Embed Size (px)
Citation preview

Fig 4. Schematic presentation of the accessory mitral valve tissues,anatomic location related to the left ventricular structures andmitral valve.
1098 CASE REPORT LOFTUS ET AL Ann Thorac SurgFLAIL TRICUSPID VALVE IN THE NEONATE 2014;98:1098–101
FEATUREARTIC
LES
muscle. At the short-axis view of the mitral valve, wecould observe both AMVT structures clearly. We alsoexamined the length between the aortic valve and thetop of the floppy AMVT. The placement of the skin inci-sion is completely different between aortotomy andatriotomy in robotic operations. Ascuitto and colleagues[5] described the difficulty of the aortic approach.Nevertheless, some surgeons have selected the aortotomyapproach for cases of enormous floppy AMVT prolapsedto the LVOT [6]. On actual examination, we selected avertical approach to the left atrium.
Edwin and colleagues have classified AMVT depend-ing on the intraoperative findings. In our case, AMVTlocated at the anterolateral site was type II-A (pedun-culated) and at the posteromedial site was type II-B2(leafletlike, well-developed chordate) (Fig 4). Thesetypes will be good indications for a robotic operation.The right-side approach is suitable for a robotic opera-tion [7]; there may be some difficulty in case of an aorticapproach.
In conclusion, we successfully performed roboticresection of dual AMVT. The daVinci surgical system wasuseful for this operation, owing to its three-dimensionalendoscope, which enabled better observation of the in-ternal heart structures.
Accepted for publication Nov 8, 2013.
Address correspondence to Dr Kaza, Department of Cardiac Surgery,Boston Children’s Hospital, 300 Longwood Ave, Bader 273, Boston,MA 02115; e-mail: [email protected].
References
1. Mclean LD, Culligan JA, Kane DJ. Subaortic stenosis due toaccessory tissue on the mitral valve. J Thorac Cardiovasc Surg1963;45:383–8.
� 2014 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
2. Meyer-Hetling K, Alexi-Meskishvili VV, D€ahnert I. Criticalsubaortic stenosis in a newborn caused by accessory mitralvalve tissue. Ann Thorac Surg 2000;69:1934–7.
3. Aoka Y, Ishizuka N, Sakomura Y, et al. Accessory mitral valvetissue causing severe left ventricular outflow tract obstructionin an adult. Ann Thorac Surg 2004;77:713–5.
4. Rovner A, Thanigaraj S, Perez JE. Accessory mitral valve in anadult population: the role of echocardiography in diagnosisand management. J Am Soc Echocardiogr 2005;18:494–8.
5. Ascuitto RJ, Ross-Ascuitto NT, Kopf GS, Kleinman CS,Talner NS. Accessory mitral valve tissue causing left ventric-ular outflow obstruction (two-dimensional echocardiographicdiagnosis and surgical approach). Ann Thorac Surg 1986;42:581–4.
6. Tamin SS, Dillon J, Aizan K, Kadiman S, Latiff HA. Anaccessory mitral valve leaflet causing left ventricular outflowtract obstruction and associated with severe aortic incompe-tence. Echocardiography 2012;29:E34–8.
7. Prifti E, Bonacchi M, Bartolozzi F, Frati G, Leacche M,Vanini V. Postoperative outcome in patients with accessorymitral valve tissue. Med Sci Monit 2003;9:RA126–33.
Neonatal Flail Tricuspid Valve:Diagnosis and ManagementPatrick D. Loftus, HBS,Cammon B. Arrington, MD, PhD, andAditya K. Kaza, MD
Pediatric Cardiothoracic Surgery and Pediatric Cardiology,University of Utah, Salt Lake City, Utah
Flail tricuspid valve in the neonate is a rare and oftenfatal condition requiring early diagnosis and interven-tion. We report 3 infants born without antenatal signs ofcardiovascular compromise. Severe hypoxemia devel-oped within hours of birth due to disruption of theanterior leaflet of the tricuspid valve. Each patient wasstabilized and required differing levels of acute careincluding prostaglandin-E2 alone, prostaglandin-E2 plusnitric oxide and milrinone, or extracorporeal membraneoxygenation. All patients underwent successful tricuspidvalve repair.
