Embed Size (px)
Citation preview

Nayera Anwar
CHAPTER
7
Introduction, 56 Injurious agents, 56
Degeneration, 57 Accumulations, 58
Apoptosis, 61 Necrosis, 64
Miscellaneous types, 66 (Autolysis, autophagy, immune-
genic cell death, keratinization, mitotic catastrophe, anoikis, ex-
citotoxicity, paraptosis, pyropto-sis, necroptosis, autoschizis, en-
tosis, symplastic changes, cell ageing and Wallerian degenera-
tion) After effects of cell death, 68
Gangrene and pathologic calcifi-cation, 68
Clinical relevance, 68 ( Diagnostic role , predictor of
survival, guide to therapy, apop-tosis targeted therapy, arterial
embolization)
Outline
INTRODUCTION
The cells undergo a variety of changes when subjected to stress or injury, usually referred to
as retrogressive changes. The type of change is largely dependent on the degree and duration of
injury. Thus, mild injuries of short duration are unlethal and produce reversible changes called
degeneration. Conversely, severe injuries of long duration, result in irreversible damage, namely
cell death. In addition, a miscellaneous group of various retrogressive changes are reported with
overlapping features and mechanisms. Biochemi-cal and electron microscopic changes appear first
(Table 7-1). The microscopic and gross changes subsequently appear. In degeneration, apoptosis
and necrosis, the changes affect the biochemical structure of the cell itself. Conversely, in another
group of retrogressive change, namely: cell accu-mulation or infiltration, an abnormal material
accumulates intracellular or extracellular as a re-sult of genetic or metabolic disorder. The cellular
degenerative changes in this case are secondary to a pressure effect of the accumulated material.
Thus, both degeneration and accumulations are characterized by abnormal structural changes
and decreased functions. The present chapter reviews these cellular retrogressive changes and
their mechanisms.
INJURIOUS AGENTS
Cell injury may be attributed to intrinsic
(genetic) or extrinsic (environmental) factors. Intrinsic or genetic factors include gene muta-
tions or deficiency of functional proteins such as enzyme defects in inborn errors of metabo-
lism or accumulation of damaged DNA. Extrin-sic factors include: (1) hypoxia, is the most
common injurious agent, (2) free radicals which are two types: (a) reactive oxygen species, ROS
(superoxide O2−, hydrogen peroxide H2O2, hydroxyl radical-OH, nitric oxide NO, peroxy-
nitrite ONOO, halide reagent HOCl), and (b) non ROS radicals (CCl4 generates highly toxic
CCl3), (3) physical agents as ionizing radiation, (4) chemical agents (chemotherapeutic drugs
and toxins), (5) infections (bacteria, rickettsia, viruses and fungi), (6) immunologic agents
(hypersensitivity reactions, anaphylactic reac-tions and autoimmune diseases), (7) nutritional
deficiency, (8) ageing, and 9) idiopathic.

DEGENERATION
The Mechanism
A common initial cause of all types of degen-
eration is damage of cell membrane and mito-chondrial membrane (adenosine triphosphate,
ATP depletion). This results in a series of chang-es including: (1) failure of sodium-potassium
pump: lack of ATP interferes with generation of phospholipids essential for membrane integrity.
This results in damage to membrane pumps (sodium-potassium and calcium pump) with con-
sequent intracellular accumulation of sodium and depletion of potassium in the cell. The accumu-
lation of sodium in the cell results in increase in intracellular water to maintain iso-osmotic pump
(hydropic degeneration), (2) intracellular lactic acidosis: with continuous depletion in ATP, aer-
obic respiration fails, followed by switch to an-aerobic glycolysis. This results in rapid depletion
of glycogen, accumulation of lactic acid, lowering the intracellular pH with subsequent clumping in
nuclear chromatin, (3) failure of calcium pump: calcium influx within the cell, causes mitochon-
drial swelling and increased permeability, and (4) reduced protein synthesis: membranes of endo-
plasmic reticulum and Golgi apparatus swell up and ribosomes detach from rough endoplasmic
reticulum. Polysomes are degraded to mono-somes, thus dispersing ribosomes in the cyto-
plasm and alter their role in protein synthesis through disturbance in protein trafficking mech-
anism (that takes proteins from one location and targets them to a second location. Within Golgi,
proteins are modified and packaged into vesicles in the ER. A group of these vesicles fuse, and
form the cisterna. As the protein moves through the stack, it is modified by resident Golgi en-
zymes at specific locations in the apparatus. The-se modifications are important because they pro-
vide the signal that determines the final destina-tion of the protein whether to lysosomes or to
cell membrane). Release of lysosomal enzymes triggers biochemical changes (mucoid degenera-
tion). Depletion of protein synthesis occurs in Golgi apparatus as well. Thus, degeneration is
the accumulation of metabolites or other sub-stances in a cell damaged by preceding injury. Up
to this point, withdrawal of the injurious agent can reverse cell injury with cell recovery.
Ultrastructural Features The plasma membrane is intact with dimin-
ish and blunting of microvilli. There is swelling of mitochondria with formation of small phos-
pholipid-rich amorphous densities in mitochon-drial matrix due to calcium influx. Swelling of
endoplasmic reticulum and Golgi apparatus is observed with ribosomes detached from rough
endoplasmic reticulum. There are intracytoplas-mic myelin figures, derived from degenerating
membranes (cell membranes, mitochondrial membranes and lysosomal membranes), enclos-
ing water and dissociated lipoproteins between the lamellae of injured membranes. Cytoskele-
ton is aggregated and nucleus shows clumped chromatin (Table 7-1).
Pathologic Features
There are three morphologic forms of degener-ation:
1. Hydropic Degeneration. Also known as cloudy swelling is the initial event in all types of degen-
eration. The condition is best seen in organs with intense metabolic rate such as the liver,
kidneys and brain. The main pathologic feature is either formation of one large clear cytoplas-
mic vacuole (ballooning degeneration) or multi-ple small vacuoles (vacuolar degeneration). The-
se cytoplasmic vacuoles represent distended segments of the ER (P 7-1).
2. Hyaline Degeneration: This is a common de-
scriptive histologic term for the pathologic ap-
pearance of glassy, homogeneous, eosinophilic,
proteinaceous material that may be intracellular
or extracellular. Four examples of intracellular
hyaline degeneration are described: (1) proximal
renal tubular epithelial cells, (2) Mallory‟s bodies
in alcoholic liver which are hyaline aggregates of
intermediate filaments/hyaline aggresomes that
form in liver cells (aggresome, multiubiquitinat-
ed molecules formed when the capacity of the
proteasome is exceeded by the production of
aggregation-prone misfolded protein), (3) cyto-
plasmic Russell bodies are immunoglobulins
that escape intracellular degradation and can
gather in distended endoplasmic reticulum, and
form intracytoplasmic globules without block-
ing normal secretory pathways. Russell bodies
are observed in inflammatory and neoplastic
plasma cells (P 7-2), and (4) Dutcher bodies are
Cell Degeneration and Death 57

