Embed Size (px)
Citation preview
Neck CancerHead and
STATEMENTS ON
January 28, 2006
Frankfurt am Main, Germany
SurgerySurgery in Multimodal Treatment
Jatin P. Shah, MD, FACSHon. FRCS (Edin), Hon. FRACS,
Hon. FDSRCS (Lond.)
Professor of Surgery
Elliot W. Strong Chair in Head and Neck Oncology
Chief, Head and Neck Service
Memorial Sloan-Kettering Cancer Center
New York, New York
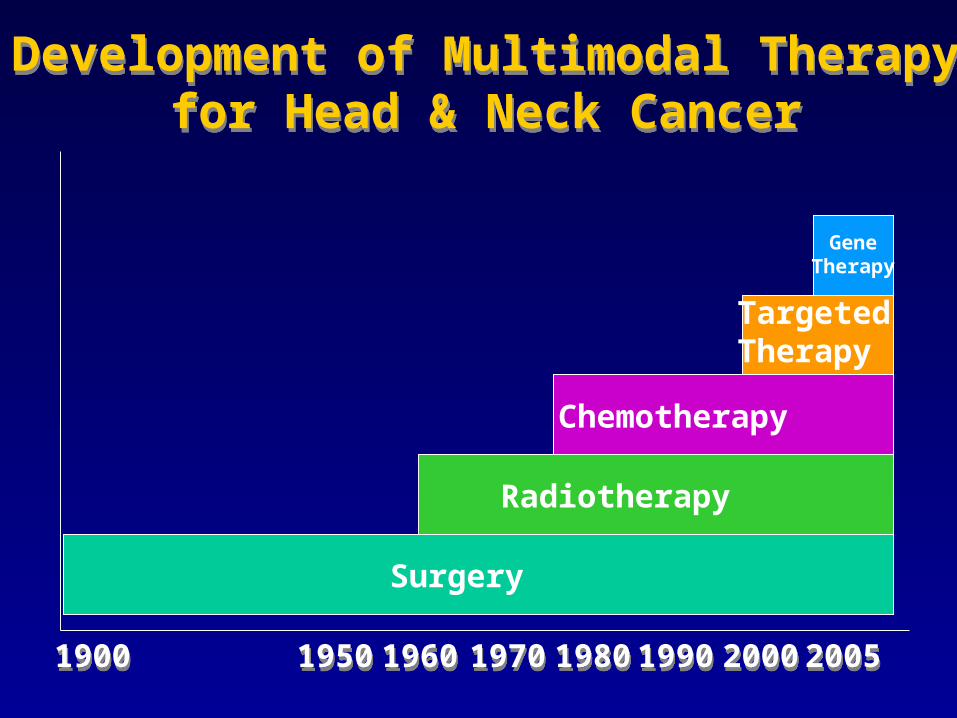
Development of Multimodal Therapyfor Head & Neck Cancer
Development of Multimodal Therapyfor Head & Neck Cancer
19001900 19501950 19601960 19801980 20002000
Surgery
Radiotherapy
Chemotherapy
1990199019701970
Targeted Therapy
20052005
GeneTherapy
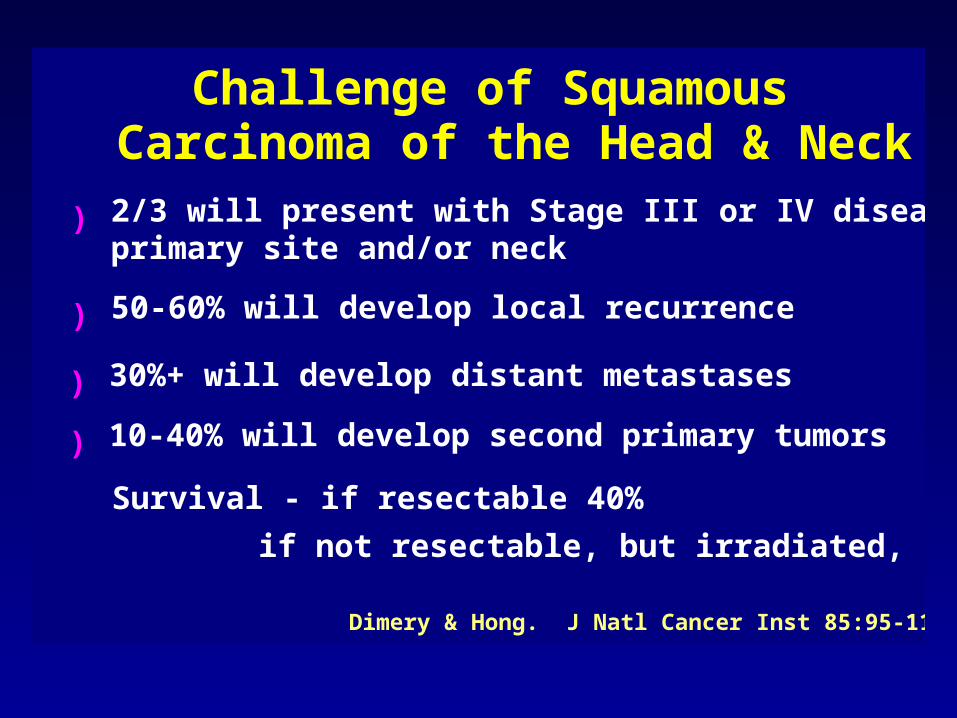
Challenge of Squamous Carcinoma of the Head & Neck2/3 will present with Stage III or IV disease at primary site and/or neck
)
50-60% will develop local recurrence)
30%+ will develop distant metastases)
10-40% will develop second primary tumors)
Dimery & Hong. J Natl Cancer Inst 85:95-111, 1993.
