Embed Size (px)
DESCRIPTION
This is a need specification document of the improvements required in the Radio Frequency Ablation process for liver cancer treatment
Citation preview
NEED SPECIFICATION DOCUMENT
Sivashyam Sundar A
EE11B103
NEED:
A method to increase the precision and configurability of the Radiofrequency
thermal ablation process in Cancer treatment which will increase the scope of
its application.
OBSERVATION: Radiofrequency thermal ablation (RFA) is a minimally invasive process which is
used to kill the cancer cells in a tumour. The size and location of the tumour is
critical to the process and current technology limits the application of this to a
small range of cancer tumours. RFA expands the medical application of heat,
which for decades has been used as a cautery device to cut tissue.
The following are the basic steps in a RFA process:
The tumours are located with ultrasound, computed tomography (CT), or
magnetic resonance (MR) imaging devices.
Then the patient is essentially turned into an electrical circuit by placing
grounding pads on the thighs.
A small needle-electrode with an insulated shaft and an un-insulated
distal tip is inserted through the skin and directly into the tumour. Ionic
vibration at the needle tip leads to frictional heat.
After 10 to 30 minutes of contact with the tumour, the radiofrequency
energy kills a 2.5- to 5-cm sphere. The dead cells are not removed, but
become scar tissue and eventually shrink.
Please refer to Appendix A for a more detailed procedure of the RFA process.
The primary application of RFA is in the treatment of primary or secondary
liver cancer, primary or secondary lung cancer and kidney cancer. The
application of RFA extends to other types of tumours as well.
The RFA procedure however, has its own limitations. This is because the
current technology cannot be applied in curing tumours of larger radius or
tumours near sensitive tissues. The need aims at developing a better RFA
technology which will help reducing such limitations. The following Disease
State Analysis will be taking into account only Liver cancer as there is more
scope of expansion of the current RFA technology to curing liver cancer
ANATOMY AND PHYSIOLGY: This part will deal with the anatomy and physiology of the Liver.
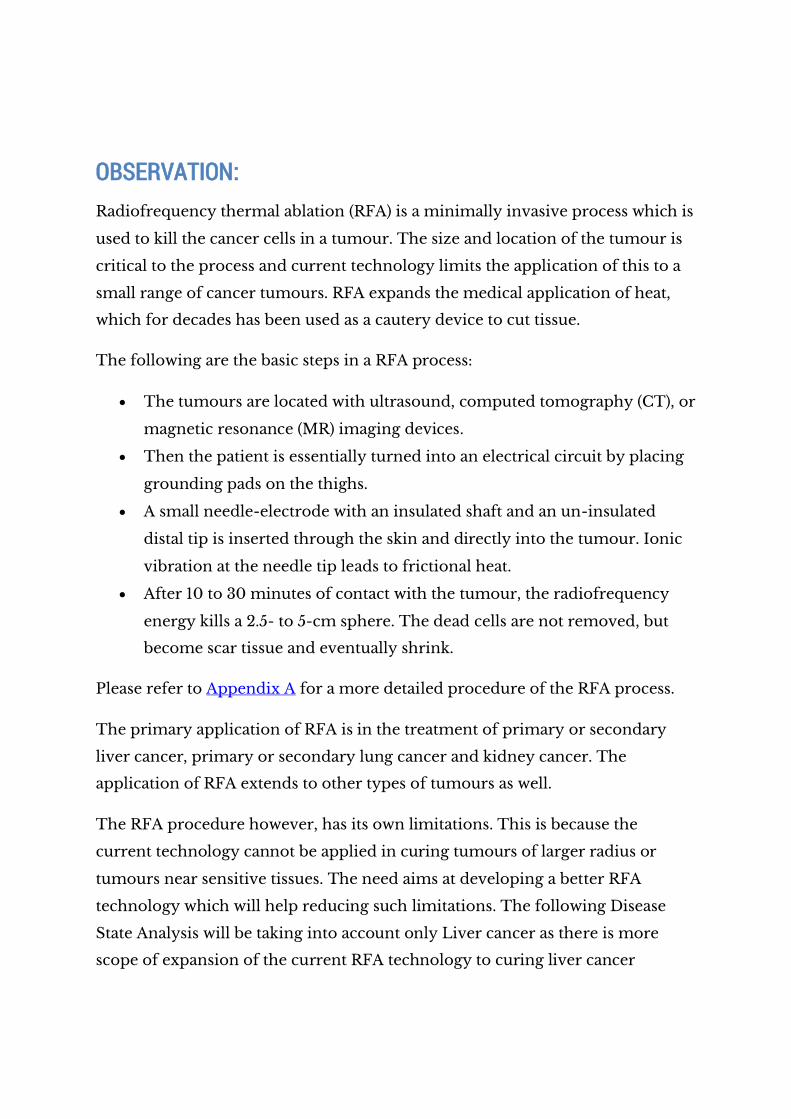
The liver is the largest solid organ in the body. In adults, the liver can weigh up
to 1.5 kilograms (kg). It is in the upper-right abdomen, just under the rib cage
and below the diaphragm (the thin muscle below the lungs and heart that
separates the chest cavity from the abdomen). The liver is part of the digestive
system.
STRUCTURE:
The liver has 2 main lobes: the larger right lobe and the smaller left lobe. Each
lobe is divided into segments.
The lobes are separated by a band of tissue called the falciform ligament (also
called the broad ligament), which helps attach the liver to the diaphragm.
A layer of connective tissue, called Glisson’s capsule or the capsule, covers the
liver.

BLOOD VESSELS:
Unlike most other organs, the liver has 2 major sources of blood:
Portal vein – carries blood from the digestive system to the liver.
Approximately 75% of the liver’s blood supply comes from the portal
vein.
Hepatic artery – supplies the liver with oxygen-rich blood from the
heart.
Most of the blood is removed from the liver through 3 hepatic veins (the right,
middle and left hepatic veins) found inside the liver.
