Embed Size (px)
Citation preview

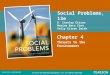
Diabetes Complication

Diabeticretinopathy
Leading causeof blindnessin working-ageadults1
Diabeticnephropathy
Leading cause of end-stage renal disease2
Cardiovasculardisease
Stroke
1.2- to 1.8-fold increase in stroke3
Diabeticneuropathy
Leading cause of non-traumatic lower extremity amputations5
75% diabetic patients die from CV events4
1Fong DS, et al. Diabetes Care 2003;26 (Suppl. 1):S99–S102. 2Molitch ME, et al. Diabetes Care 2003;26 (Suppl. 1):S94–S98. 3Kannel WB, et al. Am Heart J 1990;120:672–676. 4Gray RP & Yudkin JS. In Textbook of Diabetes 1997.
5Mayfield JA, et al. Diabetes Care 2003;26 (Suppl. 1):S78–S79.

Complication of insulin deficiency• Hyperglycemic emergencies
– Diabetic ketoacidosis (DKA)Diabetic ketoacidosis (DKA)– Hyperglycemic hyperosmolar nonketotic stateHyperglycemic hyperosmolar nonketotic state (HHS) (HHS)
• Chronic complications– NeuropathyNeuropathy– MicroangiopathyMicroangiopathy
• RetinopathyRetinopathy • NephropathyNephropathy • Foot ischemiaFoot ischemia
– Macroangiopathy – AtherosclerosisMacroangiopathy – Atherosclerosis
Risk of cardiovascular death in type 1 diabetics vs. Risk of cardiovascular death in type 1 diabetics vs. NondiabeticsNondiabetics : : >5X higher in males, 7X higher in >5X higher in males, 7X higher in femalesfemales

Complication of insulin excess
• Hypoglycemia : Activation of the sympathetic nervous system (diaphoresis, tremulousness and tachycardia) and insufficient delivery of oxygen to the brain (confusion, seizures and unconsciousness

Diabetes Complications
• Macro vascular
• Micro vascular
• Neuropathy
• Infections

Mechanisms
Hyperglycemia Tissue damage
*Repeated acute changes in cellular metabolism
**Cumulative long term changes in stable macromolecules
Genetic susceptibility
Independent accelerating factors

Macro vascular Complications

Macrovascular Complications(1)
• Have a 2 to 6 times higher risk for development of these complications than the general population
• The major cardiovascular risk factors in the non-diabetic population (smoking, hypertension and hyperlipidemia) also operate in diabetes, but the risks are enhanced in the presence of diabetes.
• Overall life expectancy in diabetic patients is 7 to 10 years shorter than non-diabetic people.

• Once clinical macro-vascular disease develops poorer prognosis for survival than normoglycemic patients with macrovascular disease
• The protective effect females have for the development of vascular disease are lost in diabetic females
• Clinical manifestation : – Ischemic heart diseaseIschemic heart disease– Cerebrovascular diseaseCerebrovascular disease– Peripheral vascular diseasePeripheral vascular disease
Macrovascular Complications(2)

CAD Morbidity and Mortality in Type 2 DM
• Framingham Data: 20 year follow-up:Age 45-74: – 2-3 fold increase in clinically evident atherosclerotic
disease in diabetics– women diabetics=male diabetics in terms of CAD
mortality
• Multiple Risk Factor Intervention Trial (MRFIT)– 5000 men with type 2 DM– Followed for 12 years– Men with type 2 DM had absolute risk of CAD-related
death 3 times higher than non-diabetic cohort

Risk Factor Clustering in Diabetes
• Type 2 Diabetes at Diagnosis:– 50% have hypertension– 30% have dyslipidemia
• UKPDS:– Prospective study– Newly detected type 2 DM:
• 335 with CAD, 8 year follow-up
– Associated with elevated LDL-C, low levels of HDL-C, systolic hypertension

Risk of MI in Diabetes
Haffner, SM et al NEJM: 339: 229-234

Glycemic Control to Reduce CAD
DCCT trial: – 1441 patients, type 1 diabetes1441 patients, type 1 diabetes– Randomized to intensive Randomized to intensive
glycemic control vs. glycemic control vs. conventional therapyconventional therapy
– Monitored prospectively for 6.5 Monitored prospectively for 6.5 yearsyears
– Results:Results:• Less retinopathy by 50%Less retinopathy by 50%
• Macrovascular complications: Macrovascular complications: 41% reduction (not statistically 41% reduction (not statistically significant)significant)
• -small number of events in -small number of events in young patient cohortyoung patient cohort
UKPDS:– 3867 patients with newly 3867 patients with newly
diagnosed type 2 DMdiagnosed type 2 DM– Intensive vs. Intensive vs.
Conventional therapyConventional therapy– 10 year follow-up10 year follow-up– Microvascular endpoints Microvascular endpoints
improvedimproved– Trend only towards Trend only towards
reduced incidence of MI ( reduced incidence of MI ( p=0.052)p=0.052)

