Embed Size (px)
Citation preview

Nasal Valves—Importance and SurgicalProceduresHelmut Fischer, M.D.1 and Wolfgang Gubisch, M.D.1
ABSTRACT
One of the most difficult aspects in rhinoplasty is resolving and preventingfunctional compromise of the nasal valve area reliably. The nasal valves are crucial for theindividual breathing competence of the nose. Structural and functional elements contributeto this complex system: the nasolabial angle, the configuration and stability of the alae,the function of the internal nasal valve, the anterior septum symmetrically separatingthe bilateral airways and giving structural and functional support to the alar cartilagecomplex and to their junction with the upper lateral cartilages, the scroll area. Sub-sequently, the open angle between septum and sidewalls is important for sufficient airflowas well as the position and function of the head of the turbinates. The clinical examinationof these elements is described. Surgical techniques are more or less well known anddemonstrated with patient examples and drawings: anterior septoplasty, reconstruction oftip and dorsum support by septal extension grafts and septal replacement, tip suspensionand lateral crural sliding technique, spreader grafts and suture techniques, splay grafts, alarbatten grafts, lateral crural extension grafts, and lateral alar suspension. The numerousliterature is reviewed.
KEYWORDS: Nasal valves, functional aesthetic rhinoplasty, septoplasty, cartilage
grafts, spreader grafts
Proper breathing is one of the most importantconstituents and features of healthiness and well-being.As rhinosurgeons treating patients who suffer frombreathing impairment, we have to turn our attention tothe nasal cavities but even more to be aware of theimportance of the anterior segment of the nose, thevestibules and nasal valve area.1
Many elements contribute to its functional stabil-ity and guarantee for the individual a feeling of unim-paired breathing. Sometimes we find a surprisingdiscrepancy between our prejudice as investigators andthe patients’ depiction.
The amount of airflow felt to be sufficient seemsto vary enormously individually. We always have tokeep in mind that we deal with a precisely coordinated
system of mobile and sufficiently stable yet weakcartilaginous structural elements and elastic fibrousconnections and suspensions as well as interwovenmuscles in the anterior segment of the nose that seemsto be balanced individually and that we are definitelygoing to compromise by any approach with scalpelsand scissors. There are patients who came for aestheticrhinoplasties and are bothered by consecutively im-paired breathing more than pleased by the successfulnasal reshaping.
Therefore, we have to analyze carefully the indi-vidual finding, the weakest element in the functionalchain, the specific risk of the planned procedure, and themost effective technique to combine functional require-ments and aesthetic objectives.
1Department of Facial Plastic Surgery, Marienhospital, Stuttgart,Germany.
Address for correspondence and reprint requests: Dr. med. HelmutFischer, Klinik fur Plastische Gesichtschirurgie, Zentrum PlastischeChirurgie/Marienhospital, Boeheimstrasse 37, 70199 Stuttgart,Deutschland.
Advanced and Comprehensive Management of the Nasal Septum;Guest Editor, Wolfgang Gubisch, M.D.
Facial Plast Surg 2006;22:266–280. Copyright# 2006 by ThiemeMedical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001,USA. Tel: +1(212) 584-4662.DOI 10.1055/s-2006-954845. ISSN 0736-6825.
266

EXAMINATION AND PLANNINGPROCEDURESPrior to surgery, the physician has to evaluate the role ofevery single element of the functional complex of theanterior part of the nose. Conceiving and understandingthe patient’s problems requires focusing on the differentelements by appropriate maneuvers and techniques toevaluate their particular importance. Anterior rhino-manometry to some extent impairs the function to bemeasured. So, first of all, precise observation of normaland forced inspiration is important and helps to under-stand the patient’s anatomical conditions, which can varyenormously yet guarantee individually normal breathing.
Consultation should include questions on a pre-ferred side of breathing impairment and obvious factorssuch as worsening under physical strain or at night.2
Incompatibility concerning a special side position whilesleeping indicates a nasal airway problem on the oppositeside, physiologically showing decongestion while there iscongestion on the dependent side. But decongestiondoes not result in airway opening of the upper side inthe lying position when there is critical obstruction.
