Embed Size (px)
Citation preview

KING EDWARD MEMORIAL HOSPITAL AND
PRINCESS MARGARET HOSPITAL
Neonatology Clinical Care Unit
DRUG PROTOCOLS
Part I

A ACETYLCYSTEINE ACICLOVIR ADENOSINE ADRENALINE ALBUMIN (HUMAN) 20% ALBUMIN (HUMAN) 4% ALPROSTADIL (PROSTAGLANDIN E1) AMIKACIN AMOXYCILLIN AMOXYCILLIN & CLAVULANIC ACID
(AUGMENTIN DUO 400 / CLAMOXYL DUO 400) AMPHOTERICIN (FUNGIZONE) AMPHOTERICIN LIPOSOMAL (AMBISOME) ATROPINE SULPHATE
B BCG (BACILLUS CALMETTE-GUÉRIN) VACCINE BENZYLPENICILLIN (PENICILLIN-G)
C CAFFEINE CALCITRIOL CALCIUM CARBONATE CALCIUM GLUCONATE CAPTOPRIL CARBAMAZEPINE CEFOTAXIME CEFTAZIDIME CEFTRIAXONE CEPHALEXIN CEPHALOTHIN CEPHAZOLIN CHLORAL HYDRATE CHLORAMPHENICOL OPHTHALMIC
PREPARATIONS CIPROFLOXACIN CLINDAMYCIN CLONAZEPAM CO-TRIMOXAZOLE
(Trimethoprim/Sulphamethoxazole)
D DEXAMETHASONE PHOSPHATE DIAZEPAM DIAZOXIDE DIGOXIN DILACAINE EYE DROPS – PMH FORMULATION DIPTHERIA-TETANUS-ACELLULAR PERTUSSIS
(DTPa), HEPATITIS B AND INACTIVATED POLIO VACCINE (INFANRIX PENTA)
DIPTHERIA-TETANUS-ACELLULAR PERTUSSIS (DTPa), HEPATITIS B, POLIOVIRUS AND HAEMOPHILUS INFLUENZAE TYPE B VACCINE (INFANRIX HEXA)
DOBUTAMINE DOMPERIDONE DOPAMINE
E ERYTHROMYCIN
ERYTHROPOIETIN
F FAT EMULSION 20% FERROUS SULPHATE FLECAINIDE FLUCLOXACILLIN FLUCONAZOLE FLUCYTOSINE FLUDROCORTISONE ACETATE FLUMAZENIL FLUTICASONE FOLIC ACID FRAMYCETIN EYE DROPS FRUSEMIDE FUSIDIC ACID
G GANCICLOVIR GENTAMICIN GLUCAGON GLYCERYL TRINITRATE GLYCERYL TRINITRATE TOPICAL GLYCOPYROLLATE
H HAEMOPHILUS INFLUENZAE TYPE B
CONJUGATE VACCINE HEPARIN SODIUM HEPATITIS B VACCINE HYALURONIDASE HYDRALAZINE HYDROCHLORIDE HYDROCHLOROTHIAZIDE HYDROCORTISONE HYDROXYCHLOROQUINE
I INDOMETHACIN INSULIN HUMAN, NEUTRAL (ACTRAPID /
HUMULIN-R) ISOPRENALINE
L LIGNOCAINE
M MAGNESIUM SULPHATE MEDIUM CHAIN TRIGLYCERIDES OIL (MCT) MEROPENEM METHYLDOPA METHYLENE BLUE METRONIDAZOLE MICONAZOLE MIDAZOLAM MORPHINE SULPHATE MYLANTA

FORMULAS 1) TO WORK OUT HOW MANY MG/KG/MIN OF GLUCOSE
Rate x dext% x 1000 = mg/hr 100 mg/hr = mg/kg/hr wt mg/kg/hr = mg/kg/min 60 Eg 4ml/hr – 1.5 kg baby – 5% glucose 4 x 5 x 1000 = 200 100 200 = 133.3 mg/kg/hr 1.5 133.3 = 2.2 mg/kg/min 60
2) TO INCREASE GLUCOSE PERCENTAGE
Vol x (req% - avail%) = amount of additive (add % - avail% glucose required To make 50ml of 13% glucose, using 50% glucose ampoules and 10% bags Eg 50 x (13-10) = 50 x 3 = 15 (50-10) 40 4 = 3.75 mls 50% glucose and 46.25 mls of 10% glucose
3) TO DECREASE GLUCOSE PERCENTAGE Required strength x volume
Stock strength = amount of stock glucose plus amount of H20 Eg decrease 5% - 3% to make a 50 ml syringe 3 x 50 30 mls 5% glucose and 20 mls of H20 5

METRIC CONVERSION 1 mg = 1000 microgram 0.1 mg = 100 microgram 0.01 mg = 10 microgram
TO CONVERT mg TO MICROGRAM mg x 1000 = microgram eg 2.3 mg = 2.3 x 1000 = 2,300 microgram
TO CONVERT MICROGRAM TO mg microgram = mg 1000 eg 100 = 0.1 mg 1000

KING EDWARD MEMORIAL AND PRINCESS MARGARET HOSPITALS NEONATOLOGY CLINICAL CARE UNIT (NCCU)
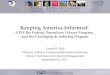
INJECTABLE DRUG GUIDELINES This table provides a guide to the compatibilities of drugs commonly infused in the NCCU. Drug compatibilities are concentration, temperature and light dependant. Do not use solutions where there is a visual change in the bag, or tubing. Contact your pharmacist for further information.
Am
phot
eric
in
Cal
cium
G
luco
nate
Dob
utam
ine
Dop
amin
e
Mor
phin
e
Sodi
um
bica
rbon
ate
TPN
*
Sodi
um
Chl
orid
e
Glu
cose
Amphotericin • No No No No Yes No No Use
Buffered\Solution
Calcium Gluconate
No • Yes Yes Yes No Yes Yes Yes
Dobutamine
No Yes • Yes Yes No Yes Yes Yes
Dopamine
No Yes Yes • Yes No Yes Yes Yes
Morphine
No Yes Yes Yes • No Yes Yes Yes
Sodium Bicarbonate
Yes No No No No • No Yes Yes
TPN *
No Yes Yes Yes Yes No • Yes Yes
TPN is the amino acid/glucose solution only. It does not include Fat Emulsion.

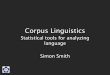
CALCULATION OF THE COMPOSITION OF DRUG INFUSIONS (50mL SYRINGE PUMP) 1. SELECT DESIRED DRUG DOSAGE TO BE DELIVERED IN microgram/kg/min. 2. SELECT INFUSION RATE OF SYRINGE PUMP IN mL/HOUR (FROM CENTRE OF TABLE). 3. CALCULATE NUMBER OF MILLIGRAMS OF DRUG TO BE MIXED IN 50mL SYRINGE. EG: 10kg CHILD, 0.1-0.2 microgram/kg/min, Infusion rate 1-2mL/hr PUT 0.3 milligram/kg (3 milligram) IN 50mL. mg= milligram Infusion rate required
0.15mg/kg in 50mL
0.3mg/kg in 50mL
0.6mg/kg in 50mL
1.5mg/kg in 50mL
3mg/kg in 50mL
6mg/kg in 50mL
15mg/kg in 50mL
30mg/kg in 50mL
60mg/kg in 50mL
Suggested doses for commencement of treatment
Microgram/ kg/min
0.05 0.1 0.2 0.3 0.4 0.5
mL/hr
1 2 4 6 8
10
mL/hr 1 2 3 4 5
mL/hr 1
1.5 2
mL/hr 1
Adrenaline, Noradrenaline infusions: 0.1-0.2 microgram/kg/min Increase to a maximum of 1.5 microgram/kg/min Isoprenaline infusion: 0.1 microgram /kg/min
0.6 0.7 0.8 0.9 1.0
12 14 16 18 20
6 7 8 9
10
3
4
5
2
mL/hr 1
Midazolam, Vecuronium infusions: 1-2 microgram/kg/min
1.5 2.0 3.0 4.0 5.0
15 20
10
20
3 4 6 8
10
1.5 2 3 4 5
mL/hr 1
1.5 2
mL/hr 1
6.0 7.0 8.0 9.0
10.0
12 14 16 18 20
6 7 8 9
10
3
4
5
2
mL/hr 1
12.0 14.0 15.0 20.0 25.0
12 14 15 20
6 7
10
3 4 5
1.5 2
mL/hr 1
Dopamine, Dobutamine infusions: 5-10 microgram/kg/min Increase to a maximum of 20 microgram/kg/min
30.0 40.0 50.0
100.0 150.0 200.0
15 20
6 8
10 20
3 4 5
10 15 20
1.5 2
5
10

DRUG: ACETYLCYSTEINE
PRESENTATION: Ampoule: 200mg/mL
Solution for direct application, instillation or nebulisation.
ACTION & INDICATION:
Mucolytic for use in bronchopulmonary disease
DOSE:
ADMINISTRATION:
COMMENTS:
0.5mL twice daily
To be diluted with 0.5mL or required amount of 0.9% sodium chloride injection and nebulised via CPAP, ETT or mask. (See instruction sheet)
Do not use in infants with renal or liver impairment
REFERENCES:
DATE: June 2008

DRUG: ACICLOVIR
PRESENTATION: Vial: 250mg / 10mL, or 250mg (powder for reconstitution)
Tablets: 200mg dispersible tablets
ACTION & INDICATION:
Antiviral agent active against Herpes simplex type I and II, and varicella virus by inhibiting viral replication. Used for the prophylaxis or treatment of herpes infection, and varicella infection.
DOSE: IV: <30 weeks: 20mg/kg/dose 24 hourly
30-32 weeks: 20mg/kg/dose 18 hourly
>32 weeks:
First week of life: 20mg/kg/dose 12 hourly
2nd to 12th week of life: 20mg/kg/dose 8 hourly
Oral: Consult Microbiologist
PREPARATION: IV: Use solution prepared by Pharmacy if available. Vial contains 250mg in 10mL. However if 250mg powder for reconstitution is supplied, add 10mL of 0.9% sodium chloride to vial (to give 250mg/10mL) .
Further dilute as follows:
Diluent: 0.9% Sodium chloride or Water for Injections Withdraw 1mL from vial and dilute to 5mL = 5mg/mL
Oral: Disperse one tablet in 20mL of water = 200mg/20mL
ADMINISTRATION: Intravenous: Infuse over 60 minutes via syringe pump.
ADVERSE EFFECTS : Renal damage with increasing urea and creatinine – risk increased by dehydration, bolus injection or other nephrotoxic drugs.
Ensure adequate hydration prior to and during therapy to avoid drug crystallisation in renal tubules. Monitor urine output, creatinine and U & E's twice weekly during therapy.
Inflammation at injection site.
Blood dyscrasias. Monitor Full Blood Count twice weekly
COMMENTS: Administer for 2 weeks for cutaneous/visceral neonatal herpes and for 3 weeks for neonatal CNS infection
Do not refrigerate – drug may precipitate from solution.
Discard reconstituted vial after 24 hours Discard dispersed tablet after 24 hours
REFERENCES:
Neonatal Pharmacopoeia 2nd Ed 2005 Pharmacy Department, The Royal Women’s Hospital Melbourne Therapeutic Guidelines. Antibiotic 13th Ed 2006
DATE: June 2008

DRUG: ADENOSINE
PRESENTATION: Vial: 6mg/2mL
ACTION & INDICATION :
Supraventricular tachycardia Slows AV node conduction and atrial automaticity. No effect on atrial flutter or fibrillation. No effect on ventricular muscle.
DOSE : Initial dose: 100 microgram/kg
Increase dose in 50 microgram/kg increments every 2 minutes until return of sinus rhythm.
Maximum dose: 300 microgram/kg/dose
PREPARATION: For doses less than 0.2mL (600 microgram) solution may be diluted. Diluent: 0.9% Sodium chloride Take 1mL and dilute to 10mL = 300 microgram / 1mL
ADMINISTRATION: Rapid IV bolus over 1 to 2 seconds
Follow with rapid sodium chloride 0.9% flush
ADVERSE EFFECTS :
Flushing, dyspnoea, irritability, transient arrhythmias, bradycardia, bronchial constriction. Contraindicated in 2nd or 3rd degree AV block or sick sinus syndrome.
COMMENTS: Monitor, and obtain ECG strip during administration.
Effect diminished by interaction with caffeine.
Refrigerate opened vial.
Discard after 24 hours.
REFERENCES: BNF for Children 2007 Pediatric Dosage Handbook 2007
DATE: June 2008

DRUG: ADRENALINE
PRESENTATION: Ampoule: 1 in 10,000, (1mg/10mL) 10mL Ampoule: 1 in 1,000, (1mg/mL) 1mL Respirator Solution : 1% 15mL
ACTION & INDICATION:
Sympathomimetic agent. For cardiac arrest, severe bradycardia, acute hypotension, bronchospasm. Low cardiac output
DOSE : Intravenous: USE 1 IN 10,000 AMPOULE ONLY 0.1 - 0.3mL/kg/dose Intravenous infusion: USE 1 in 1000 AMPOULE ONLY To be further diluted (see Preparation section) Initially 0.1microgram/kg/minute, increasing to a maximum of 1microgram/kg/min Endotracheal tube: USE 1 IN 10,000 AMPOULE ONLY 0.1 – 0.3mL/kg/dose For ease of calculation in an acute resuscitation a dose of 1mL may be given in a term infant and 0.5mL in a preterm infant. Repeated doses may be required. Nebulisation: Using Respirator Solution 0.05mL/kg/dose Using 1 in 1000 ampoule only 0.5mL/kg/dose
Dilute to 2-4mL with saline.
PREPARATION: Use solution prepared in Pharmacy if available.
To give a dose of 0.1 microgram/kg/min when infused at 1mL/hr:
Take 0.3mg of adrenaline (ie 0.3mL of 1:1000) per kilogram of baby’s weight and dilute to 50mL with glucose or glucose / saline solutions.
If a different concentration is required, refer to the Calculation of Drug Infusion table.
ADMINISTRATION: Intravenous injection Intravenous infusion Umbilical arterial/venous injection
Nebulisation
ADVERSE EFFECTS :
Tachycardia, dysrhythmias, hypertension, tremor, cold extremities, agitation.
COMMENTS: Incompatible with sodium bicarbonate If possible correct acidosis prior to adrenaline administration
REFERENCES: The Northern Neonatal Network Formulary 10th Ed
Neofax 2006 Neonatal Pharmacopoeia 2nd Ed 2005 Royal Women’s Hospital; Melbourne
DATE: June 2008

