Embed Size (px)
Citation preview

PRESENTED BY-SHRISTI AWALEROLL NO -6BDS 4TH YEAR
SEQUELAE OF DENTAL CARIES

CONTENTS• Introduction• Pulpitis
classification
reversible pulpitis
focal reversible pulpitis
irreversible pulpitis
acute pulpitis
chronic pulpitis
chronic hyperplastic pulpitis• Apical periodontitis• Chronic apical periodontitis(periapical granuloma)• Apical periodontal cyst(radicular cyst)• Periapical abscess

• Osteomyelitis• Cellulitis• Conclusion• References

INTRODUCTION
DENTAL CARIES
Dental caries is an irreversible microbial disease of the calcified tissues of the teeth characterized by demineralization of the inorganic portion and destruction of the organic substance of the tooth, which often leads to cavitations.

Pulpitis
Acute chronic
Apical peiodontitisAcute chronic
Periapical abscess Periapical granuloma
Periodontal cyst
Acute chronic
Osteomyelitis
Periosteitis
Cellulitis Abscess
Acute chronic
Focal Diffuse

PULPITIS
most cases of pulpitis are primarily a result of dental caries in which bacteria or their products invade the dentin and pulp tissue.
occasionally bacterial invasion occurs in the absence of caries as in cases of tooth fracture due to trauma, or cracked tooth syndrome.

CLASSIFICATION
(1) Based on Severity of Inflammation
I. Reversible pulpitis
a. Symptomatic (Acute)
b. Asymptomatic (Chronic)
II. Irreversible pulpitis
c. Acute
a. Abnormally responsive to cold
b. Abnormally responsive to heat
d. Chronic
a. Asymptomatic with pulp exposure
b. Hyperplastic pulpitis

2. Pulp degeneration
Calcific
Others
3. Necrosis
2) According to Involvement According to Involvement According to Severity According to presence or absence of direct communication
between dental pulp + oral environment

a) According to Involvement
• Focal /Subtotal / Partial Pulpitis
• Total / Generalized Pulpitis
b) According to Severity
• Acute
• Chronic
c) According to presence or absence of direct communication between dental pulp + oral environment
• Pulpitis Aperts (open pulpitis)
• Pulpitis Clausa (closed pulpitis)

REVERSIBLE PULPITIS
• mild to moderate inflammatory condition of pulp
• caused by noxious stimuli
• pulp is capable of returning to un-inflammed state following removal of stimuli
CAUSES
agent capable of injuring pulp like:
• trauma
• disturbed occlusal relationship
• thermal shock

CLINICAL FEATURES
• sharp pain lasting for a moment
• often brought on by cold than hot food or beverages
and by cold air
• does not continue when the cause has been removed
• tooth responds to electric pulp testing at lower current
DIAGNOSIS
symptoms + clinical test
• Cold test• Mobility and sensitivity to percussion usually absent unless
pulpal inflammation has spread beyond root apex into periapical region

TREATMENT• Pulpotomy(early stage)• RCT

FOCAL REVERSIBLE PULPITIS/ PULP HYPEREMIA• earliest form
• also known as pulp hyperemia
• Mild to moderate inflammatory condition
• Stimulus is removed - pain subsides
CAUSES
-Trauma
-Thermal shock – cavity preparation / polishing
-Excessive dehydration of cavity
- Galvanic current - Chemical stimulus
- Bacteria from caries

CLINICAL FEATURES
• sensitive to thermal changes particularly to cold• disappears upon removal of thermal irritant or restoration of
normal temperature
• Responds to electrical test stimulant at lower level of current
• teeth show:
• deep carious lesion
• large metallic restoration
• restoration with defective margins
MANAGEMENT
removal of irritants before the pulp is severely damaged

IRREVERSIBLE PULPITIS persistent inflammatory condition of pulp
caused by noxious stimulus
may be symptomatic or asymptomatic
CAUSES
• bacteria involvement of pulp through caries
• Chemical injury
• Thermal injury
• mechanical injury
CLINICAL FEATURES
Early Stage
paroxysm of pain caused by:
• sudden temperature changes like cold,
sweet, acid foodstuffs
pain often continues when cause has been removed
Tooth responds to electric pulp testing at lower current (when pulp necrosis – senstivity loss.
pain
• sharp
• piercing
• shooting
• generally severe

