Embed Size (px)
Citation preview

Neurocognitive Sequelae of Pediatric Brain Tumors
A Presentation to the FDA Center for Drug Evaluation and ResearchPediatric Oncology Subcommittee of the Oncologic Drug Advisory
Committee
Daniel Armstrong, Ph.D.Department of Pediatrics
Mailman Center for Child DevelopmentUniversity of Miami Miller School of Medicine
andHoltz Children’s Hospital at the University of Miami/Miller School of
Medicine

Mechanisms of CNS Injury
• Genetics– Direct – Genetic Modifiers
• Structural damage• Vascular injury: Large vessel, Microvascular• Neurotransmitter abnormalities (acute and
chronic)• Metabolic abnormalities• Neuroendocrine abnormalities• Disruptions in development of
– Myelin formation– Neural connections
• Environmental and Learning Factors

Things Related to Neurocognitive Late Effects
• Tumor: Size & Location• Surgery and consequences of surgery• Radiation Therapy to the head• Chemotherapy• Age at time of treatment• Gender• Shunt, Seizures• CNS Infection• Other Considerations
– Genetics and family history– Injury unrelated to cancer– Limited learning experiences

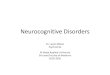
Cognitive and Adaptive Outcome in Low-Cognitive and Adaptive Outcome in Low-Grade Pediatric Cerebellar Astrocytomas Grade Pediatric Cerebellar Astrocytomas
(CCG 9891/POG 9130)(CCG 9891/POG 9130)
0
20
40
60V
IQ
PIQ
FS
IQ
VM
I
Rea
din
g
Ari
th.
Sp
ellin
g
Com
mu
n.
Dai
ly L
vg.
Soc
ial
Mot
or
AB
C
Inte
rnal
Ext
ern
al
Su
m
PopulationBase Rate
Rate in Sample
% S
core
s B
elow
Nor
mal
****
***
*
***
*** ***
IQ Tests VMI WRAT-R Vineland Adaptive Behavior Achenbach
Proportion of sub-normal scores higher than base rate: *p<.05, **p<.01, ***p<.001
Beebe, Ris,Armstrong, Fontanesi, Mulhern, & Holmes, ( J. Clin. Oncol, 2005)

Culprits
• Radiation Therapy & Chemotherapy
– Damage to small blood vessels, resulting in calcification and potentially affecting brain metabolism and chemistry
– Interference with normal brain growth and development•Myelin•Connecting structures
– Sensory impairment•Hearing with Cysplatin & RT•Peripheral neuropathy (VCR)

Long-term Cognitive Outcomes in Low Risk Long-term Cognitive Outcomes in Low Risk MedulloblastomaMedulloblastoma
0
20
40
60
80
100
Younger,SRT
Younger,RRT
Older, SRT Older, RRT
VIQPIQFSIQAttention
POG 8631: Standard vs. Reduced Dose Cranial Radiation TherapyPOG 8631: Standard vs. Reduced Dose Cranial Radiation Therapy
Mulhern, Kepner, Thomas, Armstrong, Friedman, & Kun, Mulhern, Kepner, Thomas, Armstrong, Friedman, & Kun, J Clin OncolJ Clin Oncol, 1999, 1999

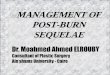
Long-term Cognitive Outcomes in Low Risk Long-term Cognitive Outcomes in Low Risk MedulloblastomaMedulloblastoma
0
20
40
60
80
100
120
Younger,SRT
Younger,RRT
Older SRT Older, RRT
ReadingMath
POG 8631: Standard vs. Reduced Dose Cranial Radiation TherapyPOG 8631: Standard vs. Reduced Dose Cranial Radiation Therapy
Mulhern, Kepner, Thomas, Armstrong, Friedman, & Kun, Mulhern, Kepner, Thomas, Armstrong, Friedman, & Kun, J Clin OncolJ Clin Oncol, 1999, 1999..

Treatment Factors Associated with Outcomes
• Neurosurgery– Focal Deficit (include sensory, motor
impairment– Bleed– Posterior Fossa Syndrome (primarily
medulloblastoma)• Mutism• Motor weakness/impairment

Treatment Factors Associated with Outcomes
• Radiation Therapy– Method of delivery
• Whole Brain, Hyper-fractionated, Stereotactic• Dose• Portal
– Possible Outcomes• Significant global intellectual impairment• Specific impairment of functions developmentally in
the RT field

Treatment Factors Associated with Outcomes
• Chemotherapy– Vincristine-
• Acute motor speed and coordination
– Anti-angiogenesis chemo (e.g., thalidomide)• Possible effects on memory, attention, processing speed
– Methotrexate (primarily used in ALL; now considered for CNS protocols)
• Breakdown in folate pathway• Calcification• White matter abnormality
– Cisplatin/Carboplatin• Hearing loss
– Cyclophosphamide, Etoposide, other New Agents
• Unknown…little experience without RT

Neruodevelopmental Model of Neurocognitive Late Effects
• Treatment seems to have its greatest effect on the part of the brain that develops after treatment. The parts of the brain that have developed before treatment seem to be relatively safe.

Emerging Cognitive Deficits: Developmental Patterns
1 2 3 4 5 6 7 8 9
Gross Motor Skills
Language SkillsAttention
Fine Motor Skills
Visual-Spatial Motor Skills

Basic Tenets of a Neurodevelopmental Model of
Neurocognitive Late Effects
• The evaluation of the functional ability is influenced by:– The timing of the treatment disruption in
the normal developmental course– The complexity of the mechanism(s)
involved (e.g., dose of radiation, types of chemotherapy).
– The age of the child at the time of assessment (expected developmental abilities-time since treatment)

Emerging Cognitive Deficits: Emerging Cognitive Deficits: Developmental PatternsDevelopmental Patterns
1 2 3 4 5 6 7 8 9
Gross Motor SkillsGross Motor Skills
Language Language SkillsSkillsAttentionAttention
Fine Motor SkillsFine Motor Skills
Visual-Spatial Motor Visual-Spatial Motor SkillsSkills

Common Late/Emerging Common Late/Emerging EffectsEffects
• Slow Processing Speed• Attention Difficulties
– Not hyperactive• Memory Difficulties
– Visual– Sequential
• Fine Motor Coordination and Speed
• Planning, Organization, Executive Function Difficulties
• Visual-Spatial-Motor Integration Difficulties
• Mathematics Difficulties (calculation, not application)
• Reading Difficulties (comprehension)
• Social Difficulties– Processing Speed– Social Cue
Detection

The Neurodevelopmental ModelTreatment-Academic Linkages
Cranial Radiation
Chemotherapy(MTX,
Steroids)
Surgery
Interrupted Myelination
Calcification
Failure of Connecting Structure
Development
Processing Speed
Visual Memory
Visual-MotorIntegration
Attention &Concentration
Organization & Planning
Structural Damage
Reading
(Comprehension)
Math (Calculations)
Handwriting
ShuntSeizureGenetics
Sensory Impairment Other
Impairment

Prevention and Treatment of Neurocognitive Late Effects
• Education• Adjust Primary Therapy (e.g., Baby
POG)• Identify neuroprotective medications• Cognitive Rehabilitation• Stimulant Medications; Other
medications?- Risks with children• Compensatory Intervention/Assistive
Technology & Accommodations• Targeted Early Intervention