Embed Size (px)
Citation preview

Week 5: Neonatal Neurology Neonatal Neurology: Clinical I Tuesday, July 28 2:30-4:00 pm EDT Moderators Zachary Vesoulis Sonia Bonifacio
EDT Abstract Title Presenting Author
2:30 pm Introduction & General Information
2:35 pm 3380853 Feasibility of ultra-high field Magnetic Resonance Imaging in neonates Kim Annink
2:45 pm 3375265 Association of postnatal heart rate variability with neuroimaging patterns in term neonates with hypoxic ischemic encephalopathy Ipsita Goswami
2:55 pm 3344524
High Blanket Temperature During Therapeutic Hypothermia is Associated with Death or Disability for Infants with Hypoxic Ischemic Encephalopathy John Flibotte
3:05 pm 3381660 Hippocampal Growth in the First Three Months of Life in Term Infants with Neonatal Encephalopathy Ting Guo
3:15 pm 3376854 MRI Score Inter-rater Reliability in Infants with Mild vs Moderate/Severe Hypoxic Ischemic Encephalopathy Michelle Machie
3:25 pm 3373844 Mild Hypoxic Ischemic Encephalopathy (HIE): Brain MRI Findings After Hypothermia Yi Li
3:35 pm 3370612 Treatment Duration and 2-Year Outcome in Neonates with Acute Symptomatic Seizures Hannah Glass
3:45 pm 3380729
Changes in Apparent Diffusion Coefficient Values and Brain Metabolite Levels after Neonatal Hypoxic-Ischemic Encephalopathy Jun Shibasaki
3:55 pm Wrap Up
Note: Schedule subject to change based on presenter availability.

< Return to Abstract Search< Return to Abstrat Search PrintPrint
CONTROL ID: 3380853TITLE: Feasibility of ultra-high field Magnetic Resonance Imaging in neonatesPRESENTER: Kim Annink
AUTHORS (LAST NAME, FIRST NAME): Annink, Kim1; van der Aa, Niek E.1; Dudink, Jeroen1; Alderliesten,Thomas1; Groenendaal, Floris1; Lequin, Maarten2; Jansen, Floor3; Rhebergen, Koenraad4; Luijten, Peter2; Hendrikse,Jeroen2; Hoogduin, Hans2; Huijing, Erik2; Versteeg, Edwin2; Visser, Fredy2; Raaijmakers, Alexander2; Wiegers, Evita2;Klomp, Dennis2; Wijnen, Jannie P.2; Benders, Manon J.1AUTHORS/INSTITUTIONS: K. Annink, N.E. van der Aa, J. Dudink, T. Alderliesten, F. Groenendaal, M.J. Benders, Department of Neonatology, UMC Utrecht Brain Center, University Utrecht, Utrecht, NETHERLANDS;M. Lequin, P. Luijten, J. Hendrikse, H. Hoogduin, E. Huijing, E. Versteeg, F. Visser, A. Raaijmakers, E. Wiegers, D. Klomp, J.P. Wijnen, Department of Radiology, University Medical Center Utrecht, University Utrecht, Utrecht, NETHERLANDS;F. Jansen, Department of Paediatric neurology, UMC Utrecht Brain Center, University Utrecht, Utrecht, NETHERLANDS;K. Rhebergen, Department of Otorhinolaryngology and Head & Neck Surgery, University Medical Center Utrecht, University Utrecht, Utrecht, NETHERLANDS;CURRENT CATEGORY: NeonatologyCURRENT SUBCATEGORY: Neurology: ClinicalKEYWORDS: Ultra-high field imaging, Feasibility, 7 Tesla MRI.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Cerebral MRI in neonates is usually performed with a field strength up to 3.0 Tesla(T). In adults, a growing number of studies have shown added diagnostic value of 7.0T MRI. In some neonates it remains difficult to predict neurocognitive problems, so 7.0T MRI might also be of additional value in neonates.
Objective: The aim of this study is to investigate the feasibility of 7.0T MRI in neonates. We show the first MR images of neonates at 7.0T MRI and provide information about the safety preparations.
Design/Methods: Before starting the clinical study, safety preparations were conducted. Specific Absorption Rate (SAR) levels during 7.0T were simulated in Sim4life using a baby and adult model. Furthermore, in a test set-up, acoustic noise was measured comparing the 3.0T Nordell hood, a newly developed 7.0T hood and no hood to optimize hearing protection during 7.0T MRI. In the prospective pilot study, clinically stable infants, between term (equivalent) age and the (corrected) age of three months, underwent a 7.0T MRI immediately after their standard 3.0T MRI. Vital parameters, temperature and comfort scales were monitored. Temperature was measured continuously during the MRI using a skin probe. 7.0T scan protocols were developed and optimized whilst scanning this cohort.
