Embed Size (px)
Citation preview

Chief Executive’s Report 6-1
Status This report contains: For decision Update Regular report
For information
MEMO
To: Board Members
From: Chris Fleming, Chief Executive
Date: 18 May 2016
Subject: Chief Executive’s Report
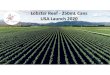
1. INTRODUCTORY COMMENTS Performance over the month of April has deteriorated against plan. The net financials for the month was a surplus of $198k against a planned surplus of $437k, $239k unfavourable for the month. On a year to date basis this brings us to a $2.261 million surplus against a plan of $4.478 million, $2.217 million unfavourable to plan. The graph below shows that the last seven months has tracked very closely to the plan albeit on a lower trajectory due to the negative first quarter we experienced. Workforce costs are the main contributor to the adverse result for the month with a $450k unfavourable variance (3.4%). The cause of the unfavourable variance is a combination of timing issues as well as some concerns over nursing resourcing versus alignment with demand. On a year to date basis, however, workforce is $130k adverse which is within 0.09% of budget. Inter District Flows, Pharmaceuticals, and Clinical Supplies continue to be over budget, however all of these areas have pegged back significantly. Aged Care expenditure has now fallen back to the levels we had projected within the budget.
We are continuing to forecast that the year end result is likely to be approximately $2 million surplus against a planned surplus of $3.856 million. Acute demand pressure is continuing to pose challenges, particularly acute medicine. This is placing increasing demands, particularly in terms of skill mix requirements in our nursing staff, and a continued increasing workload pressure for medical staff. The medical staff impact should largely be mitigated by the significant investment in Registrars. It is important to note that despite a 3.04% increase in acute caseweighted discharges, and an overall 1.73% increase in total caseweighted discharges, bed nights are marginally below the 2014/15 levels. ED presentations have increased year on year in Nelson, and have reduced in Wairau. In fact for Wairau, April was the lowest per day presentation rate for some years. Nelson’s ED attendances have increased by 5.6% over the previous year, with all the growth being in triage 1 – 3 patients, with triage 4 remaining flat and triage 5 reducing by 16%. In the past 12 months per day attendances reduced in both Nelson and Wairau over the
(1.0)
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Millions
NetSurplus(YTD)
FY15/16(A) FY15/16(B) FY14/15(A) FY13/14(A)

Chief Executive’s Report 6-2
February levels. The increase in level 4 and 5 patients presenting in Nelson in February reverted back to the normal level, while in Blenheim we have now had three months in a row where both the percentage of triage 4 and 5 patients have reduced, and the average number of patients presenting daily have reduced. It is still too early to be able to ascertain whether the reduction is directly attributable to the ED 5000 project, however the trend is promising.
2. KEY ISSUES TO NOTE
2.1. Top of the South Health Alliance The current ToSHA dashboard is attached as item 6.1. Items of interest from the broader primary and community perspective include: Primary & Community Strategy. The first draft of the Primary & Community Care strategy document has been developed and will be submitted to ToSHA for approval during May. It is expected that this will be presented to the Board at the June meeting for endorsement. Smokefree Pregnancies. Consumer interviews have been undertaken, and information from these and the stakeholder meetings has been used to draft an approach to implementation. This is being worked through with Public Health and will be with other providers before being presented to the stakeholder group for comment. There is difficulty in finalising the model with MOH still silent on how community quit services are going to be provided in 2016-17 in Nelson Marlborough. The current providers are winding up services and putting pressure on Public Health and Kimi Hauora Wairau services. Obesity Health Target. The stakeholder group is looking to redevelop Health Pathways to meet the need of the obesity health target, and to ensure we are mapping children to the best service for their needs. The DHB is currently agreeing with Kimi Hauora Wairau a changed focus to their Green Prescription and Active Family programmes by increasing the number of families able to access active families, while reducing the number of expected adult GRxs in line with demand. CAMHS is interested in providing a Triple P service for whanau with obese children. The DHB is also approaching Barnados (who have Triple P trained staff) to gauge their interest. Public Health are reviewing their data capture to ensure all referrals are being captured. Rural Services. The workstream activity is mainly focussed currently on point of care testing. Activity has slowed with the impact of conflicting demands on personnel. CVD/Diabetes Workstream. Gaps analysis of the diabetes standards of care has been completed across many of the standards and actions for closing any gaps identified. Prediabetes education in Marlborough has started. Work on a principles document to align the three self management programmes has begun. Nelson Bays Primary Health and the Diabetes Nurse Specialist service are meeting to progress integration of services.
2.2. Radiology There are some positive and negative elements around Radiology. On a positive note we now have an arrangement that allows direct access to Radiology from the Medical & Injury Centre (avoiding the Emergency Department) where the image is

Chief Executive’s Report 6-3
taken and sent back to the Medical & Injury Centre who then in turn have Christchurch Radiology Group (CRG) report on the image. It seems somewhat odd that despite having Radiologists on site, Medical & Injury Centre have to have an external company do the reporting. Then somewhat in conflict with the above, CRG has refused to fast track reporting direct access minor limb injuries in Wairau. Plain film reporting remains problematic in terms of accomplishing the reporting within reasonable timeframes, which in turn is delaying other processes. The Expression of Interest to explore potential solutions for a more consistent Radiology service provision across the district is about to be released.
2.3. Meals on Wheels On 18th May the Meals on Wheels (MOW) service moves to the new arrangement for provision of meals through the Compass Group’s snap freeze model. Planning is well advanced, involving MOW client communications on the changeover, briefing of Red Cross volunteer drivers, and consultation with CCC as the MOW referral point. Unlike some other districts in New Zealand, publicity has been generally positive. We are hopeful of a smooth transition. The next step will be to standardise the MOW assessment and referral process through Support Works.
2.4. Professional Behaviours DHB wide adoption of measures to improve communication and reduce bullying is being considered. Ros Pochin, Head of the Department of Surgery, presented on the work currently being undertaken by the Royal Australasian College of Surgeons (RACS) following the high profile public apology made by their President last year to surgical trainees and all staff affected over the years by bullying. The RACS is now working on ‘Building respect and improving patient safety’. An informal approach to address this before it reaches the stage of a formal disciplinary process has been shown to be effective, and result in a change in behaviour of 80% of those involved. A model presently adopted at Middlemore Hospital will be developed for use here, with the intention of applying it across all health care workers, not just surgeons. This also links to a current piece of work on describing the exact behaviours represented by our DHB values of respect, innovation, teamwork and integrity.
2.5. Facilities
Hospital Redevelopment. We have started initial planning on the Hospital Re-development Business Case. At this stage in our planning we have identified who should be on the Steering Group and we are also working out what control groups should be set up, and how these will report into the Steering Group. CDHB had a Clinical Leaders Group, Facilities Group and Workforce Group for their Burwood Hospital Re-development. We believe we will form similar groups, but the Workforce Group may not be as critical for us as the focus of our case is a re-build, whilst they are consolidating the services from two hospital sites onto a single site, and a significant proportion of their programme is therefore about change management. We have made initial contact with relevant GMs at Canterbury, and once our Steering Group is established we will include a visit to the Burwood site as part of the Steering Group’s induction and training. Our business case writer from the Hunter Group is away on leave until the end of May, but we envisage getting underway immediately upon her return.

