Embed Size (px)
Citation preview
Natural Killer Cell Neoplasms
Xiayuan Liang, MD1,2
Douglas K. Graham, MD, PhD3,4
1 Department of Pathology, Children’s Hospital,Denver, Colorado.
2 Department of Pathology, University of ColoradoSchool of Medicine, Denver, Colorado.
3 Section of Hematology/Oncology, Children’sHospital, Denver, Colorado.
4 Department of Pediatrics, University of ColoradoSchool of Medicine, Denver, Colorado.
Natural killer (NK) cell tumors are an uncommon and heterogeneous group of dis-
orders. The World Health Organization (WHO) classified mature NK cell neo-
plasms into 2 types: 1) extranodal NK cell lymphoma, nasal type and 2) aggressive
NK cell leukemia. The mature NK cell tumors are prevalent in Asia and Central
and South America. These tumors show polymorphic neoplastic infiltrate with
angioinvasion and/or angiodestruction, cytoplasmic azurophilic granules, CD2-
positive (CD21)/CD3-negative (CD32)/cCD3e1/CD561 phenotype, and strong
association with Epstein-Barr virus (EBV). Loss of chromosomes 6q, 11q, 13q, and
17p are recurrent aberrations. Although blastic NK cell lymphoma, currently
referred to as CD41/CD561 hematodermic neoplasm, also was included in the NK
cell lymphoma category in the WHO classification scheme, existing evidence indi-
cates a plasmacytoid dendritic cell derivation as opposed to an NK cell origin.
Recently, rare cases of CD561 immature lymphoid tumors have been reported in
the literature. These tumors are characterized by blastic appearance, CD32/CD42/
CD561/CD132/CD332 phenotype, T-cell receptor and immunoglobulin genes in
germline configuration, and no evidence of EBV, suggesting a true immature NK
cell derivation. For this article, the authors reviewed the recent concepts and pro-
gress in clinicopathologic features, pathogenesis, genetic characteristics, diagnosis,
differential diagnosis, treatment approaches, and outcomes of all subtypes of NK
cell neoplasms. Cancer 2008;112:1425–36. � 2008 American Cancer Society.
KEYWORDS: natural killer cell lymphoma, natural killer cell leukemia, naturalkiller cell, natural killer cell tumor, CD56.
N atural killer (NK) cells represent a lineage of non-T lymphocytes
and non-B lymphocytes that mediate a major histocompatibility
complex, nonrestricted cytotoxicity against tumor cells and bacterial
or viral infected cells.1 NK cells constitute <5% of peripheral blood
lymphocytes with large granular lymphocyte (LGL) morphology. NK
cells are derived in bone marrow from hematopoietic stem cells
through the intermediate developmental stages of lymphoid stem
cells, bipotential T/NK progenitor cells, and committed NK progeni-
tor cells.2–4 Therefore, NK cells express variably T-lineage-associated
antigens (CD2 and/or CD7). By definition, NK cells are surface CD3-
negatiave (CD32) and myeloperoxidase (MPO)2, and have germline
configuration of T-cell receptor (TCR) and immunoglobulin (Ig)
genes.5–7 CD16, CD56, and CD57 are NK-associated antigens.
Among these 3 markers, CD56 (neural cell adhesion molecule) is
expressed most consistently.8
NK cell neoplasms are a rare and heterogeneous group of disor-
ders with a broad spectrum of morphologic, immunophenotypic,
and clinical features. The World Health Organization (WHO) classifi-
cation encompasses 3 distinct entities: 1) aggressive NK cell leuke-
mia9; 2) extranodal NK/T-cell lymphoma, nasal type10; and 3) blastic
Address for reprints: Xiayuan Liang, MD, Depart-ment of Pathology, Children’s Hospital, 13123East 16th Avenue, Aurora, CO 80045; Fax: (720)777-7119; E-mail: [email protected]
Received August 3, 2007; revision receivedOctober 11, 2007; accepted October 16, 2007.
ª 2008 American Cancer SocietyDOI 10.1002/cncr.23316Published online 19 February 2008 in Wiley InterScience (www.interscience.wiley.com).
1425

NK cell lymphoma.11 In recent years, the conceptual
view of NK cell neoplasms has changed as the result
of further understanding of the cell derivations and
the characteristics of the malignant counterparts.
Currently, it is believed that blastic NK cell lym-
phoma derives from plasmacytoid dendritic cells
(pDCs) rather than NK cells.12–14 In this article, we
review the recent concepts and progress in clinico-
pathologic features, pathogenesis, cytogenetics, diag-
nosis, differential diagnosis, treatment strategies, and
outcomes of this group of uncommon neoplasms.
Clinicopathologic Categorizations and FeaturesOn the basis of morphology, immunophenotype,
functional NK cell activity, and expression of cyto-
toxic molecules, NK cell neoplasms can be divided
into immature and mature categories.5,7,15–20 In the
last 2 decades, a number of patients with CD56-posi-
tive (CD561) blastoid hematopoietic tumors have
been reported in the literature, suggesting the exis-
tence of neoplasms arising from immature NK
cells.6,16–32 In contrast, it is believed that aggressive
NK cell leukemia and extranodal NK cell lymphoma,
nasal type originate from mature NK cells.5,9,10,15
Precursor NK cell neoplasms and otherhistorically related entitiesPrecursor lymphoblastic lymphoma/leukemia (LBL)-
expressing NK cell-associated antigens was recog-
nized first by Sheibani et al. in 1987.16 Six tumors that
expressed CD16 and CD57 in addition to terminal de-
oxynucleotidyl transferase (TdT), CD2, and CD4 were
identified among 38 patients who were screened for
LBL. These tumors, as a group, were designated ‘‘NK-
LBL.’’16 Subsequently, CD56 has been recognized as a
sensitive marker for NK cells and has become popular
for identifying NK cell neoplasms. There are approxi-
mately 200 CD561 hematopoietic neoplasms with
immature features reported in the literature using an
array of names. However, CD56 is not a NK cell-speci-
fic marker and can be expressed by other neo-
plasms,33,34 and it has been difficult to determine
whether these tumors are of a true NK cell derivation.
Blastic NK cell lymphoma (CD41/CD561 hematodermic
neoplasm). Starting in 1994, several individual cases
or small series of lymphoblastoid-appearing tumors
that expressed CD4 and CD56 and involved the
skin, bone marrow, and lymph node were reported
that described such tumors as a distinct entity.22 An
NK cell origin was suggested for many of these
lesions based on CD56 expression in the absence of
markers of T-cell, B-cell, and myeloid lineage-specific
antigens.6,7,17–19,21,28–32 Consequently, these tumors
were classified provisionally as blastic NK cell lym-
phoma in the WHO classification scheme of hemato-
poietic tumors.11 However, CD56 is not a specific
marker for NK cells,33,34 CD4 expression is not typi-
cal of NK cell development,35 and previous attempts
to differentiate CD41/CD561 tumors into NK cells
were not successful.36,37 In searching for an alterna-
tive to an unlikely NK cell origin, an important dis-
covery of strong expression of surface CD123, a
molecule mainly expressed by dendritic cells (DCs)
and pDCs, by these CD41/CD561 tumors suggested
an origin from pDCs.14,38,39 Further progress came
with the immunophenotypic and functional evidence
that most CD41/CD561 tumors are related to the
pDC lineage.12–14 Immunophenotypically, they share
expression of CD4, CD43, CD68, CD123, human leu-
kocyte antigen-D related (HLA-DR), TCL-1, and the
cutaneous lymphocyte associated antigen (CLA).
They are negative for the major T-, B-, and myeloid
cell differentiation antigens (CD3, CD19, CD20, and
MPO).12,13 Functionally, Chaperot et al. demonstrated
that cultured CD41/CD561 tumor cells exhibited fea-
tures of pDCs like secreting interferon-a, undergoingdifferentiation to DCs with interleukin-3 stimulation,
and being able to stimulate naive T lymphocytes.14
More recently, it was demonstrated that a more spe-
cific DC marker, blood DC antigen 2 (BDCA-2), is
expressed in a subset of these CD41/CD561 tumors,
which further supports the pDC derivation of this
type of tumor.40 However, some issues remain unde-
termined, such as an association of this type of
CD41/CD561 tumor with precedent, concurrent, or
subsequent myelomonocytic tumors41 and lacking
expression of CD56 on nonneoplastic pDCs.42 More
investigation is required to establish the definitive
nature of this type of CD41/CD561 tumor.