(Ann Thorac Surg 2014;98:1098–101)� 2014 by The Society of Thoracic Surgeons
lail tricuspid valve (TV) is a rare defect that can occur
Fin utero and often leads to severe neonatal distress[1, 2]. Here we describe the diagnosis and management of3 neonates with flail TV.Case Reports
Patient 1Patient 1 was a 4.02-kg infant born at 41 weeks’ gestationto a 29-year-old G3P3 mother. The patient’s APGAR(appearance, pulse, grimace, activity, respiration) scores
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.11.003

1099Ann Thorac Surg CASE REPORT LOFTUS ET AL2014;98:1098–101 FLAIL TRICUSPID VALVE IN THE NEONATE
FEATUREARTIC
LES
were 8 at 1 and 5 minutes. Pregnancy and delivery wereuncomplicated. At approximately 3 hours of life, the pa-tient became cyanotic. A low-frequency holosystolicmurmur was noted at the left lower sternal border, and achest roentgenogram revealed cardiomegaly.
The patient was started on prostaglandin-E2 (PGE2).Echocardiography demonstrated a flail anterior TVleaflet, moderate-severe TV regurgitation, mild rightventricle dilatation, an echobright moderator band, andsevere right atrial dilation. As the pulmonary vascularresistance dropped, oxygen saturations improved into the90s and PGE2 was discontinued. Surgical repair of thevalve was performed at 36 hours after birth.
Patient 2Patient 2 was a 3.65-kg infant born at 39 weeks’ gestationafter an uncomplicated pregnancy and vaginal delivery toa 24-year-old group-B strep-positive G4P3 mother. Thepatient’s APGAR scores were 7 and 8 at 1 and 5 minutes.The mother received 3 doses of ampicillin before delivery.No concerning findings were present on prenatal ultra-sound imaging. Immediately after birth, increased workof breathing, hypoxia, and oxygen saturations in the 60%range developed in the patient despite administration of100% oxygen.
The infant was intubated and PGE2 was administered.Echocardiography demonstrated a flail anterior TVleaflet, moderate-severe tricuspid valve insufficiency, anda ruptured echobright dominant papillary muscle. Thepatient was started on nitric oxide (NO) and milrinone,and received a transfusion of packed red blood cells. After2 weeks, the patient improved enough to discontinuePGE and NO. The patient underwent a reparative oper-ation at 17 days after birth.
Patient 3Patient 3 was a 4-kg infant born by spontaneous vaginaldelivery at 38 weeks’ gestation to a 27-year-old G4P4mother. The patient’s APGAR scores were 8 at 1 and 5minutes, as described previously in Arrington and col-leagues [2]. Pregnancy was uncomplicated, with themother starting prenatal care at 25 weeks’ gestation. Noabnormalities were detected on prenatal ultrasoundimaging.
At 2 hours of age, the patient was cyanotic with roomair saturations between 20% and 50%. A harsh hol-osystolic murmur was noted. Metabolic acidosisdeveloped despite administration of PGE2, dopamine,dobutamine, mechanical ventilation, and inhaled NO.The patient was ultimately placed on venoarterial extra-corporeal membrane oxygenation (ECMO). Echocardi-ography demonstrated significant TV regurgitation, a flailanterior TV leaflet, and a ruptured papillary muscle andchordae. After 5 days, the patient improved enough tobe taken off ECMO and underwent TV repair at 9 daysafter birth.