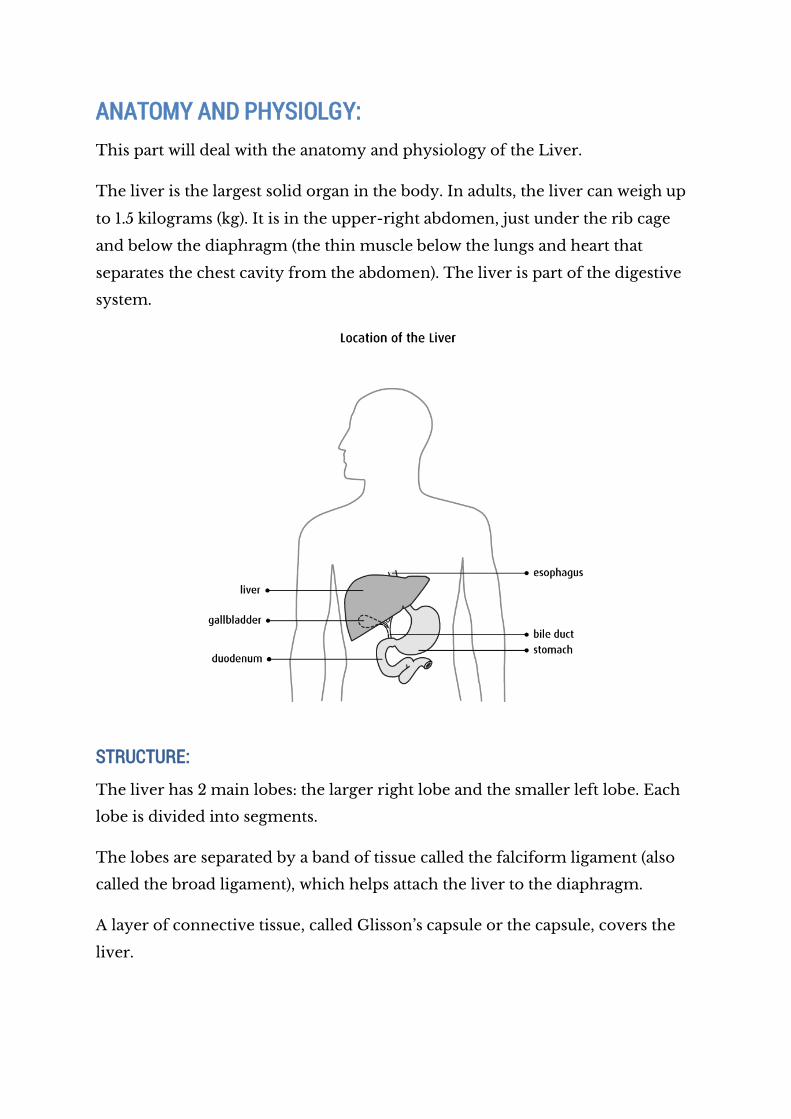
BILE DUCTS:
The liver, gallbladder and small intestine are connected by a series of thin tubes
called ducts. One function of the liver cells (hepatocytes) is to produce bile. Bile
is a yellow-green fluid that helps digest fat. Bile travels through a series of ducts
in the liver to the small intestine or to the gallbladder for storage. Bile is
collected from the liver in hepatic ducts. Two hepatic ducts leave the liver and
join to form the common hepatic duct. The cystic bile duct leaves the
gallbladder and joins the common hepatic duct to form the common bile duct.
FUNCTION:
The liver performs the following important functions in the body:
Produces bile
Absorbs and uses (metabolizes) bilirubin
Helps the body make blood-clotting (coagulation) factors
Helps the body metabolize fat
Metabolizes protein
Metabolizes carbohydrates
Stores vitamins and minerals
Filters the blood.
PATHOPHYSIOLOGY: Hepatocellular Carcinoma (HCC) is the most common form of liver cancer. The
pathophysiology of the same has been discussed here.
Initially the presence of HBV was linked to the development of HCC but it was
dismissed later. It was discovered then that most cases of hepatocellular
carcinoma developed in patients with underlying cirrhotic liver disease of
various etiologies. Inflammation, necrosis, fibrosis, and ongoing regeneration
characterize the cirrhotic liver and contribute to hepatocellular carcinoma
development.
The disease processes, which result in malignant transformation, include a
variety of pathways, many of which may be modified by external and
environmental factors and eventually lead to genetic changes that delay
apoptosis and increase cellular proliferation.
Thus HCC occurs predominantly in patients with underlying chronic liver
disease and cirrhosis. The cell(s) of origin are believed to be the hepatic stem
cells, although this remains the subject of investigation.[3] Tumours progress
with local expansion, intrahepatic spread, and distant metastases. Tumours may
present as a single mass lesion or as diffuse growth. The presentation may be
caused in part by mass effect that can lead to obstruction of the biliary system
or anywhere affecting the liver vasculature. Without aggressive surgical
resection, ablative therapy, or liver transplantation, hepatocellular carcinoma
results in liver failure and eventual death.
The staging of liver cancer is done in a lot of ways. There is no universally
accepted system for staging it. The treatment staging procedure is the simple to
understand method and clearly suggests the treatment. The 3 treatment stages
of liver cancer are:
1. Localized, resectable:
There is only one tumour in part of the liver or a limited number of
tumours in only one lobe of the liver.
The cancer is at an early stage and has not spread to other parts of the
body.
The person has good liver function (Child-Pugh grade A).
2. Locally advanced (regional), unresectable:
The tumour is too large to be removed with surgery.
The tumour has grown into the blood vessels in the liver.
The person has poor liver function.
3. Advanced:
The cancer has spread throughout the liver or to other organs in the
body.
CLINICAL PRESENTATION:
SIGNS AND SYMPTOMS:
Pain in the abdomen
Lump or mass under the ribs
Jaundice
Weight loss
Fatigue
Weakness
Changes to digestion
Change in bowel habits
Malaise
Swelling of the legs and feet (edema)
Hepatic encephalopathy
o confusion
o forgetfulness
o drowsiness
o personality changes
o breath with a sweet or musty odour
o unconsciousness, coma
Portal hypertension
DIAGNOSIS:
Serum AFP would appear to be an attractive option for screening given its low
cost and morbidity. Unfortunately, it is only 40-64% sensitive because many
tumors do not produce AFP at all or only at a very advanced stage. When
elevated, the AFP is 75-91% specific and values greater than 400 ng/mL are
generally considered diagnostic of hepatocellular carcinoma.
The best imaging modality for screening remains the subject of debate.
Ultrasonography offers a relatively inexpensive method of screening.
Ultrasound as a screening method is reported to have 60% sensitivity and 97%
specificity in the cirrhotic population, and it has been demonstrated to be cost
effective.
CLINICAL OUTCOMES:
MORBIDITY:
Often liver cancer is not found until it is at an advanced stage, which can
make it more difficult to treat.
Most liver cancers have a tendency to spread quickly.
An underlying liver disease, such as cirrhosis, can affect survival.
The severity of the desease can be associated with the stage of the disease:
1. Localized, resectable
There are 1 or 2 tumours in 1 lobe of the liver.
These tumours can be removed (resected) by surgery.
2. Locally advanced (regional), unresectable
There are several tumours that have spread to the other lobe or other
parts of the liver and have spread to the lymph nodes.
These tumours are locally advanced and cannot be removed by
surgery.
3. Advanced
1. The cancer has spread to distant organs.
MORTALITY:
Mortality in cancer diagnosis is generally given by the 5-year survival rate
which means the number of people who live 5 years after their cancer is
diagnosed.
1. Localised- 28%
2. Locally advanced- 7%
3. Advanced- 2%
For all stages combined, the relative 5-year survival rate is about 15%
EPIDEMIOLOGY: Liver cancer is the sixth most common cancer worldwide, with more
than 782,000 new cases diagnosed in 2012 (6% of the total).
Liver cancer incidence rates are highest in Eastern Asia and lowest in
South Central Asia
Liver Cancer in developing nations is over twice the incidence of that in
developed countries.
The highest incidence of hepatocellular carcinoma is in East Asia, with
incidence rates in men of 35 per 100,000 population, followed by Africa
and the Pacific Islands.
Liver cancer incidence is strongly related to age, with the highest
incidence rates being in older men and women. In the UK between 2009
and 2011, an average of 43% of cases were diagnosed in men and women
aged 75 and over, and 81% were diagnosed in those aged 65 and over
As far as prevalence is considered, worldwide, it is estimated that there
were more than 613,000 men and women still alive in 2008, up to five
years after their diagnosis.