The term agranular CD41/CD561 hematodermic
tumor originally proposed by Petrella et al.39 has the
virtues of describing a key diagnostic feature, the
most common pattern of clinical manifestation, and
the defining immunophenotype. Therefore, it seems
suitable as a provisional name to replace the misno-
mer blastic NK cell lymphoma. In the recent WHO-
European Organization of Research and Treatment of
Cancer classification of cutaneous lymphoma, the
term blastic NK cell lymphoma was replaced with
CD41/CD561 hematodermic neoplasm.43
CD42/CD561 immature NK cell tumors (provisional
precursor NK cell neoplasms). There are rare cases of
CD561 immature lymphoid tumors reported in the
literature that do not match the features of blastic
NK cell lymphoma (CD41/CD561 hematodermic
1426 CANCER April 1, 2008 / Volume 112 / Number 7

neoplasm). The cells in these tumors are character-
ized by a blastic appearance (Fig. 1) with a compos-
ite phenotype (CD42/CD561/CD132/CD332), and
they lack expression of CD3, CD19, CD20, and
MPO. Five well documented cases were identified in
the English literature (Table 1).44–48 It is noteworthy
that all of the patients in those reports were female
and were primarily of Asian and Hispanic descent
(4 of 5 patients; 80%). Those patients ranged in age
from 4 years to 57 years, and their median age was
14 years, which was much younger than the median
age for patients with blastic NK cell lymphoma
(CD41/CD561 hematodermic neoplasm) (age range,
8–96 years; median age, 63.5 years in 1 study).49
These findings were similar to the observations
reported by Sheibani et al.16 The patients frequently
presented with leukemia and lymphadenopathy
without skin involvement. These tumors were nega-
tive for EBV. TCR and/or Ig genes were in germline
configuration in all tumors in which the tests were
performed. Two patients with complete karyotype
results showed add(21)(p11). It is unclear whether
this karyotype represents a recurrent chromosome
aberration given the very small number of patients
and the limited cytogenetic data. The outcomes of
these patients were unfavorable, because only 2 of 5
patients (40%) were alive 3 years after diagnosis.
Although the characteristics of precursor NK cells
have not been defined fully, the immature morphol-
ogy with NK cell-associated phenotype and geno-
type suggest that these tumors likely represent true
precursor NK cell neoplasms.
Recent advances in the developmental biology of
T cells and NK cells indicate that both cell types are
derived from a common T/NK cell thymic precursor.
Interleukin 15 (IL-15) and transcription factor ID2
are essential for the NK cell lineage to diverge from
the T cell lineage.20 CD94 1A, a distal promoter of
the CD94 molecule (an NK cell receptor), is activated
only by IL-15.20,50,51 Lin et al. recently reported that
CD94 1A is the predominant form expressed in
immature NK cells20 and is expressed in TCR2 LBL
(NK-LBL) but not in TCR1 LBL (T-LBL). On the basis
of the expression of CD94 1A transcripts and nega-
tive TCR, those investigators identified 7 patients
with LBL of immature NK cell origin (CD94 1A1,
TCR2) by studying 21 patients with LBL. It is note-
worthy that those NK-LBLs occurred in younger
patients and had better outcomes compared with
patients who had T-LBL (CD94 1A2, TCR1), and
none of the tumors were positive for CD56. Because
CD56 is not lineage-specific, it is not surprising that
neither its presence nor its absence implies commit-
ment to NK cell lineage. Thus, the use of CD94 1A in
conjunction with TCR appears to be more precise for
identifying an immature NK cell neoplasm than
CD56 alone.
Myeloid/NK cell leukemia/lymphoma. In 1994, Scott
and colleagues described a distinct form of acute
leukemia that shared features of both myeloid and
NK cells and designated it myeloid/NK cell acute
leukemia.52 These tumors have the following charac-
teristics: 1) acute promyelocytic leukemia-like mor-
phology; 2) the presence of MPO1/Sudan Black1
cytoplasmic, fine, azurophilic granules; 3) lack of
t(15;17) and the resultant PML/RARa fusion tran-
script; 4) a unique immunophenotype (HLA-DR2/
CD331/CD561/CD162/CD32); and 5) functional NK
cell-mediated cytotoxicity in a subset of tumors.
Furthermore, those investigators also identified nor-
mal CD331/CD561/CD162 counterpart cells in pe-
ripheral blood from healthy individuals and
proposed that this type of acute leukemia may arise
from transformation of a precursor cell that is com-
mon to the myeloid and NK cell lineage.
Later, Suzuki et al. proposed another disease
entity, CD71 and CD561 myeloid/NK cell precursor
acute leukemia, based on its phenotypic similarity to
the myeloid antigen-positive NK cell precursors.53
This entity is characterized by extramedullary
involvement, blastic morphology without cytoplas-
mic granules and MPO reactivity, CD71/CD561/
CD331/CD341/CD32 phenotype, and poor progno-
sis.17,18 Several more patients with this type of leu-
kemia were reported in the literature after its initial
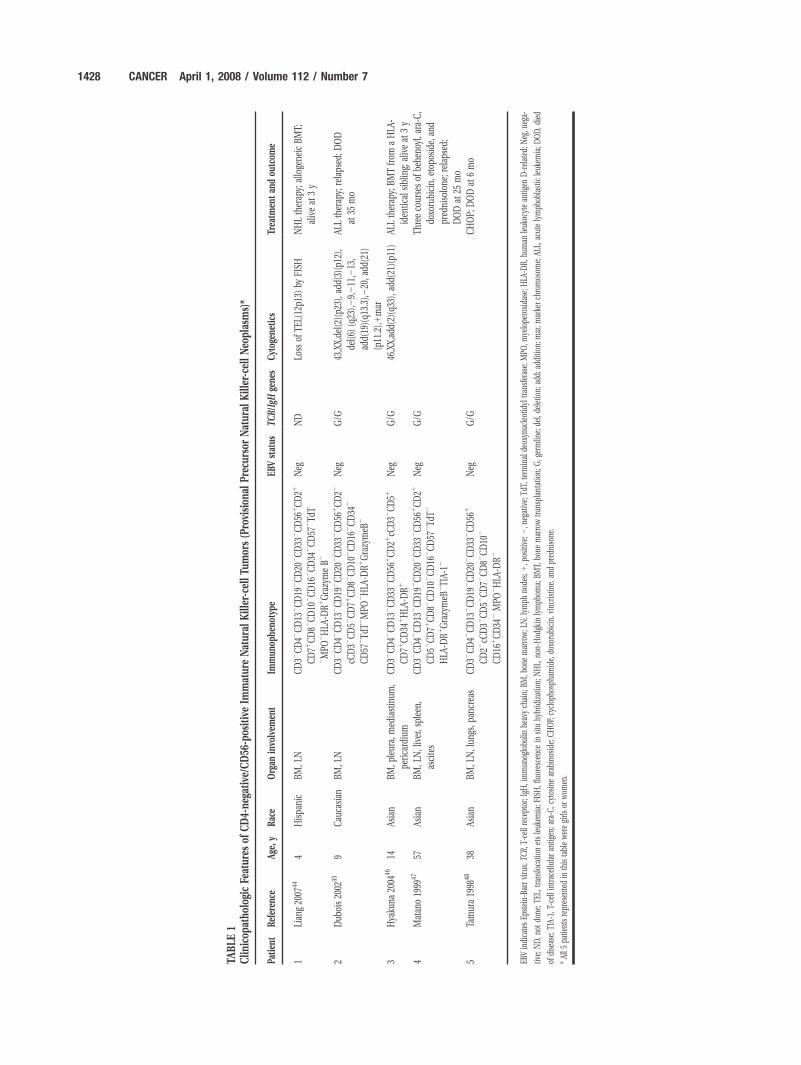
FIGURE 1. Morphologic features of a CD4-negative/CD56-positive imma-ture natural killer-cell tumor. The tumor cells show lymphoblastic features
with a high nuclear:cytoplasmic ratio, slightly dense chromatin, and indistinct
nucleolus.
