Embed Size (px)
Citation preview

Neuroimaging Evaluationin Neocortical Epilepsies
N. Colombo, N. Bargalló, and D. Redaelli
ContentsMalformations of Cortical Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4General Definition of Entities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Clinical Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Imaging Strategy (Applicable to all Epilepsy Patients) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Different Subtypes of MCDs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Focal Cortical Dysplasia (Type I, Type II, Type III) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
This publication is endorsed by: European Society ofNeuroradiology (www.esnr.org)
N. Colombo (*)Neuroradiology Department, Centro Regionale Chirurgiadell’Epilessia “Claudio Munari”, ASST Grande OspedaleMetropolitano Niguarda Cà Granda, Milano, Italye-mail: [email protected];[email protected]
N. BargallóMagnetic Resonance Image Core Facility. Institut deInvestigació Biomèdica August Pi I Sunyer (IDIBAPS),Image Diagnosis Center (CDIC). Hospital Clínic deBarcelona, Barcelona, Spaine-mail: [email protected]
D. RedaelliNeuroimaging Laboratory Scientific Institute IRCCSEugenio Medea, Lecco, Italye-mail: [email protected]
# Springer International Publishing AG, part of Springer Nature 2018F. Barkhof et al. (eds.), Clinical Neuroradiology,https://doi.org/10.1007/978-3-319-61423-6_51-1
1

General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Epidemiology/Demographic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Clinical Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Pathological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
FCD Type I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9EEG Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Pathological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9MRI Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Ancillary Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Surgical Outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
FCD Type II (a–b) (Taylor’s FCD) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Epidemiology/Demographic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10EEG Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Pathological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Etiology - Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11MRI Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Ancillary Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Surgical Outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Polymicrogyria (PMG) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13EEG Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Pathological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Etiology - Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14MRI Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Ancillary Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Surgical Treatment and Outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Heterotopias (HTP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17EEG Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Pathological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Etiology - Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17MRI Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Ancillary Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Surgical Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Hemimegalencephaly (HME) or Unilateral Megalencephaly . . . . . . . . . . . . . . . . . . . . . . . . 18General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18EEG Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20MRI Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Ancillary Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Surgical Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Acquired Epileptogenic Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
2 N. Colombo et al.

Post-Stroke Epilepsy (PSE) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Epidemiology/Demographic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Pathological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24EEG Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Neuroimaging Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Post–Traumatic Epilepsy (PTE) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25General Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Epidemiology/Demographic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26EEG Pattern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Neuroimaging Features and Structured Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Clinical Cases and Sample Reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Checklist for Reporting MRI in Neocortical Epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Sample Report 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Patient History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Clinical Suspect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Purpose of MR Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Imaging Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Full Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Ancillary Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Comment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Sample Report 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Patient History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Clinical Suspect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Purpose of MR Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Imaging Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Contrast Agent and Dose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Ancillary Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Full Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Interpretation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Comment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Sample Report 3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Patient History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Clinical Suspect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Purpose of MR Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Imaging Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Ancillary Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Full Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Interpretation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Comment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
AbstractNeocortical epilepsy is a chronic conditioncharacterized by focal or generalized seizuresstarting within the cortex of any lobe of thebrain. In this chapter, some of the most
common epileptogenic lesions will bediscussed, including malformations of corticaldevelopment (MCDs) comprising focal corti-cal dysplasia (FCD), polymicrogyria (PMG),heterotopia (HTP), hemimegalencephaly
Neuroimaging Evaluation in Neocortical Epilepsies 3

(HME), and acquired lesions after vascular andtraumatic injuries that can develop to post-stroke epilepsy (PSE) or post-traumatic epi-lepsy (PTE). Some other lesions like corticaltubers of tuberous sclerosis complex and cav-ernous angioma, which can be associated toneocortical epilepsy, are treated in other chap-ters of this book. Clinical neuroradiologyplays a pivotal role to establish the diagnosisand to select patient candidate to surgery. Theradiological technique fundamental for neo-cortical epilepsies is brain magnetic resonanceimaging (MRI). It is mandatory in patients withdrug-resistant focal epilepsy (DRFE) aimed todetect the suspected associated anatomicallesion and to define its location, extension,and relationship with the eloquent brain areas.
An epilepsy-specific protocol is needed toidentify even very subtle lesions, particularlytiny FCDs. Knowledge of the electro-clinicalpresentation is key for planning a correct MRIexamination to use the proper sequence angu-lation. The MRI study should cover the wholebrain including different weighted sequencesin three planes. Interpretation should beperformed by experienced readers and particu-larly focused on the brain area suspected as theepileptogenic zone (EZ). In non-lesional MRIpatients, re-evaluation of MRI could be helpfulafter all ancillary tests are completed, includingnuclear medicine and invasive electrophysio-logical investigation, such as stereo-electroencephalography (SEEG), to search ret-rospectively for subtle structural lesions.
KeywordsNeocortical epilepsy ·Malformation of corticaldevelopment · Focal cortical dysplasia · Post-stroke epilepsy · Post-traumatic epilepsy
List of Abbreviations18F-FDG PET 18-Fluoro-2-deoxyglucose
positron emissiontomography
DRFE Drug-resistant focal epilepsyEZ Epileptogenic zoneFCD Focal cortical dysplasiaHME Hemimegalencephaly
HTP HeterotopiaMCDs Malformations of cortical
developmentPMG PolymicrogyriaPSE Post-stroke epilepsyPSS Post-stroke seizuresPTE Post-traumatic epilepsyPTS Post-traumatic seizuresSISCOM Subtracted ictal SPECT
co-registered to MRI
Malformations of CorticalDevelopment
General Definition of Entities
Malformations of cortical development (MCDs)are a broad range of disorders that result fromdisruption of the major steps of cortical develop-ment. The Barkovich classification system basedon imaging, genetic testing, and molecular biol-ogy recognizes three major groups of MCDs com-prising disorders of (i) abnormal neuronal andglial proliferation, (ii) neuronal migration, and(iii) abnormal post-migrational development(Barkovich et al. 2012).
Epidemiology
MCDs as a group are the third most frequent histo-pathological category in surgical specimensobtained from DRFE, after hippocampal sclerosisand tumors. In a recent published multicenter studyfrom 12 European countries, MCDs were found in20%of adult specimens and around 40%of resectedspecimens in children (Blümcke et al. 2017).
Clinical Features
MCDs are common causes of refractory epilepsyin children and young people. Focal or general-ized seizures are to a variable extend associatedwith specific histologic subtypes and to localiza-tion/extension of MCDs. Neurological deficits,developmental delay, and impairment of variouscognitive functions can be present in someMCDs.
4 N. Colombo et al.

Imaging Strategy (Applicable to allEpilepsy Patients)
• Magnetic Resonance Imaging.An epilepsy-specific MRI protocol is man-
datory to achieve a prompt and accurate visu-alization of any subtypes ofMCDs (Table 1). Ageneral agreement is to acquire multi-sequenceMRI with a magnetic field strength of at least1.5 T or 3.0 T in clinical practice. Severalstudies showed that 3 T MRI provides anincrease in signal-to-noise ratio that improvesimage contrast and resolution, useful for betterdetection and characterization of MCDs, espe-cially subtle FCDs. Seven Tesla MRI, which isnow available in some institutions, provideseven a superior signal-to-noise ratio. The gen-eral agreement is that high-field-strength imag-ing should be considered for patients withintractable epilepsy and normal or equivocalfindings on 1.5 T MRI.
The baseline protocol utilized in epilepticpatients requires about 35–40 min.
Tri-planar 2D FLAIR T2-weighted or 3DFLAIR T2-weighted sequences (with or with-out fat saturation) are particularly helpful forthe detection and characterization of FCDs(Fig. 1) owing to their high contrast resolution.Similarly the 3D volumetric gradient echoT1-weighted sequences (SPGR, FFE, TFE,TFLASH, MP-RAGE) are useful for diagnos-tic purposes, due to their excellent gray matter/white matter (GM/WM) differentiation; theycan be reformatted, reoriented, and re-slicedwith different angulations for precise localiza-tion of lesions visualized on other sequences.
Susceptibility-weighted images (SWI) and/orT2*WI (gradient echo, fast field echo) are usefulto detect calcifications or hemorrhage.
Furthermore 3D-T1-weighted dataset are cru-cial for surgical purposes, as starting point forpost-processing multiplanar (MPR) and surface-based reconstructions of cortical surface, com-puted by software packages such as FreeSurfer.Contrast-enhanced T1-weighted images are notroutinely acquired, unless a tumor is suspected.
Sequences are acquired oblique-axial andoblique-coronal i.e., parallel and perpendicular
to the major axis of hippocampus for temporallobe epilepsy and parallel and perpendicular tothe bi-commissural line for extra-temporalepilepsy.
Knowledge of the electro-clinical presenta-tion is a key point to perform a correct MRIexamination, in order to focus the attention onthe brain area suspected as the EZ and to usethe proper sequence angulation.
Imaging strategy in children should takeinto account that the GM/WM signal ratiovaries during the process of myelination andthat contrast between GM andWM is maximalbefore the progression of myelination. Before6 months of age, T2WI are able to delineate thedysplastic cortex that appears hypointense incomparison to the physiological hyperintensityof the unmyelinated white matter (Fig. 2).Therefore if seizures start before 6 months ofage, MRI should be performed as soon as pos-sible; during myelination MRI is frequentlyunrevealing, and in most cases, it should berepeated at the end of myelination (around30 months of age). In case of epileptic enceph-alopathy and conclusive electro-clinical results
Table 1 Standardized MRI protocol for epilepsy
Mandatory sequences
Axial TSE T2-weighted, 5 mm (1,5 T), 3 mm (3 T)
Tri-planar �3 mm or 3D volumetric FLAIR, withisotropic 1 mm voxels
Coronal TSE T2-weighted, �3 mm
Coronal TSE IR T1-weighted, �3 mm
Axial diffusion-weighted (DWI), 5 mm
3D volumetric gradient echo T1-weighted (SPGR,FFE, TFE, TFLASH, MP-RAGE), 1 mm contiguousslices, isotropic 1 mm voxels or non-isotropic voxel(0.5 � 0.5 � 1 mm), depending on scan manufacturer,with additional multiplanar and surface reconstructions(e.g., by FreeSurfer)
Susceptibility-weighted images (SWI) and/or GRET2*-weighted (gradient echo, fast field echo) to detectcalcifications or hemorrhage.
Optional sequences
Contrast-enhanced T1-weighted (when BBB damageis suspected, not in MCDs).
N.B. sequences parameters should be adapted and opti-mized on every single magnet. Resetting of pulsesequences is required at every updating of the magnet
Neuroimaging Evaluation in Neocortical Epilepsies 5