Some patients instinctively demonstrate a Cottlemaneuver displaying the nasal vestibule as the location ofthe dysfunction. Pulling on the cheeks improves breath-ing in nasal valve incompetence (positive Cottle test).Different self-made spring-like devices of cotton buds orplastic stuff supporting the nasal alae are presented bythe patients to demonstrate the requested surgical pro-cedure.
Most important are the clinical findings of theanterior septum. It has to be straight in the midline fromthe nostrils to the area beyond the internal nasal valveswhere the nasal cavities are widened. Minimal deviationshave enormous effects on the airflow through thatnarrow nozzle, and asymmetry causes the tendency forunilateral alar and valvular collapse. Techniques ofanterior septal resection are obsolete. So recontouringand stabilization (e.g., splints such as spreader grafts orexchange techniques to bring a strong and straight septalplate into the adequate anterior septal position) have tobe considered.
Unilateral or bilateral concavity of alar cartilageshas to be detected and the functional implicationsevaluated. Small glass spatulae help to assess the missingsupport of the alar wings during inspiration and detectthe site where the support most effectively improvesbreathing, either apical, intermediate, or at the alar base.
Unilateral alar collapse indicates either increasedairflow compensating for contralateral nasal cavity ob-struction or ipsilateral structural weakness of the alarframework, for example, by lateral crural concavity oroverall weakness and dysfunction of the small nasalmuscles. Support by a flat ophthalmologic glass spatula(Fig. 1) in these cases completely relieves breathingon the side of the collapse or indicates contralateral
impairment. The site of maximum relief can be deter-mined by this maneuver. It helps to differentiate for thesurgical concept to be preferred. Is it strengthening thealar contour by a batten graft or lateralization of the alarbase? Weak and especially concave lateral crura com-bined with tension nose deformities tend to collapseduring slightly forced inspiration. The bilateral spatulamaneuver again helps to exclude the alar part of theproblem and focus on further abnormities.
Deformities in the area of the footplates caninfluence the airflow when there is significant wideningby increased footplate divergence and hypertrophic de-pressor septi muscle. Narrowing the columellar base bycompression with both branches of the speculum revealsthe contribution of the columellar width to the overalldysfunction.
In bulbous tip deformities, aesthetic rhinoplastymay exacerbate or cause airway obstruction, especially ifthe lateral crura show significant recurvature into thevestibular lumen. Intradomal sutures for tip reshapingalso narrow the bottleneck of the nostrils. The effect ofintradomal sutures can be simulated by pressure onto thetip bilaterally and simultaneously the patient has toassess grossly the impact on the airflow.
Further, the position and support of the nasal tiphave to be estimated. Is there a physiological connectionbetween the footplates and the anterior septal border or isit missing, lost by trauma or previous surgery? What doesthe patient feel when the nasal tip is pushed upward?Some patients demonstrate the procedure spontaneouslyand ask for just performing that movement by surgery.The direction of the vestibular airflow is changed and alsothe scroll area and the internal nasal valve are stabilized bypushing the cephalic rim of the lower lateral cartilagesover the caudal rim of the upper lateral cartilages.What isthe reliable analogous procedure? This question has to beanswered individually in terms of simultaneously de-manded aesthetic procedures. May the lateral crura beshortened or the scroll area reinforced and the cartilageoverlap improved? May the septum be extended andthe tip support augmented? Do the patients accept thelimitation of their aesthetic desires and are they aware ofthe conflict between aesthetic and function?
The stabilization of the nasal valve area has to besecured by additional techniques such as spreader graftsand suture techniques.
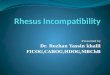
For examination of the nasal valve area, the glassspatula is again of great benefit. It adds minimal addi-tional obstruction and prevents harm to the nasal mucosaby the round tip and flat smooth spatula tip. It helps tosimulate the effect of spreader grafts by plunging it intothe subdorsal angle (Fig. 1C). Simultaneously, we canshow the patient the effect on aesthetics of the cartila-ginous nasal dorsum, which is normalized in cases ofsidewall collapse but also unpleasantly widened in othercases—important for informed consent.
