Embed Size (px)
Citation preview

GI Pathology
Neoplasias Quisticas del Páncreas
Gregory Y. Lauwers, M.D.Director, GI Pathology Service
Massachusetts General HospitalHarvard Medical [email protected]
SEAP -Aproximación Práctica a la Patología Gastrointestinal-Madrid, 26 de mayo, 2006

GI Pathology
576 Cystic Tumors of the PancreasMassachuestts General Hospital
1978 - 2005
5% Cystic Islet Cell Tumor
3% Solid Pseudopapillary
Neoplasm
22% Serous Cystadenoma
9% Mucinous
Cystadenocarcinoma
23%Mucinous Cystic
Neoplasm
3% Other
35%Intraductal PapillaryMucinous Neoplasm
Pancreatic Cystic NeoplasmsMGH 1978-2005 (n=576)
*
* lymphangioma, dermoid cyst, cystic acinar cell acrcinoma, epithelial “simple” cyst.

GI Pathology
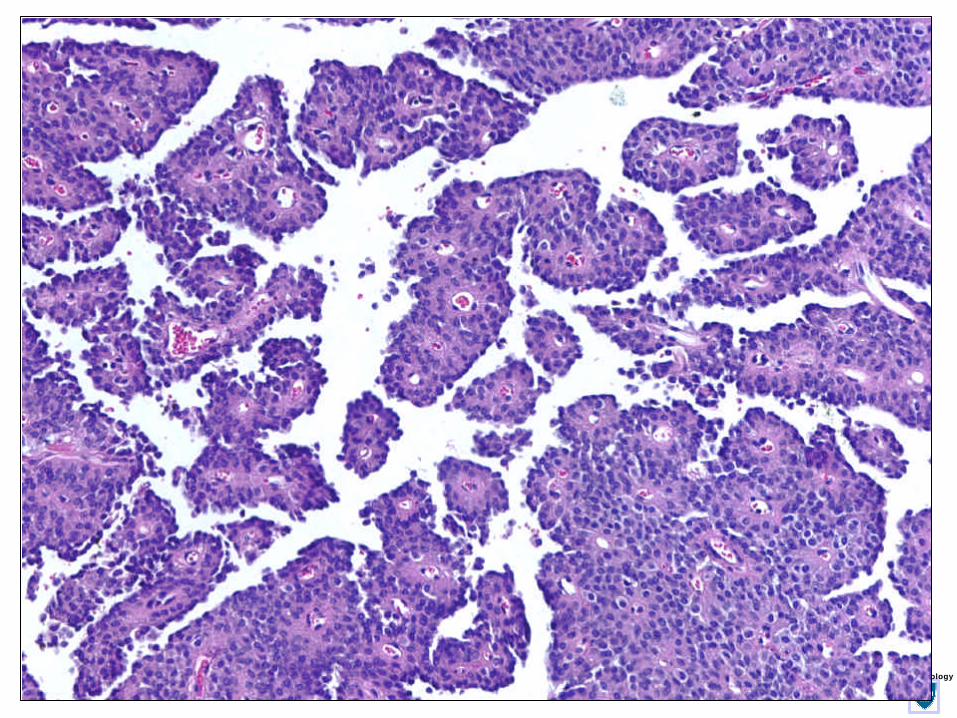
Intraductal Papillary Mucin-Producing Neoplasms (IPMNs)
Intraductal Papillary Mucin-Producing Neoplasms (IPMNs)

GI Pathology
Intraductal Papillary Mucin-Producing Neoplasms (IPMNs)
Intraductal Papillary Mucin-Producing Neoplasms (IPMNs)
• Papillary proliferations of neoplastic mucin secretory cells that arise in the main pancreatic duct or its major branches.
• Median age:6th-7th decade (mean: 68 yrs).
• 1-3% of exocrine pancreatic neoplasms (incidence rate <1 per 100,000)
• Increase in diagnosis parallels the wider use of sophisticated imaging modalities.