ECONOMIC IMPACT: Cancer has a huge economic impact worldwide. Every year millions of dollars is
spent n Cancer research, treatment and concessions by the governments.
In 2013 Cancer Research UK spent about 351 Million pounds on research and a
specific 21 Million was spent on providing information for people affected by
cancer.
However much economic details are not available for Liver cancer specifically.
SUMMARY: The report summarised the Disease state of Liver cancer. It is evident that it is
one of the deadliest diseases and a hard and fast treatment method is yet to be
discovered. In fact, this is the case for any cancer type. Hence, the importance
of biomedical device innovation comes into picture.
TREATMENT OPTIONS: There are a variety of treatment options depending on the stage of liver cancer.
We are considering all the treatment options for primary/secondary liver
cancer because it helps in identifying the gaps and whether or not
improvements in RFA technology will be able to fill them.
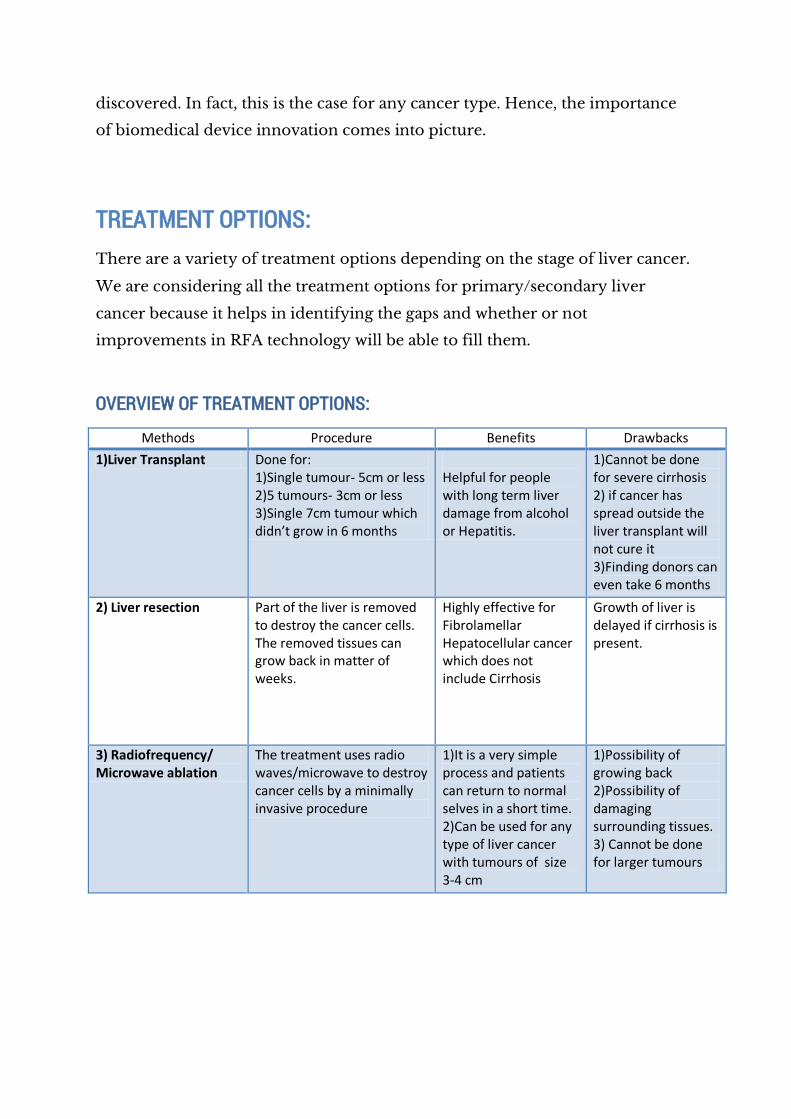
OVERVIEW OF TREATMENT OPTIONS:
Methods Procedure Benefits Drawbacks
1)Liver Transplant Done for: 1)Single tumour- 5cm or less 2)5 tumours- 3cm or less 3)Single 7cm tumour which didn’t grow in 6 months
Helpful for people with long term liver damage from alcohol or Hepatitis.
1)Cannot be done for severe cirrhosis 2) if cancer has spread outside the liver transplant will not cure it 3)Finding donors can even take 6 months
2) Liver resection Part of the liver is removed to destroy the cancer cells. The removed tissues can grow back in matter of weeks.
Highly effective for Fibrolamellar Hepatocellular cancer which does not include Cirrhosis
Growth of liver is delayed if cirrhosis is present.
3) Radiofrequency/ Microwave ablation
The treatment uses radio waves/microwave to destroy cancer cells by a minimally invasive procedure
1)It is a very simple process and patients can return to normal selves in a short time. 2)Can be used for any type of liver cancer with tumours of size 3-4 cm
1)Possibility of growing back 2)Possibility of damaging surrounding tissues. 3) Cannot be done for larger tumours
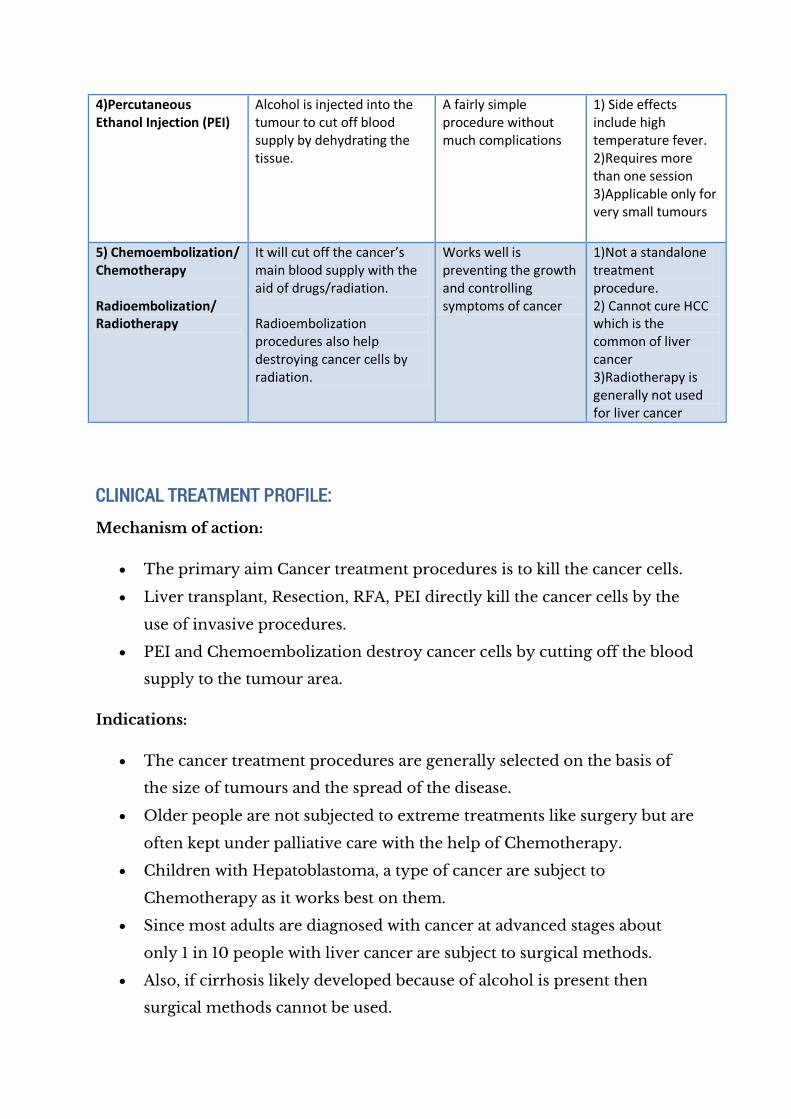
4)Percutaneous Ethanol Injection (PEI)
Alcohol is injected into the tumour to cut off blood supply by dehydrating the tissue.
