Embed Size (px)
Citation preview

National Institute of Mental HealthTreatment of Depression CollaborativeResearch ProgramGeneral Effectiveness of Treatments
Irene Elkin, PhD; M. Tracie Shea, PhD; John T.Watkins,PhD; Stanley D.Imber, PhD; Stuart M.Sotsky, MD; Joseph F. Collins, ScD;David R. Glass, PhD; Paul A. Pilkonis, PhD; William R. Leber, PhD; John P. Docherty, MD; Susan J. Fiester, MD; Morris B. Parloff, PhD
\s=b\We investigated the effectiveness of two brief psychothera-pies, interpersonal psychotherapy and cognitive behavior thera-py, for the treatment of outpatients with major depressive disor-der diagnosed by Research Diagnostic Criteria. Two hundredfifty patients were randomly assigned to one of four 16-weektreatment conditions: interpersonal psychotherapy, cognitivebehavior therapy, imipramine hydrochloride plus clinical man-
agement (as a standard reference treatment), and placebo plusclinical management. Patients in all treatments showed signifi\x=req-\cant reduction in depressive symptoms and improvement infunctioning over the course of treatment. There was a consistentordering of treatments at termination, with imipramine plus clini-cal management generally doing best, placebo plus clinical man-
agement worst, and the two psychotherapies in between butgenerally closer to imipramine plus clinical management. In ana-
lyses carried out on the total samples without regard to initialseverity of illness (the primary analyses), there was no evidenceof greater effectiveness of one of the psychotherapies as com-
pared with the other and no evidence that either of the psycho-therapies was significantly less effective than the standardreference treatment, imipramine plus clinical management.
Comparing each of the psychotherapies with the placebo plusclinical management condition, there was limited evidence of thespecific effectiveness of interpersonal psychotherapy and nonefor cognitive behavior therapy. Superior recovery rates werefound for both interpersonal psychotherapy and imipramine plusclinical management, as compared with placebo plus clinicalmanagement. On mean scores, however, there were few signifi-cant differences in effectiveness among the four treatments inthe primary analyses. Secondary analyses, in which patientswere dichotomized on intial level of severity of depressive symp-toms and impairment of functioning, helped to explain the rela-tive lack of significant findings in the primary analyses. Signifi-cant differences among treatments were present only for thesubgroup of patients who were more severely depressed and func-tionally impaired; here, there was some evidence of the effective-ness of interpersonal psychotherapy with these patients andstrong evidence of the effectiveness of imipramine plus clinicalmanagement. In contrast, there were no significant differencesamong treatments, including placebo plus clinical management,for the less severely depressed and functionally impaired patients.
(Arch Gen Psychiatry. 1989;46:971-982)
The National Institute of Mental Health (NIMH) (Rock-ville, Md) Treatment of Depression Collaborative
Research Program was the first multisite coordinated studyinitiated by the NIMH in the field ofpsychotherapy. The studyhad two major aims: (1) to test the feasibility and value of thecollaborative clinical trial model (a model frequently used inthe field ofpsychopharmacology) in the area ofpsychotherapyresearch and (2) to study, within this research model, theeffectiveness of two specific forms ofpsychotherapy (cognitivebehavior therapy [CBT] and interpersonal psychotherapy[IPT]) for treating nonbipolar, nonpsychotic depressed outpa¬tients. The study did prove to be feasible. Future publications
Accepted for publication March 2,1989.From the Mood, Anxiety and Personality Disorders Research Branch, Na-
tional Institute of Mental Health, Bethesda, Md (Drs Elkin and Shea); Depart-ment of Psychiatry and Behavioral Sciences, University of Oklahoma HealthSciences Center, Oklahoma City (Drs Watkins and Leber); University ofPittsburgh (Pa) School of Medicine and Western Psychiatric Institute andClinic (Drs Imber and Pilkonis); Department of Psychiatry and BehavioralSciences, George Washington University Medical Center, Washington, DC(Drs Sotsky and Glass); Cooperative Studies Program Coordinating Center,Veterans Administration Medical Center, Perry Point, Md (Dr Collins); Nash-ua Brookside Hospital, Nashua, NH (Drs Docherty and Fiester); and TheAmerican University, Washington, DC (Dr Parloff).
Reprint requests to National Institute of Mental Health Treatment of De-pression Collaborative Research Program, 5600 Fishers Ln, Room 10C-26,Rockville, MD 20857 (Dr Elkin).
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

will discuss the benefits and the problems ofusing the collabo¬rative clinical trial model in psychotherapy research. Thepresent article reports initial outcome findings for the twopsychotherapies, in the areas of depressive symptoms andoverall functioning. The general background of this collabora¬tive study has already been described by Elkin et al,1 andreaders are referred to that article for details regarding histo¬ry, rationale, design, and procedures of the study.
Although initial efficacy findings for both CBT and IPT hadbeen promising,2"1 they had not previously been compared direct¬ly with each other. The present study constituted the first directcomparison of these two psychotherapeutic approaches for thetreatment of depressed outpatients. In addition, it providedmore neutral settings for studying these two psychotherapies,each of which had previously been studied largely in settingsstrongly identified with the respective treatment.
lb evaluate the effectiveness of the psychotherapies, theywere compared with a reference treatment condition, ie, atreatment that had already been found to be effective with thispatient population. Since there was no specific form ofpsycho¬therapy that research had definitively established as effica¬cious with depressed patients, pharmacotherapy with a tricy¬clic antidepressant drug, imipramine hydrochloride, servedas the reference condition in the current study. Considerableresearch evidence was available, at the time this study was
planned, for the efficacy of imipramine.56 Since there was
variability, however, in both imipramine and placebo re¬
sponse rates, and since most studies had been on inpatientsamples, it was necessary to establish the effectiveness ofimipramine at these sites and with these outpatient samples.For that reason, a pill-placebo condition was also included inthe study. To standardize clinical care in the two pharmacoth¬erapy conditions, a "clinical management" (CM) componentwas developed.
In comparisons of the four treatment conditions in thisstudy, the two major questions addressed were the following:(1) Is there evidence of the effectiveness of each of the psy¬chotherapies, as compared both with the standard referencetreatment of imipramine-CM and with the placebo plus CM(PLA-CM) control condition? (2) Are there any differences inthe effectiveness of the two psychotherapies?
The present article will focus on the general effectiveness ofthese treatments in reducing depressive symptoms and im¬proving patients' functioning. These are major targets ofchange in any treatment ofdepression. The results presented,particularly on measures of depressive symptoms, will becomparable with those reported in previous studies compar¬ing CBT or IPT with antidepressant drugs.2'4,7,8 To test ade¬quately the effectiveness of these treatments, however, it isalso necessary to evaluate changes in attitudes and behaviorsspecifically targeted by each of the psychotherapies. A reportby Imber and colleagues9 addressed this issue ofmode-specificeffects.
The findings to be presented herein are limited to outcomeat termination of treatment. The issue of the temporal patternof therapeutic effects, particularly the important question ofwhether any of the treatments studied has more rapid effects,is addressed in a report by Watkins et al.10 Finally, the possi¬bility that certain patient characteristics may differentiallypredict improvement in the different treatment conditions isexplored in a report by Sotsky et al." All of these aspects ofoutcome, as well as patient status during follow-up, will haveto be considered for a comprehensive picture of the study'sfindings.
PATIENTS AND METHODS
The research design and methods have been described in detail1and will only be summarized here. At each of three research sites,
patients were randomly assigned to the four treatment conditions:CBT, IPT, imipramine-CM, and PLA-CM. A total of 250 patientswere assigned to treatment: 82 at the University of Pittsburgh (Pa)and 84 each at George Washington University (Washington, DC) andthe University of Oklahoma (Oklahoma City).
Patients
The major referral sources for the program were psychiatric outpa¬tient services at each research site, self-referrals, and other mentalhealth facilities. Prospective patients were prescreened to rule outthose who were clearly ineligible for the study. The 560 patients whopassed prescreening were then interviewed by a clinical evaluatorusing the Schedule for Affective Disorders and Schizophreniainterview.12
To be included in the study, patients had to meet Research Diagnos¬tic Criteria13 for a current episode of definite major depressive disor¬der (with the additional criterion that the required symptoms had tobe present for at least the previous 2 weeks) and had to have a score of14 or greater on an amended version of the 17-item Hamilton RatingScale for Depression (HRSD).14,1" (The amended scale includes itemsfor hypersomnia, hyperphagia, and weight gain.)
Exclusion criteria included specific additional psychiatric disorders(definite bipolar II and probable or definite bipolar I, panic disorder,alcoholism, drug use disorder, antisocial personality disorder, Bri¬quet's syndrome, and Research Diagnostic Criteria diagnosis of majordepressive disorder, psychotic subtype), two or more schizotypalfeatures, history of schizophrenia, organic brain syndrome, mentalretardation, concurrent treatment, presence of specific physical ill¬ness or other medical contraindications for the use of imipramine, andpresence of a clinical state inconsistent with participating in theresearch protocol, eg, current active suicide potential or need forimmediate treatment.
Patients passing clinical screening received a complete medicalevaluation. A 7- to 14-day wait and drug washout period followed; atthe end of this period, patients returned for a rescreening interviewwith the clinical evaluator. The 250 patients who passed rescreeningand who had given informed consent for all study procedures, includ¬ing random assignment, were then entered into the program. Assign¬ment of patients to treatment conditions was based on a separatecomputer-generated random order for each site.
