Embed Size (px)
Citation preview

NecrotizingEnterocolitis
Priscilla Joe, MDChildren’s Hospital and Research Center Oakland

2
Incidence
• Most common GI emergency in premies• 2-10% of VLBW infants < 1500 grams• Inverse relationship with gestational age• Males and females equally effected• Mean age @ diagnosis 20 days (premies) vs. 7
days (term)• Jejunum, ileum, and colon most commonly affected• 10% term infants (usually in those with pre-existing
illness)

3
Clinical Findings
• Abdominal distension (70-98%)• Increased gastric residuals ( >70%)• Emesis (>70%)• Gross blood per rectum (25-63%)• Occult GI bleeding (22-59%)• Diarrhea (4-26%)• Lethargy, temperature instability,
apnea/bradycardia, hypotension

4
Physical Findings
• Absent bowel sounds
• Abdominal tenderness
• Abdominal wall erythema
• Fixed abdominal mass (RLQ)

5

6

7
Pathophysiology
• Bacterial proliferation• Ischemic mucosal damage • Transmural necrosis allowing bacterial
translocation, increasing risk for perforation
• Endotoxin activation of inflammatory cascade

8
Risk Factors
• Prematurity
• Feeding
• Circulatory Instability
• Medications (vasoactive agents, indocin)
• Bacterial Overgrowth/Infection

9
Prematurity
• Deficient mucosal barrier (suppressed GI hormones and mucosal enzymes)
• Dysfunctional intestinal host defense system
• Decreased motility• Dysregulation of intestinal
microcirculation (increased bacterial overgrowth)

10
Feeding and NEC
• 90% of babies receive enteral feedings• Disrupts mucosal integrity• Reduces gut motility• Alters GI blood flow• Abnormal bacterial colonization
-Formula: Enterobacter-Breastmilk: Enterobacter and Bifidobacterium
• Rate of feeding advancement• Hyperosmolar feeding

11
Intestinal Ischemia
• Term infants (polycythemia, asphyxia, exchange transfusion, congenital heart disease, IUGR)
• PDA• Indocin• Cocaine exposure in utero• UAC lines?• Gastroschisis

12
Bacterial Colonization
• High risk infants susceptible to bacterial overgrowth
• Breast milk (lactobacilli and facultative anaerobes)
• Formula fed (potentially pathogenic gram-negative bacteria)

Work Up

14
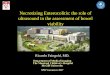
Radiographic Findings• Intestinal ileus• Dilated and thickened bowel loops, air-fluid
levels• Intramural gas (pneumatosis intestinalis);
cystic and/or linear patterns, terminal ileum and proximal colon
• Free air (football sign)• Portal venous gas• Fixed or persistent dilated loop of bowel
(sentinel loop)• Gasless abdomen with ascites

15
16

17

18

19

20
Laboratory Findings• CBC:
– Elevated or decreased WBCs– Thrombocytopenia– Low ANC = poor prognosis
• Elevated CRP• Cultures (blood, +/- stool, +/- CSF)
– Usually reveals enteric flora
• Stool Analysis - heme +, check for C. diff toxin

21
Laboratory Findings
• Coagulopathy– Prolonged PT/PTT– Low fibrinogen– Elevated D-dimers
• Electrolytes– Hypo- or hyperglycemia– Hyponatremia– Low bicarb
• ABG/VBG– Metabolic acidosis

22
Differential Diagnosis• Sepsis with ileus• Bacterial enterocolitis: C. diff, other gram
negatives• Mechanical bowel obstruction:
– Hirschsprung – Ileal atresia– Volvulus– Meconium ileus– Intussusception
• Isolated gastric perforation (indocin, steroids)