that allow the definition of the epileptogeniczone (EZ), even in MRI-negative patients,there is no reason to postpone surgery bywaiting for myelin maturation andrepeated MRI.
Advanced surface-based and texture analy-sis, searching for signal and morphologicalabnormalities, can produce maps of textureand morphometry specifically helping in thedetection of MRI-negative FCDs.
Diffusion-weighted images (DWI) are help-ful to detect transient seizure-induced abnor-malities in the acute phase of seizures,characterized by cytotoxic edema withrestricted diffusion, which usually normalizes
in few days. These transient alterations maypresent with heterogeneous topographic distri-bution, they are functional in origin, and theyshould be recognized to make a proper differ-ential diagnosis with structural lesions.
• Computed Tomography (CT) is often a firstscreening modality in adult patients with a firstepileptic manifestation but has no value for thediagnosis of FCD.
• Ancillary Technique including 18-fluoro-2-deoxyglucose positron emission tomography(18F-FDG PET) and single-photon emissioncomputed tomography (SPECT) can showareas of abnormal metabolism compatiblewith the localization of the EZ.
Fig. 1 FCD Type IIb deep in the sulcus. Sagittal, axial,coronal FLAIR T2WI (a–d), coronal IR T1WI (e), coronalTSE T2WI (f). Cortical thickening is seen in the bottom ofthe right postcentral sulcus. Owing to the direction, the“transmantle sign” is detected only on sagittal (a) and
coronal images (d–f) as increased signal of the subcorticalwhite matter on FLAIR T2WI (a, d) and TSE T2WI (f)decreasing on T1WI (e), with funnel-shaped appearance,running toward the ventricle. The gray/white matter junc-tion is sharp on T2WI (a–d, f) and blurred on T1WI (e)
6 N. Colombo et al.

Treatment
Surgical treatment is an option if the epileptogeniczone (EZ) is well defined (see Sect. IX, Chap. 7).
Different Subtypes of MCDs
1. Focal cortical dysplasia (Type I, Type IIa-IIb,Type III)
2. Polymicrogyria (PMG)3. Heterotopias (HTP)4. Hemimegalencephaly (HME) – unilateral
megalencephaly
Focal Cortical Dysplasia (Type I, TypeII, Type III)
General Definition of Entity
FCD is a peculiar malformation of cortical devel-opment, comprising three histologic subtypes(Type I, Type II, Type III), due to abnormal neu-ronal and glial maturation, differentiation, andcortical layering (Blümcke et al. 2011; Barkovichet al. 2012).
Fig. 2 Polymicrogyria in a 1-year-old boy. Axial 2DTSE-T2WI (a, b), axial 2D FLAIR T2WI (c, d), sagittal,and axial images from 3D FFE-T1W sequence (e, f). In theright frontal-parietal-occipital region, the malformed cor-tex appears thickened, and it is well detected owing to the
hypointense signal on T2WI compared to hyperintensity ofthe physiologically unmyelinated white matter (a–d). On3D images (e, f), all the MR features of polymicrogyria arebetter defined as irregularly bumpy cortical surface andfinely irregular gray/white matter junction
Neuroimaging Evaluation in Neocortical Epilepsies 7

Epidemiology/Demographic
All subtypes of FCDs, as a whole, are the mostfrequent cortical malformations found in surgicalspecimens, accounting for 70.6% of cases.
Incidence derived from surgical series how-ever is biased since it represents a mere subset ofpotential FCD diagnoses. They have been dem-onstrated in 30–50% of histopathology specimensof MRI-negative patients who undergo epilepsysurgery.
Clinical Features
DRFE with different semiology and frequency ofseizures. The electro-clinical aspect of seizuresdistinguishes FCD Type II from FCD Type I andfrom other MCDs (Tassi et al. 2012).
Pathological Features
The three histologic subtypes, recognized by theILAE (International League Against Epilepsy)
classification system, include FCD Type I iso-lated, characterized by abnormal radial and/ortangential cortical lamination (Type I a–c); FCDType II in which cortical dyslamination is associ-ated with abnormal cytology, such as large dys-morphic neurons (DNs) without balloon cells(BC) (Type IIa) and with BC (Type IIb); andFCD Type III in which cortical dyslamination(similar to FCD Type I isolated) occurs withanother lesion, e.g., hippocampal sclerosis,glioneuronal tumors, vascular malformation, andlesions acquired during early life (Type III a–d)(Fig. 3).
FCD Type I
General Definition of Entity
FCDs Type I are malformations presumably dueto post-migration abnormal cortical development.They can be “isolated” (pure) (FCD Type I a–c) or“associated” with other principal pathologies(FCD Type III a–d). FCDs Type III (not treatedin the present chapter) are still under investigation
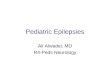
Fig. 3 Photomicrographs showing different types of focalcortical dysplasia (FCD). Thionine stain shows a micro-columnar organization of the cortex without any laminarorganization as typical of FCD Type Ia (a), immunohisto-chemical staining with NeuN antibody (selectively label-ling the neurons) (b). In this case, a FCD Type Ib, acomplete laminar disorganization of the cortex is revealed,and with the exception of Layer I, the other cortical layersare not detectable. A FCD Type IIa is shown in figure (c)and (d) immunostained, respectively, using NeuN and SMI
311 antibodies (the later specifically stains theneurofilaments); this dysplasia is characterized by a lami-nar disorganization of the cortex plus the presence of giantsand dysmorphic neurons through the cortical ribbon (inserte). A typical FCD Type IIb is shown in f; note the profounddisruption of the cortical lamination and the presence ofdysmorphic neurons (g) and balloon cells (h). Calibrationbar: (a), (b), (c), (d), and (f) 200 μm; (e), (g), and (h) 60 μm(Courtesy of: Prof. R. Spreafico, Fondazione IRCCS,Instituto Neurologico “C.Besta”, Milano)
8 N. Colombo et al.

and considered acquired lesions whose etiology isrelated to the associated principal lesions.
Epidemiology
“Isolated” FCD Type I is rare, accounting for2.8% of the total population in a recent reportedsurgical series and representing 16.6% of allFCDs subtypes (Blümcke et al. 2017).
Clinical Scenario
High frequency of early-onset seizures, startingbetween 7.4 � 9.6 years of age. Seizures havedifferent semiology including infantile spasms,generalized tonic-clonic seizures, and epilepticencephalopathy. Drug resistance is similar forFCD Type I and Type II.
EEG Patterns
FCD Type I is not associated to a defined electro-clinical phenotype, unlike FCD Type II. InterictalEEG is often misleading because of large, fre-quently bilateral ictal-onset zone or because ofmultifocal or generalized pattern.
Pathological Features
Characterized by abnormal radial and/or tangen-tial cortical lamination (Type I a–c) withoutabnormal cells.
MRI Features and Structured Reporting
The dysplastic lesion may be revealed by regionalbrain hypoplasia, with volumetric reduction of thewhite matter that exhibits mild increased signal onT2WI and decreased signal on T1WI (Table 2).No real change in cortical thickness is seen. TheGM/WM junction is blurred (Fig. 4). Corticalgyration anomalies, with no gross signal alter-ations, can be the only sign of the dysplasia
(Holthausen et al. 2014). No mass effect, calcifi-cations, or contrast enhancement is found.Caveat: such subtle changes, when present, maybe non-specific, and they should be precisely cor-related with the electro-clinical data. It is almostimpossible to delineate the precise extent of thelesion that goes far beyond the MRI-visible alter-ations. The location is mainly temporal andtemporal-occipital and frequently multilobar(Fig. 4), sub-hemispheric, or hemispheric.
Unrevealing MRI study is reported in 20–33%of cases in different surgical series (Tassi et al.2010; Holthausen et al. 2014).
MRI post-processing using surface-based anal-ysis may help in the evaluation of sulco-gyralanomalies, which may be the only sign ofdysplasia.
Ancillary Techniques
The value and practical use of interictal 18F-FDGPET for FCDs I are still controversial since noprecise correlation between hypometabolicregions and MRI features has been documentedin sufficiently large series.
Surgical Outcome
The surgical outcome is poor with less than 50%of patient becoming seizure-free (Tassi et al.2010).
FCD Type II (a–b) (Taylor’s FCD)
General Definition of Entity
FCD Type II is classified as focal malformationdue to abnormal neuronal and glial proliferation(Barkovich et al. 2012). It is consistent with theoriginal description by Taylor et al. (1971), andthus, it is also referred to as Taylor’s FCD.
Neuroimaging Evaluation in Neocortical Epilepsies 9