A fairly simple procedure without much complications
1) Side effects include high temperature fever. 2)Requires more than one session 3)Applicable only for very small tumours
5) Chemoembolization/ Chemotherapy Radioembolization/ Radiotherapy
It will cut off the cancer’s main blood supply with the aid of drugs/radiation. Radioembolization procedures also help destroying cancer cells by radiation.
Works well is preventing the growth and controlling symptoms of cancer
1)Not a standalone treatment procedure. 2) Cannot cure HCC which is the common of liver cancer 3)Radiotherapy is generally not used for liver cancer
CLINICAL TREATMENT PROFILE:
Mechanism of action:
The primary aim Cancer treatment procedures is to kill the cancer cells.
Liver transplant, Resection, RFA, PEI directly kill the cancer cells by the
use of invasive procedures.
PEI and Chemoembolization destroy cancer cells by cutting off the blood
supply to the tumour area.
Indications:
The cancer treatment procedures are generally selected on the basis of
the size of tumours and the spread of the disease.
Older people are not subjected to extreme treatments like surgery but are
often kept under palliative care with the help of Chemotherapy.
Children with Hepatoblastoma, a type of cancer are subject to
Chemotherapy as it works best on them.
Since most adults are diagnosed with cancer at advanced stages about
only 1 in 10 people with liver cancer are subject to surgical methods.
Also, if cirrhosis likely developed because of alcohol is present then
surgical methods cannot be used.
Efficacy:
The outlook for people who are diagnosed in early stages and undergo
liver transplant is the best currently. About 75% of them survive after 5
years from diagnosis.
Overall, only between 1 in 6 people (15%) and 1 in 4 people (25%) live for at
least 5 years after surgery to remove liver cancer (liver resection).
People who have cancers that are less than 3cm across, more than half
(50%) will live for more than 5 years because of procedures like RFA and
PEI.
Safety:
All the treatment procedures almost invariably have side effects.
Liver transplant is too big an operation to survive if the patient is already
very ill. Also, the drugs taken to make the body accept the new liver
damp down the activity of your immune system and reduce its ability to
control the cancer.
Liver resection possibly does not have any special side effects but it has
the usual side effects of a surgery and takes a toll on the patient.
RFA and related technologies may damage the nearby good tissues and a
complete fullstop to the cancer cells may not be guaranteed.
Chemotherapy leads to Sickness, diarrhoea, hair loss or thinning, feeling
tired and run down, sore mouth or mouth ulcers, a drop in blood cells
causing an increased risk of infection, bleeding or bruising, tiredness and
shortness of breath.
Chemoembolization may result in liver failure in patients with moderate
or higher level of Cirrhosis..
TREATMENT LANDSCAPE:
Summary of treatment options:
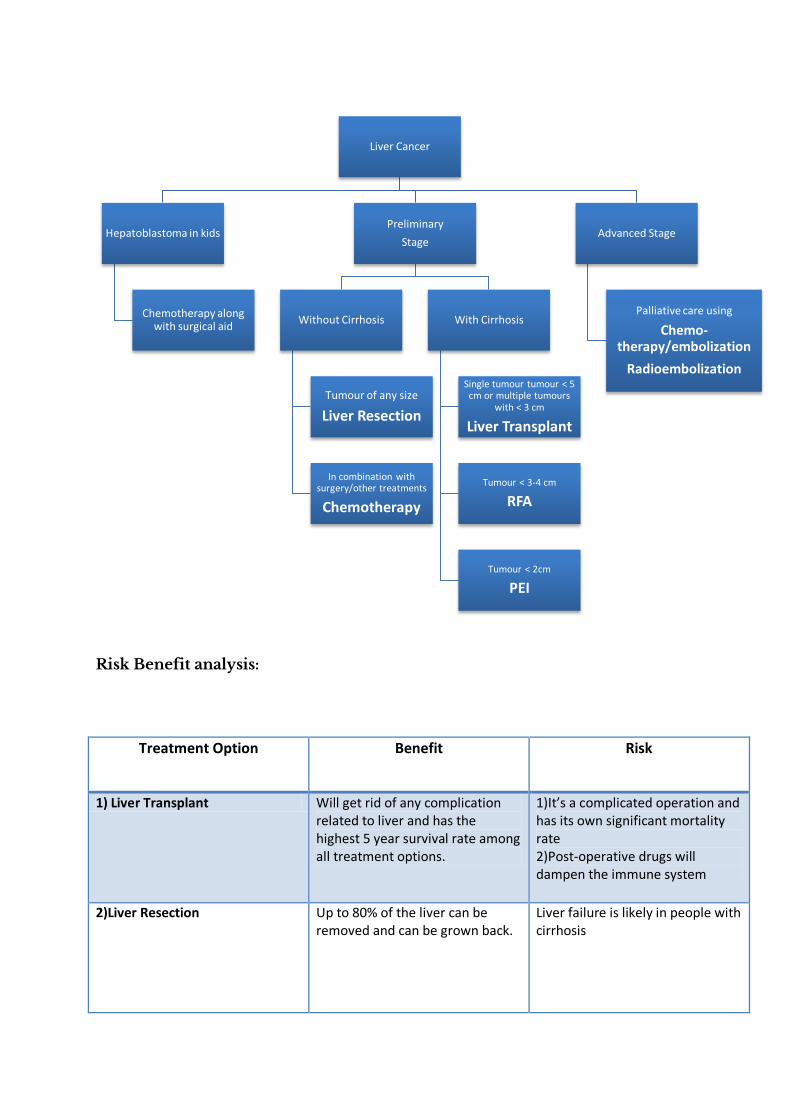
Risk Benefit analysis:
Treatment Option Benefit Risk
1) Liver Transplant Will get rid of any complication related to liver and has the highest 5 year survival rate among all treatment options.
1)It’s a complicated operation and has its own significant mortality rate 2)Post-operative drugs will dampen the immune system
2)Liver Resection Up to 80% of the liver can be removed and can be grown back.
