Embed Size (px)
Citation preview

Neo-adjuvant
TreatmentTreatment
SABCS 2011
Carlos H. Barrios, MDInstituto do Câncer HMD
Faculdade de Medicina PUCRSPorto Alegre, Brazil

Response to the Same DrugsDiffers by Subtype
Modified PAM50 subtyping in 360 patients treated with neo-adjuvant anthracycline/taxane chemotherapy (no Trastuzumab)
Overall pCR rate = 22%
Classification Residual disease pCR
Basal-like 47 (58%) 34 (42%)
Claudin-low 29 (67%) 14 (33%)
HER2-enriched 31 (63%) 18 (37%)
Luminal A 110 (98%) 2 (2%)
Luminal B 56 (85%) 10 (15%)
Normal-like 13 (76%) 4 (24%)
Perou C, et al. 2011
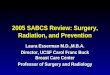
TRYPHAENA - Study design
HER2-positive EBC centrally confirmed(n = 225)
FEC
SURG
SURG
Docetaxel
Cycles 1 ‒3 4‒6
PertuzumabPertuzumab
Pertuzumab + trastuzumab
FECDocetaxel
B
A
(n = 225)GERY
GERY
Pertuzumab+ trastuzumab
Carboplatin
Docetaxel
Pertuzumab + trastuzumabC
Study dosing q3w:− FEC: 500 mg/m2, 100 mg/m2, 600 mg/m2− Carboplatin: AUC 6− Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintena nce− Pertuzumab: 840 mg loading dose, 420 mg maintenance− Docetaxel: 75 mg/m2 (escalating to 100 mg/m2 if to lerated, in Arms A and B only)
Schneeweiss A, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-6.
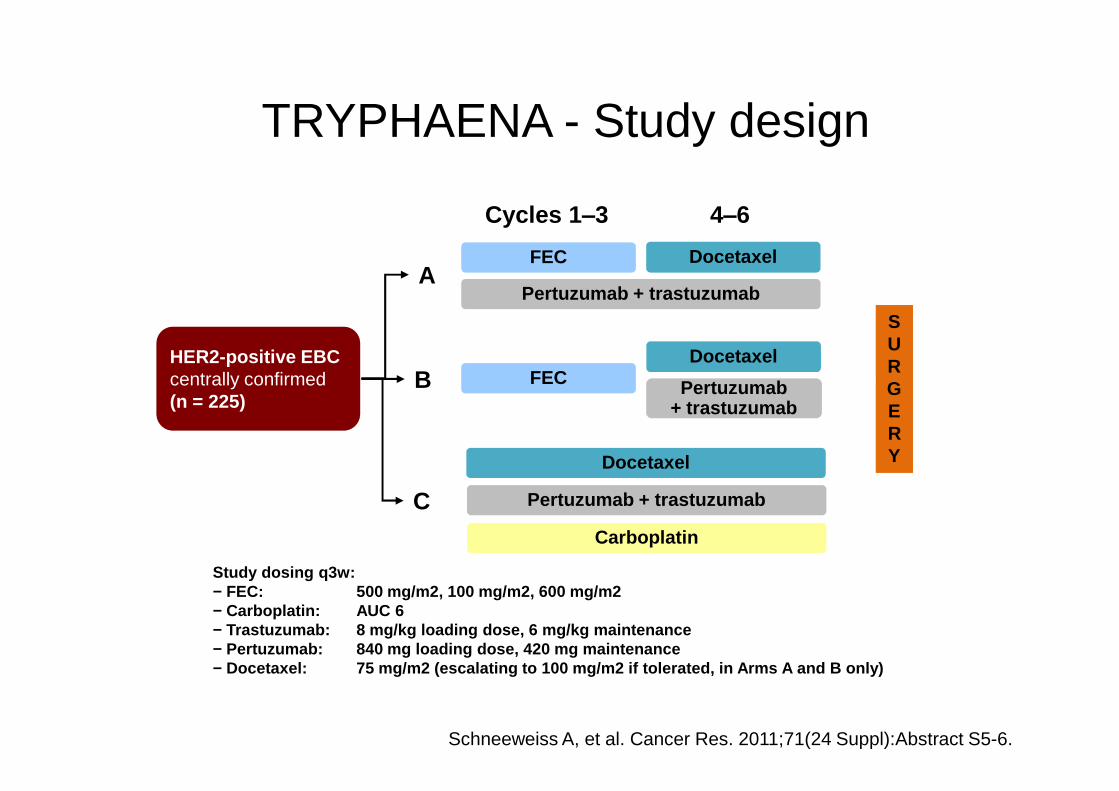
TRYPHAENA: Study endpoints
• Primary endpoint :– Cardiac safety
• Symptomatic LVSD (grade ≥3)• LVEF declines (≥10 percentage points and below 50%)
• Secondary endpoints :• Secondary endpoints :– Toxicity– pCR (defined as the absence of invasive tumor residues in the
breast at surgery; remaining in situ lesions allowed; ypT0/is)• Study was not powered for formal comparison between arms
– Clinical response rate– Rate of breast-conserving surgery
Schneeweiss A, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-6.
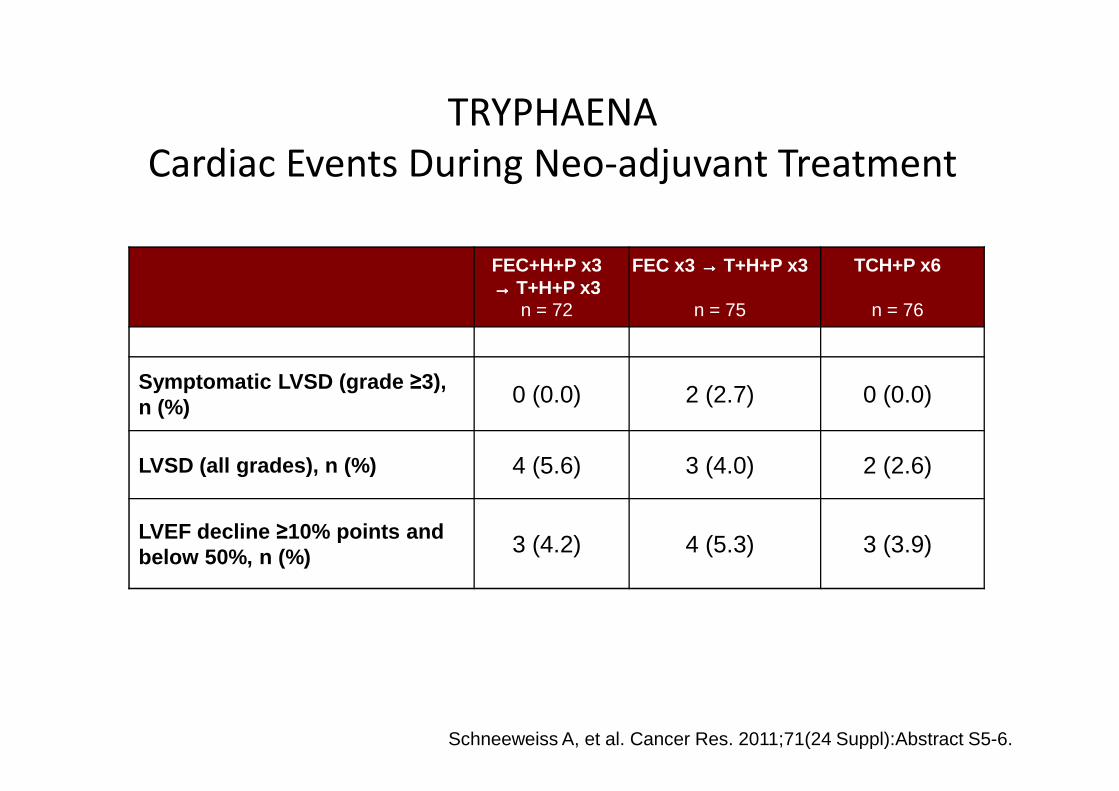
TRYPHAENA
Cardiac Events During Neo-adjuvant Treatment
FEC+H+P x3→→→→ T+H+P x3
n = 72
FEC x3 →→→→ T+H+P x3
n = 75
TCH+P x6
n = 76
Symptomatic LVSD (grade ≥3),n (%) 0 (0.0) 2 (2.7) 0 (0.0)n (%) 0 (0.0) 2 (2.7) 0 (0.0)
LVSD (all grades), n (%) 4 (5.6) 3 (4.0) 2 (2.6)
LVEF decline ≥10% points and below 50%, n (%) 3 (4.2) 4 (5.3) 3 (3.9)
Schneeweiss A, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-6.