Survival - if resectable 40%
if not resectable, but irradiated, 20%
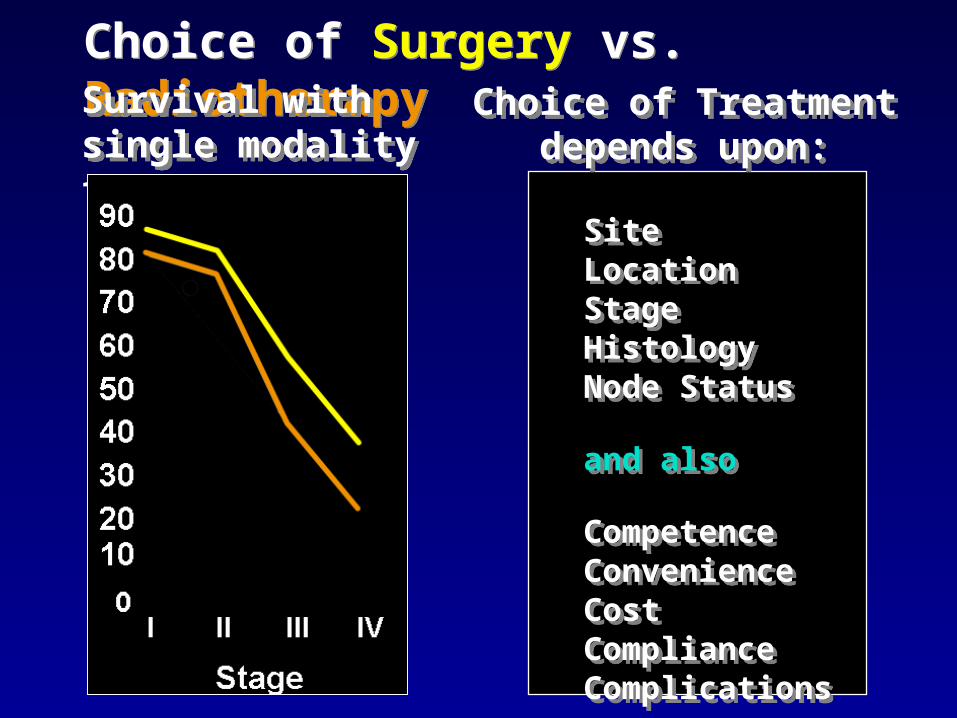
Choice of Surgery vs. RadiotherapyChoice of Surgery vs. Radiotherapy
SiteLocationStageHistologyNode Status
and also
CompetenceConvenienceCostComplianceComplications
SiteLocationStageHistologyNode Status
and also
CompetenceConvenienceCostComplianceComplications
Survival with single modality treatmentSurvival with single modality treatment
Choice of Treatment depends upon:
Choice of Treatment depends upon:
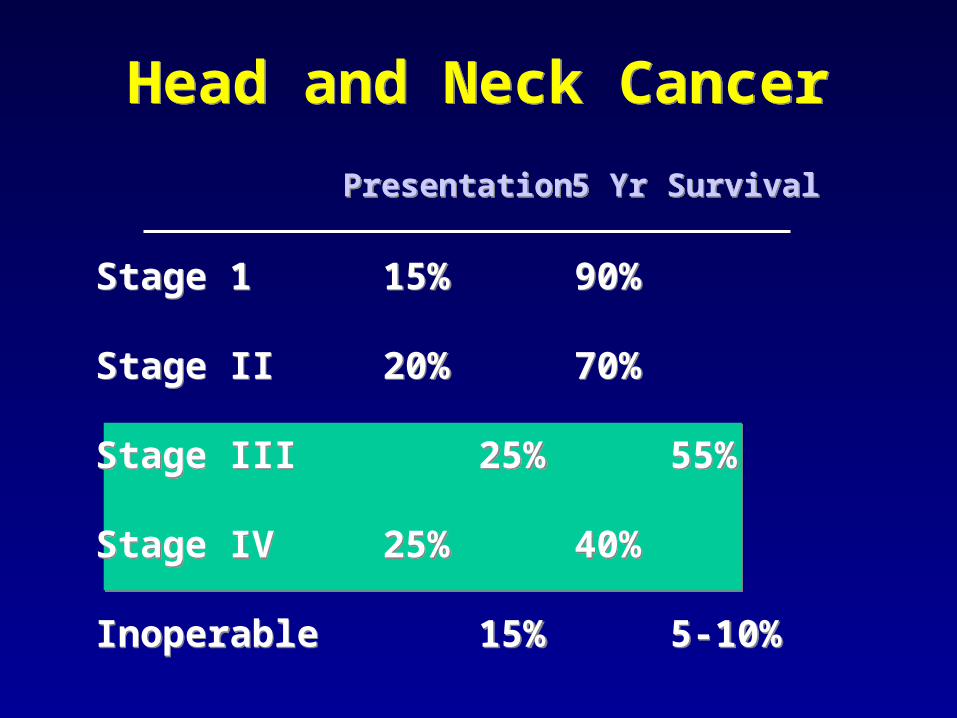
Head and Neck CancerHead and Neck Cancer
Stage 1 15% 90%
Stage II 20% 70%
Stage III 25% 55%
Stage IV 25% 40%
Inoperable 15% 5-10%
Stage 1 15% 90%
Stage II 20% 70%
Stage III 25% 55%
Stage IV 25% 40%
Inoperable 15% 5-10%
PresentationPresentation 5 Yr Survival5 Yr Survival
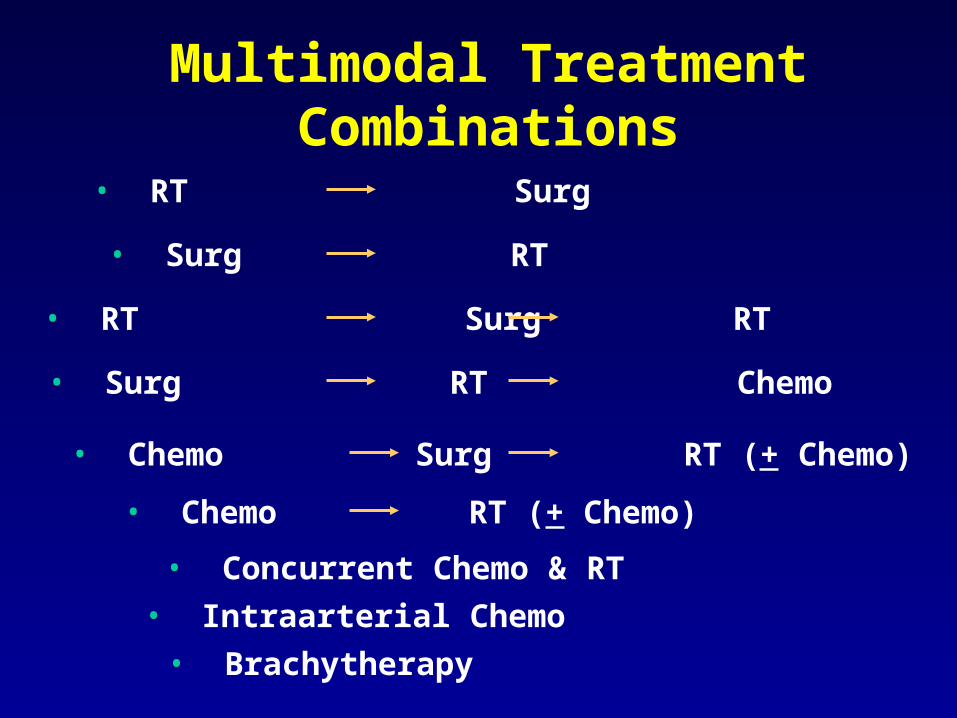
Multimodal TreatmentCombinations
• RT Surg
• Surg RT
• RT Surg RT
• Surg RT Chemo
• Chemo Surg RT (+ Chemo)
• Chemo RT (+ Chemo)
• Concurrent Chemo & RT
• Intraarterial Chemo
• Brachytherapy
