Embed Size (px)
Citation preview
1
Nausea & Vomiting:Choosing Antiemetics
Dr. Robin LoveMarch 2015
Objectives
Learn a practical approach to management of nausea and vomiting in palliative care
Practical approach…but there is very little science to back this up
2
3
Theoretical Approach
1. Identify the cause2. Identify the physiological pathway3. Identify the neurotransmitter4. Choose the most potent antagonist5. Choose the best route of administration6. Titrate the dose carefully, give the dose
regularly, review frequently7. If symptoms persist, change or add
additional treatments
Oxford Textbook of Palliative Medicine
4
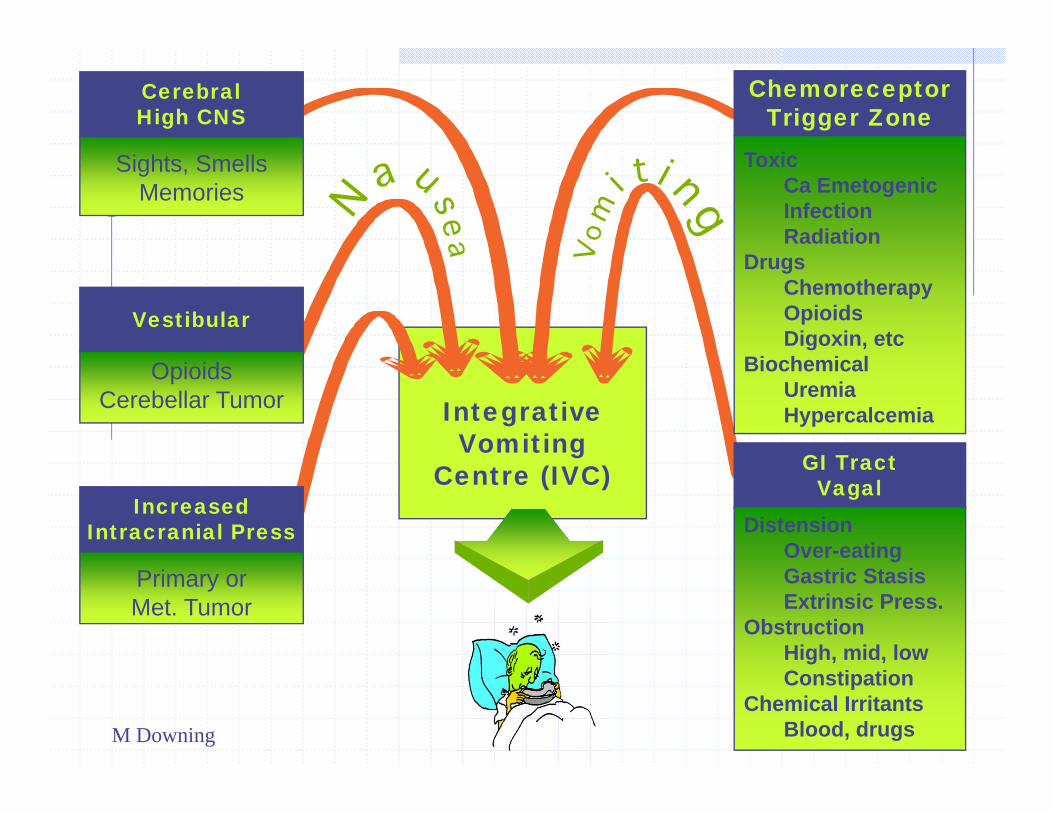
IntegrativeVomiting
Centre (IVC)
CerebralHigh CNS
Sights, SmellsMemories
ChemoreceptorTrigger Zone
ToxicCa EmetogenicInfectionRadiation
DrugsChemotherapyOpioidsDigoxin, etc
BiochemicalUremiaHypercalcemia
Vestibular
OpioidsCerebellar Tumor
IncreasedIntracranial Press
Primary orMet. Tumor
GI TractVagal
DistensionOver-eatingGastric StasisExtrinsic Press.
