Embed Size (px)
Citation preview
Update on paediatric neurology
Practical Paediatrics, June 2016
Dr Margaret KaminskaConsultant in Paediatric Neurology and NeurodisabilityComplex Motor Disorders Service
Evelina Children’s Hospital
Outline:Neurological examinationMovement disorders
examples and etiologymanagementstatus dystonicus
EpilepsyWhen to refer seizures/epilepsy
Autoimmune encephalitis
Neurological examination• Observation
– Play in waiting area
– Walking into clinic
– Facial features
– Posture
– Movements
– Speech and cognition
– Visual behaviour
– Abnormal movements, events

Neurological examination
• Fun and Games (screening)
– Standing up (chair or floor)
– Arms out
– Eyes closed
– Standing on one leg
– Hopping, skipping
– Walking on tip toes, heels, tandem walking
– Climb onto couch

Neurological examination
• Targeted formal examination– Tone (trunk and limbs)– Power (full antigravity = 3/5)– Reflexes– Cranial nerves (vision, eye movements, facial
asymmetry, swallowing diffculty, cough)– Sensation– Measurements
• Weight, height, head circumference
– Extras • Heart, abdomen, spine, hips etc
Evelina Children’s Hospital
Movement disorders

Movement disorders in children and young people
Hyperkinetic
• Tics• Tremor• Chorea• Athetosis• Dystonia• Mioclonus • Stereotypies
Hypertonic
• Spasticity• Dystonia • Rigidity
Negative signs
weakness
Reduced selective motor control
Ataxia
Apraxia
Sanger TD, Chen D et al: Definition and classification of hyperkinetic movements in childhood; Mov Disord. 2010 Aug
Sanger TD, Delgado L et al: Classification and definition of disorders causing hypertonia in childhood; Paediatrics 2003 Jan
Sanger TD, Chen D et al: Definitions and classification of negative motor signs in childhood; Paediatrics 2006
Evelina Children’s Hospital
Movement disorder can be interpreted as seizures and should be carefully differentiated!

34 children with CP: 87% had spasticity78 % had dystonia
2009

Evelina Children’s Hospital
Gait:
Evelina Children’s Hospital
Spasticity:•Velocity dependant increase of tone•Brisk jerks•Sustained ankle clonus•weakness

Dystonia
Dystonia: involuntary continuous or intermittent muscle spasms causing repeated twisting movements or postures or both.Tone not velocity dependant, jerks normal or can be absent
“Not to fast – not too slow, not to small- not too big, not too strong – not too weak”

