Embed Size (px)
Citation preview

Neonatal Infections
May 2005
Dr Patricia Fenton
Sheffield Children’s Hospital

Neonatal Infections
Hazard analysis at critical control point
A baby production line
Uterus to push chair

The Bad News Is…..
No
Pictures

The Good News Is….
994 out of every 1000 infants born in the
UK survive

Some Definitions
Infant - <1 year
Neonate - < I month
“early onset” - < 7 days

Infant Deaths 93-97 (Number)
0
1000
2000
3000
4000
5000
6000
7000
8000
Congen Infection
E and W figures Neonates account
for 67% of deaths Infection is NOT a
major cause of neonatal death.

A Hazardous Journey
The uterus: Listeria monocytogenes The birth canal: group B streptococcus The unit: Acinetobacter baumanii Devices: CNS The attendants: Staph aureus

Three Barriers to Infection
NORMALFLORA
SKIN ANDMUCOUS
MEMBRANES
IMMUNITY

Impaired Barriers
Thin skin
Raw umbilicus
Invasive devices

Small/premature =
Poor antibody response Poor neutrophil response Poor complement activation Impaired macrophage activity Poor T cell function Reduced placental IgG

Clinical Presentations
Not breathing well Not feeding well Not looking well
lethargic irritable mottled Fever and tachycardia Seizures
AND NOT A BLOOD TEST OR XRAY!

Listeria monocytogenes
1-3 cases per million per year E&W 17 pregnancy associated cases 2001 >300 pregnancy assoc. 87-89
Soft cheese, paté and chilled meals All animals 5% humans in bowel

Listeria - an interesting organism
G + rod Flagellae-RT not BT Tumbling motility Haemolytic BA Invasin (IC) Actin tails Listerioloysin O

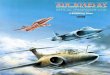
Log10 bacteria per ml
0
1
2
3
4
5
6
7
8
9
1 week 2 weeks 3 weeks 4 weeks
4 degreesminus 20

Disease Spectrum
Influenza like illness (maternal) Sepsis with stillbirth
Neonatal sepsis/meningitis
Sepsis/meningitis in impaired immunity (at any age)

Treatment, Outcome and Control
Ampicillin or amoxycillin Plus gentamicin
One third fatal
Avoidance, food quality measures, high level of suspicion, early treatment

Early Onset GBS Disease
376 cases in 2001 39 died
Important because: Identified risk factors Preventable

Risk Factors
Previous baby affected by GBS GBS in urine at any time this pregnancy Preterm labour Prolonged ROM Fever in labour
(RCOG guidelines 2003)

Screening Based Strategy
27% carry it (rectal plus vaginal swabs)
Antibiotic prophylaxis 86% reduction
Treat 1000, prevent 1.4

Risk Factor Strategy
25% women have one or more risk
Antibiotic prophylaxis 69% reduction
Treat 1000, prevent 2

The Disease
Early onset Low apgar Sepsis Pneumonia
GBS causes 70% early onset sepsis Low birth weight

Prevention
Choose your mother carefully (IgG)
Be big (mortality 6% vs. 18%)
Penicillin AT ONSET OF LABOUR

Christmas Day HH
Premature 35/40 No ANC Septic, ventilated Extubated day 11 Home “to die”
BUT….

The Unit
24 cots (2x6 bedded 1x12 bedded) Zero to two cases per year for 5 years 4 month period 11 cases clinical sepsis All cases in one 6 bedded ward area

The Bug
Acinetobacter baumannii Gram negative cocco-bacillus Water-dwelling saprophyte Long survival on dry surfaces Mattresses, air con, ventilators Up to 25% normal human skin flora Dissemination via hands?

What Happened Next?
Cultured everything.

Results?
Nothing
Followed each baby and everything that happened to them

And they found
Hydrocolloid dressings-large sheets Cut and stored Used on skin
CULTURE POSITIVE OUTBREAK STRAIN

What happened next?
Practice stopped Outbreak ended
3 babies died

Lessons Learnt
A knowledge of background infection rates useful (none to 11)
Susceptible patients are just that
Plastic wallets make good incubators

Devices
Initial response Getting worse
Central line in situ ?CNS

Coagulase negative staphylococci
Gram positive cocci Normal skin flora Low grade pathogen in normal host Hydrophobic cell surface (adheres) Polysaccharide production - biofilm Neonatal infections

Neonatal Unit B/C
CNS 234 Stau 17 E.coli 19 GNB’s 32 GBS 18

Attendants
6 week period 4 blistered babies Early discharge 14 more identified
Staph aureus Phage type 3A/3C Exfoliative toxin A

Outbreak Control
Swabs of all staff handling newborns Check all hands
One individual handled 17/18 affected Epidemic strain from nose, axilla, peri All other staff negative Treatment of carrier ended outbreak

Staphylococcus aureus
Looks like CNS and.. Normal flora (30% adults) but.. Highly pathogenic Exfoliative toxin A - SSSS Potential for cross infection
Treated with flucloxacillin

Control Measures
Wash hands
and
check hands

Conclusions
Infection: significant hazard to neonate Journey womb to push chair Bacteria for every occasion
Smaller is frailer Never give up on a neonate

Our Aim at SCH
Family focused service
Putting the needs and welfare
of children first