ObstructionHigh, mid, lowConstipation
Chemical IrritantsBlood, drugsM Downing
5
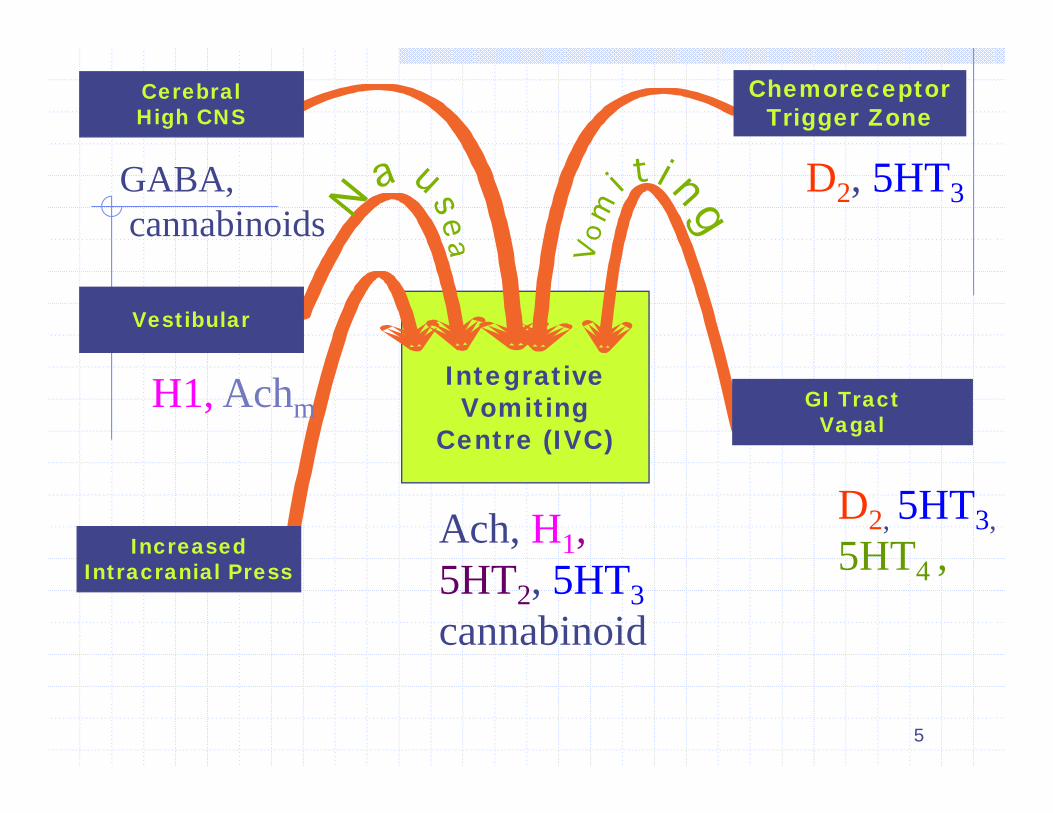
IntegrativeVomiting
Centre (IVC)
CerebralHigh CNS
ChemoreceptorTrigger Zone
Vestibular
IncreasedIntracranial Press
GI TractVagal
D2, 5HT3
D2, 5HT3,5HT4 ,
Ach, H1,5HT2, 5HT3cannabinoid
GABA,cannabinoids
H1, Achm
6
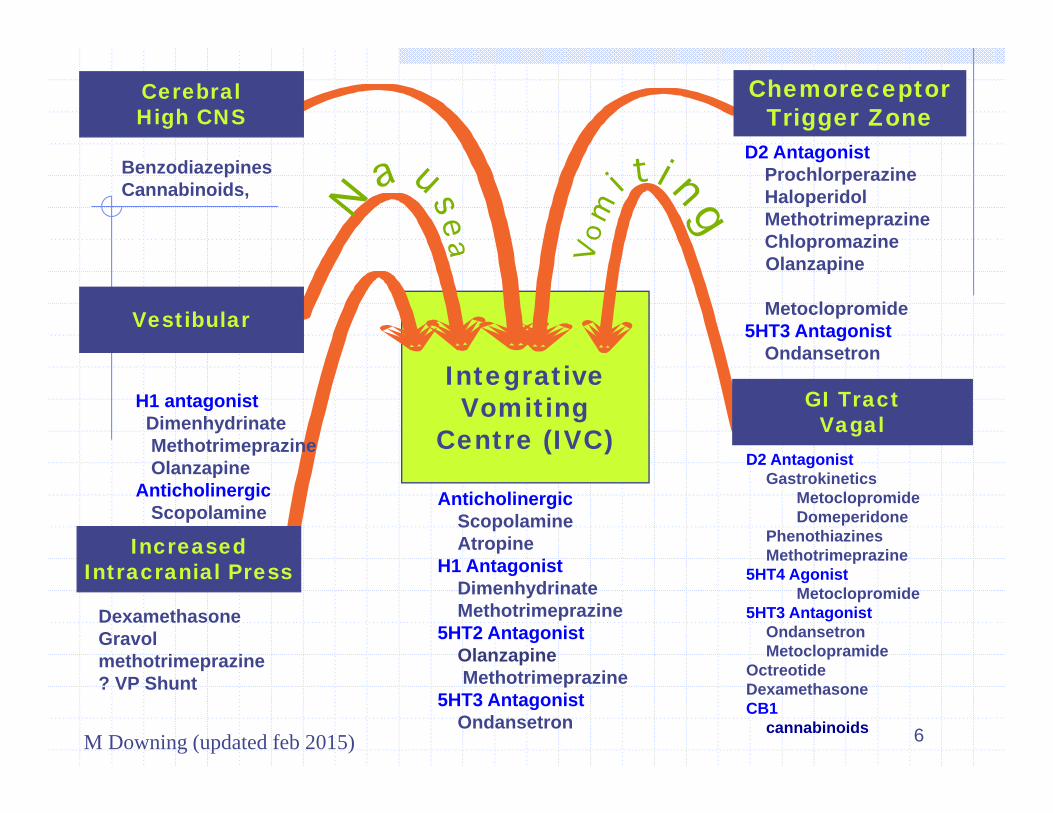
IntegrativeVomiting
Centre (IVC)
CerebralHigh CNS
ChemoreceptorTrigger Zone
Vestibular
IncreasedIntracranial Press
GI TractVagal
DexamethasoneGravolmethotrimeprazine? VP Shunt
D2 AntagonistProchlorperazineHaloperidolMethotrimeprazineChlopromazineOlanzapine
Metoclopromide5HT3 Antagonist
Ondansetron
D2 AntagonistGastrokinetics
MetoclopromideDomeperidone
PhenothiazinesMethotrimeprazine
5HT4 AgonistMetoclopromide
5HT3 AntagonistOndansetronMetoclopramide
OctreotideDexamethasoneCB1
cannabinoids
AnticholinergicScopolamineAtropine
H1 AntagonistDimenhydrinateMethotrimeprazine
5HT2 AntagonistOlanzapineMethotrimeprazine
5HT3 AntagonistOndansetron
BenzodiazepinesCannabinoids,
H1 antagonistDimenhydrinateMethotrimeprazineOlanzapine
AnticholinergicScopolamineAtropine
M Downing (updated feb 2015)
7
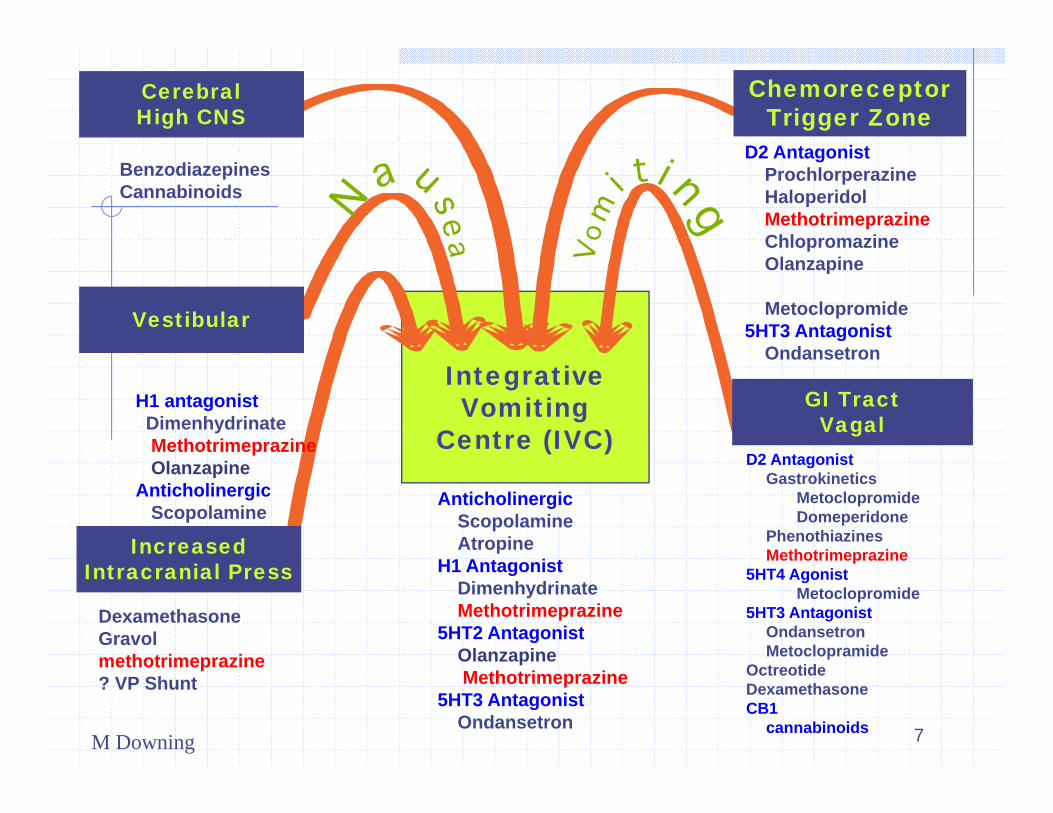
IntegrativeVomiting
Centre (IVC)
CerebralHigh CNS