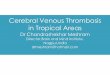
Results: Global and peak SAR levels did not exceed levels in the adult model (Table 1). Hearing protection was guaranteed with the new hood, the 7.0T hood attenuated the acoustic noise by 8.5dB and the 3.0T hood by 7dB. In this pilot study, 12 infants were scanned. No MRI-related adverse events occurred and vital parameters, comfort scales and temperature remained stable. It was feasible to obtain good quality imaging at 7.0T: MRA, MRV, SWI, single-shot T2-weighted images. MRS was of improved quality. For example, the patient shown in Figure 1E+J had an SNR of 19 at 7.0T compared to 6 at 3.0T. It was possible to correctly fit more metabolites with a Cramer–Rao lower-bound <20% at 7.0T, such as N-acetylaspartylglutamate, taurine and glycine. T1-weighted imaging was of less quality at 7.0T compared to 3.0T.
Conclusion(s): 7.0T MRI is feasible in neonates. Some sequences showed even more details at 7.0T compared to 3.0T. Further optimization of the sequences is ongoing.

Figure 1: Examples of images of different patients at 3.0T (top row) versus 7.0T MRI (bottomrow). The arrow at H points out the white matter injury that is more prominent at 7.0T because ofthe increased white-grey matter contrast. The arrow at J shows the N-acetylaspartylglutamate peakat 7.0T that is not visible at 3.0T.
IMAGE CAPTION:
Figure 1: Examples of images of different patients at 3.0T (top row) versus 7.0T MRI (bottom row). The arrow at Hpoints out the white matter injury that is more prominent at 7.0T because of the increased white-grey matter contrast. Thearrow at J shows the N-acetylaspartylglutamate peak at 7.0T that is not visible at 3.0T.
CONTROL ID: 3375265TITLE: Association of postnatal heart rate variability with neuroimaging patterns in term neonates with hypoxic ischemic encephalopathyPRESENTER: Ipsita Goswami
AUTHORS (LAST NAME, FIRST NAME): Goswami, Ipsita1; Kamino, Daphne2; Widjaja, Elysa1; Paniccia, Melissa5; Moore, Aideen M.4; Tam, Emily3
AUTHORS/INSTITUTIONS: I. Goswami, E. Widjaja, Neonatology, The Hospital for Sick Children, Toronto, Ontario, CANADA;D. Kamino, The Hospital for Sick Children, Toronto, Ontario, CANADA;E. Tam, Pediatrics, Hospital for Sick Children, Toronto, Ontario, CANADA;A.M. Moore, Pediatrics, Neonatology, The Hospital for Sick Children, Toronto, Toronto, Ontario, CANADA;M. Paniccia, Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario,CANADA;CURRENT CATEGORY: NeurologyCURRENT SUBCATEGORY: Neonatal Neurology: ClinicalKEYWORDS: Heart rate variability, Hypoxic ischemic encephalopathy, early biomarker.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Heart rate variability (HRV), a continuous non-invasive measure of autonomic regulation, can provideearly insights into pattern and severity of brain injury in hypoxic ischemic encephalopathy (HIE) aiding prognosticationand targeted therapy. Several HRV metrics (linear, non-linear, spectral analysis) exist in literature, however whichmeasures are clinically most useful during early hours of life have not yet been identified.
Objective: This study aimed to longitudinally quantify and compare multiple early HRV metrics in neonates with HIEduring therapeutic hypothermia in order to identify which HRV metrics assist in differentiating neonates with differentpatterns of brain injury.

Design/Methods: We prospectively recruited 95 term neonates who met the inclusion criteria for therapeutichypothermia and continuously recorded their electrocardiogram in the first 48 hours of life. HRV metrics were calculatedin time domain (SDNN, RMSSD), frequency domain (LFnu, HFnu, LF/HF), non-linear (SD1, SD2), cardiac vagal (CVI)and sympathetic (CSI) indices during 1-hour time-epochs at 12, 18, 24, 30, 36 and 48 hours of age. Primary outcome wasdefined as the pattern of changes on brain MRI (median age of 4 days) categorized as Normal, Focal infarct andAbnormal (HIE patterns of watershed or deep gray matter or mixed injury). The Kruskal-Wallis test was used to compareHRV metrics at specific time points between groups and linear mixed effects models were used for temporal changes inHRV metrics.