cytoplasmic immunoglobulin inclusions that
invaginate within the nucleus. Intranuclear
Dutcher bodies accumulate in macroglobuline-
mia and neoplastic plasma cells and in any cIg-
producing B-cell lymphoma (P 7-3). Extracellu-
lar hyaline examples include: hyaline degenera-
tion in leiomyoma (P 7-4), old scars, hyaline ar-
teriolosclerosis in hypertension and diabetes
mellitus, renal glomeruli in chronic glomerulo-
nephritis and corpora amylacea.
3.Mucoid Degeneration: Mucoid degeneration is a deposition of mucinous material in epithelial
and connective tissue in excessive amounts. It is a mucus like composed of proteins complexed
with mucopolysaccharides. Myxoid degenera-tion is a biochemical change that occurs in col-
lagen with pathologic weakening of fibrous tis-sue through the action of lysosomal enzymes.
Fibrous tissue collagen (type I), a fibrous pro-tein of complex helical structure, is changed to
acid glycosaminoglycans with fragmentation of collagen fibrils. Both epithelial and connective
tissue mucin stain by Alcian blue. However, epi-thelial mucin is periodic acid-Schiff (PAS) posi-
tive, whereas, connective tissue mucin is posi-tive with colloidal iron. Mucoid degeneration
may affect epithelium or connective tissue: (1) epithelial mucin: Catarrhal inflammation of mu-
cinous aero-digestive mem branes, mucocele in oral cavity and gall bladder, and mucinous tu
mors of ovary and gastrointestinal tract (P 7-5)
and (2) connective tissue mucin: myxoid changes in some tumors (e.g. myxomas, neurofibromas,
fibroadenoma, soft tissue sarcomas), myxoma-tous changes of dermis in myxedema, myxoid
changes in fibrous tissue of ganglion of joints (P 7-6).
ACCUMULATIONS
Accumulations may be intracellular or extra-
cellular. Stockpiled substances may be lipids, pro-tein, glycogen or pigment. There are four main
pathways of abnormal intracellular accumula-tions: (1) accumulation of normal constituents of
deranged cell metabolism as in steatosis, (2) pro-tein misfolding transport leading to accumulation
of abnormal proteins as in Parkinson‟s disease and Alzheimer‟s disease (3) accumulation of ab-
normal endogenous substances produced as a result of abnormal metabolism due to lack of
some metabolic enzymes. This occurs in lysoso-mal storage disease or inborn errors of metabo-
lism, and (4) inhalation or ingestion of indigesti-ble material with subsequent accumulation of
exogenous material due to lack of enzymatic mechanism to degrade the accumulated material
or transport them to other sites (exogenous pig-ments, anthracosis, asbestosis, silicosis, and
pneumoconiosis). Accumulations could be he-reditary or acquired. Degeneration is the ultimate
secondary effect of cell accumulation.
El-Bolkainy Surgical Pathology 58
Cell Content Degeneration Cell Death
Cell Membranes
Microvilli
Mitochondria
Intact
Diminished
Swelling
Disrupted and deposits
of myelin figures Lost
Vacuoles and deposits of calcium salts
RER
Ribosomes
Intact and swollen
Detached from RER
Lysis
Dispersed
Lysosomes Cytoskeleton
Nucleus
Intact Intact and aggregated
Condensed
Rupture Dispersed
Fragmentation or lysis
Table 7-1 Ultrastructure of Retrogressive Changes
RER, rough endoplasmic reticulum

Intracellular Accumulations
1. Lipid Accumulations is lipid degradation prod-
ucts in the cytoplasm of cells, which accumulate in lysosome bound vacuoles. These materials are
usually products of peroxidation of fat and may be lipofuscins, ceroid, or cholesterol. These lipid
particles accumulating in the cytoplasm of cells convert into complex, non-degradable products.
Lipid accumulation, also known as fatty changes or fatty degeneration, includes two subtypes :
a-Triglyceride accumulations; (steatosis, fatty met-amorphosis, fatty degeneration and fatty infiltra-
tion), occurs in hypoxic, toxic (CCl4, chloro-form, aflatoxins) or metabolic injury (alcohol,
obesity, diabetes and protein calorie malnutri-tion). It is seen mainly in cells involved in and
dependent on fat metabolism, mostly in liver and myocardial cells (P 7-7). Mechanism of fatty
changes of liver occur through one of following: (i) increased entry or synthesis of free fatty acids
in liver, (ii) decreased fatty acids oxidation into ketone bodies resulting in increased triglycerides,
(iii) increased α-glycerophosphate causing in-creased esterification of fatty acids to triglycer-
ides, and (iv) block in lipoprotein excretion. Fat-ty liver from chronic alcoholism is multifactorial.
b-Cholesterol accumulations: (i) xanthoma and xanthelasma (P 7-8), (ii) cholesteatosis, with fo-
cal accumulation of cholesterol laden macro-phages in gall bladder, and (iii) Niemann-Pick
disease type C, a lysosomal storage disease due to mutation in enzyme responsible for choles-
terol trafficking. 2. Protein Accumulations. These are due to bio-
chemical change in proteins or excessive accu-mulation of immunoglobulins synthesized in cis-
ternae of the rough endoplasmic reticulum of the plasma cells. Accumulations occur through dis-
turbance in protein trafficking mechanism. Pro-tein trafficking mechanism is as follows; proteins
from the rough endoplasmic reticulum are sent to the Golgi that takes proteins from one loca-
tion and targets them to a second location. With-in Golgi, proteins are modified and packaged
into vesicles in the ER. A group of these vesicles fuse, and form the cis-cisterna. As the protein
moves through the stack, resident Golgi enzymes at specific locations in the apparatus modify it.
These modifications are important because they provide the signal that determines the final desti-
nation of the protein whether to lysosomes or to cell membrane. The histology is charachterized
by protein accumulations present as hyalin, ho-mogeneous glassy eosinophilic cytoplasmic drop-
lets. Protein accumulates intracellular or extracel-lular. Intracellular variant occurs in; renal tubular
epithelium in diabetes, Mallory bodies in alcohol-ic liver, Russell bodies and Dutcher bodies in
plasma cell. 3. Glycogen Accumulations. These occur in some
diseases characterized by prolonged hyperglyce-mia such as diabetes mellitus or Cushing‟s dis-
ease (excess glucocorticoids), both are associated with defective glycogen or glucose metabolism,
thus, glycogen accumulates as clear cytoplasmic vacuoles in hepatocytes.
4. Pigment Accumulations. The pigment may be exogenous or endogenous in origin. Exogenous
indigestible pigments, such as carbon. Endoge-nous such as iron (usually due to overload, as in
hemosiderosis) or due to altered metabolism of breakdown products of melanin and hemoglo-
bin. There are three types of endogenous pig-ment: (1) melanin is the most common, and its
accumulation develops through defect in tyrosine metabolism. Melanin is granular protein contain-
ing pigment produced by melanocytes where its increased production occurs in association with
tumours of the melanocytes, excessive irradia-tion, and effect of sunlight, (2) haemoproteins
are derived from haemoglobin, cytochromes and their break down products. Haem-drived pig-
ments are “porphyrin, hemosiderin, acid hematin and bilirubin”. (i) Porphyrin accumulation is due
to inborn errors in porphyrin metabolism at-tributed to genetic deficiency of one of the en-
zymes required for haem synthesis. Porphyrin accumulation occurs in bone marrow or in liver
(erythropoietic or hepatic porphyrias), (ii) Hemo-siderin is iron pigment, encountered in trauma,
excessive hemorrhage or hemolysis. It accumu-lates in parenchymal cells (liver, pancreas, kidney,
and heart) or reticuloendothelial cells (the liver, spleen, and bone marrow). A common example
is hemochromatosis, where excess iron is stored in organs, leading to organ toxicity. Hereditary
hemochromatosis is an error of iron metabolism characterized by inappropriately high iron ab-
sorption resulting in progressive iron overload (P 7-9). Hereditary hemochromatosis occurs due to
HFE gene missense mutations, located at band 6p22. It leads to enhanced accumulation of iron
in liver, heart, pancreas, pituitary, joints, and skin. However, two other types of hemochromatosis
have been identified: juvenile hemochromatosis
Cell Degeneration and Death 59