ChemoreceptorTrigger Zone
Vestibular
IncreasedIntracranial Press
GI TractVagal
DexamethasoneGravolmethotrimeprazine? VP Shunt
D2 AntagonistProchlorperazineHaloperidolMethotrimeprazineChlopromazineOlanzapine
Metoclopromide5HT3 Antagonist
Ondansetron
D2 AntagonistGastrokinetics
MetoclopromideDomeperidone
PhenothiazinesMethotrimeprazine
5HT4 AgonistMetoclopromide
5HT3 AntagonistOndansetronMetoclopramide
OctreotideDexamethasoneCB1
cannabinoids
AnticholinergicScopolamineAtropine
H1 AntagonistDimenhydrinateMethotrimeprazine
5HT2 AntagonistOlanzapineMethotrimeprazine
5HT3 AntagonistOndansetron
BenzodiazepinesCannabinoids
H1 antagonistDimenhydrinateMethotrimeprazineOlanzapine
AnticholinergicScopolamineAtropine
M Downing
8
Framework : How do we organize our approach?All textbooks are organized differently.
Cause? Receptor? ( these are not consistent in different texts)
Drug class? Site of action Chemical type “medical class” ie antipsychotic, prokinetic…
Drug we are most familiar with? Random guess?
9
Practical
Syndrome or Best Etiology Drug
10
Antiemetic Drugs
Wide variety Several classesMuch more complex than AnalgesicsSome drugs affect more than one
receptorSome drugs act in more than one
location
11
Classes of Antiemetic Drugs:1. Dopamine Antagonist