Natural Killer Cell Tumors/Liang and Graham 1427
TABLE
1Clin
icop
atho
logicFe
atur
esof
CD4-ne
gative
/CD56
-pos
itiveIm
matur
eNatur
alKiller-cellTu
mor
s(Provision
alPr
ecur
sorNatur
alKiller-cellNeo
plasms)*
Patien
tReferen
ceAg
e,y
Rac
eOrgan
invo
lvem
ent
Immun
ophe
notype
EBVstatus
TCR/IgH
gene
sCy
toge
netics
Trea
tmen
tan
dou
tcom
e
1Lian
g20
0744
4Hispa
nic
BM,L
NCD32
CD42
CD13
2CD19
2CD20
2CD33
2CD56
1CD21
CD71
CD82
CD10
2CD16
2CD34
2CD57
2Td
T2MPO
2HLA
-DR1
GrazymeB2
Neg
ND
Loss
ofTE
L(12
p13)
byFISH
NHLtherap
y;alloge
neic
BMT;
aliveat
3y
2Dub
ois20
0245
9Cau
casian
BM,L
NCD32
CD42
CD13
2CD19
2CD20
2CD33
2CD56
1CD22
cCD32
CD52
CD71
CD82
CD10
2CD16
2CD34
2
CD57
2Td
T2MPO
2HLA
-DR1
GrazymeB
2
Neg
G/G
43,XX,de
l(2)(p2
3),a
dd(3)(p1
2),
del(6
)(q23
),29,211
,213
,
add(19
)(q1
3.3),2
20,a
dd(21)
(p11
.2),1
mar
ALLtherap
y;relaps
ed;D
OD
at35
mo
3Hya
kuna
2004
4614
Asian
BM,p
leura,
med
iastinum
,
perica
rdium
CD32
CD42
CD13
2CD33
2CD56
1CD21
cCD32
CD51
CD71
CD34
1HLA
-DR1
Neg
G/G
46,XX,ad
d(2)(q33
),ad
d(21
)(p1
1)AL
Ltherap
y;BM
Tfrom
aHLA
-
iden
tical
sibling;
aliveat
3y
4Matan
o19
9947
57As
ian
BM,L
N,liver,s
plee
n,
ascites
CD32
CD42
CD13
2CD19
2CD20
2CD33
2CD56
1CD21
CD52
CD71
CD82
CD10
2CD16
2CD57
2Td
T2
HLA
-DR1
GrazymeB
2TIA-
12
Neg
G/G
Threeco
ursesof
behe
noyl,a
ra-C
,
doxo
rubicin,
etop
oside,
and
pred
niso
lone
;relap
sed;
DOD
at25
mo
5Ta
mura19
9848
38As
ian
BM,L
N,lun
gs,p
ancrea
sCD32
CD42
CD13
2CD19
2CD20
2CD33
2CD56
1
CD22
cCD32
CD52
CD72
CD82
CD10
2
CD16
1CD34
2MPO
2HLA
-DR2
Neg
G/G
CHOP;
DOD
at6mo
EBVindica
tesEp
stein-
Barr
virus;
TCR,
T-ce
llrece
ptor;IgH
,immun
oglobu
linhe
avych
ain;
BM,b
onemarrow;L
N,lym
phno
des;
1,p
ositive
;2,n
egative;
TdT,
term
inal
deox
ynuc
leotidyl
tran
sferase;
MPO
,mye
lope
roxida
se;H
LA-D
R,hu
man
leuk
ocytean
tigen
D-related
;Neg
,neg
a-
tive;
ND,n
otdo
ne;T
EL,trans
loca
tionetsleuk
emia;F
ISH,fluoresce
ncein
situ
hybridization;
NHL,
non-
Hod
gkin
lymph
oma;
BMT,
bone
marrow
tran
splantation;
G,g
ermlin
e;de
l,de
letio
n;ad
d;ad
ditio
n;mar,m
arke
rch
romos
ome;
ALL,
acutelymph
oblastic
leuk
emia;D
OD,d
ied
ofdisease;
TIA-
1,T-ce
llintrac
ellularan
tigen
;ara-C
,cytos
inearab
inos
ide;
CHOP,
cyclop
hosp
hamide,
doxo
rubicin,
vinc
ristin
e,an
dpred
niso
ne.
*All5
patie
ntsrepresen
tedin
this
tableweregirls
orwom
en.
1428 CANCER April 1, 2008 / Volume 112 / Number 7

identification.54–58 However, because CD56 expres-
sion has been identified in approximately 20% of
patients with acute myeloid leukemia (AML),59 the
features of immature cytologic appearance and the
presence of myeloid antigen without light-micro-
scopic MPO reactivity in this type of leukemia over-
lap with those in AML with minimal differentiation
(French-American-British classification, AML-M0).
Because there were only a small number of patients
studied and the terminology of CD71 and CD561
myeloid/NK cell precursor acute leukemia has not
been recognized widely, currently, it is believed that
this subset of leukemia falls into the category of
AML-M0.60 Comparing CD71/CD561 M0 with other
M0 (CD72/CD562, CD72, or CD562), Suzuki et al.
observed a significantly younger age of onset, no 5q
abnormalities, more frequent extramedullary involve-
ment, and worse disease-free survival in the patients
with CD71/CD561 M0 disease. Multivariate analysis
demonstrated that the CD71/CD561 phenotype was
a significant and an independent poor prognostic
factor for patients with AML-M0.60 Additional clini-
copathologic studies are needed to elucidate whether
this subtype of acute leukemia represents a distinct
entity.
Mature NK cell neoplasmsThe distinct nature of NK cell tumors was acknowl-
edged formally at the Hong Kong workshop in
1996.15 Several clinicopathologic entities have been
recognized.
Extranodal NK cell lymphoma, nasal type. Both nasal
and nasal-type (extranasal) NK cell lymphomas are
more prevalent in Asia, Mexico, and Central and
South America10,61 and are characterized by extrano-
dal presentation and an aggressive clinical course.
Because nasal NK cell lymphoma and extranasal NK
cell lymphoma share the same histology, the WHO
classification groups both nasal NK cell lymphoma
and extranasal NK cell lymphoma in the same cate-
gory.10 However, nasal and extranasal NK cell lym-
phomas have different clinical manifestations,
treatment approaches, and prognoses.61
Nasal NK cell lymphomas refer to tumors that
occur in the nose and the upper aerodigestive
tract.62–67 They are the most common type among
primary lymphomas of the nasal cavity.8 Men are
affected more than women, and the median age at
diagnosis in the fifth decade. The location is primar-
ily in the midline and includes the nasal cavity, naso-
pharynx, paranasal sinuses, tonsils, hypopharynx,
and larynx. Common symptoms include nasal dis-
charge, nasal obstruction, purulent rhinorrhea, epis-
taxis, and local swelling of the nasal bridge. In
patients with more advanced disease, there may be
erythema, swelling of the face, proptosis, and impair-
ment of extraocular movement.8,62,67 The tumors
may be destructive, leading to the highly characteris-
tic midline perforation.
Extranasal NK cell lymphomas represent the
counterpart of nasal NK cell lymphomas and involve
any other part of the body. Men are affected predo-
minantly, and the median age of presentation is in
the fifth decade. Primary sites of involvement include
the skin, gastrointestinal tract, salivary glands,
spleen, and testis.7 The diagnosis of extranasal NK
cell lymphoma requires the exclusion of nasal invol-
vement at presentation. A nasal panendoscopy with
random biopsies should be performed to rule out
occult involvement.61 Patients with extranasal NK
cell lymphoma are more likely to exhibit a more
advanced stage of disease with significantly higher
International Prognostic Index and lactate dehydro-
genase levels and with significantly lower hemoglo-
bin and platelet levels compared with patients who
have nasal NK cell lymphoma.