DRUG: ALBUMIN (HUMAN) 4%
PRESENTATION: Vial: 40mg/mL (4%) 50mL
ACTION & INDICATION:
Maintains plasma colloid oncotic pressure. Used as a plasma volume expander in hypovolaemia.
DOSE :
ADMINISTRATION:
Usual dose: 0.5-1g/kg (12.5-25mL/kg)
Intravenous infusion over 30- 60 minutes, or as ordered by Consultant Neonatologist.
ADVERSE EFFECTS :
Too rapid infusion: Hypertension, vascular overload causing pulmonary oedema, cardiac failure, Intraventricular haemorrhage. Allergic reactions: Chills, fever, vomiting, urticaria, anaphylaxis.
COMMENTS: Compatible with: 0.9% Sodium chloride,
5% Glucose, Glucose and saline solutions.
Albumin (human) 20% also available (see protocol). As this is a blood product, parents are to be notified before use.
REFERENCES: Gomella T. Neonatology 5th Ed
DATE: June 2008

DRUG: ALBUMIN (HUMAN) 20%
PRESENTATION: Vial: 200mg/mL (20%) 10mL, 100mL
ACTION & INDICATION:
Hypoproteinaemia.
DOSE :
ADMINISTRATION:
Usual dose: 1-2g/kg (5-10mL/kg)
Intravenous infusion over 30- 60 minutes, or as ordered by Consultant Neonatologist.
ADVERSE EFFECTS :
Too rapid infusion: Hypertension, vascular overload causing pulmonary oedema, cardiac failure. Intraventricular haemorrhage. Allergic reactions: Chills, fever, vomiting, urticaria, anaphylaxis.
COMMENTS: Compatible with: 0.9% Sodium chloride,
5% Glucose, Glucose and saline solutions.
Albumin (human) 4% also available (see protocol). As this is a blood product, parents are to be notified before use.
REFERENCES Gomella T. Neonatology 5th Ed.
DATE: June 2008

DRUG: ALPROSTADIL (PROSTAGLANDIN E1)
PRESENTATION: Ampoule: 500 microgram/mL
ACTION & INDICATION:
Promotes dilatation of all arterioles. Used to maintain patency of ductus arteriosus in neonates with congenital heart defects dependent on ductal shunting for oxygenation and perfusion until corrective surgery can be performed. (Cyanotic heart disease, duct dependant lesions)
DOSE : Initially: 0.05 microgram/kg/minute (50 nanograms/kg/min) If effective within 30 minutes reduce to 0.025 microgram/kg/minute.
Maintenance dose : May be as low as 0.01microgram/kg/minute
PREPARATION: Use solution prepared by Pharmacy if available.
Diluent: 5% Glucose, sodium chloride 0.9%
To prepare an infusion solution to deliver 0.05 microgram/kg/minute (ie 50 nanograms/kg/minute) at a rate of 1mL/hr.
Volume of diluent required (mL) = 167 Baby's weight (kg)
Add 500 micrograms alprostadil to this volume. The infusion solution may be further diluted if required .
ADMINISTRATION: For continuous intravenous/arterial infusion via syringe pump.
ADVERSE EFFECTS:
May cause apnoea in infants especially in the first hour of infusion. Consider intubation and ventilation when using on WANTS transports
Flushing, bradycardia, tachycardia, hypotension, apnoea, fever, seizures, hypothermia.
Avoid in HMD/RDS
Contraindicated in infants with PFC (persistent foetal circulation) or anomalous pulmonary venous return. Neonates receiving alprostadil for more than 120 hours, or maintained on high doses, should be closely monitored for evidence of antral hyperplasia, gastric outlet obstruction and cortical hyperostosis (eg widening fontanelles).
COMMENTS: Maximum effectiveness within 96 hours of birth No evidence of incompatibility with heparin Infusion solution stable for 24 hours
REFERENCES: BNF for Children 2007
Neofax 2006
DATE: June 2008

DRUG: AMIKACIN
PRESENTATION: Vial: 500mg/2mL
ACTION & INDICATION:
Semi-synthetic aminoglycoside for treatment of serious infection due to susceptible strains of gram negative bacilli.
DOSE :
PREPARATION:
ADMINISTRATION:
Single daily dose:
< 30 weeks 7.5 mg/kg/dose 24 hourly 30-36 weeks 10 mg/kg/dose 24 hourly Term: 1st week of life 15 mg/kg/dose 24 hourly 2nd week of life onwards 22.5mg/kg/dose 24 hourly
Use solution prepared in Pharmacy if available.
Diluent: Water for Injections, Glucose 5%, sodium chloride 0.9%
Draw up contents of vial, make up to 50mL = 500mg in 50mL
= 10mg/mL
Intramuscular Intravenous: Infuse over 20 to 30 minutes
ADVERSE EFFECTS :
Hearing loss, reduced renal function, renal failure, vertigo, anaemia, arthralgia.
Toxicity may be enhanced by concurrent administration of diuretic.
COMMENTS: Discard vial after use
DRUG LEVELS: Trough: < 5mg/L
Sample immediately prior to 4th dose and every 3 to 5 days thereafter
Peak: Not required
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: AMOXYCILLIN
PRESENTATION: Vial: 500mg
Oral Suspension: 250mg/5mL 100mg/mL (KEMH only)
ACTION & INDICATION :
Broad spectrum penicillin antibiotic.
For treatment of sensitive organisms including Listeria monocytogenes and group B Streptococci
DOSE :
PREPARATION:
ADMINISTRATION:
< 34 weeks < 7 days 50mg/kg/dose 12 hourly ≥ 34 weeks < 7 days 50mg/kg/dose 8 hourly
All infants ≥ 7 days 50mg/kg/dose 6-8 hourly
Diluent: Water for Injections
Intravenous: Add 4.6mL Water for Injections to 500mg vial = 100mg/mL Intramuscular: Add 1.6mL diluent to vial = 250mg/mL
Oral 250mg/5mL: Add 80mL of Water for Irrigation to the powder for suspension in the bottle.
Oral 100mg/mL: Add 13mL of Water for Irrigation to the powder for suspension in the bottle
Intravenous: Infuse over 3-5 minutes.
Intramuscular: Site as per NCCU policy
Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Vomiting, diarrhoea Urticaria Anaemia Phlebitis Thrombocytopenia purpura
COMMENTS: Discard reconstituted vial immediately after use.
Store reconstituted oral suspension in refrigerator. Discard after 14 days.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: AMOXYCILLIN & CLAVULANIC ACID (AUGMENTIN DUO 400 / CLAMOXYL DUO 400)
PRESENTATION: Oral Suspension: 400mg/5mL (as amoxycillin)
ACTION & INDICATION :
Broad spectrum penicillin antibiotic in combination with a β-lactamase inhibitor.
For treatment of bacterial infections caused by sensitive organisms.
DOSE: 22.5mg/kg/dose 12 hourly
(The dose is calculated with regard to the amoxycillin content)
PREPARATION: Oral 400mg/5mL: Add 55mL of Water for Irrigation to the powder for suspension in the bottle.
ADMINISTRATION: Oral: Should be given immediately prior to feeds.
ADVERSE EFFECTS:
Vomiting, diarrhoea Urticaria Anaemia Phlebitis Cholestatic jaundice Thrombocytopenia purpura
COMMENTS: Store reconstituted oral suspension in refrigerator. Discard after 7 days.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG:
AMPHOTERICIN LIPOSOMAL (AMBISOME)
PRESENTATION:
Do not confuse with amphotericin infusion (Fungizone) Infusion solution from Pharmacy Vial: 50mg
ACTION & INDICATION:
Antifungal agent used to treat systemic fungal infections
DOSE: Initially 1mg/kg/day up to 5mg/kg/day Doses up to 10mg/kg/day may be used with Specialist consultation
PREPARATION:
Use solution supplied by Pharmacy OR To dilute vial: Add 12mL water for injection to vial =4mg/mL Shake for 15 seconds. Take 5mL and dilute up to 10mL with Glucose 5%. Filter through 5micron filter supplied before dilution. =2mg/mL
ADMINISTRATION: Intravenous solution: Infuse over 30-60 minutes If line requires flushing use glucose solutions only Do not use solutions containing sodium chloride
ADVERSE EFFECTS:
Nephrotoxicity- monitor renal function Fever, rigors, Nausea, vomiting Hypokalaemia, Rash
COMMENTS: Refrigerate infusion solution, discard after 24 hours Refrigerate reconstituted vial. Discard after 72 hours Protect from light
REFERENCES: Paediatric Pharmacopoeia 13th Ed. Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: AMPHOTERICIN (FUNGIZONE)
PRESENTATION: Do not confuse with liposomal amphotericin Infusion solution from Pharmacy Vial: 50mg
ACTION & INDICATION:
Antifungal agent used to treat systemic fungal infections.
DOSE : 0.5-1mg/kg/dose 24 hourly
PREPARATION: Use solution supplied by pharmacy OR Use kit in fridge if needed after Pharmacy hours. To dilute vial: 1.Add 10mL water for injection = 5mg/mL 2.Prepare buffered glucose solution. Add 0.6mL from potassium dihydrogen phosphate and dipotassium hydrogen phosphate concentrated injection to Glucose 5% 100mL bag. 3.Withdraw 10mL from glucose bag and discard . 4.Add 2mL from diluted amphotericin vial to bag = 1mg /10 mL Solution can be heparinised (0.5 units/mL). If line requires flushing use glucose solutions only. Do not use solutions containing Sodium chloride.
ADMINISTRATION: Intravenous infusion: Infuse over 6 hours.
ADVERSE EFFECTS:
Nephrotoxicity – monitor renal function Mild anaemia Hypokalaemia Ensure baby is well hydrated Chills, fever Vomiting, diarrhoea
COMMENTS:
Do not filter Protect from light
Refrigerate infusion solution, discard after 24 hours
REFERENCES: Paediatric Pharmacopoeia 13th Ed. Royal Children’s Hospital Melbourne BNF for Children 2007
DATE: June 2008

DRUG: ATROPINE SULPHATE
PRESENTATION: Ampoule: 400 microgram/mL
ACTION & INDICATION:
Anticholinergic agent used for:
• Pre-anaesthetic medication to inhibit excessive salivary and bronchial secretions and to diminish the risk of vagal inhibition of the heart.
• Sinus bradycardia, AV block.
DOSE : Premedication IM: 10 - 20 microgram/kg/dose IV: 10 - 30 microgram/kg/dose Oral: 40 microgram/kg/dose two hours before induction. Bradycardia IV or IM: 10 – 30 microgram/kg/dose
ADMINISTRATION: Intramuscular: Site as per NCCU policy
Intravenous : Over 1 minute
Dose may be repeated every 10 - 15 minutes to achieve desired effect. Maximum total dose 40 microgram/kg Oral
ADVERSE EFFECTS:
Arrhythmias, tachycardia
Hyperthermia
Urinary retention
Do not give to febrile infant - risk of provoking hyperthermia.
COMMENTS: Reserve use of atropine for patients unresponsive to improved oxygenation and adrenaline
REFERENCES: BNF for Children 2007 Pediatric Dosage Handbook 14th Ed Neofax 2006
DATE: June 2008

DRUG: BCG (BACILLUS CALMETTE-GUÉRIN) VACCINE
PRESENTATION: Multidose vial plus diluent.
ACTION & INDICATION:
Suspension of living organisms of an attenuated strain of Mycobacterium bovis (Bacillus Calmette-Guérin). For immunisation against tuberculosis.
DOSE : For infants under 6 months; 0.05mL
PREPARATION: Reconstitute powder in vial with 1.5mL of accompanying phosphate buffered saline diluent.
ADMINISTRATION: INTRADERMAL INJECTION : Administer above the insertion of the deltoid muscle of the right arm
To be given by appropriately trained and certified health care providers only. Infants may be referred to the Perth Chest Clinic for vaccination if trained staff are not available.
Avoid inhalation of dried vaccine. If alcohol is used to swab skin, or the rubber bung of vial, it must be allowed to evaporate before proceeding.
COMMENTS: Refrigerate reconstituted solution.
Discard 8 hours after reconstitution.
Discard contents into "sharps" container after use
REFERENCES: NH&MRC The Australian Immunisation Handbook 8th Ed
DATE: June 2008

DRUG: BENZYLPENICILLIN (PENICILLIN-G)
PRESENTATION: Vial: 600mg
ACTION & INDICATION:
Antibiotic for treatment of susceptible organisms including Group B Streptococci, non-β lactamase – producing Staphyloccocci and congenital syphilis.
DOSE : < 7 days 50 mg/kg/dose 12 hourly
≥ 7 days 50mg/kg/dose 8 hourly
For GBS septicaemia, meningitis
< 7 days 50mg/kg/dose 12 hourly
≥ 7 days 50mg/kg/dose 6 hourly
Congenital syphilis:
50mg/kg/dose 12 hourly Asymptomatic and normal CSF - 10 days therapy. Symptomatic - 14 days therapy.
PREPARATION: Diluent: Water for Injections
Intravenous : Add 5.6mL diluent to vial = 100mg/mL
Intramuscular : Add 1.6mL diluent to vial
= 300mg/mL
ADMINISTRATION: Intramuscular
Intravenous : Infuse over 3-5 minutes
ADVERSE EFFECTS:
Hypersensitivity, rash Diarrhoea Seizures with high doses Haemolytic anaemia
COMMENTS: Refrigerate reconstituted solution. Discard after 24 hours.
REFERENCES: BNF for Children 2007 Neofax 2006 Dr T Keil KEMH Microbiology
DATE: June 2008

DRUG: CAFFEINE
PRESENTATION: Oral solution:10 mg/mL (caffeine base) Ampoule: 50 mg/5 mL(caffeine base)
ACTION & INDICATION:
Stimulates central inspiratory drive and increases sensitivity of the medullary centre to CO2. Used for prevention or treatment of apnoea of prematurity or apnoeas associated with respiratory infection or anaesthesia. To aid extubation of ventilated babies.
DOSE : Loading dose: 20 mg/kg
Maintenance dose: 5 mg/kg/day commencing at least 24 hours after loading dose.
PREPARATION: Diluent: 0.9% Sodium chloride, Water for Injections
Loading dose: does not require dilution
If maintenance dose requires dilution: Dilute 50 mg/5 mL ampoule with 5mL of diluent
= 50 mg/ 10 mL
ADMINISTRATION: For intravenous, umbilical arterial / venous infusion. Infuse over 30 minutes.
Oral: Give dose with feeds.
ADVERSE EFFECTS :
Nausea, vomiting, gastric irritation Agitation Tachycardia Diuresis Overdose – arrhythmias, seizures.
DRUG MONITORING:
Sampling time: Midway between doses Therapeutic: 5 - 30 mg/L Toxic: > 50 mg/L
Drug levels
All infants: First level to be taken one week after commencing drug, then weekly only if baby symptomatic.
If Infant < 30 weeks at commencement: Check level after four weeks, or prior to late extubation.
REFERENCES: BNF for Children 2007
Neofax 2006 Acta Paediatr Scand 1989;78:786-788 (for dosing)
DATE: June 2008