• bending over exacerbates pain which
• lying down is due to change in
• change of position intrapulpal pressure
Late Stage
• more severe as if tooth is under
• throbbing constant pressure
• History of night pain
• increased by heat and sometimes relieved by cold,
although continued application of cold may intensify pain

DIAGNOSIS
• Deep cavity extending to pulp or decay under filling (open or
closed cavity)
• Exposed pulp
• Gray scum like layer over pulp and dentin
Food debris, degenerated PMN’s, microorganisms, blood cells
• Odour of decomposition
• probing – Pain and hemorrhage
RADIOGRAPH
Pulp horn/ coronal pulp involvement

• Thermal tests
• Mobility, percussion and palpation are negative
TREATMENT• complete removal of pulp or pulpectomy
• Root canal treatment
• Extraction

REVERSIBLE PULPITIS
• Pain disappears on
removal of stimulus
• Responsive to cold
• Ease in localizing origin
IRREVERSIBLE PULPITIS
• Pain persists on removal
of stimulus
• More Responsive to
heat
• Difficulty in localizing
origin
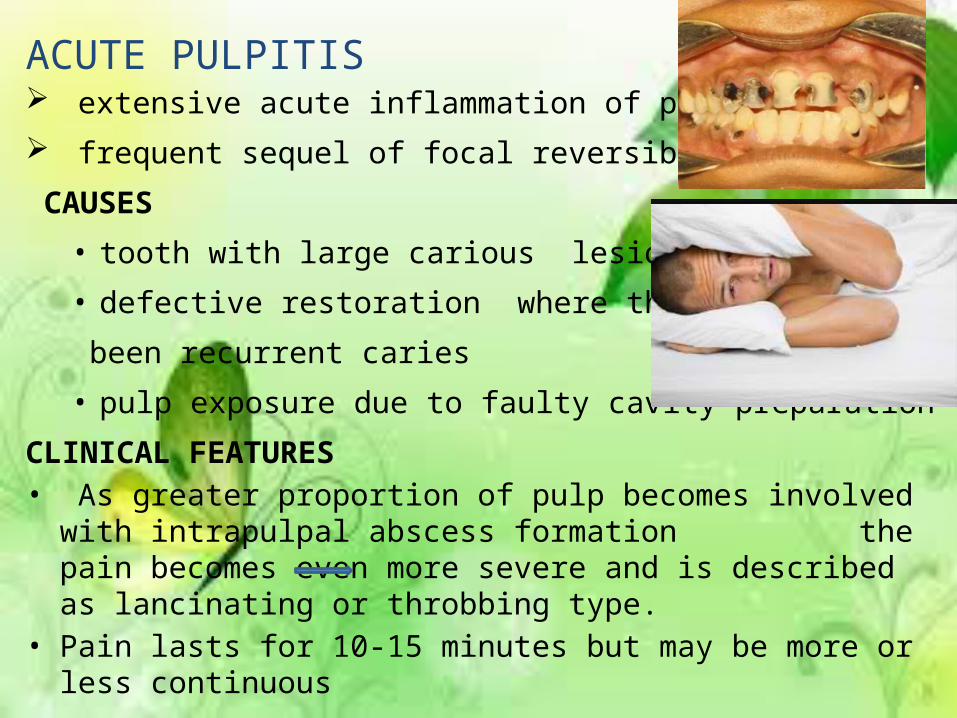
ACUTE PULPITIS extensive acute inflammation of pulp
frequent sequel of focal reversible pulpitis
CAUSES
• tooth with large carious lesion
• defective restoration where there has
been recurrent caries
• pulp exposure due to faulty cavity preparation
CLINICAL FEATURES• As greater proportion of pulp becomes involved with intrapulpal
abscess formation the pain becomes even more severe and is described as lancinating or throbbing type.
• Pain lasts for 10-15 minutes but may be more or less continuous