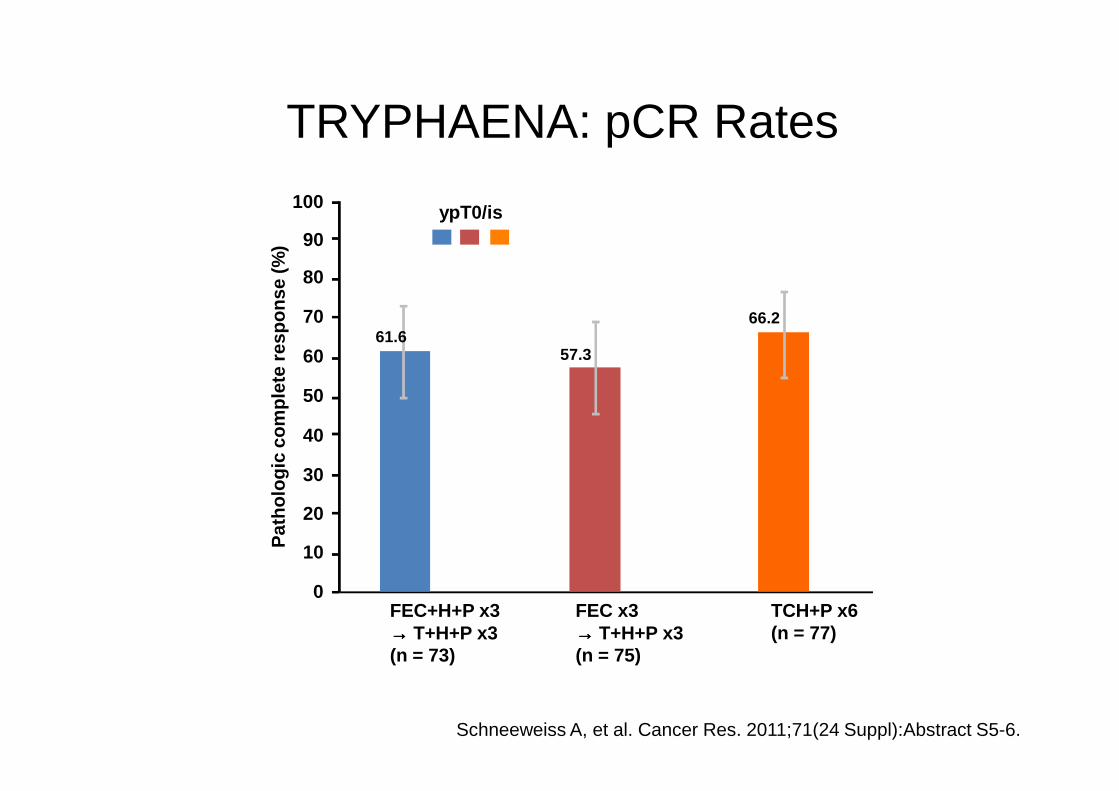
TRYPHAENA: pCR Rates
Pat
holo
gic
com
plet
e re
spon
se (%
)
ypT0/is100
90
80
70
60
50
61.666.2
57.3
Pat
holo
gic
com
plet
e re
spon
se (%
)
FEC+H+P x3→→→→ T+H+P x3(n = 73)
FEC x3→→→→ T+H+P x3(n = 75)
TCH+P x6(n = 77)
50
40
30
20
10
0
Schneeweiss A, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-6.
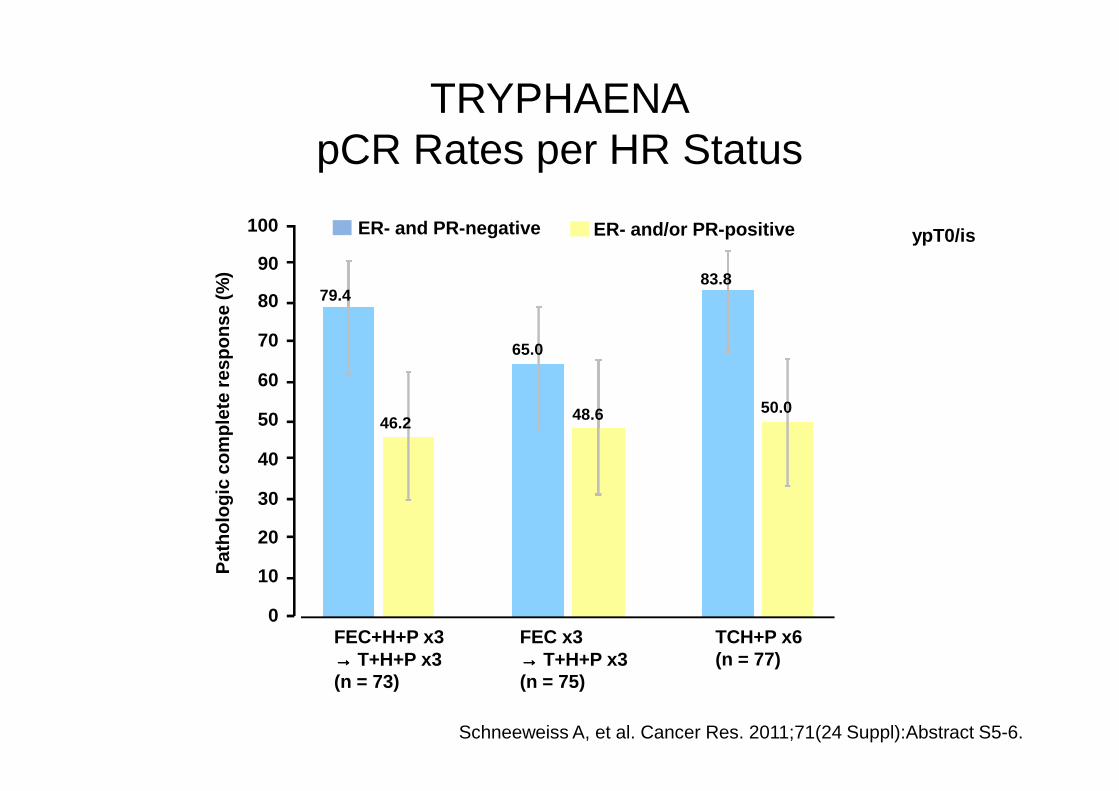
TRYPHAENApCR Rates per HR Status
Pat
holo
gic
com
plet
e re
spon
se (%
)ER- and PR-negative ER- and/or PR-positive
79.4
65.0
83.8
ypT0/is100
90
80
70
60
Pat
holo
gic
com
plet
e re
spon
se (%
)
46.2 48.6 50.0
FEC+H+P x3→→→→ T+H+P x3(n = 73)
FEC x3→→→→ T+H+P x3(n = 75)
TCH+P x6(n = 77)
50
40
30
20
10
0
Schneeweiss A, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-6.
TRYPHAENA: Summary
• Combination of trastuzumab and pertuzumab with anthracycline containing chemotherapy is feasible
• Cardiac toxicity is similar for concomitant or sequential administration of the two monoclonal antibodies with anthracyclines (as judged from early cardiac events)
• pCR rates higher than in NeoSphere suggest role for the longer 6-cycles treatment duration and/or for use with combination chemotherapy
• pCR rates consistently higher for ER negative tumors
• TRYPHAENA supports the ongoing APHINITY study (NCT01358877), a phase III trial to evaluate pertuzumab and trastuzumab plus standard chemotherapy in the adjuvant setting
Schneeweiss A, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-6.

Dual HER2 blockade alone or with chemotherapy (or with more chemotherapy?)
