Embed Size (px)
Citation preview


Neuroaxial Anesthesia:Neuroaxial Anesthesia:An overview.An overview.
Dr. Mahmoud Othman MD,Dr. Mahmoud Othman MD,Professor Of Anesthesia and SICU,Professor Of Anesthesia and SICU,
Depart. of Anesthesia and SICU, Depart. of Anesthesia and SICU,
Mansoura Faculty Of MedicineMansoura Faculty Of Medicine

The Advantages of Neuroaxial Anaesthesia:
1.Cost..
2.Patient satisfaction.
3.Respiratory disease.
4.Patent airway.
5.Diabetic patients.
6.Muscle relaxation.
7.Bleeding.
8.Splanchnic blood flow.
9.Visceral tone.
10.Coagulation.

* *PhysiologyPhysiology..……… :..……… :--Sensory BlockSensory Block… .… .…………………………… . … .… .…………………………… . --Motor blockMotor block………………………………………………………………………………………………--Autonomic BlockAutonomic Block.… …….……………………………….… …….………………………………
* *AnatomyAnatomy..…………… ..…… :..…………… ..…… :
* *PharmacologyPharmacology ..… : ..… :…………… ..…………………… ..………

Today: PNS & spinal cord
Tomorrow: CNS

Nervous system
Peripheral nervous system (PNS): nerves outside brain and s.c.
Central nervous system (CNS): brain & spinal cord
Somatic NS: nerves going from sense organs to CNS & from CNS to muscles & glands
Autonomic NS: controls heart, blood vesseles,intestines, other organs
Sympathetic NS: for vigerous activity (fight or flight)
Parasympathetic NS: vegetative, nonemergency responses

Peripheral NSPeripheral NSSomatic NSSomatic NS : :
–Sense organs Sense organs CNS CNS muscles and muscles and glandsglands
Something touches leg Something touches leg message to brain message to brain message from brain to arm muscle message from brain to arm muscle
brush thing off legbrush thing off leg
Sensory stimulation Motor response

http://www.carleton.ca/ics/courses/cgsc5001/img/06/neuron.jpg http://home.earthlink.net/~dayvdanls/REFLEXARC.GIF
Physiology

http://www.unm.edu/~jimmy/spinal_neurons.jpg
Bell-Magendie law:
The entering dorsal roots carry sensory information to the brain &
the exiting ventral roots carry motor information to the muscles and glands
In other words: Dorsal=sensory
Ventral=motor

Dorsal root (sensory in)
Ventral root(motor out)
rostral

The Spinal CordThe Spinal CordThe Spinal Cord
Figure 4.7, p82 http://www.bcs.rochester.edu/~dlee/bcs245/spinal_cord.jpg
Know above terms (for left figure) + terms circled in red for right figure!!
To be clear, DRG: collections of cell bodies of sensory neurons; cell bodies of motor neurons are within SC

Peripheral NSPeripheral NSAutonomic NSAutonomic NS : :
–Sympathetic NSSympathetic NS: axons activate organs : axons activate organs for “fight or flightfor “fight or flight ” ”
– –) ) Thoraco-lumber outflowThoraco-lumber outflow : ( : (T1 to T1 to
L2L2 –
Sympathetic ganglia are closely linked and Sympathetic ganglia are closely linked and act “in sympathy” with each otheract “in sympathy” with each other
Short pregang.
Long postgang.

Facilitates energy expenditure
Behaviors? Physiology? Fibers (short pre, long post, NT?)

Peripheral NSPeripheral NSAutonomic NSAutonomic NS : :
–Parasympathetic NSParasympathetic NS: facilitate : facilitate vegetative, nonemergency functionsvegetative, nonemergency functions
Para means “beside” or “related to”; Para means “beside” or “related to”;
opposite action of sympathetic NSopposite action of sympathetic NS
))Cranio- sacral outflowCranio- sacral outflow: (: (Cr1-12 & S2-4Cr1-12 & S2-4
consists of cranial nerves and nerves of consists of cranial nerves and nerves of sacral SCsacral SC long pregang. short postgang .