or type 2 (gene HFE2), and an adult form de-fined as hemochromatosis type 3 (gene HFE3).
Regardless to the type of hemochromatosis, the histopathologic features are similar. Once the
toxic level of iron is reached, there is four times increased rate of liver phospholipid lipoperoxida-
tion, protein oxidation and cell damage. Excess iron is hazardous, because it produces free radi-
cals. These, can produce DNA cleavage, im-paired protein synthesis, and impairment of cell
integrity and cell proliferation, leading to cell in-jury and fibrosis, (iii) Acid hematin (non- iron
pigment), seen in chronic malaria and mis-matched blood transfusion and it accumulates in
macrophages and hepatocytes, and (iv) Bilirubin or haematoidin (non-iron containing pigment) -
following excessive hemorrhage or hemolysis, and failure of the liver to conjugate bilirubin into
bile, thus, bilirubin accumulates in hepatocytes and kupffer cells, and (3) lipofuscin, lipid derived
pigment „wear-and-tear pigment‟. It is a golden brown pigment seen in ageing particularly in liver
and heart or in debilitating diseases. It is break-down product of lipid peroxidation.
Extracellular Accumulations
The two major types of extracellular accumu-
lations are cholesterol and protein. which share a common mechanism leading to changes in quan-
tity and quality of normal components, as well as the appearance of abnormal materials. The etiol-
ogy may be either congenital defect or acquired pathology.
1. Cholesterol Accumulations: it is a distinct type of lipid accumulation, different from fatty accu-
mulation in which cholesterol accumulates extra-cellularly either due to disturbance of cholesterol
and cholesterol esters metabolism or due to dis-turbance in neutral fat metabolism causing depo-
sition of lipids and lipoproteins. LDL oxidation is regulated by enzyme lipoprotein associated
phospholipase A2(Lp-PLA2), which is an en-zyme linked to inflammation of blood vessels,
and free radicals in endothelium. The common-est example is cholesterol accumulations in ath-
erosclerosis in which plaque builds up inside ar-teries. Plaque is formed of fat, cholesterol, calci-
um, and other blood substances where cholester-ol and cholesterol esters accumulate as lipid vac-
uoles within intima of arteries and crystalize in the form of long needles and present morpho-
logically as clefts within tissues (P 7-10).
2. Protein Accumulations: includes amyloidosis, hyalinosis, myxoid accumulation and elastosis:
a- Amyloidosis; (P 7-11) is the extracellular variant of protein accumulation. It is deposits of
misfolded protein of variable causes as idio-pathic, myeloma (AL protein) and chronic in-
flammatory conditions as tuberculosis or rheu-matoid arthritis (AA protein). This abnormal pro-
tein is positive for Congo red and produces green birefringence on polarized light. Amyloidosis
causes pressure atrophy and degeneration of epi-thelium in affected organs with subsequent func-
tional failure. Mechanism: during proteins synthe-sis, some misfolded protein fragments are
formed which escape proteolysis by protease, they aggregate to form oligomers. The oligomers
aggregate together to make amyloid that inter-feres with proper organ function. The type of
protein that is misfolded and the organ or tissue in which the misfolded proteins are deposited
determine the clinical manifestations of amyloi-dosis. There are four types of amyloidosis: (i) my-
eloma-associated amyloidosis, occurs in multiple myeloma where up to 15% of patients may have
systemic deposits of amyloid, (ii) familial amyloi-dosis, as in Mediterranean fever, (iii) Alzheimer‟s-
associated amyloidosis, of ageing, and (iv) endo-crine amyloidosis, is a major component in me-
dullary thyroid carcinoma and pancreatic islets, associated with type 2 diabetes mellitus where the
precursor protein, termed islet amyloid or islet-associated polypeptide (IAPP) is secreted by
β−cells of the islets. b- Hyalinosis: which is accumulation of
pathological albumin (molecules composed of albumin, lipid, carbohydrates, and antibodies). It
is a complex structure variable in variable types of vascular hyalinosis: (i) simple, consists of pro-
tein only and it occurs in hypertension, (ii) lipo-hyalin (consists of proteins and lipids) which oc-
cur in diabetes mellitus, and (iii) complex (protein and immune complex) which occurs in rheumatic
fever, autoimmune diseases. Hyalinosis occurs in old scars, thrombi and wall of renal arterioles in
long standing diabetes mellitus, autoimmune dis-eases and chronic hypertension. Hyalinosis is the
finale of fibrinoid changes and necrosis. c- Myxoid accumulation: which is accumulation
of acid mucopolysaccharides. Diagnosed histo-logically by toluidin blue, PAS reaction.
d- Elastosis: may be actinic stimulation of fibro-blasts, promoting synthesis of elastotic material;
or that the material is a degradation product of
60 El-Bolkainy Surgical Pathology