DRUG: CALCITRIOL
PRESENTATION: Oral Solution : 0.05 microgram/mL (prepared in pharmacy) Oral Solution : 1 microgram/mL (SAS authority required)
ACTION & INDICATION:
Calcitriol is 1,25-dihydrocholecalciferol, an activated form of Vitamin D3. This active hormone increases calcium and phosphorus absorption and with parathyroid hormone, increases bone resorption, maintaining calcium and phosphorous at blood levels which permit mineralisation of bone matrix.
Used to treat hypocalcaemia, hypoparathyroidism, neonatal rickets.
DOSE : Starting dose: 0.02-0.25 microgram/dose/day
Dose to be individualised depending on indication, and response.
ADMINISTRATION: Oral: If dose is ≥ 0.05 microgram, use 1 microgram/mL strength oral solution.
ADVERSE EFFECTS & COMMENTS:
Protect solution from light.
Monitor: Serum alkaline phosphatase, calcium, phosphorus, creatinine
REFERENCES: BNF for Children 2007 Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: CALCIUM CARBONATE
PRESENTATION: Oral Suspension : Calcium Carbonate
Contains: 40mg (1 mmol) Calcium per mL
ACTION & INDICATION:
Hypocalcemia
Calcium supplement for infants not receiving premature formula / fortified breast milk.
DOSE : Calcium Supplement:
Infants BW < 1.2 kg
Start on day 10, when on full feeds and continue until the baby’s weight is at least 2kg.
Dose: 1mL/kg/dose 8hrly (120mg/kg/day or 3mmol/kg/day).
ADMINISTRATION: Oral
ADVERSE EFFECTS
Flatulence, constipation Gastric hypersecretion, acid rebound with prolonged use
COMMENTS: Given in conjunction with Sodium Phosphate mixture
DO NOT MIX WITH SODIUM PHOSPHATE MIXTURE
Monitor serum calcium concentrations.
Use with caution in neonates who are currently receiving frusemide.
IF INTRAVENOUS CALCIUM THERAPY IS REQUIRED, REFER TO CALCIUM GLUCONATE PROFILE.
REFERENCES: Neofax 2006
DATE: June 2008

DRUG: CALCIUM GLUCONATE
PRESENTATION: Ampoule: 1g in 10mL, (10%).
(contains 0.22mmol Calcium per mL)
ACTION & INDICATION:
Intravenous electrolyte for the treatment of hypocalcaemia. Ionized calcium less than 0.65mmol/l (<0.75mmol/l if symptomatic) Hyperkalaemia
DOSE: Usual dose: 500mg (5mL of 10% ampoule solution) /kg/24 hours Maximum dose: 800mg/kg/24hours In hypocalcaemia seizures: Withdraw 2mL/kg of 10% solution and dilute with an equal amount of compatible fluid. Slow infusion over 10 minutes with ECG monitoring. Stop infusion if bradycardia occurs.
PREPARATION: For continuous infusion:
Withdraw 5mL/kg of 10% calcium gluconate. Dilute to 25mL with appropriate diluent. Compatible fluids: 5% and 10% Glucose, sodium chloride 0.9%, 7.5% glucose in sodium chloride 0.18%
ADMINISTRATION: For intravenous use only Infuse at 1mL/hour Give via a central line, if available. If giving through UVC make sure the tip of the UVC is not in the heart or the liver.
ADVERSE EFFECTS :
Extravasation causes tissue necrosis. Rapid infusion may cause bradycardia, hypotension, and peripheral vasodilation.
COMMENTS: Monitor serum calcium and ionized calcium concentrations. Monitor ECG when bolus doses are given.
DO NOT MIX WITH SODIUM BICARBONATE
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Pediatric Dosage Handbook 14th Ed
DATE: June 2008

DRUG: CAPTOPRIL
PRESENTATION: Oral solution: 5mg/mL
Oral solution: 1mg/mL(Prepared in Pharmacy).
ACTION & INDICATION :
Angiotensin converting enzyme inhibitor.
Antihypertensive, may also be of benefit in the management of heart failure.
DOSE : Initial dose 10 -50 microgram / kg / dose 8 hourly Titrate dose according to response to a maximum dose of 500 microgram /kg /dose 8 hourly.
ADMINISTRATION: Oral Extremely unpalatable - mix well with part of a feed if given orally (this is not necessary if being fed by intragastric tube).
ADVERSE EFFECTS & COMMENTS:
Discard oral solution 28 days after opening bottle
Use with caution
Hypotension – monitor blood pressure pre-dose, then at ½, 1, 2, 3 and 5 hours after the first and second doses, and after any change in therapy. Thereafter 8 hourly.
Rash, fever.
Gastrointestinal disturbances.
Monitor urea and electrolytes.
Hyperkalaemia – with potassium supplements or potassium sparing diuretics.
Contraindicated in bilateral renal artery stenosis.
Cough.
REFERENCES: Paediatric Pharmacopoeia 13th Ed. Royal Children’s Hospital Melbourne Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: CARBAMAZEPINE
PRESENTATION: Oral Liquid: 20mg/mL
ACTION & INDICATION:
An anticonvulsant to treat a range of neonatal seizures.
DOSE : 2mg/kg/dose every 8 hours, increasing over two weeks to 5mg/kg/dose every 8 hours
Increase dose slowly to allow for enzyme induction on initiation of therapy.
ADMINISTRATION: Oral
ADVERSE EFFECTS :
May cause: Blood dyscrasias Cardiovascular, renal, hepatic disturbances Drowsiness
COMMENTS: Drug interactions include: Phenytoin - may alter level of both drugs Erythromycin – increases level of carbamazepine
DRUG LEVELS: Sampling time: Just before next dose
Therapeutic range: 5-10mg/L
Time to reach steady rate: 2-4 weeks
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital, Melbourne
DATE: June 2008

DRUG: CEFOTAXIME
PRESENTATION: Vial: 1g
ACTION & INDICATION:
Third generation cephalosporin. For the treatment of susceptible gram negative organisms except Pseudomonas species.
DOSE : < 34 weeks < 7 days 50mg/kg/dose 12 hourly < 34 weeks ≥ 7 days 50mg/kg/dose 8 hourly
≥ 34 weeks < 7 days 50mg/kg/dose 8 hourly ≥ 34 weeks ≥ 7 days 50mg/kg/dose 6 hourly
PREPARATION: Use solution prepared by Pharmacy if available
Diluent: Water for Injections
Intravenous: Add 9.6 mL diluent to 1 g vial = 100mg/mL
Intramuscular: Add 3.6 mL diluent to 1 g vial = 250mg/mL
ADMINISTRATION: Intramuscular: As per NCCU policy.
Intravenous : Infuse over 3 - 5 minutes
ADVERSE EFFECTS:
COMMENTS:
Hypersensitivity, skin rashes.
When used with other nephrotoxic drugs, it may increase the probability of renal toxicity.
May give a false positive Clinitest result.
Phlebitis
Diarrhoea, leukopenia, granulocytopenia, eosinophilia
Refrigerate reconstituted solution
Discard after 24 hours
REFERENCES: Paediatric Pharmacopoeia 13th Royal Children’s Hospital, Melbourne BNF for Children 2007
DATE: June 2008

DRUG: CEFTAZIDIME
PRESENTATION: Vial: 1g
ACTION & INDICATION:
Third generation cephalosporin antibiotic. Used to treat infections caused by susceptible organisms with suspected resistance to other antimicrobials. Treatment of pseudomonas organisms resistant to, or as an alternative to, aminoglycosides.
DOSE : < 7 days 25-30mg/kg/dose 12 hourly ≥ 7 days 30mg/kg/dose 8 hourly
Severe infection: < 7 days 50mg/kg/dose 12 hourly ≥ 7 days 50mg/kg/dose 8 hourly
PREPARATION : Use solution prepared in Pharmacy if available Diluent: Water for Injections Intravenous: Add 8.9mL diluent to vial = 100mg/mL Intramuscular: Add 1.9mL Water for Injections or 1% lignocaine to a vial = 333mg/mL
ADMINISTRATION: Intramuscular: As per NCCU policy. Intravenous: over 3-5 minutes.
ADVERSE EFFECTS :
Hypersensitivity, rash Renally excreted – reduce dose in renal impairment Colitis – colonisation with C. difficile. Phlebitis Angioedema Anaphylaxis Diarrhoea Positive Coomb's test (approx. 5% patients), which may interfere with blood cross matching.
COMMENTS: NB: CO2 bubbles, which develop in solution, must be expelled from syringe. Refrigerate reconstituted solution. Discard after 24 hours.
REFERENCES: Neofax 2006 Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne BNF for Children 2007
DATE: June 2008

DRUG: CEFTRIAXONE
PRESENTATION: Vial: 1g
ACTION & INDICATION:
Third generation cephalosporin. Used to treat infections caused by susceptible organisms. Active against both gram negative and gram positive organisms with the exception of Pseudomonas species, enterococci.
DOSE: 50mg/kg/dose 24 hourly Meningitis : 50mg/kg/dose 12 hourly
PREPARATION: Use solution prepared in Pharmacy if available. Intravenous: Diluent: Water for Injections Add 9.3mL diluent to 1g vial = 100mg/mL Intramuscular: Diluent: Lignocaine 1% injection Add 3.2 mL or 1.8mL =250mg/mL = 385mg/mL
ADMINISTRATION: Intramuscular: As per NCCU policy Intravenous: Infuse over 30 minutes via syringe pump, or slow IV push.
ADVERSE EFFECTS :
Do not use with calcium containing solutions as precipitate may form. Displaces bilirubin from serum albumin. Use with caution, therefore, in neonates with hyperbilirubinaemia. Diarrhoea, eosinophilia, neutropenia Rash Colitis IM : very painful, avoid if possible.
COMMENTS : Refrigerate reconstituted solution.
Discard after 24 hours.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: CEPHALEXIN
PRESENTATION: Oral suspension: 250mg/5mL
ACTION & INDICATION:
First generation cephalosporin antibiotic.
For the treatment of susceptible organisms.
DOSE : <7 days 25mg/kg/dose 12 hourly 7days-21 days 25mg/kg/dose 8 hourly >21 days 25mg/kg/dose 6 hourly
PREPARATION: Oral suspension 250mg/5mL: Add 60mL of Water for Irrigation to the powder in the bottle.
ADMINISTRATION: Oral
ADVERSE EFFECTS:
GI disturbances – nausea, vomiting, diarrhoea. Hypersensitivity.
COMMENTS : Store reconstituted oral suspension in the refrigerator. Discard after 14 days
REFERENCES: BNF for Children 2007
DATE: June 2008

DRUG:
CEPHALOTHIN
PRESENTATION:
Vial : 1g
ACTION & INDICATION:
First generation cephalosporin antibiotic. Has a higher activity against Gram positive than Gram negative organisms.
DOSE:
Week 1 of life : 20 mg/kg/dose 12 hourly Week 2 of life : 20 mg/kg/dose 8 hourly (and thereafter)
PREPARATION:
Use solution prepared by Pharmacy if available. IV: Diluent : Water for Injections Add 9.5mL to 1g vial = 100mg/mL IM: Add 4.6mL to 1g vial = 200mg/1mL
ADMINISTRATION:
Intravenous : infuse over 3-5 minutes Intramuscular: As per NCCU policy.
ADVERSE EFFECTS:
Hypersensitivity – rash, urticaria, anaphylaxis Neutropenia, thrombocytopenia, haemolytic anaemia Positive direct Coomb’s test. Rise in AST, alkaline phosphatase – monitor liver function Rise in BUN. Decreased creatinine clearance.
COMMENTS:
Refrigerate reconstituted vial. Discard after 24 hours.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE:
June 2008

DRUG: CEPHAZOLIN
PRESENTATION: Vial : 1g
ACTION & INDICATION:
Cephazolin is a first generation cephalosporin antibiotic.
DOSE: IV, IM: ≤ 7 days 20mg/kg 12 hourly > 7days ≤ 2000g 20mg/kg 12 hourly > 2000g 20mg/kg 8 hourly
PREPARATION: Use solution prepared in Pharmacy if available. Intravenous: Reconstitute each 1g vial with 9.5mL of Water for Injections = 100mg/mL May be diluted further to a suitable volume if administering as an IV infusion. Intramuscular: Reconstitute each 1g vial with 2.5mL of Water for Injections = 330mg/mL
ADMINISTRATION: IV: Give over 3 to 5 minutes. May also be given by IV infusion over 10 to 15 minutes. IM
ADVERSE EFFECTS:
Rash (Stevens-Johnson syndrome has been rarely reported), pruritis, neutropenia, thrombocytopenia, transient elevations in liver enzymes, nausea, vomiting, diarrhoea.
Hypoprothrombinaemia has been associated with cephazolin use. This may affect bleeding and clotting times.
COMMENTS: Refrigerate reconstituted solution.
Discard after 24 hours.
REFERENCES: RCH Paediatric Pharmacopoeia, 13th ed
Pediatric Dosage Handbook, 14th ed
DATE: June 2008