Facilitates energy conservation
Behaviors? Physiology? Fibers (long pre, short post, NT?)

NeurotransmittersNeurotransmitters
http://members.aol.com/Bio50/LecNotes/LNPics/ln26a.gif
Few exceptions: sweat glands stimulated by Ach.
Why does that matter?? Drugs!! OTC cold meds block parasymp or increase symp activity b/c flow of sinus fluids is parasympathetic. Side effect: inh salivation & digestion and inc HR

Spinal anesthesiaSpinal anesthesia

Spinal nervesSpinal nerves
http://dentistry.ouhsc.edu/intranet-web/Courses/DH3342/images/spin_nerves.JPG
Cauda equina

Myelin SheathMyelin Sheath : :

Types of Nerve FibersTypes of Nerve Fibers::

Physiology of neuroaxial blockagePhysiology of neuroaxial blockage
11 . .zone of differential blockzone of differential block : :
level block (sympathetic > sensory > moter )level block (sympathetic > sensory > moter )
22 . .nervous systemnervous system
Sodium channel block :Sodium channel block : nerve root ,spinal cordnerve root ,spinal cord
33 . .cardiovascular systemcardiovascular system
Autonomic denervationAutonomic denervation vasodilatation vasodilatationdecrease venous decrease venous returnreturndecrease COdecrease CO hypotension hypotension
Decrease HRDecrease HR
44 . .respiratory systemrespiratory system
55 . .GI systemGI system parasympatheticparasympathetic increase bowel move increase bowel move
rupture of distened bowelrupture of distened bowel
66 . .Liver and kidneyLiver and kidney . .

Vertebral Columen CurvesVertebral Columen Curves::




Lumber Vertebrae AnatomyLumber Vertebrae Anatomy

Spinal Cord TerminalSpinal Cord Terminal

The spinal cord usually ends at the level of L1 in adults and L3 in children.
Dural puncture above these levels is associated with a slight risk of damaging the spinal cord and is best avoided.
An important landmark to remember is that a line joining the top of the iliac crests is at L4 to L4/5

Local AnesthesticLocal Anesthestic: :
A substance which reversibly inhibits nerve A substance which reversibly inhibits nerve conduction when applied directly to tissues at non-conduction when applied directly to tissues at non-toxic concentrationstoxic concentrations

Local Anesthetics- HistoryLocal Anesthetics- HistoryLocal Anesthetics- HistoryLocal Anesthetics- History
1860 - cocaine isolated from 1860 - cocaine isolated from erythroxylum coca erythroxylum coca • Koller - 1884 uses cocaine for topical anesthesia Koller - 1884 uses cocaine for topical anesthesia • Halsted - 1885 performs peripheral nerve block with Halsted - 1885 performs peripheral nerve block with
local local • Bier - 1899 first spinal anestheticBier - 1899 first spinal anesthetic

Local anesthetics - MechanismLocal anesthetics - Mechanism Local anesthetics - MechanismLocal anesthetics - Mechanism Limit influx of sodium, thereby limiting propagation of Limit influx of sodium, thereby limiting propagation of the action potential.the action potential.

Mechanism of actionMechanism of action
Local anesthetics block generation, Local anesthetics block generation, propagation, and oscillations of electrical propagation, and oscillations of electrical impulses in electrically excitable tissue.impulses in electrically excitable tissue.
Mainly by acting on Sodium Mainly by acting on Sodium channels.channels.

Esters
Local Anesthetics - ClassesLocal Anesthetics - Classes Local Anesthetics - ClassesLocal Anesthetics - Classes
Esters

PHARMACOLOGY AND PHARMACOLOGY AND PHARMACODYNAMICSPHARMACODYNAMICS
• • Clinically used local anesthetics consist of lipid-Clinically used local anesthetics consist of lipid-soluble, substituted benzene ring linked to amine soluble, substituted benzene ring linked to amine group via alkyl chain containing either an group via alkyl chain containing either an amideamide or or esterester linkage.linkage.
• • Type of linkage separates local anesthetics into Type of linkage separates local anesthetics into either either aminoamides aminoamides (metabolized in liver)(metabolized in liver) or or aminoesters aminoesters (metabolized in liver or by plasma (metabolized in liver or by plasma cholinesterase).cholinesterase).