A. AntipsychoticsDrug Haloperidol Prochlorperazine Chlorpromazine Methotrimeprazine Olanzapine
Principal Action CTZ CTZ CTZ / IVC ? CTZ / IVC / Gut ? 5HT2 plus…
Haloperidol the drug of choice:- most potent at CTZ, most specific Dopamine agent - lower side effects- available tablets, liquid, sc, iv, im- use low doses 0.5 –2 mg q8h
12
Classes of Antiemetic Drugs:1.Dopamine Antagonist
B. ProkineticDrug Metoclopramide Domperidone
Principal Action CTZ / GI GI
Metoclopramide the drug of choice:- multiple effects ( CTZ, D2 in Gut, 5HT3, 5HT4)- acts centrally and peripherally- tablets, liquid, sc, iv- watch for akathisia- doses 10-20 (..40) mg qid
13
Classes of Antiemetic Drugs:2. H1 antihistamine
Drug Diphenhydramine Dimenhydrinate Promethazine Hydroxyzine
Principal Action VC, vestibular VC, vestibular UGI tract, VC UGI tract, VC
Drug of Choice?- promethazine sc at lower doses
14
Classes of Antiemetic Drugs:3. Anticholinergic
Drug Scopolamine
(hyoscine) glycopyrrolate Hydroxyzine
Principal Action Vestibular / Vomiting
Center/GI tract Periphery/ GI tract
Scopolamine available as transdermalor sc, iv, imGlycopyrrolate – less CNS side effects
15
Classes of Antiemetic Drugs:4. Steroids
Drug Dexamethasone Prednisone Methylprednisolone
Principal action ???????