Liver failure is likely in people with cirrhosis
Liver Cancer
Hepatoblastoma in kids
Chemotherapy along with surgical aid
Preliminary
Stage
Without Cirrhosis
Tumour of any size
Liver Resection
In combination with surgery/other treatments
Chemotherapy
With Cirrhosis
Single tumour tumour < 5 cm or multiple tumours
with < 3 cm
Liver Transplant
Tumour < 3-4 cm
RFA
Tumour < 2cm
PEI
Advanced Stage
Palliative care using
Chemo-therapy/embolization
Radioembolization
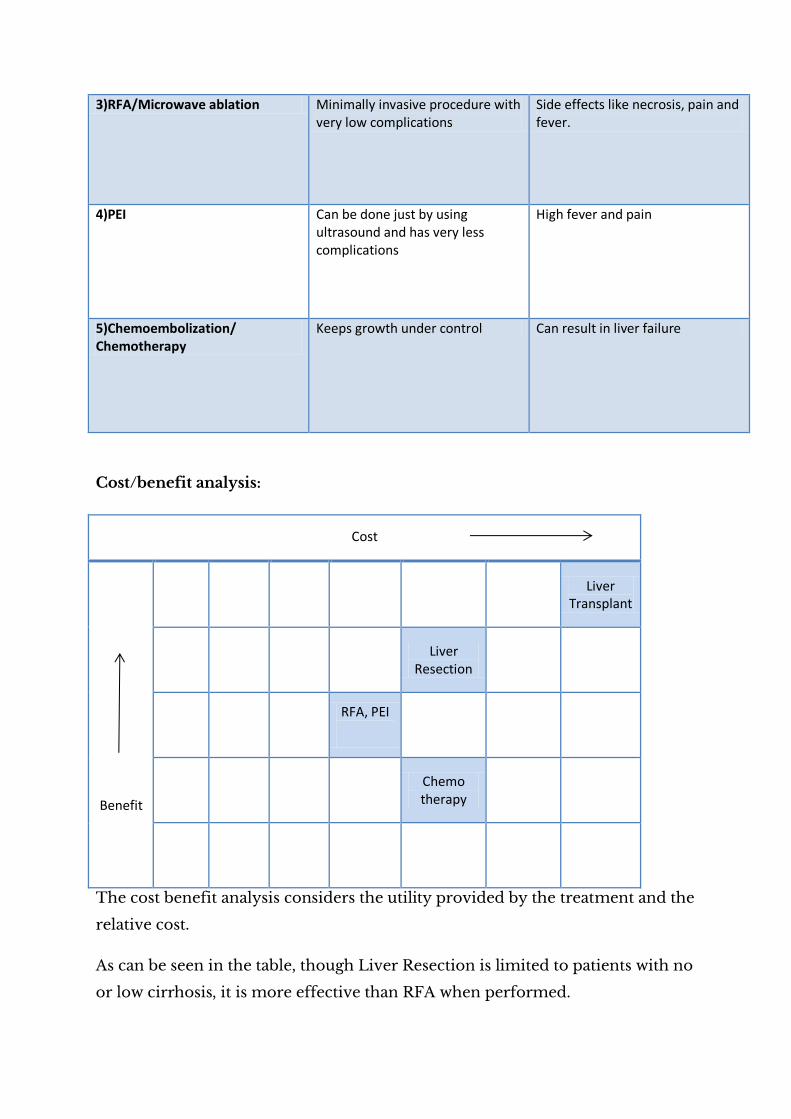
3)RFA/Microwave ablation Minimally invasive procedure with very low complications
Side effects like necrosis, pain and fever.
4)PEI Can be done just by using ultrasound and has very less complications
High fever and pain
5)Chemoembolization/ Chemotherapy
Keeps growth under control Can result in liver failure
Cost/benefit analysis:
Cost
Benefit
Liver
Transplant
Liver
Resection
RFA, PEI
Chemo therapy
The cost benefit analysis considers the utility provided by the treatment and the
relative cost.
As can be seen in the table, though Liver Resection is limited to patients with no
or low cirrhosis, it is more effective than RFA when performed.

GAP ANALYSIS:
From the analysis of treatment options we not the following points:
There is no definitive method for advance stages of liver cancer
RFA methods are limited to sites which are not critical tissues and the
maximum radius of tumour that can be ablated is 5 cm.
Surgery methods though have higher benefits, are complicated
procedures and a good health condition is needed which de facto is not
present in a cancer patient.
One major advantage of RFA procedure is that it neither has limitations on the
health condition of the patients nor on presence of other complications. Rather