Local anesthetics - Classes (Rule of “i’s”)Local anesthetics - Classes (Rule of “i’s”)
EstersEsters Cocaine Cocaine
Chloroprocaine Chloroprocaine
Procaine Procaine
TetracaineTetracaine
Am”i”desAm”i”des
BupBupiivacaine vacaine
LLiidocaine docaine
RopRopiivacaine vacaine
EtEtiidocaine docaine
MepMepiivacainevacaine

Cinchocaine (Nupercaine, Dibucaine, Procaine, Sovcaine). 0.5% hyperbaric (heavy) solution is similar to bupivacaine.
Amethocaine (Tetracaine, Pantocaine, Pontocaine, Decicain, Butethanol, Anethaine, Dikain). A 1% solution can be prepared with dextrose, saline or water for injection.
Mepivacaine (Scandicaine, Carbocaine, Meaverin). A 4% hyperbaric (heavy) solution is similar to lignocaine.

Bupivacaine (Marcaine). 0.5% hyperbaric (heavy) bupivacaine is the best agent to use if it is available. 0.5% plain bupivacaine is also popular. Bupivacaine lasts longer than most other spinal anaesthetics: usually 2-3 hours.
Lignocaine (Lidocaine/Xylocaine). Best results are obtained with 5% hyperbaric (heavy) lignocaine which lasts 45-90 minutes.

Local Anaesthetics for Spinal Anaesthesia.
Local anaesthetic agents are either heavier (hyperbaric), lighter (hypobaric), or have the same specific gravity (isobaric) as the CSF.
Hyperbaric solutions tend to spread below the level of the injection, while isobaric solutions are not influenced in this way. It is easier to predict the spread of spinal anaesthesia when using a hyperbaric agent.
Hypobaric agents are not generally available.

ADDITIVES TO LOCAL ADDITIVES TO LOCAL ANESTHETICSANESTHETICS
(1)Epinephrine(1)Epinephrine : :
• • Epinephrine added to local anesthetic mayEpinephrine added to local anesthetic may
» prolong block» prolong block
» increase intensity of block» increase intensity of block
» decrease systemic absorption» decrease systemic absorption
• • Epinephrine analgesia may act via interaction Epinephrine analgesia may act via interaction with 2-adrenergic receptors in spinal cord and with 2-adrenergic receptors in spinal cord and brainbrain

Addatives to spinal anesthesia Addatives to spinal anesthesia (Cont.)(Cont.)
))22((AnalgesicsAnalgesics:: … …
A-Opioids : .. .. . ….. As : 1- Fentanyl
2-Colinidine
B-Non-opioids: ………… As : 1- Tramadol 2-
Midazolam
3-Neostigmine.

AdvantagesAdvantages : :
- -costcost ..………………………………… . ..………………………………… .--Patient SatsifactionPatient Satsifaction ………………… …………………--Respiratory DiseasesRespiratory Diseases ……………… . ……………… .--Diabetic PatientsDiabetic Patients …………………… …………………… - -Muscle RelaxationMuscle Relaxation .………………… .…………………--Surgical BleedingSurgical Bleeding ………………… …………………- - Visceral ToneVisceral Tone ..……………………… . ..……………………… .--Coagulation(DVT, PE)Coagulation(DVT, PE) .………………… .…………………

Indications Indications for for Neuroaxial Neuroaxial Anaesthesia Anaesthesia::
AA- - Spinal anaesthesiaSpinal anaesthesia is is best reservedbest reserved for for operations below the umbilicusoperations below the umbilicus e.g e.g. hernia repairs. hernia repairs , , gynaecologicalgynaecological and and urological urological opeoperations and any operation on the perineum rations and any operation on the perineum or geor ge
nitalianitalia..
BB- Spinal anesthesia applied for - Spinal anesthesia applied for All operations on All operations on the legthe legss (orthopedic-Vascular) (orthopedic-Vascular) but but an an amputatamputationion ,, though though painless, may be an painless, may be an unpleasant exunpleasant ex
perience for an awake patientperience for an awake patient..