TherapistsA different group of experienced therapists conducted treatment in
each of the conditions, with the exception of the two pharmacotherapyconditions, which were carried out double blind by the same thera¬pists. A total of 28 therapists (10 psychologists and 18 psychiatrists)took part in the outcome study, 8 in CBT and 10 each in IPT andpharmacotherapy. The preponderance of psychiatrists (64%) was
largely due to the need to include only psychiatrists in the pharma¬cotherapy conditions. Details regarding selection, training, and certi¬fication of therapists are provided elsewhere.16"18
The average age of the therapists was 41.5 years (range, 30 to 60years), and they had an average of 11.4 years of clinical experience(range, 2 to 27 years). Twenty (71%) were male. Patients wereassigned to therapists within treatments according to availability.Each psychotherapist saw between 3 and 11 patients (except for onetherapist who moved after seeing 1 patient), and each pharmacothera-pist saw between 3 and 9 patients in each of the two pharmacotherapyconditions.
Treatments
A major focus in this study was the careful definition, or standard¬ization, of each of the treatments so that conclusions could be drawnregarding their specific effects. Each of the four treatment conditionswas carried out in accord with a detailed manual describing thetheoretical underpinning of the approach, the general strategies in¬volved, the major techniques that could be used, and suggestions fordealing with specific problems. During the training/pilot phase of thisstudy, the therapists all received further training in their respectiveapproaches, met competence criteria in carrying out the treatmentsas described in the protocol, and were monitored throughout theoutcome study. Detailed descriptions of each of the treatments can befound in the revised versions of the manuals, which have all beenpublished.19"21
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

CBT. —Cognitive behavior therapy was conducted as described byBeck and colleagues." The cognitive therapist uses strategies andtechniques designed to help depressed patients correct their nega¬tive, distorted views about themselves, the world, and the future, andthe underlying maladaptive beliefs that gave rise to these cognitions.
IPT. —Interpersonal psychotherapy was conducted as describedby Klerman et al.20 The IPT therapist seeks to help the patient toidentify and better understand his or her interpersonal problems andconflicts and to develop more adaptive ways of relating to others.
Imipramine-CM.—The pharmacotherapy conditions were con¬ducted as described by Fawcett and colleagues.21 Medication wasadministered double blind within the context of a CM session (seeplacebo condition below). The average dosage for imipramine hydro¬chloride completers, averaged over all weeks after the first 2 weeks oftreatment, was 185 mg, with 95% of the patients receiving at least 150mg. The median plasma level of imipramine plus desmethylimipra-mine for patients completing treatment was 163 ng/mL at 4 weeks and231 ng/mL at 8 weeks.
PLA-CM.—The pill-placebo condition was administered doubleblind, within the context of a CM session. The CM component of bothpharmacotherapy conditions was introduced into the study to ensurestandard clinical care, to maximize compliance, and to address ethicalconcerns regarding use of a placebo with depressed patients. The CMcomponent provided guidelines, not only for the management of medi¬cation and side effects and review of the patient's clinical status, butalso for providing the patient with support and encouragement anddirect advice if necessary. Although specific psychotherapeutic inter¬ventions were proscribed (especially those that might overlap withthe two psychotherapies), the CM component approximated a "mini¬mal supportive therapy" condition.
The placebo served primarily as a control condition for establishingthe adequacy of imipramine as a standard reference condition in thisstudy. The study would, ideally, also have included a "psychotherapy-placebo" condition against which to evaluate the specific effectivenessof each of the psychotherapies. A great deal has been written over theyears about the conceptual, ethical, and practical problems of estab¬lishing psychotherapy placebos.22"24 Despite concerted efforts, no psy¬chotherapy-placebo condition could be devised for this study that metethical concerns yet would not in itself constitute a new "treatment"rather than a "placebo." In the absence of a psychotherapy-placebocontrol, each of the psychotherapies was also compared with thecontrol condition of pill-placebo plus CM.
All treatments were planned to be 16 weeks in length, with a rangeof 16 to 20 sessions, as described previously.1 The actual averagenumber ofsessions for completers was 16.2; for early terminators, 6.2;and for the total sample, 13.0. Psychotherapy sessions were 50 min¬utes long. The initial pharmacotherapy session was 45 to 60 minuteslong, with other sessions 20 to 30 minutes long.
To determine whether therapists were adhering to their respectiveapproaches and whether the treatments (especially the psychothera¬pies) could be differentiated from one another, the CollaborativeStudy Psychotherapy Rating Scale was developed by Hollon andcolleagues25 and applied by Hill26 to outcome study audiotapes. Thetreatment approaches were reliably differentiated, with audiotapescorrectly classified more than 95% of the time. These findings, as wellas the scale development, will be described in future publications.
Outcome Assessment
The patients were assessed before treatment, at several pointsduring treatment (4, 8, and 12 weeks), at termination, and at 6-, 12-,and 18-month follow-up, on a battery of assessment instruments.1This article will focus on outcome at termination of treatment, onmeasures of depressive symptoms, overall symptoms, and generalfunctioning, from the perspectives of the clinical evaluator and thepatient.
Four scales were identified a priori as major measures for the initialoutcome analyses reported in this article: from the perspective of theclinical evaluator, the 17-item HRSD14,15 and the Global AssessmentScale (GAS)27; and from the perspective of the patient, the BeckDepression Inventory (BDI)28'29 and the Hopkins Symptom Check-list-90 Total Score (HSCL-90 T).30 These are established instrumentsfor the measurement of depressive symptoms (HRSD and BDI),overall symptoms (HSCL-90 T), and general level of functioning(GAS). The HRSD and the BDI have also been used in other studiescomparing either IPT or CBT with tricyclic drugs.2"4,7,8,31
The HRSD used in this study was a modified version of Hamilton'sscale. The scores presented in this article are based on the first 17items, comparable with those reported most frequently in the litera¬ture. The HRSD and GAS were rated by a trained clinical evaluatorfollowing a semistructured interview, the Schedule for AffectiveDisorders and Schizophrenia—Change version.32 In three reliabilitystudies (one just before and two during the outcome study), intraclasscorrelations were calculated for clinical evaluator ratings of a commonset of videotaped interviews. Intraclass correlations, across sites,ranged from .93 to .96 for the HRSD and from .83 to .88 for the GAS.
Statistical Analysis
The major analyses of outcome were 3x4 (sites x treatments) ana¬lyses of covariance (ANCOVAs) of mean scores on the four measuresand 2 analyses of categorical data (recovered/not recovered by treat¬ment) on the HRSD and BDI. These were followed by analyses ofdifferences between each pair of treatments. Paired t tests were usedto assess change from pretreatment to posttreatment within each ofthe treatment conditions. To test the effect on outcome of the initialseverity of the patient's depression, secondary 2x4 (level of severity treatments) ANCOVAs were carried out, with subsequent pair-wise comparisons. Analyses of recovery data by 2 were also carriedout within severity subgroups. Univariate, rather than multivariate,ANCOVAs were used so as not to obscure any differences in outcomedue to rater perspective, differences frequently observed in studies ofpsychotherapy.33 We also wished to ensure the separate analysis ofthe HRSD and BDI, to facilitate comparisons with previous studies.
Marital status, which was significantly related to outcome, was notdistributed evenly across treatment groups and could thus bias thefindings. For this reason, it was always used as a covariate in theANCOVAs. Pretreatment scores on the dependent variable were alsoincluded as a covariate, except in those few instances on the HRSDand GAS in which there was significant (P<.05) heterogeneity ofregression and the use of a pooled regression for the ANCOVA wasnot justified. In these instances, the ANCOVAs reported used onlymarital status, and not pretreatment score, as a covariate. The pres¬ence of significant heterogeneity of regression suggests that thetreatments act differentially for patients who have initial high vs lowpretreatment scores on the variable in question. This issue is ad¬dressed in the secondary analyses, in which patients were divided intotwo severity groups on the basis of a priori cutting scores on thepretreatment HRSD (5=20 vs <20) and on the pretreatment GAS («50vs >50). These severity analyses will help to clarify the role played bypretreatment levels of these variables.
Outcome data analyses were conducted on three samples ofpatients:
1. The completer sample included all patients who completed atleast 12 sessions and at least 15 weeks of treatment. Although therewere 162 completers, data analyses were based on 155 patients, sincetermination evaluations were not available for seven patients.
2. The end point 204 sample included all patients who received atleast 3.5 weeks of treatment (which generally included at least fourtreatment sessions). The 204 patients include the 162 completers plus42 patients who dropped out or were withdrawn after 3.5 weeks oftreatment. In this sample, the last score obtained, either at interim orearly termination evaluation, was used for the patients who droppedout or were withdrawn from the study.
3. The end point 239 sample consisted of all patients who enteredtreatment. This is also an end point sample, but it includes an addition¬al 35 patients who dropped out or were withdrawn before 3.5 weeks oftreatment. Twenty of these patients did not have interim or termina¬tion evaluations, and, to include them in the analyses, rescreening orintake scores were used as their end point scores. Examination of ourdata suggests that these scores represent a reasonable estimate oftermination status.
These are clearly not independent samples; each successive sampleincludes the previous one. Some researchers choose to report findingson one or another of these samples. To get a comprehensive picture ofthe outcome of the treatments in this study, we analyzed data from allthree samples. The completer analysis best reflects treatment effectsfor those patients who have received a full course of treatment, animportant focus in any treatment study. This analysis does not,however, take into account any possible biases due to differentialattrition in the different treatment conditions. The analysis of endpoint samples attempts to address this problem by including termina-
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

tion scores not only for completers but also for patients dropping outor withdrawn from treatment. The end point 204 sample thus reflectstermination status for all patients who had at least minimum exposureto their respective treatment, and the end point 239 sample (some¬times referred to as an "intent to treat" sample) reflects terminationstatus for all patients who entered treatment. The results of an endpoint analysis, particularly the end point 239 analysis (since it includessome patients who have barely received any treatment), may beconsidered an estimate of the overall performance of a treatmentprogram, including its ability to retain patients in treatment. Sincethere were some differences in the results of analyses of the threesamples, we include data on all three to provide the most complete andaccurate representation ofour findings.
