaging correlates of illness and illnessvulnerability.
The author thanks collaborators Joseph L. Price, Ph.D., and Marcus E.Raichle, M.D., for seminal scientific discussions that synthesized manyof the concepts presented herein.
Aspects of this work were presented at the conference “Depression inthe Twenty-First Century: New Insights into Drug Development andNeurobiology,” February 21–22, 2000, Dana Point, California. Theconference was sponsored by the Society of Biological Psychiatrythrough an unrestricted educational grant provided jointly by Pharmacia& Upjohn and Janssen Pharmaceutica.
ReferencesAbercrombie HC, Larson CL, Ward RT, Schaefer SM, Holden
JE, Perlman SB, et al (1996): Metabolic rate in the amygdalapredicts negative affect and depression severity in depressedpatients: An FDG-PET study.Neuroimage3:S217.
Adolphs R, Tranel D, Damasio H, Damasio A (1994): Impairedrecognition of emotion in facial expressions following bilat-eral damage to the human amygdala.Nature372:669–672.
Anderson AK, Phelps EA (1997): Production of facial emotionfollowing unilateral temporal lobectomy.Soc Neurosci Abstr23:2113.
Awad IA, Johnson PC, Spetzler RJ, Awad CA, Carey R (1986):Incidental subcortical lesions identified on magnetic reso-
nance imaging in the elderly, II: Postmortem pathologicalcorrelations.Stroke17:1090–1097.
Azmitia EC (1999): Serotonin neurons, neuroplasticity, andhomeostasis of neural tissue.Neuropsychopharmacology21(suppl 2):33S–45S.
Ballantine HT Jr, Bouckoms AJ, Thomas EK, Giriunas IE(1987): Treatment of psychiatric illness by stereotactic cin-gulotomy.Biol Psychiatry22:807–819.
Baumann B, Danos P, Krell D, Diekmann S, Leschinger A, StauchR, et al (1999): Reduced volume of limbic system-affiliatedbasal ganglia in mood disorders: Preliminary data from a postmortem study.J Neuropsychiatry Clin Neurosci11:71–78.
Baxter LR, Phelps ME, Mazziotta JC, Guze BH, Schwartz JM,Selin CE (1987): Local cerebral glucose metabolic rates inobsessive-compulsive disorder—a comparison with rates inunipolar depression and in normal controls.Arch Gen Psy-chiatry 44:211–218.
Baxter LR, Phelps ME, Mazziotta JC, Schwartz JM, Gerner RH,Selin CE, Sumida RM (1985): Cerebral metabolic rates forglucose in mood disorders.Arch Gen Psychiatry42:441–447.
Baxter LR, Schwartz JM, Phelps ME, Mazziota JC, Guze BH,Selin CE, et al (1989): Reduction of prefrontal cortex glucosemetabolism common to three types of depression.Arch GenPsychiatry46:243–250.
Bechara A, Damasio H, Tranel D, Anderson SW (1998): Disso-ciation of working memory from decision-making within thehuman prefrontal cortex.J Neurosci18:428–437.
Bench CJ, Frackowiak RSJ, Dolan RJ (1995): Changes inregional cerebral blood flow on recovery from depression.Psychol Med25:247–251.
Bench CJ, Friston KJ, Brown RG, Scott LC, Frackowiak RSJ,Dolan RJ (1992): The anatomy of melancholia—focal abnor-malities of cerebral blood flow in major depression.PsycholMed 22:607–615.
Biver F, Goldman S, Delvenne V, Luxen A, DeMaertelaer V,Hubain P, et al (1994): Frontal and parietal metabolic distur-bances in unipolar depression.Biol Psychiatry36:381–388.
Blair RJR, Morris JS, Frith CD, Perrett DI, Dolan RJ (1999):Neural responses to sad and angry expressions.Brain 122:883–893.
Botteron KN, Raichle ME, Heath AC, Price JL, Sternhell KE,Singer TM, Todd RD (1999): An epidemiological twin studyof prefrontal neuromorphometry in early onset depression.Biol Psychiatry45:59S.
Bowen DM, Najlerahim A, Procter AW, Francis PT, Murphy E(1989): Circumscribed changes of the cerebral cortex inneuropsychiatric disorders of later life.Proc Natl Acad SciU S A86:9504–9508.