Chief Executive’s Report 6-4
Learning & Development Centre. We have had a productive meeting with the Architects, ED and Orthopaedic Clinicians and other Clinical staff. The meeting has clarified where the Learning & Development Centre would logically sit relative to the hospital footprint. Further meetings are now underway between the Architect, ED and Orthopaedics to clarify requirements in these areas. The focus of our next round of meetings will be on additional beds and how these will work, together with what the Clinicians require from a Procedure Room. Once the short-medium term clinical spaces have been settled, the focus of the exercise will then revert to the Learning & Development Centre requirements. Arthur Wicks Building. Good progress is now being made on the Arthur Wicks strengthening and fit-out project. Seven out of the 22 gravity corbels, which must be attached to each column, have been completed with minimal disruption to the ED and HDU areas. The new walls and gib are close to being completed on the first floor. On the exterior of the building the foundations will be completed by early June. Asbestos removal work has been completed successfully. At this stage we still envisage that the first floor will be ‘handed over’ to us in late September, and that the overall strengthening work will be completed and signed off by the end of the calendar year. Churchill Trust Theatres. Churchill theatre plans have now been socialised with key stakeholders from NMDHB, who are Sue Allen (Operations Manager, Wairau), Lynley Gardner (Manager of Surgical Services) and Steve Low (Clinical Director – Surgical Systems). Initial concerns have largely been addressed. However, it is evident that some tweaking to the proposed plans will be required before all parties are happy. A Steering Group meeting including these stakeholders and key Churchill Trust stakeholders is scheduled for next week and we will utilise this Steering Group to reach conclusions about how the plans should be modified before we collectively move into more detailed design planning.
2.6. Information Technology Health Connect South continues to be a challenging project with complexity caused by the three parties involved (Orion Health, CDHB and ourselves), as well as the need to extract information from legacy information systems that were not designed to share information in the manner required. Good progress has been made on the most challenging functionality – referral and waitlist functionality. This functionality is relatively unique to Nelson Marlborough, and allows our clinicians to only use HCS, rather than being dependent on the patient administration system and other systems. Approximately 70% of the complex tasks have now been completed. Our single biggest risk is the availability of CDHB staff and their turnaround of tasks. This is challenging as the same CDHB resources are being used on PICS and MedChart and have been told that these are higher priority pieces of work. The Regional Programme Manager, CDHB CIO and myself will need to work together to find a solution to this issue. A regional cost allocation model for HCS has been developed by NMDHB on behalf of the region. This is currently being socialised, and has been sent to IS SLA for endorsement (subject to CFOs and CIOs signing off on it). We have taken an interest in developing it because, if agreed to, it will significantly lower the HCS support costs that were originally proposed to be charged to the region.

Chief Executive’s Report 6-5
The outcome of the ‘elaboration’ exercise conducted by the Orion Health team and the regional functional design group has now been published. The base case suggests that full foundational software (required for an NMDHB go-live) will not be released until December 2017, suggesting an NMDHB ‘go-live’ date of March 2018. This is simply too far into the future, and would create significant affordability challenges unless we were to ‘hibernate’ our project at the risk of a loss of momentum and skills. Before accepting the new dates we have agreed with Orion Health to thoroughly challenge the assumptions of what functionality NMDHB needs for a go-live, and to explore whether a go-live would be feasible from an earlier (eg July) software drop. A workshop, to be held next week, will tell us whether we could go-live earlier with acceptable trade-offs, and this will inform executive decision making. During the month a very productive visit to North Shore Hospital was undertaken by a small team. The visit affirmed that the initiatives we believe to be a priority under our paper-lite strategy are also the high-win opportunities their innovation lab are working on. These include electronic laboratory sign-off, electronic radiology ordering and sign-off, ‘Patientrack’ for digital early warning scores and bedside care, and MedChart utilising i-Pad minis for mobility / bedside care and to provide the information for bedside medicine dispensing. During the visit we also tested, and had some affirmation about, the sense of our proposed programme to digitise our paper medical charts. Under our proposed programme we would analyse the paper charts and archive charts that are unlikely to be called up again. These could be digitised on a ‘just in time’ basis. The remaining charts would then be scrubbed to remove the 40% overlaps between what is in the chart and what is in the electronic health record in Concerto / HCS. Once this is done the remaining 60% would be carefully indexed, have metadata applied and would then be scanned and stored in the relevant part of the electronic health record. Simultaneously the paper medical chart team would be transformed from a paper team to a digital health record team and the FTE count reduced from 17 to 5 over a 2 year programme implementation. Whilst Auckland DHB simply scanned the whole paper record, they affirmed that the approach we are looking at makes good sense. During the month we conducted a cursory analysis of a product provided by CSC called ‘UltraGenda.’ This product essentially connects applications such as the patient administration system and radiology systems together, and forms a master scheduler that works across these disparate systems. If implemented successfully the product has the potential to link the overall patient journey as electronic workflow, and to digitally manage all lists (ie lists for pre-admission clinics, radiology appointments etc). It could have a significant and positive impact on our paper-lite programme. New Zealand’s software vendors, Orion Health and CSC in particular, but also another 26 vendors have undertaken to work together to develop a common health platform where any of the vendors can offer functionality, and the purchaser can be confident that the vendor’s product will work on the common platform. Under this model Ultra-Genda could be implemented very successfully. CDHB have Ultra-Genda licences but do not have the capacity to consider its implementation so are likely to give them up. CSC is very keen to have a working version of Ultra-Genda in place for Asia-Pacific, particularly NZ and Australia. We are looking into whether we could form a strategic partnership whereby we get the licences at no cost, share the development and implementation costs with CSC and get a product at a low cost to the DHB (in return for being the first reference-able client in Australasia). This would move our paper-lite programme forward significantly.