GI Pathology

GI Pathology

GI Pathology

GI Pathology
Main Pancreatic Duct
Side Branches

GI Pathology
Side Branch IPMNs

GI Pathology

GI Pathology

GI Pathology
Main+Side Branch (combined) IPMNMain+Side Branch (combined) IPMN

GI Pathology

GI Pathology
Pancreatobiliary
Intestinal
Oncocytic
Gastric

GI Pathology

GI Pathology
MUC2
MUC6
MUC1
MUC5AC

GI Pathology

GI Pathology
MUC5AC
MUC6
MUC1
MUC2

GI Pathology

GI Pathology
MUC5AC
MUC6
MUC1
MUC2

GI Pathology
IPMN, oncocytic variant IPMN, oncocytic variant

GI Pathology
Grading of IPMNsGrading of IPMNsMALIGNANTMALIGNANTBORDERLINEBORDERLINEBENIGNBENIGN
IPMN-AdenomaIPMN-Adenoma IPMN-BorderlineIPMN-Borderline IPMN-Carcinoma(non invasive)
IPMN-Carcinoma(non invasive)

GI Pathology
Ductal adenocarcinoma Colloid adenocarcinoma

GI Pathology

GI Pathology
IPMNs - PrognosisIPMNs - Prognosis
• 5-yr survival rate (60-83%).• Excellent:
–adenoma and borderline tumor–5-year survival ~ 100%, provided that appropriate sampling has eliminated concurrent adenocarcinoma.
• Good for IPMN w/non-invasive carcinoma.

GI Pathology
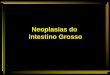
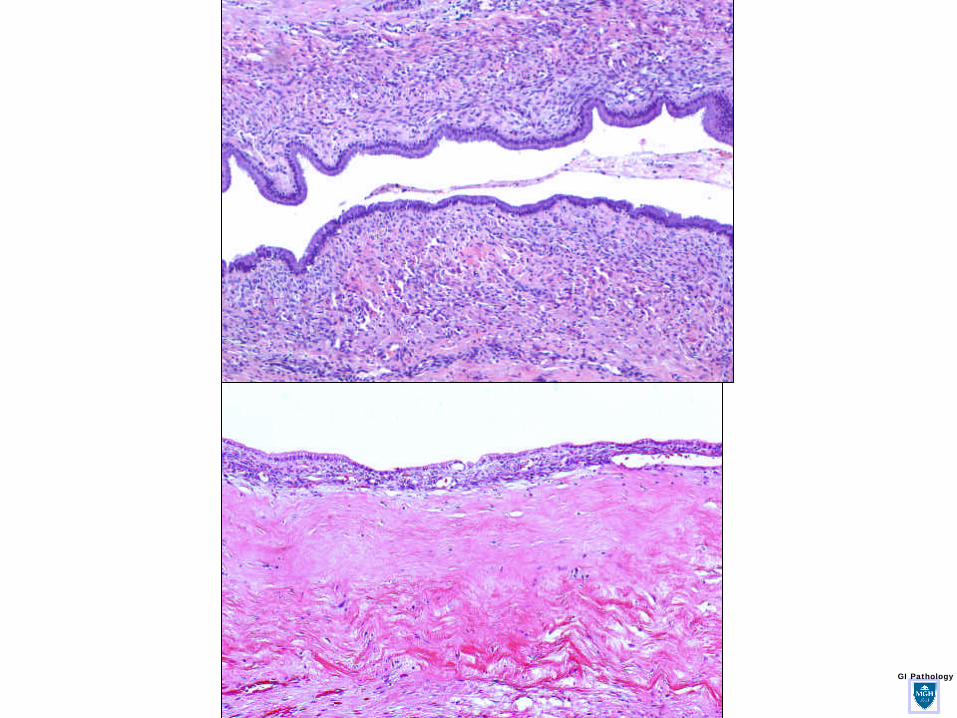
MUCINOUS CYSTIC NEOPLASMMUCINOUS CYSTIC NEOPLASM
GI Pathology