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 267
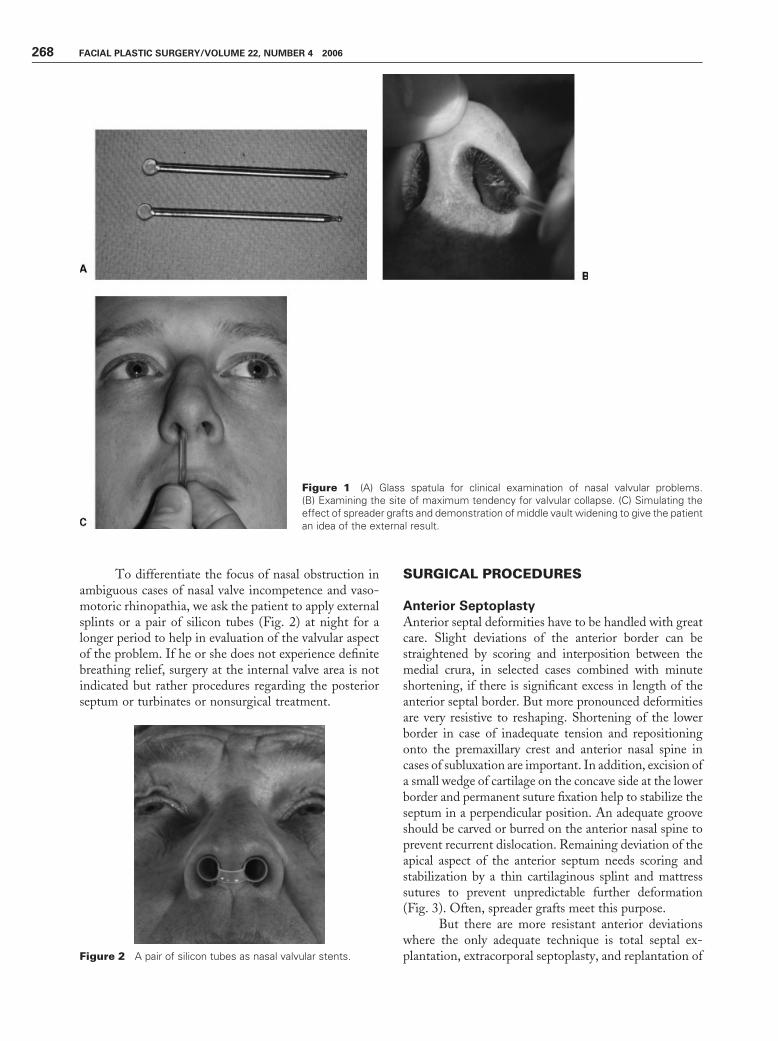
To differentiate the focus of nasal obstruction inambiguous cases of nasal valve incompetence and vaso-motoric rhinopathia, we ask the patient to apply externalsplints or a pair of silicon tubes (Fig. 2) at night for alonger period to help in evaluation of the valvular aspectof the problem. If he or she does not experience definitebreathing relief, surgery at the internal valve area is notindicated but rather procedures regarding the posteriorseptum or turbinates or nonsurgical treatment.