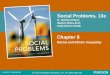
Effect of Hypertension
Mortality vs systolic blood pressure
0
10
20
30
40
50
60
70
110 120 130 140 150 160
Systolic Blood pressure (mmHg)
Te
n Y
ea
r M
orta
lity
(p
er 1
000)
Non-diabetic
Diabetic

Benefits of hypertension treatment in DM
Treating hypertension can reduce the risk of:
Death 32%
Microvascular disease 37%
Stroke 44%
Heart failure 56%
UKPDS BMJ 1998;317:703 - 713

Hypertension in Type 1 and 2 Diabetes
• Type 1– Develop after several years of DMDevelop after several years of DM, u, ultimately affects ltimately affects ~30% of ~30% of
patientspatients– Secondary toSecondary to nephropathynephropathy, a, activation of the RAASctivation of the RAAS
• Type 2– Mostly present at diagnosisMostly present at diagnosis, a, affects at least 60% of patientsffects at least 60% of patients– HyperinsulinemiaHyperinsulinemia, s, secondary to insulin resistanceecondary to insulin resistance– Activation of the sympathetic nervous systemActivation of the sympathetic nervous system
• Lower target for diabetic patients than non-diabetic patients: 130/85
UKPDS 38. BMJ 1998;317:703-713
HOT. Lancet 1998;351:1755-1762

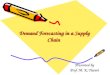
Effect of Cholesterol
Serum cholesterol vs Mortality
010203040506070
4 5 6 7
s-Cholesterol (mmol/L)
Te
n Y
ea
r M
ort
alit
y (
pe
r 1
00
0)
Non-diabetic
Diabetic

Dyslipidaemia in DM
• Most common abnormality is s HDL and s Triglyserides
• A low HDL is the most constant predictor of CV disease in DM
• Target lipid values: LDL <2.6 mmol/l, HDL >1.15 mmol/l, TG < 2.5 mmol/l

Micro vascular Complications

Eye Complications
• Retinopathy (stages)– Background– Pre-proliferative– Proliferative– Advanced diabetic eye disease– Maculopathy
• Glaucoma• Cataracts

Diabetic Retinopathy (DR)
• DR is the leading cause of blindness in the working population of the Western world
• The prevalence increase with the duration of the disease (few within 5 years, 80 – 100% will have some form of DR after 20 years)
• Maculopathy is most common in type 2 patients and can cause severe visual loss

Pre-Proliferative Retinopathy
• Rapid increase in amount of micro aneurisms
• Multiple hemorrhages• Cotton wool spots
(>5)• Venous beading,
looping and duplication
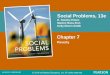
Proliferative retinopathy

Proliferative Retinopathy
• New vessels (on disc, elsewhere)
• Fibrous proliferation (on disc, elsewhere)
• Hemorrhages (preretinal, vitreous)
Panretinal photo-coagulation

Diabetic Nephropathy (DN)
• Diabetes has become the most common cause of end stage renal failure in the US and Europe
• About 20 – 30% of patients with diabetes develop evidence of nephropathy
• The prevalence of DN is higher in Black Americans than in Whites (Figures for South Africa is not available)

Stages of Diabetic Nephropathy

Stages of DN
Stage I : glomerular filtration and kidney hypertrophy
Stage II : u-albumin excretion < 30mg/24h
Stage III : Microalbuminuria (30 – 300 mg/24h)
Stage IV : Overt nephropathy (> 300mg/24h, positive u dipstick)
Stage V : ESRD characterized by blood urea and creatinine levels, hyperkalaemia and fluid overload

Screening for Nephropathy
• Type 1 Diabetes : begin with puberty, after 5 years duration of disease
• Type 2 Diabetes : start screening at the diagnosis of diabetes
• Annually, do one of the following:– u Albumin:Creatinine ratio (spot sample)– 24h u Albumin excretion rate– Early morning Albumin concentration (spot sample) – Dipstick for Microalbuminuria
• Microalbuminuria with incipient nephropathy is diagnosed if 2 or more of the tests are within the microalbumin range

Microalbuminuria
• Increased risk for overt nephropathy• Increased cardiovascular mortality
• Increased risk of Retinopathy• Increased all-cause mortality
Microalbuminuria is an indication for screening for possible vascular disease and aggressive intervention to reduce all cardiovascular risk
factors