Results: The cohort had a mean gestational age of 39 ± 1.3 weeks, 67(70%) were male and 6 infants had no MRI done.Neonates with basal ganglia/watershed/mixed pattern injury had significantly lower linear and non-linear HRV measuresin the first 24 hours of life, while significantly lower LFnu/HFnu ratio beyond 24 hours of life compared to neonates withnormal MRI and focal infarcts (Table 1). Significantly depressed CVI and CSI at all timepoints over the first 48 hourswas also associated with typical HIE pattern of brain injury (Figure 1).
Conclusion(s): Early neonatal HRV metrics during hypothermia can help differentiate watershed/deep gray patterns ofhypoxic-ischemic brain injury from focal infarcts or no injury. While frequency domain measures have been studiedmore often to date, this study suggests non-linear HRV measures (SD1, SD2, CVI) may be superior as early biomarkersof severity of brain injury. Low CVI and CSI suggests dampening of both the sympathetic and parasympathetic system inHIE.
LFnu, Low frequency normalized power, HFnu, High frequency normalized power, SD1(ms),standard deviation along the short axis of Poincare plot, SD2(ms), standard deviation along thelong axis of Poincare plot, Poincare plot (RR interval plotted against consecutive RR interval),Cardiac vagal index, CVI = SD2/SD1, Cardiac symapathetic index, CSI = log10(SD1 X SD2)
IMAGE CAPTION:LFnu, Low frequency normalized power, HFnu, High frequency normalized power, SD1(ms), standard deviation alongthe short axis of Poincare plot, SD2(ms), standard deviation along the long axis of Poincare plot, Poincare plot (RRinterval plotted against consecutive RR interval), Cardiac vagal index, CVI = SD2/SD1, Cardiac symapathetic index, CSI= log10(SD1 X SD2)
CONTROL ID: 3344524TITLE: High Blanket Temperature During Therapeutic Hypothermia is Associated with Death or Disability for Infants with Hypoxic Ischemic EncephalopathyPRESENTER: John Flibotte
AUTHORS (LAST NAME, FIRST NAME): Flibotte, John1; Laptook, Abbot R.2; Shankaran, Seetha3; McDonald,

Scott4; Baserga, Mariana5; Bell, Edward F.6; Cotten, Charles M.7; Das, Abhik8; DeMauro, Sara B.9; Dupont, Tara10;Eichenwald, Eric11; Heyne, Roy12; Jensen, Erik A.13; Van Meurs, Krisa P.14; Dysart, Kevin15; National Institute of ChildHealth and Human Development, Eunice Kennedy Shriver16
AUTHORS/INSTITUTIONS: J. Flibotte, Pediatrics/ Neonatology, Children's Hospital of Philadelphia, Philadelphia,Pennsylvania, UNITED STATES;A.R. Laptook, Pediatrics, Alpert Medical School of Brown University, Providence, Rhode Island, UNITED STATES;S. Shankaran, Pediatrics, Wayne State University, Detroit, Michigan, UNITED STATES;S. McDonald, RTI International, Raleigh, North Carolina, UNITED STATES;M. Baserga, Pediatrics, University of Utah, Park City, Utah, UNITED STATES;E.F. Bell, Department of Pediatrics, University of Iowa, Iowa City, Iowa, UNITED STATES;C.M. Cotten, Pediatrics, Duke University, Durham, North Carolina, UNITED STATES;A. Das, Biostatistics and Epidemiology, RTI International, Rockville, Maryland, UNITED STATES;S.B. DeMauro, Department of Pediatrics, University of Pennsylvania, Wallingford, Pennsylvania, UNITED STATES;T. Dupont, Pediatrics, University of New Mexico, Albuquerque, New Mexico, UNITED STATES;E. Eichenwald, Pediatrics/Neonatology, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, UNITEDSTATES;R. Heyne, Pediatrics, U.Texas Southwestern Med Center, Dallas, Texas, UNITED STATES;E.A. Jensen, Pediatrics, The University of Pennsylvania/Children's Hospital of Philadelphia, Philadelphia, Pennsylvania,UNITED STATES;K.P. Van Meurs, Pediatrics/Neonatology, Stanford University, Palo Alto, California, UNITED STATES;K. Dysart, Neonataology, Children's Hospital of Phialdephia, Philadelphia, Pennsylvania, UNITED STATES;E. National Institute of Child Health and Human Development, Pregnancy & Perinatology, NICHD, Bethesda, Maryland,UNITED STATES;CURRENT CATEGORY: NeonatologyCURRENT SUBCATEGORY: Neurology: ClinicalKEYWORDS: Therapeutic hypothermia, Hypoxic ischemic encephalopathy, Prognosis.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Recent trials of therapeutic hypothermia (TH) for infants with hypoxic ischemic encephalopathy (HIE)demonstrate improved but persistent rates of death or disability near 30%. Blanket temperature (BT) necessary tomaintain a sub-physiologic target temperature of 33.5oC has not been studied as a biomarker of outcome. Because bodytemperature is centrally regulated, BT necessary to maintain 33.5oC is a plausible indicator of brain injury.