Epidemiology/Demographic
It is the most common subtypes of FCDs found insurgical specimens, accounting for 45,3% of thetotal cases of FCDs. It is reported in 17.0% of thetotal pediatric population having surgery forDRFE (Blümcke et al. 2017).
Clinical Scenario
FCD Type II is highly epileptogenic lesion, fre-quently associated with early-onset of seizures,ranging between 5.6 and 6.9 years of age andsleep-related seizures.
Table 2 Differential MRI features for the different subtypes of FCDs
WM signal: T2WIhyper & T1WI hypo
Corticalthickening
GM/WMblurring
Tapering(transmantle sign)
Gyrationanomalies
Focal brainhypoplasia
FCDTypeIIb
Strong Yes Yes Yes (hallmark forFCD Type IIb)
Yes No
FCDTypeIIa
Less strong Yes Yes Less frequent Yes No
FCDType I
+/� subtle No Subtle No Yes Yes
Fig. 4 FCD Type I in the left temporal-parietal lobes in a2-year-old boy. Axial TSE T2WI (a), coronal FLAIRT2WI (b), coronal IR T1WI (c), coronal TSE T2WI (d),sagittal FLAIR T2WI, respectively, on the left and normalright side (e–f). Patient with physiologically incompletemyelination and partial merging of the gray matter-whitematter signal, which prevents the precise definition of the
dysplastic area. However, in the left temporal-parietallobes, mild blurring of the cortico-medullary junction andsubtle increased signal on T2WI of the white matter areevident (white arrows in a, b, d, e) by comparison with thecontralateral normal side (a, b, d, f) helping to detect thedysplasia. Hypoplasia of left anterior temporal lobe is alsonoticed (white arrows in a, b-d)
10 N. Colombo et al.

EEG Patterns
The scalp EEG recordings show a peculiarelectrographic pattern (not observed in patientswith other MCDs) characterized by rhythmic orpseudo-rhythmic spikes and polyspikes(“brushes”) enhanced during non-REM sleepand also associated with well-localized, brief,low-voltage fast activity. The occurrence of“brushes” is significantly more frequent in FCDType IIb. The stereo-electroencephalography(SEEG) recordings showed a peculiarintralesional pattern consisting of the absence ofphysiological background activity withsub-continuous rhythmic spikes and polyspikesand waves, usually with a frequency rangingbetween 1 and 3 Hz, alternating with short burstsof fast discharges (“brushes”) and interrupted bysuppression of electrical activity (Tassi et al.2012).
Pathological Features
They are characterized by complete corticaldyslamination associated with large dysmorphicneurons (DNs) without balloon cells (BCs) (TypeIIa) and with BCs (Type IIb). Ultrastructural stud-ies have shown a dysmyelination process associ-ated with severe fiber loss and abnormal cells inthe white matter of FCD Type IIb that explains thestrong signal hyperintensity on T2W MRIsequences. Less severe histopathological featureswere found in FCD Type IIa, thus reflecting theirless evident MRI alterations. The hypothesis isthat white matter abnormalities in FCD Type IIbare due to defects of the myelination processesand maturation, impaired by the presence of BCs.
Etiology - Pathophysiology
No genetic impairment has been found so far inFCDs, confirming that this dysplasia did not rep-resent somatic mosaic forms of tuberous sclerosiscomplex (TSC). However, there is some evidencethat BCs and DNs in FCD Type II express pro-genitor proteins and activation of the mammalian
target of rapamycin (mTOR) pathways. Asuggested hypothesis is that an external or envi-ronmental phenomenon can hit some of the pre-cursor cells, acting on the cytoskeletal frameworkduring the very early stage of cortical develop-ment and leading to the abnormal cells formationand to disruption of the normal cortical develop-ment due to mTOR activation (Rossini et al.2017).
MRI Features and Structured Reporting
Focal cortical thickening with blurred GM/WMjunction on T1WI and variably blurred or fairlysharp on T2WI (Figs. 1, 5, 8, 9) (Table 2). Thesubcortical white matter shows increased signalon FLAIR/T2WI and decreased signal on T1WI,frequently appearing as a radial-oriented orfunnel-shaped stripe of T2 hyperintensity, runningtoward the ventricle, referred as the “transmantlesign” (Figs. 1, 5, 7, 9). Cortical gyration is fre-quently abnormal, ranging from focal enlarge-ment of the subarachnoid spaces to highlydysmorphic cortical convolutions, with deep-running sulci (Fig. 6), better appreciated using3D T1W sequences and surface reconstructions(Fig. 8). There are no definitive distinctive MRIfeatures of FCD Type IIa versus Type IIb, but the“transmantle” sign is significantly more frequentin FCD Type IIb (Colombo et al. 2012). FCDs canbe very focal involving the “bottom of sulcus”(BOS) (Figs. 1, 5, 6, 9) or the “crown of gyrus”(similar to cortical tubers) (Fig. 7) or more exten-sive, involving one or multiple lobes (Fig. 8). Thelocation is mainly extra-temporal, with a predilec-tion for the frontal lobes (Figs. 6, 7); less fre-quently they are multilobar (especially FCDType IIa) (Fig. 8). The MRI aspect of FCDs canbe very similar to single cortical tuber. Unliketumors and cortical tubers, there is no mass effect,calcifications, or contrast enhancement.
The detection rate for FCDs Type II rangesbetween 70% and 90% in different surgical seriesand is higher (90%) for Type IIb than for Type IIa(50%) (Colombo et al. 2012).
MR post-processing techniques such as voxel-based and surface-based analysis may enhance the
Neuroimaging Evaluation in Neocortical Epilepsies 11

visibility of the lesion, helping in the identificationof MRI-negative FCDs. Surface-based analysis(including FreeSurfer) allows cortical thicknessmeasurement, assisting in the detection of FCDs,and better evaluates the gyration anomalies, facil-itating the exact localization of the dysplasia(Figs. 7, 8, 9).
Ancillary Techniques
Interictal 18F-FDG PET usually shows hypo-metabolism in the dysplastic cortex (Figs. 6, 9)and may be helpful in MRI-negative cases, espe-cially if co-registered with 3D T1WI.
Treatment
Surgical option should be considered early afterthe diagnosis, especially in children, to avoid life-long treatment with antiepileptic drugs, sideeffects like cognitive impairment, and poor sei-zures control over time. Location of the dysplasiagreatly influences the surgical feasibility andapproach, and lesions located nearby eloquentcortex required a complex pre-surgical evaluation
that includes fMRI and DTI tractography (seeSect. IX Epilepsy, Chap. 7 ▶ “Pre- and post-surgical evaluation of epilepsy”).
Surgical Outcome
The surgical outcome is good if the EZ iscompletely resected. Patients are seizure-free(Engel class I) in 91% of FCD Type IIb versus68% of FCD Type IIa (Colombo et al. 2012; Tassiet al. 2012).
Polymicrogyria (PMG)
General Definition of Entity
Polymicrogyria is a heterogeneous cortical mal-formation characterized by an excessive numberof small gyri, fused together. It is due to abnor-malities in early (impaired proliferation andmigration of neuroblasts) and late neuronal migra-tion and post-migration development.
Fig. 5 FCD Type IIb deep in the sulcus. Axial TSE T2WI(a), sagittal FLAIRT2WI (b), coronal FLAIRT2WI (c, d),coronal TSE T2WI (e, f), coronal IR T1WI (g, h). Corticalthickening is seen along and deep in the left postcentralsulcus, with gray/white matter junction variably blurred or
sharp (white arrows in b, c, e). “The transmantle sign” iswell detected on sagittal and coronal FLAIRT2WI (b, c, d)and coronal T2WI (e, f). Abnormal gyration of the dys-plastic cortex is also appreciated
12 N. Colombo et al.

Epidemiology
PMG accounts for 1% of the histopathologicaldiagnosis in patients eligible for epilepsy surgery.On MRI series, however, there is evidence thatPMG is more frequently seen in epileptic patientsbut without histologic confirmation owing to lackof surgery.
Clinical Scenario
PMG is associated with a variety of clinical symp-toms including epilepsy (78–87% of cases), intel-lectual disability, motor dysfunction, and speechdisturbance depending upon the portion(s) of
brain involved. Seizure onset ranges between4� 6 years of age (Blümcke et al. 2017). Peculiarelectro-clinical syndromes are described in asso-ciation with specific regional PMG, like bilateralperisylvian, bilateral frontal and frontal-parietal,and bilateral parasagittal parietal-occipital. PMGcan be found in metabolic disorders or in severalsyndromes.
EEG Patterns
Scalp EEG is not pathognomonic. Focal patterns arerecognizable even in hemispheric malformations. Itis frequently associated with ESES (electrical epi-leptic status during sleep). SEEG recordings show
Fig. 6 FCD Type IIb deep in the sulcus. Axial, sagittal,coronal FLAIR T2WI (a, b, c), coronal TSE T2WI (d),coronal IR T1WI (e), 18-FDG PET-MRI co-registrationimages (f, g). An abnormally deep-running sulcus is pre-sent in the left frontal region with focal thickening of the
cortex at the bottom of the sulcus and blurring of thecortico-medullary border representing the dysplastic tissue(arrows in a–e). No funnel-shaped transmantle sign is seen.18F-FDG PET scan shows congruent focal hypo-metabolism deep in the sulcus (f, g)
Neuroimaging Evaluation in Neocortical Epilepsies 13