it is limited by the size and site of the tumour. The collateral damage done
because of RFA include the tissue surrounding the tumour.
This can be cured by RFA
This cannot be treated by RFA as the tumour has grown
on the blood vessel
Thus, by increasing the accuracy of RFA technology we can extend the range of
application of the process, thereby providing a providing treatment to tumours
larger sizes for patients who cannot undergo other procedures
STAKEHOLDER ANALYSIS: The stakeholder analysis is done taking into account the benefits/costs the
stakeholders will face if the need is achieved.
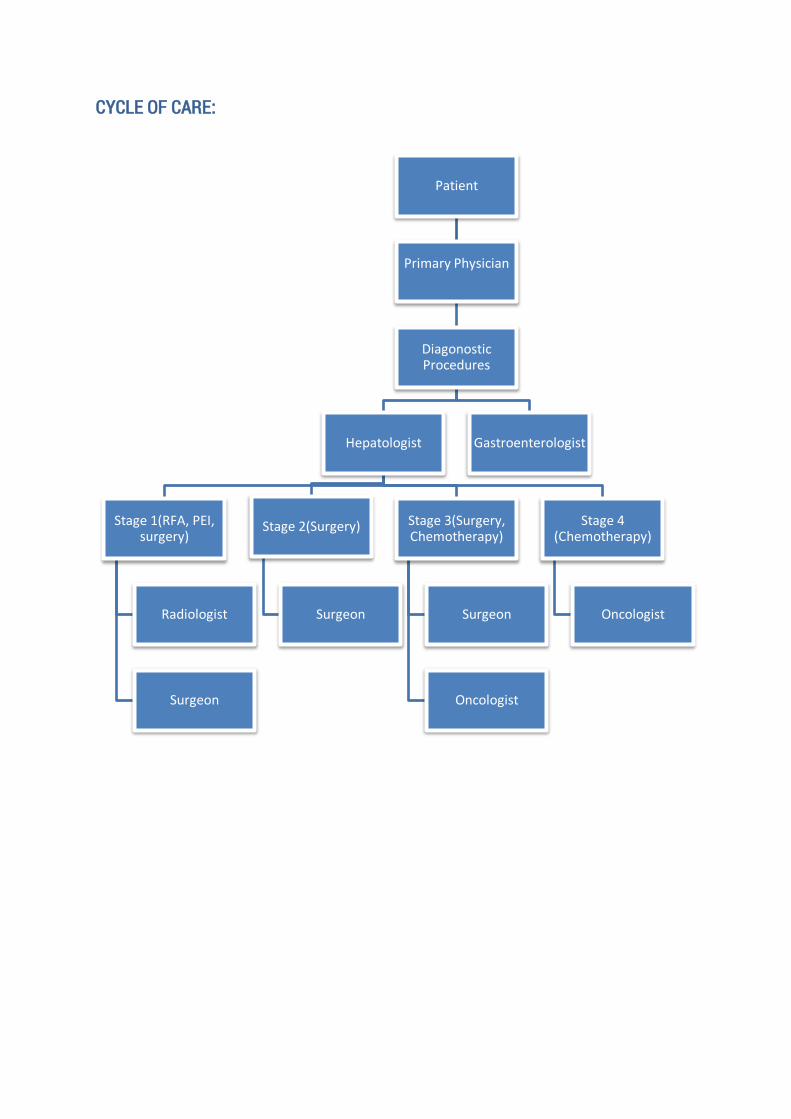
CYCLE OF CARE:
Patient
Primary Physician
Diagonostic Procedures
Hepatologist
Stage 1(RFA, PEI, surgery)
Radiologist
Surgeon
Stage 2(Surgery)
Surgeon
Stage 3(Surgery, Chemotherapy)
Surgeon
Oncologist
Stage 4 (Chemotherapy)
Oncologist
Gastroenterologist
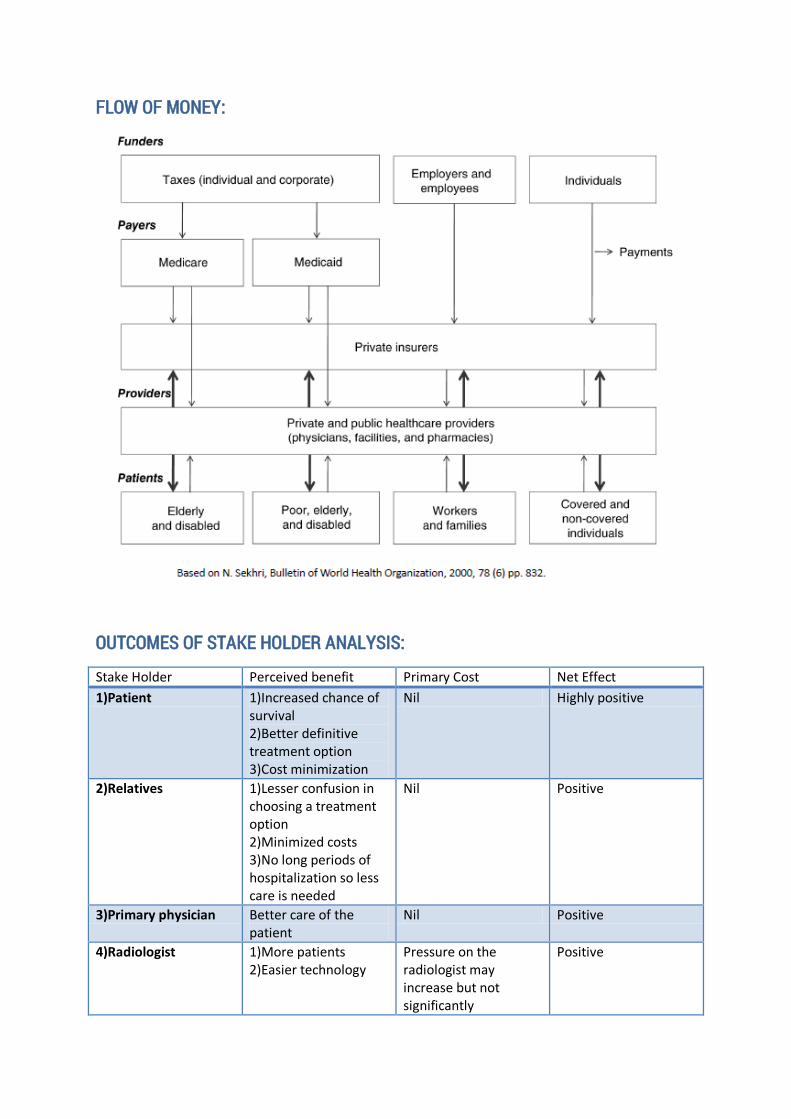
FLOW OF MONEY:
OUTCOMES OF STAKE HOLDER ANALYSIS:
Stake Holder Perceived benefit Primary Cost Net Effect
1)Patient 1)Increased chance of survival 2)Better definitive treatment option 3)Cost minimization
Nil Highly positive
2)Relatives 1)Lesser confusion in choosing a treatment option 2)Minimized costs 3)No long periods of hospitalization so less care is needed
Nil Positive
3)Primary physician Better care of the patient
Nil Positive
4)Radiologist 1)More patients 2)Easier technology
Pressure on the radiologist may increase but not significantly
Positive
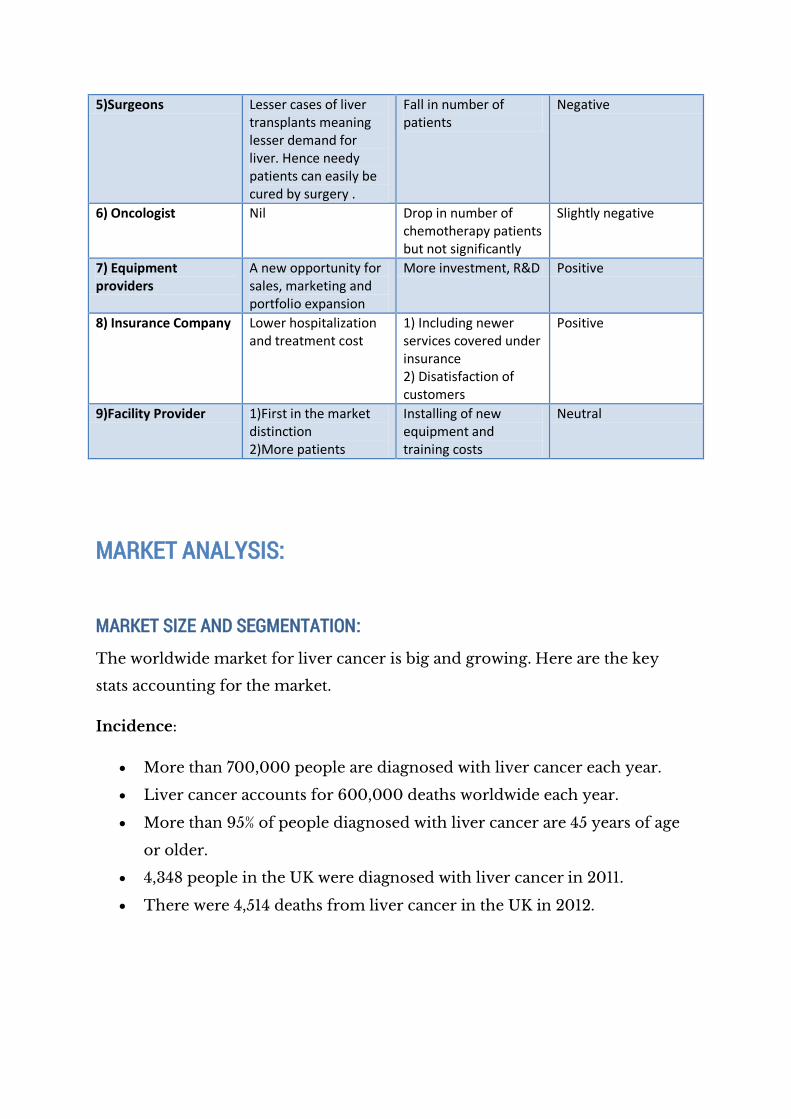
5)Surgeons Lesser cases of liver transplants meaning lesser demand for liver. Hence needy patients can easily be cured by surgery .