Myoclonus
myoclonus:
arrhythmic, short, shock-like movements caused by sudden muscle spasm or relaxation
Evelina Children’s Hospital
Chorea
Tremor
Tremor: rhytmic movements around a joint
Evelina Children’s Hospital
Tremor
What is unusual?
Evelina Children’s Hospital
• Structural brain damage– cerebral palsies
– Childhood strokes
– Encephalitis –infective/autoimmune
– Tumours
– Acquired brain injury (traumatic, hypoxic)
• Metabolic and degenerative disorders
• Other – Infection, vascular malformations,
– Genetic: Rett syndrome, DYT1, DYT11, TITF1, other genetic movement disorders
– Toxic: medication, CO
• All deserve detailed investigations
• Brain scans, blood and urine tests, genetic tests
Investigations for movement disorders –tailored to suspected aetiology
Evelina Children’s Hospital
Treatment options for a child with movement disorder
• Treatment of underlying aetiology if possible
• Treat exacerbating factors – feeding problems, reflux, pain, anxiety
• Nutrition
• Positioning
• Avoid physical restraint
• Medical treatment of tone, movement disorder
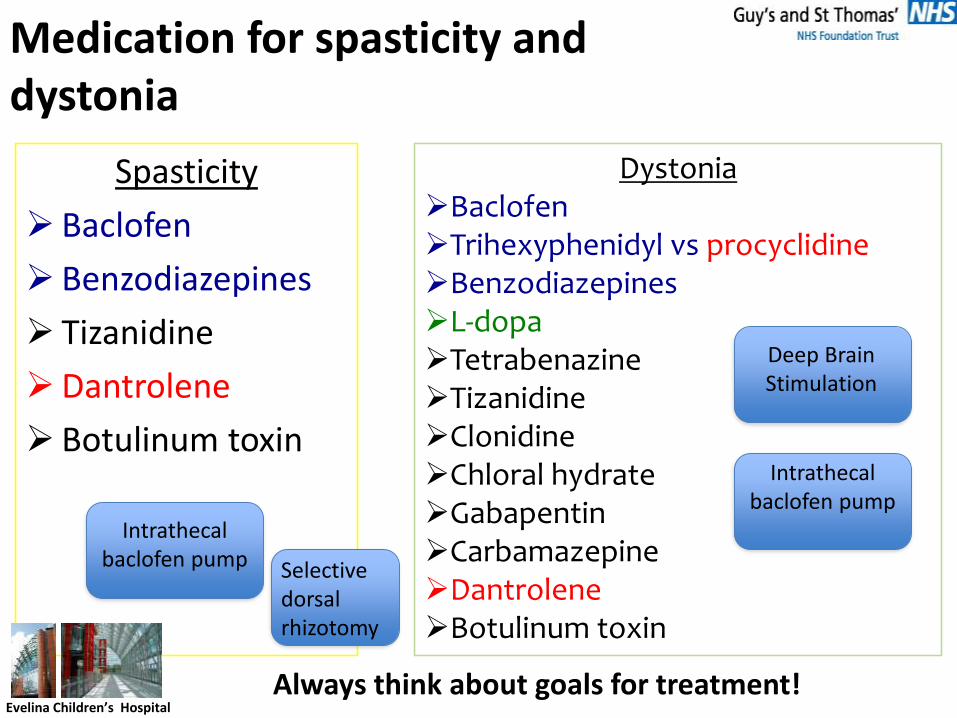
Spasticity
Baclofen
Benzodiazepines
Tizanidine
Dantrolene
Botulinum toxin
Evelina Children’s Hospital
Medication for spasticity and dystonia
DystoniaBaclofenTrihexyphenidyl vs procyclidineBenzodiazepinesL-dopaTetrabenazineTizanidineClonidineChloral hydrateGabapentinCarbamazepineDantroleneBotulinum toxin
Intrathecal baclofen pump
Deep Brain Stimulation
Intrathecal baclofen pump
Always think about goals for treatment!
Selective dorsal rhizotomy
Evelina Children’s Hospital
Status dystonicus
Evelina Children’s Hospital
Status dystonicus: case vignette
9y boy with quadriplegic CP, ex-prem, PEG1 day Hx pf fever 38.5Distressed, unsettled, increased movementsIncreased respiratory secretions
? Chest infection : CRP 9, WBC 11, Chest X-Ray – possible peri-bronchial changes in right lower lobe, urine clearUrea 7.4, normal electrolytes and creatinine
Started treatment with co-amoxiclav
Day 3 – continues to spike fever up to 39.5 at times, unsettledChest X-Ray reviewed – no convincing signs of chest infectioninflammatory markers lowmum says – sleeps very little, how much? Not documented
CK 60 000 urea 8.5 normal electrolytes creatinine – upper normal range
Evelina Children’s Hospital
Status dystonicus: definition
Life threatening movement disorder emergencyIncreasingly frequent or continuous severe episodes of generalized dystonic spasms (contractions)
Status dystonicus: Tonic – mainly sustained contractures and postures Phasic – rapid and repetitive dystonic contractions
Considered rare – only 100 reported cases, but likely underreported and underrecognised
Up to 60% between ages 5 and 16 years
Cerebral palsy – most common cause of secondary dystonia in children
Allen et al 2013