80
100
(Neo-Sphere, Neo-Altto, Tryphaena)
63%
pC
R R
ate
Dual HER2
blockade
+
Taxane
Dual HER2
blockade
+
Taxane
50%
20
40
60
Dual HER2
blockade alone
Dual HER2
blockade alone
17%
Dual HER2 blockade
+Taxane
+Other agent(anthrac., carbo)
63%
%p
CR
Ra
te
Neo ALTTO
N=450
Regimen pCR
Trastuzumab
+ Lapatinib
+ Docetaxel
51%
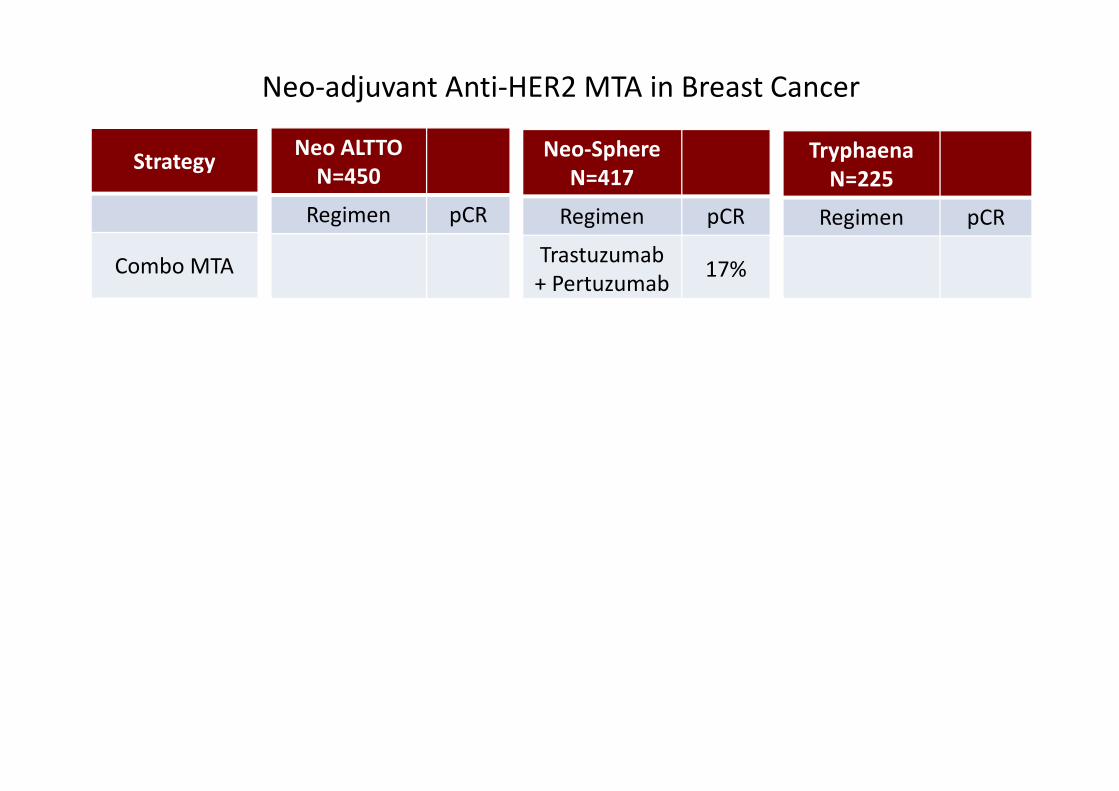
Neo-Sphere
N=417
Regimen pCR
Trastuzumab
+ Pertuzumab17%
Trastuzumab
+ Pertuzumab
+ Docetaxel
46%
Tryphaena
N=225
Regimen pCR
Trastuzumab
+ Pertuzumab
+ Doce/Carbo
66%
Strategy
Combo MTA
Combo MTA +
Chemotherapy
Neo-adjuvant Anti-HER2 MTA in Breast Cancer
+ Docetaxel
Trastuzumab
+ Paclitaxel29%
Lapatinib
+ Paclitaxel25%
+ Docetaxel
Trastuzumab
+ Docetaxel29%
Pertuzumab
+ Docetaxel24%
+ Doce/Carbo
Trastuzumab
+ Pertuzumab
FEC-Docetax
Sequential
Concomitant
57%
62%
Combo MTA +
Chemotherapy
Trastuzumab +
Chemotherapy
Single MTA +
Chemotherapy
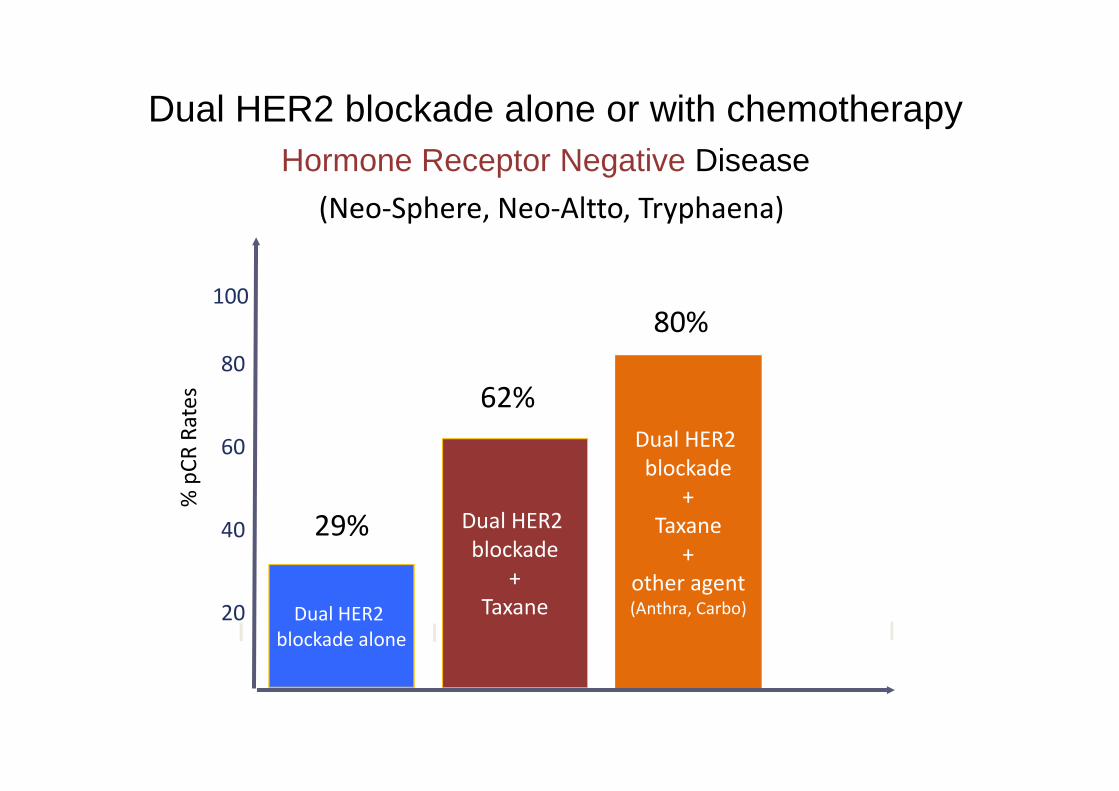
Hormone Receptor Negative Disease
62%
80
100
80%
% p
CR
Ra
tes
Dual HER2 blockade alone or with chemotherapy
(Neo-Sphere, Neo-Altto, Tryphaena)
Dual HER2
blockade
+
Taxane
62%
20
40
60
Dual HER2
blockade alone
29%
Dual HER2
blockade
+
Taxane
+
other agent(Anthra, Carbo)
% p
CR
Ra
tes

80
100 These somewhat « less impressive »results could still translate
into excellent DFS rates (?)
Hormone Receptor Positive Disease
Dual HER2 blockade alone or with chemotherapy
(Neo-Sphere, Neo-Altto, Tryphaena, Chang’s Trial)
% p
CR
Ra
tes
7.2
Trastuzumab
+
Pertuzumab
+
Taxane
26%
20
40
60
Dual HER2
blockade alone
6%
Trastuzumab
+
Lapatinib
+
Taxane
42%
Trastuzumab
+
FEC
and
Taxane
47%
Trastuzumab
+
Pertuzumab
+
Docetaxel
+
Carboplatin
21%
50%
Trastuzumab
+ Lapatinib
+ A.I.
Trastuzumab
+ Lapatinib
+ A.I.