Bowley MP, Drevets WC, O¨ ngur D, Price JL (in press): Glialchanges in the amygdala and entorhinal cortex in mooddisorders.Biol Psychiatry.
Bremner JD, Innis RB, Salomon RM, Staib LH, Ng CK, Miller HL,et al (1997): Positron emission tomography measurement ofcerebral metabolic correlates of tryptophan depletion-induceddepressive relapse.Arch Gen Psychiatry54:346–374.
Brody AL, Saxena S, Silverman DHS, Alborzian S, FairbanksLA, Phelps ME, et al (1999): Brain metabolic changes inmajor depressive disorder from pre- to post-treatment withparoxetine.Psychiatry Res Neuroimaging91:127–139.
Neuroimaging Studies of Mood Disorders 825BIOL PSYCHIATRY2000;48:813–829

Bromfield EB, Altshuler L, Leiderman DB, Balish M, Ketter TA,Devinsky O, et al (1992): Cerebral metabolism and depres-sion in patients with complex partial seizures.Arch Neurol49:617–623.
Buchel C, Morris J, Dolan RJ, Friston KJ (1998): Brain systemsmediating aversive conditioning: An event related fMRIstudy.Neuron20:947–957.
Buchsbaum MS, Wu J, Siegel BV, Hackett E, Trenary M, AbelL, Reynolds C (1997): Effect of sertraline on regionalmetabolic rate in patients with affective disorder.Biol Psy-chiatry 41:15–22.
Canli T, Zhao Z, Brewer J, Gabrieli JDE, Cahill L (2000):Event-related activation in the human amygdala associateswith later memory for individual emotional experience.JNeurosci20:RC99.
Carmichael ST, Price JL (1995): Limbic connections of theorbital and medial prefrontal cortex in Macaque monkeys.J Comp Neurol363:615–641.
Carney RM, Rich MW, teVelde A, Saini J, Clark K, FreedlandKE (1988): The relationship between heart rate, heart ratevariability and depression in patients with coronary arterydisease.J Psychosom Res32:159–164.
Casey BJ, Thomas KM, Eccard CH, Drevets WC, Dahl RE,Whalen PJ, et al (2000): Functional responsivity of theamygdala in children with disorders of anxiety and majordepression.Neuroimage11(suppl):249.
Chaput Y, deMontigny C, Blier P (1991): Presynaptic andpostsynaptic modifications of the serotonin system by long-term administration of antidepressant treatments. An in vivoelectrophysiologic study in the rat.Neuropsychopharmacol-ogy 5:219–229.
Chimowitz MI, Estes ML, Furlan AJ, Awad IA (1992): Furtherobservations on the pathology of subcortical lesions identifiedon magnetic resonance imaging.Arch Neurol49:747–752.
Cohen RM, Gross M, Nordahl TE, Semple WE, Oren DA,Rosenthal N (1992): Preliminary data on the metabolic brainpattern of patients with winter seasonal affective disorder.Arch Gen Psychiatry49:545–552.
Corsellis J, Jack AB (1973): Neuropathological observations onyttrium implants and on undercutting in the orbito-frontalareas of the brain. In: Laitinen LV, Livingston KE, editors.Surgical Approaches in Psychiatry.Lancaster, UK: Medicaland Technical Publishing, 90–95.
Damasio AR, Grabowski TJ, Bechara A, Damasio H, PontoLLB, Hichwa RD (1998): Neural correlates of the experienceof emotions.Soc Neurosci Abstr24:258.
Damasio AR, Tranel D, Damasio H (1990): Individuals withsociopathic behavior caused by frontal damage fail to respondautonomically to social stimuli.Behav Brain Res41:81–94.
Davis M (1992): The role of the amygdala in conditioned fear.In: Aggleton JP, editor.The Amygdala: NeurobiologicalAspects of Emotion.New York: Wiley-Liss, 255–305.
DeLong MR (1972): Activity of basal ganglia neurons duringmovement.Brain Res40:127–135.
Derdeyn CP, Yundt KD, Videen TO, Carpenter DA, Grubb RLJr, Powers WJ (1998): Increased oxygen extraction fraction isassociated with prior ischemic events in patients with carotidocclusion.Stroke29:754–758.
Dioro D, Viau V, Meaney MJ (1993): The role of the medial
prefrontal cortex (cingulate gyrus) in the regulation of hypo-thalamic-pituitary-adrenal responses to stress.J Neurosci3:3839–3847.
