Embed Size (px)
Citation preview

1
ReseaRch aRticle
Neoskin development in the fetus with the use of a three-layer graft: an animal model for in utero closure of large skin defects
Denise araújo lapa Pedreira1, Ruben a. Quintero2, Gregório lorenzo acácio3, elia tamaso espin Garcia caldini4, Paulo hilário Nascimento saldiva5
1Maternal-fetal specialist, Pathology Department, Faculty of Medicine, University of São Paulo (USP), São Paulo, Brazil, 2Maternal Fetal specialist, Obstetrics and Gynecology Department, University of Miami, Miami, Florida, USA, 3Maternal-fetal specialist, Obstetrics and Gynecology Department, University of Taubaté (UNITAU), Taubaté, Brazil, 4Pathologist, Professor of Pathology Department, Faculty of Medicine, University of São Paulo (USP), São Paulo, Brazil, 5Pathologist, Chairman of Pathology Department, Faculty of Medicine, University of São Paulo (USP), São Paulo, Brazil
The Journal of Maternal-Fetal and Neonatal Medicine
2011
00
00
000
000
© 2011 Informa UK, Ltd.
10.3109/14767058.2011.564486
1476-7058
1476-4954
The Journal of Maternal-Fetal and Neonatal Medicine, 2011, 1-6, Early OnlineCopyright © 2011 Informa UK, Ltd.ISSN 1476-7058 print/ISSN 1476-4954 onlineDOI: 10.3109/14767058.2011.564486
Address for Correspondence: Denise Araujo Lapa Pedreira, Rua Coronel Lisboa, 395 ap 11A, 04020-040 São Paulo, SP Brazil. Phone: (55 11) 8473-1574, Fax: (55 11) 5572-2033. E-mail: [email protected]
Objective: To assess the ability of a three-layer graft in the closuse of large fetal skin defects. Methods: Ovine fetuses under-went a large (4 × 3 cm) full-thickness skin defect over the lumbar region at 105 days’ gestation (term = 140 days). A bilaminar artificial skin was placed over a cellulose interface to cover the defect (3-layer graft). The skin was partially reapproximated with a continuous nylon suture. Pregnancy was allowed to continue and the surgical site was submitted to histopathological analysis at different post-operative intervals. Results: Seven fetuses underwent surgery. One maternal/fetal death occurred, and the remaining 6 fetuses were analyzed. Artificial skin adherence to the wound edges was observed in cases that remained in utero for at least 15 days. Neoskin was present beneath the silicone layer of the bilaminar artificial skin. Conclusions: Our study shows that neoskin can develop in the fetus using a 3-layer graft, including epidermal growth beneath the silicone layer of the bilaminar skin graft. These findings suggest that the fetus is able to reepithelialise even large skin defects. Further experience is necessary to assess the quality of this repair.
Keywords: Skin, artificial, fetal therapies, wound healing, sheep, disease models, animal, ultrasonography, prenatal video-assisted surgery, meningomyelocele
IntroductionOpen spina bifida (OSB) is a severe condition affecting 1.90 per 10,000 live births in the US [1]. In Brazil, open neural tube defects occur in 4.2 per 1000 live births, of which 47.2% represent OSB [2], which is approximately 8 times higher than the incidence in the US. Counseling of patients involves either expectant management or termination or pregnancy where this is avail-able. In utero correction of the defect via open fetal surgery was investigated in a randomized clinical trial in the United States (Management of Myelomeningocele Study, or MOMS trial) and concluded that prenatal correction is good for the fetus, but risky for the mother.
We have previously shown that OSB can be treated in utero with a cellulose patch [5] that induces the formation of a neo-dura
mater when placed above the defect in the ovine model [6]. In this model, the skin is closed over the cellulose patch. This assumes that the defect is small enough to allow primary closure of the skin.