- Dexamethasone po, sc- Mechanism of action is not clear
- Also often add this in for difficult nausea
16
Classes of Antiemetic Drugs:5. Cannabinoids
Drugs Nabilone Many new choices of
cannabinoids
Principal action VC VC
Role is unclear, but can be very helpful in some vomiting casesLots of receptors still to be sorted out
17
Classes of Antiemetic Drugs:6. 5-HT3 antagonists.
Drug Ondansetron Granisetron
Principal action UGI tract ? CNS
Reduces gastric secretions? Other effectsConstipating
18
Classes of Antiemetic Drugs:7. Benzodiazepines
Drugs Lorazepam Midazolam
Principal action adjunctive
Little direct antiemetic effect, but they reduce anxiety , akathisia and anticipatory nausea
19
Classes of Antiemetic Drugs8. miscellaneous
Drugs Octreotide Omeprazole Ranitidine Antacids
Propofol
Principal action Antisecretory etc Proton pump inhibitor H2 receptor antagonist
? CTZ or VC
20
Non Drug Measures
Nasogastric tubeGastrostomy tube ( venting)
Family and Nursing measures
Food typeOdorsPresent small portions only of what they want“Palliative Diet” – eat what they feel like eatingEducate patient and family about futility of pushing calories
21
22
Common Syndromes of Nausea
23
1. Chemically Induced
Causes Opioids Digoxin Cancer treatment Anticonvulsants Antibiotics Toxins ( tumor products,
ischemic bowel) Metabolic ( Ca , liver or
renal failure …)
Treatment Haloperidol Prochlorperazine ChlorpromazineMethotrimeprazineMetoclopramideDexamethasone LorazepamOndansetron
24
2. Motion Induced
Causes Opioids Gastroparesis CNS tumor or
metastases
Treatment Promethazine
(phenergan) Dimenhydrinate
(gravol) Scopolamine/Hyoscin
e Methotrimeprazine Doxylamine/pyridoxi
ne (Diclectin)
25
3. Gastric Stasis
Causes Opioids Anticholinergic drugs Ascites Autonomic
dysfunction Hepatomegaly Gastritis Obstruction/
mechanical
Treatment ProkineticsMetoclopramide Domperidone
Dopamine antag.Haloperidol etc.
Reduce secretions scopolamine Octreotide Omeprazole etc
26
4.Vagal Induced- stretch/distortion of visceraCauses
Constipation Obstruction Mesenteric
metastases Liver metastases Ureteric obstruction
Treatment ProkineticsMetoclopramide Domperidone
Methotrimeprazine Dimenhydrinate Scopolamine
27
5. Increased Intracranial Pressure
Causes Tumor Edema Intracranial bleed Infection ( Aids)
Treatment Dexamethasone
Dimenhydrinate Methotrimeprazine lorazepam
General Strategy ( if no obvious cause)
“ do you feel full and bloated like you ate too much or is it more of a queasy car sick kind of feeling ?”
28
metoclopramide
haloperidol
29
General Strategy ( if no obvious cause)
1. Metoclopramide 10-20 mg sc q 6h 2. +/ - Haloperidol 0.5-1 –2 mg sc q6h3. + Antihistamine4. + Dexamethasone5. + Scopolamine6. 3rd line including ondansetron, nabilone,
diclectin ….
30
Intractable Nausea
May require sedation Lorazepam, midazolam, chlorpromazine,
methotrimeprazine, etc. Propofol may be effective but not
practically available
Gastrostomy venting tube
31
Pearls
Optimize the dose depending on side effectsRe-evaluate possible causeAdd 2nd line that targets a different receptor(usually add drugs, don’t just substitute as there
may be additive effects)Continuous medication may be more effectiveMay need multiple drug combinations in high dosesDon’t forget the practical measures (reduce intake etc.)