Embed Size (px)
Citation preview

Navpreet Sahsi

“ED Doc to Bed 9”


- Sent from Pre-admission clinic because of ECG findings
- “I feel fine, I don’t know what the big deal is!”
- Asymptomatic, resting comfortably- Obese, 50 years old, male. - Meds: Spironolactone, lisinopril- T- 36.7, HR 70, BP – 205/118, RR 12, 96 %
RA- Thoughts?

“Oh, and by the way I have these bilateral adrenal tumors.”
Chart shows a recent diagosis of bilateral adrenal tumors -> hypercortisolemia
Does this change anything?


What are the “classic” ECG manifestations of pheochromocytoma???

No “classic” ECG Often present with ST elevation in a variety of
patterns, mimicking acute infarction Can also present with other ST-T changes, most
commonly T wave inversions QTc often prolonged – risk of arrythmias Case series – 25 patients with eventual
diagnosis of pheo – 17 had abnormal ECG findings, 6 had initial diagnosis of acute STEMI - > urgent angiography - > all were normal
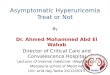
Cardiovascular Manifestations of Pheocromocytoma.AM J Em Med, 18:5; 622-629: 2000. ECG manifestations of endocrine disease. Heart 2001, 86; 679.



Copyright ©2001 BMJ Publishing Group Ltd.
DONCKIER, J. E et al. Heart 2001;85:679


Peaked T waves P wave flattening, PR prolongation, eventual
loss of p waves QRS widening Sine wave appearance



Depression of T waves ST depression (> 0.5 mm) Appearance of U waves



Sinus brady Low voltage complexes Prolonged pr and qt intervals Flattened or inverted T waves
Pericardial effusions occur in 30% of patients and may account for some of the changes

Sinus Tach – 40 % A. Fib – 10 – 22 % Nonspecific ST-T abnormalities – 25 % Interventricular conduction disturbances –
LAFB most common – 15 %


Shortenes plateau phase (phase 2) of action potential and shortens effective refractory period
ST shortening Short QT interval




T < 35.0 Tremor arifact
◦ One of earliest signs – secondary to shivering Slowing of sinus rate - > bradycardia Prolongation of PR and QT intervals Osborn/J wave

“Camel Hump sign” Extra deflection off of terminal portion of
QRS and ST segment takeoff Size correlates directly with degree of
hypothermia Usually present when temp < 32.0 deg. C Can occur in HyperCa, Massive head injury,
subarachnoid hemmorrhage

Cardiology consulted Not concerned about an acute event
because patient completely asymptomatic Decided to admit patient for pre-op workup
since he next in queue for surgery Led to angiogram - > normal Booked for surgery