Chief Executive’s Report 6-6
2.7. Public Health 2.7.1 Submissions
In the last month, the Public Health Service has prepared a submission on the Review of the Code for Advertising to Children, and the Children’s Code for Advertising Food.
2.7.2 Tap Into Water – A Campaign Reinforcing Water as the Drink of The “Tap into Water” six month campaign has been launched in Nelson and
Marlborough. The campaign will focus on three sectors (workplaces, schools, and recreational providers) and highlights the health benefits of choosing to drink water over sweet drinks. Sectors will be provided with information and resources, and will be encouraged to implement initiatives to create behaviour change within their respective sectors. This will be supported through monthly “Tap into Water” e-mails, website and Facebook page.
2.7.3 Alcohol Controlled Purchase Operations On 26th April Countdown Blenheim started its 42 day suspension to sell
alcohol as the penalty set by the Alcohol Regulatory Licensing Authority after this supermarket’s fifth failed Controlled Purchase Operation (CPO). Two more supermarkets in Blenheim are still waiting for hearing dates to be set after failing Controlled Purchase Operations. Concerns were raised by Marlborough tri agency members regarding premises not meeting their obligations under the Act to ensure substantial food is provided when alcohol is being served. Agencies are working on a plan to conduct future food CPOs.
2.7.4 Alcohol Licensing – New Supermarket Blenheim The alcohol team worked together on a Brief of Evidence and presented to a
District Licensing Committee at Marlborough District Council in March. The Medical Officer of Health has opposed elements of the proposed license relating to appropriate display of alcohol. The Marlborough DLC has released their decision and the MOH has filed notice of appeal against the decision to grant an off license for the supermarket involved. The MOH believes the Committee erred in its decision as it did not limit the exposure of shoppers to alcohol as far as reasonably practicable as required by the legislation.
2.7.5 Zig Zag Signage The Richmond store has removed their offending signage, however it still
remains in Tahunanui. A final warning letter has been sent to the premises breaching the tobacco product advertising requirements. This letter was requested by the MOH giving the premises another 14 days to remove the signs or face the possibility of prosecution.
2.8. Communications
The communications team continues its rapid phase of new channel development, with the launch of a new Staff Weekly newsletter in late April. The majority of reaction to our new Nelson Marlborough Health website has been positive, and we have started to scope further improvements for the next financial year – such as the production of better hospital maps, and the ability to ‘share’ pages

Chief Executive’s Report 6-7
on social media and ‘print-ready’ pages that would be ideal for our visitor and patient information. This basic functionality would set us up to be more paper-lite. By referring people to printable, shareable pages we can reduce the amount of brochures produced and printed.
3. PERFORMANCE INFORMATION 3.1 Health Target Provisional Information
Overall good progress continues against the Health Targets. The Faster Cancer Treatment indicator has been impacted by the Christmas / New Year period. The March quarter for Faster Cancer Treatment has fallen to 69% however April has improved back to 80%.
Target December 2015 Qtr
March 2016 Qtr
April 2016
Shorter Stays in Emergency Department
95% 97% 96% 96%
Improved Access to Elective Surgery
100%
102% 102% 102%
Faster Cancer Treatment 62 Days 85% 84% 69% 80%
Increased Immunisation 95% 92% 90% 86%
Better Help For Smokers to Quit (Primary Care)
90%
92%
N/A
N/A
More Heart & Diabetes Checks 90% 91% N/A N/A
3.2 Maori Health Target Progress
The table summarises the population comparisons between Nelson Marlborough Maori and non-Maori populations. The period is March to April 2016.
Indicator Target NMDHB
European/
Other
NM
Maori
Gap Trend Previous
Month
PHO Enrolment 100 98 84 14
No change
ASH 0 – 4 yrs 7343 4365 3952 - 413
No change
ASH 45 – 64yrs 3838 2380 4491 2111
No change
Breastfeeding (6 wks) 75 67.8 64.6 3.2
↑
Breastfeeding (3 mths) 60 64.8 50.0 14.8
↓
Breastfeeding (6 mths) 65 71.7 53.4 18.3
↓
Cardiovascular Risk Assessment 90 91.1 85.4 5.7
No Change
CVRA 35 – 44yrs (new target) 90 0 64.8 0
No Change
Angiogram in High Risk Patients 70 96.3 100 - 3.7
No Change
Post-Angio Data Collection 95 100.0 100 0 ↑
Breast screening (50 – 69yrs) 70 78.5 75.9 2.6
No Change
Cervical screening (25 – 69yrs) 80 83 70.0 13
No Change

Chief Executive’s Report 6-8
Immunisations (8mths) 95 92.1 95.7 - 3.6
No Change
Rheumatic Fever 0 Null Null Null . New target
Immunisation (Influenza) 75 67 65 2
No Change
Mental Health 0 115 285 170
No Change
Oral Health (New target) 95 85.1 56.9 28.2 New target
Key
Target Attained Within 10% of
target
Within 10-20%
of target
Greater than
20% of target
Adverse Performance There are a number of noted changes in three of the targets when compared to the
previous month:
Breastfeeding (6 weeks) – Covering the quarter to March 2016, the target showed an achieved result at 75.8% against the national target of 75%. The most recent update shows the target is tracking within 10 – 20% which is a negative trend
Breastfeeding (3 months) – Similarly, the DHB was performing well with its progress being within 10% of the national target at 59.2% for the first quarter. The DHB would have expected an improvement in the target. However, the latest results indicate a negative trend where the target is within 10 – 20%
Breastfeeding (6 months) – There has been a slight improvement in the target performance from March to April. The target was reported in March at 52.5% whereas for April it has improved to 53.4%. The national target is 65%
CVRA 35–44 years – This target covers the percentage of Maori males who have had a cardiovascular risk assessment within the past five years. It is being measured because of the higher than usual level of heart disease and mortality in this age group when compared to non-Maori. The target is new to the Maori health plan and is seen by the Ministry of Health as being preventable in primary health care. Work has started with the local PHOs about identifying actions and activities that can improve the target and sector performance in the new financial year
Oral Health – This is a new target and covers the percentage of preschool children enrolled with community oral health services. There is concern about this target and the Principal Dental Officer and Chief Medical Officer are now looking into why there are low pre-enrolments to our Community Oral Health Services, and what strategies/actions the DHB will take to improve the coverage. The Ministry of Health has set this target because it is preventable within primary health care.
Improved Performance Post Angio Data Collection – As at March the DHB performance was at 80%
achieved and within 10 – 20% of the national target of 95%. The updated April result has showed the target being achieved at 100% which is a pleasing result. As the final quarter proceeds covering April – June, the DHB will monitor closely the ongoing performance and achievement of the result.
No Change in Performance There are a number of targets which have reported a ‘No Change’ in the target
achievement since the last report was made. Where the target is within 10 – 20% of the national target the DHB will work with the sector to influence the behaviours. A ‘no change’ might mean a plateau in past actions. Either way, more work is needed to refresh the approaches and to lift the effort so that the targets are within 10% of the target or achieved.