Although our main questions concerned differences between thetwo psychotherapies and between each of them and imipramine-CM,all six possible comparisons between treatment conditions were ofinterest. To protect against inflation of the type I error rate associatedwith multiple comparisons, probability levels for comparisons be¬tween pairs of treatments were adjusted for the total number ofcomparisons, by means of the Bonferroni t test34 or Brunden's methodof partitioning significance level.35
To counterbalance this basically conservative approach, we chose aliberal overall probability level of P<.10 for accepting results as signifi¬cant. For individual comparisons between any two treatment conditions,this means that the probability level obtained must actually be <.017 tobe considered significant at an adjusted a level <.10. (We will alsoindicate "trends" toward significance where the observed probabilityvalue in individual comparisons is <.025, corresponding to an adjusted a
level of <.15.) This approach left us with satisfactory statistical power(.81 to .95) to detect medium size effects36 in our primary ANCOVAs andadequate power (. 84 to. 98) to detect large size effects in comparing pairsof treatments. In the secondary analyses, power was adequate (.82 to. 95) for detecting medium size interactions of treatment and severity andadequate (.82 to .99£) for detecting large size effects in the overallANCOVAs. Power was frequently less than adequate (.38 to .86),however, for detecting large size effects in the pairwise comparisonswithin severity groups.
RESULTSPatient Characteristics
A total of 250 patients (45% of those screened) met study criteriaand were randomized into treatment. The primary reason for rejec¬tion was failure to meet the major depressive disorder and/or HRSDinclusion criteria, at either screening or rescreening. Eleven patientsdropped out before the first treatment session (3 in CBT, 2 in IPT, and6 in impramine-CM). Of the 239 patients who actually entered treat¬ment, 168 (70%) were female and 212 (89%) were white. The average( ± SD) age was 35 ± 8.5 years. Sixty-three (26%) were single, 96 (40%)were married or cohabitating, and 80 (33%) were separated, divorced,or widowed. The sample was characterized by a high level of educa¬tion: 96 (40%) were college graduates, 83 (35%) had had some collegeeducation, and 60 (25%) had high school education or less.
The mean ( ± SD) score at rescreening on the HRSD was 19.5 ± 4.4,and 91 patients (38%) were classified as having "definite endogenous"depression by Research Diagnostic Criteria. There had been no previ¬ous episodes of major depressive disorder for 85 (36%), one or twoprevious episodes for 82 (34%), and three or more for 72 (30%). Meanage at onset of first episode of major depressive disorder was26.3 ± 10.3 years. The duration of the current episode was 6 months orless for 98 patients (41%), 6 months to 1 year for 57 (24%), and greaterthan 1 year for 84 (35%). In terms of previous treatment for depres¬sion, 36 (15%) had been hospitalized, 50 (21%) had received tricyclicantidepressants, 68 (28%) had received some kind of antidepressantmedication, 65 (27%) had received some kind of antianxiety medica¬tion, and 138 (58%) had received psychotherapy. A total of 168 pa¬tients (70%) had received some form ofprevious treatment for depres¬sion. There were no statistically significant differences amongtreatment groups on any of these characteristics in the intake sample,although there was some imbalance on marital status.
Attrition
Of the 239 patients entering treatment, 77 (32%) terminated beforecompletion, ie, had less than 15 weeks and/or 12 sessions of treatment.This includes both patients who dropped out of their own accord and
those who were withdrawn by study staff. By treatment group, therewere 19 early terminators (32%) in CBT, 14 (23%) in IPT, 19 (33%) inimipramine-CM, and 25 (40%) in PLA-CM. Excluding patients whoterminated for clearly external reasons or because they had improvedor thought they had improved, there were 59 patients (25%) whoterminated for what appeared to be negative treatment-related rea¬
sons, including, eg, dissatisfaction with treatment, desiring anothertreatment, intolerable side effects, and noncompliance. Only 9% of thepatients could be classified as clear symptomatic failures. Differencesamong treatments in these three categories of early termination (allattrition, treatment-related attrition, and symptomatic failure) wereevaluated by 2 and by life table analyses but did not achieve levels ofstatistical significance. A more detailed report of attrition findingsand their implications will be presented separately.
Because systematic or differential dropout can introduce bias in theresults and affect the interpretation of findings, we compared thosepatients who completed treatment with those who did not on themajor demographic and clinical variables obtained before treatment.One statistically significant difference (P<.05) emerged from thesecomparisons. Early terminators (across treatments) were more se¬verely depressed at intake than patients completing treatment (pre¬treatment HRSD scores, 20.6 vs 19.0, respectively; F[l,231] = 6.32,P<.02). There was no significant treatment by termination statusinteraction on the HRSD, and the difference in pretreatment scoresbetween early terminators and completers was almost identical with¬in each treatment condition. The completer patients, in general, were
fairly similar to the sample of patients entering treatment in terms ofthe distribution of patient characteristics both within and acrosstreatment conditions.
Comparisons were also made among treatments in regard to thedistribution of pretreatment demographic and clinical variables with¬in the completer sample. The pattern of attrition shifted the propor¬tion ofsingle and married patients (which had already been somewhatunevenly distributed) enough to result in a statistically significant(P<.05) differential distribution of marital status among treatmentconditions in the completer sample. Compared with IPT and PLA-CM, CBT completers included more single patients and fewer marriedpatients. As noted earlier, the variable of marital status was used as acovariate in analyses of outcome measures.
Outcome AnalysesPretreatment-Posttreatment Differences.—Paired f tests re¬
vealed highly significant differences (at P<.001) between pretreat¬ment and posttreatment means for all groups (including PLA-CM) onall four measures in all three samples.
ANCOVAs.—Table 1 presents means, SDs, and the results ofANCOVAs for the four outcome measures, in each of the threesamples. There were no significant differences among groups in theirpretreatment scores in any of these analyses. Statistically significantdifferences were found across the four groups at termination of treat¬ment in 4 of the 12 ANCOVAs. These included analyses of the twopatient measures (BDI and HSCL-90 T) in the completer sample andthe two clinical evaluator measures (HRSD and GAS) in the end point239 sample. None of the ANCOVAs of the end point 204 samplereached a level of statistical significance.
The general direction of results was similar in all 12 analyses, withPLA-CM always having the highest (most symptomatic) scores, imip¬ramine-CM (and, in one instance, IPT) having the lowest scores, andthe psychotherapies generally in between imipramine-CM and PLA-CM, but usually closer to imipramine-CM. The ANCOVAs werefollowed by pairwise comparisons. (The probability values presentedbelow for pairwise comparisons are observed probabilities. Note that,for the Bonferroni adjustment, the observed value must be multi¬plied by six.) In the completer sample, there was evidence of signifi¬cant superiority of imipramine-CM over PLA-CM (P=.006) on theHSCL-90 T. In the end point 239 sample, imipramine-CM was signifi¬cantly superior to PLA-CM (P = .010) on the GAS, and there weretrends for patients in both IPT and imipramine-CM groups to dobetter than the patients who received PLA-CM (P = .018 and .017) onthe HRSD. There were no significant differences in the end point 204sample, although there was one trend (P =. 020) for imipramine-CM todo better on the GAS than PLA-CM.
Recovery Analyses.—To address the extent to which patients inthe different treatment conditions met a predefined level of clinicalrecovery, the data were analyzed in terms of the percentage of
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

Table 1 .—Mean Pretreatment and Adjusted Termination Scores for the Four Primary Outcome Measures*
CBT IPT IMI-CM PLA-CM
Mean ± SD Mean ± SD Mean ± SD Mean ± SDSignificance
Levelf
HRSDPrestudy 37 19.2 ±3.6 47
Completer Patients
18.9 ±3.9 37 19.2 ±5.0 34 19.1 ±3.7 .984Termination 37 7.6 ±5.8 47 6.9 ±5.8 37 7.0±5.7 34 i±5.7 .458
GASPrestudy 37 52.8 ±7.2 47 52.6 ±6.6 37 51.6±7.1 34 53.1 ±7.3 .813Termination 37 9.4 + 11.0 47 70.7 ±11.0 37 72.5 ±10.8 34 67.6 ±10.7 .271
BDIPrestudy 37 26.8 ±8.4 47 25.5 ±7.7 36 27.1 ±8.8 35 28.1 ±6.7 .538Termination 37 10.2±8.7 47 7.7 ±8.6 36 6.5±8.6 35 11.0±8.5 .081
HSCL-90 Prestudy 37 1.38 ±0.55 47 1.35 + 0.45 36 1.43 ±0.46 35 1.58 ±0.49 .159Termination 37 0.47 ±0.43 47 0.48 ±0.43 36 0.38±0.42t 35 0.67 ±0.43 .046
HRSDPrestudy 50 19.6 ±3.7 55
End Point 204 Patients
19.2±4.4 49 19.1 ±4.7 50 19.0 ±4.2 .914Termination 50 9.0 ±7.0 55 9.1 ±7.0 49 8.3±6.9 50 11.3±6.9 .161
GASPrestudy 50 52.1 ±7.9 55 52.1 ±7.3 49 52.1 ±6.7 50 52.2±7.2 1.000Termination§ 50 66.5 ±12.6 55 67.2 ±12.6 49 69.7 ±12.4|| 50 63.9 ±12.4 .137
BDIPrestudy 50 27.5 ±8.1 55 25.5 ±7.6 49 25.8 ±8.6 50 27.4 ±6.8 .427Termination 50 11.5±9.7 55 10.6±9.7 49 8.6 ±9.6 50 12.5±9.6 .214
HSCL-90 Prestudy 50 1.44 ±0.55 55 1.33 ±0.44 48 1.40 ±0.48 50 1.53 ±0.47 .200Termination 50 0.60 ±0.49 55 0.60 ±0.50 48 0.51 ±0.49 50 0.70 ±0.49 .289
HRSDPrestudy 59 19.6±3.9 61
End Point 239 Patients
19.6 ±4.6 57 19.5 ±4.6 62 19.5 ±4.6 .999Terminations, 59 10.7±7.9 61 9.8±7.9|| 57 9.8±7.8|| 62 13.2 ±7.8 .053
GASPrestudy 59 52.4 + 7.9 61 52.0 ±7.1 57 52.2 ±6.7 62 52.5 ±7.1 .985Termination 59 64.4 ±12.4 61 66.3 + 12.4 57 67.4 ± 12.3t 62 61.6±12.3 .053
BDIPrestudy 59 27.0 ±7.9 61 26.0 ±7.8 57 26.8 + 8.7 62 27.1 ±6.9 .871Termination 59 13.4±10.6 61 12.0±10.6 57 11.6±10.5 62 15.0 ±10.5 .2901
HSCL-90 Prestudy 59 1.42 ±0.54 61 1.41 ±0.51 56 1.43 ±0.48 62 1.49 ±0.49 .819Termination 59 0.73 ±0.57 61 0.71 ±0.57 56 0.66 ±0.57 62 0.83 ±0.57 .413
'Prestudy scores are means from a one-way analysis of variance. Adjusted termination scores are treatment main effect least-square mean scores from atreatment by site analysis of covariance with prestudy scores and marital status used as covariates. Completer patients indicates patients with at least 12 sessionsand 15 weeks of treatment; end point 204 patients, patients with at least 3.5 weeks of treatment; end point 239 patients, all patients entering treatment; CBT,cognitive behavior therapy; IPT, interpersonal psychotherapy; IMI-CM, imipramine hydrochloride plus clinical management; PLA-CM, placebo plus clinicalmanagement; HRSD, Hamilton Rating Scale for Depression; GAS, Global Assessment Scale; BDI, Beck Depression Inventory; and HSCL-90 Hopkins SymptomChecklist-90 Total Score. Higher scores on GAS indicate better functioning.