SURGICAL PROCEDURES
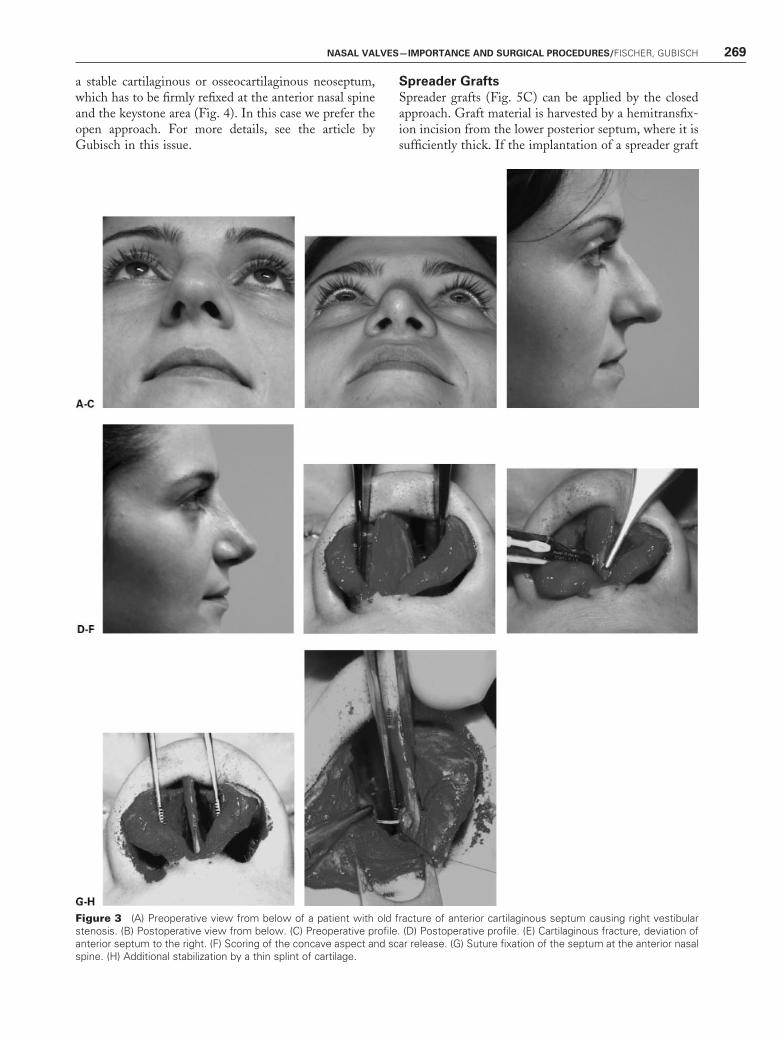
Anterior SeptoplastyAnterior septal deformities have to be handled with greatcare. Slight deviations of the anterior border can bestraightened by scoring and interposition between themedial crura, in selected cases combined with minuteshortening, if there is significant excess in length of theanterior septal border. But more pronounced deformitiesare very resistive to reshaping. Shortening of the lowerborder in case of inadequate tension and repositioningonto the premaxillary crest and anterior nasal spine incases of subluxation are important. In addition, excision ofa small wedge of cartilage on the concave side at the lowerborder and permanent suture fixation help to stabilize theseptum in a perpendicular position. An adequate grooveshould be carved or burred on the anterior nasal spine toprevent recurrent dislocation. Remaining deviation of theapical aspect of the anterior septum needs scoring andstabilization by a thin cartilaginous splint and mattresssutures to prevent unpredictable further deformation(Fig. 3). Often, spreader grafts meet this purpose.
But there are more resistant anterior deviationswhere the only adequate technique is total septal ex-plantation, extracorporal septoplasty, and replantation of
Figure 1 (A) Glass spatula for clinical examination of nasal valvular problems.(B) Examining the site of maximum tendency for valvular collapse. (C) Simulating theeffect of spreader grafts and demonstration of middle vault widening to give the patientan idea of the external result.
Figure 2 A pair of silicon tubes as nasal valvular stents.