The anterior papillary muscle in all 3 patients wasdirectly avulsed from the papillary head, causing pro-lapse of the anterior leaflet of the TV with its attachedchords and avulsed papillary tissue. In patient 1, the right
atrium was thickened, suggesting the TV regurgitationhad been present for an extended period. There was alsocalcification at the anterior papillary head. In patient 2,the papillary head at the ventricular myocardial level wasyellowish-white, indicating an ischemic process thatlikely occurred in utero. In patient 3, the anterior papil-lary muscle and head were scarred and calcified neartheir rupture point, suggesting a more subacute or evenchronic change. Three chords still attached to the anteriorleaflet were ruptured from the avulsed anterior papillarymuscle, whereas the other anterior leaflet chordsremained attached to the avulsed papillary muscle.Each patient was placed on cardiopulmonary bypass
using standard aortobicaval cannulation. Antegrade car-dioplegia was administered, and the right atrium wasopened parallel to the atrioventricular groove.Patient 1: An autologous pericardial pledget with a 6-0
Prolene suture (Ethicon, Somerville, NJ) was used todirectly reattach the avulsed papillary tissue of the ante-rior leaflet to its original insertion site on the calcifiedanterior papillary muscle. A commissuroplasty stitch wasplaced at the anteroseptal commissure. Calcification didnot make the repair difficult; however, pledgets wereused to reinforce the repair.Patient 2: The avulsed papillary muscle still attached
to the anterior chords and leaflet was directly reat-tached to the ventricular myocardium using a 6-0 Pro-lene suture with autologous pericardial pledget. Leafletunion of the anterior leaflet and septal leaflet wasperformed.Patient 3: The avulsed anterior papillary muscle still
connected to the anterior leaflet chords was directly reat-tached to the base of the anterior papillary head using a 6-0Gore-Tex suture (W.L. Gore andAssociates, Flagstaff, AZ).The 3 free-floating chords still attached to the anteriorleaflet were directly reconnected to the papillary head bya second 6-0 Gore-Tex suture. A 5-0 Prolene suture withpericardial pledgets was used to reinforce the reattachedpapillary muscle. A modified annuloplasty in the regionof the posterior septal commissure was performed using a5-0 pledgeted Prolene suture in a horizontal fashion.In each case, the valve was passively tested and noted
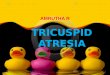
to be competent. Postoperative transthoracic echocardi-ography confirmed successful valve repair in all 3 pa-tients (Fig 1).
Comment
Cyanosis occurred in each patient within the first 2 to 4hours of life, despite reassuring APGAR scores. This shortdelay might have been due to postnatal ductal closure,because echocardiography in 2 of the 3 patients showed nopatent ductus arteriosus. Low oxygen saturations despiteadministration of supplemental oxygen and a holosystolicmurmur led to the diagnosis of flail TV by echocardiogra-phy. Echocardiographic findings indicative of flail TVincludemoderate-severeTVregurgitationdue toTV leafletprolapse, right heart enlargement, and a patent foramenovale with significant right-to-left shunting.

1100 CASE REPORT LOFTUS ET AL Ann Thorac SurgFLAIL TRICUSPID VALVE IN THE NEONATE 2014;98:1098–101
FEATUREARTIC
LES
The initial management of each patient included ox-ygen supplementation and PGE2 administration. In thefirst patient, this combination was sufficient to reducepulmonary vascular resistance and provide hemody-namic stabilization before operative repair. In the secondpatient, milrinone, NO, and packed red blood cells were
Fig 1. Images of the tricuspid valve in the 4-chamber view, using transthor(A, C, E) before and (B, D, F) after tricuspid valve repair.
necessary for stabilization. The third patient was mini-mally responsive to these measures and required ECMOin the preoperative period. The repair in each patientwas done using Prolene and Gore-Tex sutures withpledgets to provide support for the flail leaflet [3, 4]. Atthe time of follow-up (1 to 3 years), echocardiography
acic echocardiography with color Doppler, are shown for each patient

1101Ann Thorac Surg CASE REPORT MAKHIJA ET AL2014;98:1101–4 SINGLE-STAGE ANATOMIC CORRECTION OF CCTGA
demonstrated only trivial TV regurgitation in allpatients.
Potential causes of flail TV in the neonate includecongenital endocarditis, ischemia induced by prematureductal closure, maternal autoimmune disease, birthasphyxia, a thromboembolic event, or traumatic ruptureduring the birth process [1, 2, 5]. The anterior papillarymuscle is typically injured because of its location within awatershed area and its requirement for perfusion duringdiastole when systemic right ventricular pressures arereached [2]. No signs or history of maternal autoimmunedisease, sepsis, or the use of prostaglandin synthase in-hibitors were noted in any of the neonates in our series.There was no obvious indication of prenatal ischemia orreport of significant trauma or asphyxia at birth. Giventhat the etiology of flail TV is often unknown, an under-standing of the early signs of flail TV, recognition ofechocardiographic findings, and knowledge of stabiliza-tion methods is extremely important in the managementof this rare but potentially fatal condition.
FEATUREARTIC
LES
References
1. Sachdeva R, Fiser RT, Morrow WR, Cava JR, Ghanayem NS,Jaquiss RDB. Ruptured tricuspid valve papillary muscle: atreatable cause of neonatal cyanosis. Ann Thorac Surg 2007;83:680–2.