tProbability level for F test comparing the four treatment groups.^Significantly different from PLA-CM (observed P<.017; with Bonferroni correction, P<.10).§Only marital status was used as covariate because of the lack of equality of slopes between prestudy and termination scores.UTrend for difference from PLA-CM (observed P<.025; with Bonferroni correction, P<.15).^Significant (P<.10) treatment by site interaction.
patients who reached a score of6 or less on the HRSD and also in termsof the percentage who reached a score of 9 or less on the BDI. Thesecutting scores, used in other studies comparing CBT and tricyclicdrugs, ,7 reflect the presence of little or no remaining depressivesymptoms and are more stringent than most "improvement" criteria.
As can be seen in Table 2, there were significant differences acrossthe four treatment conditions, for all three samples, in the percentageof patients reaching a score of 6 or less on the HRSD. Multiplecomparisons among pairs of treatments, with the use of the Brandencorrection, showed both IPT and imipramine-CM to be significantlysuperior to PLA-CM in the end point 239 sample (P= .010 and .013,respectively). The percentages of patients entering treatment whoreached the HRSD recovery criterion were 43% and 42% for IPT and
imipramine-CM, respectively, and 21% for PLA-CM. Patients receiv¬ing CBT had a recovery rate of 36%, not significantly worse than thatwith IPT and imipramine-CM, though also not significantly betterthan that with PLA-CM. There were also trends for superiority ofIPT and imipramine-CM over PLA-CM in the completer (P = .021 and.020) and end point 204 (P= .024 and .018) samples. The percentage ofpatients reaching the recovery criterion among the patients whocompleted treatment was 57% for imipramine-CM, 55% for IPT, 51%for CBT, and 29% for PLA-CM. There were no significant differencesamong treatments on the BDI recovery criterion, at least in partbecause the patients in the PLA-CM group did so well on thiscriterion.
In the analyses of both mean scores and recovery rates, no signifi- at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

Table 2.—Patients Recovered at Termination*
No. (%)CBT IPT IMI-CM
-' SignificancePLA-CM Levelf
37Completer Patients
47 37 34HRSDS6 19 (51) 26 (55)+ 21 (57)t 10 (29) .074BDIs9 24 (65) 33 (70) 25 (69) 18 (51)
(N = 36) (N = 35).299
50End Point 204 Patients
55 49 50HRSD==6 20 (40) 26 (47)+ 24 (49)t 13 (26) .076BDI==9 29 (58) 33 (60) 30 (61) 25 (50) .668
59End Point 239 Patients
61 57 62HRSD<6 21 (36) 26 (43)§ 24 (42)§ 13 (21) .042BDI==9 29 (49) 34 (56) 30 (53) 25 (40) .353
*See Table 1 for explanation of abbreviations.fProbability level for 2 test comparing the four treatment groups.t-Trend for difference from PLA-CM (observed P<,025; with Brunden
correction, P<.15).§Significantly different from PLA-CM (observed P<.017; with Brunden
correction, P<.10).
cant differences were found either between the two psychotherapiesor between either of them and imipramine-CM.
Secondary Analyses.—The patient sample had included, by de¬sign, a fairly wide range of severity of depression. To investigate theinfluence of pretreatment severity on outcome, two separate sets ofanalyses were carried out. These analyses must be considered explor¬atory, since the design did not include stratification on this variable.In the first set of these exploratory analyses, patients' conditionswere considered more severe if they had a score of 20 or greater ontheir rescreening HRSD. In the second set of analyses, they wereconsidered more severe if they had a score of 50 or less on the GAS.Forty-four percent of the sample met the HRSD criterion for sever¬ity; 41%, the GAS criterion; and 25%, both criteria. These cuttingscores, defined a priori, reflect a severe level of symptoms (HRSD) ora severe level ofboth symptoms and impairment of functioning (GAS),within the context of an outpatient sample. The GAS cutting scoreprovided a useful differentiation in a study of recurrent depression.37
Analyses of covariance of the four measures in all three samples,with the use of the HRSD severity breakdown, yielded two significanttreatment by severity interactions. These were both on the HRSD, inthe completer and end point 204 samples. The interaction for theHRSD in the end point 239 sample barely missed our criterion forstatistical significance (P=.ll), and since there was a significantinteraction for the HRSD in the other two samples, the end point 239sample was also included in the subsequent analyses describedbelow.
Similar ANCOVAs, with the GAS severity criterion, yielded sevensignificant severity x treatment interactions: for two measures in thecompleter sample (HRSD and HSCL-90 T), one in the end point 239sample (HRSD), and all four measures in the end point 204 sample.
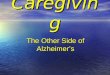
Figure 1 illustrates the pattern of the interaction in the end point204 sample for HRSD scores, with the use of the HRSD severitycriterion, and for GAS scores, with the use of the GAS severitycriterion. (These two examples were chosen because, in addition tothe significant severity by treatment interactions, there was alsosignificant heterogeneity of regression for the GAS and near-signifi¬cant [P = .06] heterogeneity for the HRSD.) The pattern for the twovariables was somewhat different. On the GAS, the interaction wasdue largely to the marked difference between imipramine-CM and theother groups, particularly PLA-CM. All treatments did about thesame for the less severely depressed and impaired patients, butimipramine-CM did much better for the more severely depressed andimpaired patients and PLA-CM did much worse for these patients.Cognitive behavior therapy and IPT were similar to each other anddid somewhat worse for the more severely depressed and impairedthan the less severely depressed and impaired patients. On theHRSD, on the other hand, IPT was more like imipramine-CM, bothdoing about the same for the more and less severely depressed pa-
o
< <r
161514131211109
5-4-3-2-
y
PLA
CBT
IPTIMI
Less Severe More SevereHRSD Severity
7473727170696867666564636261605958
o1PLA
Less Severe More SevereGAS Severity
Fig 1 .—Treatment se¬verity interactions. Ham¬ilton Rating Scale forDepression (HRSD)scores are least-squaremean termination scoresfrom a two-way analysisof covariance with mari¬tal status used as acovariate; less severeindicates a prestudy to¬tal score of less than20, and more severe, aprestudy total score of20 or more. Global As¬sessment Scale (GAS)scores are least-squaremean termination scoresfrom a two-way analysisof covariance with mari¬tal status used as acovariate; less severeindicates a prestudyscore of greater than50, and more severe, aprestudy score of 50 orless. Data are for endpoint 204 sample. PLAindicates placebo plusclinical management;CBT, cognitive behaviortherapy; IPT, interper¬sonal psychotherapy;and IMI, imipramine hy¬drochloride plus clinicalmanagement.
tients, while CBT and PLA-CM did better for the less, than for themore, severely depressed patients. These patterns were fairly repre¬sentative ofmost of the other measures and samples within each of theseverity breakdowns.
Subsequent ANCOVAs were carried out for the more and lesssevere subsamples wherever there was a significant severity x treat¬ment interaction. No differences were found among the less severelydepressed treatment groups in any of these analyses. Significantdifferences across treatments were found, for the more severelydepressed patients, in every instance in which there had been asignificant treatment severity interaction. Pairwise comparisonsrevealed that IPT was significantly more effective than PLA-CM inthree instances, all on the HRSD in end point samples, while imipra¬mine-CM was quite consistently significantly more effective thanPLA-CM (in 8 of 10 instances), across a number of measures.
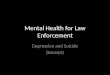
Data for more and less severely depressed subgroups were alsoanalyzed in terms of the percentage of patients who reached therecovery criterion of a score of 6 or less on the HRSD. The left-handside of Fig 2 presents these percentages for the more and less severelydepressed groups, as defined by the HRSD, while the right-hand sideof Fig 2 presents the percentages for the more and less severelydepressed and impaired groups, as defined by the GAS.