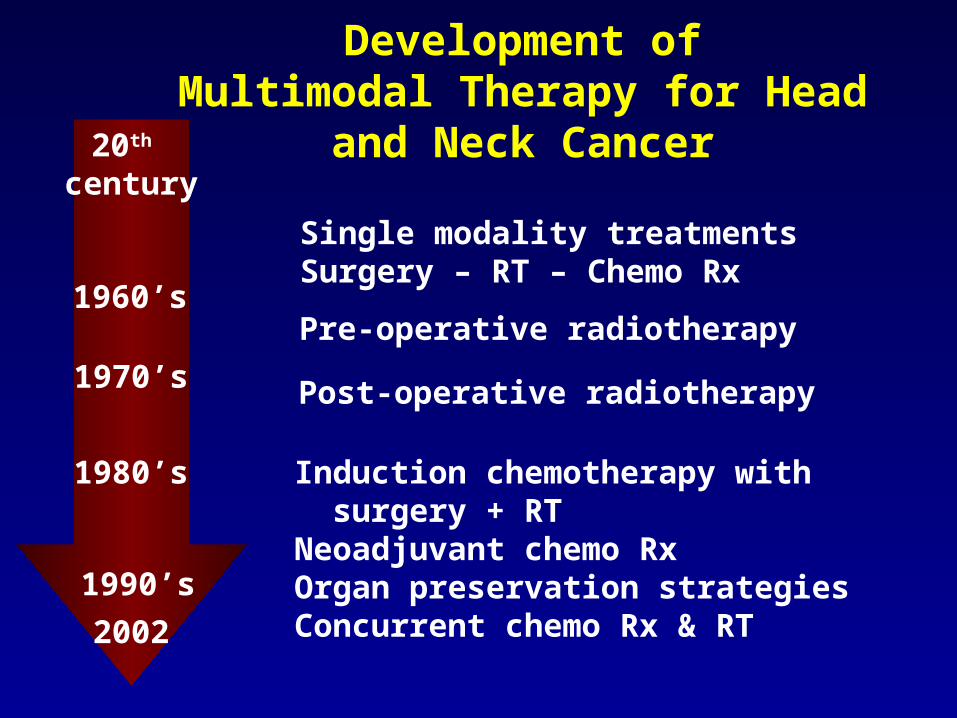
Development ofMultimodal Therapy for Head and
Neck Cancer20th century
1960’s
1970’s
1980’s
2002
Single modality treatmentsSurgery – RT – Chemo Rx
Pre-operative radiotherapy
Post-operative radiotherapy
Induction chemotherapy with surgery + RTNeoadjuvant chemo RxOrgan preservation strategiesConcurrent chemo Rx & RT
1990’s

Levels of Evidence
1. Randomized controlled trial or
Meta-analysis
2. Nonrandomized controlled clinical trial, subset analysis of RCT
3. Case series, population based, consecutive or not
4. Opinions of respected authorities based upon clinical experience or reports of expert committees
MEDLINE
• Over 9 million articles, dating to 1966
• 31,000 added each month– 754,383 (8.4%) - human cancer – 131,760 (1.5%) - clinical trials– 68,301 (0.75%) - prospective randomized
• 5,811 (0.06%) human cancer prospective randomized clinical trials
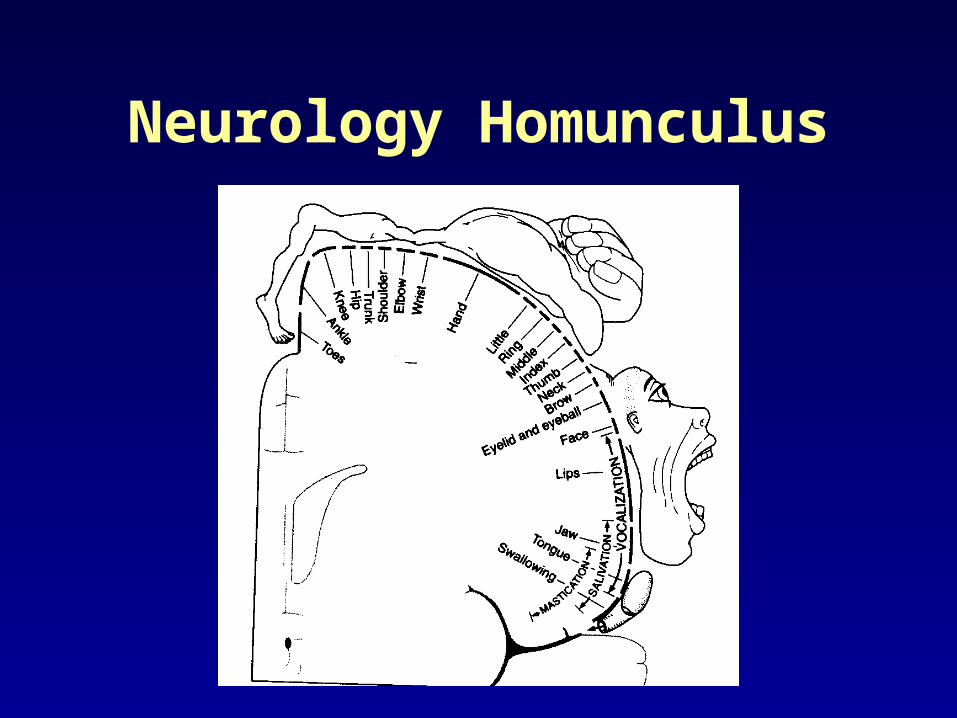
Neurology Homunculus
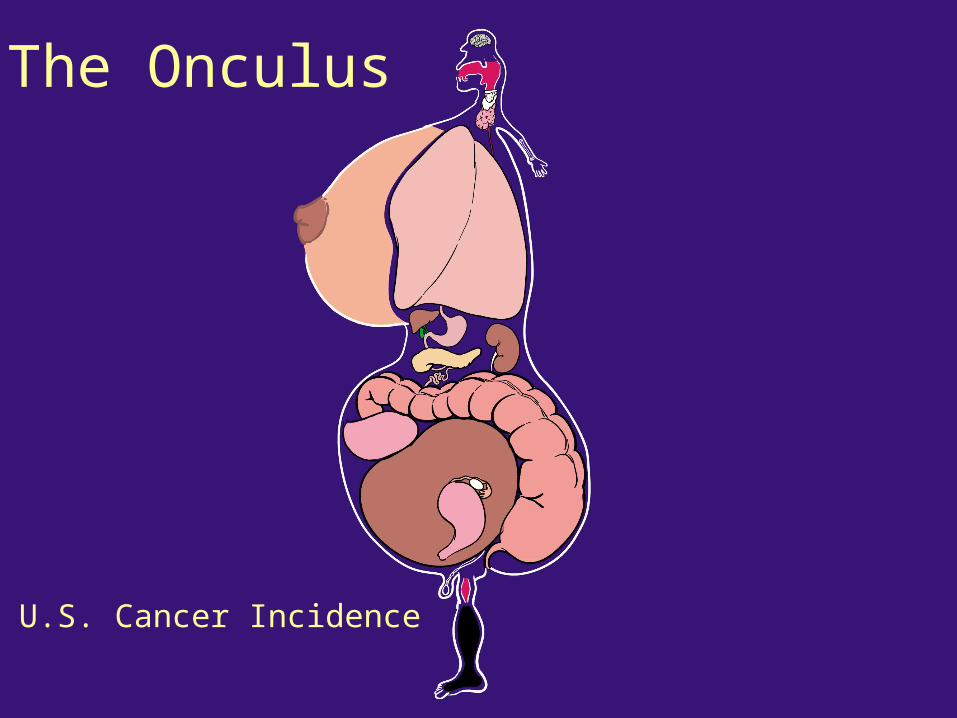
U.S. Cancer Incidence
The Onculus
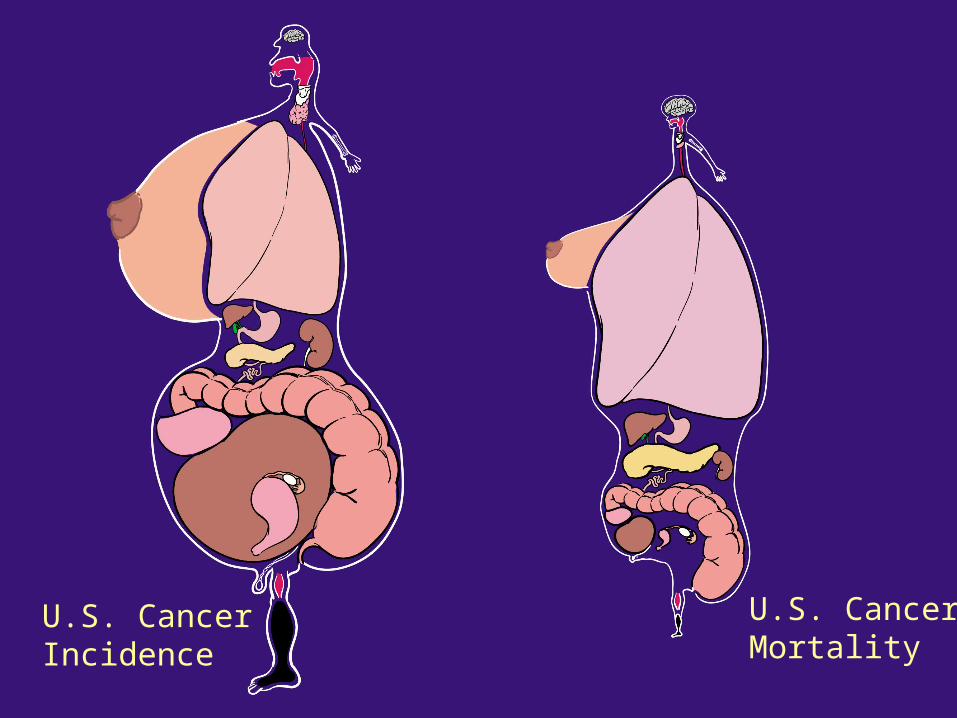
