Embed Size (px)
Citation preview

NeoadjuvantChemotherapyfor Ca Breast
CY Choi
UCH
JHSGR Sep 2004
Synonyms
Primary chemotherapyPrimary chemotherapy NeoadjuvantNeoadjuvant chemotherapy chemotherapy Induction chemotherapyInduction chemotherapy Preoperative chemotherapyPreoperative chemotherapy
JHSGR Sep 2004
Development
IndicationsIndications:: Inoperable Ca breastInoperable Ca breast Locally advanced Ca breastLocally advanced Ca breast Large operable Ca breastLarge operable Ca breast ? All Biopsy confirmed invasive Ca breast? All Biopsy confirmed invasive Ca breast
JHSGR Sep 2004
Advantages
1.1. tumour size and allow tumour size and allow breast conservationbreast conservation
2.2. evaluate evaluate chemoresponsivenesschemoresponsiveness of tumour of tumour
3.3. effectiveness of systemic treatment for effectiveness of systemic treatment for micrometastasismicrometastasis
4.4. stimulation of metastatic cancer cell by tumour stimulation of metastatic cancer cell by tumour excisionexcision
5.5. May turn off surgically induced growth factorsMay turn off surgically induced growth factors
6.6. Treat Treat LNLN, , axillary dissection axillary dissection
JHSGR Sep 2004
Disadvantages
1.1. May treat in situ disease(if only FNA done)May treat in situ disease(if only FNA done)2.2. ability of pathology to act as ability of pathology to act as prognosticprognostic
indicatorindicator3.3. ability of surgical ability of surgical assessment of original assessment of original
tumourtumour after chemotherapy after chemotherapy4.4. ability to evaluate axillary LN statusability to evaluate axillary LN status5.5. ability to evaluate biologic characteristics ability to evaluate biologic characteristics
of tumourof tumour
JHSGR Sep 2004
Review
LiteratureLiterature
Chemotherapy RegimeChemotherapy Regime
Treatment of axillaTreatment of axilla
JHSGR Sep 2004
Response to chemotherapy
ClassificationClassification
complete response complete response (( 100%) 100%)
partial response partial response ((>50%)>50%)
static diseasestatic disease
disease progression disease progression ((>25%)>25%)
JHSGR Sep 2004
Predictors of response to primary chemotherapy pCR is good prognostic factorpCR is good prognostic factor for disease for disease
free and overall survivalfree and overall survival pCR is predictive of complete axillary LN pCR is predictive of complete axillary LN
responseresponse pCR more seen in ER-, anaplastic, small pCR more seen in ER-, anaplastic, small
size tumoursize tumourKuerer, McMasters. J Clin Oncol 1999Kuerer, McMasters. J Clin Oncol 1999
JHSGR Sep 2004
Perioperative management
MarkMark the tumour before chemotherapy the tumour before chemotherapy MonitorMonitor tumour response regularly tumour response regularly Residual mass in mammogram and USG may not Residual mass in mammogram and USG may not
be viable tissue, ?role of MRI be viable tissue, ?role of MRI (Cancer 1996)(Cancer 1996)
Well planned surgeryWell planned surgery Resection marginResection margin Tumour/breast size ratioTumour/breast size ratio Extent of microcalcificationsExtent of microcalcifications

Evidence
JHSGR Sep 2004
NSABP-B18 J Clin Oncol 1998