23
Mean Age at Presentation
Gestational age (weeks)
< 30
31-33
34
Full term
Age at onset (days)
20
14
5
2

Clinical Management
Medical Vs. Surgical

25
Medical Management• Successfully treats ½ to 2/3 of patients• Consult surgery from the start• Bowel rest - NPO, gastric decompression, TPN• Broad spectrum antibiotics for 7-14 days• Cardiopulmonary support• Correction of metabolic acidosis and electrolyte
abnormalities• Treatment of coagulopathy and/or
thrombocytopenia• Serial exams, labs, and x-rays

26
Signs Of Ongoing Necrosis
• Increasing distension
• Persistent:– Metabolic acidosis
– Thrombocytopenia
– Hypotension from third spacing

27
Indications for Surgical Intervention
• Severe peritonitis
• Pneumoperitoneum
• Intra-abdominal abscess
• Positive paracentesis findings (bile & stool)
• Portal venous gas seen on X-ray

28
Surgical Management
• 34-50% of patients
• Laparotomy with resection, formation of enterostomy and mucous fistula
• Patch, drain, and wait
• Primary peritoneal drainage
• Eventual reanastomosis
29
Potential Complications
• Short bowel syndrome• TPN-associated cholestasis with liver
cirrhosis and liver failure• Catheter related sepsis• Intestinal strictures and partial small
bowel obstruction• Enterocolic fistulas• Developmental and growth delay (50%)

30
Long-term Outcome: What’s Important?
• Length of residual bowel• Ileum vs. jejunum (better adaptation)• Presence of ileocecal valve• Presence of intact colon• Maturity of infant and general
condition

31
Survival Without Transplantation
• Patients with > 25cm of normal bowel who have an intact ileocecal valve
Normal bowel length:Term infants 200-300 cmPreterm infants 100-200
cm
• Patients with >40cm of normal bowel who have no ileocecal valve
32
Short Bowel Syndrome• Fluid & electrolyte losses
• Bile acid and Vit B12 malabsorption
• Gastric acid hypersecretion inactivates pancreatic enzymes and causes fat malabsorption
• Secretory diarrhea
• Bacterial overgrowth- Increases malabsorption, lactic acidosis, colitis, Vit B12 deficiency

33
Malabsorption
• Fat: Bacterial deconjugation of bile salts and acids
• Protein and carbohydrates: enzyme and transport deficiencies
• Vit B12: bacterial uptake

34
Sites of Nutrient Absorption
• Duodenum: iron
• Jejunum: Carbohydrates, proteins, fats and vitamins, copper
• Ileum: Bile acids, Vit B12

35
Short Gut: Symptoms
• Distension
• Diarrhea
• Cramping
• Weight loss
• Anemia (occult blood loss, Vit B12 deficiency)

36
Treatment of Short Gut Syndrome
• Promotion of villous hyperplasia:• Drip feedings using elemental formulas
– Long-chain fats stimulate intestinal adaptation– MCT diet bypasses need for bile acids– Hydrolyzed proteins absorbed rapidly
• Cholestyramine (bile acid binder)• Trimethoprim-sulfa, metronidazole treats
bacterial overgrowth• Proton pump inhibitors or H2 blockers

37
Formulas
Elemental:• Require minimal digestive function and
cause less pancreatic secretion• Individual amino acids or short peptides• Glucose polymers• Low fat (long chain triglycerides)• MCT absorbed in absence of lipase or
bile salts

38
Monitoring
• Stool output for fluid losses
• Carbohydrate malabsorption (low stool pH or stool reducing substances)
• Anticipate slow gut adaptation over years
• Weight gain and growth

39
Lengthening Procedures

40

41
Prevention of NEC
• Prenatal steroids• Correction of hypovolemia and hyperviscosity• Slow, gradual advancement of feeds• Breastfeeding• Probiotics - Oral immunoglobulins and bifidobacterium?• Oral antibiotics?• Acidification of feedings (avoidance of PPIs and
H2 blockers)?• Glutamine or arginine supplemenation?
42
Trophic Feedings
• No increased risk of NEC
• Increases gut motility
• Reduces cholestasis
• Improves tolerance of subsequent feedings
• May prevent gut atrophy, inflammation, and bacterial translocation