• Intensity of pain increase as the patient lies down.• Application of heat causes acute exacerbation of pain.• Tooth responds to electric pulp testing at lower level of
current( necrosis of the pulp-sensitivity lost)• The pulpal pain is poorly localized and may be felt in any of the
teeth of the upper or lower jaw of the affected side.
• the pulpal pain
- caused by the pressure built-up due to lack of escape of inflammatory exudate
-by pain producing substances released by the inflammatory reaction.• rapid spread of inflammationthrough pulp with pain + necrosis

MANAGEMENT
Early stages : pulpotomy
(removal of coronal pulp)
-and placing material that favors calcification such as: calcium hydroxide over entrance of root canals
Root canal filing with inert material like gutta percha should be done

CHRONIC PULPITIS
• may develop with or without episodes of acute pulpitis
• The signs and symptoms are milder than those in the acute form of the disease.
• A special form of chronic pulpitis chronic hyperplastic pulpitis.

CLINICAL FEATURES
• dull aching type
• more often intermittent than continuous
• The reaction to thermal change is dramatically reduced in comparision to that in acute pulpitis
• Due to degeneration of nerve tissue in the affected pulp, the threshold for stimulation by the electric pulp vitality tester is often increased.
TREATMENT
• root canal therapy followed by crown restoration
• extraction

CHRONIC HYPERPLASTIC PULPITIS• Also called as pulp polyp or pulpitis aperta• Essentially an excessive exuberant proliferation of chronically
inflammed dental pulp tissue
Causes
• slow progressive exposure of pulp
• bacterial infection
Clinical Features
• most commonly involved
are deciduous molars + 1st permanent molar
• excellent blood supply
• large root opening
• seen only in teeth of children+ young adults

polypoid tissue appears
• fleshy
• reddish pulpal mass filling most of pulp chamber
• or even extend beyond confines of tooth
• Less sensitive than normal pulp but more sensitive than
gingiva
• Cutting – No pain
• Easy bleeding

R/F – large open cavity with direct access to pulp chamber
Thermal tests - Feeble or no response
– Extreme cold temperature
– Ethyl chloride spray
Electric test more current required
D/D – Proliferating gingival tissue (Trace the stalk of the tissue origin
TREATMENT
• Elimination of polypoid mass followed by Extirpation of pulp
• extraction of tooth can also be done
PROGNOSIS: Favorable after RCT

DISEASE OF THE PERIAPICAL TISSUES• Once infection has become
established in the dental pulp,
spread of the process can be
only in one direction through
the root canals into periapical
region.• A certain degree of
reversibility is possible in some lesions.

APICAL PERIODONTITIS
Inflammation of periodontal ligament around root apex
CAUSE
spread of infection following pulp necrosis, occlusal trauma, inadvertent endodontic procedures etc.
TYPES:
1.Acute Apical Periodontitis
2.Chronic Apical Periodontitis

ACUTE APICAL PERIODONTITIS It is a painful inflammation of the periodontium as a result of trauma, irritation or infection through the root canal, regardless of whether the pulp is vital or non-vital
CLINICAL FEATURES• History of previous pulpitis• Thermal changes does not induce pain.
• Slight extrusion of tooth from socket.
• The tooth is tender to percussion
• Cause tenderness on mastication due to inflammatory edema collected in PDL.

RADIOGRAPHIC FEATURES:
• Appear normal except for widening of PDL space
TREATMENT & PROGNOSIS:
• Selective grinding if inflammation due to occlusal trauma.
• Extraction & endodontic treatment be done to drain exudate

CHRONIC APICAL PERIODONTITIS (PERIAPICAL GRANULOMA)
• Growth of granulation tissue continuous with the
periodontal ligament resulting from the death of the pulp
and the diffusion of bacteria and bacterial toxins from the
root canal into the surrounding periradicular tissues
• Low grade defensive reaction
• Lateral granuloma

CLINICAL FEATURES:
Tooth involved is non vital / slightly tender on percussion.
Percussion may produce dull sound instead metallic due to granulation tissue at apex.
Mild pain on chewing on solid food.
Tooth may be slightly elongated in socket.
Sensitivity is due to hyperemia, edema & inflammation of PDL.
In many cases, asymptomatic
No perforation of bone & oral mucosa forming fistulous tract unless undergoes acute exacerbation.