U.S. CancerIncidence
U.S. CancerMortality
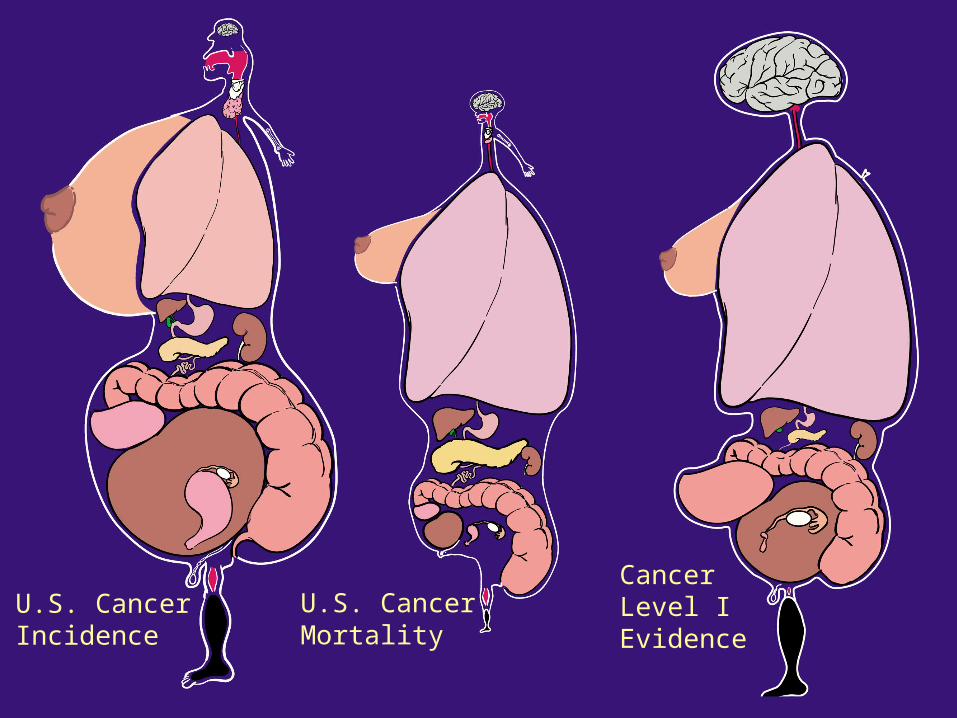
Cancer Level I Evidence
U.S. CancerIncidence
U.S. CancerMortality
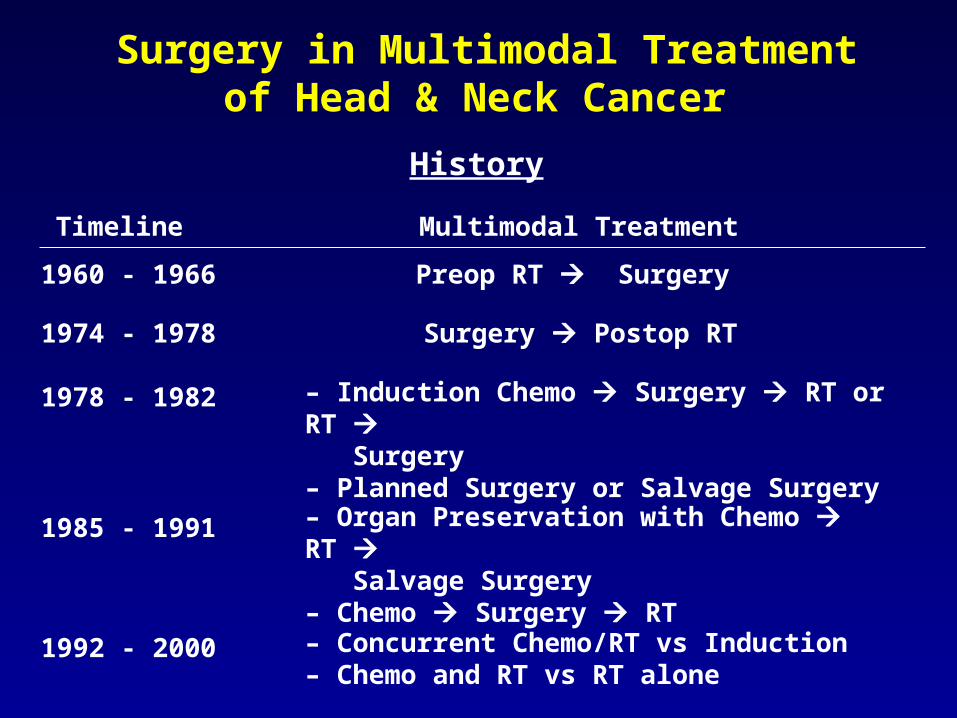
Surgery in Multimodal Treatment of Head & Neck Cancer
Timeline
1960 - 1966 Preop RT Surgery
Surgery Postop RT
– Induction Chemo Surgery RT or RT Surgery– Planned Surgery or Salvage Surgery
History
Multimodal Treatment
1974 - 1978
1978 - 1982
1985 - 1991 – Organ Preservation with Chemo RT Salvage Surgery– Chemo Surgery RT
1992 - 2000 – Concurrent Chemo/RT vs Induction– Chemo and RT vs RT alone
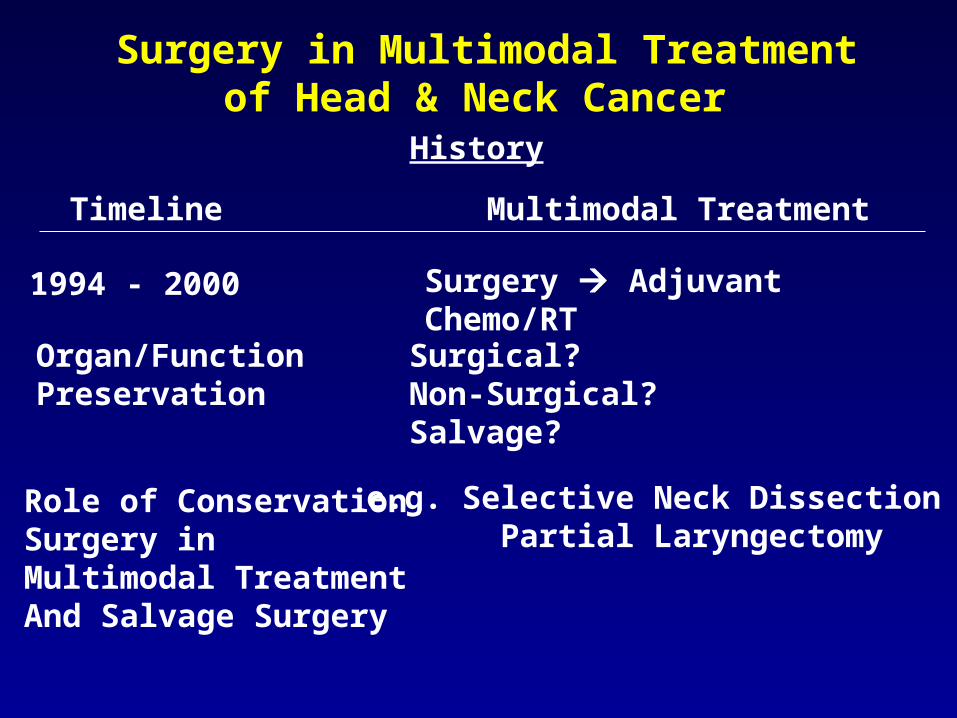
Surgery in Multimodal Treatment of Head & Neck Cancer
Timeline
History
Multimodal Treatment
1994 - 2000 Surgery Adjuvant Chemo/RT
Organ/FunctionPreservation
Role of ConservationSurgery in Multimodal TreatmentAnd Salvage Surgery
Surgical?Non-Surgical?Salvage?
e.g. Selective Neck Dissection Partial Laryngectomy
Preoperative Radiation and Radical Neck Dissection
1960 – 1966348 Patients
Surg Clin North Am. Apr 1969; 49(2):271-276.