Chief Executive’s Report 6-9
3.3 Clinical Services Overall volumes continue in line with expectations. The only major challenge is the
mix change between medicine and other services which is placing resource pressure on the medicine teams.
3.4 Mental Health 3.4.1 Activity – Specialist Psychogeriatric demand is significant at present with staff and the facility
under some pressure.
April 2015
YTD
Last Month
Variance YTD
Actual Planned # % # %
Caseweighted Discharges
Acute
Medical 6,422 6,258 164 2.62% 6,089 333 5.47% 2.25%
Neonatal / Maternity 1,467 1,556 (89) (5.72%) 1,553 (86) (5.54%) (6.71%)
Surgical 4,279 4,625 (346) (7.48%) 4,167 112 2.69% (7.69%)
Total Acute 12,168 12,439 (271) (2.18%) 11,809 359 3.04% (2.55%)
Elective
Medical 646 490 156 31.84% 527 119 22.58% 30.72%
Neonatal / Maternity 0 0 0 0.00% 0 0 #DIV/0! 0.00%
Surgical 5,265 5,590 (325) (5.81%) 5,436 (171) (3.15%) (6.07%)
Total Elective 5,911 6,080 (169) (2.78%) 5,963 (52) (0.87%) (3.08%)
Total Caseweighted Discharges 18,079 18,519 (440) (2.38%) 17,772 307 1.73% (2.72%)
Outpatients
First Specialist Assessments
Medical* 4,887 5,635 (748) (13.27%) 6,818 (1,931) (28.32%) 18.43%
Neonatal / Maternity 668 607 61 10.05% 707 (39) (5.52%) 6.70%
Surgical 11,164 10,896 268 2.46% 10,769 395 3.67% 1.43%
Total First Specialist Assessments 16,719 17,138 (419) (2.44%) 18,294 (1,575) (8.61%) 7.23%
Follow Ups
Medical 10,856 12,851 (1,995) (15.52%) 12,965 (2,109) (16.27%) (6.45%)
Neonatal / Maternity 644 590 54 9.15% 714 (70) (9.80%) 9.70%
Surgical 18,324 18,727 (403) (2.15%) 18,920 (596) (3.15%) (3.39%)
Total Follow Ups 29,824 32,168 (2,344) (7.29%) 32,599 (2,775) (8.51%) (4.38%)
Total Outpatient Assessments 46,543 49,306 (2,763) (5.60%) 50,893 (4,350) (8.55%) (0.35%)
ED Attendances
- Nelson 23,710 22,444 1,266 5.64% 5.85%
- Wairau 16,877 17,501 (624) (3.57%) (0.60%)
Total ED Attendances 40,587 39,945 642 1.61% 3.04%
Bed Nights
- Nelson 32,856 33,409 (553) (1.66%) (0.20%)
- Wairau 13,761 13,565 196 1.44% 5.28%
Total Bed Nights 46,617 46,974 (357) (0.76%) 1.37%
* Cardiology Volumes have been corrected in the current year as there was some duplicate counting. This means comparison to
last year is not valid
April 2016 YTD Variance
Variance To Last
Year

Chief Executive’s Report 6-10
3.4.2 Activity – NGO
No formal advice has been received from MOH as yet regarding the Te Whare Mahana contract. There continues to be no Nelson Marlborough clients utilising the DBT program provided by Te Whare Mahana.
The staff member who was providing data from Emerge/Richmond NZ has
left the company, and as they are still unable to report to PRiMD, we have been unable to source data for the last couple of months.
Year to Date Year End 14/15
Feb-16 Mar-16 Apr-16 Monthly Average Monthly Average
Inpatient Acute Admissions 23 21 25 25 25
Inpatient Acute LOS (days) 12.27 12.05 12.81 12.9 12.4
Inpatient Seclusion Use (hours)* 241.6 50.0 194.1 305.8 234.5
Inpatient Seclusion Client Count 8 5 5 8 9
Community Crisis Contacts* 185 114 84 129 129
Community After Hours Call 57 60 59 46 53.9
Community Caseload Numbers 2661 2688 2605 2712 2865
Psychogeriatric IP Admissions* 6 7 5 5.3 5.0
Psychogeriatric IP Occupancy (%)* 109.3% 110.6% 117.3% 102.3% 86.7%
*Provisional @ 8 May 2016
Last Three Months
Service Last 12 months Year End 13/14
Feb-16 Mar-16 Apr-16 Monthly Average Monthly Average
Emerge* 28 0 0 30 32
Gateway Housing Trust 179 172 163 174 168
MHSS 36 35 35 36 37
Te Whare Mahana 42 36 30 41 51
Te Ara Mahi 80 80 0 88 77
Health Action Trust (Kotuku) 17 20 27 21 23
Care Marlborough - day activity
(average clients per day)16 15 14 16 16
The White House (average clients
per day)13 14 15 14 18
SF Nelson (contact hours) 87 81 72 82 55
SF Blenheim (contact hours) 111 107 97 145 92
St. Marks 28 32 35 40 44
Te Piki Oranga# 278 299 286 257
Last Three Months
*Reports directly to PRiMD, which has a reporting timeframe of the 20th of the month, so numbers are provisional only.
# Te Piki Oranga is still unable to report to PRiMD and have provided provisional data that is incomplete in the interim.