% p
CR
Ra
tes
Neo-adjuvant pertuzumab (P) and trastuzumab (H):
Biomarker analyses of a 4-arm randomized Phase II study
(NeoSphere) in patients (pts) with
HER2-positive breast cancer (BC)
L Gianni, G Bianchini, A Kiermaier, G Bianchi, Y.-H Im, T Pienkowski,
L Roman, M-C Liu, L-M Tseng, J Ratnayake, T Szado, G Ross, P Valagussa
on behalf of the ‘NeoSphere’ study investigators
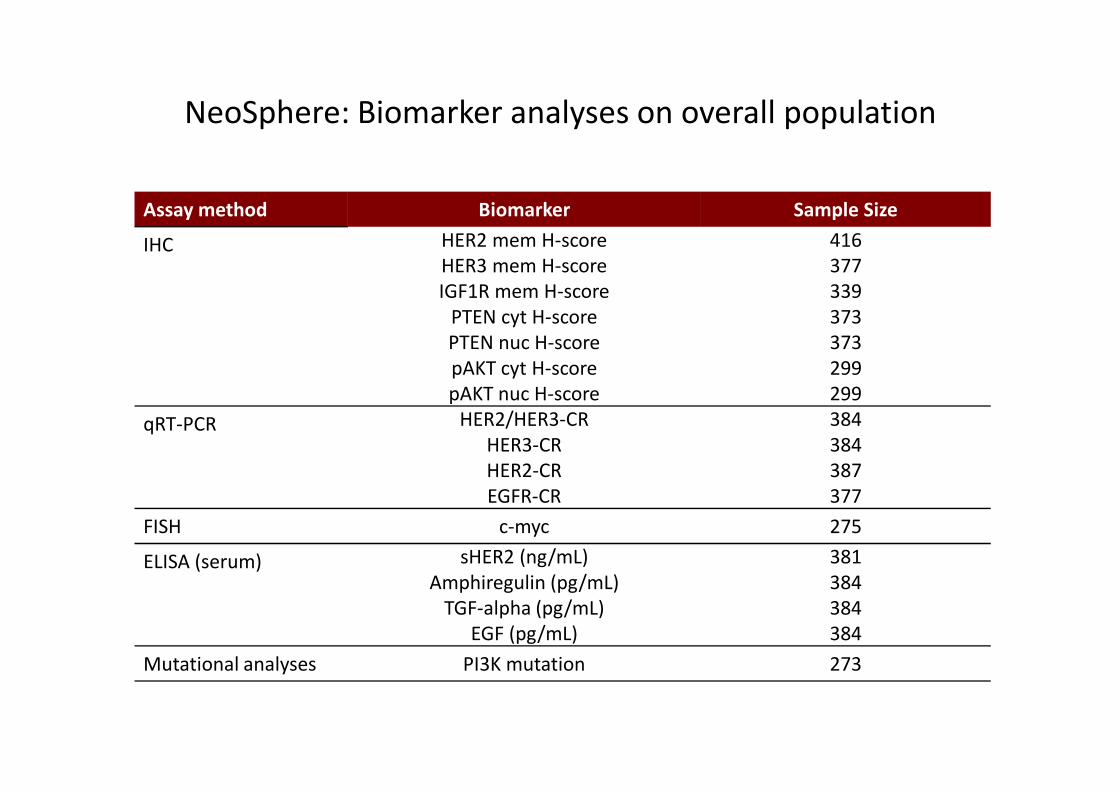
NeoSphere: Biomarker analyses on overall population
Assay method Biomarker Sample Size
IHC HER2 mem H-score 416
HER3 mem H-score 377
IGF1R mem H-score 339
PTEN cyt H-score 373
PTEN nuc H-score 373
pAKT cyt H-score 299
pAKT nuc H-score 299pAKT nuc H-score 299
qRT-PCR HER2/HER3-CR 384
HER3-CR 384
HER2-CR 387
EGFR-CR 377
FISH c-myc 275
ELISA (serum) sHER2 (ng/mL) 381
Amphiregulin (pg/mL) 384
TGF-alpha (pg/mL) 384
EGF (pg/mL) 384
Mutational analyses PI3K mutation 273
Summary of NeoSphere biomarker analyses
• HER2 expression (H-score) associated with sensitivity to
pertuzumab
• PI3K mutations in exon 9 linked to lack of sensitivity to HER2-
directed Mab’s
• Intrinsic differences between HER2+ tumors based on hormone • Intrinsic differences between HER2+ tumors based on hormone
receptor status
• No predictive role for truncated forms of the HER2 receptor
including p95HER2
• So far none of the analyses provided clinically useful assays for
patient and/or regimen selection in addition or alternative to the
conventional assessment of HER2 by IHC or FISH
2
GEPAR-TRIO trial
Neoadjuvant chemotherapy adapted by interim
response improves overall survival of primary breast
cancer patients
Results of the GeparTrio trial.