Strong EW.
Elective Postoperative Radiation Therapy in Stages III and IV
Epidermoid Carcinoma of the Head and Neck
Vikram B, Strong EW, Shah J, Spiro RH.
Am J Surg. Oct 1980; 140(4):580-584.
1974 – 1978104 Patients
Adjuvant Chemotherapy for Advanced Head and Neck
Squamous Carcinoma
Final Report of the Head and Neck Contracts Program.
Cancer. Aug 1 1987; 60(3):301-311.
1978 – 1982462 Patients
Induction Chemotherapy Plus Radiation Compared with
Surgery Plus Radiation in Patients with Advanced Laryngeal Cancer
The Department of Veterans Affairs Laryngeal Cancer Study Group
N Engl J Med. Jun 13 1991; 324(24):1685-1690.
1985 – 1991332 Patients
Concurrent Chemotherapy and Radiotherapy for Organ Preservation in
Advanced Laryngeal Cancer
Forastiere AA, Goepfert H, Maor M, et al.N Engl J Med. Nov 27 2003; 349(22):2091-2098.
1992 – 2000547 Patients
Postoperative Irradiation with or without Concomitant Chemotherapy for
Locally Advanced Head and Neck Cancer
Bernier J, Domenge C, Ozsahin M, et al.N Engl J Med. May 6 2004; 350(19):1945-1952.
1994 – 2000334 Patients
Postoperative Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma
of the Head and Neck
Cooper JS. Pajak TF, Forastiere AA, et al.N Engl J Med. May 6 2004; 350(19):1937-1944.
1995 – 2000459 Patients
Limitations to OrganPreservation Approach
• Previous radiotherapy
• Cartilage invasion
• T4 primary
• Non laryngeal sites (BOT, hypopharynx)
• < C.R.
• Medical contraindications (renal, pulmonary, otologic)
2. SCC of Nasal Cavity and Paranasal Sinuses
Surgery Remains Initial Definitive Treatment for Most Sites in Head & Neck
3. Advanced Carcinomas (T4) of the Larynx and Hypopharynx
1. SCC of Oral Cavity
4. Salivary Tumors
5. Thyroid Cancer
6. Sarcomas
7. Skin Cancer and Melanoma
Surgery Employed as Planned Intervention in
Multimodal Treatment Programs
N2 – N3 Disease
Post Chemo/RT?
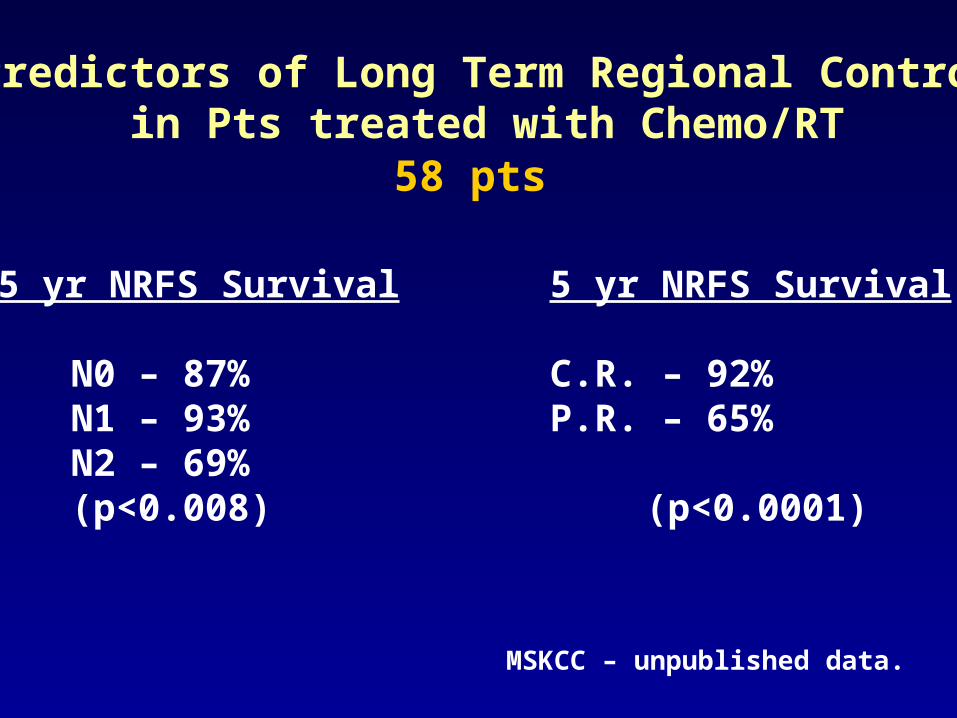
Predictors of Long Term Regional Controlin Pts treated with Chemo/RT
5 yr NRFS Survival 5 yr NRFS Survival
N0 – 87% C.R. – 92%N1 – 93% P.R. – 65%N2 – 69%(p<0.008) (p<0.0001)
MSKCC – unpublished data.