DiRocco RJ, Kageyama GH, Wong-Riley MT (1989): Therelationship between CNS metabolism and cytoarchitecture:A review of 14C-deoxyglucose studies with correlation tocytochrome oxidase histochemistry.Comput Med ImagGraph 13:81–92.
Dolan RJ, Bench CJ, Liddle PF (1993): Dorsolateral prefrontalcortex dysfunction in the major psychoses: Symptom or diseasespecificity?J Neurol Neurosurg Psychiatry56:1290–1294.
Dolan RJ, Fletcher P, Morris J, Kapur N, Deakin JF, Frith CD(1996): Neural activation during covert processing of positiveemotional expressions.Neuroimage4:194–200.
Drevets WC (1999): Prefrontal cortical-amygdalar metabolism inmajor depression.Ann N Y Acad Sci877:614–637.
Drevets WC (2000): Functional anatomical abnormalities inlimbic and prefrontal cortical structures in major depression.Prog Brain Res126:413–431.
Drevets WC (1995): PET and the functional anatomy of majordepression. In: Nakajima T, Ono T, editors.Emotion, Memoryand Behavior-Study of Human and Nonhuman Primates.Tokyo: Japan Scientific Societies Press, 43–62.
Drevets WC, Botteron K (1997): Neuroimaging in psychiatry. In:Guze SB, editor.Adult Psychiatry.St. Louis: Mosby, 53–81.
Drevets WC, Burton H, Simpson JR, Videen TO, Snyder AZ,Raichle ME (1995a): Blood flow changes in human somato-sensory cortex during anticipated stimulation.Nature 373:249–252.
Drevets WC, Frank E, Price JC, Kupfer DJ, Holt D, Greer PJ, etal (1999a): PET imaging of serotonin 1A receptor binding indepression.Biol Psychiatry46:1375–1387.
Drevets WC, Gadde K, Krishnan R (1999b): Neuroimagingstudies of depression. In: Charney DS, Nestler EJ, BunneyBJ, editors. Neurobiology of Mental Illness.New York:Oxford University Press, 394–418.
Drevets WC, Price JL, Simpson JR, Todd RD, Reich T, VannierM, Raichle ME (1997): Subgenual prefrontal cortex abnor-malities in mood disorders.Nature386:824–827.
Drevets WC, Raichle ME (1998): Reciprocal suppression ofregional cerebral blood flow during emotional versus highercognitive processes: Implications for interactions betweenemotion and cognition.Cogn Emotion12:353–385.
Drevets WC, Simpson JR, Raichle ME (1995b): Regional bloodflow changes in response to phobic anxiety and habituation.J Cereb Blood Flow Metab15:S856.
Drevets WC, Spitznagel E, Raichle ME (1995c): Functionalanatomical differences between major depressive subtypes.J Cereb Blood Flow Metab15:S93.
Drevets WC, Todd RD (1997): Depression, mania and relateddisorders. In: Guze SB, editors.Adult Psychiatry.St. Louis:Mosby, 99–141.
Drevets WC, Videen TO, Price JL, Preskorn SH, Carmichael ST,Raichle ME (1992): A functional anatomical study of unipo-lar depression.J Neurosci12:3628–3641.
Drevets WC, Videen TO, Snyder AZ, MacLeod AK, Raichle ME(1994): Regional cerebral blood flow changes during antici-patory anxiety.Abstr Soc Neurosci20:368.
Duman RS, Heninger GR, Nestler EJ (1997): A molecular andcellular theory of depression.Arch Gen Psychiatry54:597–606.
826 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

Ebert D, Feistel H, Barocka A (1991): Effects of sleep depriva-tion on the limbic system and the frontal lobes in affectivedisorders: A study with Tc-99 m-HMPAO SPECT.Psychia-try Res Neuroimaging40:247–251.
Elliott R, Dolan RJ, Frith CD (2000): Dissociable functions inthe medial and lateral orbitofrontal cortex: Evidence fromhuman neuroimaging studies.Cereb Cortex10:308–317.
Fazekas F (1989): Magnetic resonance signal abnormalities inasymptomatic individuals: Their incidence and functionalcorrelates.Eur Neurol29:164–168.