that PMG is variably intrinsically epileptogenic,able to generate high-frequency interictal spikingand ictal discharges. Not the entire malformationis always involved in the origin of seizures.
Pathological Features
Gross neuropathology shows many small gyri,packed tightly together, separated by swallowsulci, mimicking thickened cortex. Both corticalsurface and GM/WM junction have irregular andlumpy appearance. At microscopy, the cortex isabnormally thin, unlayered or four-layered; thesmall gyri are fused at the first molecular layerand pia bridges across multiple gyri.
Etiology - Pathophysiology
The origin of PMG is heterogeneous includingcongenital infections (particularly cytomegalovi-rus), localized or diffuse intrauterine ischemicinjury, or various genetic mutations. Some muta-tions that affect the role of microtubules are possi-ble contributors, but not cause, of PMG (TUBB2B,TUBA1A and TUBB3 mutations). There is evi-dence that disturbance in the formation of theleptomeninges or loss of their normal signalingfunctions highly contributes to PMG throughmechanical constraints on the developing cortex.
Fig. 7 FCD Type IIb on crown of gyrus. Coronal, sagittal,axial FLAIR T2WI (a, b, c), FreeSurfer cortical thicknessmapping, and pial surface-based reconstruction (d, e).Focal thickening of the cortex is seen involving thecrown of the right precentral gyrus with hyperintensity ofsubcortical white matter and blurred gray/white matter
junction (a, b, c). The transmantle sign is barely seen oncoronal image (white arrow in a). FreeSurfer cortical thick-ness mapping (d, e) confirms the focal thickening of thedysplastic cortex (maximum thickness in yellow based onthe bar of significance) that is projected over the pialsurface-based reconstruction (white dashed arrows in d, e)
14 N. Colombo et al.

MRI Features and Structured Reporting
The cortex made by many/small gyri simulatescortical thickening on 2D images resembling“pachygyria.” 3D T1WI or 3 mm IR sequencebetter shows the microgyric structure of the cortexhaving irregular surfaces on both the pial andGM/WM junction sides, with lumpy-bumpyappearance (Figs. 10, 11). The dysmorphic cortexcan follow the skull convexity or be variablyinfolded or developing along schizencephaliccleft (Fig. 11 upper row). In fully myelinatedpatients, no T2 signal alteration of the white mat-ter is present, not even any GM/WM “blurring,”contrary to FCDs. The subarachnoid spaces
overlying area of polymicrogyria are enlarged,containing amplified dysplastic leptomeningealveins (Fig. 11). Hemispheric hypoplasia can beseen in case of hemispheric PMG (Fig. 11 lowerrow). PMG can be associated to other brain abnor-malities including corpus callosum dysgenesis,cerebellar hypoplasia, schizencephaly (Fig. 11upper row), nodular heterotopia, and dysmorphicbasal ganglia in tubulinopathies. The extensioncan be focal, multifocal, or diffuse with unilateralor bilateral symmetric or asymmetric distribution.The most common location is bilateral perisylvian(Fig. 10), bilateral frontal and frontal-parietal, andbilateral parasagittal parietal-occipital regions.
Fig. 8 FCD Type IIa. 4-year-old boy. Axial TSE T2WI(a), axial and sagittal FLAIR T2WI (b, c), two contiguousaxial images from 3D T1W sequence (d, e), FreeSurfersurface-based reconstruction of pial surface (f). Extensiveparietal-frontal dysplasia is seen on the left characterizedby gyration anomalies involving the mesial and dorsolat-eral cortex that appears thickened, with blurred interfacewith the underlying white matter, which exhibits mildincreased signal on T2WI by comparison with the contra-lateral side. The dysplasia is better visualized on axial
images due to signal alterations (a, b) and abnormal gyra-tion (d, e), and it is barely visible on sagittal view (whitearrow in c). FreeSurfer pial surface reconstruction withlabelling of the precentral (violet) and postcentral gyri(red) shows abnormal gyration mainly in the parietallobe: the posterior branch of the Sylvian fissure continuesupward in an unusual sulcus running vertically (whitearrows in f). The intraparietal sulcus and the supramarginalgyrus are not recognizable
Neuroimaging Evaluation in Neocortical Epilepsies 15

Ancillary Techniques
18F-FDG PET usually shows normal metabolismor mild hypermetabolism in PMG compared tonormal cortex (Figs. 10, 11 upper row). Hyper-metabolism is believed to be due to the greateramount of gray matter inside the PMG cortex thatis made up by an excessive number of gyri.
Surgical Treatment and Outcome
The best surgical strategy is still under discussion.Good surgical outcome is reached in a subset of
patients in whom invasive recording is able todefine the EZ that should be removed.
Heterotopias (HTP)
General Definition of Entity
Heterotopias are cortical malformations made byclusters of disorganized normal neurons in abnor-mal location, due to arrested/disrupted migrationfrom the periventricular germinal zone (GZ).Three major types are recognized: periventricularnodular (PNH), subcortical nodular (SNHTP) or
Fig. 9 FCD Type IIb deep in the central sulcus. AxialFLAIR T2WI (a), axial 3D FFE T1WI (b), coronal andsagittal FLAIR T2WI (c, d) FreeSurfer pial surface recon-struction (e, f), 18F-FDG PET-MRI co-registration images(g, h, i). On axial images, even on 3D T1W sequence, it isquite difficult to exactly localize the dysplasia (whitearrows in a, b) with respect to the central sulcus. TheFreeSurfer surface reconstruction with parcellation and
labelling of the precentral (light blue) and postcentral(light red) gyrus identifies the central sulcus (black dashedarrow in e). In (f) the lesion obtained by manual counteringof the lesion’s borders visible at axial FLAIR sequence isrepresented in red, and it is exactly localized deep in thecentral sulcus. 18F-FDG PET scan shows focal hypo-metabolism in the dysplastic cortex (line crossing in g–i)
16 N. Colombo et al.

laminar (subcortical band-HTP= SBH or “doublecortex”), and leptomeningeal HTP (not detectableby imaging).
Epidemiology
Heterotopias represent 15–20% of all MCDs indifferent imaging and surgical series. Theyaccount for <1% of the histopathological diagno-sis in patients submitted to epilepsy surgery(Blümcke et al. 2017).
Clinical Scenario
PNH in pediatric patients is often associated toother brain malformations, mental retardation,and a severe course of epilepsy. In adults PNHcauses focal seizures starting usually in the seconddecade. SBH can be associated to refractorymultifocal or generalized onset seizures, althoughthey could be clinically silent as well in mutationcarriers.
EEG Patterns
Interictal and ictal scalp EEG patterns are related tothe location of PNH. SEEG monitoring showsinterconnections between PNH-SBH and the over-lying cortex: seizures are recorded in the PNH,SBH, and/or in the overlying cortex, propagatingfrom one structure to the other in variable way.
Pathological Features
Focal masses or ribbons of gray matter made bynormal but disorganized neurons.
Etiology - Pathophysiology
Classic bilateral PNH is often genetic, found infemales, with filamin A (FLNA) gene commonlyinvolved on Xq28. SBH (mild form of type Ilissencephaly) with posterior expression is mainly
due to deletion of LIS1 on 17p13.3; anteriorexpression is mainly due to deletion of DCX(double cortin) on Xq22.3-q23. Acquired formsare rare, due to toxin/infections disturbing migra-tion and cortical positioning of neurons.
MRI Features and Structured Reporting
All types of heterotopias are better visualized on3D T1W or 3 mm IRW sequences, exhibitingsignal intensity similar to normal cortex on allsequences.
PNH are tiny or massive nodules indenting theventricle. Usually their signal intensity matchesthe one of normal cortex, but in few cases, it canbe slightly hyperintense on FLAIR and T2WI.Nodules can be connected with the overlying cor-tex by radial band with signal hyperintensity onT2WI (Fig. 12); huge PNH can merge with theoverlying cortex that is often thinned and multi-gyral appearing (Fig. 13 upper row). In huge andcomplex forms, the ipsilateral hemisphere can besmall and the ipsilateral ventricle large. PNH canbe unilateral or bilateral, single or multiple, andcontiguous, lining the ventricles especially neartrigons and temporal horns.
SNHTP are isles of gray matter inside thesubcortical white matter (Fig. 13 lower row) andcan be an incidental finding.
SBH is shown by complete or incomplete rib-bon of subcortical gray matter, separated by a thinlayer of normal-appearing white matter from theprimary cortex. Posterior-anterior gradient ofdevelopment is the most frequent (Fig. 14).
Ancillary Techniques
At 18F-FDG PET, PNH can have no glucoseuptake or reduced glucose uptake compared tonormal cortex (Fig. 12). Glucose uptake in SBHis reported similar to or greater than in normalcortex.
Neuroimaging Evaluation in Neocortical Epilepsies 17

Surgical Treatment
PNH have good surgical outcome if SEEG delin-eates a well-defined EZ within the nodule and/orthe overlying cortex that can be removed. Stereo-tactic thermal/laser ablation can be proposed fortreating PNH and SNHTP. SBH is no surgicallytreatable.
Hemimegalencephaly (HME) orUnilateral Megalencephaly
General Definition of Entity
Hemimegalencephaly is a cortical malformationdue to abnormal proliferation or decreased apo-ptosis of neurons and glial cells.
Epidemiology
It is rare, accounting for 0.2% of cases of childhoodepilepsy and for 0,6% of surgical cases (Blümckeet al. 2017). No gender predilection is known.
Clinical Scenario
Severe intractable epilepsy is present in more than90% of patients, usually starting in the first year oflife. Seizures can be partial or characterized bytonic manifestations or infantile spasm with theEEG features of Ohtahara or West syndromes.Macrocephaly at birth with no sign of raised intra-cranial pressure, developmental delay, contralat-eral hemiparesis, and hemianopia is frequent.
Fig. 10 Bilateral perisylvian polymicrogyria. Coronal IRT1WI (a), coronal TSE T2WI (b), coronal FLAIR T2WI(c), multiplanar reconstructions (MPR) from 3D FFET1WI (d, e, f), 18F-FDG PET scan (g, h, i). Gyrationanomaly and irregularity of the cortex that surrounds boththe enlarged Sylvian fissures are seen. The cortex is made
by multiple small gyri merging together, better identifiedon 3D images (d–f), and shows lumpy-bumpy appearanceat the GM/WM interface (a, d–f). 18F-FDG PET scanshows hypermetabolism within the polymicrogyric cortex(g–i)
18 N. Colombo et al.