Screening Tests for Microalbuminuria
Category
24h u collectio
n(mg/24h)
Timed collectio
n(mg/min)
Spot collectio
n(mg/mg creat)
Normal 30 20 30
Microalbuminuria
30 - 299 20 - 199 30 - 299
Albuminuria Overt
300 200 300

Management of Nephropathy
• Improvement of glycemic control• Treatment of hypertension• Treatment with angiotensin converting enzyme
(ACE) inhibitors or angiotensin II receptor antagonis (AIIRA)
• Restriction of dietary intake of protein• Once persistent elevation in u-Albumin is found
refer to a Internist or Nephrologist

Diabetic Neuropathy
• Sensorimotor neuropathy (acute/chronic)
• Autonomic neuropathy
• Mononeuropathy– Spontaneous– Entrapment– External pressure palsies
• Proximal motor neuropathy

Sensorimotor Neuropathy
• Patients may be asymptomatic / complain of numbness, paresthesias, allodynia or pain
• Feet are mostly affected, hands are seldom affected
• In Diabetic patients sensory neuropathy usually predominates

Complications of Sensorimotor neuropathy
• Ulceration (painless)• Neuropathic edema• Charcot arthropathy• Callosities

Autonomic Neuropathy
• Symptomatic• Postural hypotension• Gastroparesis• Diabetic diarrhea• Neuropathic bladder• Erectile dysfunction• Neuropathic edema• Charcot arthropathy• Gustatatory sweating
• Subclinical abnormalities• Abnormal pupillary reflexes• Esophageal dysfunction• Abnormal cardiovascular
reflexes• Blunted counter-regulatory
responses to hypoglycemia• Increased peripheral blood
flow

Entrapment Neuropathies• Carpal tunnel syndrome (median nerve)
• Ulnar compression syndrome• Meralgia paresthetica (lat cut nerve to the thigh)
• Lat Popliteal nerve compression (drop foot)• All the above are more common in diabetic patients
Mononeuropathies• Cranial nerve palsies (most common are n. IV,VI,VII)
Proximal Motor Neuropathy• Amyotrophy – most common proximal neuropathy, affects
the Quadriceps muscles with weakness and atrophy (synonym: Diabetic Femoral radiculo-neuropathy)

Screening for Neuropathy
• 128 Hz tuning fork for testing of vibration perception
• 10g Semmers monofilament
The main reason is toidentify patients at riskfor development ofdiabetic foot

Using of the Monofilament

Management of Neuropathy
• Burning pain – TADs / Capsaicin• Lancinating pain – Anticonvulsants / TAD /
Capsaicin• Painful cramps – Quinidine sulphate• Restless legs - Clonazepam

Infections
• The association between diabetes and increased susceptibility to infection in general is not supported by strong evidence
• However, many specific infections are more common in diabetic patients and some occur almost exclusively in them
• Other infections occur with increased severity and are associated with an increased risk of complications

Infections (cont)
• Several aspects of immunity are altered in patients with diabetes
• There is evidence that improving glycemic control patients improves immune function

Specific Infections
• Community acquired pneumonia
• Acute bacterial cystitis
• Acute pyelonephritis• Emphysematous
pyelonephritis• Perinephric abscess• Fungal cystitis
• Necrotizing fasciitis• Invasive otitis externa• Rhinocerebral
mucormycosis• Emphysematous
cholecystitis

44
Acute Complications of Diabetes
DKADKA
HHNKHHNK
HypoglycemiaHypoglycemia

45
• Diabetic Ketoacidosis• Most serious complication in Type 1 diabetes• Precipitating Causes
– Not enough insulinNot enough insulin– Skipping insulinSkipping insulin– Stress, traumaStress, trauma– Insulin resistanceInsulin resistance
• Ketosis• Dehydration• Electrolyte imbalance
Diabetic Keto-Acidosis

46
Symptoms of DKA
• Abdominal pain
• Anorexia
• Dehydration
• Fuity breath
• Kussmaul’s
• Change LOC
• Hypotension
• N&V
• Polyuria
• Somnolence
• Tachycardia
• Thirst
• Visual disturbances
• Warm, dry skin
• Weakness
• Wt. loss

Assessment DKA
• Hyperglycemia• Hyperosmolality• Dehydration• Electrolyte
imbalances• Metabolic acidosis• Hypoglycemia• Fluid overload
• Rehydrate• Reverse shock• Give Potassium• Corret pH• Give insulin
47

48
Treatment principle
• IV Fluids
• Potassium Replacement
• Correct pH
• Give Regular Insulin only – Initial bolus IV (0.15u/kg)– Then Regular Insulin IV drip