RADIOGRAPHIC FEATURES
• Earliest change - thickening of pdl at the root apex, loss of lamina
dura
• Later – radiolucent lesion
Well defined – sclerotic border
Poorly defined – merges with surrounding bone • Long standing lesion may show varying
degrees of root resorption.
TREATMENT & PROGNOSIS:
Extraction & RCT with / without apicoetomy.
If untreated apical periodontal cyst formation.

APICAL PERIODONTAL CYST(Radicular cyst,periapical cyst)
Common odontogenic cyst encountered.
True cyst, since consits of pathological cavity lined by epithelium &fluid filled.
Epithelium may be derived from:
• respiratory epithelium of the maxillary sinus• oral epithelium from a fistulous tract• oral epithelium proliferating apically from PDL pocket

ETIOPATHOGENISIS
Caries, trauma, periodontal disease
Pulp death
Apical bone inflammation
Granuloma formation
Stimulation, then proliferation of epithelial cell rests of Malassez
Cystification

• CLINICAL FEATURES:
• Most cases are Assymptomatic
• Age: commonly 20-60 yrs, decidous teeth.
• Common tooth maxillary anteriors.
• Non vital tooth/deep caries/restoration which is painfull on percussion.
• In some cases, cyst may undergo acute exacerbation & develop abscess that may proceed to cellulitis/ fistula.
• RADIOGRAPHIC FEATURES:
• Radolucency – round/ ovoid with a narrow opaque margin which is continuous with lamina dura.
• In long standing cyst- bone resorption of affected teeth & occasional resorption of adj. teeth may be seen.

TREATMENT & PROGNOSIS:
Extraction & curettage of apical zone.
RCT with apicoectomy.
Surgery

PERIAPICAL ABSCESS(DENTO-ALVEOLAR ABSCESS, ALVEOLAR ABSCESS)
Localized collection of pus in the alveolar bone at the
root apex following death of the pulp, with extension
of the infection through the apical foramen into the periradicular tissues
CAUSE :-
• Acute apical periodontitis
• Periapical granuloma Pulp infection
• Traumatic injury – pulp necrosis Endodontic procedures

CLINICAL FEATURES:
Tenderness of tooth, which relives after pressure application.
Extreme painful tooth extrude from socket.
Systemic manifestations like lymphadenitis & fever may present.
Extension to bone marrow spaces produce osteomyelitis.
Chronic abscess generally presents no features, since it is mild, well circumscribed area of suppuration which spread from local area.
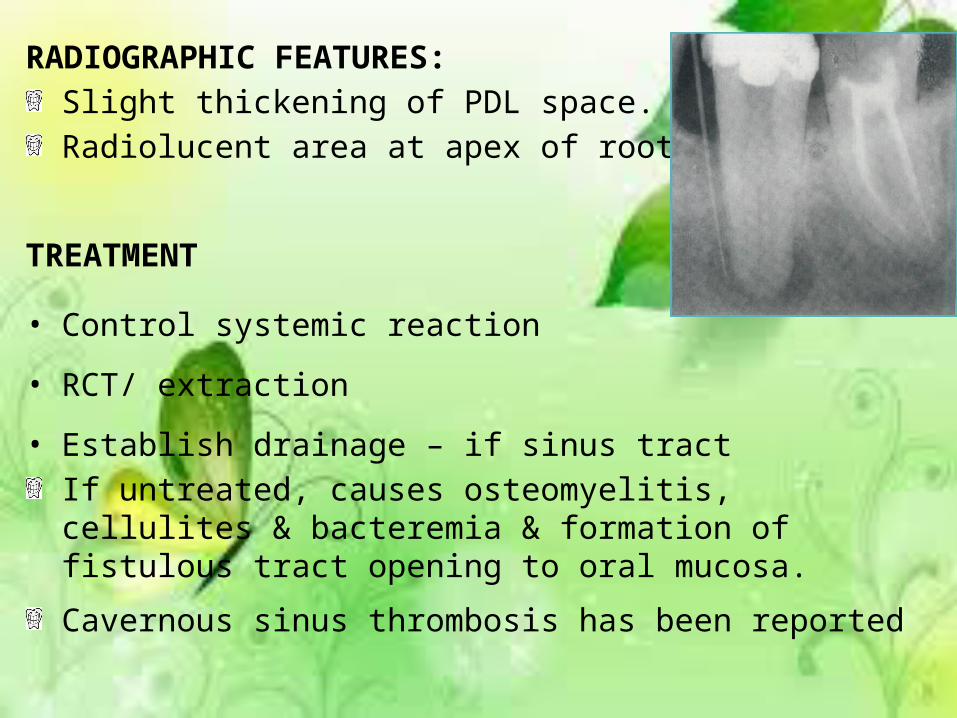
RADIOGRAPHIC FEATURES:
Slight thickening of PDL space.
Radiolucent area at apex of root
TREATMENT
• Control systemic reaction
• RCT/ extraction
• Establish drainage – if sinus tract
If untreated, causes osteomyelitis, cellulites & bacteremia & formation of fistulous tract opening to oral mucosa.
Cavernous sinus thrombosis has been reported