2. Arrington CB, Kouretas PC, Mart CR. Extracorporeal mem-brane oxygenation as a bridge to surgical treatment of flailtricuspid valve in a neonate. Cardiol Young 2005;15:660–2.
3. Boon R, Hruda J, Schoof PH. Repair of ruptured tendinouschords in the newborn with flail tricuspid valve and functionalpulmonary atresia. Int J Card 2007;116:e78–9.
4. Anagnostopoulos PV, Alphonso N, Nolke L, et al. Neonatalmitral and tricuspid valve repair for in utero papillary musclerupture. Ann Thorac Surg 2007;83:1458–62.
5. Kaulitz R, Haen S, Sieverding L, Ziemer G. Intrauterinerupture of anterior tricuspid valve papillary muscle: tricuspidvalve chordae replacement on the first day of life. J ThoracCardiovasc Surg 2012;143:241–3.
One-Stage MidlineUnifocalization and AnatomicCorrection of CorrectedTransposition With PulmonaryAtresia and Absence of CentralPulmonary ArteriesZeena Makhija, MD, Smita Mishra, MD,Apoorva Goel, MD, and Rajesh Sharma, MCh
Division of Congenital Cardiac Surgery, Department of PediatricCardiology, and Department of Radiology, Fortis Escorts HeartResearch Institute, Delhi, India
A concomitant double-switch procedure and uni-focalization were performed in a child with congenital
Accepted for publication Oct 22, 2013.
Address correspondence to Dr Makhija, Fortis Escorts Heart ResearchInstitute, New Delhi, India; e-mail: [email protected].
� 2014 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
corrected transposition of the great arteries, ventricularseptal defect, pulmonary atresia, absence of central pul-monary arteries and major aortopulmonary collateral ar-teries. Predischarge echocardiography showed noresidual shunts with laminar flow in baffles and outflowtracts. Follow-up computed tomographic angiographyrevealed good neo—main pulmonary artery confluencewith satisfactory pulmonary blood flow.
(Ann Thorac Surg 2014;98:1101–4)� 2014 by The Society of Thoracic Surgeons
he advantages of anatomic repair of congenitally
Tcorrected transposition of the great arteries (CCTGA)over conventional repair are well described in the litera-ture, as are also those of one-stage unifocalization of themajor aortopulmonary collateral arteries (MAPCAS) inpatients with absence of central pulmonary arteries [1, 2].The operation described here brings together boththese sets of advantages and, in our opinion, despite itscomplexity, provides the ideal result in this complicatedassociation.To the best of our knowledge, there has been no report
so far of single-stage repair of CCTGA, ventricular septaldefect (VSD), and pulmonary atresia (PA) with MAPCAs.
A 1-year-old boy with a history of recurrent respiratorytract infections and failure to thrive was referred to us forfurther evaluation and management. Transthoracicechocardiography revealed dextrocardia, atrioventriculardiscordance, and aorta arising from the right ventricle(RV). A large inlet VSD was present, which seemednonroutable to an anteriorly placed aorta. Single-outletpulmonary atresia was present. The child had MAPCAs,which were further profiled on computed tomographic(CT) pulmonary angiography. CT confirmed atresia of themain pulmonary artery and absence of the central branchpulmonary arteries (Figs 1, 2). The child was scheduledfor elective complete intracardiac repair.A median sternotomy was used for access. The thymus
was excised, and a pericardial patch was obtained andtreated with 6% gluteraldehyde. The collaterals weredissected up to their lobar branches and looped. Cannu-lation of the aorta, inferior vena cava, and right atriumwas done, and cardiopulmonary bypass (CPB) wascommenced. The patient was cooled to 26�C. The collateralflow was restricted by the application of occlusive clips.The collaterals were sequentially ligated at their aorticends by use of a transfixation Prolene suture in addition tosilk ties. The stenosed collateral supplying the right lowerlobe was patched with untreated autologous pericardium.The superior and inferior collaterals draining the left lungwere anastomosed to each other, as were the collaterals onthe right side to create a neo—left pulmonary artery and aneo—right pulmonary artery. The right and left neo–pul-monary arteries so created were joined across the midlineto create neo–pulmonary artery confluence by suturingtheir posterior walls together.The heart was fibrillated at this stage, and the left
atrium was vented through the right superior pulmonary
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.10.091