“Large” meningomyeloceles are defined as defects where a tension-free skin closure is not possible by simple undermining of the skin edges. In the neonatal period, this usually occurs when the defect is larger than 5.0–6.0 cm [7]. In a study on the prenatal correction of MMC in human fetuses, large defects were reported in 23.2% 13 out of 56 of cases [8]. For such defects, a bipendic-ular flap closure technique (9) has been proposed. However, the results were suboptimal. Treatment of such a large defect using only our previously described cellulose graft would be ineffective. The purpose of our study was to assess an alternative grafting technique for cases with large skin defects.
Materials and methodsMixed-breed, Hampshire ewes were acclimatised for 7 days prior to surgery. The mean gestational age at surgery was 105 days (range: 94–114 days; term = 140 days). Before surgery, the animals were submitted to a 48-h food and 24-h fluid fast. While still in the pen, pre-anaesthetic medication was administered (0.2–0.4 mg/kg of 1% acepromazine and 0.3–0.5 mg/kg of midazolam, IV). The animals were then taken to the operating room under seda-tion. Anaesthesia was supplemented by intravenous thiopental (7.5–10.0 mg/kg) followed by endotracheal intubation and was maintained with 2% isofluorane. A single dose of intravenous enrofloxacin (5.0 mg/kg) was given for antibiotic prophylaxis. Maternal vital signs parameters were controlled by the veterinary in charge of the anaesthesia and post-operative period.
A left para-midline incision was performed, followed by uterine exteriorisation, myometrial incision and fetal partial exposure. A 4.0 × 3.0 cm full-thickness segment of skin was removed from the back of the fetus at the level of the lumbar spine.
The skin defect was then repaired endoscopically under gasless fetoscopy [9]. Briefly, three modified laparoscopic cannulas, one 5.0 mm (Edlo, Brazil) and two 3.5 mm (Stryker, USA), were inserted in the uterine cavity after placement of a secure suture around each trocar site. One hundred cc of amniotic fluid were
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 20
1.81
.74.
163
on 0
8/17
/11
For
pers
onal
use
onl
y.

2 D.A.L. Pedreira et al.
The Journal of Maternal-Fetal and Neonatal Medicine
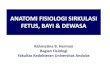
removed to create a “dry” space inside the amniotic cavity. This fluid was stored at body temperature. The uterine wall was suspended using a helicoidal device. Surgery was performed using a 4.0 mm 30 degree angle view endoscope (27005 BA, Karl Storz, HStrattner, Brazil).and standard 3.0 mm laparoscopic surgery instruments (Stryker, São Paulo, Brazil). A 3.0 × 1.5 cm piece of biosynthetic cellulose (Bionext®, Bionext, São Paulo, Brazil) was placed over the defect (Figure 1B) and the bilaminar artificial skin (Integra®, Promedon, São Paulo, Brazil) measuring 3.0 × 2.0 cm, was placed over the cellulose (Figure 1C).
The artificial skin is a bilaminar membrane system consisting of a porous coprecipitate of bovine tendon type I collagen and shark glycosaminoglycan (chondroitin-6-sulfate) covered by a temporary epidermal substitute made of silicone. The biosynthetic or microbial cellulose is a bacterial derived product designed as a temporary skin substitute initially developed for use in small burns. The artificial skin was chosen to isolate the underlying cellulose matrix from the amniotic cavity.
The skin edges were partially approximated with a continuous running suture of monofilamentous 4-0 nylon (Figure 1D)
without incorporating the grafting material. The amniotic fluid was restored and the uterus and abdomen were closed in layers. The ewes were returned to their pen after recovery from anaes-thesia. No additional medication was administered in the post operative period. Behavioral habits were monitored twice a day by a veterinarian. The presence of vaginal bleeding or discharge, and signs of labor were recorded.
Near term, at 135 days ( term = 140 days) ewes were eutha-nized with an overdose of thiopenthal and KCl, except for those cases were spontaneous preterm labor/delivery occurred. Fetuses were harvested, weighed, photographed and fixed in 10% form-aldehyde for 7 days. Three transverse sections (cranial, medial and caudal) of the defect were made and were decalcified with **EDTA. Representative slides stained with haematoxylin & eosin were reviewed independently by two pathologists (PHNS and EC). Picrosirius-stained sections were analyzed with polarization microscopy to study the structural organization of collagenous fibers. The study was approved by the Institutional Research Ethics Committee of the Albert Einstein Hospital in Sao Paulo, Brazil.