GI Pathology
MUCINOUS CYSTIC NEOPLASMMUCINOUS CYSTIC NEOPLASM
• Exclusively in women (almost).
• No communication w/ ductal system.
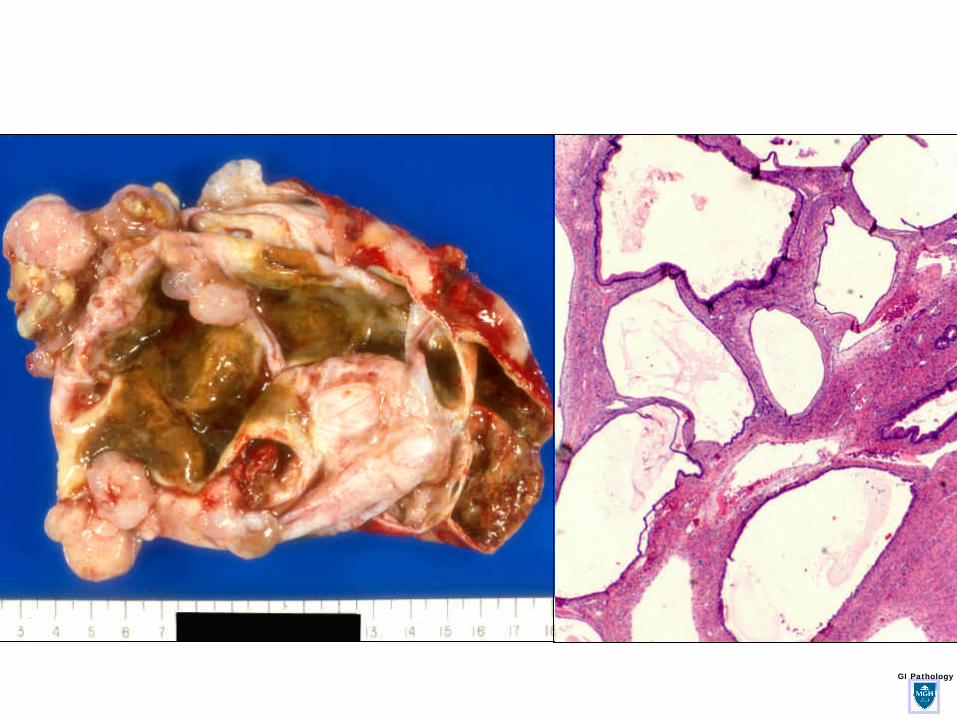
• Columnar mucin-producing epith. supported by ovarian-type stroma.
• 5th decade (range:20- 82)
GI Pathology
Estrogen ReceptorEstrogen Receptor
Progesterone ReceptorProgesterone Receptor
GI Pathology

GI Pathology
MCN-Adenoma
MCN-Adenoma
MCN-BorderlineMCN-Borderline
MCN-Carcinoma(non invasive)
MCN-Carcinoma(non invasive)

GI Pathology

GI Pathology

GI Pathology
Prognosis of MCNs:Prognosis of MCNs:
• Excellent:–Noninvasive lesion
- completely removed- regardless of the degree of cellular atypia.
• Poor:–Inv. Mucinous cystadenocarcinoma
1) correlates w/ amount of invasion of tumor wall and surrounding tissues.
2) lower survival rate if >50 years.

GI Pathology

GI PathologySerous CystadenomaSerous Cystadenoma

GI Pathology

GI Pathology

GI Pathology

GI Pathology
PAS

GI Pathology
Serous CystadenomaSerous Cystadenoma
• Composed of various numbers of cystic structures lined by glycogen-rich cuboidal epithelium.
• Adults, F>>M (70% vs 30%).
• Age: 18-91 yrs old, (median: 7th decade)
• Etiology and pathogenesis unknown. – Asso. w/ Von Hippel-Lindau and chromosomal
alterations (deletion /mutation) of 3p25 found in most cases.