Objective: Determine whether BT during maintenance phase of TH associates with death or disability at 18-22 monthsfor infants with HIE.
Design/Methods: Retrospective study of infants who received TH at 33.5oC for 72h in the Neonatal Research Network’sInduced Hypothermia and Optimizing Cooling trials. Maintenance phase of TH began when infant esophagealtemperature was 33.5+0.1oC after equilibration from any overshoot in the first 4h. BTs were recorded during TH: atbaseline, every 15 min during the first 4-5h, hourly until 12h, and then every 4h through rewarming. We rank orderedeach infant’s BTs and divided them into quartiles. The mean of the upper quartile (Q4, ≥ 75%) was used as the highestBT. Logistic regression was used to determine if death or moderate/ severe disability was associated with high BT,adjusting for initial Sarnat stage, center, trial, and maternal education. Similar analyses examined associations betweenoutcome and BT using: the overall median; mean of the lowest quartile; and, burden of consecutive blanket temperaturesabove 33.5oC in the first 24 and 48h of TH.
Results: 197 infants received TH at 33.5oC for 72h (Table 1); 187 had adequate data. Of these, 37% (69/187) died orsurvived with disability. Results from analysis of BT quartiles appear in Table 2. Each 0.5oC increase above 33.5oC inthe upper quartile mean was associated with a 58% increase in the adjusted odds of death or disability (aOR 1.58, 95% CI1.14-2.19). aOR of death/ disability based on persistence of high BTs appear in Table 3. Infants with >8 consecutive BTsabove 33.5oC in the first 48 hour of TH had an aOR of death/ disability of 7.51 (95% CI 2.42-23.2). Figure 1 depictsrates of death/ disability based on number of consecutive BTs above 33.5oC in the first 24 and 48h of TH.
Conclusion(s): Higher BT during maintenance phase of TH is associated with death or moderate/ severe disabilityamong infants with HIE and may be an early, clinically useful biomarker to inform prognosis and treatment.


IMAGE CAPTION:
CONTROL ID: 3381660TITLE: Hippocampal Growth in the First Three Months of Life in Term Infants with Neonatal EncephalopathyPRESENTER: Ting Guo
AUTHORS (LAST NAME, FIRST NAME): Guo, Ting2; Annink, Kim3; Groenendaal, Floris3; Chau, Vann2; Benders,Manon J.3; van der Aa, Niek E.3; Wagenaar, Nienke3; Chakravarty, Mallar1; de Vries, Linda S.3; Miller, Steven P.2
AUTHORS/INSTITUTIONS: M. Chakravarty, The Douglas Research Centre & McGill University, Montreal, Quebec, CANADA;T. Guo, V. Chau, S.P. Miller, The Hospital for Sick Children & University of Toronto, Toronto, Ontario, CANADA;K. Annink, F. Groenendaal, M.J. Benders, N.E. van der Aa, N. Wagenaar, L.S. de Vries, Wilhelmina Children’s Hospital & University Medical Center Utrecht, Utrecht, NETHERLANDS;CURRENT CATEGORY: NeurologyCURRENT SUBCATEGORY: Neonatal Neurology: TranslationalKEYWORDS: Neonatal Encephalopathy, Hippocampus, Brain injury.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Central to memory and learning, hippocampus is particularly vulnerable to acute hypoxia. Hippocampal atrophy was shown in children and adults with neonatal and/or perinatal hypoxic-ischemic injury and associated with deficits in recall. Hippocampal volume and growth from the neonatal period to 3 months in term infants with neonatal encephalopathy (NE) remain unclear. Whether total number of antiseizure drugs is associated with impaired early hippocampal growth needs to be studied.
Objective: (1) to assess hippocampal growth from the neonatal period to 3 months (2) to investigate the relationship between total number of antiseizure drugs and early hippocampal growth.
Design/Methods: 42 term infants (mean 40 weeks GA) with NE, were scanned in the neonatal period (median DOL 5, IQR: 3-5) and at 3 months (median DOL 97, IQR: 91-104) at Wilhelmina Children’s Hospital, Utrecht. Brain injury types included: basal ganglia-thalamus (BGT, N=7), watershed/white matter (WS, N=22), and stroke (N=13). Hippocampus and total cerebral volume (TCV) were segmented on T2-weighted MRI using MAGeT-Brain. Hippocampal volumes and growth from the neonatal period to 3 months were calculated. The associations of hippocampal volume and growth with total number of antiseizure drugs were assessed using multivariable generalized linear models, adjusting for sex, birth GA, and brain injury type.