Figure 1. Defect’s closure at 100 days of gestation. (A) External view of the exposed uterus, note the suspension device and the three cannulas (C). (B) Fetoscopic image of the biosynthetic cellulose (BC) being placed over the defect (D), marked by the dotted line. (C) The artificial skin (AS) is placed over the cellulose. (D) External view of the continuous running suture (arrows), a “gap” is seen where the skin edges (dotted white line) could not be re-approximated.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 20
1.81
.74.
163
on 0
8/17
/11
For
pers
onal
use
onl
y.

Neosokin in the fetus 3
Copyright © 2011 Informa UK, Ltd.
ResultsSeven ewes underwent surgery. One maternal/fetal death occurred 20 h after the procedure (case 6). This case was excluded from further analysis. Preterm delivery occurred in four cases 3, 4, 15, and 25 days after surgery. All preterm deliveries occurred overnight without any warning signs. Two fetuses remained in utero until near term, when they were harvested according to the protocol at 130 and 135 days of gestation. The average postopera-tive intrauterine stay was 17.2 days (Table 1). All 6 fetuses were studied.
Macroscopic findings
The continuous running stitch was in place in all cases. The artifi-cial skin and cellulose were present and held in place by the suture in all but one fetus (Figure 2). In the three cases that remained for at least 15 days after surgery, the scar/wound size was of the same shape and size as the artificial skin, with obvious adherence to the surrounding skin. There was no tension on the suture. Some small areas of silicone detachment, starting from the outer edges and going towards the centre of the defect (Figure 2) were observed.
Microscopic findings
Of the 6 cases submitted for microscopic analysis, 2 were excluded. In one case, neither the artificial skin, nor the cellulose were
present over the lesion (case 3); and in another case, because signs of mild wound infection were present (case 4). Stages of dermal matrix repopulation were assessed after 3, 21, 25, and 35 days of surgery (Table 1). The repopulation of the dermal matrix16 was assessed as follows.
The imbibition phase, which consists of filling of the inter-stices with exudates, which fosters adherence of the matrix to the wound, was observed as early as 3 days post-op (case 5) (Figure 3A). Migration, neovascularisation, and remodelling/maturation (16), were observed in the remaining three cases and were characterized by endothelial cell migration and fibroblast matrix repopulation (Figure 5B).
A newly formed epidermis grew beneath the silicone layer, starting from both edges of the former epidermis (Figure 4A). New dermal components where observed, growing toward the top of the artificial skin dermal matrix (Figure 4B–E) supporting the new epidermis. The new skin lacked adnexal structures. The entire gap between the edges of the defect was closed by new skin in specimens remaining until term (Figure 5A). In none of the specimens, the new epidermis was observed to grow directly over the artificial skin dermal matrix (Figure 4C and E); instead, the artificial matrix served as a scaffold over which the new dermal component could grow. The new dermis itself, characterised by new fibroblasts, myofibroblasts and organised formed collagen (Figure 4B–E), was observed to serve as a “bridge” for the growth of the new epidermal cells.
Table 1 . Gestational length after surgery and pregnancy outcome details
Case GA (days)
Average fetoscopy
time (min)Pregnancy outcome
Pregnancy length (days)
Postoperative intrauterine stay (days)
1 102 - PD 127 252 94 - S 130 353 100 90 PD 104 4*4 108 120 PD 123 15†5 106 120 PD 109 36 112 100 MD - -7 114 60 S 135 21
Average 105.1 98 - 121.3 17.2GA = gestational age at surgery, MD = maternal death, PD = premature delivery,
S = sacrifice*No Integra or Bionext found, †Local infection.
Figure 2. Surgery site at harvesting on the 135th day of gestation (case 7). The artificial skin is held in place by the suture (white arrows) and some small areas of silicone detachment (black arrows) are apparent. These detachment areas appear to start from the outside beginning from the outside edges and moving towards the centre of the defect.