58 pts
• Planned Comprehensive Neck Dissection• Planned Selective Neck Dissection• Nidusectomy• Observation• Imaging – PET/CT/MRI
Management of the NeckAfter Chemo/Radiotherapy
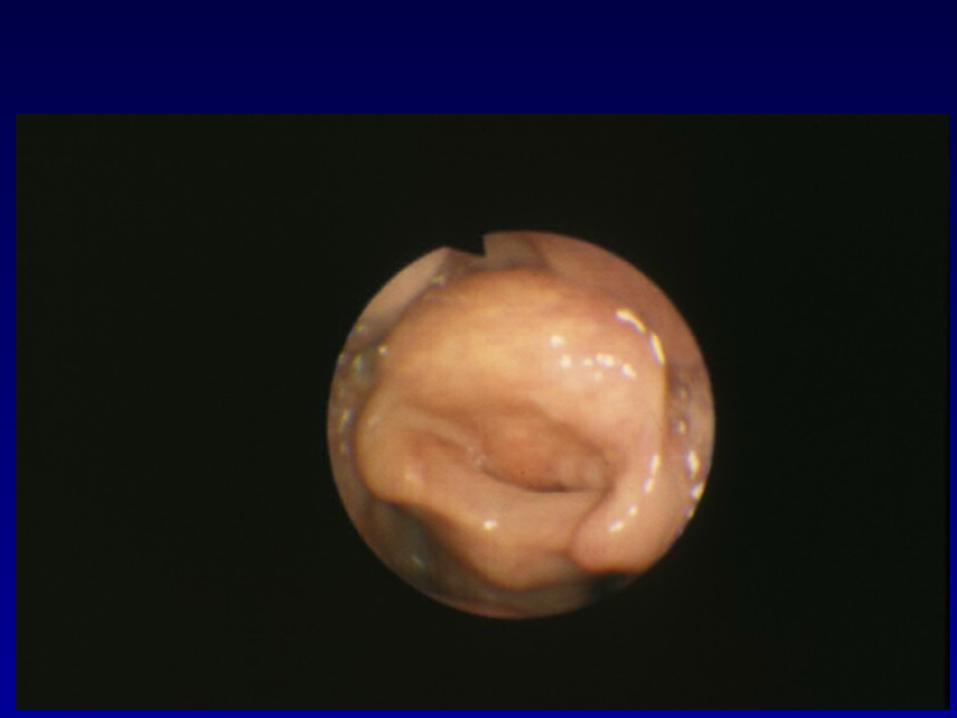
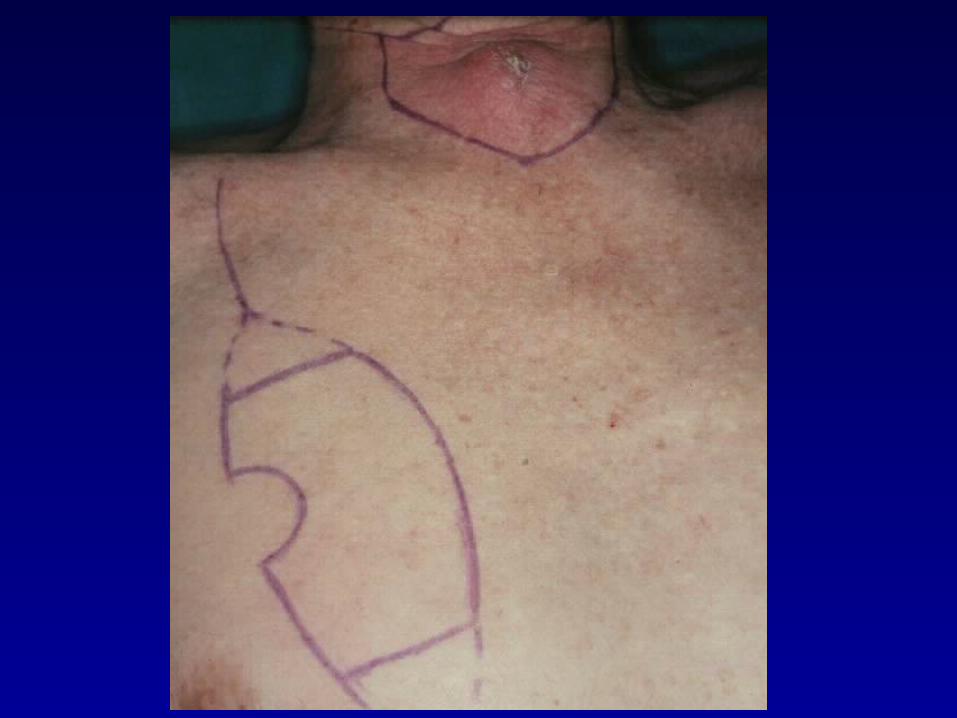
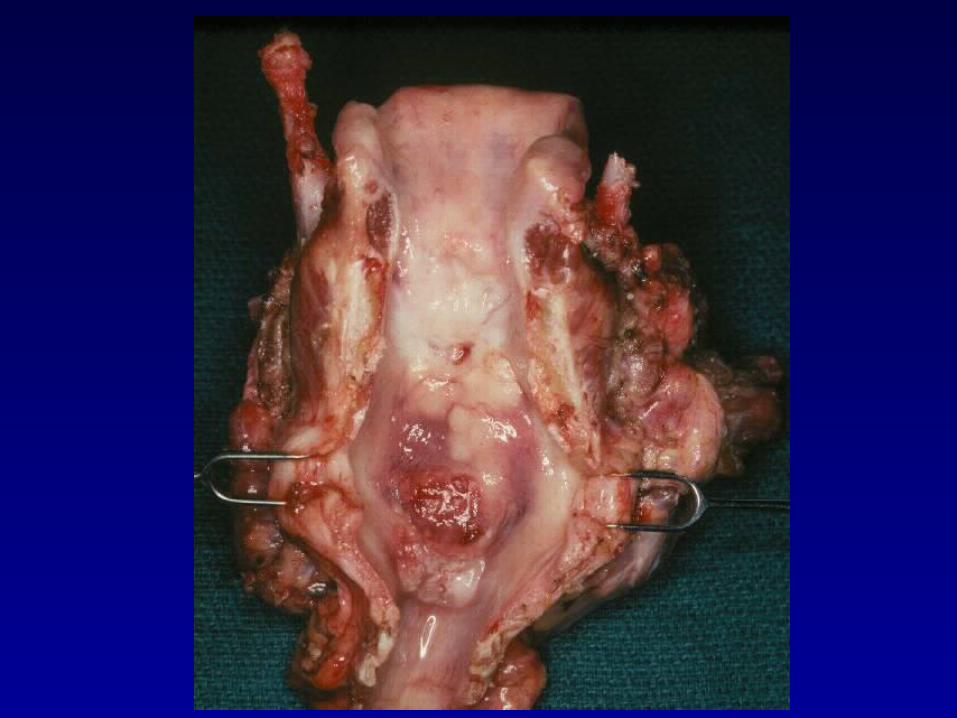
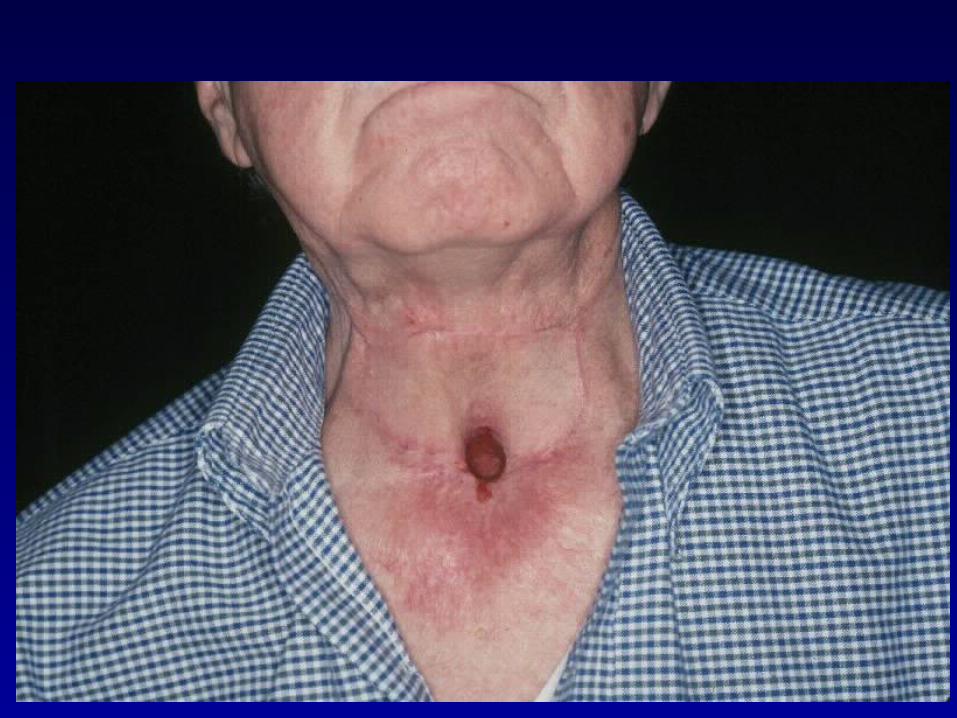
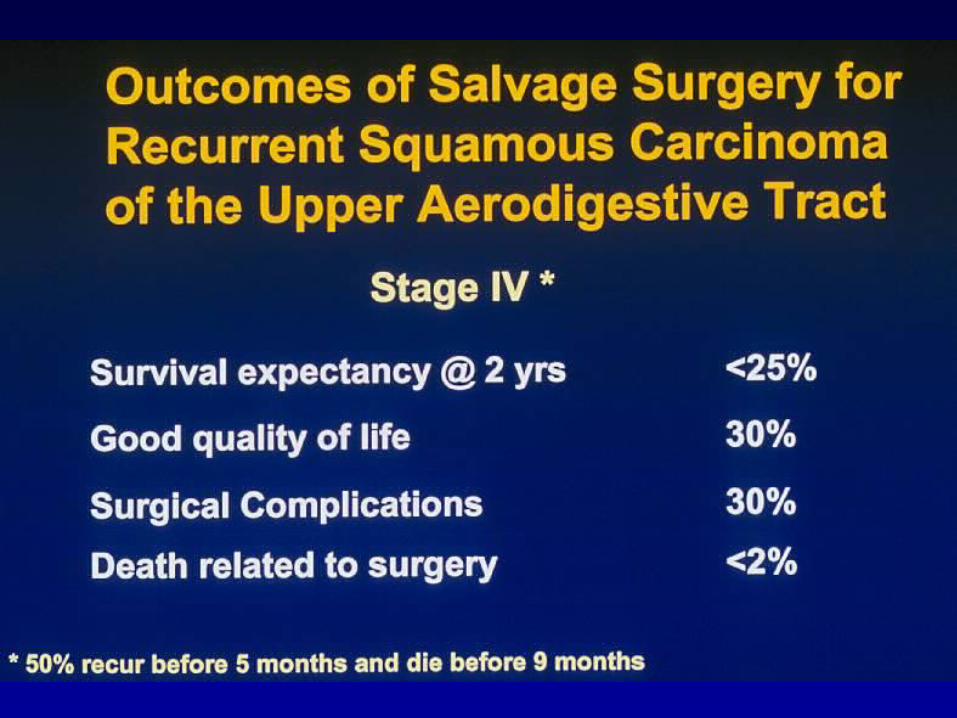
Surgery Employed asSalvage Treatment for
Chemo/RT Failure/Recurrence
1. Ca of Oropharynx
2. Ca of Larynx/Hypopharynx
3. Ca of Nasopharynx (?)
4. Metastatic Ca to Neck Nodes
• 139 pts – treated with RT
• 35 recurred in neck
Salvage of Recurrent Neck Diseasein Radiated Neck
• Salvage attempted in 9, but successful in 2
• 75 pts with OPH treated with RT
• Mendenhall W.M., et al (1984)
• Peters L.J., et al (1996)
• 62 had a CR
• 8 recurred in neck