C - C - O Older patientslder patients and and those those with with systemic dise systemic diseasease such as chronic respiratory disease, hepatic, ren such as chronic respiratory disease, hepatic, ren
al and endocrine disorders such as diabetesal and endocrine disorders such as diabetes..
DD- - It is suitable for managing patients with It is suitable for managing patients with traumatrauma if theif they have been adequately resuscitated and y have been adequately resuscitated and are not hyare not hy
povolaemicpovolaemic..
EE- - In In obstetricsobstetrics, it is ideal for manual , it is ideal for manual removal of removal of a rea retained placentatained placenta (again, provided there is no hypovola (again, provided there is no hypovola
emia).emia). Also spinal anesthesia is best choice for Also spinal anesthesia is best choice for casearan sectioncasearan section and and instrumental dlivery instrumental dlivery There are There are
definite advantages for both mother and babydefinite advantages for both mother and baby in in comparison to general anesthesiacomparison to general anesthesia
. .

Preoperative VisitPreoperative Visit::
Indications of spinal anesthesiaIndications of spinal anesthesia : : --General surgeryGeneral surgery .… … … .… … … --Orthopedic surgeryOrthopedic surgery.…… ……………………….…… ………………………--Gynacological surgeryGynacological surgery…… ………………………… ……………………--Obestatric surgeryObestatric surgery.……………………………….………………………………--Urological surgeryUrological surgery ……… .…………………… ……… .……………………--Vascular surgeryVascular surgery .……………………………… .………………………………
Medical ExaminationMedical Examination : :
Laboratory InvestigationsLaboratory Investigations : : Intravenous PreloadingIntravenous Preloading : :

Contraindictions Of Neuroaxial Contraindictions Of Neuroaxial AnesthesiaAnesthesia::
..Inadaquat Resuscitation FacilitiesInadaquat Resuscitation Facilities … . … .HypovolaemiaHypovolaemia …… …………………… …… ……………………..Patient RefusalPatient Refusal ……………………… ………………………..septicaemiasepticaemia .. …………………… .. ……………………..Local infectionLocal infection ………………… ………………… . . Neurological DiseasesNeurological Diseases … . . … . . --Coagulation DefectsCoagulation Defects.………………………….…………………………..Infants and childern(expert anesthetist)Infants and childern(expert anesthetist)
……

Absolute contraindicationAbsolute contraindicationss : :
11.. sepsissepsis
22.. bacteremiabacteremia
33.. skin infection at injection siteskin infection at injection site
44.. severe hypovolemiasevere hypovolemia
55.. coagulopathycoagulopathy
66.. increase intracranial pressureincrease intracranial pressure
77.. lack of consentlack of consent

Relative contraindicationRelative contraindicationss::
11.. peripheral neuropathyperipheral neuropathy . .
22.. uncooperative patientsuncooperative patients
33.. psychosis psychosis or emotional instabilityor emotional instability . .
44.. Mini dose heparinMini dose heparin . .
55.. aspirin or antiaspirin or anticoagulantcoagulant drug drug . .
66.. demyelating CNSdemyelating CNS . .
77.. certain cardiac lesions certain cardiac lesions (valve(valve stenosis stenosis)) . .
88.. prolongprolongeded surgery surgery . .
99.. surgery of uncertain durationsurgery of uncertain duration
1010 .…… .……infants and young childern (experience)infants and young childern (experience) . . . .

Pre-operative Visit.
Patients should be told about their anaesthetic during the pre-operative visit.
It is important to explain that although spinal anaesthesia abolishes pain, they may be aware of some sensation in the relevant area, but it will not be uncomfortable and is quite normal.
They must be reassured that, if they feel pain they will be given a general anaesthetic.