Folstein SE, Peyser CE, Starkstein SE, Folstein MF (1991):Subcortical triad of Huntington’s disease—a model for aneuropathology of depression, dementia, and dyskinesia. In:Carrol BJ, Barrett JE, editors.Psychopathology and theBrain. New York: Raven, 65–75.
Francis PT, Poynton A, Lowe SL, Najlerahim A, Bridges PK,Bartlett JR, et al (1989): Brain amino acid concentrations andCa21-dependent release in intractable depression assessedantemortem.Brain Res494:314–324.
Friston KJ, Frith CD, Liddle PF, Frackowiak RSJ (1991):Comparing functional (PET) images: The assessment ofsignificant change.J Cereb Blood Flow Metab11:690–699.
Frysztak RJ, Neafsey EJ (1994): The effect of medial frontalcortex lesions on cardiovascular conditioned emotional re-sponses in the rat.Brain Res643:181–193.
George MS, Ketter TA, Parekh PI, Horwitz B, Herscovitch P,Post RM (1995): Brain activity during transient sadness andhappiness in healthy women.Am J Psychiatry152:341–351.
Graybiel AM (1990): Neurotransmitters and neuromodulators inthe basal ganglia.Trends Neurosci13:244–254.
Haddjeri N, Blier P, de Montigny C (1998): Long-term antide-pressant treatments result in tonic activation of forebrain5-HT1A receptors.J Neurosci18:10150–10156.
Haxby JV, Horwitz B, Ungerleider LG, Maisog JM, Pietrini P,Grady CL (1994): The functional organization of humanextrastriate cortex: A PET-rCBF study of selective attentionto faces and locations.J Neurosci14:6336–6353.
Herman JP, Cullinan WE (1997): Neurocircuitry of stress:Central control of the hypothalamo-pituitary-adrenocorticalaxis.Trends Neurosci20:78–84.
Hirayasu Y, Shenton ME, Salisbury DF, Kwon JS, Wible CG,Fischer IA, et al (1999): Subgenual cingulate cortex volumein first-episode psychosis.Am J Psychiatry156:1091–1093.
Holsboer F (1995): Neuroendocrinology of mood disorders. In:Bloom FE, Kupfer DJ, editors.Psychopharmacology: TheFourth Generation of Progress.New York: Raven, 957–969.
Iversen SD, Mishkin M (1970): Perseverative interference inmonkeys following selective lesions of the inferior prefrontalconvexity.Exp Brain Res11:376–386.
Kegeles LS, Malone KM, Slifstein M, Anjilvel S, XanthopoulosC, Campell M, et al (1999): Response of cortical metabolicdeficits to serotonergic challenges in mood disorders.BiolPsychiatry45:76S.
Ketter T, Kimbrell TA, Little JT, George MS, Sachs N, WinsbergME, et al (1999, December): Differences and commonaltiesin cerebral function in bipolar compared to unipolar depres-sion. Presented at the 38th annual meeting of the AmericanCollege of Neuropsychopharmacology, Acapulco, Mexico.
Knight G (1965): Stereotactic tractotomy in the surgical treat-ment of mental illness.J Neurol Neurosurg Psychiatry28:30.
Krishnan KRR, McDonald WM, Doraiswamy PM, Tupler LA,Hussain M, Boyko OB, et al (1993): Neuroanatomical sub-strates of depression in the elderly.Eur Arch PsychiatryNeurosci243:41–46.
Krishnan KRR, McDonald WM, Escalona PR, Doraiswamy PM,Na C, Husain MM, et al (1992): Magnetic resonanaceimaging of the caudate nuclei in depression: Preliminaryobservations.Arch Gen Psychiatry49:553–557.
Kupfer DJ, Targ E, Stack J (1992): Electroencephalographicsleep in unipolar depressive subtypes. Support for a biologicaland familial classification.J Nerv Ment Dis170:494–498.
Kuroda M, Price JL (1991): Synaptic organization of projectionsfrom basal forebrain structures to the mediodorsal nucleus ofthe rat.J Comp Neurol303:513.
LaBar KS, Gatenby JC, Gore JC, LeDoux JE, Phelps EA (1998):Human amygdala activation during conditioned fear acquisi-tion and extinction: A mixed trial fMRI study.Neuron20:937–945.
LeDoux J (1996):The Emotional Brain.New York: Simon andSchuster.