EEG Patterns
Scalp EEG is characterized by suppression-burstand/or hemi-hypsarrhythmia over the malformedhemisphere that progressively spreads to the con-tralateral one. Bilateral EEG abnormalities arecommon.
Pathology
Gross pathology shows partial or completehamartomatous overgrowth of one hemisphere.Cortex is affected by polymicrogyria, pachygyria,
lissencephaly, and agyria intermingled withappearing normal cortex. At microscopy, variabledegree of cortical dyslamination is present, withgiant neurons, balloon cells, and hypertrophic/atypical cells also scattered throughout the whitematter. Dystrophic calcifications can be foundwithin the cortex and white matter. Cystic degen-eration, impaired myelination, and gliosis are alsopresent in the white matter.
Fig. 11 Polymicrogyria edging “closed lip”schizencephaly (upper row). Axial and coronal reconstruc-tions from 3D FFE T1WI (a, b). 18F-FDG PETscan (c, d).The MRI shows irregular cortex with polymicrogyricaspect lining a CSF-filled cleft, with kissing lips, extendingtoward the right lateral ventricle. Pointing of the wall of thelateral ventricle is a key feature for schizencephaly.18F-FDG PET scan shows hypermetabolism within thepolymicrogyric cortex (c, d). Hemispheric polymicrogyria
on the right (lower row). Axial TSE T2WI (e), multiplanarreconstructions (MPR) from 3D FFE T1WI (f, g, h). PMGis characterized by irregularly bumpy cortical surface andlumpy GM/WM junction, involving the whole right hemi-sphere, with no signal changes of the WM. Hypoplasia ofthe right hemisphere with diffuse enlargement of the sub-arachnoid spaces and of the ipsilateral ventricle is alsonoticed
Neuroimaging Evaluation in Neocortical Epilepsies 19

Etiology
The isolated form is cryptogenic. HME associatedto body hemi-hypertrophy, of different degree, isfound in syndromes like epidermal nevus,Klippel-Trenaunay, McCune-Albright, Proteus,unilateral hypomelanosis of Ito, neurofibromato-sis type 1, and tuberous sclerosis.
MRI Features and Structured Reporting
• Enlargement of a portion or entire cerebralhemisphere is the major finding.
• The ventricle in the affected hemisphere isdilated, frequently showing abnormal shapeof the frontal horn (straight, pointed). In case
of occipital megalencephaly, the posterior falxis displaced contralateral (Fig. 15).
• The cortex shows areas of increased thickness,with variable abnormal gyral patterns, resem-bling polymicrogyria, agyria, pachygyria, andlissencephaly. The GM/WM junction is fre-quently blurred.
• White matter abnormalities are constant,related to gliosis and myelination impairmentchanging over time. In the first year of life,“accelerated” myelination causes WM hyper-intensity on TWI and hypointensity on T2WI.In older children and adults, the WM fre-quently contains alternating bands of hypo-and hyperintense signal on different weightedsequences, reminiscent of band heterotopia(Fig. 15) associated with nodular heterotopiasof any kind.
Fig. 12 Bilateral periventricular nodular heterotopia.Axial IR T1WI (a), axial FLAIR T2WI (b), coronal IRT1WI (c), coronal TSE T2WI (d), 18F-FDG PET-MRIco-registration (e–g). Multinodular periventricular hetero-topia is shown along the temporal horns. Heterotopic
nodules have the same signal intensity of gray matter inall pulse sequences and are connected with the overlyingcortex by radial band (arrows in c, d). 18F-FDG PETimages show intermediate uptake in the heterotopic nod-ules, less than normal cortex (e–g)
20 N. Colombo et al.

• Dystrophic calcifications are well detected onGRE T2*WI or SWI.
• Developmental venous anomalies inside thedysplastic cortex can be visualized on SWIand Gad-enhanced T1WI.
HME is hemispheric or lobar, mainly affectingthe occipital lobe. The contralateral hemisphere issmaller than hemispheres of age-matched normalsubjects.
DTI tractography can assist in the demonstra-tion of intra- and interhemispheric abnormal fibertract connection and supernumerary and hypertro-phic fiber tracts (Fig. 15).
Ancillary Techniques
18F-FDG PET shows hypometabolism in theaffected hemisphere in 50% of cases. IctalSPECT shows variable decreased or increasedglucose uptake inside the malformation.
Surgical Treatment
Hemispheric surgery (hemispherectomy, func-tional hemispherotomy, or disconnection) is thetreatment of choice in isolated HME. Seizurescontrol is reached in less than 60% of cases. Theabnormal contralateral hemisphere may explainthe poor surgical and cognitive outcomes.
Fig. 13 Unilateral periventricular nodular heterotopia(upper row). Axial and coronal IR T1WI (a–c). Nodulesof heterotopic gray matter are seen along the ventriculartrigone and temporal horn on the right, with transmantleextension merging with the overlying cortex that showsdysplastic multigyral appearance and gyration anomalies.
Subcortical nodular heterotopia (lower row). A 5-year-oldboy with right frontal epilepsy starting at 2 years of age.Axial TSE T2WI (d), coronal IRT1WI (e), coronal FLAIRT2WI (f). Single heterotopic nodule is present in rightfrontal subcortical white matter, isointense to gray matterin all sequences. The overlying cortex looks like normal
Neuroimaging Evaluation in Neocortical Epilepsies 21

Acquired Epileptogenic Lesions
There are some pathological conditions such ascerebrovascular disease, brain trauma, or infec-tion that presumably produce epileptogenesis.The term acquired epileptogenic lesions wasrevised in 2013 by the working group of theILAE and defined as the development and exten-sion of tissue capable of generating spontaneous
seizures, resulting in epileptic disorder with pos-sible progression after the disorder is established.The epileptogenic process is classified in threesteps: inciting event, silent period, and onset ofspontaneous recurrent seizures. This type of inju-ries usually involves the cortex. Although in somecases the patient has seizures in the acute phase ofbrain injury, in most cases the epilepsy appearsafter an interval of months or years.
Fig. 14 Bilateral double cortex (upper row) in a 20-year-old female with seizures originating in the left temporo-occipital region. Axial and coronal IR T1WI (a, b). Homo-geneous band of gray matter intensity separated from theprimary cortex by a layer of normal-appearing white matteris seen. The band is thicker in the posterior and thinner inthe anterior. The overlying cortex has normal thickness but
slightly shallow sulci. Incomplete band heterotopia (lowerrow) in a 30-year-old male with left frontal epilepsy. Axialand coronal IR T1WI (c, d). In the left frontal lobe, a thinband of heterotopic neurons is present, separated from theoverlying cortex by normal white matter; the overlyingcortex appears normal
22 N. Colombo et al.

In this section, neocortical epilepsy caused bystroke and brain trauma will be describedseparately.
Post-Stroke Epilepsy (PSE)
General Definition of Entity
Post-stroke epilepsy (PSE) is defined as theappearance of epilepsy after a cerebrovascularevent, especially ischemic or hemorrhagic arterialor venous stroke. One of the most common causesof epilepsy in middle age patients is cerebralinfarction. On the other end of the age spectrum,neonates are also susceptible to presenting
cerebrovascular events (perinatal stroke) and sub-sequent epilepsy.
In the epilepsy units, it is not infrequent toobserve young patients with a history of cerebralinfarction during the perinatal stage, who, after aperiod of latency, present with epilepsy that inmany cases is difficult to manage with anti-epileptic drugs.
It is important to distinguish between post-stroke seizures (PSS) and post-stroke epilepsy(PSE). The ILAE defines PSS as single or multi-ple convulsive episodes that are thought to berelated to reversible or irreversible cerebral ische-mic damage, regardless of time of onset followingthe stroke. If seizures occur within the first2 weeks, they are denominated “post-stroke
Fig. 15 Right hemimegalencephaly in a 3-year-old boy.Axial IR T1WI at two different levels (a, b), axial TSET2WI (c), sagittal FLAIR T2WI (d), coronal IR T1WI (e).The right hemisphere is enlarged, made of thickened cortexwith fewer, broader gyri and shallow sulci, predominant inthe temporal-parietal and occipital region. Abnormal alter-nating bands of hyper/hypointensity are evident in the
temporal-parietal-occipital white matter, due to gliosisand band of subcortical heterotopia (black arrows in a).The anterior commissure fibers and the splenium of corpuscallosum are hypertrophic on the right (white arrow ina–b). Contralateral displacement of the posterior falx(a–c, e) is also noticed
Neuroimaging Evaluation in Neocortical Epilepsies 23