Premedication is not always necessary, but if a patient is apprehensive,
a benzodiazepine such as 5-10 mg of diazepam may be given orally 1 hour before the operation.
Other sedative or narcotic agents may also be used. Anticholinergics such as atropine or scopolamine (hyoscine) are unnecessary

Preparation for Lumbar Puncture.:
1 . spinal needle.
2 . Introducer
3 . 5ml syringe for the spinal anaesthetic solution.
4 . 2 ml syringe for local anaesthetic to be used for skin
infiltration.
5 . selection of needles for drawing up the local anaesthetic solutions and for infiltrating the skin.
6 . gallipot with a suitable antiseptic for cleaning the skin, eg chlorhexidine, iodine, or methyl alcohol.
7 . Sterile gauze swabs for skin cleansing.

8 . sticking plaster to cover the puncture site.
The local anaesthetic to be injected intrathecally should be in a single use ampoule.
Never use local anaesthetic from a multi-dose vial for intrathecal injection.

Pre-loading.
All patients having spinal anaesthesia must have a large intravenous cannula inserted and be given intravenous fluids immediately before the spinal.
The volume of fluid given will vary with the age of the patient and the extent of the proposed block. A young, fit man having a hernia repair may only need 500 mls. Older patients are not able to compensate as efficiently as the young for spinal-induced vasodilation and hypotension and may need 1000mls for a similar procedure. If a high block is planned, at least a 1000mls should be given to all patients. Caesarean section patients need at least 1500 mls.

-The fluid should preferably be normal saline or Hartmann's solution.
-Colloids like hetasrach, dextran, can be used.
-5% dextrose is readily metabolised and so is not effective in maintaining the blood pressure.
CO-spinal Fluid thrapy

PositionPosition
11 . .Lateral ( Lt lateral )Lateral ( Lt lateral )
22 . .SittingSitting
33 . .ProneProne

Postioning Of PatientPostioning Of Patient

The sitting position is preferable in the obese whereas the lateral is better for uncooperative or
sedated patients.

Males tend to have wider shoulders than hips and so are in a slight "head up" position when lying on their sides, whilst for females with their wider hips, the opposite is true.


approachapproach11..median approachmedian approach
22..paramedian approachparamedian approach

Spinal TechniqueSpinal Technique : :

Anatomy. The skin.
Subcutaneous fat..
The supraspinous ligament
The interspinous ligament
The ligamentum flavum
The epidural space
The dura. sac.
The subarachnoid space.


Layers to be piercedLayers to be pierced::
1-Skin :
2-Sc tissues:
3-Sup Spin Lig:
4-Inter Spin Lig
5-Lig Flavum :
6-Epidural Sp .
7-Dura Matter
8-Arachenoid :
9-Subarach Sp .

Continuous spinal anesthesia


Assessing the Block.
1. the patient is unable to lift his legs from the bed, the block is at least up to the mid-lumbar region.
2. It is unnecessary to test sensation with a sharp needle
3. It is better to test for a loss of temperature sensation using a swab soaked in either ether or alcohol.
4. the patient can be gently pinched with artery forceps or fingers on blocked and unblocked segments
5. Surgeons and patients should be reminded that when a block is successful, a patient may still be aware of touch but will not feel pain.

Assessing Of Spinal Assessing Of Spinal AnesthesiaAnesthesia
**-Sp. gr.(CSF) =1.003-1.008
-**Sp.gravity…. (bupivacaine)
0.5%(heavy) =1.028..……
-**Sp.gravity..… (bupivacaine)
0.5%)isobaric(
=1.006………

Factors Affecting Spread Of Factors Affecting Spread Of Local AnestheticLocal Anesthetic::
11 - -Baricity; (heavy-Isobaric)Baricity; (heavy-Isobaric) .…………..… .…………..… 22--PositionPosition . .. .…………………………… . .. .……………………………33--Volume injectedVolume injected.… . .. ………….… . .. …………44--Level of InjectionLevel of Injection.……….……… ,,,…….……….……… ,,,……55--Concentration Of local anesthConcentration Of local anesth . … … . . … … .66 - -Speed Of injectionSpeed Of injection .… ... . ..…… .… ... . ..……77--Abdomial pressure…(asites-Abdomial pressure…(asites-
pregnancy-tumours)pregnancy-tumours) . .