collagen, elastin or both. The responsible gene is ELN gene, lies on chromosome 7 and en-
codes a protein that is one of the two compo-nents of elastic fibers. Deletions and mutations
in ELN gene are associated with supravalvular aortic stenosis and autosomal dominant cutis
laxa.
CELL DEATH
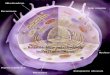
The five types of cell death are illustrated in (Figure 7-1) most important types are apoptosis
and necrosis. Comparison between the two types are illustrated in ( Table 7-2).
APOPTOSIS
Apoptosis is a Greek term means "falling
off" leaves of tree. It is a process of pro-grammed cell death that occurs in multicellular
organisms. Apoptosis is type I cell death which may be physiologic or pathologic. Physiologic Pro-
cesses: separation of finger webs in embryo, en-dometrial shedding, regression of lactating
breast, normal cell destruction followed by re-placement proliferation such as in intestinal
epithelium, and involution of the thymus in ear-ly age. Between 50 and 70 billion cells die each
day due to apoptosis in the average human adult. Pathologic Processes: which is due to: therapy
effect (radiotherapy, chemotherapy), cytotoxic T cell in immune mechanisms (graft- rejection re-
actions), progressive depletion of CD4+ T cells in the pathogenesis of AIDS, viral infections,
prostatic atrophy after orchiectomy, and neuro-degenerative diseases of CNS.
The Mechanism
Apoptosis is executed through the action of a family of 12 cytoplasmic enzymes, called
caspases, which cleave the protein of cytoskele-ton. They have been divided into two main clas-
ses, namely: initiator procaspases (caspase 1, 2, 4, 5, 8, 9, 11 and 12) and effector caspases
(caspase 3, 6 and 7). Initiator caspases initiate and propagate the apoptotic signal, whereas, ef-
fector caspases cleave cell proteins. Caspase 3 is the main caspase, which mediate apoptosis. It is
critical executioner of apoptosis, as it is either partially or totally responsible for the proteolytic
cleavage of many key proteins such as the nucle-ar enzyme poly (ADP-ribose) polymerase
Cell Degeneration and Death 61
Fig 7-1 Types of cell death. (A) Apoptosis. The cell shrinks, chromatin is condensed and fragmented, develops blebs, but cell membrane is intact. The resulting apoptotic sacs are phagocytosed by histiocytes. (B) Necrosis. The
cell swells, cell membrane rupture and cell organelles are indistinct. (C) Autophagy (self eating). The cell contains a prominent lysosomal vesicle which leads to autophagocytosis. (D) Paraptosis. The cell is normal in
size but contains multiple cytoplasmic vacuoles. (E) Autoschizis. The cell shrinks in size mainly due to loss of cytoplasmic mass.

(PARP), thus, activation of caspase 3 leads to the activation of other enzymes such as endonucleas-
es and proteases. Endonucleases induce the clas-sic internucleosomal DNA fragmentation of
multiple of 180 base pairs producing a character-istic ladder-like pattern by electrophoresis. Prote-
ases induce protein cross-linking and cell shrink-age. There are two main pathways to activate
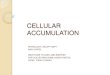
caspases, namely: the extrinsic or membranous, and the intrinsic or mitochondrial pathways (Fig
7-2).
The extrinsic apoptotic pathway recognizes and eliminates cells with foreign protein on their sur-
face. Examples include: (1) NK and cytotoxic lymphocytes expression of perforin and
granzyme B, (2) FAS-mediated elimination of autoreactive T-cells in the thymus, and (3) TNF-
α and death receptors. The procaspase 8 is acti-vated by these membrane signals.
The intrinsic pathway functions to eliminate se-
nescent or damaged cells of the organism, and caspases are activated by the liberation of cyto-
chrome c from the mitochondria to the cyto-plasm. Telomere shortening or any DNA dam-
age by anoxia, irradiation or mutation is sensed by the tumor suppressor gene TP53 which acti-
vates the proapoptotic genes (BAX and BAD) leading to the liberation of cytochrome c from
the mitochondria to the cytoplasm (Fig 7-2). Cy-tochrome c binds with the adapter protein Apaf-
1, and procaspase-9 to form an “apoptosome” complex, which activates caspases. It is paradoxi-
cal that cytochrome c, a most useful electron transfer agent in oxidative phosphorylation in
mitochondrion, becomes a deadly killer to the cell when released into the cytoplasm.
Apoptosis is under strict control by a variety of genes (Fig 7-2). BAX and BAD gene expressions
are proapoptotic, whereas, Bcl-2 and Bcl-x are antiapoptotic. NOXA, which inhibits Bcl-2, is
considered proapoptotic. These proteins act by affecting the permeability of mitochondrial
membrane to cytochrome-c. Thus, BAX in pres-ence of calcium ions increases mitochondrial
membrane permeability, a process blocked by Bcl-2.
Apoptosis is considered the physiologic mech-anism of choice to remove cells damaged by ag-
ing or genetic mutation, hence protection against cancer. Normal adult cells have only a limited
capacity of cell division.
The ends of chromosomes (telomeres) contain many copies of guanine (G)- rich repeats
(TTAGGG)N . The enzyme DNA polymerase is unable to replicate telomeres, which shorten by
about 100 base pairs with each division. This is referred to as the end replication problem. When
DNA shortening reaches a critical level after 50 divisions, it is sensed by TP53 as a DNA break,
resulting in expression of p21 and Bax with per-manent arrest of cell cycle (cell senescence) and sub-
sequent apoptosis. In this way, telomeres may be considered as death timers. The enzyme telomer-
ase can correct telomere shortening (Chapter 2). Germ cells, stem cells and malignant cells are
rich in telomerase, hence they are immortal. Con-versely, normal somatic cells lacking this enzyme
are short-lived.
Role of Apoptosis in Carcinogenesis Generally, the mechanisms by which evasion
of apoptosis occurs can be broadly divided into: (1) disrupted balance of pro-apoptotic and anti-
apoptotic proteins, (2) reduced caspase function, and (3) impaired death receptor signaling.
Morphologic Features
1. Ultrastructural Features: there is extensive plasma membrane blebbing, but with maintained
integrity until the final stages of the process, apoptotic bodies (near spherical bodies, com-
posed of cytoplasm and condensed organelles, with or without nuclear fragments), nuclear
shrinkage (pyknosis), nuclear fragmentation into two or more fragments (karyorrhexis), chromatin
condensation, chromosomal DNA fragmenta-tion, and global mRNA decay. It is worthy to
mention that early phases of apoptosis do not affect membrane permeability, nor do they alter
mitochondrial activity (Table 7-2, P 7-12). 2. Histopathologic Features: apoptotic cells ap-
pear as round to oval shrunken cell of intensely eosinophilic cytoplasm containing pyknotic nu-
cleus with condensed chromatin (Fig 7-1A and P 7-13). Apoptosis is not associated with any in-
flammation since apoptotic cells do not break and release their cell contents. Also, apoptotic
cells are immediately phagocytosed by surround-ing cells, thus, escaping necrosis, and these phag-
ocytes do not produce anti-inflammatory cyto-kines. In general, the light microscopy approach
can provide both qualitative and quantitative data (Table 7-2).
62 El-Bolkainy Surgical Pathology