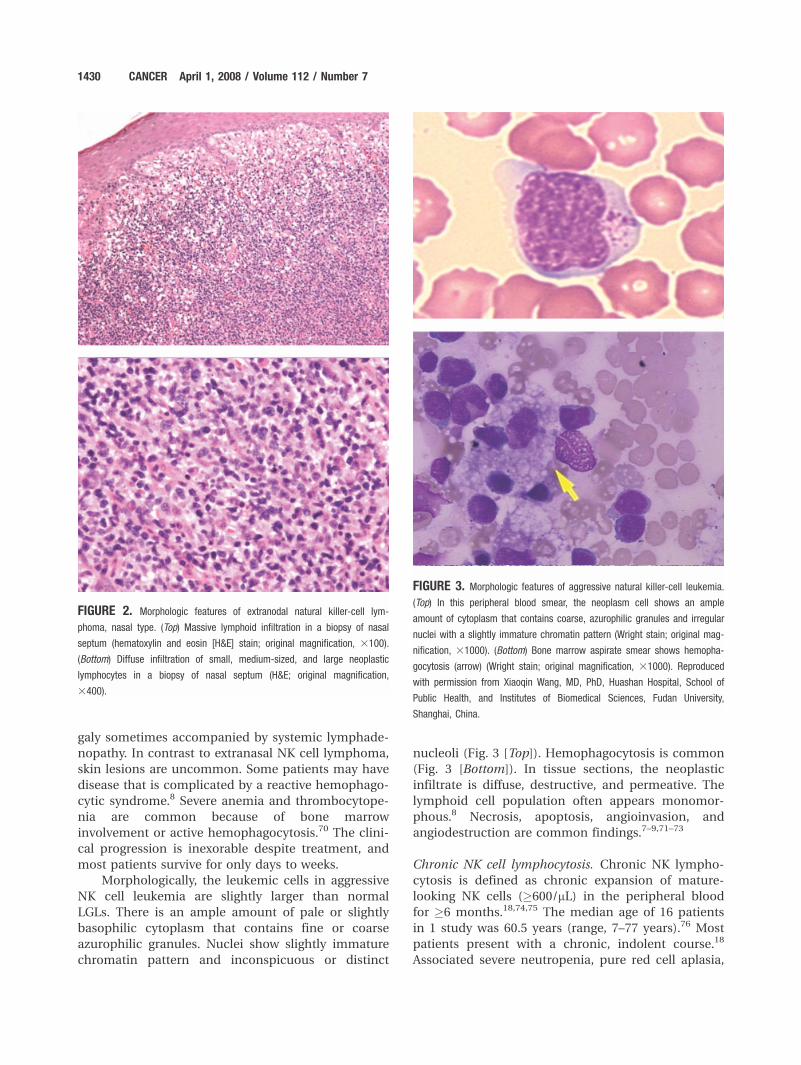
The histologic features are similar regardless of
the involved sites. Mucosal sites often show ulcera-
tion. The lymphomatous infiltrate is diffuse (Fig. 2
[Top]). An angiocentric and angiodestructive growth
pattern with associated fibrinoid changes in the
blood vessels is observed frequently. Coagulative ne-
crosis and apoptosis are common. In most patients,
the tumor is composed of medium-sized cells or a
mixture of small and large lymphoid cells with mod-
erate amount of cytoplasm, irregular or elongated
nuclei, granular or vesicular chromatin, and incon-
spicuous, small nucleoli (Fig. 2 [Bottom]). Mitotic
figures are found easily. In Giemsa-stained touch pre-
parations, azurophilic cytoplasmic granules com-
monly are detected. There may be admixture of
inflammatory cells consisting of small lymphocytes,
plasma cells, histiocytes, and eosinophils in some
patients.10
Aggressive NK cell leukemia. Aggressive NK cell leu-
kemia was characterized first by Imamura et al.68,69
This is a catastrophic, systemic disease and also is
more prevalent in Asians than in Caucasians.9 It is
characterized by the presence of neoplastic NK cells
mainly in the peripheral blood and bone marrow
and by a rapidly progressive clinical course. There is
an equal sex incidence in men and women. The dis-
ease typically affects young to middle-aged adults
with a median age in the third decade. Patients usu-
ally are very ill at presentation with fever, systemic
symptoms, liver dysfunction, and hepatosplenome-
Natural Killer Cell Tumors/Liang and Graham 1429
galy sometimes accompanied by systemic lymphade-
nopathy. In contrast to extranasal NK cell lymphoma,
skin lesions are uncommon. Some patients may have
disease that is complicated by a reactive hemophago-
cytic syndrome.8 Severe anemia and thrombocytope-
nia are common because of bone marrow
involvement or active hemophagocytosis.70 The clini-
cal progression is inexorable despite treatment, and
most patients survive for only days to weeks.
Morphologically, the leukemic cells in aggressive
NK cell leukemia are slightly larger than normal
LGLs. There is an ample amount of pale or slightly
basophilic cytoplasm that contains fine or coarse
azurophilic granules. Nuclei show slightly immature
chromatin pattern and inconspicuous or distinct
nucleoli (Fig. 3 [Top]). Hemophagocytosis is common
(Fig. 3 [Bottom]). In tissue sections, the neoplastic
infiltrate is diffuse, destructive, and permeative. The
lymphoid cell population often appears monomor-
phous.8 Necrosis, apoptosis, angioinvasion, and
angiodestruction are common findings.7–9,71–73
Chronic NK cell lymphocytosis. Chronic NK lympho-
cytosis is defined as chronic expansion of mature-
looking NK cells (�600/mL) in the peripheral blood
for �6 months.18,74,75 The median age of 16 patients
in 1 study was 60.5 years (range, 7–77 years).76 Most
patients present with a chronic, indolent course.18
Associated severe neutropenia, pure red cell aplasia,
FIGURE 2. Morphologic features of extranodal natural killer-cell lym-phoma, nasal type. (Top) Massive lymphoid infiltration in a biopsy of nasal
septum (hematoxylin and eosin [H&E] stain; original magnification, 3100).
(Bottom) Diffuse infiltration of small, medium-sized, and large neoplastic
lymphocytes in a biopsy of nasal septum (H&E; original magnification,
3400).
FIGURE 3. Morphologic features of aggressive natural killer-cell leukemia.(Top) In this peripheral blood smear, the neoplasm cell shows an ample
amount of cytoplasm that contains coarse, azurophilic granules and irregular
nuclei with a slightly immature chromatin pattern (Wright stain; original mag-
nification, 31000). (Bottom) Bone marrow aspirate smear shows hemopha-
gocytosis (arrow) (Wright stain; original magnification, 31000). Reproduced
with permission from Xiaoqin Wang, MD, PhD, Huashan Hospital, School of
Public Health, and Institutes of Biomedical Sciences, Fudan University,
Shanghai, China.
1430 CANCER April 1, 2008 / Volume 112 / Number 7

vasculitic syndromes, and fever with undetermined
origin are reported in some patients.76,77 Occasion-
ally, patients present with a slowly progressive
increase of peripheral blood NK cells and with organ
involvement. These cases may be labeled chronic NK
cell leukemia, but the clonality of the NK cells must
be proven. In rare cases, the disease transforms to
aggressive NK cell leukemia.18 Cytologically, the cir-
culating neoplastic cells show LGL morphology.
There is a moderate amount of pale cytoplasm that
contains �3 azurophilic granules (Fig. 4).76,77
All subtypes of mature NK cell neoplasms share
a typical immunophenotype of CD21/CD32/
cCD3e1/CD561/MPO2 and are cytotoxic molecule-
positive.9,10,76–79 The TCR gene typically is in germ-
line configuration. Another characteristic feature of
mature NK cell neoplasms, in contrast to immature
NK cell neoplasms, is the strong association with
EBV.79–81 Nasal NK cell lymphoma is associated
almost invariably with EBV infection (Fig. 5). Most
patients with aggressive NK cell leukemia, extranasal
NK cell lymphoma, and chronic NK cell lymphocyto-
sis also are positive for EBV. A large comprehensive
study of NK cell neoplasms in Japan by Oshimi et al.
indicated that EBV was detected in all patients with
nasal NK cell lymphoma (101 of 101 patients), in 22
of 25 patients with extranasal NK cell lymphoma, in
10 of 12 patients with aggressive NK cell leukemia,
and in 6 of 7 patients with chronic NK cell lympho-
cytosis.79 Analysis of the terminal repeat region of
the EBV genome indicated that the virus is in a clo-
nal episomal form. This finding, in addition to pro-
viding an indirect proof of the clonal nature of the
lymphoid proliferation, also implies that the EBV
may play an etiologic role in mature NK cell neo-
plasms rather than being a bystander.8,82,83
Conventional cytogenetic analysis of mature NK
cell neoplasms is difficult, partly because of necrosis
and the scarcity of specimens.8 A study by Wong
et al.84 demonstrated that 77% (23 of 30) of patients
with mature NK cell neoplasms had abnormal clonal
karyotypes. Most patients exhibited pseudodiploidy
(57%; 13 of 23 patients), hypodiploidy (<46 chromo-
somes) was identified in 3 of 23 patients (13%), and
7 patients (30%) were hyperdiploid (>46 chromo-
somes).84 Abnormalities of chromosome 6 were the
most frequent findings. A common deletion on 6q in
the target area 6q21-25 has been defined by fluores-
cence in situ hybridization and molecular genetic
methods.85,86 Comparative genomic hybridization
and loss of heterozygosity studies have indicated
that, in addition to deletion of 6q21-25, deletions in
chromosome 11q, 13q and 17p also were pres-
ent.8,87,88 The putative genes implicated in these
deletions have not been identified.
Diagnostic Criteria and Differential DiagnosisDiagnosis of NK cell neoplasms requires the integra-
tion of clinical presentation, morphology, immuno-
phenotype, and genotype. Expression of at least 1 NK
cell marker (CD56, CD16, or CD57); lack of expres-
sion of surface CD3, B-cell antigens (CD19 and
CD20), MPO, and other lineage markers; and/or TCR
and Ig genes in germline configuration in tumors are
FIGURE 4. Morphologic features of chronic natural killer-cell lymphocyto-sis. A peripheral blood smear shows a large granular lymphocyte (arrow)
with moderate amount of cytoplasm containing a few fine, azurophilic gran-
ules (Wright stain; original magnification, 31000).