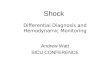
In the horizontal supine position ,hyperbaric local anesthetic solutions injected at the height of the lumbar lordosis (circle) flow down the lumbar lordosis to pool in the sacrum and in the thoracic kyphosis. Pooling in the thoracic kyphosis is thought to explain the fact that hyperbaric solutions produce blocks with an average height of T4-6.

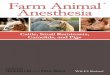
spinal anesthesia: level and duration of block
drugdrugLevelLevel
durationduration L4L4T10T10T4T4
Heavy(Heavy(05.05. % % ) )
bupivacainebupivacaine
4-84-8
mgmg..
8-128-12 mgmg14-2014-20 mgmg90-11090-110
minmin
Isobaric(Isobaric(0.0.55 % ) % )
bupivacainebupivacaine
1010--1212
mgmg1212--1515 mgmg15-2015-20
mgmg180180
minmin

Factors Affecting the Spread of the Local Anaesthetic Solution.
1- The baricity of the local anaesthetic solution
2- position
3- Dosage , concentration
4- volume injected
5- the level of injection
6- Speed of injection
7- Abdominal pressure.

Problems With Spinal BlockProblems With Spinal Block::
11--NO block at allNO block at all .. .. …………………… .. .. ……………………22--Block is one sidedBlock is one sided… .…… … …………… .…… … …………33--Block is not high enoughBlock is not high enough .… … …… .… … ……44--Block is too highBlock is too high..…………………………..…………………………55--Nausea &VomitingNausea &Vomiting...... ..… . ……………...... ..… . ……………66--ShiveringShivering . ..… ………………………… . ..… …………………………

Monitoring.
It is essential to monitor
1) Pulse
2) Blood pressure
3) Respiration
4) Consiosness


MonitoringMonitoring: :
11--ECG traceECG trace . .…………… . .……………22--Heart rateHeart rate. .……………………,…………. .……………………,…………33--Artial blood pressureArtial blood pressure . … .. .. .. ,, , . . … .. .. .. ,, , .44--Respiratory patternRespiratory pattern .. . .. …,,… ,.. .. . .. …,,… ,..55--Artial SpO2Artial SpO2 . ……………… .,,………… . ……………… .,,…………66--Level of consciousnessLevel of consciousness..……………,,,,…..……………,,,,…


Disadvantages Of spinal Disadvantages Of spinal AnesthesiaAnesthesia::
11--Diffculty (Ageing-Deformity)Diffculty (Ageing-Deformity) .…… … ..… .…… … ..…
22--hypotension(high level)hypotension(high level) .…………………… .……………………
33--Total spinalTotal spinal .……… ….……………………… .……… ….………………………
44--Longer Surgery(more than 2 hs)Longer Surgery(more than 2 hs)..… ..… ………………
55--Psychological aspect(sedation)Psychological aspect(sedation) ……………… ………………

CONt. Spinal CONt. Spinal Anesth.DisadaventAnesth.Disadavent..::
66--Postdural puncture headechePostdural puncture headeche ..… ……… .. ..… ……… .. 77--Risk of infection(meningitis)Risk of infection(meningitis).…….…………… .…….……………
88--Risk of heamtoma(clotting defects)Risk of heamtoma(clotting defects)......…......…
99--Neurological injury(cauda equina)Neurological injury(cauda equina).… ………….… …………
1010--Urine retensionUrine retension......……………………………......……………………………

ComplicationsComplications::
11..Immediate complicationsImmediate complications : :
- -hypotensionhypotension - - total spinal blocktotal spinal block - - systemic toxicitysystemic toxicity
22..Late complicationsLate complications : :
- -post dural puncture headache (PDPH)post dural puncture headache (PDPH).. --Epidural hematomaEpidural hematoma . .
- - focal neurological deficitfocal neurological deficit . . - - bacterial meningitisbacterial meningitis . .
- -