Figure 3. Pathological examination of the defect after three days in utero. (A) (PSP 10x) Note the imbibition phase of the dermal matrix (DM) re-population: the interstice is filled with fluid, scattered red blood and inflammatory cells can be noted. (B) (H&E 10x) Bellow the dermal matrix, the biosynthetic cellulose (BC) can be seen and the same inflammatory cells are concentrated on its bottom edge.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 20
1.81
.74.
163
on 0
8/17
/11
For
pers
onal
use
onl
y.

4 D.A.L. Pedreira et al.
The Journal of Maternal-Fetal and Neonatal Medicine
DiscussionOur study suggests that large fetal skin defects can be treated with a three-layer grafting technique that includes a basal cellulose layer and a bilaminar artificial skin. Contrary to the experience in adult grafts, the fetus can generate neo dermis and epidermis. The fetal skin can generate epidermis beneath the silicone layer, thus capable of sealing the defect without additional grafting proce-dures. These findings may be useful in the management of large skin lesions, such as those seen in 23.2% of OSB [8].
Meningomyeloceles are considered “large” if the defect is bigger than 5.0–6.0 cm [7] In such cases, primary skin closure may not be possible. To close such large defects, a bipendicular flap technique has been suggested, which consists of performing bilateral relaxing skin incisions. In one series, the lateral incisions were performed in utero [8]. At birth, none of the fesuses showed healing of the relaxing incisions, and the aesthetic results were considered very poor. The authors suggested that alternative tech-niques for prenatal closure should be sought.
Several surgical techniques have been proposed to close large meningomyeloceles after birth, including skin incisions, flap advancements, latissimus dorsi V-Y flaps, and gluteus maximus flaps [7]. Because such techniques may be associated with signifi-cant morbidity, including flap-related complications, the develop-ment of simpler and faster techniques have been suggested [10]. In the newborn period, Cole et al. [11] report a case where a
purse-string suture was used to approximate the skin edges and a pigskin sheet was used to cover the central remaining skin defect. Danish et al. [12] reported two cases in which a human acelular dermal matrix was sutured directly to the skin edges. Grigoryants et al. [13] report one case of use a dural substitute in association with a dermal matrix and Nakasawa et al. [14] used a temporary artificial dermis, in two other cases. In the prenatal period, only two skin substitutes have been used so far, the acellular dermal matrix [15,16] and the association of an absorbable patch covered with a nonabsorbent polytetrafluoroethylene patch [17]. The bilaminar artificial skin used in our study has not being used in humans fetuses.
The artificial skin we used was originally developed for large burns, but is increasingly being used in post-burn and other reconstructive surgeries [19]. In adults, surgical application of artificial skin requires its suture to the adjacent native skin. After 4 weeks, the silicone layer is surgically removed and an epidermal skin graft is placed over the “mature” exposed dermis. Our study showed that the fetus is not only capable of repopulating the arti-ficial dermal matrix, but can also induce the generation of a new dermis and epidermis as well [19]. Therefore, fetal healing may obviate steps typically seen or required in adult healing a finding not previously reported.
Studiyng the artificial skin in adults, Moiemen et al. described four stages of dermal regeneration: imbibition, fibroblast
Figure 4. Pathological examination of the defect after 21 days in utero. (A) (PSP no magnification) Actual pathological specimen. (B) (PSP 2,5x) The newly formed dermis (ND) and epidermis (NE) growing towards the top of dermal matrix (DM), the transition is marked by the dotted curved line. (C) Magnification (10x) same field using polarization, the new fetal collagen can be seen in a more organised pattern (white arrows). The new epidermis stops exactly at the edge of the dermal matrix (arrow). (D) (PSP 2,5x) and (E) polarization 2,5x.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 20
1.81
.74.
163
on 0
8/17
/11
For
pers
onal
use
onl
y.

Neosokin in the fetus 5
Copyright © 2011 Informa UK, Ltd.
migration, neovascularisation, and remodelling/maturation [19]. Our study showed a similar sequence of events in the repopula-tion of artificial dermis in the fetus. Furthermore, we observed hyperkeratosis over the neo formed epidermis. We believe this may be the result of the chronic friction of the silicone layer onto the new epithelium.