• Salvage attempted in 7, but successful in 1







Jerry Goodwin
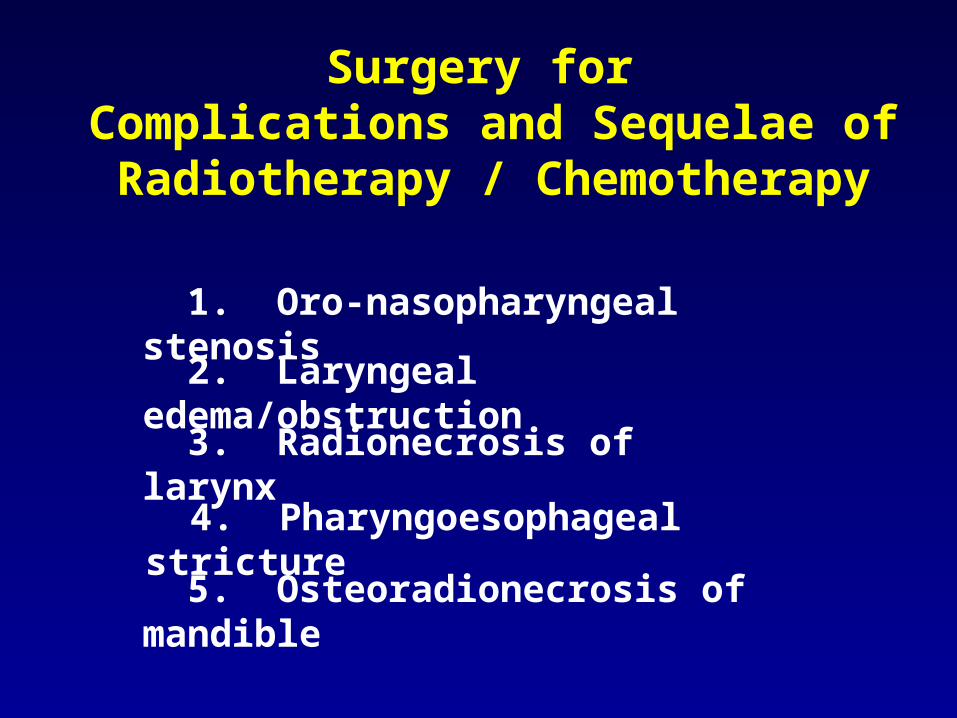
2. Laryngeal edema/obstruction
Surgery for Complications and Sequelae of Radiotherapy / Chemotherapy
3. Radionecrosis of larynx
1. Oro-nasopharyngeal stenosis
4. Pharyngoesophageal stricture
5. Osteoradionecrosis of mandible
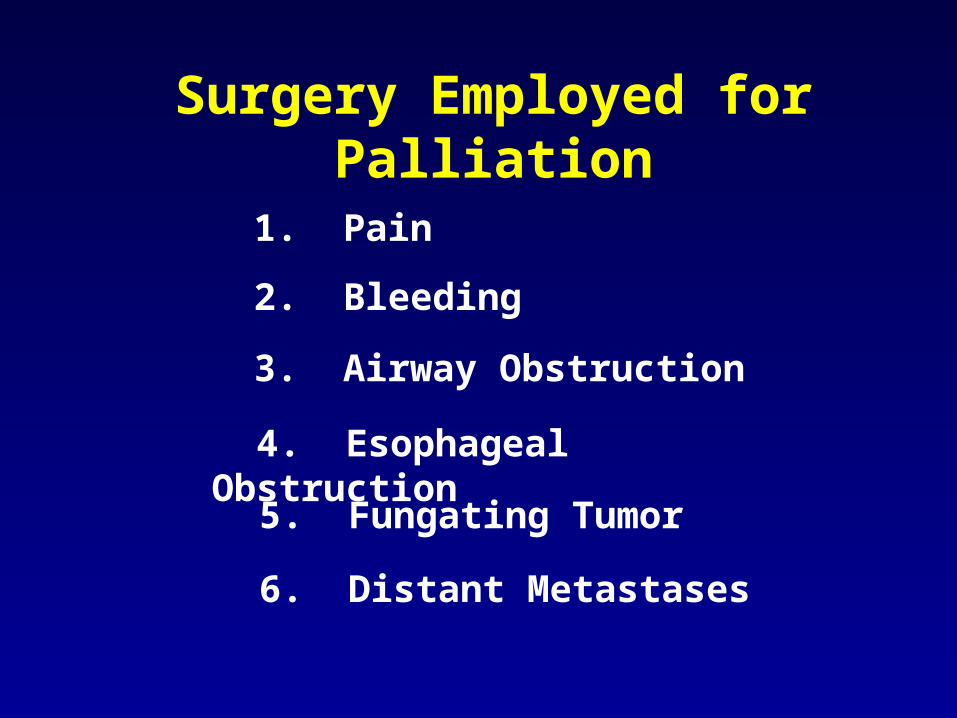
2. Bleeding
Surgery Employed for Palliation
3. Airway Obstruction
1. Pain
4. Esophageal Obstruction
5. Fungating Tumor
6. Distant Metastases




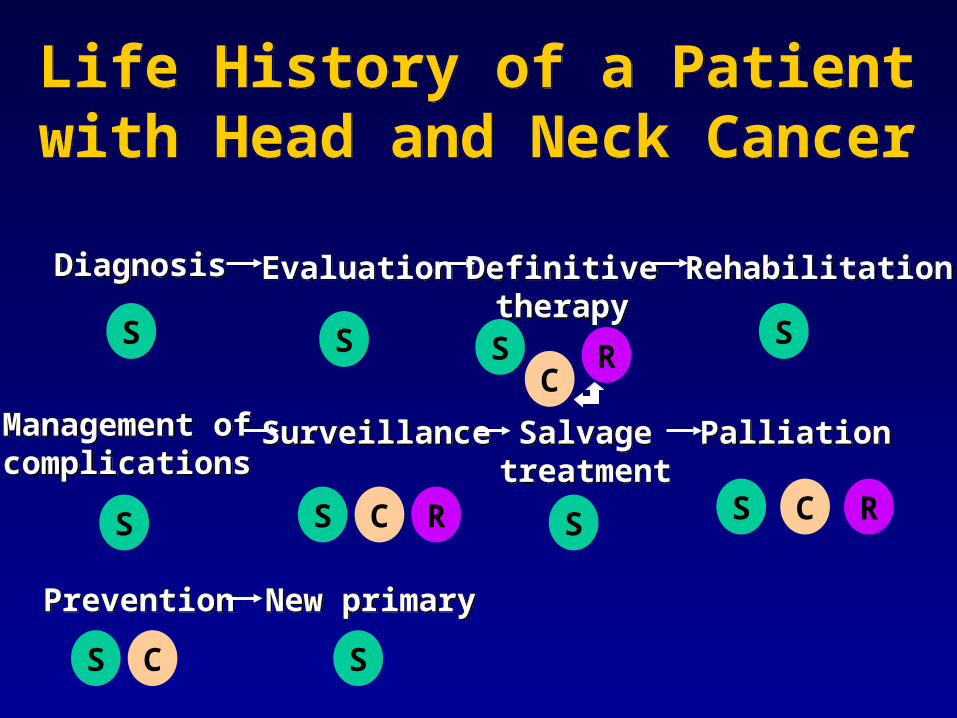
Life History of a Patientwith Head and Neck Cancer
Life History of a Patientwith Head and Neck Cancer
DiagnosisDiagnosis EvaluationEvaluation Definitivetherapy
Definitivetherapy
RehabilitationRehabilitation
Management ofcomplications
Management ofcomplications