The results are similar to those reported for the mean scores.Again, there were no significant differences among treatments for theless severely depressed groups, although the two psychotherapieshad slightly higher rates than the two pharmacotherapy conditions forthe GAS-defined less severely depressed and impaired patients. Forthe more severely depressed groups (using both severity criteria),there were consistently significant differences in recovery ratesamong treatments in all three samples. Pairwise comparisons re¬vealed that, for the more severely depressed patients, IPT wassignificantly superior to PLA-CM in five of six tests and imipramine-CM was significantly superior to PLA-CM in all six tests.
Pairwise comparisons for the more severely depressed and im¬paired subgroup, as defined by the GAS, also yielded a significantdifference between one of the psychotherapies and imipramine-CM,
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

HRSD Severity Criterion GAS Severity Criterion
= 33 35 30 35Less Severe
D CBT D IPT
26 26 27 27More Severe
38 34 32 38Less Severe
21 27 25 24More Severe
!3 IMI-CM PLA-CM
Fig 2.—Percentage of pa¬tients in more and lessseverely depressed groups"recovered" at termination, bytreatment condition. Top,Completer patients; middle,end point 204 patients; andbottom, end point 239 pa¬tients. For the Hamilton Rat¬ing Scale for Depression(HRSD), less severe indi¬cates a prestudy total scoreof less than 20, and moresevere, a prestudy total scoreof 20 or more. For theGlobal Assessment Scale(GAS), less severe indicatesa prestudy score of greaterthan 50, and more severe, aprestudy score of 50 or less.CBT indicates cognitive be¬havior therapy; IPT, interper¬sonal psychotherapy; IMI-CM,imipramine hydrochloride plusclinical management; andPLA-CM, placebo plus clinicalmanagement.
with imipramine-CM being superior to CBT in the end point 204sample. With the exception of this lone finding, there were no signifi¬cant differences between either of the psychotherapies and imipra¬mine-CM. As in the analyses of the total sample, there were nosignificant differences between the two psychotherapies.
COMMENTEffectiveness of IPT and CBT
lb evaluate the effectiveness of IPT and CBT, they were
compared both with a standard reference treatment of tricy¬clic medication and with a control treatment of pill-placebo,each combined with CM, a minimal supportive therapy. Com¬parison with a standard reference treatment addresses thequestion of whether the "experimental" treatments, in thiscase both psychotherapies, are less (or more) effective thanthe currently accepted treatment for a disorder. In the majoranalyses in this study, there was no evidence that either of thepsychotherapies was significantly less (or more) effectivethan imipramine-CM. (Evidence of greater effectiveness ofimipramine-CM during the course of treatment is described inthe report by Watkins et al.I0)
Thus, there is no evidence in the major analyses that eitherof the psychotherapies was inferior to the standard referencetreatment at termination oftreatment on measures ofdepres¬sive symptoms or general functioning. These statistical ana¬
lyses do not, of course, permit the inference that the psy¬chotherapies and the standard reference treatment were
"equal" in effectiveness. However, since we had satisfactorypower in these analyses for detecting large effect size differ¬ences between pairs of treatments (in the total unstratifiedsample), it is unlikely that very large or important differenceswere missed.
We also compared each of the psychotherapies to the PLA-CM condition. This served as a control for regular contact withan experienced and supportive therapist, as well as the more
general support provided by the research setting. Since thiscondition also included expectations related to the drug ad¬ministration, it was not an ideal control for the psychothera¬pies. Nonetheless, it could serve as a useful comparison groupfor evaluating the specific effectiveness of the psycho¬therapies.
There was limited evidence of the specific effectiveness ofIPT and no evidence of the specific effectiveness of CBT, whencompared with PLA-CM, in the major outcome analyses.There was some, but not a great deal of, evidence of thesuperiority of imipramine-CM over PLA-CM in these ana¬
lyses. The order of the treatments was quite consistent, withimipramine-CM (and in one instance IPT) doing best, PLA-CM doing worst, and the psychotherapies generally in be¬tween, but the magnitude of the differences in mean scoreswas not large. There was some evidence of the superiority ofIPT, as well as imipramine-CM, over PLA-CM in the recoveryanalyses.
The general lack of significant differences between the
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

psychotherapies and PLA-CM does not seem to be due to a
poor showing by the psychotherapies. The results for bothCBT and IPT were, by and large, comparable with those inother studies3,4,7,8,31,38 comparing them with antidepressantdrugs. (The one exception here was the study by Rush et al,2 inwhich their patients receiving CBT showed more improve¬ment than those receiving CBT in the present study. Onepossible reason for this difference was the more intensivesupervision received by the therapists throughout the Rush etal study; in the present study, intensive supervision in thetraining phase was replaced by more infrequent consultationduring the outcome study.) In addition, highly significantdifferences (P<.001) were found between pretreatment andposttreatment means for the patients in IPT and CBT; thiswas true, however, for patients in the PLA-CM condition aswell.
The main reason for the general lack of significant findingsseems to be due, not to lack of improvement in the psychother¬apy groups, but rather to the very good performance of thePLA-CM condition. This is in contrast to the finding of fairlypoor performance ofwaiting-list or delayed-treatment groupsused as controls in other studies of brief psychotherapies fordepression.39 It is important to remember that, because of theCM component, PLA-CM in this study is not a no-treatmentcondition or even an "inactive" placebo condition. Patientswere seen once a week for 20 to 30 minutes by a well-trainedand experienced psychiatrist, who not only administered themedication and reviewed symptoms, side effects, and generalfunctioning, but also offered support and encouragement.This combination of minimal supportive therapy and expecta¬tions regarding the medication, along with the generally sup¬portive research and treatment environment, may be suffi¬cient for many patients to achieve a significant reduction indepressive symptoms and improvement in general function¬ing. This may be true, however, only for that subgroup ofpatients with major depressive disorder who are less severelydepressed and functionally impaired, as will be discussed inthe section on "Initial Severity" below.
Standard Reference Treatment.—The fact that therewere also relatively few significant differences, in the primaryanalyses, between imipramine-CM and PLA-CM gives rise toan important question: Was imipramine-CM an adequatestandard reference treatment in this study? Our imipramine-CM condition compared favorably with the tricyclic conditionsin the comparative studies cited earlier.2"4,7,8,31,38 It is difficult tomake direct comparisons between our findings and those inthe broader psychopharmacologic literature, however, be¬cause the studies differ in a number of ways. Our study was
longer than most antidepressant drug studies, and this mayprovide more chance for improvement; on the other hand, our
"recovery" criterion was more stringent than the "improve¬ment" criteria used in most of these studies. Also, unlike inmany of these studies, we reported on all patients entered intothe study, regardless of level of compliance, reason for attri¬tion, etc. Perhaps of greatest importance, our clinician dataare based on ratings by independent clinical evaluators, whilemost of the psychopharmacologic studies report therapistratings.
To provide information more comparable with that in thepsychopharmacologic literature, we carried out several addi¬tional analyses, using the end point 204 sample. Eight-weekend point analyses for just the imipramine-CM and PLA-CMgroups yielded significant differences favoring imipramine-CM over PLA-CM on both the clinical evaluator-rated HRSD(P<.05) and the therapist-rated HRSD (P<.01). Differencesat termination of treatment between imipramine-CM andPLA-CM, both in mean scores and in recovery rates on thetherapist-rated HRSD, were significantly different in allthree samples (ranging from = .001 to = .014). Perhaps
most striking were the high recovery rates at termination (asjudged by therapists) for patients in the imipramine-CMgroup having at least 3.5 weeks of treatment (78%). Given thestringency of this recovery criterion, this should demonstratethat, by usual psychopharmacology standards, imipramine-CM was an effective treatment in this study and set a highcomparison standard for the psychotherapies.
It is important to note that therapists rated patients asmore improved than did clinical evaluators, and therapistsalso differentiated more clearly between patients in activedrug and placebo groups. It is these differences betweentherapist and clinical evaluator ratings that make for an ap¬parent discrepancy between the very favorable findings forimipramine-CM with "usual psychopharmacology standards"and the more modest results presented in this article (for theprimary analyses), based on ratings by independent clinicalevaluators. (Results using therapist measures, which alsodemonstrated significant differences between the psychoth¬erapies and PLA-CM, are not presented herein because of thelack of calibration of the different groups of therapists and thepossible biases that may be associated with different frames ofreference of the psychotherapists and pharmacotherapists.)
Alternative Statistical Criteria. —It has been suggestedthat the relative lack of significant findings reported for our
major analyses of clinical evaluator and patient measures maybe due to the stringency of our statistical criteria for signifi¬cance of differences between pairs of treatments. We consideras most appropriate the a levels that were chosen a priori (andreported in the "Results" section), particularly given the needto protect against type I error when findings on several nonin-dependent variables are reported, and the necessary precau¬tions when analyzing subgroups in a clinical trial.40 Nonethe¬less, in response to questions raised, we have also examinedthe results of our major data analyses with an alternativeapproach to significance levels. Using F-protected t tests,with a conventional a level of.05 for the overall F test and an aof .05 for subsequent t tests between pairs of treatments, wefound the following:
Only 1 of our 12 ANCOVAs (HSCL-90 in the completersample) resulted in an F significant at <.05; in pairwise com¬
parisons, IPT as well as imipramine-CM was now significantly(P = .049) superior to PLA-CM. If the significance criterion isrelaxed to include the two F values at =.053 (HRSD andGAS in the end point 239 sample), the previous trends forsuperiority of IPT and imipramine-CM over PLA-CM on theHRSD become significant, and IPT is added to imipramine-CM as being significantly superior to PLA-CM on the GAS.Using this alternative set of criteria would result, then, in anincrease in evidence of the superiority of IPT over PLA-CM.There would still be only 3 tests of 12, however, in which IPTand imipramine-CM were significantly superior to PLA-CM,none in which CBT was superior to PLA-CM, and no evidenceof differences in effectiveness between either of the psychoth¬erapies and imipramine-CM.