49
HHNKHyperglycemic Hyperosmolar Noketotic
Syndrome
• Most commonly occurs in older adults with Type II diabetes
• Always look for precipitating factors
• Factors Associated with HHNK : Drugs, procedures, chronic illness, acute illness

50
• Four Major Clinical Features– Severe hyperglycemiaSevere hyperglycemia– No or slight ketosisNo or slight ketosis– Profound dehydrationProfound dehydration– HyperosmolalityHyperosmolality
• Treatment– Similar to DKASimilar to DKA– More agresive fluid replacementMore agresive fluid replacement– Find underlying causeFind underlying cause

51
Hypoglycemia
• Also known as insulin reaction or hypoglycemic reaction
• Risk Factors– Overdose of insulinOverdose of insulin– Omitting a mealOmitting a meal– OverexertionOverexertion– Nausea and vomitingNausea and vomiting– Alcohol intakeAlcohol intake

52
Symptoms of Hypoglycemia
• Adrenergic– ShakinessShakiness– IrritabilityIrritability– NervousnessNervousness– TachycardiaTachycardia– TremorTremor– HungerHunger– DiaphoresisDiaphoresis– PallorPallor– ParesthesiasParesthesias
• Neuroglycopenic– HeadacheHeadache– Mental illnessMental illness– Inability to concentrateInability to concentrate– Slurred speechSlurred speech– Blurred visionBlurred vision– ConfusionConfusion– Irrational behaviorIrrational behavior– LethargyLethargy– LOC, coma, seizureLOC, coma, seizure

53
Interventions
• Mild– carbohydrate 10-15 gramcarbohydrate 10-15 gram
• Moderate– 20-30 gram of carbs20-30 gram of carbs– Glucagon, 1 mg SC or IMGlucagon, 1 mg SC or IM
• Severe– 50% dextrose 25 g IV50% dextrose 25 g IV– Glucagon 1 mg IM or IVGlucagon 1 mg IM or IV



• Retinopathy• microaneurysms cluster at macula->terminal
vessels obstructed->ischemia->new vessel proliferation
• Nephropathy-leads to hypertension. Assoc with the highest mortality.
• Cardiovascular disease- “silent ischemia”• Peripheral neuropathy- numbness and tingling
progressing to total insensitivity• Stiff joint syndrome- “prayer sign” and atlanto-
occipital joint involvement

• Autonomic nervous system dysfunction
-orthostatic hypotension, resting tachycardia, absent beat-to-beat variation
-hypogylcemic unawareness
-gastroparesis occurs in 20-30%


DKA
• Insulin transfers glucose and amino acids into the cells.
• Hyperglycemia->osmotic diuresis->dehydration->acidosis. Also, a build up of amino acids in the blood->lipolysis->free fatty acids->converted to ketone bodies in the liver
• Results in a intravascular fluid volume deficit of 5-8 liters, potassium deficit of 200-400 mEq, and NaCl deficit of 350-600 mEq

Treatment of DKA
• Intubate for CNS depression• Regular insulin 10 units IVP followed by 5-10
units/hr IV• Normal saline 5-10 ml/kg/hr IV• Add 5% glucose when serum blood sugar<250
mg/dl• Potassium 0.3-0.5 mEq/kg/hr IV• Monitor blood sugar, potassium, arterial pH and
urine ketones hourly• Identify cause (sepsis, MI, compliance)


HYPEROSMOLAR, HYPERGLYCEMIC NONKETOTIC COMA
-elderly, insulin deficiency, renal insufficiency, thirst deficiency
-sepsis, hyperalimentation or drugs (corticosteriods)-glucose >600 mg/dl-osmotic diuresis->hypokalemia and dehydration-serum osmolarity >350 mOsm/L-pH >7.3-hypovolemia (severe, up to 25% total body water)-patients are insulin deficient but liver insulin levels
sufficient for metabolism of free fatty acids->no ketosis-coma due to shrinkage of brain cells


Do’s and Don'ts of foot care
Patient should – check feet dailycheck feet daily– Wash feet dailyWash feet daily– Keep toenails shortKeep toenails short– Protect feetProtect feet– Always wear shoesAlways wear shoes– Look inside shoes before Look inside shoes before
putting them onputting them on– Always wear socksAlways wear socks– Break in new shoes graduallyBreak in new shoes gradually

Conclusion
• This is just an outline of the major diabetic complications, and doesn't aim to be comprehensive
• All complications are preventable with good glycaemic control
• The progression of most complications can be halted if detected early and appropriate therapy instituted