early-onset seizures” having a high peak duringthe first 24 h. If they appear after the first 2 weeks,then they are defined as “post-stroke late-onsetseizures,” having a peak within 6–12 monthsand a greater correlation with a higher seizurerecurrence.
The presence of early- or late-onset post-strokeseizures facilitates the development of PSE,which is defined as “recurrent seizures followingstroke with confirmed diagnosis of epilepsy.” Itshould be noted that both in childhood and adultage, there are risk factors associated with cerebralinfarction that increase the possibility of sufferingfrom PSE. They include the severity of the ische-mic stroke, the cortical location, the extent of theinfarction, the patient’s age, the presence of sei-zures during the acute onset of stroke, and thepresence of hemorrhage.
Epidemiology/Demographic
The long-term cumulative risk of PSE variesbetween 2% and 15% in adult patients, althoughthere are factors that increase the risk, especiallyhemorrhagic cortical infarcts and stroke involvingall the anterior and middle cerebral arteries’territories.
Estimated rates of PSE after perinatal strokevary widely, ranging from 17% to 56%,depending on selection criteria and the durationof follow-up. A pediatric population study dem-onstrates that the cumulative risk of active epi-lepsy after stroke is 13% at 5 years and 30% at10 years, although this varies depending on theextension and the location of the vascular territoryaffected (Benbir et al. 2006).
Pathological Features
After stroke, different pathological alterations caninvolve the infarcted brain tissue includingencephalomalacia that is softening of the braintissue with more or less hemorrhagic content,gliosis that refers to the development of astrocytesappearing as a scar on imaging, and porencephalic
cavities filled with cerebrospinal fluid (CSF),mainly due to brain insults during early gestation.
Pathophysiology
During the acute stage of an ischemic stroke, thereare several factors that can explain the onset ofseizures. The rupture of cell membranes and theentry of Ca2+ and Na+ ions into the neurons willalter the cellular polarization, and other changesrelated to cellular hypoxia will occur in addition.
In the post-stroke period, the presence of scarsor hemosiderin deposits from hemorrhage withinthe injured brain tissue may facilitate theepileptogenesis and may explain the appearanceof PSS and the development of PSE.
If the ischemic event occurred during the peri-natal period, cortical malformations can progres-sively develop in the cortex nearby the infarctedtissue, characterized by cortical dyslaminationwithout cytoarchitectural anomalies (FCD TypeIII d), possibly contributing to epileptogenesis(Blümcke et al. 2011).
Clinical Scenario
In adults the type of fits most frequently observedare partial simple or complex seizures, commonlyof motor type, which can secondarily generalizeand even present as status epilepticus.
In neonates, stroke usually debuts clinicallywith focal seizures in an apparently healthybaby. Subsequently, the child can become asymp-tomatic or have different degrees of hemiparesis,depending on the location of the stroke. After aperiod of latency, these patients may suffer fromlate-onset seizures, which can be isolated or mayappear repetitively and stereotyped, thereforeclassified as PSE.
The most common type of crisis in thesepatients is neocortical focal seizures with motorfits since the motor cortex is frequently damaged(anterior and middle cerebral artery territory). Sei-zures usually spread rapidly and may becomegeneralized.
24 N. Colombo et al.

Children with PSE are also at increased risk ofassociated cognitive delay.
EEG Patterns
On scalp EEG, the most frequent finding is slowactivity in the hemispheric side of the infarct.Several EEG patterns have been described: dif-fuse slowing, intermittent rhythmic delta activity,or periodic lateralized epileptic discharges.
Neuroimaging Features and StructuredReporting
It is important to emphasize that in patients withPTE unresponsive to medical treatment, a specificMRI protocol for epilepsy is mandatory. CT scanis usually utilized in the acute phase of stroke butalone is not sufficient to manage these patients.
CT and MRI scans easily detect porencephaliccavities and encephalomalacia in the infarctedtissue.
They will show a cystic or multicystic lesionwith density or signal equal to CSF. Cysts can belarge, encompassing much of the anterior vascularterritory. Frequently they affect the frontal andinsular region, and the left hemisphere is themost commonly involved (Fig. 16).
Occasionally, in neonates that have suffered amore severe and prolonged hypoxia, lesions canbe observed in watershed territories, especiallyinvolving the parietal-occipital or frontal-parasagittal regions, bilaterally. In the acutephase, watershed lesions are seen only forrestricted diffusion on DWI. As the injuryevolves, cortical thinning and reduction of theunderlying WM are seen. Ex vacuo dilatation ofthe adjacent lateral ventricle may be seen.
If the ischemic event occurred in older childrenand adults, the encephalomalacic cavities aremore frequently surrounded or intermingled withgliosis, with hyperintense signal on T2WI andFLAIR sequences.
FCD Type IIId can be hardly recognized anddifferentiated from the ischemic tissue, evenon MRI.
SWI sequences are particularly helpful todetect hemosiderin deposits that are known tocontribute to epileptogenesis.
If a patient has several lesions, it is important toperform a functional neuroimaging study such asSPECT or SISCOM (subtracted ictal SPECTco-registered to MRI) that will help to identifywhich lesion is the epileptogenic one or to delin-eate the seizure-onset area adjacent to theencephalomalacic cavity (Fig. 16). 18F-FDGPET provides information of the hypoperfusedzone associated with the infarction and may helpto plan the surgical resection.
Treatment
Middle-age patients with PSE usually have a goodresponse to antiepileptic drugs, and single therapycan control the seizures in about 88% of cases.
Surgical options should be considered espe-cially in children, to avoid side effects like cogni-tive impairment and poor seizure control overtime. In many occasions, depending on the exten-sion of the infarct, disconnective surgery such asfunctional hemispherectomy or hemispherotomycan be the only resort. When the residual infarct issmall and well localized, the surgical procedurewill be partial lobar resection, always respectingthe eloquent functioning areas.
Post–Traumatic Epilepsy (PTE)
General Definition of Entity
Post-traumatic epilepsy (PTE) refers to recurrentand unprovoked post-traumatic seizures (PTS). Iffits occur in the first week after trauma, they aredefined as early-onset PTS. They are thought to beprovoked by the traumatic brain injury itself.
When seizures appear after 1 week from thetrauma, they are considered late-onset PTS.
The presence of early-onset PTS does not nec-essary indicate that the patient will develop PTE;however their presence increases the risk of late-onset PTS and PTE.
Neuroimaging Evaluation in Neocortical Epilepsies 25

Similar to post-stroke epilepsy, there is a latentperiod between the brain trauma and the late-onsetPTS and PTE.
There are several independent risk factors thatfavor seizures and epilepsy after traumatic braininjury (TBI) mostly related to the severity oftrauma, such as acute intracerebral hematoma,acute subdural hematoma, brain contusion, pene-trating brain injury, depressed skull fractures, andcoma during the first 24 h. Also repetitive trau-matic injuries support PTE. The severity of thetrauma and the early-onset PTS are related to drugresistance of epilepsy.
Epidemiology/Demographic
TBI is the most frequent cause of symptomaticepilepsy in people from 15 to 24 years of age.Epilepsy develops in 10–25% of patients withmoderate to severe injuries. The cumulative inci-dence of PTE is about 9% in the first 3 years afterTBI. PTE debuts in 50% of patients during thefirst year and in 80% of patients during the secondyear after TBI (Pitkänen and Immonen 2014).
Pathophysiology
Contusions and intracranial hematomas are focalinsults that will produce scars in the cortex or
subcortical regions with the consequent cascadeof inflammation, gliosis, and finally of abnormalneurogenesis that is believed to generate aberrantnetworks. Iron deposition from extravasatedblood and accumulation of glutamate are postu-lated as causes of excitotoxicity. However, theexact pathophysiological epileptogenic processthat occurs after brain trauma is still not clearlyelucidated.
Clinical Scenario
Patients can present fits during the first week afterbrain trauma with different semiology dependingon the location of the brain injury. Seizures can bepartial, focal secondary generalized, orgeneralized.
Temporal lobe lesions are the most commonlyinvolved in PTE, and typical temporal lobe sei-zures are common. Seizures are characterized byan aura that can be autonomic, psychic, or witholfactory and gustatory hallucination. Alterationof consciousness will follow the aura and in fewpatients will develop to secondary generalization.If the frontal lobe is involved, secondary general-ization is common.
Fig. 16 A 16-year-old boy with epilepsy and righthemiparesis following perinatal vascular injury. A largemulticystic encephalomalacia that involves left middlecerebral artery territory is seen. There is hyperintensity onT2WI in the white matter due to gliosis, Wallerian
degeneration of the adjacent cortico-spinal tract, and atro-phy of the cerebral peduncle. The left cranial vault isthickened. SISCOM image shows the ictal hyperperfusionarea indicating the seizure-onset location adjacent to thecavity (a, b, axial T2WI; c, coronal FLAIR; d, SISCOM)
26 N. Colombo et al.