Comparison of IPT and CBT
A second major question in this study was whether therewere any differences in the effectiveness of IPT and CBT.These two psychological treatments, both developed fortreating depression, had never before been compared withinthe same study. In interpreting the findings for the twopsychotherapies (and for pharmacotherapy as well), it is im¬possible in this study to separate treatments from the thera¬pists carrying out those treatments. We will, in future analy¬sis, explore the contribution to our outcome findings byindividual therapists within each treatment approach. Fornow, however, it is important to keep in mind that we are notcomparing IPT and CBT per se, but rather a "package" ofeach
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

of the treatment approaches with those therapists who choseto and were chosen to carry it out.41,42
We found no significant differences between IPT and CBTin any of the major analyses (or, for that matter, in thesecondary severity analyses). Furthermore, an examinationof mean scores reveals that, with a few exceptions, the actualnumerical differences between IPT and CBT and the relatedeffect sizes were very small. This was true even in some caseswhere IPT was significantly different from PLA-CM, butCBT was not. Thus, there is no evidence in this study of thegreater effectiveness of one of the psychotherapies on mea¬sures of depressive symptoms and overall functioning (al¬though, again, there was adequate power in the primaryanalyses for detecting any large effect size differences thatmight exist). These findings are consistent with many re¬
ported in the psychotherapy literature43 of a general lack ofdifferences in outcome between different forms ofpsychother¬apy. Despite the similar outcome in the analyses reportedherein, however, one might still expect to find differences onmeasures more specifically related to each of the treatmentapproaches. Even on such measures, however, Imber et al9found few differences. The general lack ofdifferences betweenthe two psychotherapies, together with the good results forthe PLA-CM condition, suggests once again the importance ofcommon factors in different types ofpsychologically mediatedtreatment.44
Factors Influencing Outcome
Initial Severity.—The primary analyses reported in thisarticle were based on all patients within each sample. It was
recognized from the outset, however, that a diagnosis ofmajordepressive disorder did not guarantee a homogeneous patientsample.45 A separate report11 presents analyses exploring thepredictive role of a number of patient demographic, clinical,and personality variables. Pretreatment severity of illness isconsidered such a crucial variable, however, that its possiblerole in influencing outcome deserves special attention. Re¬views ofboth the psychotherapy and pharmacotherapy litera¬ture46,47 had suggested that initial level of symptoms and func¬tioning may influence outcome of treatment. We were
especially interested in the possible differential role of sever¬
ity in the different treatment conditions. For that reason, we
reported secondary analyses ofthe influence on outcome of theinitial severity of the patient's illness.
These exploratory severity analyses suggested that initialseverity was, in fact, a very important variable in this study.A number of significant severity x treatment interactionswere found, especially for the GAS breakdown. The treat¬ment x severity interactions help to explain the relative lackof significant findings in the total, unstratified sample (partic¬ularly in the end point 204 sample). Looking separately at themore and less severely depressed subgroups, results were
quite consistent: there were no differences among treatments(including PLA-CM) in the less severely depressed patientgroup, while, for the more severely depressed patients, quiteconsistent differences emerged between the active treat¬ments and PLA-CM. For these patients, especially thosedefined by the GAS as more severely depressed and function¬ally impaired, IPT was superior to PLA-CM on both theHRSD mean scores and recovery criterion, while imipramine-CM was quite consistently superior to PLA-CM on a broaderrange of measures. Cognitive behavior therapy, though notvery different from IPT in this sample, did not do well enough,across the board, to demonstrate significant superiority toPLA-CM.
The effectiveness of imipramine-CM for the more severelydepressed and functionally impaired patients was especiallymarked in the end point 204 sample, where it was significantly
superior to PLA-CM on all four outcome measures and on therecovery criterion. Interpersonal psychotherapy was superi¬or to PLA-CM only on the HRSD measures, both mean scoresand recovery criterion. The end point 204 sample, whichincludes all patients who had at least 3.5 weeks of treatment,seems most likely to favor the active drug treatment; follow¬ing 3.5 weeks of treatment, patients might be expected toshow considerable improvement if they had received tricyclicmedication but would probably not be expected to do so if theyhad received psychotherapy. This points to one of the difficul¬ties inherent in comparing pharmacotherapy and psychother¬apy48 and should be taken into account in interpreting resultsof the end point 204 sample.
These secondary analyses (particularly for the GASbreakdown) led to two observations of potential clinicalsignificance.
1. The PLA-CM treatment did not do well for the more
severly depressed patients, particularly those with morefunctional impairment, and rarely brought them to a level ofrecovery. More specific targeted forms of treatment are indi¬cated for these patients. Imipramine-CM was especially effec¬tive for this subgroup, both in reducing depressive symptomsand in improving general functioning, and there was also someevidence of the specific effectiveness of IPT in reducing de¬pressive symptoms.
2. For the less severely ill patients, there were no signifi¬cant differences across treatments on any of the measures,although there was sufficient statistical power for detectinglarge effect size differences. Thus, there was no evidence ofthe superiority of any of the treatments (including imipra¬mine-CM) over PLA-CM in this subgroup. These findings arein accord with an observation by Downing and Rickels,49 who,after reviewing the drug literature, concluded that "a moreintense psychotherapy relationship may tend to obscure dif¬ferences between response to active drug and response toplacebo." Our pharmacotherapy-treated patients did not re¬ceive "intense" psychotherapy; however, they probably didreceive more contact and support than is present in many drugstudies. It is difficult to compare our PLA-CM results withthose of traditional placebo conditions in the psychopharma¬cology literature, due to many méthodologie differences.Where it is possible to focus, however, on what appear to becomparable samples or subsamples, PLA-CM seems moreeffective than drug study placebos.50"52
It must be stressed that the present findings do not meanthat the less severely depressed and functionally impairedpatients do not need any treatment, especially since otherstudies report significant superiority ofbriefpsychotherapiesfor depression over waiting-list or delayed-treatment controlgroups,39 which evidence little change. Further work will bedirected toward understanding the therapeutic properties ofthe PLA-CM condition in this study. The present findings doraise the possibility that some type of minimal supportivetherapy in the hands of an experienced practitioner may besufficient to bring about a significant reduction of depressivesymptoms (at least in the short run) for the less severelydepressed patients. The findings, if replicated, also raisequestions regarding the need for antidepressant medicationor for highly specified forms of psychotherapy for the resolu¬tion ofthe depressive episode in these patients. It is ofinterestthat the patients in this subgroup constituted almost 60% ofour sample and are probably seen with some frequency inmany outpatient settings.
Since we did not include severity as a stratifying variable inour original design, these findings must be considered explor¬atory. We find the results based on our poststudy stratifica¬tion provocative, however, especially as they help to explainthe relative lack of significant findings in our total unstratifiedsample. Severity of initial illness has been a fairly consistent
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

predictor of outcome in the psychotherapy literature,46 andsome recent studies in both psychopharmacology and psycho¬therapy have also found that poststudy stratification on sever¬
ity revealed interesting differential treatment outcomes.37,50,53Although clinicians and researchers alike acknowledge thepossible importance of severity in influencing the outcome oftreatments for depression, there is little systematic pre¬planned research on this subject. We hope that these resultswill encourage other investigators to try to replicate thefindings, to prestratify on severity, or to focus on specificlevels of severity in their research. À later article will explorein more detail the severity findings in the present study andtheir implications. The article will include further explorationof the regression data and of the differences found with thetwo different severity criteria.
Research Site Differences.—There were two significantdifferences in outcome due to research site; in both, two of theresearch sites generally did better than the third. What wewere particularly concerned about, however, was the possibleinteraction of treatments and sites, which would indicate adifferential effectiveness of the treatments depending on set¬ting. In the major analyses, there was only one significanttreatment x site interaction. This interaction, on the BDI inthe end point 239 sample, seemed to be due to a particularlypoor outcome on this measure for PLA-CM in one site and forCBT in another site. (Since there was no treatment effect onthis variable, the interaction did not alter the findings re¬
ported in this article.)More consistent interactions of treatment and site seem to
be present, however, in the more severely depressed andimpaired subsample, as defined by the GAS. Site had not beenincluded in the severity analyses because there was an insuffi¬cient number of severe cases at one of the sites. Exploratoryanalyses of the data for the two sites with sufficient numbersof patients revealed consistently significant treatment by siteinteractions for the more severely depressed and functionallyimpaired patients. Patients receiving CBT at one site didextremely well and had mean scores very similar to those forpatients receiving imipramine-CM, and the same was true forpatients receiving IPT at another site. Outcome for imipra¬mine-CM was more consistent at the two sites. Further anal¬yses will explore the extent to which these interactions may bedue to the distribution of particular patient characteristics,therapist performance variables, or some other aspects of thetreatment settings. Until we unravel these findings, finaljudgment must be withheld about the specific effectiveness ofthe two psychotherapies with more severely depressed andimpaired patients.
Patient Samples and Perspectives.—There were alsosome differences in findings, depending on whether onelooked at completers or at one or another of the end pointsamples. We have already commented on the particularlystriking performance of imipramine-CM in the GAS-definedseverely depressed and impaired group in the end point 204sample. Some of the other differences in findings for particularsamples are confounded with the perspective from whichratings were made. For example, significant differences be¬tween pairs of treatments on clinical evaluator-rated mea¬sures are found largely in the end point samples, but not in thecompleter sample, although the pattern ofresults is similar forthe completers. This finding is partly due to the increasednumber ofpatients in the end point samples, but, at least in thecase of IPT, it also seems due in part to the lower attritionfrom this treatment as compared with PLA-CM. Since earlyterminators generally had poorer scores at termination, moreof these poor scores were included for the PLA-CM group(which had a 40% attrition rate) than for the IPT group (whichhad a 23% attrition rate), increasing the difference betweenPLA-CM and IPT means in the end point samples. Thus, the
relative superiority of IPT over PLA-CM in the end pointsamples for the clinical evaluator measures is probably due inpart to the ability of IPT to retain patients long enough forthem to benefit from the treatment.