Chief Executive’s Report 6-11
3.5 Disability Support Services
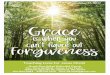
3.6 Emergency Department Presentations The month of April saw a dramatic reduction in ED attendances in both Nelson and
Wairau. This drop is a pattern with April 2015 also registering a drop in both Nelson and Wairau. For Wairau the reduction saw the lowest per day presentations for many years, while Nelson the level of attendances were five patients a day more than last April.
The table below shows the movement in ED presentations by triage category for both
Nelson and Wairau. The biggest increases are in Triage 2 district wide with a relatively consistent growth on both sides of the hill for Triage 3. Both locations have seen a reduction in Triage 4 & 5, however Wairau continues to be over represented in Triage 3, 4 & 5s. The ED 5000 project is, however, delivering results which is pleasing to see.
We need to continue to investigate further opportunities to reduce demand in ED on both sides of the hill as Nelson ED attendances per capita appear to be around 300 per 1,000 while Wairau has reduced to 450. The national average is approximately 240.
Intellectual & Physical Disabilities
Contracted Services IDSS PDSS Total ID & PD Total ID & PD
Current Moh
Contract
As per Contracts at month
end 159 15 174
Beds – Moh
Individual contracts
As per Contracts at month
end 16 1 17
Beds – P&F -
Chronic Health
Conditions
As per Contracts at month
end 3 8 11
Beds – Individual
contracts with ACC
As per Contracts at month
end 1 1 2
Total number of
service users
contracted
Residential contracts -
Actual at month end 179 25 204
Vacant Beds Actual at month end 11 4 15
Warwick St now
counted
Total available beds 190 29 219
Total number of
service users
supported
Residential service users -
Actual at month end 179 25 204
Beds – Respite Service users at month end 1 1 2
Personal cares service
users - Actual at month end 1 1 2
Total service users
supported 181 27 208
Last month 209 - 1
death
Total available bed days 5,760 720 6,480 65,452
Total Occupied Bed
days
Actual for full month -
includes respite 5,439 690 6,129 62,876
Note: **2 PDSS service
users occupy ID beds
Total Occupied Beds
Based on actual bed days
for full month (includes
respite volumes) 94% 96% 95% 96%
YTD April 2016Current April 2016
Service provided

Chief Executive’s Report 6-12
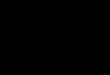
3.7 Acuity / Workload The acuity / workload graphs below show a continuation of the recent trends. The
general trend is showing increasing acute pressure in Nelson while Wairau remains relatively flat. Winter has not yet hit us in terms of acute presentations. Last year winter started to pick up in April. This has not yet occurred, however inevitably this will arrive over the next month or so.
2014/15 2015/16 Movement 2014/15 2015/16 Movement Nelson Wairau
Triage 1 141 174 23.4% 104 100 -3.8% 64% 36%
Triage 2 3574 4312 20.6% 1398 1795 28.4% 71% 29%
Triage 3 10411 11099 6.6% 7822 8349 6.7% 57% 43%
Triage 4 7239 7225 -0.2% 7497 6139 -18.1% 54% 46%
Triage 5 1079 906 -16.0% 648 495 -23.6% 65% 35%
22444 23716 5.7% 17469 16878 -3.4% 58% 42%
NELSON WAIRAU % of Total By Triage
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
120
125
130
135
140
145
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
NMDHB ED Performance
Presentations Per Day NMDHB 6 Hr Target Results ED 6 Hour Target
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
% of ED Attendances Admitted
Total ED Admissions Nelson ED Admissions Wairau ED Admissions
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
64
69
74
79
84
89
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Nelson ED Performance
Presentations Per Day NMDHB 6 Hr Target Results ED 6 Hour Target
91.0%
92.0%
93.0%
94.0%
95.0%
96.0%
97.0%
98.0%
48
50
52
54
56
58
60
62
64
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Wairau ED Performance
Presentations Per Day NMDHB 6 Hr Target Results ED 6 Hour Target
0
500
1000
1500
2000
2500
3000
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Nelson ED Attendances by Triage Category
Triage 1 Triage 2 Triage 3 Triage 4 Triage 5
0
500
1000
1500
2000
2500
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Wairau ED Attendances by Triage Category
Triage 1 Triage 2 Triage 3 Triage 4 Triage 5
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Nelson ED Attendances by Triage Category - %
Triage 5
Triage 4
Triage 3
Triage 2
Triage 10.0%
10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%90.0%
100.0%
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6Wairau ED Attendances by Triage Category - %
Triage 5
Triage 4
Triage 3
Triage 2
Triage 1

Chief Executive’s Report 6-13
0
100
200
300
400
500
600
700
800
900
1,000
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Acute CWD's Nelson
Medical Acute CWDs Surgical Acute CWDs Neonatal & Maternity Acute CWDs
0
100
200
300
400
500
600
700
800
900
1,000
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Elective CWDs - Nelson
Medical Elective CWDs Surgical Elective CWDs
0
200
400
600
800
1,000
1,200
1,400
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Acute Discharges (Raw ) - Nelson
Medical Acute Discharges Surgical Acute Discharges Neonatal / Maternity Acute Discharges
0
200
400
600
800
1,000
1,200
1,400
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Elective Discharges (Raw) - Nelson
Medical Elective Discharges Surgical Elective Disharges
-
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Acute CWD Per Discharge - Nelson(Excl Emergency)
Medical Acute Surgical Acute Neonatal & Maternity Acute
-
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Elective CWD Per Discharge - Nelson
Medical Elective Surgical Elective
0
50
100
150
200
250
300
350
400
450
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Acute CWDs - Wairau
Medical Acute CWDs Surgical Acute CWDs Neonatal & Maternity CWDs
0
50
100
150
200
250
300
350
400
450
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Elective CWDs - Wairau
Medical Elective CWDs Surgical Elective CWDs
0
100
200
300
400
500
600
700
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Acute Discharges (Raw) - Wairau
Medical Acute Discharges Surgical Acute Discharges Maternity & Neonatal Discharges
0
100
200
300
400
500
600
700
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Elective Discharges (Raw) - Wairau
Medical Elective Discharges Surgical Elective Discharges