Cell Degeneration and Death 63
Feature Apoptosis Necrosis
Pathobiology
Etiology Genetically determined (suicidal) Accidental (homicidal)
Nature Physiologic or pathologic Pathologic
Mechanism Mitochondrial membrane
permeability Cell membrane damage
Trigger pathway
DNA breakdown
Intrinsic or extrinsic
Internucleosomal
Extrinsic
Random
Degrading
enzymes
Caspases Non-caspase
Caspase inhibtors* Present Absent
ATP Sustained Lost
Cell Morphology
Cell death
Single cells
Groups of cells
Cell size Shrinkage Swelling initially
Cell membrane Intact Ruptured
Cell contents Present Released
Nucleus Fragmentation Lysis
Apoptotic bodies Lysosomes
Present Intact
Absent Breakdown
Inflammation Absent Always present
Table 7-2 Comparison of Apoptosis and Necrosis
Fig 7-2 The two pathways of apoptosis. The extrinsic pathway is a reaction to foreign protein, whereas, the intrinsic pathway is a programmed cell death to eliminate senescent or DNA damaged cells. The enzymes
caspases play a major role in both pathways.
* Includes : (zVAD, FmK, p53, BAF), Xiap and Bcl-xL

64
Detection Techniques
These can be grouped into four main
groups, namely:
1. The immunohitochemical techniques: These detect
apoptosis by using antibodies which recognize activated caspase-3, caspase-cleaved cytokeratin
18 or TUNEL assay.
(a) Cleaved Caspase 3: detection of activated caspase-3 is an easy, sensitive, and reliable meth-
od for detecting and quantifying apoptosis. It is a specific tool for identifying apoptotic cells in tis-
sue sections, even before all the morphological features of apoptosis occur.
(b) Cleaved Cytokeratin 18 (CK18): during apop-tosis, CK18 undergoes dramatic reorganization
and is cleaved by the caspases (caspase-3, -6, -7 or -9), generating an apoptosis-specific neo-
epitope recognized by the monoclonal antibody M30 (MAb M30). C-K18 is expressed in carcino-
mas such as lung, liver, prostate, breast and co-lon, but absent in lymphoid, bone marrow and
neuronal cells (P 7-14). (c) TUNEL Assay: The terminal deoxynucleo-
tidyl transferase (TdT)-mediated dUTP nick-end labeling (TUNEL) technique has been used for
the detection and quantification of late apoptosis in histological tissue sections (P 7-15). It is time-
consuming and needs numerous cells to be ex-amined and is associated with a number of tech-
nical problems. 2. Apoptotic index: is determined by the number
of apoptotic cells per 1000 tumor cells or the number of apoptotic cells per 10 high-power
fields. This could be assessed by computer-assisted image analysis. Apoptotic index has been
shown to be of clinical and biological relevance in breast carcinomas, hepatocellular carcinoma,
renal cell carcinoma, prostatic carcinoma, laryn-geal carcinoma, and cervical carcinoma. Accurate
detection of apoptosis in various stages help in assessing apoptotic index, which is known to be
a predictor of chemotherapy response and is an indicator of prognosis and metastasis thereby
predicts outcome of the treatment. 3. Flow Cytometry (FCM); is applied by using
labeled annexin, which is Annexin V in conjunc-tion with fuorescent dye (DNA marker) such as
propidium iodide (PI). Thus, combination of the two can be used to monitor the progression of
apoptosis: early-stage apoptosis shows annexin expression whereas; late-stage apoptosis and cell
death show both annexin and PI expression. Other flow cytometric fuorescent dyes include
propidium iodide (PI) and DAPI staining (4,6-diamidino-2-phenylindole) , however, it is not
highly specific. 4. DNA-Ladder electrophoresis assays; the princi-
ple is to demonstrate the Apoptotic DNA frag-mentation in the DNA of treated cells.
NECROSIS
Persistent effect of injurious agent, results in
irreversible damage or point of no return and cell death. Irreversible cell injury is characterized by
severe damage of three vital cell systems: (1) irre-versible mitochondrial damage, (2) severe dam-
age of the membranes (cell membrane, mito-chondrial, and lysosomal), and (3) Damage of
genetic apparatus (DNA and RNA).
The Mechanism
The mechanism of cell death is mainly through excess calcium influx that causes cell
injury through several mechanisms: (1) mito-chondrial damage: due to excess calcium influx
where calcium collects in the mitochondria disa-bling its function, (2) Severe membrane damage:
is due to activated phospholipases and is accom-plished by: (a) either decreased mitochondrial
phospholipid synthesis or increased phospholip-id breakdown due to calcium overload, (b) acti-
vation of endogenous phospholipases which de-grade membrane phospholipids, (c) activation of
intracellular proteases, break down both mem-brane and cytoskeletal proteins, and (d) reactive
oxygen species that trigger lipid peroxidation and cause phospholipid depletion, (3) lysosomal
membrane damage: due to activated lysosomal hydrolytic enzymes by oxygen depletion in the
cell and acidic pH. Activation of hydrolytic en-zymes (e.g. hydrolase, RNAase, DNAase, prote-
ase, glycosidase, phosphatase, lipase, amylase, cathepsin etc) induces enzymatic digestion of
cellular components and hence cell death, and (4) nuclear damage: is due to activation of endo-
nuclease. Finally, the cell dies by necrosis, invari-ably associated with inflammation and ends with
autolysis. The enzymes that digest the necrotic cells are derived from lysosomes of the dying
cells or from lysosomes of leuckocytes (induced as a component of inflammatory reaction).
Estimation of the elevated serum lysosomal en-zymes (glutamic oxaloacetic transaminase
(SGOT), lactic dehydrogenase (LDH), isoen-zyme of creatine kinase (CK-MB), and cardiac
troponins (cTn) may be used as clinical parame-
El-Bolkainy Surgical Pathology