268 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006
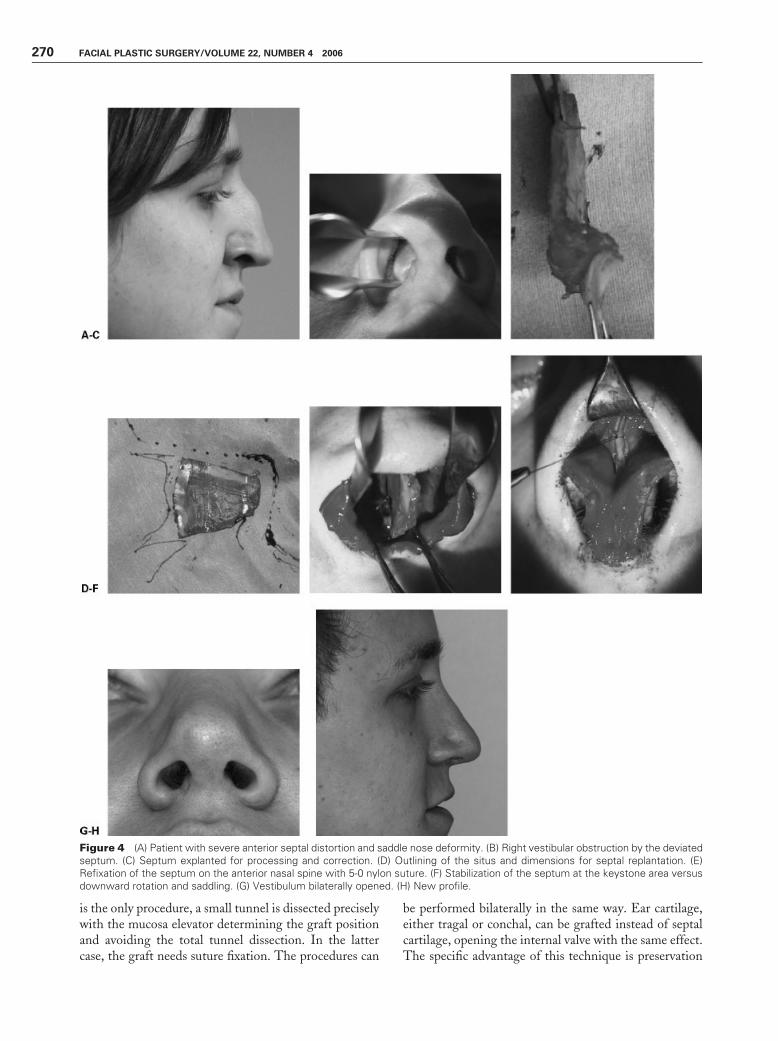
a stable cartilaginous or osseocartilaginous neoseptum,which has to be firmly refixed at the anterior nasal spineand the keystone area (Fig. 4). In this case we prefer theopen approach. For more details, see the article byGubisch in this issue.
Spreader GraftsSpreader grafts (Fig. 5C) can be applied by the closedapproach. Graft material is harvested by a hemitransfix-ion incision from the lower posterior septum, where it issufficiently thick. If the implantation of a spreader graft
Figure 3 (A) Preoperative view from below of a patient with old fracture of anterior cartilaginous septum causing right vestibularstenosis. (B) Postoperative view from below. (C) Preoperative profile. (D) Postoperative profile. (E) Cartilaginous fracture, deviation ofanterior septum to the right. (F) Scoring of the concave aspect and scar release. (G) Suture fixation of the septum at the anterior nasalspine. (H) Additional stabilization by a thin splint of cartilage.
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 269
is the only procedure, a small tunnel is dissected preciselywith the mucosa elevator determining the graft positionand avoiding the total tunnel dissection. In the lattercase, the graft needs suture fixation. The procedures can
be performed bilaterally in the same way. Ear cartilage,either tragal or conchal, can be grafted instead of septalcartilage, opening the internal valve with the same effect.The specific advantage of this technique is preservation
Figure 4 (A) Patient with severe anterior septal distortion and saddle nose deformity. (B) Right vestibular obstruction by the deviatedseptum. (C) Septum explanted for processing and correction. (D) Outlining of the situs and dimensions for septal replantation. (E)Refixation of the septum on the anterior nasal spine with 5-0 nylon suture. (F) Stabilization of the septum at the keystone area versusdownward rotation and saddling. (G) Vestibulum bilaterally opened. (H) New profile.