RCT (RCT (PreopPreop vs vs PostopPostop chemotherapy) chemotherapy)
doxorubicin/cyclophosphamide x 4 coursesdoxorubicin/cyclophosphamide x 4 courses
1523 F1523 F
Stage I/II/III Breast cancer (Tumour size 2-5cm Stage I/II/III Breast cancer (Tumour size 2-5cm
60%, >5cm 13%)60%, >5cm 13%)
FU 5yrFU 5yr
JHSGR Sep 2004
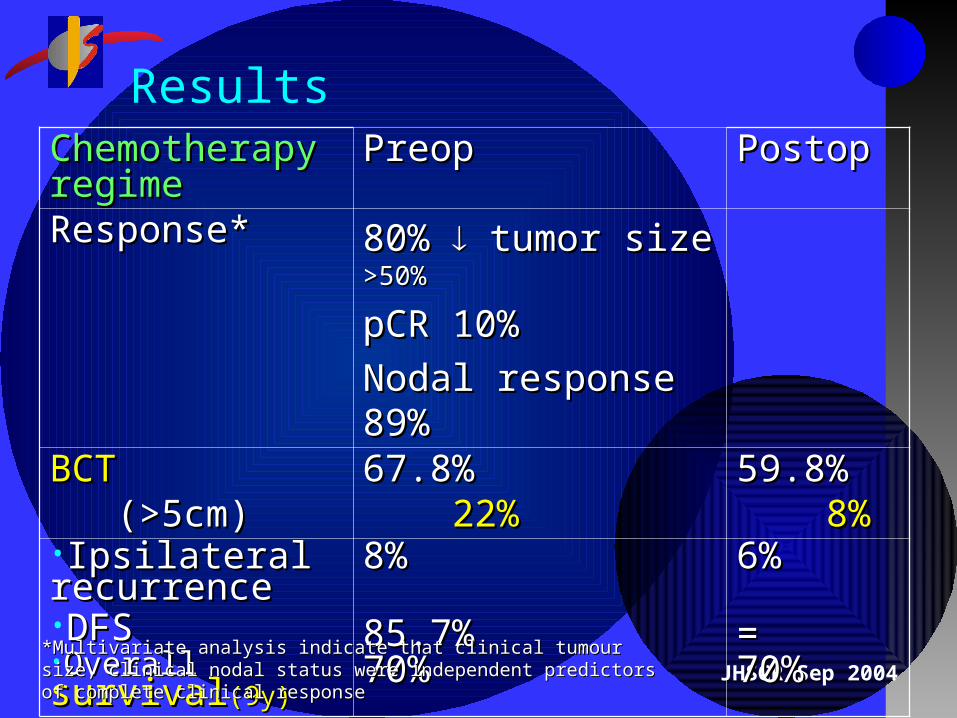
ResultsChemotherapy Chemotherapy regimeregime
PreopPreop PostopPostop
Response*Response* 80% 80% tumor size tumor size >50%>50%
pCR 10%pCR 10%
Nodal response 89%Nodal response 89%
BCTBCT (>5cm)(>5cm)
67.8%67.8% 22%22%
59.8%59.8% 8%8%
•Ipsilateral Ipsilateral recurrencerecurrence•DFSDFS•Overall Overall survivalsurvival(9y)(9y)
8%8%
85.7%85.7%70%70%
6%6%
==70%70%
*Multivariate analysis indicate that clinical tumour size, clinical nodal status were *Multivariate analysis indicate that clinical tumour size, clinical nodal status were independent predictors of complete clinical responseindependent predictors of complete clinical response
JHSGR Sep 2004
Bordeaux Study Annals of Oncology 1999
RCT (single institution)RCT (single institution) MRM +/- adjuvant chemo vs MRM +/- adjuvant chemo vs Primary chemo+ surgeryPrimary chemo+ surgery(mastectomy >2cm, BCT+RT (mastectomy >2cm, BCT+RT
<2cm)<2cm) Chemotherapy regime:Chemotherapy regime:
3 cycles of epirubicin, vincristine, methotrexate, 3 cycles of epirubicin, vincristine, methotrexate, then 3 cycles of mitomycin C, thiotepa, vindesinethen 3 cycles of mitomycin C, thiotepa, vindesine
272F272F Clinical T>3cmClinical T>3cm Median FU: 124monthsMedian FU: 124months
JHSGR Sep 2004
ResultsResults Preop chemotherapyPreop chemotherapy
BCT possible in 45%BCT possible in 45%More local recurrencesMore local recurrencesSimilar survivalSimilar survival
LimitationLimitation Treatment arms not really balancedTreatment arms not really balanced
JHSGR Sep 2004
Milan trials J Clin Oncol 1998
Prospective (Prospective (nonRCTnonRCT)) Chemotherapy regimeChemotherapy regime
3-4 cycles of CMF / FAC / FEC / FNC / adriamycin3-4 cycles of CMF / FAC / FEC / FNC / adriamycin 536F536F T>2.5cmT>2.5cm Median age 49Median age 49 Median FU 65 monthsMedian FU 65 months ResultsResults
Overall response 76% - cCR 16%Overall response 76% - cCR 16% - pCR 3%- pCR 3% - PR 60%- PR 60% Stable disease 5%Stable disease 5% Minor response(<50% reduction) 16%Minor response(<50% reduction) 16% Progressive disease 5%Progressive disease 5%
JHSGR Sep 2004
BCT possibleBCT possible in 85%(in 62% patients with in 85%(in 62% patients with tumour >5cm)tumour >5cm)
Local relapse after BCT 6.8%Local relapse after BCT 6.8% Response Response in receptor –ve tumour, unrelated to in receptor –ve tumour, unrelated to
age, menopausal status, chemo regimenage, menopausal status, chemo regimen Multivariate analysis showed response to primary Multivariate analysis showed response to primary
chemo and axillary LN involvement correlate with chemo and axillary LN involvement correlate with disease free survivaldisease free survival
JHSGR Sep 2004
NSABP-B 27 Just closed
Randomised to preop chemotherapyRandomised to preop chemotherapy Gp 1 AC+ TAM -> surgeryGp 1 AC+ TAM -> surgery Gp 2 AC+ TAM -> Gp 2 AC+ TAM -> taxotere taxotere -> surgery-> surgery Gp 3 AC+ TAM -> surgery-> taxotereGp 3 AC+ TAM -> surgery-> taxotere