Chief Executive’s Report 6-14
Bed utilisation has reduced back in both Nelson and Wairau in April, and this was
reflected in lower volumes both in terms of ED attendances and lower caseweighted discharges.
The trendcare clinical hours variance below is concerning. On one hand this is a positive result in as much as the vast majority of areas have adequate resourced nursing hours when compared to resourced nursing hours required based on clinical acuity. This is at a monthly level, and on a daily basis there would have been more variability. However on the other hand for the past two months there has been approximately 3,500 hours per month in excess of clinical needs. This equates to approximately $170k of resources. We have also noticed that there are a significant number of changes to the rosters after they have been published, with not as much annual leave as planned in the rosters being taken.
A review by the Operations Manager / Associate Directors of Nursing and the Director of Nursing is underway to identify what actions we can take in terms of mitigating these issues, whilst at the same time not wishing to see a return to any significant negative variances. The goal must be to minimise variances both positive and negative. The positive variance in Trendcare Clinical Hours is definitely being seen in the negative financial results for personnel.
-
0.25
0.50
0.75
1.00
1.25
1.50 Ja
n-1
4
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Acute CWDs Per Discharge - Wairau(Excl Emergency)
Medical Acute Surgical Acute Neonatal & Maternity Acute
-
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Elective CWDs Per Discharge - Wairau
Medical Elective Surgical Elective
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Bed Utilisation - Trendcare
Nelson Hospital Utilisation Wairau Hospital Utilisation
Mental Health & Alex Utilisation

Chief Executive’s Report 6-15
3.8 Elective / Acute Arranged Services The elective service performance is presented in three components:
MOH Elective / Acute Arranged Discharges
Caseweighted Discharges
ESPI Performance.
3.8.1 MOH Elective / Acute Arranged Discharges Production plan elective discharges are tracking in line with expectations for
the year. There is a small under provision internally, but this is more than offset with inter district flow electives.
-1,500
-1,000
-500
-
500
1,000
1,500
2,000
2,500
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Trendcare Clinical Hours Variance - Nelson
SCBU Nn
Paeds Nn
Post Natal Nn
Delivery Nn
DSU& ON overflow Nn
AT&R Nn
ICCU Nn
MU Nn
Ward 9
Ward 10 Nn
-1,500
-1,000
-500
-
500
1,000
1,500
2,000
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Trendcare Clinical Hours Variance - Wairau
DSU
Paeds
Postnatal
Delivery
HDU/AAU
IPU Surgical
Inpatient Medical
Inpatient/AT&R

Chief Executive’s Report 6-16
NMDHB
MoH / Production Plan Elective Discharges
April 2016
Service
Unit
CodeDescription Type Annual Plan Budget YTD Actual YTD Vol Variance
Actual %
Complete vs
YTD Plan
Medical M00001 General Medicine - Discharges Elective Disch 17 14 6 -8 43.1%
Arranged Admit 10 8 17 9 207.7%
General Medicine - Discharges Total 27 22 23 1 104.1%
M10001 Cardiology - Discharges Elective Disch 98 80 105 25 131.0%
Arranged Admit 15 13 7 -6 54.9%
Cardiology - Discharges Total 113 93 112 19 120.5%
Medical Total 140 115 135 20 117.4%
SubSpec S40001 Ophthalmology - Discharges Elective Disch 690 569 512 -57 90.1%
Arranged Admit 26 22 30 8 138.4%
Ophthalmology - Discharges Total 716 590 542 -48 91.8%
S70001 Urology - Discharges Elective Disch 426 354 389 35 109.8%
Arranged Admit 170 142 167 25 117.5%
Urology - Discharges Total 596 496 556 60 112.0%
SubSpec Total 1312 1087 1098 11 101.1%
Surgical D01001 Dental - Discharges Elective Disch 18 15 16 1 108.6%
Arranged Admit 1 1 0 -1 0.0%
Dental - Discharges Total 19 16 16 0 102.9%
MS02016 Skin Lesions excisions Elective Disch 475 392 574 182 146.3%
Arranged Admit 0 0 10 10 0.0%
Skin Lesions excisions Total 475 392 584 192 148.8%
S00001 General Surgery - Discharges Elective Disch 1210 1002 952 -50 95.0%
Arranged Admit 264 229 158 -71 69.0%
General Surgery - Discharges Total 1474 1231 1110 -121 90.2%
S05001 Anaesthetics - Discharges Arranged Admit 31 26 63 37 243.9%
Anaesthetics - Discharges Total 31 26 63 37 243.9%
S25001 ENT - Discharges Elective Disch 700 571 519 -52 90.8%
Arranged Admit 20 17 22 5 131.0%
ENT - Discharges Total 720 588 541 -47 92.0%
S45001 Orthopaedics - Discharges Elective Disch 1108 927 920 -7 99.3%
Arranged Admit 334 284 282 -2 99.3%
Orthopaedics - Discharges Total 1442 1211 1202 -9 99.3%
S75001 Vascular - Discharges Elective Disch 53 47 18 -29 38.3%
Arranged Admit 31 25 7 -18 27.6%
Vascular - Discharges Total 84 72 25 -47 34.6%
Surgical Total 4245 3536 3541 5 100.1%
W C & Y M55001 Paediatric Medical - Discharges Elective Disch 0 0 0 0 0.0%
Arranged Admit 1 1 0 -1 0.0%
Paediatric Medical - Discharges Total 1 1 0 -1 0.0%
S30001 Gynaecology - Discharges Elective Disch 825 725 682 -43 94.0%
Arranged Admit 151 133 120 -13 90.4%
Gynaecology - Discharges Total 976 858 802 -56 93.5%
W C & Y Total 977 859 802 -57 93.4%
Grand Total 6674 5596 5576 -20 99.6%
Inter District Flows 726 638 792 154 124.1%
Grand Total 7400 6234 6368 134 102.1%
The Elective Health Target section in the CSR has been changed in line with the 2015_16 criteria.
Where discharge type is one of the following:
1. Elective discharge from a surgical purchase unit
2. Elective surgical discharge from a non surgical purchase unit
3. Arranged discharge from a surgical purchase unit
4. Arranged surgical discharge from a non surgical purchase unit
Note that the caseweight section is aligned with the Price Volume Schedule and Production Plan caseweights (includes IDF inflows) while the MoH
Elective Health Target discharges are aligned to the MoH and Production Plan discharges (excludes IDF inflows)
This means that the MoH Elective Health Target discharges show patients whose caseweights are displayed in both Elective AND Acute sections
of the caseweight report, depending on their status as a Waitlist or an Arranged admission