OSTEOMYELITIS Inflammation of the bone and its medullary contents
PREDISPOSING FACTORS:
• trauma, accidents, gunshot wounds, radiation damage, Paget’s disease & osteoporosis.
• systemic conditions like malnutrition, acute leukemia, uncontrolled DM, sickle cell anemia & chronic alcoholism.
Types: 1. Acute suppurative osteomyelitis
2. Chronic suppurative osteomyelitis:
i. Chronic Focal Sclerosing Osteomyelitis
ii. Chronic Diffuse Sclerosing steomyelitis

CLINICAL FEATURES• Deep intense Pain • Trismus• Paresthesia of lips• Elevation of temperature• Regional lymphadenopathy• WBC count elevated• Loose teeth• Pus • after periostitis – swelling of overlying mucosa• Signs & symptoms – milder, with less pain in chronic suppurative
osteomyelitis.• Acute exacerbation may occur periodically.• Suppuration may perforate bone & overlying skin or mucosa to
form fistulous tract & empty on surface.

RADIOGRAPHIC FEATURESAcute Osteomyelitis:
Ill defined area of radiolucency of right body of mandible.
CHRONIC OSTEOMYELITIS
Ill defined area of radiolucency of
right body of mandible on extracton site.

TREATMENT
• Antibiotic medications• Debridement, Drainage• Sequestrum – large; removed

CELLULITIScellulitis is diffuse inflammation of soft tissues,which
tends to spread through tissue spaces and along fascial plane.
-infection by microorganisms that produces streptokinase, hyaluronidase.
CLINICAL FEATURES
-Painful swelling due to inflammatory
edema
-if superficial tissue spaces involved skin inflammed,orange peel appearance
-inflammatory spread along deeper planes normal colour
• Maxillary teeth infection- above buccinator attachment; swelling of upper half of the face;
Eye cavernous sinus thrombosis• Mandibular teeht infection- below buccinator attachment
swelling of lower half of the face and cervical spread• Abscess formation- suppuration; discharge
TREATMENT• Removal of the origin of infection• Antibiotics• Incision and drainage

CONCLUSION
Odontogenic infection is one of the most common infections in humans. An oral infection can originate in the dental pulp and extend through the root canals of the tooth into the periapical tissues. Later it may perforate the outer cortical bone and spread in various tissue spaces or discharge onto a free mucous membrane or skin surface. It is very dangerous if the infection escapes from the confines of the bone of the maxilla or the mandible.
So, efficient methods should be implemented for prevention and management of dental caries and its sequelae.

REFERENCEShafer, Hine, Levy. Shafer’s textbook of Oral Pathology 7TH edition






![Surveillance for Dental Caries, Dental Sealants, Tooth ... · trained to use modified Radike's criteria (5) to diagnose dental caries and its sequelae (missing teeth [due to disease]](https://img.pdfslide.us/doc/110x75/5b7b46797f8b9abf2d8de46d/surveillance-for-dental-caries-dental-sealants-tooth-trained-to-use-modified.jpg)