The sheep has been established as an animal model for the study of prenatal correction of spina bifida since 1995 [20]. We recently reviewed the literature [20, 21, 22, 23, 24, 25, 26, 27, 28] concerning materials and techniques for the prenatal MMC closure in fetal sheep, and also reported our results using a simpli-fied technique [5,29]. Our experience suggests that the use of “interface materials” over the placode is essential to avoid adhe-sion of the medulla to the skin scar. This is aimed at preventing the tethering of the cord. However, the ideal material to prevent this complication has not been established. In a previous study [6], we compared the performance of biosynthetic cellulose to the acellular dermal matrix, and found the cellulose to be a better choice. The biosynthetic cellulose not only avoided adhesion, but also induced formation of a neo-dura mater layer over the neural placode, both highly desired effects. The same neo-dura mater formation effect was found by Mello et al. [30] studying the biosynthetic cellulose as a dural substitute after craniotomy in dogs.
Biosynthetic cellulose, also known as microbial cellulose, is a biological product derived from bacterial production and initially developed as a skin substitute for burn patients. The material was approved by the United States Food and Drug Administration (FDA) in 1995. Biosynthetic celllulose is relatively impermeable to water. We were concerned that this feature could impair the dermal repopulation, as cell migration to AS is expected to start at the bottom and progress to the top of the dermal component [19].
Our study showed more cells on the edges rather than in the centre of the defect, but this did not appear to compromise the AS function as skin substitute, also this can possibly be overcome by a longer intrauterine staying period of time.
In summary, our study showed a re-epithelialisation process of the artificial skin not previously seen in adults. The mechanisms responsible for this different behaviour of the artificial skin in the fetus compared to the adult is poorly known, though recent evidence suggests that variations in differentiated inflamma-tory cells in embryonic wounds may play a significant role [31]. Artificial skin has all the important characteristics required for a skin substitute in the correction of fetal MMC: remarkable adher-ence, impermeability and induction of the new skin formation. Our findings support the possibility that the new skin could cover the entire defect, provided that the fetus remains enough time in utero. This would render the use of post-natal skin grafting unnecessary. Future studies should address both the biological mechanisms involved in the phenomena observed as well as the development of clinically-applicable miniamally-invasive tech-niques for use in humans.
AcknowledgmentsWe would like to thank Rogério Chaccur Abou-Jamra (in memo-riam) and Rita de Cássia Sanchez e Oliveira, for their collaboration in the surgeries. I would also like to thank Erica Stein Ciasca Stein and Silvia Rejane Fontoura Herrera, M.D. for their collaboration in the elaboration of the manuscript. The Albert Einstein Teaching and Research Institute Ethics Committee− São Paulo− Brazil (Instituto de Ensino e Pesquisa da Sociedade Beneficente Israelita Albert Einstein) approved the study (CEUA/Einstein: number 245-07 on 17 May 2007). This study was funded by a grant from
Figure 5. Pathological examination of the defect after 35 days in utero. At the caudal end of the defect, complete re-epithelialisation occurred. (A) (HE 2,5x) Transition of the original fetal skin (FS) to the new skin (ND+NE). Adnexal structures are absent in the new one, the original fetal skin (FS) is full of hair follicles (HF). Hyperkeratosis (H) occurred below the place where the silicone was present. (B) (HE 10x) The new dermis (ND) covers the entire dermal matrix (DM). (C) Using polarization (2.5x), the transition is more evident (arrows), the dermal matrix collagen is “brighter” then the newly synthesised one.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 20
1.81
.74.
163
on 0
8/17
/11
For
pers
onal
use
onl
y.

6 D.A.L. Pedreira et al.
The Journal of Maternal-Fetal and Neonatal Medicine
Instituto de Ensino e Pesquisa da Sociedade Beneficente Israelita Albert Einstein− São Paulo− SP− Brazil.