DRUG: CHLORAL HYDRATE
PRESENTATION: Oral solution : 100mg/ mL
ACTION & INDICATION :
CNS depressant. In hypnotic use, produces quiet, deep sleep.
Higher doses lead to general anaesthesia and concurrent depression of respiratory and vasomotor centres.
Used as a sedative and hypnotic.
DOSE :
Sedative: 8 mg/kg/dose 6 - 8 hourly
Hypnotic: 25 - 50 mg/kg/dose
ADMINISTRATION: Oral
ADVERSE EFFECTS :
Gastric irritation - dilute dose well with milk or water.
Skin rashes, peripheral vasodilation, hypotension, myocardial depression.
Upper airway obstruction secondary to decreased pharyngeal tone.
COMMENTS: Rapidly absorbed, acting within 30 minutes.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: CHLORAMPHENICOL OPHTHALMIC PREPARATIONS
PRESENTATION: Ophthalmic solution 0.5% 10mL
Each mL contains Chloramphenicol 5mg Hypromellose 3mg Ophthalmic ointment 1%
ACTION & INDICATION:
Antibiotic eye drops / ointment. Used to treat susceptible infections of the eyes.
DOSE: Ophthalmic drops:
One drop every two to six hourly for 2 to 3 days after clinical symptoms have resolved, and then decrease to 3 to 4 times a day. Ophthalmic ointment: Apply 0.5 to 1cm up to 3 hourly, or at night when drops used during the day. Eye toilet / care should be performed prior to administration of each dose.
ADVERSE EFFECTS/ COMMENTS:
Blood dyscrasias with prolonged therapy.
Overgrowth of new susceptible organisms with prolonged use. Discard 30 days after opening
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: CIPROFLOXACIN
PRESENTATION: Oral suspension: 50 mg/mL Injection: 200mg/100mL
ACTION & INDICATION:
Quinolone antimicrobial agent. Broad spectrum antibiotic, more active against Gram negative organisms including Pseudomonas aeruginosa.
DOSE: 7.5 mg/kg/dose 12 hourly
ADMINISTRATION:
ADVERSE EFFECTS:
COMMENTS:
Oral: IV: Infuse over 30 to 60 minutes Fever, nausea, rash, vomiting, diarrhoea Seizures
Injection solution may be used undiluted Well absorbed orally. Do not use unless there is no suitable alternative, as it may cause joint and cartilage arthropathy. Reduce dose in impaired renal function. Ensure adequate hydration prior to and during therapy to avoid crystalluria May increase caffeine levels
REFERENCES: BNF for Children 2007 Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: CLINDAMYCIN
PRESENTATION: Ampoule: 600mg/4mL
ACTION & INDICATION:
Antimicrobial agent which inhibits bacterial protein synthesis.
Effective against sensitive organisms including Mycoplasma hominis.
DOSE:
All pre-term and <7 days 5 mg to 7.5 mg/kg/dose every 12 hours ≤ 29weeks, >28days 5 - 7.5mg/kg/dose 8 hourly
30-36weeks >14 days 5 - 7.5mg/kg/dose 8 hourly
37-44 weeks > 7 days 5 - 7.5mg/kg/dose 8 hourly
PREPARATION:
Use solution prepared in Pharmacy if available.
OR
Withdraw 150mg (1mL) and dilute to 30mL = 150mg/30mL, that is, = 5mg/mL.
May be further diluted if required.
Diluent: 0.9% Sodium chloride and glucose solutions.
ADMINISTRATION: Intravenous infusion over 30 minutes.
ADVERSE EFFECTS:
Nausea, vomiting, abdominal cramps, diarrhoea
Pseudomembranous colitis
Hypersensitivity reactions, rash
Arrhythmias if administered too quickly
COMMENTS: Ampoule contains benzyl alcohol 9mg/mL
REFERENCES: Neofax 2006
DATE: June 2008

DRUG: CLONAZEPAM
PRESENTATION: Oral: Drops 2.5mg/mL (1 drop = 100 microgram) Ampoule: 1mg/mL
ACTION & INDICATION:
Benzodiazepine anticonvulsant for status epilepticus and all forms of epilepsy.
DOSE: Initial dose: 100-250 microgram (NOT per kg) Repeat if necessary in one hour Maintenance dose: 10 microgram/kg/dose every 8 hours. Maintenance dose may be increased every third day to a maximum of 200microgram/kg/day
Infusion Dose: 10 micrograms /kg/hour, adjusted according to response to a maximum dose of 60 micrograms/kg/hour.
PREPARATION: Intravenous: Do not use diluent supplied by manufacturer. Dilute ampoule to 10mL with Water for Injections = 1000 microgram/10mL = 100 microgram/mL
Infusion: Dilute 0.5mL (500micrograms) to 50mL with Glucose/Saline solutions =10 microgram/mL
Oral: Doses less than 100 microgram must be diluted as follows: Take 0.1mL of oral drops and dilute to 1mL = 250 microgram/mL = 25 microgram/0.1mL of diluted solution
ADMINISTRATION:
Continuous infusion via syringe pump
Intravenous: over 5 minutes
Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Clonazepam has a long half life and repeated dosing leads to accumulation. CNS and respiratory depression. Behavioural changes – irritability. Salivary and bronchial hypersecretion. May be absorbed onto infusion equipment
COMMENTS: Discard intravenous preparations after 12 hours.
DRUG LEVELS: Sampling time : midway between doses Therapeutic range 20-70 microgram/L (60 to 150nanomol/L) Time to reach steady state – 1 week.
REFERENCES: Neonatal Pharmacopoeia 2nd Ed. Royal Women’s Hospital Melbourne
BNF for Children 2007
DATE: June 2008

DRUG: CO-TRIMOXAZOLE (Trimethoprim/Sulphamethoxazole)
PRESENTATION: Ampoule: Trimethoprim 80mg - Sulphamethoxazole 400mg per 5mL
Oral Suspension: Trimethoprim 40mg - Sulphamethoxazole 200mg per 5mL
ACTION & INDICATION:
Antimicrobial agent for susceptible gram positive and gram negative organisms May be used to treat urinary tract infections and for prophylaxis of urinary tract infections in infants once urine is sterile.
DOSE:
IV: Trimethoprim 3mg/kg /dose –
Sulphamethoxazole 15 mg/kg/dose 12 hourly (Equivalent to 0.19mL/kg/dose 12 hourly) Oral: Treatment: 0.3 - 0.5 mL/kg/dose 12 hourly equivalent to : Trimethoprin 2.4 – 4mg/kg/dose - Sulphamethoxazole 12 - 20mg/kg/dose 12 hourly Prophylaxis: 0.25mL/kg/dose at night
PREPARATION: DUE TO ITS POTENTIAL INSTABILITY, THIS CAN NOT BE PREPARED IN PHARMACY IV: Diluent : Glucose 5% Withdraw required volume from ampoule. Dilute in the ratio of 1mL (drug) to 25mL (with diluent).
ADMINISTRATION: Intravenous infusion over 60 minutes.
Oral: May be given with or after feeds.
ADVERSE EFFECTS:
Neutropenia Photosensitivity G.I. upset with oral doses.
COMMENTS: Not usually recommended in infants under 4 weeks of age. Should not be used in jaundiced infants. Avoid in G6PD deficiency.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne BNF for Children 2007
DATE: June 2008

DRUG: DEXAMETHASONE PHOSPHATE
PRESENTATION: Oral Solution : 1 mg/mL (1000 microgram/mL)
Ampoule: 4 mg/mL (4000 microgram/mL)
ACTION & INDICATION:
Synthetic glucocorticoid which acts as an anti-inflammatory or immunosuppressive agent. Used in neonates for respiratory insufficiency and oedema with acute non-infectious laryngospasm.
DOSE :
Days 1 - 3: 75 microgram/kg/dose 12 hourly
Days 4 – 6: 50 microgram/kg/dose 12 hourly Days 7 – 8: 25 microgram/kg/dose 12 hourly Days 9 – 10: 10 microgram/kg/dose 12 hourly Duration of Course: As advised by Consultant Neonatologist
PREPARATION: Diluent: Water for Injections Draw up 0.5 mL (2 mg) of drug and dilute to 20mL with Water for Injections = 100microgram /mL
ADMINISTRATION:
Oral: Given with or immediately after feeds.
Intravenous: over 3 - 5 minutes
ADVERSE EFFECTS:
Sepsis, hyperglycaemia, hypertension, adrenal suppression, behavioural disturbances, acute adrenal insufficiency in abrupt withdrawal.
G.I. bleeding.
Increases urinary calcium excretion.
Osteoporosis, growth restriction Increases risk of cerebral palsy
REFERENCES: DART Regimen Paediatric Research 56(3):477 September 2004
DATE: June 2008

DRUG: DIAZEPAM
PRESENTATION: Ampoule: 10mg/2mL
ACTION & INDICATION:
Benzodiazepine. Used as anticonvulsant to treat seizures (NOT DRUG OF FIRST CHOICE - see Phenobarbitone).
DOSE:
100 – 300microgram /kg /dose
Repeat dose every 15-30 minutes when necessary.
ADMINISTRATION: Intravenous: over 3 - 5 minutes.
DO NOT DILUTE
INTRAMUSCULAR ADMINISTRATION IS NOT RECOMMENDED.
ADVERSE EFFECTS:
Respiratory depression, hypotension.
CNS depression, phlebitis.
Contraindicated in jaundiced infants
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne BNF for Children 2007
DATE: June 2008

DRUG: DIAZOXIDE
PRESENTATION: Oral mixture: 10mg/mL (prepared in pharmacy).
ACTION & INDICATION:
Increases blood glucose concentration by inhibiting pancreatic insulin secretion. It may increase the hepatic output of glucose.
For
(i) profound or prolonged hypoglycaemia unresponsive to other forms of therapy, or
(ii) idiopathic hypoglycaemia of infancy.
DOSE: Initial dose: 5 mg / kg / dose twice daily
Adjust dose according to response
Maximum dose: 15 mg / kg / day.
ADMINISTRATION: Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Hypotension – monitor BP pre-dose and 30 minutes post dose, continue until stabilised for 48 hours then twice daily.
Hyperbilirubinaemia
Thrombocytopenia
Hyperglycaemia
Dysrhythmias
Commonly causes fluid retention
COMMENTS: Use cautiously in patients with impaired cardiac or cerebral circulation. Use of the mixture is restricted to patient’s for whom SAS approval has been obtained (contact the ward pharmacist).
REFERENCES: BNF for Children 2007
DATE: June 2008

DRUG: DIGOXIN
PRESENTATION: Ampoule: 50 microgram / 2mL
Paediatric elixir: 50 microgram / mL
ACTION & INDICATION:
Increases myocardial contractility and cardiac output. Slows AV conduction Congestive heart failure, atrial fibrillation, supraventricular tachycardia.
DOSE: Oral/Intravenous Loading dose: < 34 weeks 15-25 microgram/kg ≥ 34 weeks 30-40 microgram/kg Give ½ total loading dose initially, then ¼ total loading dose in 8 hours then last ¼ loading dose in 8 hours.
Maintenance: 4 – 5 microgram/kg/dose 12 hourly
Oral bioavailability is 80% of intravenous. Use lower dose in range for intravenous use.
PREPARATION:
Use undiluted if possible. If dilution required, contents of ampoule must be diluted at least fourfold.
Diluent: Water for Injections, 0.9% Sodium chloride, Glucose and Saline Solution.
Dilute contents of ampoule to 10mL = 50 microgram / 10mL
ADMINISTRATION: Administer over 5 minutes
ADVERSE EFFECTS:
Bradycardia, dysrhythmias Vomiting, diarrhoea Factors influencing toxicity: Hypoxia, acid base imbalance, hypocalcaemia, hypokalaemia, hypomagnesaemia.
DRUG MONITORING:
Sampling time: 6 hours post dose. Therapeutic range: 0.5 - 2.2 microgram/L 0.6 - 2.8 mmol/L Time to reach steady state: 1 week
REFERENCES: Pediatric Dosage Handbook 14th Ed Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital
DATE: June 2008

DRUG: DILACAINE EYE DROPS – PMH FORMULATION
PRESENTATION: Eyedrops 3mL. Each mL contains:
Proxymetacaine HCl 1.25mg
Cyclopentolate HCl 2.5mg
Tropicamide 2.5mg
Phenylephrine HCl 25mg
ACTION & INDICATION:
Mydriatic, anaesthetic eyedrop.
Examination of the fundus of the eye.
DOSE : 1 drop in each eye one hour prior to examination.
Instil another drop of Dilacaine in each pupil thirty minutes prior to the examination.
ADMINISTRATION: Use according to Doctor's instructions. See above.
ADVERSE EFFECTS:
Increased intraocular pressure.
May cause vasoconstriction of facial skin.
COMMENTS: Princess Margaret Hospital formulation
Refrigerate.
Discard bottle after use.
For individual patient use discard one month after opening.
DATE: June 2008

DRUG: COMBINED DIPTHERIA-TETANUS-ACELLULAR PERTUSSIS (DTPa), HEPATITIS B AND INACTIVATED POLIO VACCINE (INFANRIX PENTA)
PRESENTATION: Prefilled syringe
ACTION & INDICATION:
For Indigenous Children only
The vaccine is indicated for immunisation of infants from the age of 6 weeks against diptheria, tetanus, pertussis, hepatitis B and poliomyelitis. Use as a booster dose at 18 months of age if boosting with hepatitis B and poliomyelitis, as well as diptheria, tetanus, and pertussis is required.
DOSE: 0.5mL
1st dose 2 months 2nd dose 3-4 months 3rd dose 5-6 months Booster 6-12 months after primary course or at 18 months of age (only if required) Haemophilus b Conjugate Vaccine (PedvaxHIB) must also be administered in this dosing schedule
PREPARATION: Ready to use sterile suspension
ADMINISTRATION: Intramuscular: As per NCCU policy
ADVERSE EFFECTS & COMMENTS:
Redness, swelling A nodule may be palpable at site for a few weeks. Fever, malaise, irritability Persistent screaming, vomiting, shock, collapse
Infanrix penta should not be administered to subjects with known hypersensitivity to components of the vaccine.
Infanrix penta is contraindicated if the child has experienced encephalopathy of unknown aetiology, occurring within 7 days following previous vaccination with pertussis containing vaccine. In these circumstances pertussis vaccination should be discontinued and vaccination continued with diptheria-tetanus, hepatitis B, inactivated polio and Hib vaccines.
REFERENCES: West Australian Vaccination Schedule July 2007
The Australian Immunisation Handbook 9th Ed NHMRC
DATE: June 2008

DRUG: COMBINED DIPTHERIA-TETANUS-ACELLULAR PERTUSSIS (DTPa), HEPATITIS B, POLIOVIRUS AND HAEMOPHILUS INFLUENZAE TYPE B VACCINE (INFANRIX HEXA)
PRESENTATION: Prefilled syringe, plus a white pellet in a glass vial
ACTION & INDICATION:
For Non-Indigenous Children
The vaccine is indicated for primary immunisation of infants from the age of 6 weeks against diptheria, tetanus, pertussis, hepatitis b, poliomyelitis, and Haemophilius influenzae type b. It is also indicated for use as a booster dose at 18months of age if boosting with hepatitis B, poliomyelitis, and Haemophilius influenzae type b, as well as diptheria, tetanus and pertussis is required.
DOSE: 0.5mL 1st dose 2 months 2nd dose 3-4 months 3rd dose 5-6 months Booster 6-12 months after primary course or at 18 months of age ( only if required)
PREPARATION: Inspect the contents of the syringe and the pellet for discolouration. If discoloured, discard.
Shake the suspension in the syringe well until it is evenly mixed .
Add the entire contents of the syringe to the vial containing the Hib pellet. Shake until pellet is completely dissolved.
Draw up 0.5mL dose. Inject immediately after reconstitution.
ADMINISTRATION: Intramuscular: As per NCCU policy
ADVERSE EFFECTS & COMMENTS:
Redness, swelling. A nodule may be palpable at site for a few weeks. Fever, malaise, irritability. Persistent screaming, vomiting, shock, collapse
Infanrix hexa should not be administered to subjects with known hypersensitivity to components of the vaccine.
Infanrix hexa is contraindicated if the child has experienced encephalopathy of unknown aetiology, occurring within 7 days following previous vaccination with pertussis containing vaccine. In these circumstances pertussis vaccination should be discontinued and vaccination continued with diptheria-tetanus,hepatitis B, inactivated polio and Hib vaccines.
REFERENCES: West Australian Vaccination Schedule July 2007 The Australian Immunisation Handbook 9th Ed NHMRC
DATE: June 2008