EEG Pattern
Several scalp EEG patterns have been described:diffuse slow activity, intermittent rhythmic deltaactivity, or periodic lateralized temporal or frontalepileptic discharges.
Neuroimaging Features and StructuredReporting
After early-onset PTS, a neuroimaging study ismandatory. CT scan is utilized to detect intracere-bral hemorrhages, contusions, and extra-axialhematomas, most frequently involving the tempo-ral and frontal lobes. MRI is not usuallyperformed for study early-onset PTS, but corticalpossibly epileptogenic lesions (contusions andhemorrhages) can be easily detected.
In case of late-onset PTS and PTE, MRI is thetechnique of choice. It is important to use a dedicatedepilepsy protocol adding SWI sequences to detectsmall cortical or subpial old blood products. High-resolution structural sequences such 3D MP-RAGEor 3D FLAIR could help in detecting small corticallesions related to brain injuries (Fig. 17).
It is common to detect several post-traumaticlesions within the brain parenchyma, and it can bedifficult to establish which of them is the epilep-togenic one. The ictal SPECT or SISCOM,together with the semiology of seizures and the
EEG patterns, will provide information aboutwhich lesions are generating seizures.
Treatment
There is no clinical evidence that the use of anti-epileptic drugs for prophylaxis, after moderate orsevere TBI, could prevent PTE. Of note is that inpatients with PTE, the presence of drug resistanceis common. In these cases, resective surgical treat-ment can be an option. However it must emphasizethe difficulty to treat these patients that frequentlyhave multiple lesions because of the difficulty tolocalize the epileptogenic one or for the presence ofmulti-epileptogenic lesions. Therefore invasiverecordings are often required to precisely definethe EZ that should be resected. When resectivesurgery is precluded, palliative options mayinclude neuromodulatory approaches.
Clinical Cases and Sample Reports
Checklist for Reporting MRIin Neocortical Epilepsy
Relevant findings:
• Cortical signal changes (focal or diffuse)• White matter signal changes (subcortical or
deep/periventricular; focal or diffuse)
Fig. 17 Patient withhistory of brain trauma thatdeveloped PTE. The SWI(on the left) shows subpialand cortical hemosiderindeposition in the rightlateral central region (blackarrow). The T1WI (on theright) shows a focal corticalatrophy and a small olddepressed fracture of theright parietal bone (blackarrow)
Neuroimaging Evaluation in Neocortical Epilepsies 27

• Abnormal cortical thickness (increased ordecreased, focal, or diffuse)
• Blurring of the gray/white matter interface• Gyration anomalies (focal or diffuse)• Cortical-subcortical atrophy (focal, diffuse, or
hemispheric)• Hypertrophy of a focal brain area, of a lobe, or
of an entire cerebral hemisphere• Presence of calcifications• Presence of hemorrhage• Number of lesions: Single or multiple• Topography of lesion: Unilobar/multilobar/
hemispheric; indicate the lobe/lobes involved• Location of lesion: Cortical, cortical-
juxtacortical, subcortical, periventricular, inthe crown of the gyrus, and deep in the sulcus
• Establish if the structural lesion is congruentwith the epileptogenic zone defined on the baseof the electro-clinical data
• Establish if there is any incidental or unex-pected finding not congruent with the electro-clinical data
• Establish if the MRI examination isunrevealing
Red flag:
Transient seizure-induced cytotoxic edema in thepostictal phase can mimic a structural lesionowing to increased signal on T2W/FLAIRsequences. Caveat: Cytotoxic edema is identi-fied by restricted diffusion (low ADC)
Patients <3 yrs. old with uncompletedmyelinization may show terminal zones ofsubcortical myelination (in frontal and tempo-ral lobe) that can mimic a structural lesion
The presence of mass effect, perilesional edema,and contrast enhancement is against the diag-nosis of MCD
Sample Report 1
Patient History
A 17-year-old man with drug-resistant partial epi-lepsy since 6 years of age. Neurological examina-tion is normal.
Semiology of seizures: hypertonic posture withflexion in the right elbow, head version, and devi-ation of the mouth to the right.
Electro-clinical findings derived from video-EEG: ictal theta waves in the left frontal-centralregion.
Clinical Suspect
Epilepsy symptomatic of a structural lesion in theleft frontal-mesial region, suspected as the epilep-togenic zone (EZ).
Purpose of MR Study
To detect and to characterize the suspected struc-tural lesion, whose identification can influence theprognosis, the pre-surgical planning, and the sur-gical outcome.
Imaging Technique
MRI: performed with 1.5 Tesla scan, covering thewhole brain. Sequences were acquired in threeplanes including 5 mm axial TSE T2W; 3 mmcoronal TSE T2W, 3 mm coronal TSE IR T1W,and 3 mm TSE FLAIR T2WI in three orthogonalplanes; 3D volumetric TSE FLAIR T2WI withisotropic 1 mm voxel, 5 mm axial DWI, 5 mmGRE T2*WI, and SWI, 3D GRE T1WI (1 mmcontiguous slices). No gadolinium injection.
Full Findings
None of the following MRI signs are seen partic-ularly in the suspected EZ (Fig. 18a, b, c):
• Focal signal alteration of the cortex and sub-cortical white matter
• Abnormal cortical thickness (increased ordecreased, focal or diffuse)
• Blurring of the gray/white matter interface• Gyration anomalies (focal or diffuse)• Cortical-subcortical atrophy (focal, diffuse, or
hemispheric)
28 N. Colombo et al.

• Focal, lobar, or hemispheric hypertrophy of thebrain
• Calcifications• Hemorrhage
No incidental or unexpected findings are visu-alized all throughout the brain.
Ancillary Technique
18F-FDG PET obtained by PET-CT tomographyshows focal reduced uptake of the tracer in the leftfrontal-mesial region (arrow in Fig. 18d).
Comment
The patient is candidate for surgery. Owing tounrevealing MRI results and the uncertainty to
rely on the PET scan, for the precise delineationof the EZ that should be removed, invasive inves-tigation based on stereo-electroencephalography(SEEG) was performed. The EZ was localized inthe left parasagittal frontal area that was surgicallyremoved (Fig.18e, f, g). Histological diagnosiswas FCD Type IIa. Surgical outcome: Engelclass 1a at 5 years clinical follow-up.
Sample Report 2
Patient History
A 13-year-old girl with drug-resistant focal epi-lepsy since the age of 8 years. Neurological exam-ination is normal. No cutaneous manifestationsare present.
Semiology of seizures: head flexion and devi-ation to the right, tonic extension of the left arm,
Fig. 18 MRI-negative patient with suspected EZ in the left frontal-mesial region. TSE FLAIR T2W images in the threeorthogonal planes at investigation (a, b, c) and post-surgery (e, f, g). 18F-FDG PET (d)
Neuroimaging Evaluation in Neocortical Epilepsies 29

and flexion and stiffness of the right arm accom-panied by legs extension.
Electro-clinical findings derived from video-EEG: slow waves and spikes over the rightfrontal-central and frontal-parietal region duringboth weak and sleep conditions.
Clinical Suspect
Epilepsy associated with a structural lesion in theright frontal-central region, which is suspected asthe epileptogenic zone (EZ).
Purpose of MR Study
To identify and define the type of the suspectedstructural lesion, whose detection is known toinfluence the prognosis, the pre-surgical planning,and surgical outcome.
Imaging Technique
MRI: the whole brain was investigated with 1.5Tesla scan. Sequences were acquired in threeplanes including 5 mm axial TSE T2W; 3 mmcoronal TSE T2W, 3 mm coronal TSE IR T1W,and 3 mm TSE FLAIR T2WI in three orthogonalplanes; 3D volumetric TSE FLAIR T2WI withisotropic 1 mm voxel, 5 mm axial DWI, 5 mmGRE T2*WI, and SWI, 3D GRE T1WI (1 mmcontiguous slices) pre- and post-gadoliniuminjection.
Contrast Agent and Dose
Single injection of macrocyclic gadolinium agent(0.1 mmol/kg bw).
Ancillary Technique
Single-voxel proton magnetic resonance spectros-copy (1HMRS): PRESS technique (TR/TE 2000/144 ms).
Full Findings
A single lesion is visualized in the frontal-parasagittal region on the right. The lesion ischaracterized by appearing thickened cortex(Fig.19a, d, e, f). Spots of signal alterations arepresent within the subcortical white matter, show-ing low signal on T1WI (white arrows in Fig.19c,f) and high signal on T2W and FLAIR images(arrows in Fig. 19a–b, d–e).
The gray matter/white matter junction appearsblurred on axial and sagittal images (arrows inFig.19a, d, e, f) and focally sharp on coronalTSE T2W and IR images (arrows in Fig. 19b, c).
A very thin and incomplete radial extension ofthe white matter signal changes toward the corti-cal mantle is recognizable only on coronal images,resembling the “transmantle sign” (dashed arrowsin Fig. 19b, c). The cortex shows increased T2signal less than white matter (Fig.19a, b, d, e). Nolesional contrast enhancement is present(Fig. 19f).
No intralesional calcifications and hemorrhageare present, neither perilesional edema.
The lesion doesn’t produce mass effect:although on axial images the regional sulci seemsmoothed, they are focally enlarged on coronalimages.
No any incidental or unexpected finding, notcongruent with the electro-clinical data, is seen.
MR spectroscopy shows relative increase inCho/Cr and a reduction in NAA/Cr within thelesion as compared to contralateral appearing nor-mal side (Fig. 20).
Interpretation
The lesion is in differential diagnosis betweenfocal cortical dysplasia (FCD) Type II,low-grade glioma, glioneuronal tumor, and witha single cortical tuber. Red flag: no mass effect,contrast enhancement, or intralesional calcifica-tions were found, excluding tumors and calcifiedcortical tuber. Despite the absence of a well-defined “trasmantle sign,” which is the hallmarkfor FCD Type II, the lesion fulfills all theremaining criteria for the diagnosis of FCD Type
30 N. Colombo et al.