LeDoux JE, Thompson ME, Iadecola C, Tucker LW, Reis DJ(1983): Local cerebral blood flow increases during auditoryand emotional processing in the conscious rat.Science221:576–578.
Leichnetz GR, Astruc J (1976): The efferent projections of themedial prefrontal cortex in the squirrel monkey (saimirisciureus).Brain Res109:455–472.
Lesser IM, Mena I, Boone KB, Miller BL, Mehringer CM, MohlM (1994): Reduction of cerebral blood flow in older de-pressed patients.Arch Gen Psychiatry51:677–686.
Lewis DA, Kathol RG, Sherman BM, Winokur G, Schlesser MA(1983): Differentiation of depressive subtypes by insulinsubsensitivity in the recovered phase.Arch Gen Psychiatry40:167–170.
Lewis DA, McChesney C (1985): Tritiated imipramine bindingdistinguishes among subtypes of depression.Arch Gen Psy-chiatry 42:485–488.
Links JM, Zubieta JK, Meltzer CC, Stumpf MJ, Frost JJ (1996):Influence of spatially heterogenous background activity on“hot object” quantitation in brain emission computed tomog-raphy.J Comput Assist Tomogr20:680–687.
Lopez JF, Chalmers DT, Little KY, Watson SJ (1998): Regula-tion of serotonin1A, glucocorticoid, and mineralocorticoidreceptor in rat and human hippocampus: Implications for theneurobiology of depression.Biol Psychiatry43:547–573.
Magarinos AM, Deslandes A, McEwen BS (1999): Effects ofantidepressant and benzodiazepine treatments on the dendriticstructure of CA3 pyramidal neurons after chronic stress.EurJ Pharmacol371:113–122.
Magistretti PJ, Pellerin L, Martin JL (1995): Brain energymetabolism: An integrated cellular perspective. In: BloomFE, Kupfer DJ, editors.Psychopharmacology: The FourthGeneration of Progress.New York: Raven, 921–932.
Manji HK, Moore GJ, Chen G (1999): Lithium at 50: Have theneuroprotective effects of this unique cation been over-looked?Biol Psychiatry46:929–940.
Mayberg HS, Brannan SK, Mahurin RK, Jerabek PA, BrickmanJS, Tekel JL, et al. (1997): Cingulate function in depression:A potential predictor of treatment response.Neuroreport8:1057–1061.
Neuroimaging Studies of Mood Disorders 827BIOL PSYCHIATRY2000;48:813–829
Mayberg HS, Liotti M, Brannan SK, McGinnis BS, Mahurin RK,Jerabek PA, et al (1999): Reciprocal limbic-cortical functionand negative mood: Converging PET findings in depressionand normal sadness.Am J Psychiatry156:675–682.
Mayberg HS, Starkstein SE, Sadzot B, Preziosi T, Andrezejew-ski PL, Dannal RF, et al (1990): Selective hypometabolism inthe inferior frontal lobe in depressed patients with Parkin-son’s disease.Ann Neurol28:57–64.
Mayeux R (1982): Depression and dementia in Parkinson’sdisease. In: Marsden CO, Fahn S, editors.Movement Disor-ders.London: Butterworth, 75–95.
McEwen BS (1999): Stress and hippocampal plasticity.AnnuRev Neurosci22:105–122.
Mogenson GJ, Brudzynski SM, Wu M, Yang CR, Yim CCY(1993): From motivation to action: A review of dopaminergicregulation of limbic3 nucleus3 accumbens3 ventralpallidum3 pedunculopontine nucleus circuitries involved inlimbic-motor integration. In: Kalivas PW, Barnes CD, edi-tors. Limbic Motor Circuits and Neuropsychiatry.London:CRC Press, 193–236.
Morgan MA, LeDoux JE (1995): Differential contribution ofdorsal and ventral medial prefrontal cortex to the acquisitionand extinction of conditioned fear in rats.Behav Neurosci109:681–688.
Morris JS, Frith CD, Perrett DI, Rowland D, Young AW, CalderAJ, Dolan RJ (1996): A differential neural response in thehuman amygdala to fearful and happy facial expression.Nature383:812–815.
Musselman DL, Nemeroff CB (1993): The role of corticotropin-releasing factor in the pathophysiology of psychiatric disor-ders.Psychiatr Ann23:676–681.