Chief Executive’s Report 6-17
3.8.2 Caseweighted Discharges Caseweighted discharges are slightly behind plan but ahead of the same
year to date period last year.
3.8.3 Elective Service Performance Indicators ESPI 2 results improved in February, however it had slipped backwards
again in March. This has subsequently returned back to acceptable levels in April. These indicators are very sensitive due to the target being very low numbers.
Caseweights
NMDHBApril 2016 Year to Date
Type ServiceAnnual
Plan
Budget
YTDActual YTD
Vol
Variance
Last YTD
Actual
Against
2015/16
Plan
Against
April 2015
Actual
Acute Med 6926 5807 5975 168 5648 103% 106%
SubSpec 279 231 360 129 306 156% 118%
Surg 4898 4205 3728 -477 3657 89% 102%
W C & Y 2690 2194 2104 -90 2198 96% 96%
Acute Total 14792 12437 12167 -271 11810 98% 103%
Elective Med 530 434 598 165 458 138% 131%
SubSpec 1588 1308 1305 -3 1324 100% 99%
Surg 4343 3615 3293 -323 3414 91% 96%
W C & Y 870 725 716 -9 767 99% 93%
Elective Total 7331 6082 5912 -170 5963 97% 99%
Grand Total 22122 18519 18079 -440 17772 98% 102%
Variance Year to Date

Chief Executive’s Report 6-18
ESPIs – 4 months
3.9 Theatre Cancellations Current theatre cancellations for April have reduced back to 41 (31 for Nelson and 10
in Wairau). Year-to-date there has been 388 cancellations (321 in Nelson and 67 in Wairau). Cancellations reduced back from high in February, however they remain of concern in Nelson.

Chief Executive’s Report 6-19

Chief Executive’s Report 6-20
3.10 Enhanced Access to Diagnostics Good progress continues to be made on both CT and MRI waiting times. A small rise
occurred for CTs in April, however we expect this to peg back moving forward.
3.11 Improving Diagnostic Waiting Times – Colonoscopy Substantial achievement continues in the colonoscopy waiting times.
3.12 Outpatient – First Specialist Assessments The cardiology FSA numbers have now been corrected in the year to date results.
However the comparison to last years actual are now meaningless. This will self correct as we move into the new year.
0
100
200
300
400
Diagnostic Reporting Template - CT (DHB wide) Total Number accepted referrals
waiting outside 6 weeks (excluding referrals for scans that are planned patient
events)
0
100
200
300
400
500
Diagnostic Reporting Template - MRI Total Number accepted referrals
waiting outside 6 weeks (excluding referrals for scans that are planned
patient events)
0
20
40
60
80
100
120
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Diagnostic Reporting Template - CTCTotal number accepted referrals waiting outside 6 weeks (excluding referrals for scans that are planned patient events
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Urgent Diagnostic Colonoscopy
Actual % treated < 14 days Target % treated < 14 days
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Non Urgent Diagnostic Colonoscopy
Actual % treated < 42 days Target % treated < 42 days
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Surveillance Colonoscopy
Actual % treated < 84 days Target % treated < 84 days

Chief Executive’s Report 6-21
3.13 Oral Health
Arrears are at 16%, with DNA rates at 8% (representing 209 appointments)
DNA rates appear higher at Blenheim and Nelson hubs. The reason for this is being investigated
We are reviewing mobiles as arrears climb, which may require a return to two chair staffing for a period of time
We are maintaining minimum requirement for each therapist to undertake seven examinations per day plus treatment appointments
The number of children <5yrs enrolled is 6,469 with the target for this year being 7,242.
There are a number of initiatives which are progressing in this service including:
“First Smiles” baby appointments programme in Marlborough progressing really well – led by Blenheim based educator
Primary schools “Breakfast Club” underway at four primary schools in Nelson Region (Tahunanui, Stoke, Victory and Parklands) – Led by Nelson based COHS Educator
Ready to consult on new COHS leadership structure – awaiting guidance on appropriateness/timing going forward
Developing an Oral Health Education focus (along with adolescent service) for 2016 – “Water is Best”.
Outpatient Attendances
First Specialist Assessments
NMDHBApril 2016
Service Unit Code Description Annual Plan Budget YTD Actual YTDVol
Variance
Act %
Complete
vs YTD Plan
Last FY-
YTD
Actual
Medical M00002 General Medicine - 1st attendance 1530 1252 1016 -236 81% 1143
M10002 Cardiology - 1st attendance 1100 900 657 -243 73% 1892
M15002 Dermatology - 1st attendance 340 283 228 -55 80% 236
M20004 Diabetes - 1st attendance 120 98 86 -12 87% 91
M25002 Gastroenterology - 1st attendance 1000 818 814 -4 99% 721
M30002 Haematology - 1st attendance 130 106 86 -20 81% 85
M40002 Infectious Diseases - 1st attendance 40 33 37 4 113% 24
M45002 Neurology - 1st attendance 400 327 256 -71 78% 226
M50020 Oncology - 1st attendance 450 368 320 -48 87% 314
M50022 Radiation Oncology - 1st 170 139 134 -5 96% 149
M60002 Renal Medicine - 1st attendance 55 45 23 -22 51% 42
M65002 Respiratory - 1st attendance 290 237 161 -76 68% 209
M70002 Rheumatology (incl immunology) - 1st att 280 229 304 75 133% 219
Medical Total 5905 4837 4122 -715 85% 5351
SubSpec S25002 Ear Nose and Throat - 1st attendance 1300 1061 1383 322 130% 1254
S40002 Ophthalmology - 1st attendance 1800 1483 1481 -2 100% 1223
S70002 Urology - 1st attendance 1300 1081 1156 75 107% 1113
SubSpec Total 4400 3625 4020 395 111% 3590
Surgical S00002 General Surgery - 1st attendance 3000 2484 2406 -78 97% 2104
S45002 Orthopaedics - 1st attendance 2150 1798 1445 -353 80% 2821
S45004 Fracture Clinic - 1st attendance 1850 1548 1934 386 125% 0
S75002 Vascular Surgery 1st Attendance 280 230 102 -128 44% 170
Surgical Total 7280 6060 5887 -173 97% 5095
W C & Y M55002 Paediatric Medical Outpatient - 1st at 975 798 765 -33 96% 641
S30002 Gynaecology - 1st attendance 1450 1211 1257 46 104% 992
W03002 1st obstetric consults 720 607 668 61 110% 636
W C & Y Total 3145 2616 2690 74 103% 2269
Grand Total 20730 17139 16719 -420 98% 16305