Disclosure of interestThe Promedon, a Latin American sales company for Integra (Plainsboro, USA), provided, without charges (donated), the Integra® (artificial skin) used in the present study. No other conflict of interest, including shares, employment, reimburse-ment for attending a meeting, fees for speaking, and funds for a member of staff, research consulting and organising education, was obtained from this or any other companies. The authors declare no conflict of interest and are solely responsible for the content of their paper.
References1. MMWR. Morb Mortal Wkly Rep 2009;9:1409–13.2. Aguiar MJ, Campos AS, Aguiar RA, Lana AM, Magalhães RL, Babeto
LT. [Neural tube defects and associated factors in liveborn and stillborn infants]. J Pediatr (Rio J) 2003;79:129–134.
3. Adzick NS, Thom EA, Spong CY, Brock JW 3rd, Burrows PK, Johnson MP, Howell LJ, Farrell JA, Dabrowiak ME, Sutton LN, Gupta N, Tulipan NB, D’Alton ME, Farmer DL; MOMS Investigators. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med 2011;364:993-1004.
4. Sutton LN. Fetal surgery for neural tube defects. Best Pract Res Clin Obstet Gynaecol 2008;22:175–188.
5. Abou-Jamra RC, Valente PR, Araújo A, Sanchez e Oliveira Rde C, Saldiva PH, Pedreira DA. Simplified correction of a meningomyelocele-like defect in the ovine fetus. Acta Cir Bras 2009;24:239–244.
6. Oliveira RCS, Valente PR, Abou-Jamra RC, Araújo A, Saldiva PH, Pedreira DAL. Comparison of two interface materials for the in utero repair of fetal meningomielocele in sheep model. Acta Cir Bras 2007;22:174–181.
7. Ozçelik D, Yildiz KH, Is M, Dösoglu M. Soft tissue closure and plastic surgical aspects of large dorsal myelomeningocele defects (review of techniques). Neurosurg Rev 2005;28:218–225.
8. Mangels KJ, Tulipan N, Bruner JP, Nickolaus D. Use of bipedicular advancement flaps for intrauterine closure of myeloschisis. Pediatr Neurosurg 2000;32:52–56.
9. Pedreira DA, Oliveira RC, Valente PR, Abou-Jamra RC, Araújo A, Saldiva PH. Gasless fetoscopy: a new approach to endoscopic closure of a lumbar skin defect in fetal sheep. Fetal Diagn Ther 2008;23:293–298.
10. Yannas IV, Burke JF. Design of an artificial skin. I. Basic design principles. J Biomed Mater Res 1980;14:65–81.
11. Cole P, Armenta A, Dauser R, Hollier L Jr. Simplifying soft tissue closure of the large meningomyelocele defect: a technical note. J Plast Reconstr Aesthet Surg 2008;61:192–194.
12. Danish SF, Samdani AF, Storm PB, Sutton L. Use of allogeneic skin graft for the closure of large meningomyeloceles: technical case report. Neurosurgery 2006;58:ONS–E376; discussion ONS.
13. Grigoryants V, Jane JA Jr, Lin KY. Salvage of a complicated myelomeningocele using collagen (Duragen) and dermal (Alloderm) matrix substitutes. Case report and review of the literature. Pediatr Neurosurg 2007;43:512–515.
14. Nakazawa H, Kikuchi Y, Honda T, Isago T, Nozaki M. Successful management of a small infant born with a large meningomyelocele using a temporary artificial dermis. Scand J Plast Reconstr Surg Hand Surg 2005;39:53–56.
15. Sutton LN, Adzick NS, Bilaniuk LT, Johnson MP, Crombleholme TM, Flake AW. F etal Surgery for Myelomeningocele: Improvement in Hindbrain Herniation Demonstrated by Serial Fetal Magnetic Resonance Imaging Following. JAMA 1999;282:1826–1831.
16. Danzer E, Adzick NS, Rintoul NE, Zarnow DM, Schwartz ES, Melchionni J, Ernst LM, et al. Intradural inclusion cysts following in utero closure of myelomeningocele: clinical implications and follow-up findings. J Neurosurg Pediatr 2008;2:406–413.