Gunter von Minckwitz, Jens Uwe Blohmer, Serban Dan Costa, Carsten Denkert, Holger Eidtmann, Wolfgang
Eiermann, Bernd Gerber, Claus Hanusch, Jörn Hilfrich, Jens Huober, Christian Jackisch, Manfred Kaufmann,
Sherko Kümmel, Stefan Paepke, Andreas Schneeweiss, Michael Untch, Dirk Michael Zahm, Keyur Mehta, Sibylle
Loibl
Courtesy of G. von Minckwitz. SABCS 2011
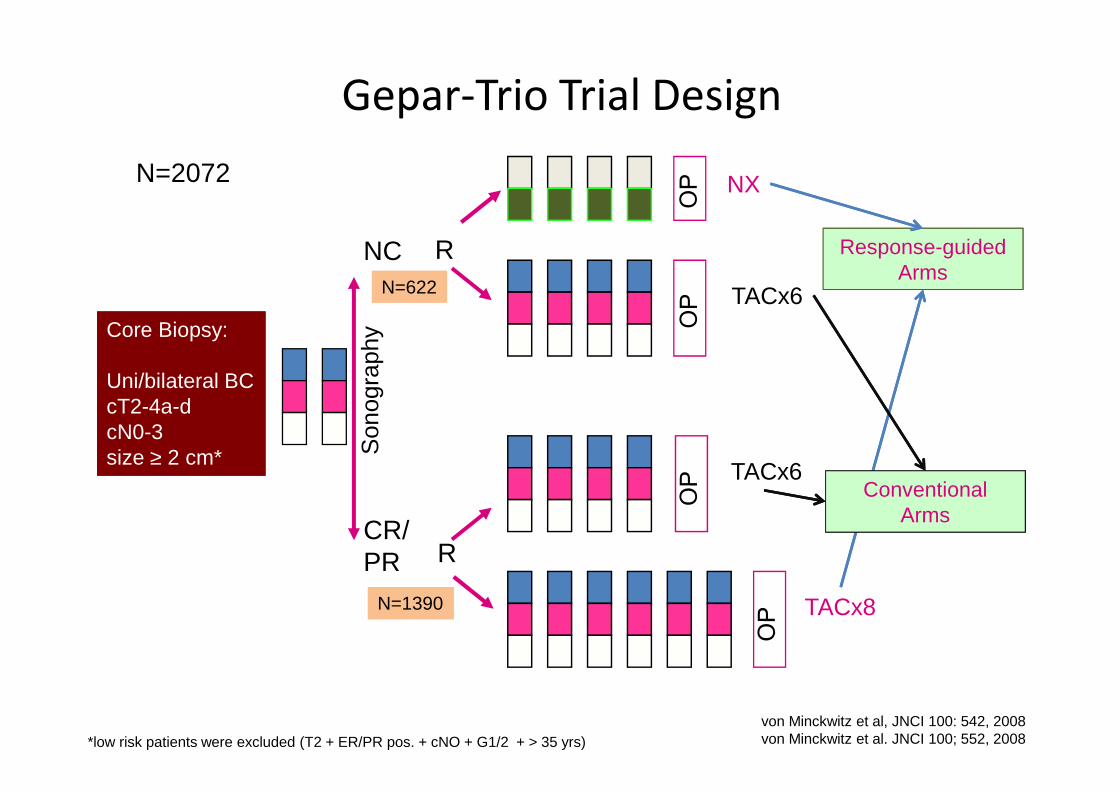
Core Biopsy:
Uni/bilateral BC cT2-4a-d
Core Biopsy:
Uni/bilateral BC cT2-4a-d
NC
Son
ogra
phy
NX
TACx6
R
Gepar-Trio Trial Design
N=2072
Response-guidedArms
N=622
cT2-4a-dcN0-3size ≥ 2 cm*
cT2-4a-dcN0-3size ≥ 2 cm*
CR/PR
Son
ogra
phy
TACx8
TACx6
R
*low risk patients were excluded (T2 + ER/PR pos. + cNO + G1/2 + > 35 yrs)von Minckwitz et al, JNCI 100: 542, 2008von Minckwitz et al. JNCI 100; 552, 2008
Conventional Arms
N=1390N=1390
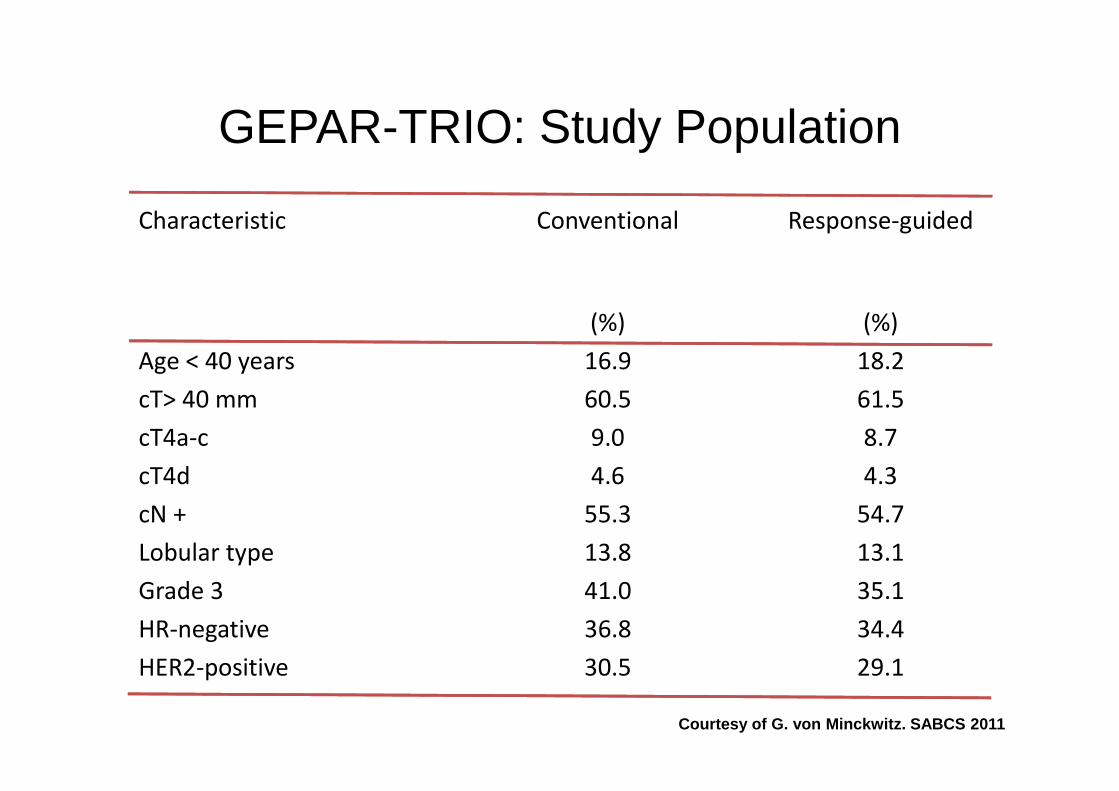
GEPAR-TRIO: Study Population
Characteristic Conventional Response-guided
(%) (%)
Age < 40 years 16.9 18.2
cT> 40 mm 60.5 61.5cT> 40 mm 60.5 61.5
cT4a-c 9.0 8.7
cT4d 4.6 4.3
cN + 55.3 54.7
Lobular type 13.8 13.1
Grade 3 41.0 35.1
HR-negative 36.8 34.4
HER2-positive 30.5 29.1
Courtesy of G. von Minckwitz. SABCS 2011
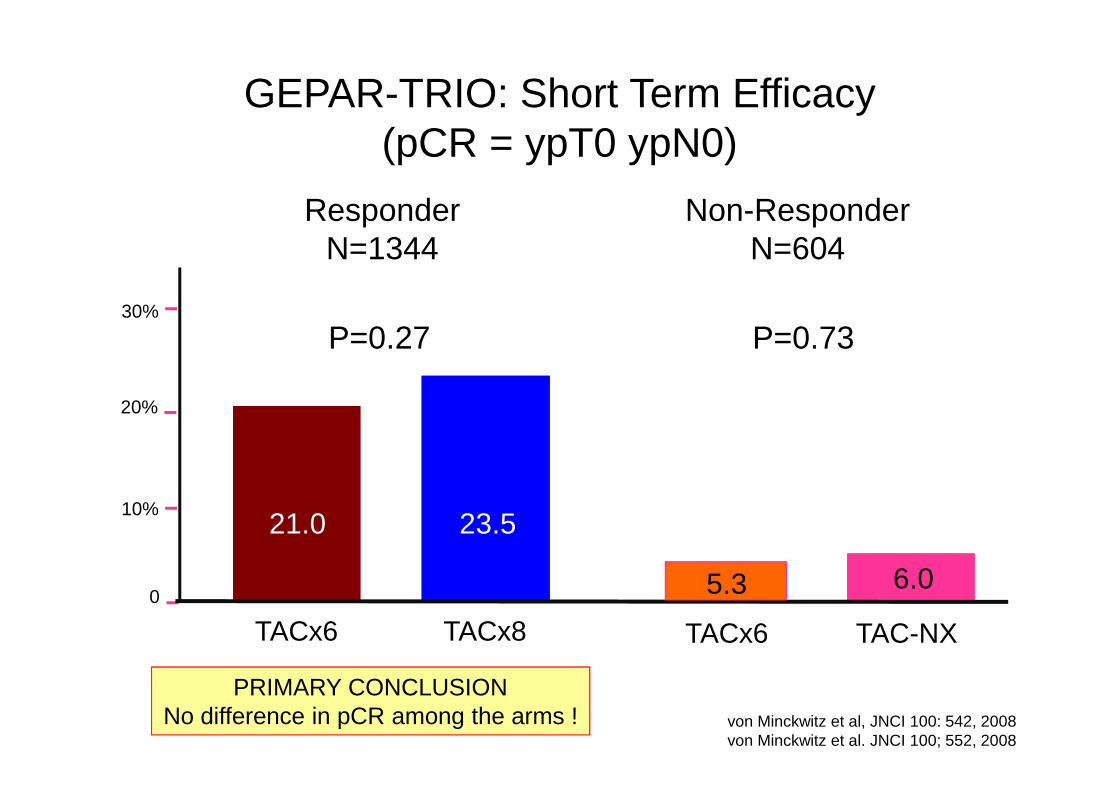
GEPAR-TRIO: Short Term Efficacy (pCR = ypT0 ypN0)
Non-ResponderN=604
ResponderN=1344
P=0.73P=0.2730%
6.06.0
20%
0
TAC-NXTACx6
23.5
TACx6 TACx8
21.0
5.3
10%
von Minckwitz et al, JNCI 100: 542, 2008von Minckwitz et al. JNCI 100; 552, 2008
PRIMARY CONCLUSIONNo difference in pCR among the arms !

Core Biopsy:
Uni/bilateral BC cT2-4a-d
Core Biopsy:
Uni/bilateral BC cT2-4a-d
NC
Son
ogra
phy
NX
TACx6
R