Results: In term infants with NE, those with BGT had smaller hippocampal volumes and growth (Figure 1) (not statistically significant). Total number of antiseizure drugs was associated with smaller hippocampal volume in the neonatal period (β=-51.58, p=0.001) and at 3 months (β=-95.61, p<0.001). BGT brain injury predicted smaller hippocampus at 3 months (β=-215.23, p=0.032). The results remain significant after adjusting for DOL at MRI and TCV. Total number of antiseizure drugs was also associated with reduced hippocampal growth to 3 months (β=-74.29,p=0.004) adjusting for neonatal hippocampal volume (β=-0.655, p=0.007) and weeks between scans.
Conclusion(s): Hippocampal volumes and growth from the neonatal period to 3 months are strongly related to the total number of antiseizure drugs and BGT brain injury in term infants with NE. These findings support the vulnerability of the hippocampus to acute profound hypoxic-ischemic events in children impacted by NE. Cognitive and memory assessments of the study cohort are ongoing and their relationship with early hippocampal growth will be studied.

Figure 1. TCV and hippocampal volumes from the neonatal period to 3 months in three braininjury groups
IMAGE CAPTION:Figure 1. TCV and hippocampal volumes from the neonatal period to 3 months in three brain injury groups
CONTROL ID: 3376854TITLE: MRI Score Inter-rater Reliability in Infants with Mild vs Moderate/Severe Hypoxic Ischemic EncephalopathyPRESENTER: Michelle Machie
AUTHORS (LAST NAME, FIRST NAME): Machie, Michelle1; Weeke, Lauren4; deVries, Linda S.2; Rollins, Nancy1;Sepulveda, Pollieanna M.1; Chalak, Lina F.3AUTHORS/INSTITUTIONS: M. Machie, N. Rollins, P.M. Sepulveda, Pediatric Neurology, The University of Texas Southestern Medical Center, Dallas, Texas, UNITED STATES;L.S. deVries, Wilhelmina Children's Hospital, University Medical Centre Utrecht, Utrecht, NETHERLANDS;L.F. Chalak, pediatrics, ut southwestern medical center, Dallas, Texas, UNITED STATES;L. Weeke, University Medical Center Utrecht, Utrecht, NETHERLANDS;CURRENT CATEGORY: NeurologyCURRENT SUBCATEGORY: Neonatal Neurology: ClinicalKEYWORDS: Hypoxic Ischemic Encephalopathy, Brain Injury, Magnetic Resonance Imaging.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Multiple magnetic resonance imaging (MRI) scores have been well validated in infants with moderate or severe hypoxic ischemic encephalopathy (HIE). Infants with mild HIE may have different patterns of injury, and none of the existing MRI scores have been tested in this group.
Objective: The objective of this study is to test the inter-rater reliability of three different MRI scores, and to compare their diagnostic accuracy to detect abnormalities in infants with varying HIE severity.
Design/Methods: Single center prospective cohort study of infants ≥ 36 weeks gestation with mild, moderate, or severe HIE born at a level III neonatal intensive care unit from 2017 to 2019. All Infants with HIE underwent an MRI on median day of life 5, only infants with moderate or severe HIE underwent therapeutic hypothermia. Experienced MRI readers assigned three different scores (Barkovich score, NICHD Neonatal Research Network (NRN) score, and the Weeke score) to each MRI, and each MRI was scored independently by two readers blinded to clinical outcomes.
Results: 42 newborns with varying HIE severity (16 mild) underwent MRI on median day of life 5. Abnormalities were detected in N= 3 (7%) infants using the Barkovich score, in N= 10 (24%) infants using the NICHD NRN score, and in N= 24 (57%) infants using the Weeke score. Among experienced readers, agreement was excellent for each score: Barkovich score (k=1.0), NICHD NRN (k=0.92), and Weeke (k=0.9), and agreement did not differ with HIE severity. The adjudicated scores correlated moderately, (r=0.68, p<0.01) for Weeke and Barkovich, and (r= 0.65, p<0.01) for Weeke and NICHD NRN score.
Conclusion(s): Subtle injury in mild HIE was detected with highest accuracy using the Weeke score but excellent inter-rater reliability was observed for all three scores. Findings suggest that infants with mild HIE have subtle MRI abnormalities which are better detected with detailed scoring systems. Study findings are timely for the planning of trials of neuroprotection investigating the benefit of hypothermia in mild HIE. The prognostic value of these scoring systems in

predicting long term neurodevelopmental outcomes in mild HIE still needs to be determined and is under study.