FIGURE 5. Epstein-Barr virus (EBV) signal was detected in tumor cells byin situ hybridization for EBV-encoded small RNA in a patient with extranodal
natural killer-cell lymphoma, nasal type (original magnification, 3400).
Natural Killer Cell Tumors/Liang and Graham 1431

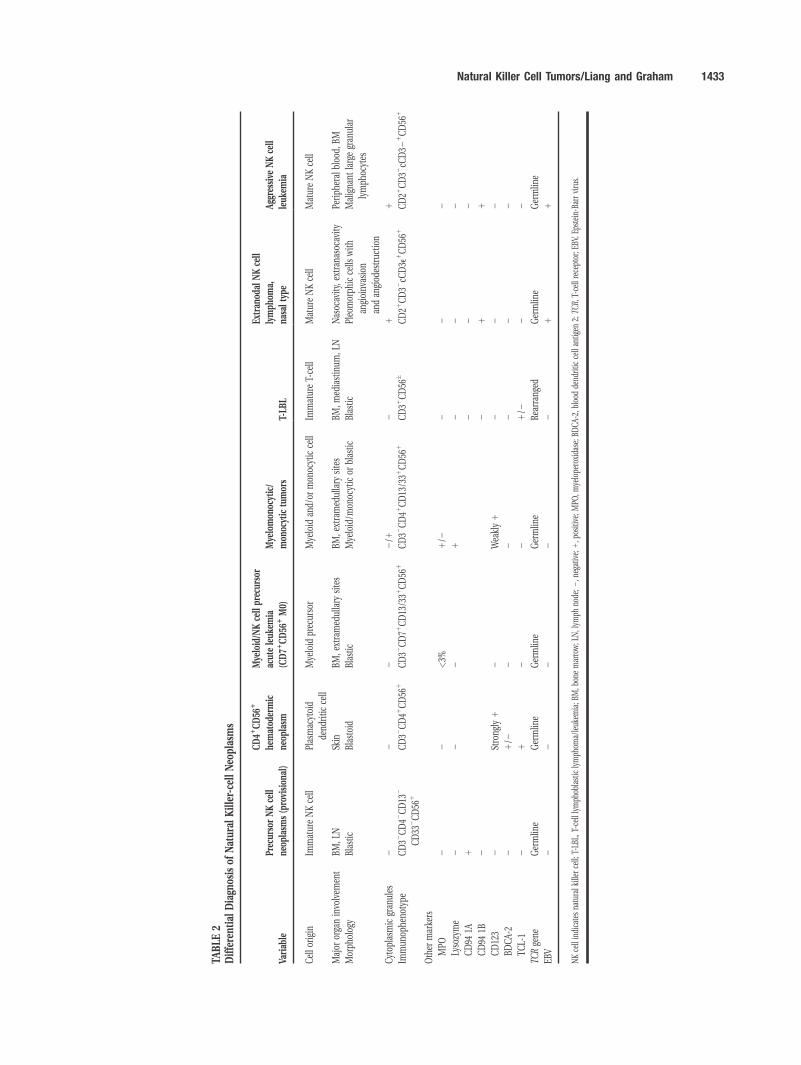
essential. EBV status is supportive. It is important to
distinguish T-cell neoplasms, myelomonocytic neo-
plasms, and myeloid neoplasms with CD56 expres-
sion and CD41/CD561 hematodermatic neoplasm
from true NK cell neoplasms. The differential diag-
nostic features are proposed and summarized in
Table 2.
Treatment and PrognosisCD42/CD561 immature NK cell tumors (provisionalprecursor NK cell neoplasms)A standard treatment protocol for immature NK cell
neoplasms has not been established because of the
paucity of patients. Chemotherapy, non-Hodgkin
lymphoma, or acute lymphoblastic leukemia (ALL)
therapeutic strategies were the most common. How-
ever, the overall outcomes were dismal. Two pediatric
patients (Patients 1 and 3) (Table 1) who received
non-Hodgkin lymphoma therapy and ALL therapy,
respectively, followed by allogeneic hematopoietic
stem cell transplantation (HSCT) achieved complete
remission for 3 years. Three other patients (Patients
2, 4, and 5) who did not undergo bone marrow trans-
plantation died of disease between 6 months and 35
months. Further studies are necessary to determine
whether increased survival can be obtained with
aggressive chemotherapy followed by HSCT. It is pos-
sible that allogeneic HSCT could provide additional
graft versus leukemia/lymphoma benefit. The age of
disease onset also appears to be an important prog-
nostic factor. Two patients who were in remission
were pediatric patients (Patients 1 and 3). This obser-
vation is consistent with other studies.19 In the study
on CD561 blastic tumors by Suzuki et al., patients
aged >30 years had worse outcomes than patients
aged <30 years.19
Mature NK cell neoplasmsThe clinical outcome of patients with nasal NK cell
lymphoma is variable. Most observational studies
have demonstrated consistently that radiotherapy is
superior to chemotherapy alone in patients with
stage I/II disease.89–91 Some patients with early-stage
disease are cured by radiation therapy. It has been
demonstrated that radiotherapy, either as initial
treatment or as part of the chemotherapy regimen, is
the single most important key to a successful out-
come.66,90,93–96 However, some patients with early-
stage disease have early local or systemic recurrences
and die of disease. For patients with stage III/IV
disease, chemotherapy is the mainstay of treat-
ment.61 In several published series, the median sur-
vival of patients with advanced-stage disease was
approximately 12 months.62,70
Extranasal NK cell lymphomas are clinically
aggressive. Because the disease may be disseminated,
chemotherapy usually is the initial choice of treat-
ment.8 The response is poor, and most patients die
within 6 months after diagnosis.7,97 The long-term
remission rate with allogeneic HSCT reportedly is
<10%.67,92
Aggressive NK cell leukemia is a catastrophic dis-
ease with an almost uniform mortality. A few
patients have a clinical response with conventional
chemotherapy,61 although the response typically is
transient. Survival is measured in days to weeks.
Allogeneic HSCT reportedly results in short-term
remission in a few patients.98,99 To our knowledge,
no survival >1 year has been recorded.100
Patients with chronic NK cell lymphocytosis usu-
ally have an indolent clinical course and respond to
immunosuppressive therapy.77 Because of the poten-
tial long-term side effects of immunosuppressive
therapy, limiting specific therapy only to patients
with symptomatic disease is recommended.77
New therapeutic strategiesBecause of the inferior outcomes with current thera-
pies for NK cell neoplasms, novel approaches must
be considered to improve survival. Chemotherapeutic
agents currently being tested in cutaneous T-cell
lymphoma (CTCL) and peripheral T-cell lymphoma
(PTCL) provide possible new agents to consider for
NK cell treatment protocols. Examples of such agents
with efficacy in CTCL and/or PTCL include gemcita-
bine and liposomal doxorubicin as well as the purine
analogs, such as fludarabine and clardribine.101
Furthermore, the use of histone deacetylase inhibi-
tors (depsipeptide and vorinostat) is being tested in
CTCL.102,103 Monoclonal antibodies like alemtuzu-
mab have some activity in PTCL and are being inves-
tigated in combination with other therapy.101
Although no NK cell-specific antibodies are under
active development, the future availability of such
antibodies may offer novel treatment options. In
addition, a greater understanding of the signaling
pathways activated in NK cell neoplasms could make
other biologically targeted agents potential candi-
dates for inclusion in NK cell treatment protocols.