The significant findings for patient measures, on the otherhand, occurred mainly in the completer sample (and for GAS-defined severely ill patients in the end point 204 sample). Thegeneral lack of significant findings in the end point samplesseems to be due, at least in part, to the fact that some patientswho received imipramine-CM who terminated very early rat¬ed themselves as poorly as those in PLA-CM. Further workwill be carried out to explore the reasons for some of theseperspective/sample differences.
CONCLUSIONS
In the set of findings for the total unstratified sample ofpatients in our primary analyses, it is clear that there is noevidence of greater effectiveness of one of the psychothera¬pies as compared with the other and no evidence that either ofthe psychotherapies was significantly less effective than thestandard reference treatment. All treatment conditions (in¬cluding PLA-CM) evidenced significant change from pre¬treatment to posttreatment. Comparing each of the psycho¬therapies with the placebo plus minimal supportive therapycondition, there was limited evidence of the specific effective¬ness of IPT and none of the specific effectiveness of CBT. Ingeneral, the results for the two psychotherapies fell betweenthose for imipramine-CM and PLA-CM, being neither signifi¬cantly less effective than imipramine-CM nor (with some ex¬
ceptions for IPT) significantly more effective than PLA-CM.They were in general, however, closer to imipramine-CM thanto PLA-CM.
The secondary analyses dichotomizing the patient sampleaccording to two severity criteria suggest that a very impor¬tant role was played by this variable. For the less severelydepressed patients, there was no evidence of the specificeffectiveness of any of the treatments over the placebo com¬bined with minimal supportive therapy. There was evidence,however, of the specific effectiveness of the active treatmentsfor the more severely depressed and functionally impairedpatients; here, the imipramine-CM condition did extremelywell, the PLA-CM condition did poorly, and the two psychoth¬erapies were in between, with IPT slightly but sufficientlyahead of CBT so that IPT (but not CBT) was more effectivethan PLA-CM in reducing depressive symptoms. The moststriking findings, here, were on the recovery data, where bothIPT and imipramine-CM were consistently superior to PLA-CM. These "severity" findings (as well as the results of theprimary analyses) should not be generalized beyond the cur¬rent patient sample, ie, nonpsychotic, nonbipolar outpatientsmeeting criteria for a major depressive disorder.
Although this study was designed as a psychotherapy inves¬tigation, the inclusion of the standard reference and controlconditions provides information about the effectiveness ofimipramine. The present results may serve to reaffirm thevalue of imipramine in treating depressed outpatients, at leastthose who are more severely ill. Imipramine-CM was morefrequently superior to PLA-CM than were the psychothera¬pies and showed significant effects over a broader range ofmeasures. This was not true, however, for the less severely illpatients, for whom imipramine-CM was not significantly su¬perior to PLA-CM. The secondary analyses suggest a meansof identifying those more severely ill patients who are espe¬cially responsive to the drug. The results reported by Watkinset al10 also demonstrate that, although all of the groups im¬proved over time, the effects of imipramine-CM were more
rapid.Several factors should be taken into account in interpreting
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

the findings reported for the two psychotherapies. The firstrelates to the specific effectiveness of IPT. Interpersonalpsychotherapy was consistently superior to PLA-CM, al¬though the differences reached a level of statistical signifi¬cance only on the HRSD. It should be noted that the HRSD isprobably the most established instrument in studies of thetreatment of depression. The fact that IPT did so well on thestringent recovery criterion, and especially with the more
severely depressed and impaired patients, is of clinicalsignificance.
The additional exploratory analyses suggested that, whilethe effects of imipramine-CM were fairly consistent acrossresearch settings for the more severely depressed and func¬tionally impaired patients, IPT showed a similar degree ofeffectiveness at one research site and CBT at another. Thepossible reasons for these site differences must be exploredand hypotheses generated and tested to begin to determinethe conditions under which each of the psychotherapies maybe effective in treating severely depressed outpatients.
In drawing conclusions from the comparisons of the twopsychotherapies with the standard reference treatment, itshould be borne in mind that imipramine-CM was a veryeffective treatment, especially for the GAS-defined severelydepressed subgroup (in which 76% of the imipramine-CMcompleters reached the recovery criterion, compared with18% of the patients in PLA-CM), and thus provided a strin¬gent "standard" for comparison with the psychotherapies.Since the imipramine condition, as well as the placebo condi¬tion, included the CM component, the success of this conditionwith the more severely ill patients may have been due to thecombination of drug and minimal supportive therapy. Thisstudy did not include a treatment condition combining phar¬macotherapy with a specific form of psychotherapy. It ispossible that the effects of such a combination would havebeen superior to that of any of the individual treatments,although results in the literature have been inconsistent.39
The current findings address only the question of the short-term effectiveness of these treatments. To evaluate fully the
outcome for the psychotherapies, however, it will be neces¬
sary to consider their possible role in the maintenance ofimprovement and in the prevention of relapse. Future publi¬cations reporting analyses of data obtained at 6-, 12-, and 18-month follow-up evaluations will address these issues.
The NIMH Treatment of Depression Collaborative Research Program is amultisite program initiated and sponsored by the Psychosocial TreatmentsResearch Branch, Division of Extramural Research Programs (now part of theMood, Anxiety and Personality Disorders Research Branch, Division ofClinicalResearch), NIMH. The program was funded by cooperative agreements to sixparticipating sites (George Washington University [MH 33762], University ofPittsburgh [MH 33753], University of Oklahoma [MH 33760], Yale University,New Haven, Conn [MH 33827], Clarke Institute of Psychiatry, Toronto, Ontar¬io [MH 38231], and Rush Presbyterian-St Luke's Medical Center, Chicago, 111[MH 35017]). The principal NIMH collaborators are Irene Elkin, PhD, coordina¬tor, M. Tracie Shea, PhD, associate coordinator (formerly at George Washing¬ton University), John P. Docherty, MD (now at Nashua Brookside Hospital,Nashua, NH), and Morris B. Parloff, PhD (now at The American University,Washington, DC). The principal investigators and project coordinators at thethree participating research sites are as follows: George Washington Universi¬ty, Stuart M. Sotsky, MD, and David R. Glass, PhD; University of Pittsburgh,Stanley D. Imber, PhD, and Paul A. Pilkonis, PhD; and University of Oklaho¬ma, John T. Watkins, PhD, and William R. Leber, PhD. The principal investiga¬tors and project coordinators at the three sites responsible for training thera¬pists are as follows: Yale University, Myrna Weissman, PhD (now at ColumbiaUniversity, New York, NY), Eve Chevron, MS, and Bruce J. Rounsaville, MD;Clarke Institute of Psychiatry, Brian F. Shaw, PhD, and T. Michael Vallis,PhD; and Rush Presbyterian-St Luke's Medical Center, Jan A. Fawcett, MD,and Phillip Epstein, MD. Collaborators in the data management and dataanalysis aspects of the programs are C. James Klett, PhD, Joseph F. Collins,ScD, and Roderic Gillis of the Veterans Administration Cooperative StudiesProgram, Perry Point, Md.
We would like to thank members of the Advisory Group to the CollaborativeStudy (Paul Chodoff, MD, Sol L. Garfield, PhD, Martin M. Katz, PhD, DonaldF. Klein, MD, Perry London, PhD, Morris B. Parloff, PhD, Jeanne S. Phillips,PhD, Hans H. Strupp, PhD, and Eberhard H. Uhlenhuth, MD) for theirimportant contributions throughout the study. We would also like to thank H.Alice Lowery, MA, for various helpful contributions to the study, Robert F.Prien, PhD, for his valuable comments on an earlier draft of the manuscript,Regina T. Dolan, MA, Deborah Dowdall, and Doreen Grant for their assistancein preparing the manuscript, and Robert M. A. Hirschfeld, MD, chief of theMood, Anxiety and Personality Disorders Research Branch, for his advice andsupport. We are grateful for the many contributions of our statistical consul¬tant, C. James Klett; we also profited from discussions with Jacob Cohen andJohn Bartko.
References
1. Elkin I, Parloff MB, Hadley SW, Autry JH. NIMH Treatment of Depres-sion Collaborative Research Program: background and research plan. Arch GenPsychiatry. 1985;42:305-316.
2. Rush AJ, Beck AT, Kovacs M, Hollon S. Comparative efficacy of cognitivetherapy and pharmacotherapy in the treatment of depressed patients. CognitTher Res. 1977;1:17-37.
3. Weissman MM, Prusoff BA, DiMascio A, Neu C, Goklaney M, KlermanGL. The efficacy of drugs and psychotherapy in the treatment of acute depres-sive episodes. Am J Psychiatry. 1979;136:555-558.
4. DiMascio A, Weissman MM, PrusoffBA, Neu C, Zwilling M, Klerman GL.Differential symptom reduction by drugs and psychotherapy in acute depres-sion. Arch Gen Psychiatry. 1979;36:1450-1456.
5. Kessler KA. Tricyclic anti-depressants: mode ofaction and clinical use. In:Lipton MA, DiMascio A, Killam KF, eds. Psychopharmacology: A GenerationofProgress. New York, NY: Raven Press; 1978:1289-1302.
6. Morris JB, Beck AT. The efficacy of anti-depressant drugs. Arch GenPsychiatry. 1974;30:667-674.
7. Murphy GE, Simons AD, Wetzel RD, Lustman PJ. Cognitive therapy andpharmacotherapy: singly and together in the treatment ofdepression. Arch GenPsychiatry. 1984;41:33-41.
8. Hollon SD, DeRubeis RJ, Evans MD, Tuason VB, Weimer MJ, GarveyMJ. Cognitive Therapy, Pharmacotherapy, and Combined Cognitive-Pharma-cotherapy in the Treatment ofDepression, I: Differential Outcome. Minneapo-lis, Minn: University of Minnesota and St Paul Ramsey Medical Center; 1986.