SurveillanceSurveillance SalvagetreatmentSalvage
treatmentPalliationPalliation
PreventionPrevention New primaryNew primary
S S S S
S S S S
S S
R
R R
C
C C
C

Copyright restrictions may apply.
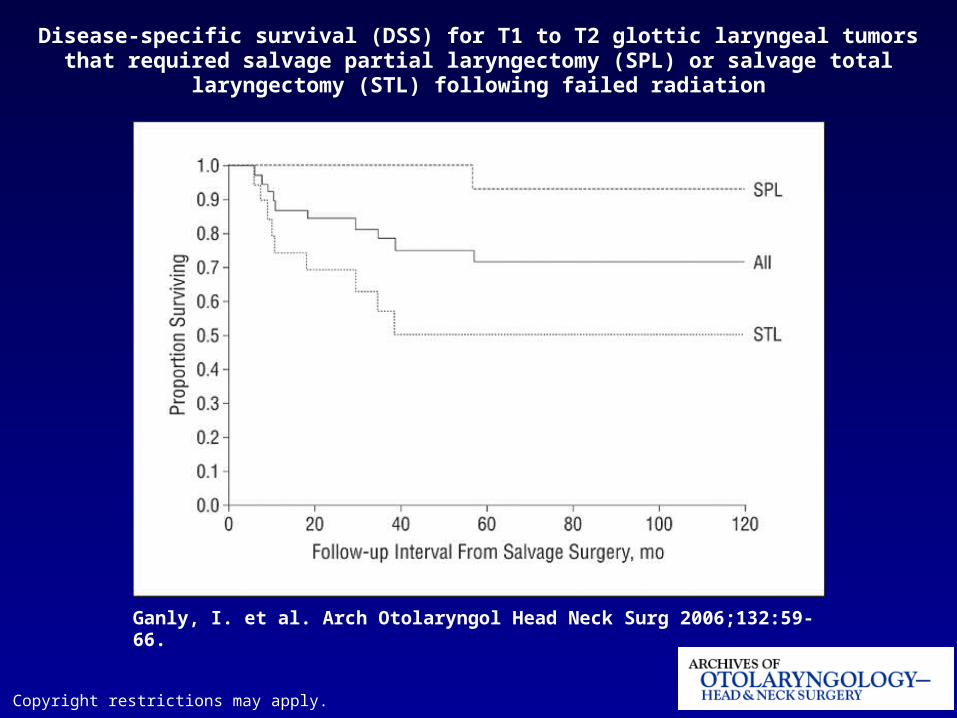
Ganly, I. et al. Arch Otolaryngol Head Neck Surg 2006;132:59-66.
Disease-specific survival (DSS) for T1 to T2 glottic laryngeal tumors that required salvage partial laryngectomy (SPL) or salvage total laryngectomy (STL) following failed radiation
Copyright restrictions may apply.
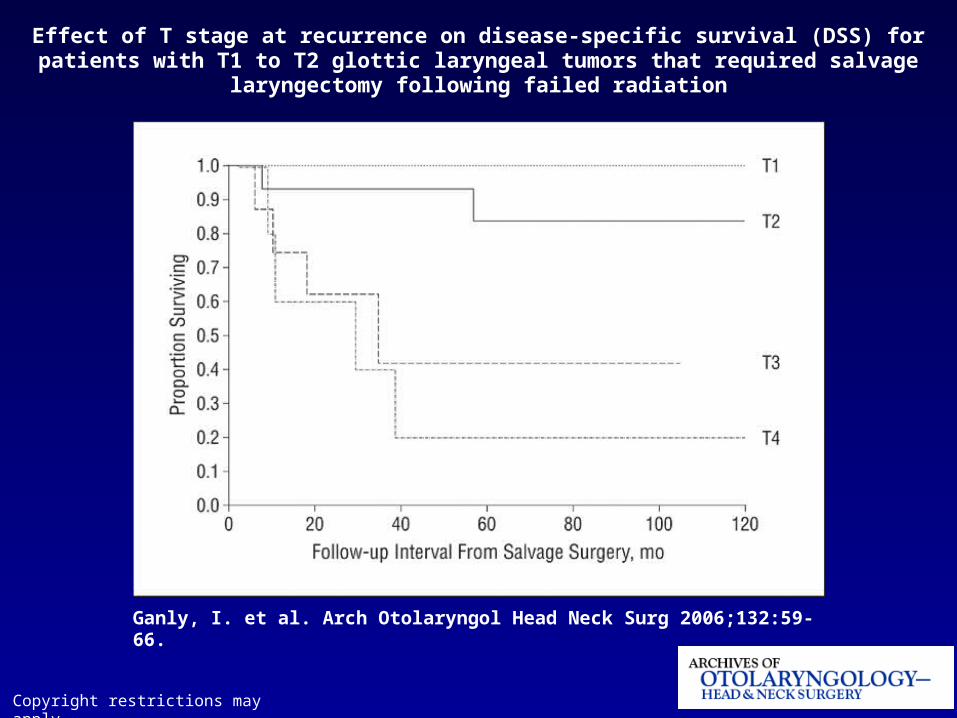
Ganly, I. et al. Arch Otolaryngol Head Neck Surg 2006;132:59-66.
Effect of T stage at recurrence on disease-specific survival (DSS) for patients with T1 to T2 glottic laryngeal tumors that required salvage laryngectomy following failed radiation





