cT1-3, N0-1cT1-3, N0-1 2411F2411F Results: Results:
no difference in BCT (60%)no difference in BCT (60%) Gp 2 increase pCR(26.1 vs 13.7%)Gp 2 increase pCR(26.1 vs 13.7%)
Pending 5 yr survival 2005Pending 5 yr survival 2005
JHSGR Sep 2004
EORTC 10902 J Clin Oncol 2001
RCT (RCT (Preop Preop vsvs Postop Postop chemotherapy) chemotherapy) 4 cycles of 5FU, Epirubicin, cyclophosphamide4 cycles of 5FU, Epirubicin, cyclophosphamide 698698F (Yr 1991-1999)F (Yr 1991-1999) (T1c, T2, 3, 5b, N0, 1 and M0)(T1c, T2, 3, 5b, N0, 1 and M0) Median FU 56mosMedian FU 56mos Results:Results:
No difference in OS, PFS, LRRNo difference in OS, PFS, LRR 23% downstaged23% downstaged
JHSGR Sep 2004
Chemotherapy Regime Which has Which has Response Rate Response Rate ? ? Primary chemotherapy with doxorubicin Primary chemotherapy with doxorubicin
and docetaxel is well tolerated and highly and docetaxel is well tolerated and highly activeactive
TaxaneTaxane to to pCR comparing with FAC pCR comparing with FAC Sequential treatmentSequential treatment schedule is a little schedule is a little
more active than combination therapy, but a more active than combination therapy, but a higher toxicityhigher toxicity
JHSGR Sep 2004
Role of Sentinel LN biopsy or axillary dissection Incidence of histological negative axillary LN 37% greater Incidence of histological negative axillary LN 37% greater
- - NSABP B-18NSABP B-18
23% has 23% has histological conversionhistological conversion from + to from + to – (MD Anderson)– (MD Anderson)
Can axillary irradiation replace ALNDCan axillary irradiation replace ALND in patients in patients
downstaged from node + to – ?downstaged from node + to – ?
Axillary irradiation without axillary LN dissection may Axillary irradiation without axillary LN dissection may
provide adequate local control in patients with at least a provide adequate local control in patients with at least a
partial response. partial response. Lenert JT. Ann Surg Oncol 99 Lenert JT. Ann Surg Oncol 99
Buzdar AU, J Clin Buzdar AU, J Clin
Oncol 99.Oncol 99.
JHSGR Sep 2004
SLN
Small sample size, Variable results for SLN Small sample size, Variable results for SLN identification and FN finding(1-11%)identification and FN finding(1-11%)
SLNB is reliable for accurate staging of SLNB is reliable for accurate staging of axillaaxilla in advanced Ca breast in advanced Ca breast Haid A. Cancer 2001Haid A. Cancer 2001
SLN accurately predict axillary LN status in SLN accurately predict axillary LN status in 96% patients(325/340) 96% patients(325/340) ASCO Annual meeting 2002ASCO Annual meeting 2002
FN rateFN rate 9% 9% NSABP B27NSABP B27 4.3% 4.3% MD Anderson CCMD Anderson CC
JHSGR Sep 2004
Conclusion Neoadjuvant chemotherapy Neoadjuvant chemotherapy
breast conservationbreast conservation survival benefitsurvival benefit
Recommended for Recommended for Stage II, IIIStage II, III Ca breast Ca breast ?extrapolate to early Ca breast?extrapolate to early Ca breast Prognostic value of axillary LNPrognostic value of axillary LN Accuracy of SLNBAccuracy of SLNB not affected not affected Study on QOLStudy on QOL