SummaryOverall, NK cell tumors are an uncommon, aggressive,
and heterogeneous group of disorders. Precursor NK
cell lymphoma/leukemia is an extremely rare clini-
copathologic entity that is characterized by blastic
morphology, CD32/CD42/CD561/CD132/CD332
immunophenotype with predominant CD94 1A
expression, TCR germline configuration, and lack of
1432 CANCER April 1, 2008 / Volume 112 / Number 7
TABLE
2Different
ialDiagn
osis
ofNatur
alKiller-cellNeo
plasms
Variab
lePr
ecur
sorNK
cell
neop
lasm
s(pro
vision
al)
CD41
CD56
1
hematod
ermic
neop
lasm
Mye
loid/N
Kce
llpr
ecur
sor
acut
eleuk
emia
(CD71
CD56
1M0)
Mye
lomon
ocytic/
mon
ocytic
tumor
sT-LB
L
Extran
odal
NK
cell
lymph
oma,
nasalt
ype
Aggressive
NK
cell
leuk
emia
Cello
rigin
ImmatureNKce
llPlasmac
ytoid
dend
ritic
cell
Mye
loid
prec
urso
rMye
loid
and/
ormon
ocytic
cell
ImmatureT-ce
llMatureNKce
llMatureNKce
ll
Major
orga
ninvo
lvem
ent
BM,L
NSk
inBM
,extramed
ullary
sites
BM,e
xtramed
ullary
sites
BM,m
ediastinum
,LN
Nasoc
avity
,extrana
soca
vity
Periph
eral
bloo
d,BM
Morph
olog
yBlastic
Blastoid
Blastic
Mye
loid/m
onoc
ytic
orblastic
Blastic
Pleo
morph
icce
llswith
angioinv
asion
andan
giod
estruc
tion
Maligna
ntlargegran
ular
lymph
ocytes
Cytop
lasm
icgran
ules
22
22/1
21
1Im
mun
ophe
notype
CD32
CD42
CD13
2
CD33
2CD56
1CD32
CD41
CD56
1CD32
CD71
CD13
/331
CD56
1CD32
CD41
CD13
/331
CD56
1CD31
CD56
�CD21
CD32
cCD3e
1CD56
1CD21
CD32
cCD32
1CD56
1
Other
marke
rs
MPO
22
<3%
1/2
22
2Ly
sozyme
22
21
22
2CD94
1A1
22
2CD94
1B2
21
1CD12
32
Strong
ly1
2Wea
kly1
22
2BD
CA-
22
1/2
22
22
2TC
L-1
21
22
1/2
22
TCRge
neGermlin
eGermlin
eGermlin
eGermlin
eRe
arrang
edGermlin
eGermlin
e
EBV
22
22
21
1
NKce
llindica
tesna
turalk
iller
cell;
T-LB
L,T-ce
lllymph
oblastic
lymph
oma/leuk
emia;B
M,b
onemarrow;L
N,lym
phno
de;2
,neg
ative;
1,p
ositive
;MPO
,mye
lope
roxida
se;B
DCA
-2,b
lood
dend
ritic
cellan
tigen
2;TC
R,T-ce
llrece
ptor;E
BV,E
pstein-B
arrvirus.
Natural Killer Cell Tumors/Liang and Graham 1433
EBV positivity. Extranodal NK cell lymphoma, nasal
type; aggressive NK cell leukemia; and chronic NK cell
lymphocytosis originate from mature NK cells and
have distinct geographic distribution. A consistent
association with EBV infection suggests that the virus
may be of pathogenetic significance in these sub-
types. Further studies are needed to define the molec-
ular pathogenesis and biologic markers that aid in the
diagnosis of NK cell neoplasms. Furthermore, clinical
trials and/or multi-institutional cooperation are
necessary to define the optimal therapeutic strategies
that will lead to better outcomes in patients with this
uncommon group of disorders.
REFERENCES1. Spits H, Lanier LL, Phillips JH. Development of human T
and natural killer cells. Blood. 1995;85:2654–2670.
2. Lanier LL, Spits H, Phillips JH. The developmental rela-
tionship between NK cells and T cells. Immunol Today.
1992;13:392–395.
3. Sanchez MJ, Muench MO, Roncarolo MG, et al. Identifica-
tion of a common T/natural killer cell progenitor in
human fetal thymus. J Exp Med. 1994;180:569–576.
4. Spits H, Blom B, Jaleco AC, et al. Early stages in the devel-
opment of human T, natural killer and thymic dendritic
cells. Immunol Rev. 1998;165:75–86.
5. Jaffe ES. Classification of natural killer (NK) cell and NK-
like T cell malignancies. Blood. 1996;87:1207–1210.
6. DiGiuseppe JA, Louie DC, Williams JE, et al. Blastic nat-
ural killer cell leukemia/lymphoma: a clinicopathologic
study. Am J Surg Pathol. 1997;21:1223–1230.
7. Chan JK, Sin VC, Wong KF, et al. Nonnasal lymphoma
expressing the natural killer cell marker CD56: a clinico-
pathologic study of 49 cases of an uncommon aggressive
neoplasm. Blood. 1997;89:4501–4514.
8. Siu LLP, Chan JKC, Kwong YL. Natural killer cell malignan-
cies: clinicopathologic and molecular features. Histol His-
topathol. 2002;17:539–554.
9. Chan JK, Wong KF, Jaffe ES, et al. Aggressive NK-cell leu-
kemia. In: Jaffe ES, Harris NL, Stein H, Vardiman JW. eds.
World Health Organization Classification of Tumours:
Pathology and Genetics, Tumours of Hematopoietic and
Lymphoid Tissue. Lyon, France: IARC Press; 2001:198–200.
10. Chan JK, Jaffe ES, Ralfkiaer E. Extranodal NK/T-cell lym-
phoma, nasal type. In: Jaffe ES, Harris NL, Stein H, Vardi-
man JW, eds. World Health Organization Classification of
Tumours: Pathology and Genetics, Tumours of Hemato-
poietic and Lymphoid Tissue. Lyon, France: IARC Press;
2001:204–207.
11. Chan JKC, Jaffe ES, Ralfkiaer E. Blastic NK-cell lymphoma.
In: Jaffe ES, Harris NL, Stein H, Vardiman JW., eds. World
Health Organization Classification of Tumours: Pathology
and Genetics, Tumours of Hematopoietic and Lymphoid
Tissue. Lyon, France: IARC Press; 2001:214–215.
12. Herling M, Teitell MA, Shen RR, et al. TCL 1 expression
in plasmacytoid dendritic cells (DC2s) and the related
CD41 CD561 blastic tumors of skin. Blood. 2003;101:
5007–5009.
13. Petrella T, Meijer C, Dalac S, et al. TCL1 and CLA expres-
sion in agranular CD4/CD56 hematodermic neoplasms
(blastic NK-cell lymphomas and leukemia cutis. Am J Clin
Pathol. 2004;122:307–313.
14. Chaperot L, Bendriss N, Manches O, et al. Identification
of a leukemic counterpart of the plasmacytoid dendritic
cells. Blood. 2001;97:3210–3217.
15. Jaffe ES, Chan JKC, Su IJ, et al. Report of the workshop on
nasal and related extranodal angiocentric T/natural killer
cell lymphomas. Am J Surg Pathol. 1996;20:103–111.
16. Sheibani K, Winberg CD, Burke JS, et al. Lymphoblastic
lymphoma expressing natural killer cell-associated anti-
gens: a clinicopathologic study of 6 cases. Leukemia Res.
1987;11:371–377.
17. Suzuki R, Nakamura S. Malignancies of natural killer (NK)
cell precursor: myeloid/NK cell precursor acute leukemia
and blastic NK cell lymphoma/leukemia. Leukemia Res.
1999;23:615–624.
18. Oshimi K. Leukemia and lymphoma of natural killer line-
age cells. Int J Hematol. 2003;78:18–23.
19. Suzuki R, Nakamura S, Suzumiya J, et al. Blastic natural
killer cell lymphoma/leukemia (CD56-positive blastic tu-
mor): prognostication and categorization according to
anatomic sites of involvement. Cancer. 2005;104:1022–
1031.
20. Lin CW, Liu TY, Chen SU, et al. CD94 1A transcripts char-
acterize lymphoblastic lymphoma/leukemia of immature
natural killer cell origin with distinct clinical features.
Blood. 2005;106:3567–3574.
21. Graham DK, Liang X, Miller KL, et al. Disseminated naso-
pharyngeal natural killer cell lymphoblastic lymphoma in
a child. Med Pediatr Oncol. 2003;40:251–253.
22. Adachi M, Maeda K, Takekawa M, et al. High expression
of CD56 (N-CAM) in a patient with cutaneous CD4-posi-
tive lymphoma. Am J Hematol. 1994;47:278–282.
23. Brody JP, Allen S, Schulman P, et al. Acute agranular
CD4-positive natural killer cell leukemia: comprehensive
clinicopathologic studies including virologic and in vitro
culture with inducing agents. Cancer. 1995;75:2474–
2483.
24. Waski MA, Sackstein R, Novick, et al. Cutaneous CD561large T-cell lymphoma associated with high serum con-
centration of IL-2. Hum Pathol. 1996;27:738–744.
25. Dummer R, Potoczna N, Haffner AC, et al. A primary
cutaneous non-T, non-B CD41CD561 lymphoma. Arch
Dermatol. 1996;132:550–553.