Nauta WJH (1973): Connections of the frontal lobe with thelimbic system. In: Laitinen LV, Livingston KE, editors.Surgical Approaches in Psychiatry. Baltimore: UniversityPark Press, 303–314.
Nauta WJH, Domesick V (1984): Afferent and efferent relation-ships of the basal ganglia. In: Evered D, O’Connor M, editors.Function of the Basal Ganglia,CIBA Foundation Sympo-sium 107. London: Pitman, 3–29.
Newcombe R (1975): The lesion in stereotactic subcaudatetractotomy.Br J Psychiatry126:478.
Nobler MS, Sackeim HA, Prohovnik I, Moeller JR, Mukherjee S,Schnur DB, et al (1994): Regional cerebral BF in mooddisorders, III. Treatment and clinical response.Arch GenPsychiatry51:884–897.
Nofzinger EF, Nichols TE, Meltzer CC, Price J, Steppe DA,Miewald JM, et al (1999): Changes in forebrain function fromwaking to REM sleep in depression: Preliminary analyses of[18F]FDG PET studies.Psychiatry Res Neuroimaging91:59–78.
Nowak G, Ordway GA, Paul IA (1995): Alterations in theN-methyl-D-aspartate (NMDA) receptor complex in the fron-tal cortex of suicide victims.Brain Res675:157–164.
Ongur D, Drevets WC, Price JL (1998): Glial reduction in thesubgenual prefrontal cortex in mood disorders.Proc NatlAcad Sci U S A 95:13290–13295.
Paul IA, Nowak G, Layer RT, Popik P, Skolnick P (1994):Adaption of the N-methyl-D-aspartate receptor complex fol-lowing chronic antidepressant treatments.J Pharmacol ExpTher 269:95–102.
Pearlson GD, Barta PE, Powers RE, Menon RR, Richards SS,Aylward EH, et al (1997): Medial and superior temporal gyralvolumes and cerebral asymmetry in schizophrenia versusbipolar disorder.Biol Psychiatry41:1–14.
Phelps EA, Anderson AK (1997): Emotional memory: Whatdoes the amygdala do?Curr Biol 7:R311–R314.
Poline JB, Holmes A, Worsley K, Friston KJ (1997): Makingstatistical inferences. In: Frackowiak R, Friston KJ, Frith CD,Dolan RJ, Mazziotta JC, editors.Human Brain Function.London: Academic Press, 85–106.
Price JL (1999): Networks within the orbital and medial prefron-tal cortex.Neurocase5:231–241.
Price JL, Carmichael ST, Drevets WC (1996): Networks relatedto the orbital and medial prefrontal cortex: A substrate foremotional behavior? In: Holstege G, Bandler R, Saper CB,editors.Progress in Brain Research: The Emotional MotorSystem.107:523–536.
Raichle ME (1987): Circulatory and metabolic correlates of brainfunction in normal humans. In: Brookhart JM, MountcastleVB, editors.Handbook of Physiology—the Nervous System V.Baltimore: American Physiological Society, 643–674.
Rajkowska G (2000): Postmortem studies in mood disordersindicate altered numbers of neurons and glial cells.BiolPsychiatry48:766–777.
Rajkowska G, Miguel-Hidalgo JJ, Wei J, Dilley G, Pittman SD,Meltzer HY, et al (1999): Morphometric evidence for neuro-nal and glial prefrontal cell pathology in major depression.Biol Psychiatry45:1085–1098.
Rajkowska G, Selemon LD, Goldman-Rakic PS (1997): Markedglial neuropathology in prefrontal cortex distinguishes bipolardisorder from schizophrenia.Schizophr Res24:41.
Rauch SL, Jenike MA, Alpert NM, Baer L, Breiter H, Savage CR,Fischman AJ (1994): Regional cerebral blood flow measuredduring symptom provocation in obsessive-compulsive disorderusing oxygen 15-labeled carbon dioxide and positron emissiontomography.Arch Gen Psychiatry51:62–70.
Reiman EM, Lane RD, Ahern GL, Schwartz GE, Davidson RJ,Friston KJ, et al (1997): Neuroanatomical correlates ofexternally and internally generated human emotion.Am JPsychiatry154:918–925.
Ring HA, Bench CJ, Trimble MR, Brooks DJ, Frackowiak RSJ,Dolan RJ (1994): Depression in Parkinson’s disease: Apositron emission study.Br J Psychiatry165:333–339.