IMAGE CAPTION:
CONTROL ID: 3373844TITLE: Mild Hypoxic Ischemic Encephalopathy (HIE): Brain MRI Findings After HypothermiaPRESENTER: Yi Li
AUTHORS (LAST NAME, FIRST NAME): Li, Yi1; Wisnowski, Jessica L.2; Mathur, Amit3; McKinstry, Robert C.4;Mayock, Dennis E.5; Chang, Taeun6; Van Meurs, Krisa P.7; Wu, Tai-Wei8; Ahmad, Kaashif A.9; Goodman, Amy10;Chalak, Lina F.11; Wu, Yvonne12
AUTHORS/INSTITUTIONS: Y. Li, Radiology, University of California San Francisco, Corte Madera, California, UNITED STATES;J.L. Wisnowski, Radiology & Neonatology, Children's Hospital Los Angeles, Los Angeles, California, UNITED STATES;A. Mathur, Pediatrics, Saint Louis University School of Medicine, St. Louis, Missouri, UNITED STATES;R.C. McKinstry, Radiology, Washington University, Saint Louis, Missouri, UNITED STATES;D.E. Mayock, Pediatrics/Neonatology, University of Washington, Seattle, Washington, UNITED STATES;T. Chang, Neurology, Children's National Medical Center, Washington, District of Columbia, UNITED STATES;K.P. Van Meurs, Pediatrics/Neonatology, Stanford University, Palo Alto, California, UNITED STATES;T. Wu, Neonatology, Children's Hospital Los Angeles, Los Angeles, California, UNITED STATES;K.A. Ahmad, Pediatrics, Pediatrix Medical Group & Baylor College of Medicine, San Antonio, Texas, UNITED STATES;A. Goodman, Neurology, University of California, San Francisco, San Francisco, California, UNITED STATES;L.F. Chalak, pediatrics, ut southwestern medical center, Dallas, Texas, UNITED STATES;Y. Wu, UCSF, San Francisco, California, UNITED STATES;CURRENT CATEGORY: NeurologyCURRENT SUBCATEGORY: Neonatal Neurology: ClinicalKEYWORDS: Hypoxic Ischemic Encephalopathy, Therapeutic Hypothermia, MRI.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Therapeutic hypothermia (TH), the standard of care for moderate/severe HIE, is increasingly used to treat neonates with mild HIE; yet little is known about outcomes after TH.

Objective: We report the pattern, severity, and timing of MRI brain injury in mild HIE treated with TH.
Design/Methods: 7 hospitals screened all newborns receiving TH in 2017-18 as part of a separate study ofmoderate/severe HIE (HEAL). Mild HIE was defined as ≥ 1 Sarnat abnormality (consciousness, activity, tone, posture,primitive reflexes, autonomic) at 1-6 hours of age, but not meeting criteria for moderate/severe HIE (≥ 3 abnormalities).Clinical brain MR was performed after TH at mean age 5.4 (SD 3.5) days. MRIs were reviewed by 4 experts and scoredby consensus using a previously validated classification system.1 We determined whether rate of injury varied bymaternal/infant clinical factors and by definition of mild HIE.
Results: Of 77 newborns (mean gestation 39.3 weeks, birthweight 3233g, cord pH 7.01) who received TH for mild HIE,38 (50%) had brain lesions on MRI. Median injury score was 4 (IQR 0-9) and severity was mild (n=26; 34%), moderate(n=10; 13%) or severe (n=2; 3%). Injury patterns included punctate white matter (n=12; 15%), central gray (n=10, 13%),peripheral watershed (n=7; 9%), focal parenchymal lesion including hemorrhage (n=8; 10%), arterial ischemic stroke(n=2; 3%), and atypical lesions (n=15, 19%). 12 (16%) had > 1 injury pattern. 9 (12%) had an atypical pattern only.Among 71 (92%) patients with MRI performed at < 8 days of age, timing of injury was 19 (27%) acute, 20 (28%)subacute, and 1 (1%) chronic. 9 (13%) patients had both acute and subacute injuries; 1 (1%) had both acute and chronicinjuries. 3 had large subdural hemorrhages with mass effect and 1 had a large intraventricular hemorrhage. The rate ofabnormal brain MRI was no different when we applied 2 alternative published definitions of mild HIE. Neitherchorioamnionitis, sentinel event (e.g., placental abruption, prolapsed cord), cord pH nor Apgar score were associatedwith risk of MRI brain injury. At discharge, 13 (17%) required nasogastric tube and 1 (1%) required gastrostomy tube.Median hospital stay was 9 (IQR 7-13) days.