Evelina Children’s Hospital
Status dystonicus: dystonia severity grades
Evelina Children’s Hospital
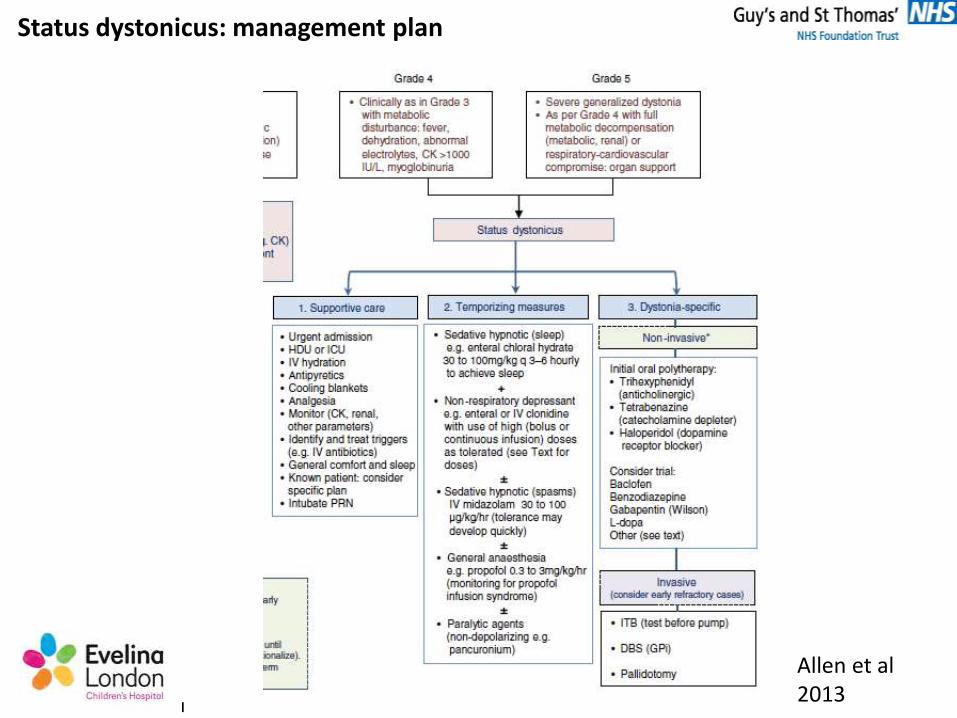
Status dystonicus: management plan
Allen et al 2013
Evelina Children’s Hospital
Status dystonicus: management plan
Consider if increased stiffness, movements, irritability, poor sleep, fever Check CK, electrolytes, urea, creatinine, liver, Ca, Mg, P, BGLook for contributing factors and treat– infection, pain (otitis, fracture , gut), ITB or DBS
malfunction.Talk to your paediatric neurology team
Maintain feeding if possibleEnsure good hydration enteral/IV– monitor urine output, fluid chart, renal function tests,
BG as required, CK, urine dipstick for blood (myoglobinuria)Sleep chart to clearly document periods of sleepExtreme spasms, discomfort particularly if airway compromise – IV lorazepam/PR diazepam
or buccal midazolam as temporizing measure“sleep abolishes dystonia”
chloral hydrate 30-50mg/kg as required up to 4-6 hourlyclonidine first dose 1mcg/kg and repeat 4-6-8 hourly
every next dose can be increased by 1mcg/kg up tp 25mcg if response unsatisfactorydoses up to 2mcg/kg/hour IV or enteral. Monitor BP and HR.
Consider midazolam infusion but tolerance develops quickly.
Clonidine
Dystonia treatmentSpinal and supraspinal α 2 adrenergic receptor agonistReduces aspartate and glutamate release in presynaptic
terminals anitinocioceptive properties
Initially used for treatment of arterial hypertensionSide effects : somnolence, bradycardia, low BPSame oral/transdermal and IV daily dose
Clonidine - our experience
• 1 mcg /kg test dose - monitor BP
• 3 – 8 doses or continuous IV infusion
• Max dose used in our group:
3-4 mcg/kg/hour enteral and
48 mcg/kg/day (2mcg/kg/hour) IV
• Side effects at high doses (in combination with chloral hydrate):
•
Chloral hydrate
Sedative and hypnotic through enhancing GABA receptorsIngredient of Mickey FinnMetabolizes to tri-chloro-ethanol
Dose: 30-50 mg/kg or 100mg/kg/24h in 3-4doses, max 4g/24h
Side effects: deep sedation, respiratory depression, low bloodpressure, liver failure, tolerance, dependency, withdrawalsymptoms
James Bond says, "that's...chloral hydrate" in the movie "The Living Daylights" before collapsing from it's effects
Evelina Children’s Hospital
EpilepsyWhen to refer?
Evelina Children’s Hospital
Case study 4/12 boy
• Term delivery, IUGR, thrombocytopenia resolved
• New onset of focal seizures: eyes deviation and flickering +/- upper
limb jerks
• Seizures stopped after phenytoin load
• Normal CT, baseline bloods and LP
• Refer to neurology? Y N
• Clinic or on call service?
Evelina Children’s Hospital
InfantsAbnormal imagingFocal onset seizuresContinuing seizures following trials of 2
AEDs (refractory epilepsy)Possible neuro-degenerationUncertainties re diagnosisOngoing ? Non-epileptic events
Neurology referralKnow your service and pathway!