DRUG: DOBUTAMINE
PRESENTATION: Vial: 250mg/20mL
ACTION & INDICATION:
Inotropic agent used to increase cardiac output. Cardiovascular shock.
DOSE : 1 – 20 microgram / kg / minute Initially 5 microgram / kg / minute. Adjust according to response to 2 to 15 microgram / kg / minute
PREPARATION: Use solution prepared in Pharmacy if available.
Withdraw 30mg of dobutamine per kg of baby's weight (2.4mL/kg) and dilute to 50 mL with appropriate infusion fluid.
This will give the following infusion rate
0.5 mL / hour = 5 microgram / kg / minute
1 mL / hour = 10 microgram / kg / minute
1.5 mL / hour = 15 microgram / kg / minute If a different concentration is required, refer to the Calculation of Drug Infusion table.
ADMINISTRATION: Intravenous infusion or umbilical arterial or venous infusion via syringe pump.
ADVERSE EFFECTS:
Tachycardia
Dysrhythmias
Hypertension – blood pressure must be continuously monitored during infusion.
Avoid extravasation
COMMENTS:
Refrigerate solution.
Discard after 24 hours.
Solution may exhibit pink discolouration without loss of potency.
REFERENCES: BNF for Children 2007 Neofax 2006
DATE: June 2008

DRUG: DOMPERIDONE
PRESENTATION: Oral suspension: 5mg/5mL
ACTION & INDICATION:
Dopamine antagonist with a prokinetic effect on the gastrointestinal tract, enhancing gastric emptying and intestinal motility.
DOSE: 100 to 300microgram//kg/dose 4 to 6 times daily
ADMINISTRATION: Give prior to feeds.
ADVERSE EFFECTS:
Dry mouth, headache Galactorrhoea, gynecomastia, rash, insomnia Extrapyramidal effects (rare)
COMMENTS: Suspension prepared from tablets
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
BNF for Children 2007
DATE: June 2008

DRUG: DOPAMINE
PRESENTATION: Ampoule: 200mg / 5mL
ACTION & INDICATION:
Inotropic agent which increases cardiac output and renal perfusion.
DOSE: 2 to 20 microgram / kg / minute
Begin at 3 microgram / kg / minute and titrate dose according to response.
PREPARATION: Use solution prepared in Pharmacy if available.
Diluent: 0.9% Sodium chloride, Glucose 5% and 10%, Glucose and Saline Solutions.
Withdraw 30mg of dopamine per kg of baby’s weight (0.75mL/kg) and dilute to 50mL with appropriate infusion fluid.
This will give the following infusion rates:
0.5mL / hr = 5 microgram / kg / minute
1mL / hr = 10 microgram / kg / minute
1.5mL / hr = 15 microgram / kg / minute If a different concentration is required, refer to the Calculation of Drug Infusion table.
ADMINISTRATION:
Intravenous or umbilical venous infusion (umbilical arterial is not the preferred route)
ADVERSE EFFECTS & COMMENTS:
Ectopic beats, bradycardia, tachycardia, vasoconstriction, excessive diuresis.
Hypertension – blood pressure must be continuously monitored during infusion.
Extravasation can cause tissue necrosis.
REFERENCES: Neofax 2006 BNF for Children 2007
DATE: June 2008

DRUG: ERYTHROMYCIN
PRESENTATION: Oral suspension : 400mg/5mL
Vial: 1g
ACTION & INDICATION :
Broad spectrum macrolide antimicrobial agent for the treatment of sensitive organisms including Chlamydia trachomatis, Mycoplasma and Ureaplasma. May be used as a prokinetic agent to treat neonatal gut dysmotility
DOSE : Preterm and first week of life
10 mg/kg/dose 12 hourly
2- 4 weeks
10 mg/kg/dose 8 hourly
≥5 weeks
12.5mg/kg/dose 6 hourly As a prokinetic agent: 3 mg/kg/dose 6hourly
PREPARATION: Intravenous Diluent: Water for Injections Add 18.2 mL of Water for Injections to 1g vial = 50mg/mL Take 1 mL of the above solution and dilute it to 5 mL with Water for Injections or 0.9% Sodium chloride (do not use Glucose solutions) = 10 mg/mL Oral Suspension 400mg/5mL: Add 77mL of Water for Irrigation to the powder in the bottle. For small oral doses the oral suspension may be further diluted - eg Take 0.5mL and dilute to 4mL =10mg/mL
ADMINISTRATION: Intravenous: Infuse over 30 – 60 minutes via syringe pump. Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Pain on injection, phlebitis Bradycardia, hypotension Gastric irritation May increase serum levels of digoxin, theophylline, carbamazepine Increased risk of infantile hypertrophic pyloric stenosis
COMMENTS: Refrigerate reconstituted vial. Discard after 24 hours. Discard further diluted solution immediately after use. Store reconstituted oral suspension in refrigerator. Discard after 10 days.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne BNF for Children 2007 (GI Stasis)
DATE: June 2008

DRUG: ERYTHROPOIETIN (Epoietin alfa)
PRESENTATION: Prefilled syringes: varying strengths
Vial: 40,000U/mL
ACTION & INDICATION:
Stimulates erythropoiesis.
Decreases the need for blood transfusions in pre-term infants.
Anaemia of prematurity
DOSE: 200 units/kg on alternate days OR 100 units kg/daily Supplement with: Ferrous sulphate mixture 0.5mL/kg/day initially 1mL/kg/day at full feeds Multivitamins Folic acid 100 microgram daily Vitamin E 10-15 units daily
PREPARATION: Use syringe prepackaged for individual patient use.
ADMINISTRATION: Intravenous: over 3-5 minutes
Subcutaneous: As per NCCU policy
ADVERSE EFFECTS :
Neutropenia
Hypertension
Cutaneous rashes
Seizures
COMMENTS: Monitor (at start of treatment and then weekly):
Full blood count with differential, reticulocyte count and platelet count.
Cease treatment if granulocyte count< 1000 or haematocrit >45.
Protect from light
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: FAT EMULSION 20%
PRESENTATION: Prefilled syringes: 20% fat emulsion (1g = 5mL of fat emulsion)
Infusion: 500mL
ACTION & INDICATION:
Concentrated source of energy and essential fatty acid for babies unable to receive enteral feeding because of immaturity or illness.
Included in total parenteral nutrition regimen.
DOSE: Commencing dose: 0.5-1g/kg 24 hourly
Increasing to: 2-3g/kg 24 hourly
Dose increments: 0.5-1g/kg 24 hourly
ADMINISTRATION:
Do not dilute
Intravenous infusion:
Infants<34 weeks 0.5-1mL/hour
Infants ≥34 weeks 0.5-3mL/hour Do not infuse in excess of 0.15g/kg/hour.
COMMENTS: Use with caution in the presence of hepatic disease or unconjugated hyperbilirubinaemia.
Rapid infusion may interfere with pulmonary diffusion of gases. Fat overload can occur with rapid infusion. Protect from light. Supplied in amber syringes but amber lines are not used Do not add medication to fat emulsion syringes.
REFERENCES: Neofax 2006
DATE: June 2008

DRUG: FERROUS SULPHATE
PRESENTATION: Elixir: contains 150mg/5mL ferrous sulphate- equivalent to 30mg/5mL of elemental iron.
ACTION & INDICATION:
Iron Supplement, iron deficiency anaemia.
For all infants born at less than 33 completed weeks gestation, starting at four weeks of age, when on full enteral feeds or prior to discharge or transfer, at the discretion of the Consultant Neonatologist.
DOSE : Prophylaxis (if required, for fully breast-fed babies only): 0.15mL/kg 12 hourly
Treatment: 1mL/kg/day
ADMINISTRATION: Oral
Preferably prior to a feed, otherwise administer with feeds.
ADVERSE EFFECTS:
Contraindicated in thalassaemia and anaemia not due to iron deficiency.
Nausea, GI irritation, constipation.
COMMENTS: Iron supplementation should not be started until adequate vitamin E is supplied in the diet. Contains 70% Sorbitol solution 100mg/mL
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Neofax 2006
DATE: June 2008

DRUG: FLECAINIDE
PRESENTATION: Ampoule: 10mg/mL (15mL in each ampoule)
Oral Solution : 5mg/mL (SAS authority required)
ACTION & INDICATION
Membrane stabilizing antiarrhythmic agent. Used for the suppression and prevention of ventricular arrhythmias and supraventricular tachycardia.
DOSE: IV: 0.5mg/kg/dose 12 hourly (maximum dose 2mg/kg)
ORAL: Initially 2mg/kg/dose twice daily. Dose may be titrated at intervals of 4 days to a maximum of 6mg/kg/day
ADMINISTRATION: Intravenous infusion over 30 minutes. Diluent: 5% glucose
Oral: Milk may reduce absorption. Separate doses from feeds
ADVERSE EFFECTS & COMMENTS:
Monitor cardiac function - proarrhythmic effects can occur.
Heart failure – may worsen or cause CCF.
Reduce dose in impaired renal or liver function.
Palpitations, diarrhoea, rash, tremor, dyspnoea.
Monitor electrolytes.
Monitor urine pH - rate of excretion increases with drop in urine pH. Do not refrigerate oral mixture. May crystallise.
MONITORING DRUG LEVELS:
Sampling time: Just before next dose.
Therapeutic range: 200 – 1000 microgram/L
Time to reach steady state: 5 - 7 days
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: FLUCLOXACILLIN
PRESENTATION: Oral suspension: 250 mg/5 mL Vial: 500 mg
ACTION & INDICATION:
β-lactamase resistant penicillin, usually used for the treatment of staphylococcal infection.
DOSE : < 34 weeks < 14 days 25 mg/kg/dose 12 hourly < 34 weeks ≥ 14 days 25 mg/kg /dose 8 hourly ≥ 34 weeks < 14 days 25 mg/kg/dose 8 hourly ≥ 34 weeks ≥ 14 days 25 mg/kg/dose 6 hourly For Staph aureus bacteraemia, meningitis, osteomyelitis, use 50mg/kg/dose.
PREPARATION:
Diluent: Water for Injections Intravenous: Add 4.6 mL diluent to vial =100 mg/mL May be further diluted if required Intramuscular: Add 2.1 mL diluent to vial = 200 mg/mL Oral suspension 250mg/5mL: Add 60mL of Water for Irrigation to the powder for suspension in the bottle.
ADMINISTRATION: Oral: Give 30 minutes before feeds Intramuscular: As per NCCU policy. Intravenous: Infuse over 10 minutes
ADVERSE EFFECTS:
Hypersensitivity, rash Colitis (oral).
COMMENTS: Reconstituted vial stable for 24 hours under refrigeration Refrigerate reconstituted oral suspension. Discard after 14 days.
REFERENCES: BNF for Children 2007 Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: FLUCONAZOLE
PRESENTATION: Vial : 2mg/mL (50mL, 100mL) Oral suspension : 50mg/5mL
ACTION & INDICATION:
Antifungal. For the treatment of systemic Candidal infections. Prophylaxis against candidal colonization in very low birthweight infants.
DOSE:
For systemic infections: Loading dose: 12mg/kg/dose Maintenance dose: 6mg/kg/dose Age: ≤ 14 days once every three days 15-27 days: once every two days ≥ 28days once daily For prophylaxis: On Consultant’s prescription 3mg/kg/dose once every three days
PREPARATION: Use solution prepared in Pharmacy if available. IV: Use undiluted. Oral: Add 24mL of Water for Irrigation to the powder for suspension in the bottle = 50mg/5mL.
ADMINISTRATION: IV: Infuse over at least 60 minutes Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Rash GI upset Reversible transaminase enzyme elevation.
COMMENTS:
Discard vial immediately after use. Oral suspension: Store at room temperature. Discard after 14 days. Alters metabolism of phenytoin, barbiturates, caffeine, midazolam. Monitor levels of these drugs if used concomitantly. Reduce dose in renal impairment. Contains 15mmol Na/100mL
REFERENCES: Neofax 2006 Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: FLUCYTOSINE
PRESENTATION: Infusion solution: 2.5 g/250 mL
Unit dose syringes: 10 mg/mL (Prepared in Pharmacy).
Oral Solution: 10mg/mL (Prepared in Pharmacy).
ACTION & INDICATION :
Antifungal agent for systemic fungal infections. Should always be used in combination with another appropriate antifungal agent.
DOSE: Usual dose: 25-37.5 mg/kg/dose 6 hourly Severe infection: 50 mg/kg/dose 6 hourly Acute infections: 2 - 4 weeks therapy Subacute/chronic infections: prolonged therapy
ADMINISTRATION: Intravenous: Infuse over 30 minutes via syringe pump Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Bone marrow toxicity Hepatotoxicity
COMMENTS:
Increase interval between doses in renal impairment.
Must be used in combination with another antifungal agent.
Store intravenous preparations between 15 and 25 C Cytotoxic handling and disposal procedures should be followed
DRUG MONITORING:
Sampling time: Pre and post levels to be taken at the THIRD dose (so as to ensure therapeutic levels) and weekly thereafter.
Trough level: Immediately prior to dose. Peak level: IV: 30 minutes after completion of infusion. Oral: 3 hours post dose
Trough: 25 - 40 mg/mL Peak: 60 – 80 mg/mL
REFERENCES:
Neofax 2006 Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: FLUDROCORTISONE ACETATE
PRESENTATION: Tablet: 100 microgram
ACTION & INDICATION:
Adrenal insufficiency requiring mineralcorticortoid replacement.
Salt losing forms of congenital adrenogenital syndrome.
DOSE: 50 - 100 microgram daily Adjust dose according to response Usual range 50-300 microgram daily
ADMINISTRATION: Oral: Give with or immediately after feeds.
ADVERSE EFFECTS:
Severe oedema
Hypertension
Electrolyte imbalance (monitor - weight, blood pressure and serum electrolytes).
COMMENTS: Often used in combination with hydrocortisone
REFERENCES: BNF for Children 2007 Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG:
FLUMAZENIL
PRESENTATION:
Ampoule : 100microgram/mL (5mL in each ampoule)
ACTION & INDICATION:
Benzodiazepine antagonist. Reverses the central sedative effects of benzodiazepines.
DOSE:
10 microgram/kg Repeat every 60 seconds to a total of 40 microgram/kg Infusion : 2-10 microgram/kg/hr
PREPARATION:
Diluent : Water for Injections. Take 1mL and dilute to 10mL = 10 microgram/mL
ADMINISTRATION:
Intravenous : rapid injection into large vein IV infusion
ADVERSE EFFECTS:
Nausea, vomiting
COMMENTS:
Repeated doses may be required as flumazenil has a short duration of action.
REFERENCES:
Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne BNF for Children 2007
DATE:
June 2008