Other ComplicationsOther Complications ::
As the As the sacral autonomic fibres are among the last to resacral autonomic fibres are among the last to recover following a spinal anaestheticcover following a spinal anaesthetic, , urinaryurinary retentioretentionn may occur. If fluid pre-loading has been excessive, may occur. If fluid pre-loading has been excessive, a painful distended bladder may result and the patiea painful distended bladder may result and the patie
nt may need to be nt may need to be catherisedcatherised..
Permanent neurological complicationsPermanent neurological complications are extremely ra are extremely rare. Many of those that have been reported were due tre. Many of those that have been reported were due to the o the injection of inappropriate drugsinjection of inappropriate drugs or chemicals i or chemicals into the CSF producing nto the CSF producing meningitis,meningitis, arachnoiditis, traarachnoiditis, transverse myelitis or the cauda equina snsverse myelitis or the cauda equina syyndromendrome with with varying patterns of varying patterns of neurological impairment and sphneurological impairment and sph
incter disturbancesincter disturbances . .

Vasopressors
1. Ephedrine 2.5-6mg titrated against the blood pressure. Its effect generally lasts about 10 minutes and it may need repeating.
It can also be given intramuscularly but its onset time is delayed although its duration is prolonged..
2. Metaraminol (Aramine).
3. Methoxamine (Vasoxine).
4. Phenylephrine.
5. Noradrenaline (Levophed).
6. Adrenaline/Epinephrine.

Treatment of spinal Hypotension.
Hypotension is due to vasodilation and a functional decrease in the effective circulating volume.
1.vasoconstrictor drugs
2.All hypotensive patients should be given OXYGEN by mask until the blood pressure is restored.
3. raising their legs thus increasing the return of venous blood to the heart. spinal anaesthetic has been injected in the preceding 15 minutes as it will result in the block spreading higher and the hypotension becoming more severe.

4.Increase the speed of the intravenous infusion to maximum until the blood pressure is restored to acceptable levels .
5. pulse is slow, give atropine intravenously.

Treatment of Total Spinal.:
1. Hypotension - Remember that nausea may be the first sign of hypotension. give vassopressors.
2. Bradycardia - give atropine
3. Increasing anxiety - reassure.
4. Numbness or weakness of the arms and hands, indicating that the block has reached the cervico-thoracic junction.
5. Difficulty breathing - as the intercostal nerves are blocked the patient may state that they can't take a deep breath. As the phrenic nerves (C 3,4,5) which supply the diaphragm become blocked, the patient will initially be unable to talk louder than a whisper and will then stop breathing.

6. Loss of consciousness.
Ask for help - several pairs of hands may be useful!
Intubate and ventilate the patient with 100% oxygen.
Once the airway has been controlled and the circulation restored, consider sedating the patient with a benzodiazepine

HeadacheHeadache (PDPH) (PDPH) : :..
A characteristic headache may occur following spinal A characteristic headache may occur following spinal anaesthesia. It begins anaesthesia. It begins within 24-72 hours and may lawithin 24-72 hours and may la
st a week or morest a week or more..
It is postural, being made It is postural, being made worse by standing or even raworse by standing or even raising the head and relieved by lying downising the head and relieved by lying down..
It is often It is often occipital and may be associated with a stiff noccipital and may be associated with a stiff neck. Nausea, vomiting, dizziness and photophobia freck. Nausea, vomiting, dizziness and photophobia fr
equently accompany itequently accompany it..
It is more common in the It is more common in the young, in females andyoung, in females and
especially in obstetric patientsespecially in obstetric patients . .

It is thought to be caused by the It is thought to be caused by the continuing loss of CScontinuing loss of CSF through the holeF through the hole made in the dura by the spinal ne made in the dura by the spinal needle. This results in traction on the meninges and paedle. This results in traction on the meninges and pa
inin..
The incidence of headache is related directly to the sizThe incidence of headache is related directly to the size of the needle used. A e of the needle used. A 16 gauge needle will cause h16 gauge needle will cause headache in about 75% of patients, a 20 gauge needle eadache in about 75% of patients, a 20 gauge needle
in about 15% and a 25 gauge needle in 1-3%in about 15% and a 25 gauge needle in 1-3% . .
As the fibres of the dura run parallel to the long axis of As the fibres of the dura run parallel to the long axis of the spine, if the bevel of the needle is parallel to thethe spine, if the bevel of the needle is parallel to the
m, it will part rather than cut them and therefore, leavm, it will part rather than cut them and therefore, leave a smaller holee a smaller hole . .