Fall in number of patients
Negative
6) Oncologist Nil Drop in number of chemotherapy patients but not significantly
Slightly negative
7) Equipment providers
A new opportunity for sales, marketing and portfolio expansion
More investment, R&D Positive
8) Insurance Company Lower hospitalization and treatment cost
1) Including newer services covered under insurance 2) Disatisfaction of customers
Positive
9)Facility Provider 1)First in the market distinction 2)More patients
Installing of new equipment and training costs
Neutral
MARKET ANALYSIS:
MARKET SIZE AND SEGMENTATION:
The worldwide market for liver cancer is big and growing. Here are the key
stats accounting for the market.
Incidence:
More than 700,000 people are diagnosed with liver cancer each year.
Liver cancer accounts for 600,000 deaths worldwide each year.
More than 95% of people diagnosed with liver cancer are 45 years of age
or older.
4,348 people in the UK were diagnosed with liver cancer in 2011.
There were 4,514 deaths from liver cancer in the UK in 2012.
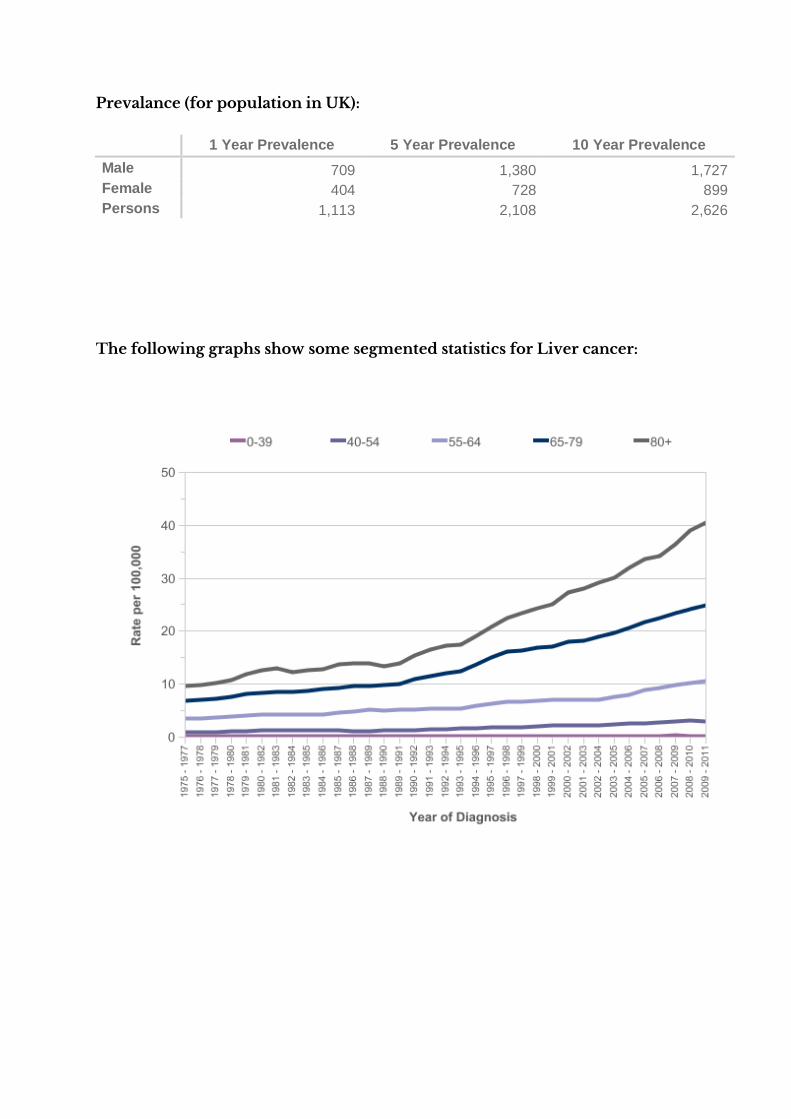
Prevalance (for population in UK):
1 Year Prevalence 5 Year Prevalence 10 Year Prevalence
Male 709 1,380 1,727
Female 404 728 899
Persons 1,113 2,108 2,626
The following graphs show some segmented statistics for Liver cancer:
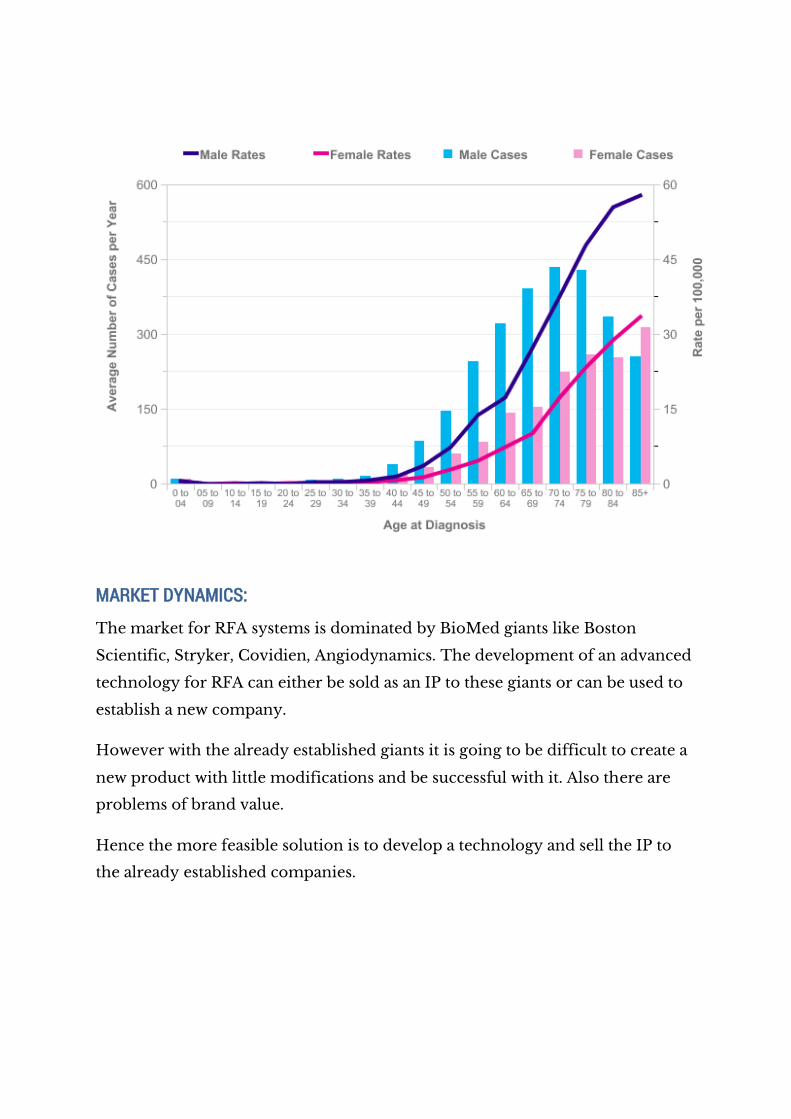
MARKET DYNAMICS:
The market for RFA systems is dominated by BioMed giants like Boston
Scientific, Stryker, Covidien, Angiodynamics. The development of an advanced
technology for RFA can either be sold as an IP to these giants or can be used to
establish a new company.