GI Pathology
0
2
4
6
8
10
12
14
16
18
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Years
Max
imu
m D
iam
eter
(cm
)
Median rate of growthfor all tumors (n=24)
= 0.60 cm/year
9/03 4/04
Tseng JF. in press

GI Pathology
Solid Serous CystadenomaSolid Serous Cystadenoma

GI Pathology
Serous cystadenocarcinomaSerous cystadenocarcinoma
• Gastric varices, invasion of stomach and splenic vein, jaundice, and palpable abdominal masses.
• Size:2.5-12 cm.
• Maintain a spongy appearance.
• Deceptive histology.– Mild focal nuclear pleomorphism can be found.– Perineural & vascular invasion, LN mets
reported.
• Slow-growing - prolonged survival.

GI PathologySolid pseudopapillary neoplasm

GI Pathology
GI Pathology

GI Pathology

GI Pathology

GI Pathology
Solid pseudopapillary neoplasm (SPN)"solid and cystic," "papillary cystic," "solid and papillary epithelial” neoplasm.
Solid pseudopapillary neoplasm (SPN)"solid and cystic," "papillary cystic," "solid and papillary epithelial” neoplasm.
• <10% of cystic pancreatic neoplasm.
• Benign - predilection for young women.–Mean age 35 yrs (range 8 to 67).
• Etiology unknown–differences in sex and age point to genetic and hormonal factors

GI Pathology
? Catenin? Catenin
• ? 1-antitrypsin• (chymotrypsin)• VIM• progesterone receptors• (Chromogranin A)• SYN• (CA19.9)• Pan-CK
CD10CD10
CD56CD56

GI Pathology
SPN-PrognosisSPN-Prognosis
• Extremely good.–> 95% cured after complete resection.
–Local spread to peritoneum and hepatic mets, not inconsistent w/ relatively indolent course and long disease-free periods.

GI Pathology
Predictors of poor prognosis– Venous invasion– Nuclear atypia– High mitotic activity– Necrobiotic cell nests– Geographic necrosis– Sarcomatoid
transformation.

GI Pathology
Pancreatic Endocrine NeoplasmsPancreatic Endocrine Neoplasms

GI Pathology
Cystic Pancreatic Adenocarcinoma

GI PathologyAcinar Cystadenocarcinoma

GI Pathology
Similar to solid type. Aggressive neoplasm with a slightly better prognosis than ductal adenocarcinoma
<1%6-7thM>FAcinar cell cystadenocarcinoma
Dismal prognosis, similar to solid adenocarcinoma type.<1%6-7thM?FDuctalAdenocarcinoma with cystic degeneration
Similar to solid neuroendocrine type.<10%5-6thF=MCystic endocrine neoplasm
Indolent neoplasm with rare nodal and extranodal metastases. Excellent prognosis when completely resected.
<10%4thF>>MSPN
Excellent prognosis for lesionsshowing only adenomatous andborderline cytologic atypia. Poor prognosis when invasive carcinoma is present.
21 to 33%6-7thF=MIPMN
Resection is curative regardless of the degree of epithelial dysplasia.Poor prognosis when invasive adenocarcinoma is present.
10 to 45%5thF>>MMucinous cystic neoplasm
Resection is curative. Serous cystadenocarcinoma is rare.
32 to 39%7thF>>MSerous cystadenoma
Malignant potential / Natural history% of Cystic tumorsPeak decades
Gender predilectio
nType
![Neoplasias Introd [Modo de Compatibilidade]files.fisiologica.webnode.com.br/200000087-192bd1a25b/UQM Mod 7.… · 17/03/2011 2 NormalNormal Neoplasia Neoplasia ÓbitoÓbito QQTT Neoplasias](https://img.pdfslide.us/doc/110x75/5bad50aa09d3f2cb568d7a47/neoplasias-introd-modo-de-compatibilidadefiles-mod-7-17032011-2-normalnormal.jpg)