65 Cell Degeneration and Death
ters of cell death.
Morphologic Features 1. Ultrastructural Features: There is nuclear
lysis. Plasma membranes appear discontinuous and may show rupture. This discontinuous mem-
brane is caused by cell blebbing and the loss of microvilli. There are evident myelin figures
(phospholipids derived from damaged cell mem-branes), and indistinct organelles (Fig 7-1B).
There is marked dilatation of mitochondria showing large flocculent, amorphous densities
(formed of calcium salts) in mitochondrial matrix (Table 7-1 and Table 7-2).
2. Histopathologic Features: The nuclear chang-
es in necrosis are determined by the manner in which its DNA breaks down: (a) Pyknosis, is
shrinkage, condensation and clumping of nucleus which becomes dark basophilic, (b) karyorrhex-
is, the shrunken nucleus fragments into small dispersed bits, and (c) karyolysis, is dissolution of
the nucleus due to the loss of the DNA by deg-radation. The two main features of cell necrosis
are: nuclear staining (usually negative) and evi-dence of inflammation and damage in surround-
ing tissues. Based on etiology and morphologic appearance, there are six distinctive morphologic
patterns of necrosis: coagulative, liquefactive, caseous, fat, fibrinoid and hemorrhagic necrosis:
Coagulative Necrosis
This is the most common type of necrosis caused by sudden cessation of blood flow,
(ischemic necrosis), and less commonly due to bacterial and chemical agents. It is necrosis of
portion in some organs as heart, kidney, adrenal and spleen in which the architecture of the tis-
sue is maintained, and can be observed by light microscopy. Coagulation occurs as a result of
protein denaturation, causing albumin to trans-form into a firm and opaque state. Gangrenous
necrosis can be considered a type of coagulative necrosis, characterized by ischemia of lower
limb and the gastrointestinal tracts with super-imposed infection
Histopathologic features; the cellular outlines are retained for a long time but their cytoplasmic and
nuclear details are lost. The necrotic cells are swollen and have eosinophilic cytoplasm, at-
tributed in part to the loss of cytoplasmic RNA and in part to denatured cytoplasmic proteins (P
7-16).
Liquefactive Necrosis Liquefactive necrosis is characterized by the
digestion of dead cells to form cystic spaces. It is encountered in suppurative inflammation and
brain infarcts. Because brain has high amounts of digestive enzymes and lipids, cells therefore
can be readily digested by their own enzymes. Histopathologic features; There are necrotic dead
leukocytes (pus), surrounding wall is formed by histiocytes, inflammatory cells with proliferating
capillaries and fibroblasts (P 7-17).
Caseous Necrosis
Caseous necrosis is a distinct type of coagula-tive necrosis with esinophilic granular appearance
(Dead cells disintegrate but are not completely digested, leaving granular particles). Caseous ne-
crosis is typically caused by mycobacteria (tuberculosis) due to cytotoxic effect of lipopoly-
saccharides present in the capsule of the tubercle bacilli.
Histopathologic features: Granuloma center shows areas of necrosis, formed of structureless
eosinophilic material having amorphous granular debris. Necrosis is rimmed by elongated radially
arranged epithelioid cells (modified elongated macrophages having slipper-shaped vesicular nu-
clei), fibroblasts, lymphocytes, histiocytes and Langhans giant cells (P 7-18).
Fat Necrosis Fat necrosis may be due to traumatic or enzy-
matic factors. It results from the action of acti-vated lipases on fat-rich anatomic location such
as breast, pancreas and mesenteric fat respec-tively (P 7-19). Enzymatic fat necrosis is ob-
served in peritoneal cavity after acute pancreati-tis because the released lipases cause hydrolysis
and rupture of adipocytes and release of neutral fat that changes into glycerol and free fatty ac-
ids. The leaked out free fatty acids complex with calcium to form calcium soaps (saponification)
and dystrophic calcification.
Fibrinoid Necrosis
Fibrinoid necrosis is a special form of necro-sis caused by immune-mediated vascular dam-
age. This occurs when complexes of antigens and antibodies are deposited in the walls of ar-
teries. These “immune complexes,” together with fibrin that has leaked out of vessels, result
in a pink filamentous structure or network

66
called fibrinoid. Histopathologic features: fi-brinoid necrosis is identified by bright eosino-
philic, hyaline-like deposition in the arterial wall. Necrotic focus is surrounded by nuclear debris
of neutrophils (P 7-20). .
Hemorrhagic Necrosis Hemorrhagic necrosis is necrosis associated
with hemorrhage. Hence, it is common in high-ly vascular organs such as the spleen and intes-
tine due to blockage of arterial and venous drainage of the affected organ. It may result
from vascular occlusion (volvulus) or non-occlusive intestinal infarction. In spleen, it is
due to embolism (splenic infarction), which is typically triangular in shape grossly.
Histopathologic features: there is diffuse hemor-rhage in intestinal mucosa, engorgement of mu-
cosal and submucosal veins with some fibrin thrombi in capillaries of necrotic mucosa (P 7-
21).
MISCELLANEOUS RETROGRESSIVE CHANGES
A heterogeneous group of retrogressive changes some have special features and represent special types of apoptosis and others have their
own mechanism of action.
Autolysis Autolysis (i.e. self-digestion) is total disintegra-
tion of the cell by its own hydrolytic enzymes generated and liberated from lysosomes. It is
encountered in vascular occlusions or as a post-mortem change or when tissue biopsy is re-
moved from the body and left unfixed. Autolysis is fast in tissues rich in hydrolytic enzymes such
as in the pancreas, and gastric mucosa; interme-diate in heart, liver and kidney; and slow in fi-
brous tissue. Autolysis is identified pathologically as homogeneous eosinophilic cytoplasm with
loss of cellular details and remains of cell debris (P 7-22).
Autophagy Autophagy (self eating) is classically observed
in starvation. Biochemically, autophagy is caspa-se-independent with increased lysosomal activity.
Autophagic cell contains massive autophagic vacuolization of the cytoplasm, prominent lyso-
somal vesicle and absent chromatin condensa-tion (Fig 7-1C). Detection methods include: elec-
tron microscopy, protein-degradation assays, as-says for marker-protein translocation to au-
tophagic membranes, but no DNA laddering.
Immunogenic cell death (ICD) Immunogenic cell death or immunogenic
apoptosis is a form of cell death caused by cyto-static agents such as anthracyclines, or radiother-
apy and photodynamic therapy (PDT), bacteria and viruses. Injury produces structural modifica-
tion of proteins and rendering them antigenic. The best example of immunogenic cancer cell
death is methotrexate therapy in gestational cho-riocarcinoma. Unlike normal apoptosis, immuno-
genic apoptosis of cancer cells can trigger an an-titumor immune response through activation of
dendritic cells (DCs) and consequent activation of specific T cell response. Most of the agents
inducing immunogenic cell death are targeting endoplasmic reticulum (ER), leading to ER stress
and production of reactive oxygen species (ROS). Both ER stress and ROS have a role in
regulating the immunogenicity of dying cancer cells. ICD is characterized by secretion of dam-
age-associated molecular patterns (DAMPs). These DAMPs are translocated after the induc-
tion of immunogenic apoptosis to the surface of dying cell where it functions as an “eat me” sig-
nal for professional phagocytes.
Keratinization Keratinization represents both: (1) a terminal
differentiation of stem cells and epidermis ending in a process of apoptosis and exfoliation and (2)
elimination of cytosolic organelles. It leads to the formation of corneocytes by protease activation.
Keratinization of squamous epithelium, both normal and neoplastic, is a biologic process that
terminates in apoptosis, hence, the term terminal differentiation. Cleaved CK18 immunohisto-
chemistry is conclusive for apoptosis. Cornifica-tion is exclusive to the eyes.
Mitotic Catastrophe
This denotes abnormalities in cell cycle, which explain a mechanism of a delayed mitotic-linked
cell death. It results from defective cell cycle check points or damage to microtubules leading
to aberrant chromosomal segregation. The main causes are chemotherapy and ionizing radiation.
Mitotic catastrophe is caspase-independent (at early stage) and shows abnormal CDK1/cyclin B
activation. The common detection methods in-clude: electron microscopy and assays for mitotic
El-Bolkainy Surgical Pathology