270 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006
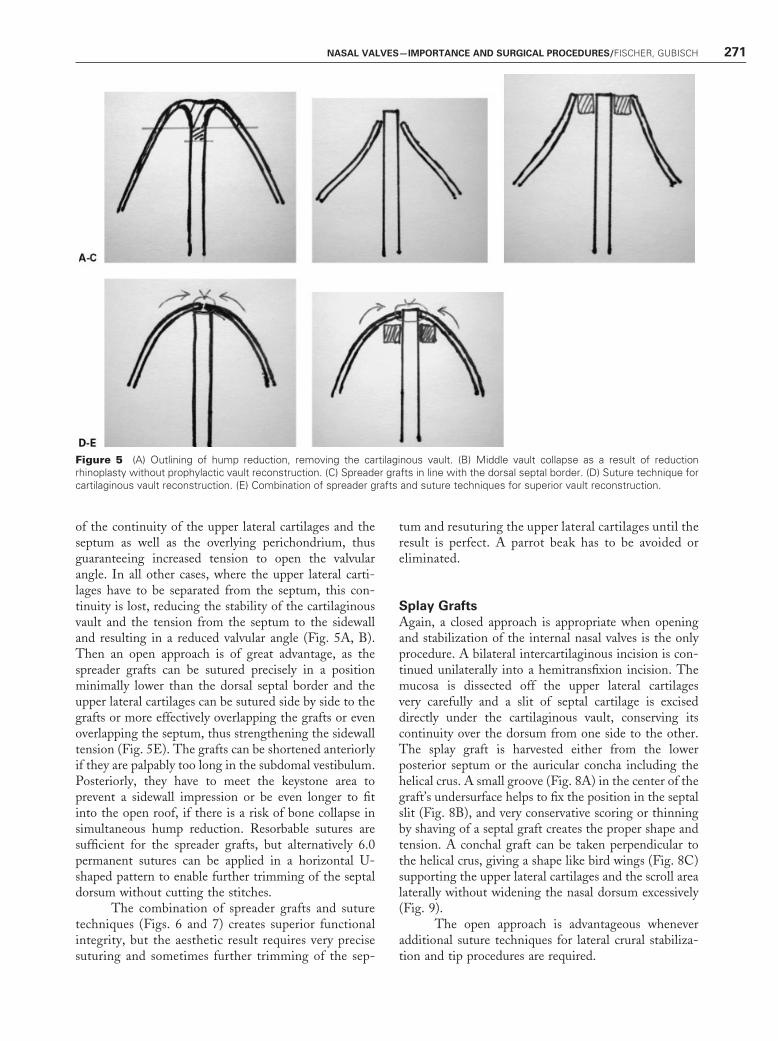
of the continuity of the upper lateral cartilages and theseptum as well as the overlying perichondrium, thusguaranteeing increased tension to open the valvularangle. In all other cases, where the upper lateral carti-lages have to be separated from the septum, this con-tinuity is lost, reducing the stability of the cartilaginousvault and the tension from the septum to the sidewalland resulting in a reduced valvular angle (Fig. 5A, B).Then an open approach is of great advantage, as thespreader grafts can be sutured precisely in a positionminimally lower than the dorsal septal border and theupper lateral cartilages can be sutured side by side to thegrafts or more effectively overlapping the grafts or evenoverlapping the septum, thus strengthening the sidewalltension (Fig. 5E). The grafts can be shortened anteriorlyif they are palpably too long in the subdomal vestibulum.Posteriorly, they have to meet the keystone area toprevent a sidewall impression or be even longer to fitinto the open roof, if there is a risk of bone collapse insimultaneous hump reduction. Resorbable sutures aresufficient for the spreader grafts, but alternatively 6.0permanent sutures can be applied in a horizontal U-shaped pattern to enable further trimming of the septaldorsum without cutting the stitches.
The combination of spreader grafts and suturetechniques (Figs. 6 and 7) creates superior functionalintegrity, but the aesthetic result requires very precisesuturing and sometimes further trimming of the sep-
tum and resuturing the upper lateral cartilages until theresult is perfect. A parrot beak has to be avoided oreliminated.