26. Bastian BC, Ott G, Muller-Deubert S, et al. Primary cuta-
neous natural killer/T-cell lymphoma. Arch Dermatol.
1998;134:109–111.
27. Savoia P, Fierro MT, Novelli M, et al. CD56 positive cuta-
neous lymphoma: a poorly recognized entity in the spec-
trum of primary cutaneous disease. Br J Dermatol. 1997;
137:966–971.
28. Falco RP, Garcia AB, Margues MG, et al. Blastic CD4 NK
cell leukemia/lymphoma: a distinct clinical entity. Leuke-
mia Res. 2002;26:803–807.
29. Child EJ, Mitchell TJ, Whittaker SJ, et al. Blastic natural
killer cell and extranodal natural killer cell-like T-cell lym-
phoma presenting in the skin: report of 6 cases from the
U.K. Br J Dermatol. 2003;148:507–515.
30. Chang SE, Choi HJ, Huh J, et al. A case of primary cuta-
neous CD561, TdT1, CD41, blastic NK-cell lymphoma in
a 19-year-old woman. Am J Dermatopathol. 2002;24:72–
75.
31. Penven K, Macro M, Salaun V, et al. Skin manifestations
in CD41, CD561 malignancies. Eur J Dermatol.
2003;13:161–165.
32. Shapiro M, Wasik MA, Junkins-Hopkins JM, et al. Com-
plete remission in advanced blastic NK-cell lymphoma/
1434 CANCER April 1, 2008 / Volume 112 / Number 7
leukemia in elderly patients using hyper-CVAD regimen.
Am J Hematol. 2003;74:46–51.
33. Mori KL, Egashira M, Oshimi K. Differentiation stage of
natural killer cell-lineage lymphoproliferative disorders
based non phenotypic analysis. Br J Haematol. 2001;115:
225–228.
34. Kern WF, Spier CM, Miller TP, et al. NCAM (CD56)-posi-
tive malignant lymphoma. Leukemia Lymphoma. 1993;12:
1–8.
35. Almasri NM, Mitchell D, Braylan RC. Blastic natural killer
cell [letter]. Am J Surg Pathol. 1999;23:991–992.
36. Carayol G, Robin C, Bourhis JH, et al. NK cells differen-
tiated from bone marrow, cord and peripheral blood stem
cells exhibit similar phenotype and functions. Eur J
Immunol. 1998;28:1991–2002.
37. Berardi AC, Meffre E, Pflumio F, et al. Individual
CD341CD38lowCD19-CD10-progenitor cells from human
cord blood generate B lymphocytes and granulocytes.
Blood. 1997;89:3554–3564.
38. Feuillard J, Jacob MC, Valensi F, et al. Clinical and biologic
features of CD41 CD561 malignancies. Blood. 2002;99:
1556–1563.
39. Petrella T, Comeau MR, Maynadie M, et al. ‘‘Agranular
CD41 CD561 hematodermic neoplasm’’ (blastic NK-cell
lymphoma) originated from a population of CD561 pre-
cursor cells related to plasmacytoid monocytes. Am J Surg
Pathol. 2002;26:852–862.
40. Joye DL, Geigerman CM, Herling M, et al. The pattern of
expression of the plasmacytoid dendritic cell marker
BDCA-2 supports a spectrum of maturation among CD41CD561 blastoid tumors. Mod Pathol. 2006;19:1555–1562.
41. Facchetti F, Vermi W. Plasmacytoid monocytes and plas-
macytoid dendritic cells: immune system cells linking
innate and acquired immunity [in Italian]. Pathologica.2002;94:163–175.
42. Herling M, Jones D. CD41/CD561 hematodermic tumor:
the features of an evolving entity and its relationship to
dendritic cells. Am J Clin Pathol. 2007;127:687–700.
43. Willemze R, Jeffe ES, Burg G, et al. WHO-EORTC classifi-
cation for cutaneous lymphomas. Blood. 2005;105:3768–
3785.
44. Liang X, Greffe B, Garrington T, Graham DK. Precursor
natural killer cell leukemia. Pediar Blood Cancer. 2007 Apr
6 [Epub ahead of print].
45. Dubois SG, Etzell JE, Matthay KK, et al. Pediatric acute
blastic natural killer cell leukemia. Leukemia Lymphoma.
2002;43:901–906.
46. Hyakuna N, Toguchi S, Higa T, et al. Childhood blastic NK
cell leukemia successfully treated with L-asparaginase
and allogeneic bone marrow transplantation. Pediatr
Blood Cancer. 2004;42:631–634.
47. Matano S, Nakamura S, Nakamura S, et al. Monomorphicagranular natural killer cell lymphoma/leukemia with no
Epstein-Barr virus association. Acta Haematol. 1999;101:
206–208.
48. Tamura H. Ogata K, Mori S, et al. Lymphoblastic
lymphoma of natural killer cell origin, presenting as pan-
creatic tumour. Histopathology. 1998;32:508–511.
49. Petrella T, Bagot M, Willemze R, et al. Blastic NK-cell lym-
phomas (agranular CD41CD561 hematodermic neo-
plasms). Am J Clin Pathol. 2005;123:662–675.
50. Chang C, Rodriguez A, Carreterro M, et al. Molecular
characterization of human CD94: a type II membrane gly-
coprotein related to the C-type lectin superfamily. Eur J
Immunol. 1995;9:2433–2437.
51. Lopez-Botet M, Perez-Villar JJ, Carreterro M, et al. Struc-
ture and function of the CD94 C-type lectin receptor
complex involved in recognition of HLA class I molecules.
Immmunol Rev. 1997;155:165–174.
52. Scott AA, Head DR, Kopecky KJ, et al. HLA-DR2, CD331,
CD561, CD162 myeloid/natural killer cell acute leukemia:
a previously unrecognized form of acute leukemia poten-
tially misdiagnosed as French-American-British acute
myeloid leukemia-M3. Blood. 1994;84:244–255.
53. Suzuki R, Yamamoto K, Seto M, et al. CD71 and CD51myeloid/natural killer cell precursor acute leukemia: a
distinct hematolymphoid disease entity. Blood. 1997;90:
2417–2428.
54. Nagai M, Bandoh S, Tasaka T, et al. Secondary myeloid/
natural killer cell precursor acute leukemia following
essential thrombocytopenia. Hum Pathol. 1999;30:868–
871.
55. Inaba T, Shimazaki C, Sumikuma T, et al. Clinicopatholo-
gical features of myeloid/natural killer (NK) cell precursor
acute leukemia. Leukemia Res. 2001;25:109–113.
56. Handa H, Motohashi S, Isozumi K, et al. CD71 and
CD561 myeloid/natural killer cell precursor acute leuke-
mia treated with idarubicin and cytosine arabinoside.
Acta Haematol. 2002;108:47–52.
57. Ikewaki J, Otsuka E, Satou J, et al. Myeloid/natural killer
cell precursor acute leukemia with minor bcr/abl mRNA
transcript. Br J Haematol. 2002;118:684–685.
58. Tezuka K, Nakayama H, Honda K, et al. Treatment of a
child with myeloid/NK cell precursor acute leukemia with
L-asparaginase and unrelated cord blood transplantation.
Int J Hematol. 2002;75:201–206.
59. Seymour JF, Pierce SA, Kantarjian HM, Keating MJ, Estey
EH. Investigation of karyotypic, morphologic and clinical
features in patients with acute myeloid leukemia blast
cells expressing the neural cell adhesion molecule (CD56).
Leukemia. 1994;8:823–826.
60. Suzuki R, Murata M, Kami M, et al. Prognostic signifi-
cance of CD71CD561 phenotype and chromosome 5
abnormalities for acute myeloid leukemia M0. Int J
Hematol. 2003;77:482–489.
61. Kwong YL. Natural killer-cell malignancies: diagnosis and
treatment. Leukemia. 2005;19:2186–2194.
62. Cheung MM, Chan JK, Lau WH, et al. Primary non-
Hodgkin’s lymphoma of the nose and nasopharynx: clin-
ical features, tumor immunophenotype, and treatment
outcome in 113 patients. J Clin Oncol. 1998;16:70–
77.
63. Cuadra-Garcia I, Proulx GM, Wu CL, et al. Sinonasal lym-
phoma: a clinicopathologic analysis of 58 cases from the
Massachusetts General Hospital. Am J Surg Pathol.
1999;23:1356–1369.
64. Gaal K, Sun NC, Hernandez AM, et al. Sinonasal NK/T-
cell lymphomas in the United States. Am J Surg Pathol.