DRUG: FLUTICASONE
PRESENTATION: Aerosol: Fluticasone propionate
50 microgram per metered dose
ACTION & INDICATION:
Glucocorticoid with potent anti-inflammatory action in the airway. Has low systemic bioavailability. For treatment of bronchopulmonary dysplasia (BPD).
DOSE: 50 -100 microgram twice daily
ADMINISTRATION: Use the inhaler via an Aerochamber® (from the Physiotherapy Department).
ADVERSE EFFECTS :
Candidiasis of mouth and throat Hoarseness
COMMENTS: Wash mouth with water after use
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: FOLIC ACID
PRESENTATION: Ampoule: 15mg/mL
Oral solution : 500 microgram/mL
ACTION & INDICATION:
B-group vitamin.
For megaloblastic anaemia or folic acid deficiency.
All preterm infants under 34 weeks gestation commencing at 2 weeks of age may be ordered daily folic acid at the discretion of the Consultant Neonatologist
DOSE: 50 microgram daily.
PREPARATION:
Intravenous: Diluent: Water for Injections
Take 0.1mL and dilute to 15mL with diluent. = 100 microgram/mL
ADMINISTRATION:
Oral: May be given at any time with regard to feeds.
Intravenous: over 3-5 minutes
Intramuscular
ADVERSE EFFECTS:
Allergic type reactions.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne BNF for Children 2007
DATE: June 2008

DRUG: FRAMYCETIN EYE DROPS
PRESENTATION: Ophthalmic solution
Each mL contains: Framycetin 5mg
Benzalkonium Chloride preservative
ACTION & INDICATION:
Aminoglycoside antibiotic eye drop with activity against both gram-positive and gram-negative bacteria.
DOSE: 1 or 2 drops 4 hourly with feeds for 4 days. Eye toilet / care should be performed prior to the administration of each dose.
ADVERSE EFFECTS :
Do not use eye drops for more than 5 days as chemical conjunctivitis may occur.
Local hypersensitivity reactions.
DATE: June 2008

DRUG: FRUSEMIDE
PRESENTATION: Ampoule: 20mg / 2mL
Oral Solution: 10mg / mL
ACTION & INDICATION:
Diuretic. Adjunct therapy for chronic lung disease, congestive heart failure, renal failure. Oedema.
DOSE: IV/IM: 0.5 - 1 mg / kg / dose 12 - 24 hourly
Oral: 0.5 - 2 mg / kg / dose 12 – 24 hourly.
Dose may be increased to 6mg / kg / dose in resistant cases
ADMINISTRATION: Oral: May be given at any time with regard to feeds.
Intramuscular: As per NCCU policy.
Intravenous : Over 3-5 minutes May be diluted with Water for Injections, Sodium Chloride 0.9%
ADVERSE EFFECTS:
Disturbance of water and electrolyte balance - monitor urea and electrolytes.
Consider addition of potassium sparing diuretic with prolonged therapy.
Displaces bilirubin from albumin.
Potentially ototoxic
Refrigerate oral solution.
Discard 21 days after opening.
REFERENCES: BNF for Children 2007 Paediatric Pharmacopoeia 13th Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: FUSIDIC ACID
PRESENTATION: Vial : 500mg (sodium fusidate)
Mixture : 50mg/mL of fusidic acid (equivalent to 35mg/mL sodium fusidate) (Manufactured in Pharmacy)
ACTION & INDICATION:
Narrow spectrum, antistaphylococcal antibiotic for the treatment of resistant organisms. It inhibits protein synthesis by the prevention of translocation on the ribosomes.
DOSE: Oral : 15mg/kg/dose 8 hourly (Fusidic acid)
IV : 10mg/kg/dose 12 hourly (Sodium fusidate)
PREPARATION: Use solution prepared in Pharmacy if available. IV : Dissolve the contents of a vial in 10mL of buffer solution provided. Take 1mL and dilute to 25mL with Sodium chloride 0.9% = 2mg/mL
ADMINISTRATION: Oral: Given with or immediately after feeds. IV : Infuse over at least 2 hours into a large vein.
ADVERSE EFFECTS:
Monitor liver function – may rapidly elevate liver enzymes Jaundice Gl side effects Venospasm, thrombophlebitis Skin rashes Granulocytopenia, haemolytic anaemia Severe allergic reactions are rare
COMMENTS: In severe infections or where prolonged therapy is required, fusidic acid must be given concurrently with other antistaphylococcal therapy Refrigerate reconstituted vial. Discard after 24 hours.
REFERENCES: BNF for Children 2007
DATE: June 2008

DRUG: GANCICLOVIR PRESENTATION: Individual patient syringes: (Supplied by Oncology Pharmacy at
PMH) Oral suspension: 25mg/mL
ACTION & INDICATION
Antiviral preparation used for the management of cytomegalovirus infection (CMV)
DOSE: IV: 5mg/kg/dose every 12 hours ORAL: 25mg/kg/dose every 6 hours
Reference: Dr T Keil
ADMINISTRATION: IV infusion: Over 1 hour Oral: Administer oral dose with feeds to enhance absorption
ADVERSE EFFECTS: Neutropenia and thrombocytopenia have been reported frequently. Dose may need to be reduced. Fever, rash, abnormal liver function test results. Chills dysrhythmias and haematuria
COMMENTS: Cytotoxic handling and disposal procedures should be followed. (Contact your ward pharmacist for information) Renally excreted – increase dose interval with renal impairment. Store oral suspension at room temperature.
REFERENCES: Dr T Keil Microbiology KEMH Neofax 2006 Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: GENTAMICIN
PRESENTATION: Ampoules: 80 mg/2 mL
ACTION & INDICATION:
Aminoglycoside antibiotic for the treatment of infections caused by susceptible organisms including E. Coli, Pseudomonas, Klebsiella.
DOSE: <30 weeks 0-7days 5mg/kg once every 48 hours >7days 5mg/kg once every 24 hours 30-35 weeks 0-7days 6mg/kg once every 48 hours >7days 6mg/kg once every 24 hours >35 weeks 0-14days 4½mg/kg once every 24 hours >14days 7mg/kg once every 24 hours
PREPARATION:
Diluent: 0.9% Sodium chloride or Water for Injections
Intravenous: Take 2mL and dilute to 8mL = 10mg/mL
ADMINISTRATION: Intravenous : Give over 10 minutes Intramuscular: Use undiluted
ADVERSE EFFECTS: Nephrotoxicity - may be increased by cephalosporins.
Ototoxicity
COMMENTS: Monitor serum levels Monitor urine output - withhold dose if poor urine output. Inactivated by β-lactam antibiotics eg. penicillin and cephalosporins. Do not give doses simultaneously.
DRUG MONITORING: IM, IV:
A single blood level estimation should be performed in those infants requiring a prolonged course of Gentamicin (>5days). This decision will generally be made once the results of relevant cultures are available . A request for levels will be ordered by the medical staff. Blood levels may need repeating if a drug dose is altered or if the infant’s clinical situation (ie renal failure) is likely to lead to unpredictable levels. Monitoring: Trough level: 0.4mL blood immediately prior to dose. Peak level : 0.4mL blood 1 hour post dose. For all babies calculate “area under the curve” using the results obtained. Area Under The Curve (AUC): Ideal range is

80 – 100mg/L.hour Expected levels: Peak: >10mg/L Trough level at 24 hours post dose: < 2mg/L Trough level at 48 hours post dose: < 1mg/L Consult a senior physician if levels are outside these AUC parameters. To calculate the “Area Under the Curve”, a computer programme called “48-NeoGent” has been written. To perform the calculations and generate a report, please follow these instructions; 1. Using the computer mouse, move the cursor over the “48-
NeoGent” icon on the main screen. 2. ‘Double-click’ on this icon. 3. Click once on the option ‘enable macros’ (if this message
appears). 4. Type in the patient’s name. Move to the next box by hitting the
‘TAB’ key on the computer keyboard. 5. Type in the times of drug administration and taking the levels, but
bear in mind; (i) You need to put the hour in one box and the minutes in the
other. (ii) Use a ’24 hour’ clock format. For example, if a time is 2pm,
type it in as 14 (ie 12 noon + 2 hours) 6. Type in the date (dd/mm/yy format, for example, 23/07/02 for 23rd
July 2002). 7. Using the ‘mouse, move the cursor and click on the button that
says ‘click here’. This will print off a report, clear all of the data you have just typed in and switch off the programme.
8. Take the printed report from the printer, bring it to the attention of a medical officer and place it into the patient’s file.
REFERENCES: KEMH/PMH research/audits Monitoring: J. Ailakis Pharmacist PMH Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008

DRUG: GLUCAGON
PRESENTATION: Vial: 1mg powder with 1mL syringe of Water for Injections as diluent.
ACTION & INDICATION:
A pancreatic hormone which increases blood glucose concentrations by stimulating hepatic glycogenolysis.
For prolonged hypoglycaemia unresponsive to routine therapy.
DOSE: IV, IM, SC 200 microgram/kg (Maximum dose 1mg)
Dose may be repeated in 20 mins if required.
Intravenous Infusion: 5-20 microgram/kg/hour
PREPARATION: Dilute powder with diluent supplied. = 1000 microgram/mL
To prepare infusion :
Dilute the contents of reconstituted vial to 50mL with 10% glucose solution to make a 1000 microgram/50mL solution. 0.5mL/kg/hour = 10 microgram/kg/hour
ADMINISTRATION: Subcutaneous: As per NCCU policy
Intramuscular: As per NCCU policy
Intravenous : over 3-5 minutes
Intravenous infusion : via syringe pump
COMMENTS: Monitor plasma glucose levels and adjust drug dose accordingly.
1mg is equivalent to 1 unit of activity.
REFERENCES: Neofax 2006 BNF for Children 2007
DATE: June 2008

DRUG: GLYCERYL TRINITRATE
PRESENTATION: Ampoule: 50mg / 10mL
ACTION & INDICATION:
Vasodilating agent. For control of hypertension associated with surgical procedures such as cardiac surgery.
DOSE: IV: 1 to 10 microgram / kg / minute
PREPARATION: Use solution prepared in Pharmacy if available.
Diluent: Glucose 5% only Add 3mg / kg to 50mL of diluent. This is then infused at a rate of 1 - 10 mL / hr = 1 microgram / kg / minute to 10 microgram / kg /minute For other concentrations refer to the Calculation of drug infusion table.
ADMINISTRATION:
Intravenous infusion.
Use only polyethylene tubing – Portex manometer or Go Medical V2V4, V set tubing, as GTN migrates readily into plastic.
Do not filter.
ADVERSE EFFECTS:
Tachycardia Bradycardia Hypotension Vomiting Use gloves, or wash hands well when handling GTN to prevent severe headaches.
COMMENTS: Do not use if turbidity or crystallisation present in prepared solution (concentration > 20mg/50mL).
GTN IS NOT LIGHT SENSITIVE
Compatible with Morphine and Dopamine solutions providing they are diluted in Glucose 5% and rate of administration is similar.
REFERENCES: BNF for Children 2007
DATE: June 2008

DRUG: GLYCERYL TRINITRATE TOPICAL
PRESENTATION: Ointment: 0.2%
ACTION &
INDICATION
Vasodilator. May be used to reverse peripheral tissue ischaemia secondary to arterial line complications in neonates
DOSE: 1 centimeter / kg .Repeat dose every eight hours if necessary
ADMINISTRATION: Apply as a thin film over affected areas
ADVERSE EFFECTS:
Tachycardia, paradoxical bradycardia, flushing, headache Nausea, vomiting, heartburn, dizziness Avoid use with increased intracranial pressure, severe anaemia, hypotension. Avoid concomitant administration of sildenafil, nitric oxide.
COMMENTS: Use gloves when applying ointment to avoid side effects in person administering drug. The 2% ointment (Nitro-Bid) is no longer available in Australia Glyceryl trinitrate patches (release rate 5mg/24 hours), cut into strips have also been used. Apply for 2 to 4 hours. Review the area then reapply if desired. Each strip may be used for up to 24 hours.
REFERENCES: BNF for Children 2007 Baserga MC, Pur A, Sola A. The use of topical nitroglycerine ointment to treat peripheral tissue ischaemia secondary to arterial line complications in neonates. J Perinatol 2002;22(5):416-9
DATE: July 2008

DRUG: GLYCOPYROLLATE
PRESENTATION: Vial: 200 microgram/mL (suitable for ORAL use) Oral solution: 200microgram /mL (Prepared by Auspman)
ACTION & INDICATION:
Antimuscarinic agent with atropine-like actions. It is used to reduce excessive respiratory tract secretions.
DOSE:
IV/IM: 4– 10 microgram/kg/dose every 3 to 4 hours. Oral: 40-100microgram/kg/dose 3 to 4 times daily
ADMINISTRATION:
Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Drowsiness, insomnia, tachycardia, urinary retention, constipation, inhibition of sweating.
COMMENTS:
Glycopyrrolate is also referred to as ‘glycopyrronium’. Antidote: Neostigmine.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Pediatric Dosage Handbook 14th Ed BNF for Children 2007`
DATE: June 2008

DRUG: HAEMOPHILUS INFLUENZAE TYPE B CONJUGATE VACCINE (PedvaxHIB)
PRESENTATION: Vial: 0.5mL
ACTION & INDICATION:
Active immunisation against invasive diseases caused by Haemophilus influenzae type B in infants and young children.
DOSE:
ADMINISTRATION:
ADVERSE EFFECTS: COMMENTS:
For Indigenous Infants. To be administered in conjunction with Infanrix Penta
0.5mL (7.5 micrograms ) 1st dose 2 months 2nd dose 4 months 3rd dose 12 months
Intramuscular: As per NCCU policy.
DO NOT GIVE INTRAVENOUSLY OR INTRADERMALLY.
Swelling, erythema, soreness at injection site
Fever
Do not give during febrile illness or acute infection.
REFERENCES: Western Australian Vaccination Schedule July 2007 The Australian Immunisation Handbook NH&MRC
DATE: June 2008

