-
7/28/2019 2007.06.27 Acute Pulmonary Edema
1/25
Acute Pulmonary Edema
NEJM December 2005
Presentation: R2
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
2/25
Clinical Case
A 62-year-old man presents with a three-dayhistory ofprogressive
dyspnea,nonproductive cough, and low-grade fever
Congestive heart failure history
His blood pressure is 95/55 mm Hg, hisheart rate 110 beats per
minute, his
temperature 37.9 degreesC, and his oxygensaturation while
breathing ambient air86percent
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
3/25
Clinical Case
Chest auscultation reveals rales and rhonchibilaterally
A chest radiograph showsbilateralpulmonary infiltrates
consistent withpulmonary edema and borderlineenlargement of the
cardiac silhouette
How should this patient be evaluated toestablish the cause of
the acute pulmonaryedema and to determine appropriate therapy
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
4/25
The Clinical Problem
Cardiogenic pulmonary edema (also termed
hydrostatic or hemodynamic edema)
Noncardiogenic pulmonary edema (alsoknown as
increased-permeability pulmonary
edema, acute lung injury, or acute
respiratory distress syndrome)
Difficult to distinguish because of their
similar clinical manifestations
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
5/25
The Clinical Problem
Cardiogenic pulmonary edema
diuretics and afterload reduction
coronary revascularization
Noncardiogenic pulmonary edemalung-protective strategy of
ventilation
a low tidal volume (6 ml per kilogram of predicted
bodyweight)
a plateau airway pressure less than 30 cm of waterSevere
sepsis
activated protein C
low-dose hydrocortisone
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
6/25
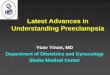
Microvascular Fluid Exchangein the Lung
Fluid and solutes that are filtered from the
circulation into the alveolar interstitial space
Do not enter the alveoli because the alveolar
epithelium is composed of very tight junctions
It moves proximally into the peribronchovascular
space
The lymphatics remove most of this filtered fluidfrom the
interstitium and return it to the systemic
circulation
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
7/25
Microvascular Fluid Exchangein the Lung
Increased hydrostatic pressure in thepulmonary capillaries
elevated pulmonary venous pressure
increased left ventricular end-diastolic pressureand left atrial
pressure
As left atrial pressure rises further (>25 mm
Hg)edema fluid breaks through the lung epithelium
flooding the alveoli with protein-poor fluid
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
8/25
Microvascular Fluid Exchangein the Lung
Noncardiogenic pulmonary edema
increase in the vascular permeability of the lung
resulting in an increased flux of fluid andprotein into the lung
interstitium and air spaces
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
9/25
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
10/25
History
Interstitial edema causes dyspnea and
tachypnea
Alveolar flooding leads to arterialhypoxemia
Cough and expectoration of frothy edema
fluid
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
11/25
History
Cardiogenic pulmonary edema
ischemia with or without myocardial infarction
exacerbation of chronic systolic or diastolic heart failure,
and dysfunction of the mitral or aortic valveparoxysmal
nocturnal dyspnea or orthopnea
Noncardiogenic pulmonary edema
pneumonia
sepsisaspiration of gastric contents
major trauma associated with the administration ofmultiple
blood-product transfusions
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
12/25
Physical Examination
Cardiogenic pulmonary edema
auscultation of an S3 gallop
a murmur consistent with valvular stenosis or
regurgitationelevated neck veins, an enlarged and tender liver,
andperipheral edema
cool extremities
Noncardiogenic pulmonary edemaabdominal, pelvic, and rectal
examinations areimportant
warm extremities
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
13/25
Laboratory Testing
Electrocardiography
Elevated troponin levels
Measurement of electrolytes, the serumosmolarity, and a
toxicology screen
Serum amylase and lipase
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
14/25
Laboratory Testing
BNP is secreted predominantly by the cardiac
ventricles in response to wall stretch or increased
intracardiac pressures
BNP level below 100 pg per milliliter indicatesthat heart
failure is unlikely (negative predictive
value, >90 percent)
BNP level greater than 500 pg per milliliterindicates that heart
failure is likely (positive
predictive value, >90 percent)
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
15/25
Laboratory Testing
BNP levels between 100 and 500 pg per milliliter
provide inadequate diagnostic discrimination
BNP can also be secreted by the right ventricle,
and moderate elevations have been reported inpatients with acute
pulmonary embolism, cor
pulmonale, and pulmonary hypertension
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
16/25
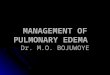
Chest Radiography
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
17/25
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
18/25
Echocardiography
The first approach to assessing leftventricular and valvular
function in patientsin whom the history, physical and
laboratory
examinations, and the chest radiograph donot establish the cause
of pulmonary edema
Less sensitive in identifying diastolic
dysfunctionDoes not rule out cardiogenic pulmonaryedema
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
19/25
Pulmonary-ArteryCatheterization
Assess thepulmonary-artery occlusion pressure
Is considered the gold standard for determining the
cause of acute pulmonary edema
Monitoring of cardiac filling pressures, cardiac
output, and systemic vascular resistance
Common complications included hematoma at the
insertion site, arterial puncture, bleeding,arrhythmias, and
bloodstream infection
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
20/25
Measurement ofcentral venous pressure
should not be considered a valid substitute
for pulmonary-artery catheterization
available data suggest that there is often a poor
correlation between the two
acute or chronic pulmonary arterial
hypertension and right ventricular overloadin the absence of any
increase in left atrial
pressure
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
21/25
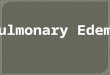
Stepwise Approach
The noninvasive approaches for diagnosis
will inevitably lead to the misclassification
of some patients
repeated and ongoing assessment is necessary
requiring simultaneous diagnosis and treatment
10 percent of patients with acute pulmonary
edema have multiple causes of edema
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
22/25
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
23/25
Guidelines
There are currently no published guidelines
from professional societies between
cardiogenic and noncardiogenic pulmonary
edema
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
24/25
Conclusions andRecommendations
Treatment can be provided while thediagnostic steps are
taken
begin with a careful history and physical
examinationelectrocardiogram
measurement of plasma BNP
chest radiograph
transthoracic echocardiogram
pulmonary-artery catheter
-
7/28/2019 2007.06.27 Acute Pulmonary Edema
25/25
Thanks for your attention