Evelina Children’s Hospital
Case study: 18/12 girl
Ex prem 29/40
Neonatal sepsis, early seizures
Developmental delay
Evolving motor disorder – tone mostly increased in left UL, brisk DTR
Meds: valproate + phenobarbiton
Mum reports episodes of stiffness with glazed look
Valproate increased
trihexyphenidyl started – some improvement
EEG normal

Evelina Children’s Hospital
18/12 girl, ex prem - home videoMedication: Na valproate, phenobarbiton, trihexyphenidyl

• Was it epileptic?
infant toddler Older child
Normal movements
‘Shuddering attacks’
Rigors
Sleep myoclonus
Gratification disorder
Gastro-oesophageal
reflux
Movement disorder
(eg paroxysmal tonic
upgaze)
Cardiac arrhythmia
BehaviouralBreath holdingNight terrorsGratification disorderStereotypiesDay-dreamingLearning Diffs
MigraineSyncopeCardiacBenign paroxysmal vertigoMovement disorder Fabricated illness
Tic disorderCardiacVaso-vagal syncope
Movement disorder
Pseudo-seizures/non epileptic attacks

Paediatric Epilepsy Training
• Standardised courses
• Available in all regions
• PET 1
• PET 2
• PET 3
www.bpna.org.uk/pet

Encephalitis
Autoimmune encephalitis
Case: 5 year old girl
• Intermittent slurred speech 3 days after minor head injury
• Normal brain MRI
• Within next few days: progressive episodes of confusion and behavioural change
• Chorea of the left hand

Case: 5y old girl
• Few focal seizures
• Speech problems worsen to no speech
• chorea one hand persists
• EEG encephalopathic
• CSF – normal cells, sugar and protein
• Viral serology and cultures negative
• Rx: antibiotics, antivirals, phenytoin
Case: 5y old girl
• NMDA receptor antibody positive
• High dose steroids
• Full recovery at 12 months FU
Auto-immune encephalitides
• Treatable cause of encephalitis• Neuropsychiatric features very common:
behavioural change 63%confusion 50%hallucinations 25%Seizures 83% and movement disorder 38%
Hacohen et al 2013 • Auto-antibodies to cell surface antigens, crucial for
neurotransmission• VGKC, GAD, NMDA receptor antibodies . . .• >400 cases clinically relevant elevated titres in UK over last 3
years• Increasingly diagnosed in children
still under diagnosed• Paraneoplastic – much more frequent in adults
NMDA encephalitis
• Short history – days/weeks
• Seizures/odd episodes
• Behavioural change, encephalopathy
• Involuntary movements
• EEG abnormal, lymphocytes in CSF, +/- imaging abnormalities
• NMDA receptor antibody positive
• N-methyl-D-aspartate glutamate voltage-dependent channels
• Association with ovarian teratoma and other neoplasia (20-50% adults)
VGKC encephalitis
• Can present as limbic encephalitis, but other presentations possible
• Subacute personality change, memory problems, seizures within first few days; temporal lobe epilepsy
• MRI changes – high signal medial temporal lobe often with contrast enhancement
• Association with malignancy
(adults; recent UK study – 39 children VGKC Ab+, none had neoplasm; presented at BPNA conference 2014)
• often monophasic illness
• Antibody titres fall with treatment
Auto-immune encephalitisearly treatment
• Byrne et al, 2014:
NMDAR encephalitis, literature review, 43 cases
88% treated within 15 days had full recovery36% treated after 15 days had full recovery
Treatment: steroids, IVIG, plasma exchange, rituximab
Autoimmune encephalitis – diagnostic criteriaZuliani et al 2012
Criteria•Acute or subacute (<12 weeks) onset of symptoms
•Evidence of CNS inflammation (at least one of):
CSF (lymphocytic pleocytosis, CSF specific oligoclonal bands or elevated
IgG index)
MRI inflammatory changes
Inflammatory neuropathology on biopsy
•Exclusion of other causes (infective, trauma, toxic, metabolic, tumors,
demyelinating or history of previous CNS disease
Supportive features• History of other autoimmune disorder
• Preceding infectious illness or viral-disease-like prodromes

Dr Margaret KaminskaPractical Paediatrics, June 2016