Conclusion(s): Brain parenchymal abnormalities were present in 50% of newborns with mild HIE, even after receivingTH. Clinical trials are urgently needed to evaluate the efficacy of TH for mild HIE. Observational studies of cooled andnon-cooled newborns with mild HIE are needed to inform trial design.
(No Image Selected)
CONTROL ID: 3370612TITLE: Treatment Duration and 2-Year Outcome in Neonates with Acute Symptomatic SeizuresPRESENTER: Hannah Glass
AUTHORS (LAST NAME, FIRST NAME): Glass, Hannah10; Soul, Janet1; Chang, Taeun2; Wusthoff, Courtney J.3;Chu, Catherine J.4; Massey, Shavonne L.5; Abend, Nicholas S.6; Lemmon, Monica E.7; Thomas, Cameron8; Guillet,Ronnie9; Franck, Linda S.10; Sturza, Julie11; Rogers, Elizabeth E.10; McCulloch, Charles E.10; Shellhaas, Renee A.11
AUTHORS/INSTITUTIONS: J. Soul, Boston Children's Hospital, Boston, Massachusetts, UNITED STATES;T. Chang, Neurology, Children's National Medical Center, Washington, District of Columbia, UNITED STATES;C.J. Wusthoff, Child Neurology, Stanford University, Palo Alto, California, UNITED STATES;C.J. Chu, Neurology, Massachusetts General Hospital, Boston, Massachusetts, UNITED STATES;S.L. Massey, Neurology, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, UNITED STATES;N.S. Abend, Neurology, CHOP/Pemm, Philadelphia, Pennsylvania, UNITED STATES;M.E. Lemmon, Pediatrics, Duke University Medical Center, Durham, North Carolina, UNITED STATES;C. Thomas, Division of Neurology, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, UNITED STATES; R. Guillet, Pediatrics, University of Rochester, Rochester, New York, UNITED STATES;H. Glass, L.S. Franck, E.E. Rogers, C.E. McCulloch, Family Health Care Nursing, University of California, San Francisco, San Francisco, California, UNITED STATES;J. Sturza, R.A. Shellhaas, Pediatrics, University of Michigan, Ann Arbor, Michigan, UNITED STATES;CURRENT CATEGORY: NeurologyCURRENT SUBCATEGORY: Pediatric NeurologyKEYWORDS: seizures, epilepsy, cerebral palsy.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|Platform

ABSTRACT BODY: Background: Treatment duration for acute symptomatic neonatal seizures is highly variable. Anti-seizure medication(ASM) may be discontinued prior to discharge or continued for months.
Objective: To assess whether ASM treatment duration after acute symptomatic neonatal seizures alters the risk ofepilepsy, cerebral palsy (CP), or functional outcome.
Design/Methods: Prospective, observational comparative effectiveness study of ASM duration for >300 infants withacute symptomatic neonatal seizures born between 7/2015-3/2018 and enrolled at 9 Neonatal Seizure Registry sites.Propensity for ASM at discharge was defined by logistic regression in a model that included: seizure etiology, gestationalage, hypothermia, worst EEG background, days of EEG seizures, and discharge exam (all significant at adjusted p<0.1,except etiology, which was included for face value). At 2-years, epilepsy and CP (Gross Motor Functional ClassificationSystem [GMFCS]) were determined by parent interview and corroborated by medical records. Functional outcome wasassessed by the Warner Initial Developmental Evaluation of Adaptive and Functional Skills (WIDEA). Risk of eachoutcome was adjusted for propensity to receive ASM at discharge.
Results: Characteristics of the first 230 children with 2-year follow-up data are presented (Table). ASMs were prescribedat discharge for 64% for median 4 (IQR 3, 8) months, with a higher propensity for those with high seizure burden,complex clinical course, and abnormal discharge exam. Risk of epilepsy for children whose ASM was discontinued priorto vs. after neonatal discharge was similar (11% vs 12%, p=0.9, propensity adjusted OR 0.6, 95% CI 0.2-1.5, p=0.3), aswas age of epilepsy onset (HR 0.5, 95% CI 0.2-1.2, p=0.13, adjusted HR 0.97, 95% CI 0.4-2.4, p=0.95). The risk ofGMFCS >2 did not differ by ASM treatment duration (10% vs 16%, p=0.2; adjusted OR 1.3, 95% CI 0.5-3.1, p=0.6).WIDEA scores were similar for children whose ASM was discontinued prior to vs. after discharge (158 vs 153, p=0.2,adjusted average -2 points, 95% CI -11-7, p=0.7).