DRUG: HEPARIN SODIUM
PRESENTATION: Ampoule: 1000 units / mL
ACTION & INDICATION:
Anticoagulant.
Prophylaxis and treatment of thromboembolic disorders eg. Thrombophlebitis, pulmonary embolus and occlusive vascular disease.
Prevention of thromboembolic complications arising from cardiac and vascular surgery, dialysis and other perfusion procedures.
As a flush solution for umbilical, arterial and intravenous catheters to maintain patency.
As an anticoagulant in blood transfusions.
DOSE:
Treatment:
Intravenous: Low dose: 75 units / kg stat, then 5 - 15 units / kg / hr
Full dose: 50 - 200 units / kg stat, then 15 - 30 units / kg / hr. Adjust dose according to clotting times Prophylaxis:
Infusion 0.5 units / mL of solution solution: Intra-arterial, umbilical venous and peripheral longlines only.
ADVERSE EFFECTS & COMMENTS:
Haemorrhage ranging from minor local ecchymoses to major haemorrhagic complications.
Delayed onset thrombocytopenia. Hypersensitivity: pruritis, urticaria, asthma like symptoms. Monitor APTT if treatment dose is used
REFERENCES: Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: HEPATITIS B VACCINE
PRESENTATION: Unit dose syringe or vial: H-B-Vax II Preservative-free 0.5mL ( 5 micrograms ) or, if this is unavailable ENGERIX-B 0.5mL ( 10 micrograms )
ACTION & INDICATION:
Hepatitis B surface antigen induces protective antibody formation to Hepatitis B virus (Anti-HBs). Used as prophylaxis for all infants and for the management of babies born to HBs Ag positive mothers.
DOSE: 0.5mL The different brands may be interchanged. For preterm infants <32 weeks of age : 1st dose at birth or no later than 2 weeks of age 2nd dose at 2 months 3rd dose at 4 months 4th dose at 6 months 5th dose at 12 months if antibody titre low If infant less than 1000g omit birth dose and give first dose at 2 months of age. All other infants : 1st dose at birth or in the first 2 weeks of life 2nd dose at 2 months of age 3rd dose at 4 months of age 4th dose at either 6 or 12 months
ADMINISTRATION: Intramuscular injection Shake syringe well before administration. Air bubble in syringe does not need to be expelled before administration; Withhold dose if there is a known or suspected coagulopathy DO NOT GIVE INTRAVENOUSLY OR INTRADERMALLY Administer in anterolateral thigh
ADVERSE EFFECTS:
Swelling, erythema, soreness at injection site
COMMENTS: Hepatitis B vaccine is now recommended for all children. If the monovalent dose at birth is missed, vaccination against Hepatitis B should be continued with a multivalent vaccine following the routine schedule. Hepatitis B vaccine is a component of Infanrix Hexa and

Penta, and is admininistered in this form at 2,4 and 6 month doses When available, it is preferable to administer H-B-Vax II PRESERVATIVE-FREE. For infants of Hepatitis B positive mothers on the day of birth: IM Hepatitis B immunoglobulin 100 IU to be given in conjunction with initial Hepatitis B vaccine. These products must be administered separately and in different sites. Current information from the Health Department regarding the different manufacturers of the vaccine states that although ENGERIX B Vaccine = 10microgram/0.5mL and H-B –VAX 11 = 5microgram/0.5mL the required dose is still 0.5mL
REFERENCES: The Australian Immunisation Handbook 9th Ed 2007 NH&MRC West Australian Vaccination Schedule July 2007
DATE: June 2008

DRUG: HYALURONIDASE
PRESENTATION: Ampoule: Powder for reconstitution 1500 units
ACTION & INDICATION: Hyaluronidase is an enzyme that promotes the reabsorption of extravasated fluid by temporarily breaking down the hyaluronic acid of tissue cement. After administering hyaluronidase this tissue cement is broken down for 24 - 48 hours. The extravasated fluid is spread over a large absorptive area, but irritation is said to be minimised by dilution in tissue fluids.
DOSE: a) Infiltration of hyaluronidase alone into extravasation injury without Sodium Chloride 0.9% irrigation
Hyaluronidase 1ml dose (15units/mL concentration) through existing IV cannula
AND/OR Hyaluronidase 1mL dose in 5 aliquots of 0.2mL (300units/mL concentration) into the periphery of the extravasation injury.
OR
b) Infiltration of hyaluronidase into the extravasation injury followed by Sodium Chloride 0.9% irrigation
Hyaluronidase 1mL dose in 5 aliquots of 0.2mL (1000units/mL concentration) around and through the extravasation injury. Followed by Irrigation with sodium chloride 0.9% as described in the protocol
PREPARATION: See dose section above for concentration required.
For 15 units/mL concentration Dissolve the contents of ampoule in 1mLwater for injections. Withdraw and dilute to 10mL (150Units/mL) Take 1mL (150Units/mL) of above dilution and further dilute to 10mL. Final concentration is 15units/mL For 300 units/mL concentration Dissolve the contents of ampoule in 1mL of water for injections. Withdraw and dilute to 1.5mL. Take 0.3mL of this dilution and further dilute to 1mL (300Units/mL) For 1000units/mL concentration Dissolve the contents of ampoule in 1mL of water for injections. Withdraw and dilute to 1.5mL. (1000units/mL)
ADMINISTRATION: Subcutaneous or intradermal injection
ADVERSE EFFECTS : Not recommended for IV use
COMMENTS: Do not use for extravasations of vasoconstrictive agents (eg dopamine, adrenaline, noradrenaline…see phentolamine ) Use within one hour for best results. Use only freshly prepared dilutions. Discard excess immediately after use.
REFERENCES:
NCCU Clinical Guidelines Section 5
DATE: June 2008

DRUG:
HYDRALAZINE HYDROCHLORIDE
PRESENTATION: Ampoule: 20 mg Oral Solution: 10 mg/mL
ACTION & INDICATION:
Peripheral vasodilator. Moderate to severe hypertension, congestive cardiac failure.
DOSE: Intravenous: Initial dose: 100 - 500 microgram / kg /dose 6 to 8 hourly Dose may be increased slowly as required to a Maximum dose: 2 mg/kg/dose Continuous intravenous infusion: 12.5 – 50 microgram/kg/hour Oral: Initial dose: 250 microgram to 1mg/ kg/ dose 6 to 8 hourly Increase gradually to 2mg/kg/dose.
PREPARATION: IV : Reconstitute using 1mL of Water for Injections. Then dilute 1mL to 20mL with 0.9% Sodium chloride. = 1mg/mL (1000microgram/mL) May be further diluted if required. Continuous intravenous solution: Withdraw 1250microgram (1.25mL) of the 1mg/mL dilution, per kg of baby’s weight, and dilute to 50mL with 0.9% Sodium chloride. This will give the following infusion rate: 1mL/hr = 25microgram/kg/hour
ADMINISTRATION: IV: Slow IV over 5 to 20 minutes Oral: Give with feeds to enhance absorption.
ADVERSE EFFECTS:
Hypotension – also precipitated by anaesthetic agents. Reflex tachycardia - modified by β blocking drugs. Sodium, water retention. Flushing; dyspnoea, urticaria, fever. Anaemia, leucopenia, thrombocytopenia.
COMMENTS: Monitor blood pressure pre and ½ hour post-dose, continue until stabilized for 48 hours, then twice daily. U & E's at commencement and at any change in therapy Discard dilution immediately after use. Incompatible with glucose containing solutions
REFERENCES: Neofax 2006 BNF for Children 2007
DATE: August 2008


DRUG: HYDROCHLOROTHIAZIDE
PRESENTATION: Oral suspension : 50mg/5mL (prepared in pharmacy)
ACTION & INDICATION:
Thiazide diuretic. Used for hypertension and the prevention and treatment of broncho-pulmonary dysplasia (BPD).
DOSE:
1 - 2mg/kg/dose every 12 hours
ADMINISTRATION: Oral: May be given at any time with regard to feeds
ADVERSE EFFECTS:
Hypokalaemia, and other electrolyte abnormalities – monitor electrolytes Hyperglycaemia Hyperuricaemia
COMMENTS:
Decreases renal excretion of calcium. Do not use in hepatic or renal impairment. Effect increased in combination with frusemide or spironolactone.
REFERENCES: Neofax 2006
DATE: June 2008

DRUG: HYDROCORTISONE
PRESENTATION: Vial: 100mg
Oral Solution: 1mg/mL, 10mg/mL (Prepared in Pharmacy).
Tablet: 4mg
Topical: 0.5%, 1% (cream or ointment)
ACTION & INDICATION:
Corticosteroid Used in:- (i) intractable hypoglycaemia (ii) replacement therapy in adrenal insufficiency (iii) anti-inflammatory (including dermatitis) (iv) hypotension refractive to inotropic agents (v) stress/crisis/severe hypotension
DOSE: Intractable hypoglycaemia1 IV/Oral: 1-2mg/kg/dose 6 hourly
Titrate dose according to clinical response
Anti-inflammatory2 IV : 2 - 4 mg/kg/dose 6 hourly for 24 hours Taper over several days Physiological replacement5 Oral : 8 to 18 mg/m2 per day divided into 3 doses IV: 8 to 18 mg/m2 per day divided into 4 hourly doses See next page for Body Surface area calculation Early neonatal hypotension4
IV : 2mg/kg/dose stat, then 1mg/kg/dose 6 hourly Stress/crisis/severe hypotension5
IV: <3kg 12.5mg stat >3kg 25mg stat Maintenance : 100 mg/m2 per day divided into 4 hourly doses Topically Apply sparingly 1 - 3 times daily
PREPARATION:
Diluent: Water for Injections or sodium chloride 0.9%
Add 1.5mL of diluent to each vial, then withdraw and dilute to 2mL= 100mg/2mL May be further diluted if required, that is; Take 2mL of the above solution and dilute it to 10mL = 10 mg/mL

ADMINISTRATION: Intramuscularly Intravenously: Over 3-5 minutes Oral: Given with or immediately after feeds. Topical: Apply sparingly to the affected areas only.
ADVERSE EFFECTS: Hypokalaemia, abdominal distension, oesophagitis, impaired
wound healing, thin fragile skin, petechiae, convulsions, manifestations of latent diabetes mellitus, growth suppression in children, hypertension, hyperglycaemia. Contraindication - Systemic Fungal infection. Topical hydrocortisone is contraindicated in untreated bacterial, fungal or viral skin lesions.
COMMENTS: Refrigerate reconstituted parenteral solution and discard after 24 hours. Body Surface Area3
Weight(Kg) Surface Area (sq.metres)
0.6 0.08 1 0.1
1.4 0.12 2 0.15 3 0.2 4 0.25
*BSA (m2) = (0.05 x kg)+0.05
REFERENCES: 1.Pediatric Dosage Handbook 14th Ed Lexicomp 2.Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne 3.Neofax 2006 4. Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne 5. Sperling Pediatric Endocrinology 2006 Lifshitz Pediatric Endocrinology 2007 Brook Clinical Paediatric Endocrinology 2007
DATE: July 2008

DRUG: HYDROXYCHLOROQUINE
PRESENTATION: Mixture: Hydroxychloroquine sulphate 200mg/5mL Contains - hydroxychloroquine base 155mg/5mL (prepared in Pharmacy).
ACTION & INDICATION:
Anti-malarial agent with anti-inflammatory activity.
Usually used to treat rheumatoid arthritis, systemic lupus erythematosis.
May be used to treat chronic lung disease.
DOSE: Dose stated in terms of hydroxychloroquine base.
5mg/kg/dose daily
ADMINISTRATION: Oral: Given with or immediately after feeds.
ADVERSE EFFECTS :
Visual disturbances – changes to retina and cornea. Rash, alopecia Bone marrow depression Gastrointestinal disturbances Muscle weakness.
REFERENCES: J. Pediatr 1990;116:61-7
DATE: June 2008

DRUG: INDOMETHACIN
PRESENTATION: Vial: 1mg (1000 microgram)
Oral Suspension: 250 microgram/mL (Prepared in Pharmacy).
ACTION & INDICATION:
Prostaglandin synthetase inhibitor.
Closure of haemodynamically significant patent ductus arteriosus.
Prevention of intraventricular haemorrhage.
DOSE:
Oral / Intravenous:
Initial dose: 200microgram /kg/ dose 2nd and 3rd doses : 100microgram /kg /dose Interval between doses : 24 hours
PREPARATION:
IV: Diluent: 0.9% Sodium chloride or Water for Injections. Do not use solutions containing Glucose. Add 2mL of diluent to each vial, then withdraw the vial contents and dilute it to 20mL = 1000 microgram/20 mL (that is = 100 microgram/2mL)
ADMINISTRATION:
Oral: Given with or immediately after feeds. Intravenous: Infuse over 30 minutes to 2 hours. Flush line over at least 30 minutes
ADVERSE EFFECTS:
COMMENTS: REFERENCES:
Nephrotoxicity - use with caution with other renally excreted drugs. Hyponatraemia, hyperkalaemia, oedema, GI bleeding, abdominal distension, transient ileus, NEC, decreased platelet aggregation
Monitor daily urea and electrolytes. Use freshly prepared solution. Discard after use Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Neofax 2006 BNF for Children 2007
DATE: June 2008