Treatment of spinal headacheTreatment of spinal headache
..
11.. RRemain emain lying flat in bedlying flat in bed as this relieves the pain as this relieves the pain..
22.. They should be encouraged to They should be encouraged to drinkdrink freely or, if nec freely or, if necessary, be given essary, be given intravenous fluids to maintain adequintravenous fluids to maintain adequ
ate hydrationate hydration..
33.. Simple analgesicsSimple analgesics such as paracetamol, aspirin or c such as paracetamol, aspirin or codeine may be helpfulodeine may be helpful,,
44.. IIncreasencreasedd intra-abdominal intra-abdominal and hence epidural pre and hence epidural pressure. ssure. (Abdominal binder)(Abdominal binder) . .

55.. Caffeine containing drinksCaffeine containing drinks such as tea, coffee or such as tea, coffee or Coca-Cola are often helpfulCoca-Cola are often helpful..
66 . . Prolonged or severe headachesProlonged or severe headaches may be treated may be treated with with epidural blood patchepidural blood patch performed by aseptical performed by aseptically injecting 15-20ml of the patient's own blood intly injecting 15-20ml of the patient's own blood into the epidural space. This then o the epidural space. This then clotsclots and seals tand seals t
he hole and prevents further leakage of CSFhe hole and prevents further leakage of CSF..
It used to be thought that bedrest for 24 hours folloIt used to be thought that bedrest for 24 hours following a spinal anaesthetic would help reduce the wing a spinal anaesthetic would help reduce the incidence of headache, but this is now no longer incidence of headache, but this is now no longer
believed to be the casebelieved to be the case . .

It is widely considered that It is widely considered that pencil-point needlespencil-point needles (White(Whiteacre or Sprotte)acre or Sprotte) make a smaller hole in the dura and make a smaller hole in the dura and
are associated with a lower incidence of headache (1are associated with a lower incidence of headache (1%) than conventional %) than conventional cutting-edged needles (Quinckcutting-edged needles (Quinck
e)e)
To minimize PDPH

Headache prophylaxis with spinal anesthesia

If If inadequate sterile precautionsinadequate sterile precautions are taken are taken bacterial mebacterial meningitis or an epidural abscessningitis or an epidural abscess
Finally, permanent paralysis can occur due to Finally, permanent paralysis can occur due to 'anterior 'anterior spinal artery syndromespinal artery syndrome.'.'
This is most likely to affect This is most likely to affect elderly patientselderly patients who are su who are subjected to prolonged periods of bjected to prolonged periods of hypotension and mahypotension and ma
y result in permanent paralysis of the lower limbsy result in permanent paralysis of the lower limbs..
Other complications:

SummarySummary))11 ( (AdvantagesAdvantages : :))22 ( (Physiology / Anatomy/ PharmacologyPhysiology / Anatomy/ Pharmacology : :))33 ( (Preoperative visit.. : IndicationsPreoperative visit.. : Indications.……… .……… ExaminationExamination.……….………InvestigationsInvestigations..……..……-Intravenous Preload of fluidsIntravenous Preload of fluids -))44 ( (Contraindications to neuroaxial Contraindications to neuroaxial
anesthesiaanesthesia..………..………-))55 ( ( Technique of neuroaxial anesthesiaTechnique of neuroaxial anesthesia ..................... .....................
-))66 ( (Factors affect spread of neuroaxial spianl Factors affect spread of neuroaxial spianl
anesthesanesthes-))77 ( (Monitoring during neuroaxial anesthesiaMonitoring during neuroaxial anesthesia .………… .…………
-))88 ( (Complications and mangement of neuroaxial …… Complications and mangement of neuroaxial …… anesthesiaanesthesia

Thanks For Your AttentionThanks For Your Attention
Dr.Mahmoud Othman