Conclusion(s): Discontinuing ASM prior to discharge home for infants with acute symptomatic neonatal seizures doesnot increase the risk of epilepsy, CP, or functional disability at 2-years. Data from this large, prospective, multicenterstudy help support routine discontinuation of ASM prior to hospital discharge after resolution of acute symptomaticneonatal seizures, which reflects a change in practice at many centers.
IMAGE CAPTION:
CONTROL ID: 3380729TITLE: Changes in Apparent Diffusion Coefficient Values and Brain Metabolite Levels after Neonatal Hypoxic-Ischemic Encephalopathy

PRESENTER: Jun Shibasaki
AUTHORS (LAST NAME, FIRST NAME): Shibasaki, Jun1; Niwa, Tetsu2; Tomiyasu, Moyoko3; Morisaki, Naho4;Fujii, Yuta1; Aida, Noriko1
AUTHORS/INSTITUTIONS: J. Shibasaki, Y. Fujii, N. Aida, Neonatology, Kanagawa Children's Medical Center,Yokohama, JAPAN;T. Niwa, Tokai University, Isehara, JAPAN;M. Tomiyasu, National Institute of Radiological Sciences, Chiba, Chiba, JAPAN;N. Morisaki, National Research Institute for Child Health and Development, Tokyo, JAPAN;CURRENT CATEGORY: NeonatologyCURRENT SUBCATEGORY: Neurology: ClinicalKEYWORDS: Apparent Diffusion Coefficient, proton magnetic resonance spectroscopy, hypoxic-ischemicencephalopathy.SESSION TITLE: Neonatal Neurology: Clinical I |Neonatal Neurology: Clinical ISESSION TYPE: Webinar|PlatformABSTRACT BODY: Background: Apparent diffusion coefficient (ADC) values and brain metabolite levels on proton magnetic resonancespectroscopy (1H-MRS) of the deep gray matter have been reported to accurately predict prognosis in neonates withhypoxic-ischemic encephalopathy (HIE) treated with therapeutic hypothermia. However, the time-course changes inADC values and brain metabolite levels after HIE have not been investigated thoroughly.
Objective: To evaluate the time-course changes in ADC values and brain metabolite levels after HIE and improve thepredictive accuracy of these markers in cooled neonates.
Design/Methods: For this retrospective study, 37 neonates aged 35–41 gestational weeks with HIE admitted between2009 and 2018 to our hospital for therapeutic hypothermia underwent a 3-T MR examination twice, at 18–100 h and 7–14 days after birth. A total of 74 ADCs from 37 neonates were calculated using signal intensities for diffusion-weightedimaging with b=0 and 1500 s/mm2, at the basal ganglia and thalamus. A total of 72 1H-MRS (echo time/repetition time:30/5000 ms) data in the deep gray matter were obtained from 36 neonates, and each metabolite level was calculated.Adverse outcome was defined as death or neurodevelopmental impairment at age 18–22 months. Areas under thereceiver-operating characteristic curve (AUC) were used to evaluate the prognostic values of ADC and metabolite levels.
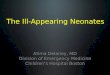
Results: At 18–100 h, the ADCs at the thalamus and basal ganglia were significantly lower in the neonates with adversethan in those with favorable outcomes. Increases in ADCs to days 7-14 were significantly higher among neonates withadverse outcomes compared to those with favorable outcomes although they increased in both groups. The AUC of theADCs at the thalamus and basal ganglia for predicting adverse outcomes were respectively 0.93 and 0.84 at 18–100 h and0.75 and 0.69 on days 7–14. The N-acetylaspartate (NAA) levels were lower and the lactate levels were higher in theneonates with adverse outcomes than in those with favorable outcomes at 18–100 h, with decreases on days 7–14. TheAUC of the NAA and lactate levels for predicting adverse outcomes were respectively 0.98 and 0.96 at 18–100 h and0.98 and 0.74 on days 7–14.
Conclusion(s): At 18–100 h, both lower ADCs at thalamus and NAA accurately predicted adverse outcomes. On days 7-14, the ADC levels of the neonates with adverse outcomes increased, reducing prognosis predictability, while NAAlevels further decreased and pertained prognosis predictability.

Scatterplot showing the change over time of ADC values and metabolites. 1cutoff value ofmeasurements at 18–100 hours after birth. 2cutoff value of measurements at 7–14 days after birth.
IMAGE CAPTION:
Scatterplot showing the change over time of ADC values and metabolites. 1cutoff value of measurements at 18–100hours after birth. 2cutoff value of measurements at 7–14 days after birth.
< Return to Abstract Search< Return to Abstract Search PrintPrint