However with the already established giants it is going to be difficult to create a
new product with little modifications and be successful with it. Also there are
problems of brand value.
Hence the more feasible solution is to develop a technology and sell the IP to
the already established companies.
MARKET NEEDS:
Need of segments:
As can be seen from the statistics, a better technology is always welcomed in
cancer. Research is going on in every part of the world to improve the everyday
life and reduce the mortality rate of cancer.
Radiofrequency Ablation process has already been quoted as an emerging
technology and hence more and more people are seeking to benefit from it
instead of choosing conventional surgical/chemo methods. The main barrier in
this technology being the accuracy of the tech because of which tumours in
critical tissues cannot be cured.
An improvement in the accuracy would even mean a breakthrough depending
upon the extent of improvement. However, this might significantly affect the
income of surgeons. But, considering the greater good this is an important need
in cancer research.
WILLINGNESS TO PAY:
As far as this technology is concerned it results in almost the same cost like
chemo or other treatment methods for the patient. For the hospitals to it is a
matter of one time investment. Even if the cost of treatment were supposed to
increase the patients are willing to pay as this is going to be a less painful
method than surgery and chemotherapy.
The target market will be all the cancer treatment centres and research
institutes.
NEED CRITERIA:
DEMANDS:
Should be able to destroy tumour cells of radius < 5 cm without
damaging the surrounding tissue.
Should be able to destroy larger tumour cells with the accuracy of
existing technology.
Should have a method to accurately position the tip of the electrode.
ENHANCEMENTS:
A robot steered positioning which will automatically position the tip and
move inside if needed.
WISHES:
The cost of new technology should be the same the older technology by
using additional
REFERENCES:
http://www.macmillan.org.uk/information-and-support/treating/supportive-and-other-
treatments/other-treatments/radiofrequency-
ablation.html?utm_source=content&utm_medium=clickthrough&utm_content=radiofreque
ncyablation&utm_campaign=factfile#tcm:9-19847
http://www.cc.nih.gov/drd/tumortherapy.html#liver
http://www.biomedical-engineering-online.com/content/5/1/24#sec6
http://www.hopkinsmedicine.org/liver_tumor_center/conditions/cancerous_liver_tumors/h
epatocellular_carcinoma.html
http://emedicine.medscape.com/article/197319-overview#a0199
http://www.cancerresearchuk.org/cancer-info/cancerstats/types/liver/incidence/uk-liver-
cancer-incidence-statistics
http://www.cancer.ca/en/cancer-information/cancer-type/liver/prognosis-and-
survival/?region=on
http://www.cancer.org/cancer/livercancer/detailedguide/liver-cancer-survival-rates
http://www.cancerresearchuk.org/about-cancer/type/liver-cancer/treatment/statistics-and-
outlook-for-liver-cancer
http://www.medscape.com/viewarticle/727459
http://www.moloncol.org/article/S1574-7891(08)00040-9/fulltext#sec3.1
http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/documen
t/acspc-027766.pdf
http://globalcancermap.com/
http://www.cancerresearchuk.org/sites/default/files/annual_review_highlights_2013-14.pdf
http://www.cancerresearchuk.org/about-cancer/type/liver-cancer/treatment/the-stages-of-
primary-liver-cancer
http://www.cancerresearchuk.org/about-cancer/type/liver-cancer/where-this-liver-cancer-
information-comes-from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1356249/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2408961/
http://www.bostonscientific.com/en-US/products/capital-equipment--therapy/RF3000-
Radiofrequency-Generator.html
http://www.wikiwand.com/en/Radiofrequency_ablation
http://www.indiacancersurgerysite.com/india-price-comparison.html
http://www.hindustantimes.com/newdelhi/liver-cancer-emerges-as-fast-growing-threat-in-
country/article1-837216.aspx
http://www.cancer.org/cancer/livercancer/detailedguide/liver-cancer-risk-factors
http://www.cancerresearchuk.org/cancer-info/cancerstats/types/liver/uk-liver-cancer-
statistics
http://www.cancerresearchuk.org/cancer-info/cancerstats/types/liver/incidence/
http://www.ncbi.nlm.nih.gov/pubmed/23892758
http://www.angiodynamics.com/products/what-is-rfa
APPENDIX A: RADIOFREQUENCY TUMOUR ABLATION PROCESS
Radiofrequency thermal ablation can usually be performed as an outpatient
procedure under general anesthesia or conscious sedation. Alternatively, RFA
may be performed laparoscopically or during open surgery.[36]
Under light sedation, lidocaine or bupivacaine is administered subcutaneously
at the needle entry site and down to the liver capsule. A needle is placed
through the skin and into the tumour with imaging guidance. Treatment
sessions of percutaneous RFA are easily monitored using real-time ultrasound
imaging, computed tomography, or magnetic resonance imaging. Most patients
feel little pain during the procedure and go home the same day or the day after
the procedure, usually with minimal to no pain or soreness, although there is a
spectrum, and some patients will experience severe pain the day of the
procedure.
During a 10- to 30-minute treatment session, nitrogen micro-bubbles gradually
create a hyperechoic area on ultrasound that provides a rough estimation of the
treated tissue, which is 2.5 to 5 cm per 10- to 30-minute treatment sphere. CT,
MR imaging, or positron emission tomography (PET) imaging may provide
more exquisite detail for follow-up verification of the treatment zone and for
finding residual or recurrent neoplastic tissue. Although real-time MR imaging
and CT are available, they are not in widespread use. Ultrasound is a safe,
common, and easy guidance method, although it is somewhat operator
dependent.
Once the needle has been properly positioned within the tumour, the tissue is
heated. At temperatures exceeding 50o C, cells are destroyed. To treat tumours
of different size and shape, the needle is available in different lengths and
shapes of exposed tips.[37]
Energy is transferred from the uninsulated distal tip of the needle to the tissue
as current rather than as direct heat. The circuit is completed with grounding
pads placed on the patient's thighs. As the alternating current flows to the
grounding pads, it agitates ions in the surrounding tissue, resulting in frictional
heat. The tissue surrounding the needle is desiccated, creating an oval or
spherical lesion of coagulation necrosis, typically 2.5 to 5 cm in diameter for
each 10- to 30-minute treatment. These spheres are added together in three
dimensions to overlap and completely envelop the tumour. Ideally, the treated
tissue will contain the entire tumour plus a variable rim of healthy tissue as a
safety margin.
Failure to ablate the entire tumour with clean edges results in regrowth of the
tumour. Depending on the size and configuration of new growth, the patient
may or may not be suited for another treatment session. Over months to years,
as the dead necrotic cells are reabsorbed and replaced by scar tissue and
fibrosis, the size of the thermal lesion shrinks, although the remaining cells are
ideally dead. The possibility of successful surgical resection may be augmented
by decreasing the number of tumours.[38] Treatment of a tumour in one lobe
may broaden the surgical indications of a tumour in the other lobe. Due to the
natural course of the disease, new or recurrent tumours may be suited for
additional treatment sessions as well.
Source: http://www.cc.nih.gov/drd/tumourtherapy.html





