17. Kohl T, Tchatcheva K, Weinbach J, Hering R, Kozlowski P, Stressig R, Gembruch U. Partial amniotic carbon dioxide insufflation (PACI) during minimally invasive fetoscopic surgery: early clinical experience in humans. Surg Endosc 2010;24:432–444.
18. Pedreira DA, Valente PR, Abou-Jamra RC, Pelarigo CL, Silva LM, Goldenberg S. Successful fetal surgery for the repair of a ‘myelomeningocele-like’ defect created in the fetal rabbit. Fetal Diagn Ther 2003;18:201–206.
19. Moiemen NS, Vlachou E, Staiano JJ, Thawy Y, Frame JD. Reconstructive surgery with Integra dermal regeneration template: histologic study, clinical evaluation, and current practice. Plast Reconstr Surg 2006;117:160S–174S.
20. Meuli M, Meuli-Simmen C, Yingling CD, Hutchins GM, Hoffman KM, Harrison MR, Adzick NS. Creation of myelomeningocele in utero: a model of functional damage from spinal cord exposure in fetal sheep. J Pediatr Surg 1995;30:1028–32; discussion 1032.
21. Copeland ML, Bruner JP, Richards WO, Sundell HW, Tulipan NB. A model for in utero endoscopic treatment of myelomeningocele. Neurosurgery 1993;33:542–4; discussion 545.
22. Meuli-Simmen C, Meuli M, Hutchins GM, Harrison MR, Buncke HJ, Sullivan KM, Adzick NS. Fetal reconstructive surgery: experimental use of the latissimus dorsi flap to correct myelomeningocele in utero. Plast Reconstr Surg 1995;96:1007–1011.
23. Meuli M, Meuli-Simmen C, Yingling CD, Hutchins GM, Timmel GB, Harrison MR, Adzick NS. In utero repair of experimental myelomeningocele saves neurological function at birth. J Pediatr Surg 1996;31:397–402.
24. Paek BW, Farmer DL, Wilkinson CC, Albanese CT, Peacock W, Harrison MR, Jennings RW. Hindbrain herniation develops in surgically created myelomeningocele but is absent after repair in fetal lambs. Am J Obstet Gynecol 2000;183:1119–1123.
25. Kohl T, Hartlage MG, Kiehitz D, Westphal M, Buller T, Achenbach S, Aryee S, et al. Percutaneous fetoscopic patch coverage of experimental lumbosacral full-thickness skin lesions in sheep. Surg Endosc 2003;17:1218–1223.
26. Bouchard S, Davey MG, Rintoul NE, Walsh DS, Rorke LB, Adzick NS. Correction of hindbrain herniation and anatomy of the vermis after in utero repair of myelomeningocele in sheep. J Pediatr Surg 2003;38:451–8; discussion 451.
27. Yoshizawa J, Sbragia L, Paek BW, Sydorak RM, Yamazaki Y, Harrison MR, Farmer DL. Fetal surgery for repair of myelomeningocele allows normal development of the rectum in sheep. Pediatr Surg Int 2003;19:162–166.
28. Eggink AJ, Roelofs LA, Feitz WF, Wijnen RM, Mullaart RA, Grotenhuis JA, van Kuppevelt TH, et al. In utero repair of an experimental neural tube defect in a chronic sheep model using biomatrices. Fetal Diagn Ther 2005;20:335–340.
29. Pedreira DA. Keeping it simple: a “two-step” approach for the fetoscopic correction of spina bifida. Surg Endosc 2010;24:2640–1; author reply 2642.
30. Mello LR, Feltrin LT, Fontes Neto PT, Ferraz FA. Duraplasty with biosynthetic cellulose: an experimental study. J Neurosurg 1997;86:143–150.
31. Occleston NL, Laverty HG, O’Kane S, Ferguson MW. Prevention and reduction of scarring in the skin by Transforming Growth Factor beta 3 (TGFbeta3): from laboratory discovery to clinical pharmaceutical. J Biomater Sci Polym Ed 2008;19:1047–1063.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 20
1.81
.74.
163
on 0
8/17
/11
For
pers
onal
use
onl
y.