Gepar-Trio Trial Design
N=2072
Response-guidedArms
N=622
cT2-4a-dcN0-3size ≥ 2 cm*
cT2-4a-dcN0-3size ≥ 2 cm*
CR/PR
Son
ogra
phy
TACx8
TACx6
R
*low risk patients were excluded (T2 + ER/PR pos. + cNO + G1/2 + > 35 yrs)von Minckwitz et al, JNCI 100: 542, 2008von Minckwitz et al. JNCI 100; 552, 2008
Conventional Arms
N=1390N=1390
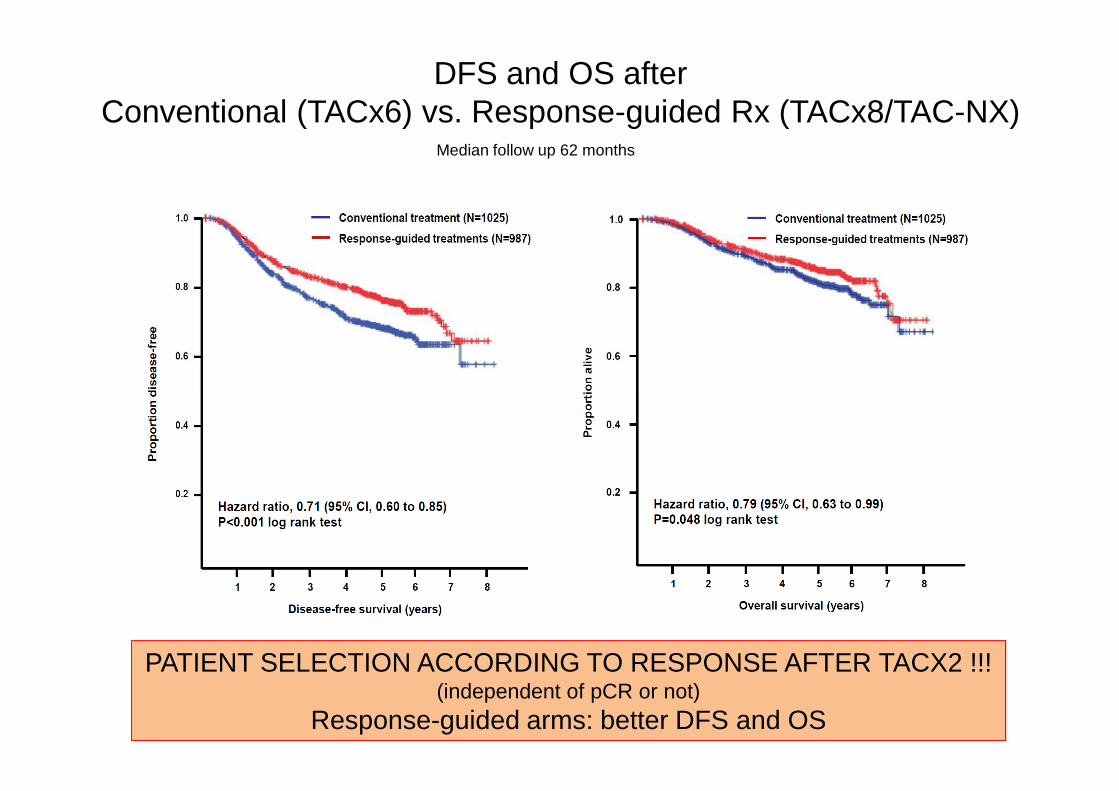
DFS and OS after Conventional (TACx6) vs. Response-guided Rx (TACx8/TAC-NX)
Median follow up 62 months
Courtesy of G. von Minckwitz. SABCS 2011
PATIENT SELECTION ACCORDING TO RESPONSE AFTER TACX2 !!!(independent of pCR or not)
Response-guided arms: better DFS and OS
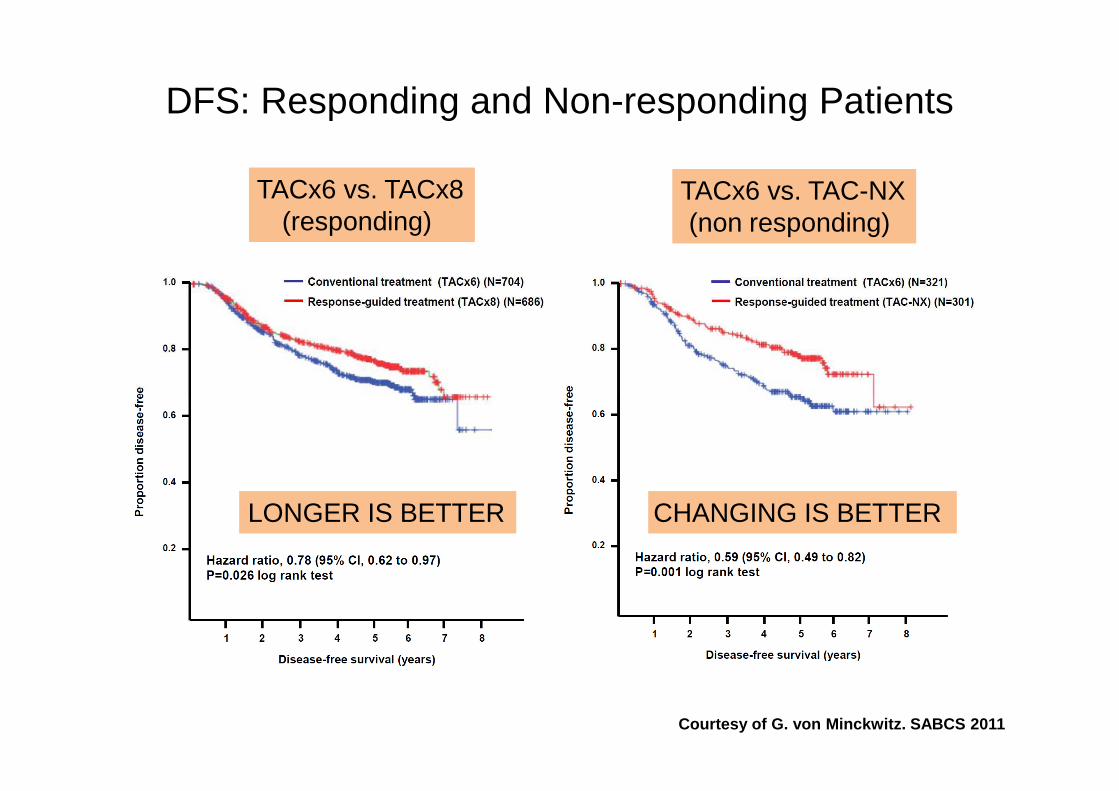
DFS: Responding and Non-responding Patients
TACx6 vs. TACx8(responding)
TACx6 vs. TACx8(responding)
TACx6 vs. TAC-NX(non responding)
TACx6 vs. TAC-NX(non responding)
Courtesy of G. von Minckwitz. SABCS 2011
LONGER IS BETTERLONGER IS BETTER CHANGING IS BETTER CHANGING IS BETTER
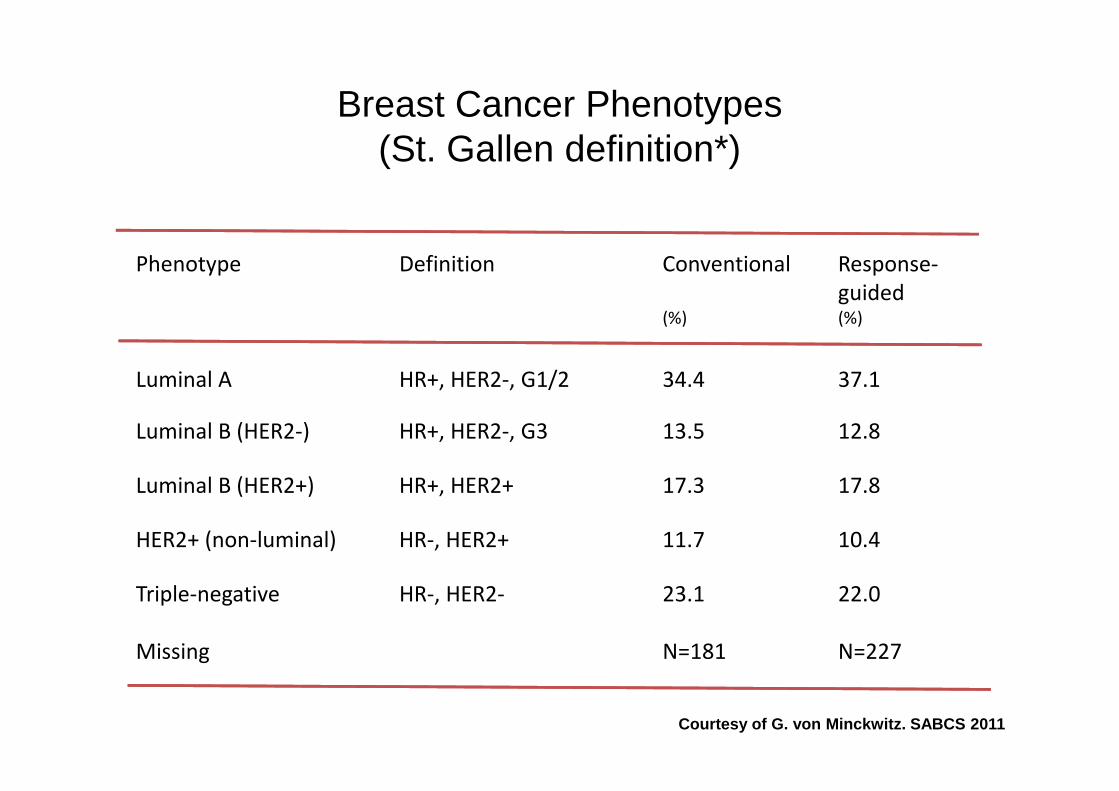
Breast Cancer Phenotypes (St. Gallen definition*)
Phenotype Definition Conventional Response-
guided(%) (%)
Luminal A HR+, HER2-, G1/2 34.4 37.1
Luminal B (HER2-) HR+, HER2-, G3 13.5 12.8
Luminal B (HER2+) HR+, HER2+ 17.3 17.8
HER2+ (non-luminal) HR-, HER2+ 11.7 10.4
Triple-negative HR-, HER2- 23.1 22.0
Missing N=181 N=227
Courtesy of G. von Minckwitz. SABCS 2011
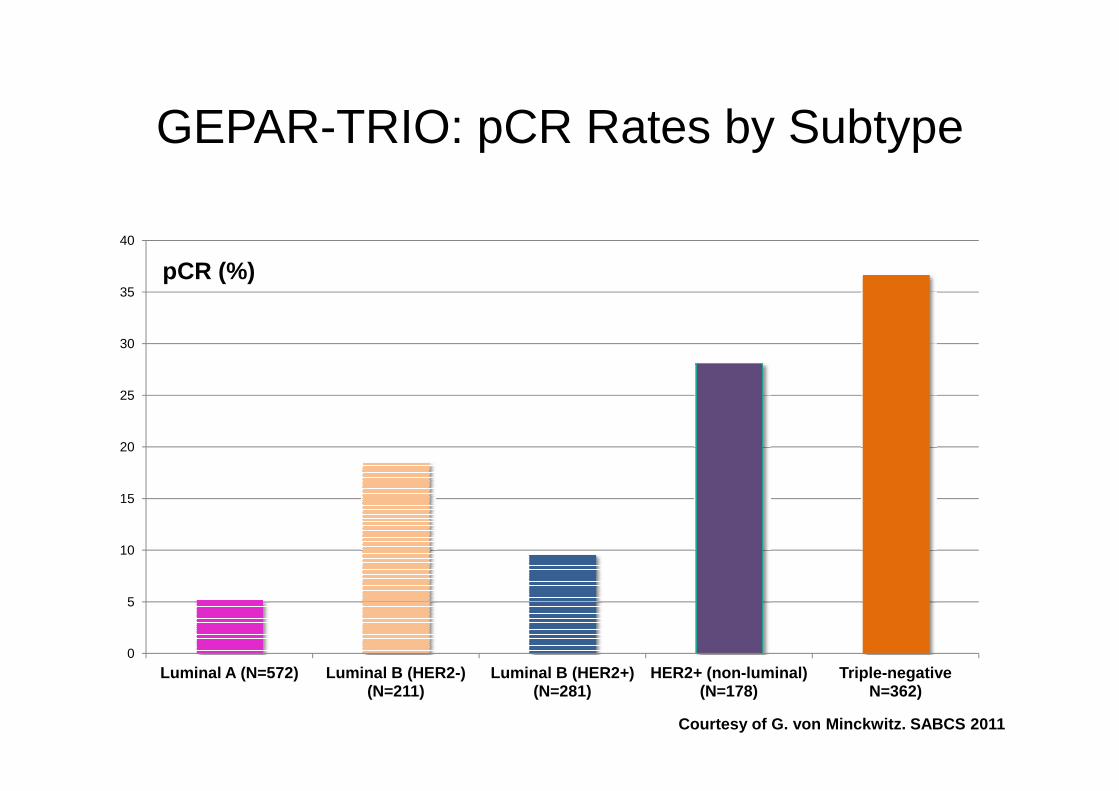
GEPAR-TRIO: pCR Rates by Subtype
25
30
35
40
pCR (%)
0
5
10
15
20
25
Luminal A (N=572) Luminal B (HER2-) (N=211)
Luminal B (HER2+) (N=281)
HER2+ (non-luminal) (N=178)
Triple-negative N=362)
Courtesy of G. von Minckwitz. SABCS 2011