II. Loss of NAA and increase in Cho on MRIspectroscopy are shared features of FCD Type IIand glioma; however the NAA decrease in FCD isless pronounced, like in the present case. On thewhole, all the MRI features are consistent with thediagnosis of FCD Type II.
Comment
Owing to the concordance between electro-clinical findings and the location of the lesion onconventional MRI, no invasive investigation, likestereo-electroencephalography (SEEG), is neededfor planning surgery. Patient underwent surgicalresection, and histological examination confirmedthe diagnosis of FCD Type IIb. Surgical outcome:Engel class 1a at 2 years clinical follow-up.
Sample Report 3
Patient History
A 9-year-old boy without personal or familialantecedents. Seizures started at 2 months of age,with spasms, completely cured with steroid treat-ment. At 8 years of age, multiple episodes ofsimple febrile convulsions and focal seizuresrecurred, characterized by fear sensation followedby loss of consciousness, clonic jerks to the upperlimbs, and enuresis. Multiple daily seizures werepresent despite the assumption of different anti-epileptic drugs.
Electro-clinical findings derived from video-EEG: interictal and ictal spikes and spike/waveson the left anterior frontal region.
Fig. 19 Axial and coronal TSE T2W images (a, b), TSE IR T1W image (c), axial and sagittal TSE FLAIR T2W images(d, e), axial 3D GRE T1W image post-gadolinium injection
Neuroimaging Evaluation in Neocortical Epilepsies 31

Fig. 20 Single-voxel 1H MRS: volumes of interest (VOI) are placed on the lesion (up) and for comparison on thenormal-appearing contralateral brain region (down)
32 N. Colombo et al.

Clinical Suspect
Epilepsy associated with a structural lesion in theleft frontal area, which is suspected as theepileptogenic zone (EZ).
Purpose of MR Study
To identify and to define the type of the suspectedstructural lesion, whose detection is known toinfluence the prognosis, the pre-surgical planning,and surgical outcome.
Imaging Technique
MRI: the whole brain was investigated with 1.5Tesla scan. Sequences were acquired in threeplanes including 5 mm axial TSE T2W; 3 mmcoronal TSE T2W, 3 mm coronal TSE IR T1W,
and 3 mm TSE FLAIR T2WI in three orthogonalplanes; 3D volumetric TSE FLAIR T2WI withisotropic 1 mm voxel, 5 mm axial DWI, 5 mmGRE T2*WI, and SWI, 3D GRE T1WI (1 mmcontiguous slices). No gadolinium injection.
Ancillary Technique
18F-FDG positron emission tomography (PET)obtained by PET-CT tomography.
Full Findings
In the left frontal lobe, abnormal gyration of thecortex is seen, along both mesial and lateral sur-faces (Fig. 21a–d). The cortex is mildly tick; thegray/white matter interface is not well definedmainly due to the mild signal alteration of thesubcortical white matter that exhibits increased
Fig. 21 Brain 1.5 T MRI scan: two coronal images from 3D T1W sequence (a, b), coronal FLAIR T2WI (c), coronalT2WI (d), axial FLAIR T2WI (e)
Neuroimaging Evaluation in Neocortical Epilepsies 33

signal on TSE T2W/FLAIR T2W images(Fig. 21c–e) and decreased signal on T1W images(Fig. 21a, b). No funnel-shaped “transmantlesign” is evident nor atrophy/hypoplasia of theleft frontal lobe.
18F-FDG PET scan shows hypometabolism inthe left anterior frontal region, with topographiccorrelations with the MRI findings (arrows inFig. 22).
Interpretation
MRI features are suggestive of wide cortical dys-plasia in differential diagnosis between focal cor-tical dysplasia (FCD) non-Type II andpolymicrogyria (PMG). Red flag: the absence ofthe “transmantle sign” is against the diagnosis ofFCD Type II. PMG can be suspected since on 3DT1WI the cortical-white matter interface seems tohave lumpy appearance but it is rule out owing tothe presence of signal alteration of the subcorticalwhite matter that is normally absent in PMG.
Fig. 22 18F-FDG PET
Fig. 23 FLAIR T2Wimages in the threeorthogonal planes post-surgery
34 N. Colombo et al.

Furthermore 18F-FDG PET usually shows iso-metabolism or mild hypermetabolism of PMGcompared to normal cortex, while FCDs are hypo-metabolic. Both MRI and PET findings are con-sistent with the diagnosis of FCD non-Type II.
Comment
The positive correlation between imaging andelectro-clinical data is sufficient for planning sur-gery without invasive investigation. The patientunderwent left frontal lobectomy (postoperativeMRI in Fig. 23), and the histological diagnosiswas FCD Type IIa. Surgical outcome: Engel class1a at 2 years clinical follow-up.
References
Barkovich AJ, Guerrini R, Kuzniecky RI, et al. Adevelopmental and genetic classifications formalformations of cortical development: update 2012.Brain. 2012;135:1348–69. https://doi.org/10.1093/brain/aws019.
Benbir G, Ince B, Bozluolcay M. The epidemiology ofpost-stroke epilepsy according to stroke subtypes.Acta Neurol Scand. 2006;114(1):8–12. https://doi.org/10.1111/j.1600-0404.2006.00642.x.
Blümcke I, Thom M, Aronica E, et al. The clinicopatho-logic spectrum of focal cortical dysplasias: a consensusclassification proposed by an ad hoc task force of theILAE diagnostic methods commission. Epilepsia.2011;52(1):158–74. https://doi.org/10.1111/j.1528-1167.2010.02777.x.
Blümcke I, Spreafico R, Haaker G, et al. Histopathologicfindings in brain tissue obtained during epilepsy sur-gery. N Engl J Med. 2017;377:1648–56. https://doi.org/10.1056/NEJMoa1703784.
Colombo N, Tassi L, Deleo F, et al. Focal corticaldysplasia type IIa and type IIb: MRI aspects in118 cases proven by histopathology. Neuroradiology.2012;54(10):1065–77. https://doi.org/10.1007/s00234-012-1049-1.
Holthausen H, Pieper T, Coras R, et al. Isolated focalcortical dysplasias type Ia (FCD type Ia) as cause ofsevere focal epilepsies in children. Neuropediatrics.2014;45(Suppl):51–5. https://doi.org/10.1055/s-0034-1390564.
Pitkänen A, Immonen R. Epilepsy related to traumaticbrain injury. Neurotherapeutics. 2014;11(2):286–96.https://doi.org/10.1007/s13311-014-0260-7.
Rossini L, Villani F, Granata T, et al. FCD type II andmTOR pathway: evidence for different mechanisms
involved in the pathogenesis of dysmorphicneurons. Epilepsy Res. 2017;129:146–56. https://doi.org/10.1016/j.eplepsyres.2016.12.002.
Tassi L, Garbelli R, Colombo N, et al. Type I focal corticaldysplasia: surgical outcome is related to histopathol-ogy. Epileptic Disord. 2010;12:181–91. https://doi.org/10.1684/epd.2010.0327.
Tassi L, Garbelli R, Colombo N, et al. Electroclinical, MRIand surgical outcomes in 100 epileptic patients withtype II FCD. Epileptic Disord. 2012;14(3):257–66.https://doi.org/10.1684/epd.2012.0525.
Taylor DC, Falconer MA, Bruton CJ, et al. Focal dysplasiaof the cerebral cortex in epilepsy. J Neurol NeurosurgPsychiatry. 1971;34:369–87.
Suggested Readings
Barkovich AJ, Dobyns WB, Guerrini R. Malformations ofcortical development and epilepsy. Cold Spring HarbPerspect Med. 2015;5(5):a022392. https://doi.org/10.1101/cshperspect.a022392.
Bernasconi A, Bernasconi N, Bernhardt BC, et al.Advances in MRI for “cryptogenic” epilepsies. NatRev Neurol. 2011;7:99–108. https://doi.org/10.1038/nrneurol.2010.199.
Cianfoni A, Caulo M, Cerase A, et al. Seizure-inducedbrain lesions: a wide spectrum of variablyreversible MRI abnormalities. Eur J Radiol.2013;82(11):1964–72. https://doi.org/10.1016/j.ejrad.2013.05.020.
Cossu M, Pelliccia V, Gozzo F, et al. Surgical treatment ofpolymicrogyria-related epilepsy. Epilepsia. 2016;57(12):2001–10. https://doi.org/10.1111/epi.13589.
Fischl B. FreeSurfer. NeuroImage. 2012;62(2):774–81.https://doi.org/10.1016/j.meuroimage.2012.01.021.
Mellerio C, Labeyrie MA, Chassoux F, et al. 3T MRIimproves the detection of transmantle sign in type2 focal cortical dysplasia. Epilepsia.2014;55(1):117–22. https://doi.org/10.1111/epi.12464.
Pitkänen A, Roivainen R, Lukasiuk K. Development ofepilepsy after ischaemic stroke. Lancet Neurol.2016;15(2):185–97.
Thesen T, Quinn BT, Carlson C, et al. Detection of epilep-togenic cortical malformations with surface-based MRImorphometry. PLoS One. 2011;6(2):e16430. https://doi.org/10.1371/journal.pone.0016430.
Wagner J, Weber B, Urbach H, et al. Morphometric MRIanalysis improves detection of focal cortical dysplasiatype II. Brain. 2011;134(Pt 10):2844–54. https://doi.org/10.1093/brain/awr204.
Veersema TJ, Ferrier CH, Van Eijsden P, et al. Seven teslaMRI improves detection of focal cortical dysplasia inpatients with refractory focal epilepsy. EpilepsiaOpen. 2017;2(2):162–71. https://doi.org/10.1002/epi4.12041.
Neuroimaging Evaluation in Neocortical Epilepsies 35