Cell Degeneration and Death 67
markers (mitotic phosphoprotein 2 (MPM2). Mitotic catastrophe produce three outcomes
namely: (1) aneuploid cells with malignant potential, (2) multinucleated giant cell (P 7-23), a result of en-
domitosis (nuclear division without cytoplasmic division) this results in a sterile multinucleated
giant cells, (3) Micronuclei which result if small fragments of chromosomes fail to segregate dur-
ing telophase (P 7-24). Multinucleated giant cells, as well as, cells with micronuclei are sterile non-
dividing cells that will ultimately die.
Anoikis
Anoikis (means, to be homeless). It is a type of programmed cell death almost identical to
apoptosis except in its induction. It is induced by a loss of correct cell/extracellular matrix attach-
ment. Cells require intact integrin family recep-tors to suppress anoikis, and the process requires
mitochondrial integrity. Metastatic cells are re-sistant to anoikis and often have increased levels
of the death receptor-inhibiting protein FLIP.
Excitotoxicity Excitotoxicity is the pathological process
by which nerve cells are damaged or killed by excessive stimulation by neurotransmitters such
as glutamate. This occurs when receptors for the excitatory neurotransmitter glutamate (glutamate
receptors) are over activated by glutamatergic storm. Excitotoxins bind to these receptors.
Pathologically high levels of glutamate, can cause excitotoxicity by allowing high levels of Ca2+ in-
flux into cells with subsequent mitochondrial damage, thus, activates a number of enzymes
(phospholipases, endonucleases, and proteases such as calpain). These enzymes damage some
cell structures (cytoskeleton, membrane, and DNA). Excitotoxicity may be involved in spinal
cord injury, hearing loss (through ototoxicity), multiple sclerosis, Alzheimer's disease and Park-
inson‟s disease.
Paraptosis Paraptosis is a type of programmed cell death,
morphologically distinct from apoptosis and ne-crosis. It presents as multiple cytoplasmic vacu-
oles (Fig 7-1D). Paraptosis lacks several charac-teristics of apoptosis: (1) it is independent of
caspase activation, and (2) it lacks apoptotic mor-phology such as membrane blebbing, chromatin
condensation, and nuclear fragmentation. Several cancer drugs that can avoid many harmful side
effects of traditional chemotherapy could induce parapotosis.
Pyroptosis
Pyroptosis is a programmed cell death observed in cells infected by microbes. Unlike paraptosis,
pyroptosis involves activation of caspase-1. The cell is normal in size but contains multiple cyto-
plasmic vacuoles.
Necroptosis Necroptosis occurs in viral infections (ligation
of viral protein to TNFR1). It resembles necrosis morphologically and apoptosis in its mechanism
(programmed cell death). It resembles necrosis in being: caspase- independent, associated with re-
lease of reactive oxygen species (ROS), lysoso-mal membrane injury, cell membrane damage
and associated inflammation. Necroptosis is con-sidered the most understood form of regulated
or programmed necrosis.
Autoschizis Autoschizis is a term derived from the Greek
language, which means, "split itself". It describes a unique form of cell death induced during can-
cer treatment by ATP depletion (Fig 7-1E). The cell shrinks in size due to the loss of cytoplasmic
mass without loss of cell organelles. Only the nucleus and organelles remain surrounded by a
thin rim of cytoplasm. There is mitochondrial condensation as well as morphologic degradation
of the nucleus and nucleolus without the for-mation of apoptotic bodies and destruction of
the cell membrane. Thus, autoschizis shows both apoptotic and necrotic morphologic characteris-
tic.
Entosis Entosis was originally described as a form of
„cellular cannibalism‟ in lymphoblasts from pa-tients with Huntington's disease, in which one
cell engulfs one of its live neighbors, which then dies within the phagosome through lysosomal
degradation. Entosis is not inhibited by Bcl-2 or Z-VAD-fmk.
Symplastic Changes
This denotes a deformed shape, and is ob-served in nuclei of some soft tissue and endo-
crine tumors. It is characterized by large pleo-morphic hyperchromatic nuclei that characteristi-
cally lack mitotic activity (P 7-25). This phenom-

68
-enon is probably the result of disturbed cell cycle with DNA synthesis without mitosis
(unsynchronized cycle) resulting in hyperploidy. The ultimate fate of such abnormal cells is most
probably degeneration and death.
Cell Ageing Cell ageing or senescence is the impaired ability
of the cell to undergo replication or repair. Cellu-lar ageing result from a combination of several
factors including: (1) increased cell damage, (2) reduced ability of DNA repair, (3) impaired
chaperone and proteasome functions (defective protein homeostasis), and (4) reduced capacity of
cells to divide secondary to progressive shorten-ing of chromosomal ends, namely the telomeres.
Ubiquitin is a stress protein that directs intra-cellular protein molecules for either degradation
or synthesis. An age-related impairment of ubiq-uitin-dependent proteolysis results in enhanced
accumulation of abnormal damaged-cytotoxic proteins. This mechanism is associated with neu-
rodegenerative disorders including Alzheimer‟s and Parkinson‟s disease. It is noteworthy that
damaged and aggregated proteins are turned over by two proteolytic pathways: ubiquitin- pro-
teasome system and autophagy.
Wallerian Degeneration Wallerian degeneration occurs in nervous sys-
tem, in which part of a neuron or axon degener-ates without affecting the main nerve cell body.
This term describes degeneration of cell process-es only (incomplete degeneration), (P 7-26).
AFTER EFFECTS OF CELL DEATH
Gangrene: Gangrene is defined as ischemic necrosis with
super-added putrefaction, as a result of vascular occlusion. There are three main types of gan-
grene dry, wet and gas: (1) Dry gangrene. It results from arterial occlusion and common causes in-
clude: atherosclerosis, Burger disease and diabe-tes with affection of foot. A line of separation
marks the junction of viable and gangrenous tis-sues. (2) Wet gangrene. It results from simultane-
ous occlusion of both arteries and veins supply-ing the tissues. Common sites affected include
the small intestine (volvulous or mesenteric vas-cular occlusion) and lung infarcts. The line of
demarcation is indistinct between viable and gan
grenous tissues. Any case of dry gangrene can progress to wet gangrene if there is secondary
bacterial infection (C. Perfringens). (3) Gas gan-grene is a special form of wet gangrene caused by
gas forming clostridia.
Pathologic Calcification Pathologic calcification is deposition of calci-
um salts in tissues other than osteoid or enamel. It is of two types: dystrophic and metastatic cal-
cification. (1) Dystrophic calcification is characterized by deposition of calcium salts in dead and degen-
erated tissues with normal calcium metabolism and normal serum calcium level e.g. in caseous
granuloma, infarction, dead parasites, severe ath-erosclerosis, old scars and in some tumors
(papillary thyroid tumors, serous papillary ovari-an carcinoma, breast carcinoma). The mecha-
nism of calcium deposition in dystrophic calcifi-cation is increased binding of phosphates with
degenerated and dead tissues, which in turn bind to calcium forming calcium phosphate deposits.
(2) Metastatic calcification is caused by hypercalcae-mia which is encountered in : hyperparathyroid-
ism and pathologic bone destruction (myeloma, metastasis). The condition is reversible and
commonly affects kidney, stomach and lung due to change in pH at these sites.
CLINICAL RELEVANCE
The various retrogressive phenomena dis-
cussed in this chapter have important clinical applications, particularly in oncology, both diag-
nostic and therapeutic. The following is a short account of the main uses.
Diagnostic Role of Necrosis
Necrosis is helpful in: (1) differentiation be-tween caseous granuloma (TB) and non caseous
granulomas (sarcoidosis), (2) typing and grading of astrocytoma where necrosis is a feature of
glioblastoma, and (3) necrosis has an essential diagnostic criterion in some soft tissue sarcomas
as leiomyosarcoma and GIST. Grading of Therapy Effect
Histopathological grading of neoadjuvant chemotherapy effect in resected specimens is
usually applied in patients with osteosarcoma or breast carcinoma. In osteosarcoma, a 3-tiered
grading system is used (Picci et al, 1985) based on the extent of tumor necrosis. Thus grade I.
El-Bolkainy Surgical Pathology