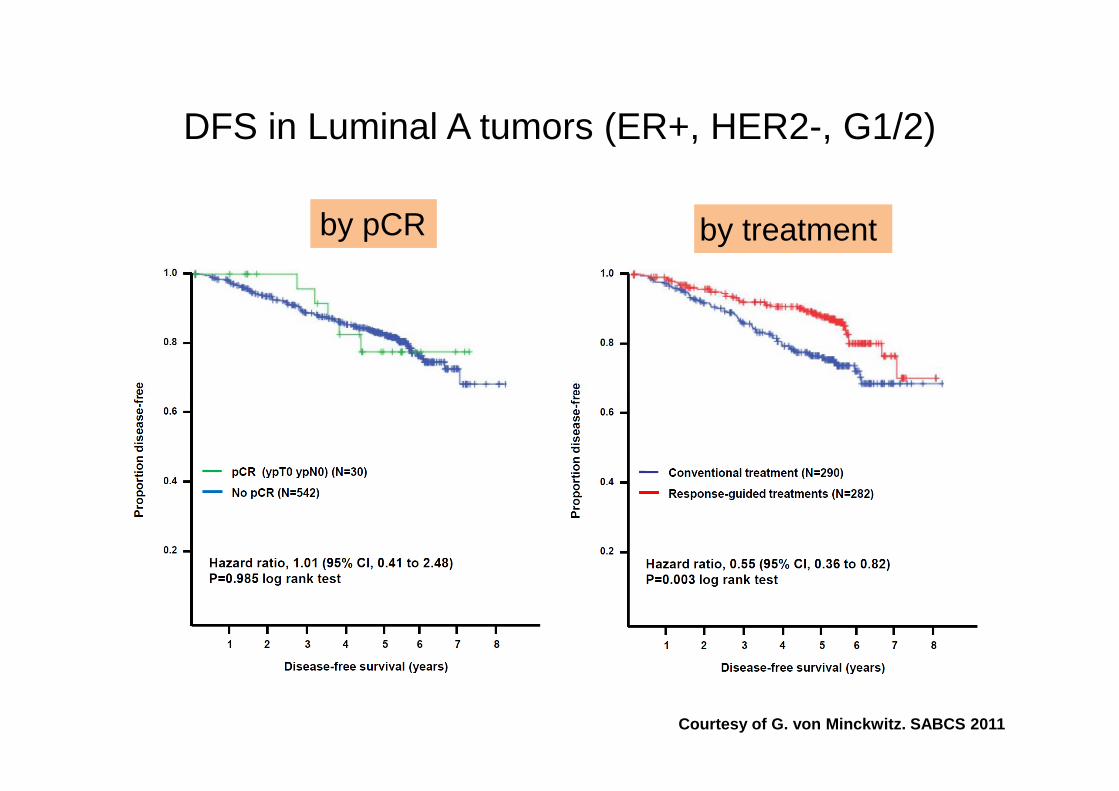
DFS in Luminal A tumors (ER+, HER2-, G1/2)
by pCRby pCR by treatment by treatment
Courtesy of G. von Minckwitz. SABCS 2011
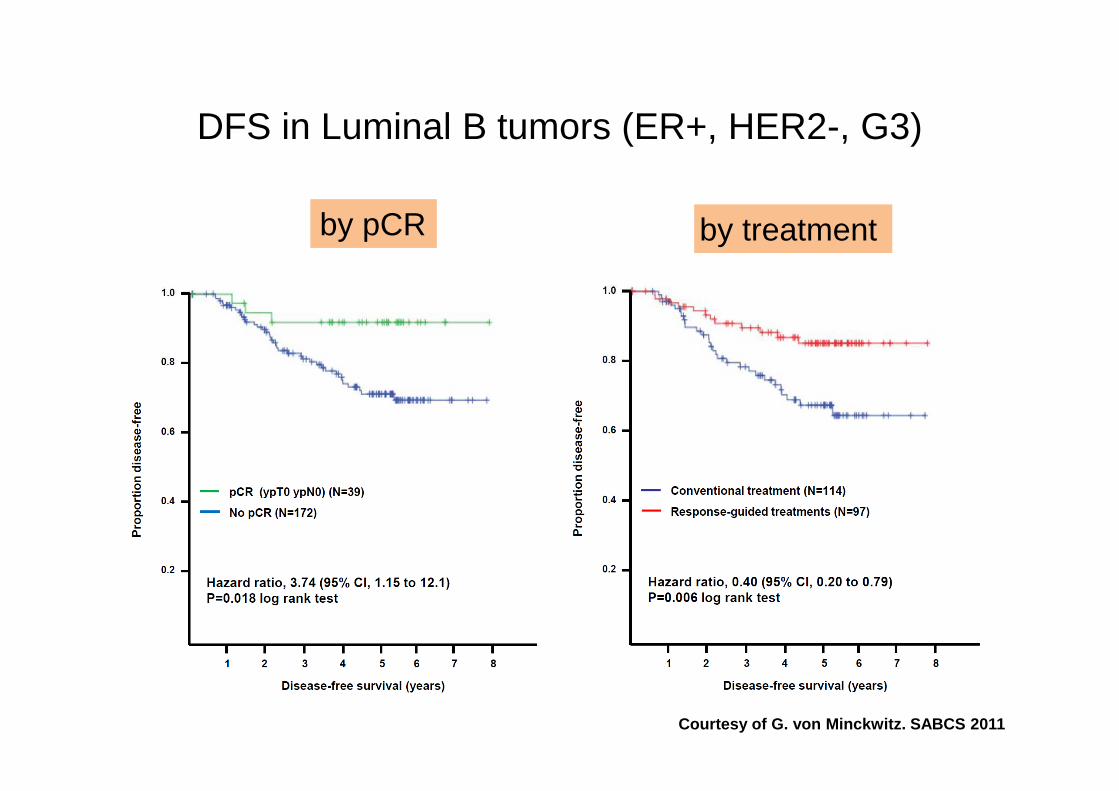
DFS in Luminal B tumors (ER+, HER2-, G3)
by pCRby pCR by treatment by treatment
Courtesy of G. von Minckwitz. SABCS 2011
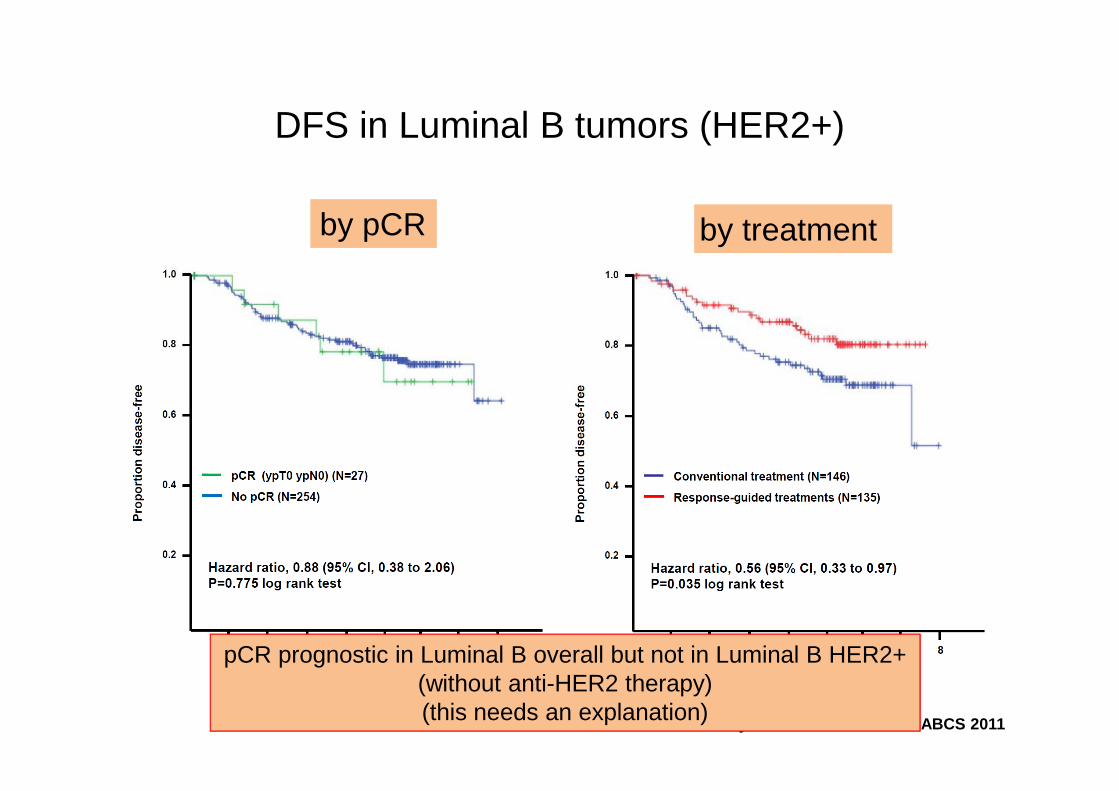
DFS in Luminal B tumors (HER2+)
by pCRby pCR by treatment by treatment
Courtesy of G. von Minckwitz. SABCS 2011
pCR prognostic in Luminal B overall but not in Luminal B HER2+(without anti-HER2 therapy)(this needs an explanation)
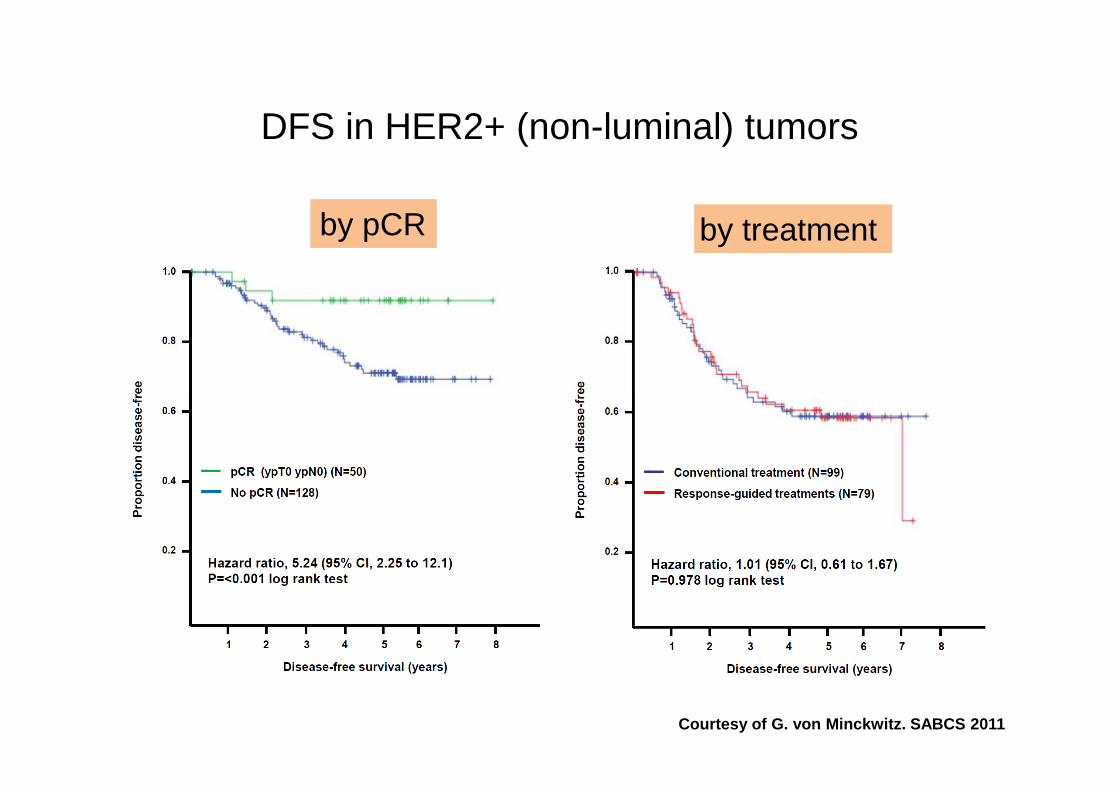
DFS in HER2+ (non-luminal) tumors
by pCRby pCR by treatment by treatment
Courtesy of G. von Minckwitz. SABCS 2011

DFS in Triple Negative Tumors
by pCRby pCR by treatment by treatment
Courtesy of G. von Minckwitz. SABCS 2011

Gepar-Trio
• Early assessment of clinical response as a surrogate of efficacy is a provocative finding and needs confirmation
• Response-guided therapy has two different regimens (TAC-NX and TCx8) that are analyzed in conjunction
• Even though the distribution in both groups seemed adequate, definition of molecular sub-groups was retrospective (needs more information)
• Different predictive/prognostic results for pCR according to molecular sub-groups needs confirmation/validation.

vs p=0.295
pCRpCR
n= 662 HER2+ with trastuzumabn= 3060 HER2 negativen= 665 HER2+; no trastuzumab
n= 662 HER2+ with trastuzumabn= 3060 HER2 negativen= 665 HER2+; no trastuzumab
n= 662 HER2+ with trastuzumabn= 3060 HER2 negativen= 665 HER2+; no trastuzumab
Log-rankvs p=0.058vs p=0.134
No pCRNo pCR