Rogers RD, Everitt BJ, Baldacchino A, Blackshaw AJ, SwainsonR, Wynne K, et al (1999): Dissociable deficits in thedecision-making cognition of chronic amphetamine abusers,opiate abusers, patients with focal damage to prefrontalcortex, and tryptophan-deleted normal volunteers: Evidencefor monoaminergic mechanisms.Neuropsychopharmacology20:322–339.
Rolls ET (1995): A theory of emotion and consciousness, and itsapplication to understanding the neural basis of emotion. In:Gazzaniga MS, editor.The Cognitive Neurosciences.Cam-bridge, MA: MIT Press, 1091–1106.
Sapolsky RM (1996): Stress, glucocorticoids, and damage to thenervous system: The current state of confusion.Stress1:1–19.
Sargent PA, Kjaer KH, Bench CJ, Rabiner EA, Messa C, MeyerJ, et al (2000): Brain serotonin1A receptor binding measuredby positron emission tomography with [11C]WAY-100635.Arch Gen Psychiatry57:174–180.
828 W.C. DrevetsBIOL PSYCHIATRY2000;48:813–829

Schneider F, Gur RE, Alav A, Mozley LH, Smith RJ, MozleyPD, et al (1995): Mood effects on limbic blood flow correlatewith emotion self-rating: A PET study with oxygen-15labeled water.Psychiatry Res Neuroimaging61:265–283.
Schultz W (1997): Dopamine neurons and their role in rewardmechanisms.Curr Opin Neurobiol7:191–197.
Scott SK, Young AW, Calder AJ, Hellawell DJ, Aggleton JP,Johnson M (1997): Impaired auditory recognition of fear andanger following bilateral amygdala lesions.Nature385:254–257.
Shulman GL, Corbetta M, Buckner RL, Fiez JA, Miezen FM,Raichle ME, Petersen SE (1997): Common blood flowchanges across visual tasks: II. Decreases in cerebral cortex.J Cogn Neurosci9:647–662.
Smith KA, Morris JS, Friston KJ, Cowen PJ, Dolan RJ (1999):Brain mechanisms associated with depressive relapse andassociated cognitive impairment following tryptophan deple-tion. Br J Psychiatry174:525–529.
Sporn J, Sachs G (1997): The anticonvulsant lamotrigine intreatment-resistant manic-depressive illness.J Clin Psycho-pharmacol17:185–189.
Starkstein SE, Robinson RG (1989): Affective disorders andcerebral vascular disease.Br J Psychiatry154:170–182.
Sullivan RM, Gratton A (1999): Lateralized effects of medialprefrontal cortex lesions on neuroendocrine and autonomicstress responses in rats.J Neurosci19:2834–2840.
Teneback CC, Nahas Z, Speer AM, Molloy M, Stallings LE,Spicer KM, et al (1999): Changes in prefrontal cortex andparalimbic activity in depression following two weeks ofdaily left prefrontal TMS.J Neuropsychiatry Clin Neurosci11:426–435.
Timms RJ (1977): Cortical inhibition and facilitation of thedefense reaction.J Physiol (Lond)266:98–99.
Veith RC, Lewis N, Linares OA, Barnes RF, Raskind MA,Villacres EC, et al (1994): Sympathetic nervous systemactivity in major depression.Arch Gen Psychiatry51:411–422.
Winokur G (1982): The development and validity of familialsubtypes in primary unipolar depression.Pharmacopsychia-try 15:142–146.
Winokur G (1997): All roads lead to depression: Clinicallyhomogenous, etiologically heterogenous.J Affect Disord45:97–108.
Wooten GF, Collins RC (1981): Metabolic effects of unilaterallesion of the substantia nigra.J Neurosci1:285–291.
Wu J, Gillin C, Buchsbaum MS, Hershey T, Johnson JC, BunneyWE (1992): Effect of sleep deprivation on brain metabolismof depressed patients.Am J Psychiatry149:538–543.
Young EA, Kotun J, Haskett RF, Grunhaus L, Greden JF,Watson SJ, Akil H (1993): Dissociation between pituitary andadrenal suppression to dexamethasone in depression.ArchGen Psychiatry50:395–403.
Neuroimaging Studies of Mood Disorders 829BIOL PSYCHIATRY2000;48:813–829