9. Imber SD, Pilkonis PA, Sotsky SM, Elkin I. NIMH treatment of depres-sion collaborative research program: differential treatment effects. Read beforethe annual meeting of the American Psychiatric Association; May 13, 1986;Washington, DC.
10. Watkins JT, Leber WR, Imber SD, Collins JF. NIMH treatment ofdepression collaborative research program: temporal course of symptomaticchange. Read before the annual meeting of the American Psychiatric Associa-tion; May 13,1986; Washington, DC.
11. Sotsky SM, Glass DR, Shea MT, Pilkonis PA. NIMH treatment ofdepression collaborative research program: patient predictors of treatmentresponse. Read before the annual meeting of the American Psychiatric Associa-
tion; May 13,1986; Washington, DC.12. Endicott J, Spitzer RL. A diagnostic interview: the Schedule for Affec-
tive Disorders and Schizophrenia. Arch Gen Psychiatry. 1978;35:837-844.13. Spitzer RL, Endicott J, Robins E. Research Diagnostic Criteria: ratio-
nale and reliability. Arch Gen Psychiatry. 1978;35:773-782.14. Hamilton MA. A rating scale for depression. JNeurol Neurosurg Psychi-
atry. 1960;23:56-62.15. Hamilton MA. Development of a rating scale for primary depressive
illness. Br J SocClin Psychol. 1967;6:278-296.16. Rounsaville BJ, Chevron ES, Weissman MM. Specification of techniques
in interpersonal psychotherapy. In: Williams JBW, Spitzer RL, eds. Psycho-therapy Research: Where Are We and Where Should We Go? New York, NY:Guilford Press; 1984:160-172.
17. Shaw BF. Specification of the training and evaluation of cognitive thera-pists for outcome studies. In: Williams JBW, Spitzer RL, eds. PsychotherapyResearch: Where Are We and Where Should We Go? New York, NY: GuilfordPress; 1984:173-189.
18. Waskow IE. Specification of the technique variable in the NIMH Treat-ment of Depression Collaborative Research Program. In: Williams JBW,Spitzer RL, eds. Psychotherapy Research: Where Are We and Where ShouldWe Go? New York, NY: Guilford Press; 1984:150-159.
19. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy of Depres-sion. New York, NY: Guilford Press; 1979.
20. Klerman GL, Weissman MM, Rounsaville BJ, Chevron ES. Interperson-al Psychotherapy of Depression. New York, NY: Basic Books Inc Publishers;1984.
21. Fawcett J, Epstein P, Fiester SJ, Elkin I, Autry JH. Clinical Manage-ment\p=m-\Imipramine/PlaceboAdministration Manual: NIMH Treatment of De-pression Collaborative Research Program. Psychopharmacol Bull. 1987;23:309-324.
22. Rosenthal D, Frank JD. Psychotherapy and the placebo effect. PsycholBull. 1956;53:294-302.
23. O'Leary KD, Borkovec TD. Conceptual, methodological, and ethicalproblems of placebo groups in psychotherapy research. Am Psychol.1978;33:821-830.
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from

24. ParloffMB. Placebo controls in psychotherapy research: a sine qua non ora placebo for research problems. J Consult Clin Psychol. 1986;54:79-87.
25. Hollon SD, Waskow IE, Evans M, Lowery HA. System for ratingtherapies for depression. Read before the annual meeting of the AmericanPsychiatric Association, Los Angeles, May 9,1984. For copies of the Collabora-tive Study Psychotherapy Rating Scale and related materials prepared underNIMH contract 278-81-003 (ER), order "System for Rating PsychotherapyAudiotapes" from US Dept of Commerce, National Technical InformationService, Springfield, VA 22161.
26. Hill CE. Adherence in cognitive/behavioral therapy, interpersonal thera-py, and clinical management. Read before the annual meeting of the Society forPsychotherapy Research; June 15,1988; Santa Fe, NM.
27. Endicott J, Spitzer RL, Fleiss JL, Cohen J. The Global AssessmentScale: a procedure for measuring overall severity of psychiatric disturbance.Arch Gen Psychiatry. 1976;33:766-771.
28. Beck AT, Ward CH, Mendelsohn M, Mock J, Erbaugh J. An inventory formeasuring depression. Arch Gen Psychiatry. 1961;4:561-571.
29. Beck AT, Beamesderfer A. Assessment of depression: the DepressionInventory. In: Pichot P, ed. Modern Problems of Pharmacopsychiatry. Psy-chological Measurements in Psychopharmacology. Basel, Switzerland;1974;7:151-169.
30. Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatricrating scale\p=m-\preliminary report. Psychopharmacol Bull. 1973;9:13-28.
31. Blackburn IM, Bishop S, Glen AIM, Whalley LJ, Christie JE. Theefficacy of cognitive behavior therapy in depression: a treatment trial usingcognitive therapy and pharmacotherapy, each alone and in combination. Br JPsychiatry. 1981;139:181-189.
32. Endicott J, Cohen J, Nee J, Fleiss JL, Sarantakos S. Hamilton Depres-sion Rating Scale: extracted from regular and change versions of the Schedulefor Affective Disorders and Schizophrenia. Arch Gen Psychiatry. 1981;38:98\x=req-\103.
33. Lambert MJ, Shapiro DA, Bergin AE. The effectiveness ofpsychothera-py. In: Garfield SL, Bergin AE, eds. Handbook ofPsychotherapy and BehaviorChange. New York, NY: John Wiley & Sons Inc; 1986:157-211.
34. Miller RG. Simultaneous Statistical Inference. New York, NY:McGraw-Hill International Book Co; 1966.
35. Brunden MN. The analysis of non-independent 2\m=x\2tables using ranksums. Biometrics. 1972;28:603-607.
36. Cohen J. Statistical Power Analysis for the Behavioral Sciences. NewYork, NY: Academic Press Inc; 1977:284-288.
37. Prien RF, Kupfer DJ, Mansky PA, Small JG, Tuason VB, Voss CB,Johnson WE. Report of the NIMH Collaborative Study Group comparinglithium carbonate, imipramine, and a lithium combination. Arch Gen Psychia\x=req-\try. 1984;41:1096-1104.
38. DiMascio A, Klerman GL, Weissman MM, Prusoff BA, Neu C, Moore P.A control group for psychotherapy research in acute depression: one solution to
ethical and methodologic issues. J Psychiatr Res. 1979;15:189-197.39. Shea MT, Elkin I, Hirschfeld RMA. Psychotherapeutic treatment of
depression. In: Hales RE, Frances AJ, eds. Psychiatry Update: The AmericanPsychiatric Association Annual Review. Washington, DC: American Psychiat-ric Press; 1988;7:235-255.
40. Brown BW. Statistical considerations in clinical trials. In: Carter SK,Glatstein E, Livingston R, eds. Principles of Cancer Treatment. New York,NY: McGraw-Hill International Book Co; 1982:46-52.
41. Elkin I, Pilkonis PA, Docherty JP, Sotsky SM. Conceptual and method-ological issues in comparative studies of psychotherapy and pharmacotherapy,I: active ingredients and mechanisms of change. Am J Psychiatry.1988;145:909-917.
42. Kazdin AE. Comparative outcome studies of psychotherapy: method-ological issues and strategies. J Consult Clin Psychol. 1986;54:95-105.
43. Luborsky L, Singer B, Luborsky L. Comparative studies ofpsychothera-pies. Arch Gen Psychiatry. 1975;32:995-1008.
44. Frank JD. Persuasion and Healing. Baltimore, Md: The Johns HopkinsUniversity Press; 1973.
45. Klein DF, Gittelman R, Quitkin F, Rifkin A. Diagnosis and Drug Treat-ment ofPsychiatric Disorders: Adults and Children. Baltimore, Md: Williams& Wilkins; 1980.
46. Luborsky L, Crits-Christoph P, Mintz J, Auerbach A. Who Will BenefitFrom Psychotherapy? New York, NY: Basic Books Inc; 1989.
47. Bielski RJ, Friedel RO. Prediction of tricyclic antidepressant response.Arch Gen Psychiatry. 1976;33:1479-1489.
48. Elkin I, Pilkonis PA, Docherty JP, Sotsky SM. Conceptual and method-ological issues in comparative studies of psychotherapy and pharmacotherapy,II: nature and timing of treatment effects. Am J Psychiatry. 1988;145:1070\x=req-\1076.
49. Downing RW, Rickels K. Nonspecific factors and their interaction withpsychological treatment in pharmacotherapy. In: Lipton MA, DiMascio A,Killam KF, eds. Psychopharmacology: A Generation of Progress. New York,NY: Raven Press; 1978:1419-1428.
50. Stewart JW, Quitkin FM, Liebowitz MR, McGrath PJ, Harrison WM,Klein DF. Efficacy ofdesipramine in depressed outpatients. Arch Gen Psychia\x=req-\try. 1983;40:202-207.
51. Feighner JP, Aden GC, Fabre LF, Rickels K, Smith WT. Comparison ofalprazolam, imipramine, and placebo in the treatment of depression. JAMA.1983;249:3057-3064.
52. Rickels K, Chung HR, Csanalosi IB, Hurowitz AM, London J, WisemanK, Kaplan M, Amsterdam JD. Alprazolam, diazepam, imipramine, and placeboin outpatients with major depression. Arch Gen Psychiatry. 1987;44:862-866.
53. Woody GE, McLellan AT, Luborsky L, O'Brien CP, Blaine J, Fox S,Herman I, Beck AT. Severity ofpsychiatric symptoms as a predictor ofbenefitsfrom psychotherapy: the Veterans Administration-Penn Study. Am J Psychia-try. 1984;141:1172-1177.
at Mt Sinai School Of Medicine, on March 13, 2012 www.archgenpsychiatry.comDownloaded from