pCR as Surrogate for OS in HER2+
vs p=0.295vs p=0.384
Loibl S, Von Minckwitz G, Blohmer J, et al. pCR as a surrogate in HER2-positive patients treated with trastuzumab.
Cancer Research. 2011;71(24 suppl 3). Abstract S5-4.
Arm N Events
HER2 + w/trast 481 35
HER2 + w/o trast 546 75
HER2 Negative 2606 310
Arm N Events
HER2 + w/trast 181 1
HER2 + w/o trast 119 9
HER2 Negative 454 14
vs p=0.134
Virtually no deaths in pts reaching pCR with a trastuzumab-containing regimen !!
pCR HER2+ without Trastuzumab seems to do worse than pCR with Trastuzumab
HER2+ patients with no pCR require new alternatives
Moving Forward
• Changing a clinical research paradigm?
• Neo-adjuvant trials have advantages:
– Smaller, faster trials can guide larger definitive trials
– Embedded tissue-based studies key to selection strategies– Embedded tissue-based studies key to selection strategies
– Needs an effective multidisciplinary model.
• Different subtypes respond differently to the same drugs – be
careful about generalizing the results.
• Information on long term outcome (DFS, OS) is essential !!!
(ex.: Luminal A, Luminal B HER2+ or not, pCR HER2 positive w and w/out Trastuzumab)

Moving Forward
• Recognize that metastasis are complex
– Distant disease may be similar but not the same as the
primary
– Importance of the microenvironment
– Impact of time and therapy (i.e. the disease evolves with – Impact of time and therapy (i.e. the disease evolves with
time and is forced to change with therapy)
• Tissue-based studies are key (many questions)
– Need to biopsy metastases?
– When to biopsy?
– Serial biopsies (early and late pts) to guide/optimize
therapy?