Chief Executive’s Report 6-22
3.14 Specials & Watches Specials and watches continue to be a concern as the level equates to significant
unplanned resources.
2016 TCR Arrears % PSR
April
Nelson 3924 528 13 % 1348
Stoke 2945 473 16 % 977
Richmond 3514 388 11 % 875
Motueka 1693 281 17 % 542
Tasman Mobile 2031 175 9 % 564
Blenheim 4692 1109 24 % 1610
Mobile 1775 368 21 % 553
Totals 20574 3322 16 % 6469
April 2016 Treatment Visits DNAs
Pre School Total
Nelson 51 291 342 58 17 %
Stoke 98 334 432 34 8 %
Richmond 108 483 591 22 4 %
Motueka 31 132 163 14 9 %
Tasman Mobile 31 143 174 2 1 %
Blenheim 163 420 583 54 9 %
Marlborough Mobile 48 172 220 25 11 %
Total 530 1975 2505 209 8 %

Chief Executive’s Report 6-23
3.15 Faster Cancer Treatment – Oncology Overall achievement in FCT is positive, however the third quarter is somewhat lower
than the previous quarter. This has been significantly impacted by the Christmas / New Year period. It is expected that this will continue to improve.
3.16 Allied Health Services Increasing concern is being highlighted on the increase in the number of patients
waiting for allied health services. The number of patients waiting on the allied health waiting lists has progressively been increasing since early 2015.
There are specific actions within each Allied Health discipline, however at this stage
the confidence of the effectiveness of the actions planned has not been tested. This will be undertaken over the next month as having a significant number of patients waiting greater than 6 months is not good practice and improvements must be delivered.
0
500
1000
1500
2000
2500
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Specials & Watches (Med / Surg / AT&R)
Nelson Wairau
0
1000
2000
3000
4000
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Specials & Watches Mental Health & Alex
MHAU Alex
FCT Monthly Report - April 2015 Reporting Month: March 2016 - Quarter 3 2015-2016
As at 21/04/2016
62 Day Indicator Records
TARGET SUMMARY
Within 62 Days Exceeded 62 Days Within 62 Days Exceeded 62 Days Within 62 Days Exceeded 62 Days Within 62 Days Exceeded 62 Days Within 62 Days Exceeded 62 Days
80% 20% 82% 18% 60% 67% 80% 20% 76% 24%
Number of Records 8 2 23 5 12 8 8 2 163 52
Total Number of Records 10 28 20 10 215
83 82 75 83 84
Within 62 Days Exceeded 62 Days Within 62 Days Exceeded 62 Days
1 69% 31% 56% 44%
46 21 141 109
67 250
82 108
YEAR TO DATE
Tumour Stream % Within 62 Days
Within
62 Days
% Exceeded
62 Days Exceeded 62 Days
Total
Records Column1 Ethnicity Column2 % Within 62 Days
Within
62 Days
% Exceeded
62 DaysExceeded 62
Days
Total
Records
Brain/CNS #DIV/0! 0 #DIV/0! 0 0 European not further defined 57% 4 43% 3 7
Breast 97% 63 3% 2 65 Latin American /Hispanic 100% 1 0% 0 1
Gynaecological 94% 16 6% 1 17 not stated #DIV/0! 0 #DIV/0! 0 0
Haematological 86% 12 14% 2 14 NZ European 76% 136 24% 44 180
Head & Neck 44% 8 56% 10 18 NZ Maori 73% 8 27% 3 11
Lower Gastrointestinal 67% 10 33% 5 15 Other Asian 100% 1 0% 0 1
Lung 61% 14 39% 9 23 Other Ethnicity 100% 2 0% 0 2
Other 100% 1 0% 0 1 Other European 80% 8 20% 2 10
Sarcoma 0% 0 100% 2 2 response unidentifiable 100% 1 0% 0 1
Skin 94% 15 6% 1 16 Southeast Asian 100% 1 0% 0 1
Upper Gastrointestinal 86% 12 14% 2 14 Tongan 100% 1 0% 0 1
Urological 40% 12 60% 18 30 Grand Total 76% 163 24% 52 215
Blank #DIV/0! 0 #DIV/0! 0 0
All Streams 76% 163 24% 52 215
85% of patients had their 1st
treatment within: # days
Quarter 3 Previous Year
Completed Records
62 Day Indicator Records
Apr -2016
(in progress)Mar-16 Feb-16
Quarter 4
(in progress)Year to Date

Chief Executive’s Report 6-24
3.17 Service User Compliments and Complaints NMDHB received a total of 27 compliments in April, and 39 complaints. This
compares to 41 complaints in March (of which there was a 95% response rate within 20 working days).

Chief Executive’s Report 6-25
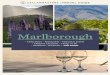
3.18 Official Information Act Requests Fifteen OIA requests were received for response during the month of April 2016. Of
the 15 requests, one was transferred (a partial transfer to the Ministry of Health and a partial transfer to TAS) as the information requested was believed to be more closely connected with the functions of MOH and TAS, and one was withdrawn by the requestor.
Of the 13 remaining OIA requests, all were responded to within the 20 day statutory
timeframe. This is a 100% response rate in line with the first three months of 2016, and up from 86% for December.
One of the 15 responses was a Notice of the Decision on the Request where
NMDHB had reached a decision to grant the request under section 15(1)(b) of the Act, that it would take us some time to prepare the information for release; that the information requested would be made available without undue delay; that an estimated timeframe for release would be an additional two working days following the original 20 working day time period after receiving the request, and the right to seek a review of the decision under section 28.
The 2014/2015/2016 financial year, year to date OIA requests received and response
timeframes are detailed in the following graph:
3.19 Human Resources 3.19.1 Performance Appraisals
Performance appraisal results continue to increase. We are now at 67.9% which represents 1,697 staff with current performance appraisals. The same time last year we were at 45.5% or 1,114 staff. This is a significant achievement, however we are still well short of the 90% target.
16
6
10
7
5
3
5
12
29
9
11
13
19
14
18
26
28
14
10
17
5
15
0
5
10
15
20
25
30
35
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
Nu
mb
er
of
OIA
Re
qu
est
s
% Answered in 20 days % Target # of OIAs

Chief Executive’s Report 6-26

Chief Executive’s Report 6-27
3.19.2 Management and Administration FTE Cap
Cap
April 2016
Variance
Established 371 355 16
Surrendered to support DHBSS priorities 2012/13
3 (3)
Surrendered to support SIAPO 2013/14 1 (1)
PICS Unit 8 (8)
TOTALS 359 355 4

Chief Executive’s Report 6-28
3.20 NMDHB At A Glance The NMDHB at a Glance for April is attached as agenda item 6.2.
Chris Fleming CHIEF EXECUTIVE RECOMMENDATION: THAT THE CHIEF EXECUTIVE’S REPORT BE RECEIVED.