2000;24:1511–1517.
65. Kim CE, Cho JH, Yang WI, et al. Angiocentric lymphoma
of the head and neck: patterns of systemic failure after
radiation treatment. J Clin Oncol. 2000;18:54–63.
66. Chim CS, Ma SY, Au WY, et al. Primary nasal natural killer
cell lymphoma: long-term treatment outcome and rela-
tionship with the International Prognostic Index. Blood.
2004;103:216–221.
67. Davison SP, Habermann TM, Strickler JG, et al. Nasal and na-
sopharyngeal lymphomas. Laryngoscope. 1996;106:139–143.
68. Imamura N, Kisunoki Y, Kajihara H, et al. Aggressive nat-
ural killer cell leukemia/lymphoma with N901-positive
Natural Killer Cell Tumors/Liang and Graham 1435
surface phenotype: evidence for the existence of a third
lineage in lymphoid cells. Acta Hematol. 1988;80:121–128.
69. Imamura N, Kisunoki Y, Kawa-Ha K, et al. Aggressive nat-
ural killer cell leukemia/lymphoma: report of 4 cases and
review of the literature. Possible existence of a new clini-
cal entity originating from the third lineage of lymphoid
cells. Br J Hematol. 1990;75:49–59.
70. Kwong YL, Chan AC, Liang R, et al. CD561 NK lympho-
mas: clinicopathological features and prognosis. Br J Hae-
matol. 1997;97:821–829.
71. Mori N, Yamashita Y, Tsuzuki T, et al. Lymphomatous fea-
tures of aggressive NK cell leukaemia/lymphoma with
massive necrosis, haemophagocytosis and EB virus infec-
tion. Histopathology. 2000;37:363–371.
72. Yatabe Y, Mori N, Hirabayashi N, et al. Natural killer cell
leukemia, an autopsy case. Arch Pathol Lab Med. 1994;
118:1201–1204.
73. Quintanilla-Martinez L, Jaffe ES. Aggressive NK cell lym-
phomas: insights into the spectrum of NK cell derived
malignancies. Histopathology. 2000;37:372–374.
74. Oshimi K, Yamada O, Kaneko T, et al. Laboratory findings
and clinical courses of patients with granular lympho-
cyte-proliferative disorders. Leukemia. 1993;7:782–788.
75. Tefferi A, Li C-Y, Witzig TE, et al. Chronic natural killer
cell lymphocytosis: a descriptive clinical study. Blood.
1994;84:2721–2725.
76. Morice WG, Leibson PJ, Tefferi A. Natural killer cells and
the syndrome of chronic natural killer cell lymphocytosis.
Leuk Lymphoma. 2004;41:277–284.
77. Tefferi A. Chronic natural killer cell lymphocytosis. Leuk
Lymphoma. 1996;20:245–248.
78. Ryder J, Wang X, Bao L, et al. Aggressive natural killer cell
leukemia: report of a Chinese series and review the litera-
ture. Int J Hematol. 2007;85:18–25.
79. Oshimi K, Kawa K, Nakamura S, et al. NK-cell neoplasms
in Japan. Hematology. 2005;10:237–245.
80. Weiss LM, Arber DA, Strickler JG. Nasal T-cell lymphoma.
Ann Oncol. 1994;5(suppl 1):S39–S42.
81. Tao Q, Ho FCS, Loke SL, et al. Epstein-Barr virus is loca-
lized in the tumor cells of nasal lymphomas of NK, T or B
cell types. Int J Cancer. 1995;60:315–320.
82. Medeiros LJ, Peiper SC, Elwood L, et al. Angiocentric
immunoproliferative lesions: a molecular analysis of 8
cases. Hum Pathol. 1991;22:1150–1157.
83. Minarovits J, Hu LF, Imai S, et al. Clonality, expression
and methylation patterns of the EBV genomes in lethal
midline granulomas classified as peripheral angiocentric
T-cell lymphomas. J Gen Virol. 1994;75:77–84.
84. Wong KF, Zhang YM, Chan JKC. Cytogenetic abnormalities
in natural killer cell lymphoma/leukemia: Is there a con-
sistent pattern? Leuk Lymphoma. 1999;34:241–250.
85. Zhang Y, Matthiesen P, Harder S, et al. A 3-cM commonly
deleted region in 6q21 in leukemias and lymphomas deli-
neated by fluorescence in situ hybridization. Genes Chro-
mosomes Cancer. 2000;27:52–58.
86. Sun HS, Su IJ, Lin YC, et al. A 2.6 Mb interval on chromo-
some 6q25.2-q25.3 is commonly deleted in human nasal
natural killer/T-cell lymphoma. Br J Haematol. 2003;122:
590–599.
87. Siu LL, Wong KF, Chan JK, et al. Comparative genomic
hybridization analysis of natural killer cell lymphoma/leu-
kemia. Recognition of consistent pattern of genetic altera-
tions. Am J Pathol. 1999;155:1419–1425.
88. Siu LL, Chan V, Chan JK, et al. Consistent patterns of alle-
lic loss in natural killer cell lymphoma. Am J Pathol.
2000;157:1803–1809.
89. Sakata K, Hareyama M, Ohuchi A, et al. Treatment of le-
thal midline granuloma type nasal T-cell lymphoma. Acta
Oncol. 1997;36:307–311.
90. Koom WS, Chung EJ, Yang WI, et al. Angiocentric T-cell
and NK/T-cell lymphomas: radiotherapeutic viewpoints.
Int J Radiat Oncol Biol Phys. 2004;59:1127–1137.
91. Robbins KT, Fuller LM, Vlasak M, et al. Primary lympho-
mas of the nasal cavity and paranasal sinuses. Cancer.
1985;56:814–819.
92. Cheung MM, Chan JK, Wong KF. Natural killer cell
neoplasms: a distinctive group of highly aggressive
lymphoma/leukemias. Semin Hematol. 2003;40:221–
232.
93. Cheung MM, Chan KF, Lau WH, et al. Early stage nasal
NK/T-cell lymphoma: clinical outcome, prognostic fac-
tors, and the effect of treatment modality. Int Radiat
Oncol Biol Phys. 2002;54:182–190.
94. You JY, Chi KH, Yang MH, et al. Radiation therapy versus
chemotherapy as initial treatment for localized nasal nat-
ural killer (NK)/T-cell lymphoma: a single institute survey
in Taiwan. Ann Oncol. 2004;15:618–625.
95. Ribrag V, Ell Hajj M, Janot F, et al. Early locoregional high-
dose radiotherapy is associated with long-term disease
control in localized primary angiocentric lymphoma of
the nose and nasopharynx. Leukemia. 2001;15:1123–
1126.
96. Li CC, Tien HF, Tang JL, et al. Treatment outcome and
pattern of failure in 77 patients with sinonasal natural
killer/T-cell or T-cell lymphoma. Cancer. 2004;100:366–
375.
97. Kern WF, Spier CM, Hanneman EH, et al. Neural cell ad-
hesion molecule-positive peripheral T-cell lymphoma: a
rare variant with propensity for unusual sites of involve-
ment. Blood. 1992;79:2432–2437.
98. Ebihara Y, Manabe A. Tanaka R, et al. Successful treat-
ment of natural killer (NK) cell leukemia following a long-
standing chronic active Epstein-Barr virus (CAEBV) infec-
tion with allogeneic bone marrow transplantation. Bone
Marrow Transplant. 2003;31:1169–1171.
99. Okamura T, Kishimoto T, Inoue M, et al. Unrelated bone
marrow transplantation for Epstein-Barr virus-associated
T/NK-cell lymphoproliferative disease. Bone Marrow
Transplant. 2003;31:105–111.
100. Kwong YL, Chan AL, Liang RHS. Natural killer cell lym-
phoma/leukemia: pathology and treatment. Hematol
Oncol. 1997;15:71–79.
101. Greer JP. Therapy of peripheral T/NK neoplasms. Hematol
Am Soc Hematol Educ Program. 2006;:331–337.
102. Piekarz RL, Robey R, Sandor V, et al. Inhibitor of histone
deacetylation, depsipeptide (FR901228), in the treatment
of peripheral and cutaneous T-cell lymphoma: a case
report. Blood. 2001;98:2865–2868.
103. Duvic M, Talpur R, Ni X, et al. Phase 2 trial of oral vorino-
stat (suberoylanilide hydroxamic acid, SAHA) for refrac-
tory cutaneous T-cell lymphoma (CTCL). Blood. 2007;
109:31–39. Erratum in: Blood. 2007;109:5086.
1436 CANCER April 1, 2008 / Volume 112 / Number 7