69 Cell Degeneration and Death
<50% necrosis, Grade II. 50 – 80% necrosis, and grade III. > 80% necrosis, indicating a good
therapeutic response. In breast cancer, a 5-tiered grading system is used (Ogston et al, 2003) which
depends on quantitation of residual tumor tissue after therapy. Thus, grade I shows no tumor cell
loss (a poor response), grade II minor cell loss (<30%), grade III moderate cell loss (30-90%),
grade IV marked cell loss (only microscopic re-sidual tumor cell) and grade V 100% cell loss, no
viable tumor cells, denoting complete therapy response.
Also, therapy effect is graded according to percent of necrosis in other tumors nephroblas-
toma, germ cell tumors and the primitive neu-roectodermal tumors (PNET/Ewing‟s).
Prediction of Survival
Post chemotherapy tumor necrosis is a power-ful predictor of survival in patients with skeletal
osteosarcoma and the primitive neuroectodermal tumors Ewing‟s/PNET. Data are more conflict-
ing regarding the prognostic significance of ne-crosis in other soft tissue sarcomas. This is relat-
ed in part to the greater heterogeneity of soft tissue subtypes and to the inherent necrosis asso-
ciated with high-grade sarcomas unrelated to therapy effect. Therapy response is graded based
on percentage of necrosis in Ewing‟s/PNET and percentage of acellular osteoid in osteosarcoma.
Tumors with at 95% or more necrosis have a superior prognosis.
Guide to Therapy
Necrosis is a guide to therapy; (1) poor thera-py response in Ewing‟s is indicative of postop-
erative radiotherapy, (2) complete therapy re-sponse in low risk nephroblastoma patients
(good responders; 100% necrosis), is indicative of no postoperative chemotherapy and (3) com-
plete therapy response in germ cell tumors (100% necrosis), is indicative of no postopera-
tive chemotherapy.
Apoptosis Targeted Therapy
Both chemotherapy and radiotherapy kill can-cer cells by apoptosis. Accordingly, the aim of
targeted therapy in this case is to enhance apop-tosis in the tumor. This is accomplished by the
following different strategies: 1) to restore wild p53 in tumor through gene therapy hence, re-
storing normal p53 apoptotic action, 2) targeting mutated p53 in tumor cells by introducing a ge-
netically engineered adenovirus, leading to selec-tive destruction of tumor cells, 3) caspase–based
targeted therapy to activate these apoptosis in-ducing enzymes and 4) targeting the antiapoptot-
ic gene Bcl-2, through silencing its expression and 5) inhibition of expression of the prolifera-
tion promoting gene (survivin). These approach-es are currently under trial in patients with leuke-
mia, hepatocellular carcinoma, small cell lung cancer, lymphoma and melanoma.
Arterial Embolization
The rationale behind embolization therapy is to occlude the feeding vessel of a tumor, hence,
induce its necrosis with minimal harmful effect on surrounding normal cells. Microspheres of
microscopic size (1 nm to 1 mm) made of glass or resin are used as emboli. To enhance their
effect, microspheres may contain a chemothera-peutic agent (chemoembolization) or radioactive
mat e r i a l suc h as y t t r i um – 9 0 (radioembolization). Palliative arterial emboliza-
tion is used in hepatic, head and neck, as well as brain tumors. A favourable response rate was
reported in about 34% of cases.
REFERENCES
Archana M, Bastian, Yogesh TL, Kumaraswamy KL: Various methods available for detection
of apoptotic cells- A review- Indian J Cancer. Date of Web Publication 23- Sep-2013
Kroemer G, Galluzzi L, Vandenabeele P,
Abrams J, Alnemri, ES, Baehrecke EH et al: Classification of cell death: Recommendations
of the Nomenclature Committee on Cell Death (NCCD) 2009. Cell Death and Differ.
16 (1); 3-11, 2009
Mohan H: Cell Injury, Cellular Adaptations and
Cellular Ageing, Chapter 2 in Textbook of Pathology, 7th ed. The Health Sciences Pub-
lishers. New Delhi, 2015
Ogston KN, Miller ID and Payne: A new histo-
logical grading system to assess response of breast cancer to primary chemotherapy.
Breast, 12: 320-327, 2003
Picci P, Bacci G and Campanacci: Histologic evaluation of necrosis in osteosarcoma induced
by chemotherapy, regional mapping of viable and non-viable tumor. Cancer, 56: 1515-1521,
1985
Robbins and Cotran: Cellular Responses to Stress
and Toxic Insults: Adaptation, Injury, and

70
Death, Chapter 2, in Pathologic Basis of Dis-ease, 9th ed. Elsevier Saunders, 2015
Saadat YR, Saeidi N, Vahed SZ, Barzegari A, and Barar J: An update to DNA ladder assay
for apoptosis detection. Bioimpacts. 5 (1): 25-28, 2015
Wong R SY: Apoptosis in cancer: from patho-genesis to treatment. Journal of Experimental
and Clinical Cancer Research. 30:87, 2011.
El-Bolkainy Surgical Pathology