DRUG: INSULIN HUMAN, NEUTRAL (ACTRAPID / HUMULIN-R)
PRESENTATION: Vial: 100 units/mL 10mL
ACTION & INDICATION:
A pancreatic hormone. It promotes cellular uptake of glucose, fatty acids and amino acids, and their conversion to storage forms in most tissues. Used in (a) patients with glucose intolerance, and (b) in the reduction of elevated blood potassium levels.
DOSE:
IV/SC: 0.05 – 0.2 units/kg/dose 6 to 12 hourly Infusion: Initial dose: 0.01 – 0.1 units/kg/hour TITRATE TO PATIENT REQUIREMENTS
PREPARATION:
Use solution prepared by Pharmacy. If unavailable dilute as follows: Diluent: 0.9% Sodium chloride and Glucose solutions. Albumin 0.3g/100mL may be added to infusion solutions containing insulin to reduce absorption to plastic. Draw up 0.5mL (50 units) and dilute to 50mL with Water for Injections 50 units in 50mL 1unit in 1mL Dilute 3mL (3 units) per kilogram of baby’s weight of the 1 unit in 1mL insulin dilution to make a final volume of 30mL (0.1unit/kg/mL) 0.5mL/hr = 0.05 units/kg/hr 1 mL/hr = 0.1 units/kg/hr If a more concentrated solution is required Draw up 0.5mL ( 50 units) and dilute to 10mL with Water for Injections 50 units in 10mL 0.5 units in 0.1mL
ADMINISTRATION:
Intravenous injection over 3 – 5 minutes. Intravenous infusion via syringe pump. To prime the line for IV infusion, make up double volume of the concentration required. Prime the line, wait 20 minutes, then discard contents in line. Re-prime the line and infusion is then ready to commence. Subcutaneous: As per NCCU policy.
ADVERSE EFFECTS:
Hypoglycaemia CLOSE MONITORING OF PLASMA GLUCOSE LEVELS IS MANDATORY
COMMENTS: Discard excess solution immediately
REFERENCES: Neofax 2006 Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE:
June 2008

DRUG: ISOPRENALINE
PRESENTATION: Ampoule: 1000 microgram/5mL
ACTION & INDICATION:
Cardiac stimulation, peripheral vasodilation, relaxation of bronchial smooth muscle.
Acts on Beta-1 and Beta-2 adrenergic receptors.
To treat shock, cardiac arrest, ventricular arrhythmias due to AV block, bronchospasm.
DOSE: 0.05 - 0.5 microgram/kg/minute
PREPARATION: Use solution prepared in Pharmacy if available.
Diluent: 0.9% Sodium chloride and Glucose solutions.
To give a dose of 0.1 microgram/kg/minute when infused at 1mL/hour.
Take 300 microgram of isoprenaline per kg of baby’s weight (1.5mL/kg) and dilute to 50mL. If a different concentration is required, refer to the Calculation of Drug Infusion table.
ADMINISTRATION: Intravenous infusion via syringe pump.
ADVERSE EFFECTS:
Tachycardia – continuously monitor heart rate.
Cardiac dysrhythmia, hypertension, hypotension, vomiting, tremor.
REFERENCES: Neofax 2006
DATE: June 2008

DRUG: LIGNOCAINE
PRESENTATION: Ampoule: 50mg in 5mL (1%)
ACTION & INDICATION:
Type 1b anti-arrhythmic agent used for control of ventricular arrhythmias.
DOSE: Loading dose: 0.5 - 1mg/kg.
Maintenance dose: 10-50 microgram/kg/minute
PREPARATION: Dilution for Infusion: Withdraw 30mg/kg from each ampoule and dilute it to 50mL with glucose 5%. Infuse at 1mL/hour = 10 microgram/kg/minute
ADMINISTRATION: Intravenous : Over 5 minutes
Intravenous infusion
ADVERSE EFFECTS:
CNS toxicity: drowsiness, agitation, vomiting, muscle twitching.
Seizures, loss of consciousness, respiratory, depression.
Cardiac toxicity - bradycardia, hypotension, heart block, cardio-vascular collapse.
COMMENTS: Continuous monitoring of heart rate, blood pressure and ECG.
REFERENCES: Neofax 2006
DATE: June 2008

DRUG: MAGNESIUM SULPHATE
PRESENTATION: Ampoule: 2.47g (49.3% w/v) in 5mL that is, contains 10mmol magnesium in 5mL
Oral solution : 400mg/mL
ACTION & INDICATION:
Electrolyte supplement, pulmonary vasodilator. For magnesium deficiency. Persistent pulmonary hypertension of the newborn.(PPHN)
DOSE: Magnesium deficiency IV/IM: 0.2 - 0.4 mmol /kg /dose 12 hourly
( equivalent to 50 – 100mg/kg/dose)
Persistent pulmonary hypertension of the newborn IV: Loading dose: 0.8 mmol / kg (200 mg / kg) over 30 minutes
Maintenance dose: 0.08 - 0.3 mmol / kg / hour (20 – 75 mg/kg/hour) to maintain plasma magnesium concentration between 3.5 – 5.5mmol/L. May be used for up to 5 days.
PREPARATION: Infusion:
Diluent: 0.9% Sodium chloride or Glucose solutions Take 2.5 mL (5 mmol) and dilute to 50mL = 1 mmol in 10mL
May be further diluted if required.
Minimum dilutions: IV: Take 1mL 10mmol in 5 ml solution and dilute to 5mL = 0.4 mmol/mL IM: Take 1mL 10mmol in 5 mL solution diluted to 2.5mL = 0.8 mmol/mL
ADMINISTRATION: Intramuscular: As per NCCU policy. Intravenous – over 20 minutes Intravenous infusion
COMMENTS: Monitor magnesium levels. Range 0.75-1.2mmol/L PPHN : Levels to be 3.5 – 5.5 mmol/L Monitor blood pressure Use with caution with impaired renal function. May increase effects of neuromuscular blocking agent or respiratory depressants.
REFERENCES: BNF for Children 2007 Neonatal Pharmacopoeia 2nd Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: MEDIUM CHAIN TRIGLYCERIDES OIL (MCT)
PRESENTATION: Oil: 1mL = 35 kJ (8.3 kcal )
ACTION & INDICATION:
Mixture of triglycerides produced from medium chain fatty acids that are more easily digested and absorbed than conventional food fat.
Source of calories and as an adjunct to the dietary management of infant with disorders of fat absorption and transport.
DOSE : Initial dose:
1mL/kg/dose 8 hourly
ADMINISTRATION: Give diluted with feeds or as supplied in feeds by the milk room staff.
ADVERSE EFFECTS:
Gastrointestinal symptoms - diarrhoea, abdominal distension.
REFERENCES: Martindale 35th Ed
DATE: June 2008

DRUG: MEROPENEM
PRESENTATION: Vial: 500 mg
ACTION & INDICATION:
A carbapenem antibiotic, which is stable to human dehydropeptidase-1. It acts by interfering with bacterial cell wall synthesis and is used for the treatment of severe infections. It is active against a broad spectrum of aerobic and anaerobic bacteria.
DOSE: < 7 days 20 mg/kg/dose 12 hourly ≥ 7 days 20 mg/kg/dose 8 hourly
Meningitis : 40mg/kg/dose 8 hourly
PREPARATION: Use solution prepared in Pharmacy if available.
Diluents: Water for Injections, 0.9% Sodium chloride, Glucose solutions. Add 9.56mL diluent to vial: = 50 mg/mL
If more dilute solution required add 19.6mL diluent to vial:
= 25mg/mL
ADMINISTRATION: Intravenous infusion: Infuse over 30 minutes.
ADVERSE EFFECTS:
Thrombophlebitis Rash, pruritis, urticaria. Eosinophilia, thrombocytopenia, neutropenia.
COMMENTS: Refrigerate reconstituted solution.
Discard after 24 hours.
Discussion with Clinical Microbiologist is mandatory for suspected/proven meningitis therapy.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne Neofax 2006
DATE: June 2008

DRUG: METHYLDOPA
PRESENTATION: Oral Suspension: 25mg/mL (Prepared in Pharmacy).
ACTION & INDICATION:
A centrally acting antihypertensive agent.
DOSE: Starting dose: 2.5mg/kg/dose 8 hourly
Maximum dose: 15mg/kg/dose.
ADMINISTRATION: Oral: May be given at any time with regard to feeds.
ADVERSE EFFECTS:
Hypotension
Drowsiness
Drug induced fever
Can cause fluid and sodium retention, diuretic therapy may be necessary.
Positive Coomb's test
COMMENTS: Monitor blood pressure pre dose and 1/2 hourly post dose, continue until stabilised for 48 hours then twice daily.
U & E's at commencement and after any change in therapy.
REFERENCES: BNF for Children 2007
DATE: June 2008

DRUG: METHYLENE BLUE
PRESENTATION: Ampoule: 50mg in 5mL
ACTION & INDICATION:
A normally dormant reductase enzyme system is activated, which reduces methylene blue to leucomethylene blue, which in turn reduces methaemoglobin to haemoglobin.
Higher than recommended doses may accentuate methaemoglobinaemia.
For the treatment of drug-induced methaemoglobinaemia.
DOSE: 1-2mg/kg/dose
Dose may be repeated after one hour.
PREPARATION: May be diluted with Sodium chloride 0.9% if needed to aid administration.
ADMINISTRATION: Give IV over 5 minutes.
ADVERSE EFFECTS:
Blue green discolouration of urine/faeces
Nausea, vomiting, diarrhoea, abdominal pain
Hypertension
Cyanosis
Diaphoresis
May cause methaemoglobinaemia
Contraindicated in patients with G6PD deficiency and renal insufficiency.
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Women’s Hospital Melbourne
DATE: June 2008

DRUG: METRONIDAZOLE
PRESENTATION: Infusion: 500 mg/100 mL Oral suspension: 200 mg/5 mL
ACTION & INDICATION:
Antimicrobial agent used for treating infection (anaerobic or protozoal). May be used prophylactically.
DOSE: < 7 days : Initial dose : 15mg/kg then after 24 hours Maintenance : 7.5mg/kg/dose 24 hourly ≥ 7 days : Initial dose : 15mg/kg then after 12 hours Maintenance : 7.5mg/kg/dose 12 hourly
If ≥ 44 weeks : Maintenance dose : 7.5mg/kg/dose 8 hourly, commencing 8 hours after the loading dose of 15mg/kg.
ADMINISTRATION: Oral: Administer half to one hour before feeds. Intravenous; umbilical arterial: Infuse over 20 minutes
ADVERSE EFFECTS:
Leucopenia, monitor white cell count and differential. CNS effects, seizures (rare).
Peripheral neuropathy - discontinue immediately. Gastrointestinal effects.
COMMENTS: Discard IV bag immediately after use. Do not refrigerate intravenous solution.
REFERENCES: Neofax 2006 BNF for Children 2007
DATE: June 2008

DRUG: MICONAZOLE
PRESENTATION: Cream: 2% (20mg/g)
Ointment: Miconazole 2.5mg/g and (Daktozin) Zinc oxide 150mg/g
Oral Gel: 20mg/mL
ACTION & INDICATION:
Antifungal agent for the treatment of topical and oral fungal infections.
DOSE: Oral Gel: Apply approximately ONE centimeter of gel four times a day to mouth. Rub around gums and inside of mouth using a cotton bud or finger. Do not use a spoon to administer gel.
Cream: Apply twice daily
Ointment: Apply at each nappy change for at least seven days.
COMMENTS: Avoid contact with the eyes.
REFERENCES: APP Guide 2007
DATE: June 2008

DRUG: MIDAZOLAM
PRESENTATION: Ampoule: 15mg/3mL Oral Solution : 2.5mg/mL (2500 microgram/mL)
ACTION & INDICATION:
Midazolam is a short acting sleep-inducing agent for; • short procedures, • induction of anaesthesia and • for the prolonged sedation of ventilated patients. It enhances the central sedative effects of tranquillisers, narcotics, analgesics, and anaesthetics.
DOSE:
Oral: 200 - 500 microgram/kg/dose 4 - 8 hourly IV: Intermittent dosing: 100-200 microgram/kg/dose 4-8 hourly Continuous infusion: 1-2 microgram/kg/minute.
PREPARATION:
Use solution prepared in Pharmacy if available. Diluent: 0.9% Sodium chloride or Glucose solutions. For infusion: To give a dose of 1microgram /kg/min when infused at 1mL/hr Take 3mg of midazolam per kilogram of baby’s weight and dilute to 50mL . If a different concentration is required, refer to the Calculation of Drug Infusion table.
ADMINISTRATION:
Oral: May be given at any time with regard to feeds. Intravenous over at least 5 minutes. Intravenous infusion
ADVERSE EFFECTS:
Observe for apnoea, respiratory depression, obtundation, impaired conscious state.
COMMENTS:
May be used in conjunction with morphine. Antidote: Flumazenil (see monograph)
REFERENCES: Neonatal Pharmacopoeia 2nd Ed
DATE: June 2008

DRUG: MORPHINE SULPHATE
PRESENTATION: Ampoule: 1mg/mL (1,000 microgram/mL) Mixture: 1mg/mL (as hydrochloride)
ACTION & INDICATION:
Opioid analgesic Sedative to assist ventilation Management of opioid dependent infants with Neonatal Abstinence Syndrome
DOSE: DOSE MUST BE ORDERED IN MICROGRAMS Intermittent dose: 100-200 microgram/kg/dose 4-6 hourly Infusion dose: 10-40 microgram/kg/hour Neonatal Abstinence Syndrome: See NCCU guidelines at the back of this manual.
PREPARATION: Use solution prepared in Pharmacy if available. Ampoule contains 1000microgram in 1mL = 100 microgram in 0.1mL Infusion dilution : Dilute 500microgram (0.5mL) per kilogram of baby’s weight to 50mL with appropriate infusion fluid Infuse at 1mL/hour = 10 microgram/kg/hour Example: To prepare an infusion solution for a 780g baby Take 500 microgram (0.5mL) x 0.78 = 390microgram (0.39mL ) and dilute to 50mL with appropriate infusion solution Infuse at 1mL/hour = 10 microgram/kg/hour Compatible with glucose, Sodium chloride 0.9%, glucose/saline solutions.
ADMINISTRATION: Intramuscular: As per NCCU policy. Use undiluted. Intravenous injection: over 3-5 minutes, or Intravenous infusion Oral
ADVERSE EFFECTS:
Hypotension CNS depression, respiratory depression. Monitor respiratory and cardiovascular status
COMMENTS: Antidote: Naloxone (see monograph) If baby is has been on a morphine infusion for a least one week, wean morphine dose slowly
REFERENCES: Gomella: Neonatology 5th Ed Neofax 2006
DATE: September 2008

DRUG: MYLANTA
PRESENTATION: Oral suspension
Each 10mL contains: Magnesium Hydroxide 400mg Aluminium Hydroxide (dried) 400mg Simethicone 40mg
ACTION & INDICATION:
Antacid for the prevention and treatment of gastrointestinal haemorrhage.
DOSE : 0.5mL/kg/dose 4 hourly
ADMINISTRATION: Oral
ADVERSE EFFECTS:
Hypermagnesaemia - monitor serum magnesium with prolonged use.
COMMENTS: May decrease absorption of oral medications. Separate from other drug administration by two hours.
Refrigerate suspension. Discard 6 months after opening
REFERENCES: Paediatric Pharmacopoeia 13th Ed Royal Children’s Hospital Melbourne
DATE: June 2008