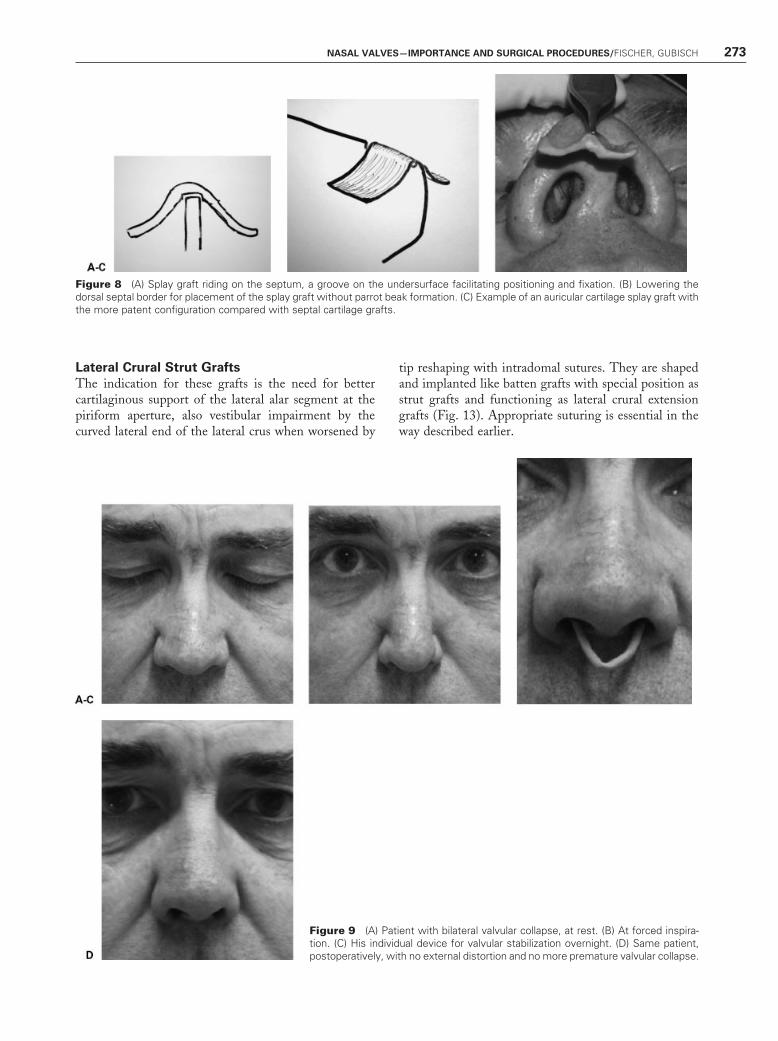
Splay GraftsAgain, a closed approach is appropriate when openingand stabilization of the internal nasal valves is the onlyprocedure. A bilateral intercartilaginous incision is con-tinued unilaterally into a hemitransfixion incision. Themucosa is dissected off the upper lateral cartilagesvery carefully and a slit of septal cartilage is exciseddirectly under the cartilaginous vault, conserving itscontinuity over the dorsum from one side to the other.The splay graft is harvested either from the lowerposterior septum or the auricular concha including thehelical crus. A small groove (Fig. 8A) in the center of thegraft’s undersurface helps to fix the position in the septalslit (Fig. 8B), and very conservative scoring or thinningby shaving of a septal graft creates the proper shape andtension. A conchal graft can be taken perpendicular tothe helical crus, giving a shape like bird wings (Fig. 8C)supporting the upper lateral cartilages and the scroll arealaterally without widening the nasal dorsum excessively(Fig. 9).
The open approach is advantageous wheneveradditional suture techniques for lateral crural stabiliza-tion and tip procedures are required.
Figure 5 (A) Outlining of hump reduction, removing the cartilaginous vault. (B) Middle vault collapse as a result of reductionrhinoplasty without prophylactic vault reconstruction. (C) Spreader grafts in line with the dorsal septal border. (D) Suture technique forcartilaginous vault reconstruction. (E) Combination of spreader grafts and suture techniques for superior vault reconstruction.
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 271
Batten GraftsBatten grafts work like a laminated or compound spring(Fig. 10). They are placed in pockets according to thesite of maximum effect in the clinical examination. Theyreinforce the ala in cases of lateral crural deformation oroverresection. An alar rim incision is appropriate. Ingiven cases, scar tissue should be resected to prevent alarthickening with the risk of a reverse effect by narrowingthe vestibule. We place the graft on top of the alarcartilage with fine resorbable transvestibular sutures, theknots lying in the vestibular lumen (Fig. 11). Underbatten grafts are an alternative. The grafts should be
curved for superior reconstruction of the alar convexity.Auricular conchal cartilage fits perfectly, but septalcartilage can be bent by careful scoring and is as effectivewith increased stability.
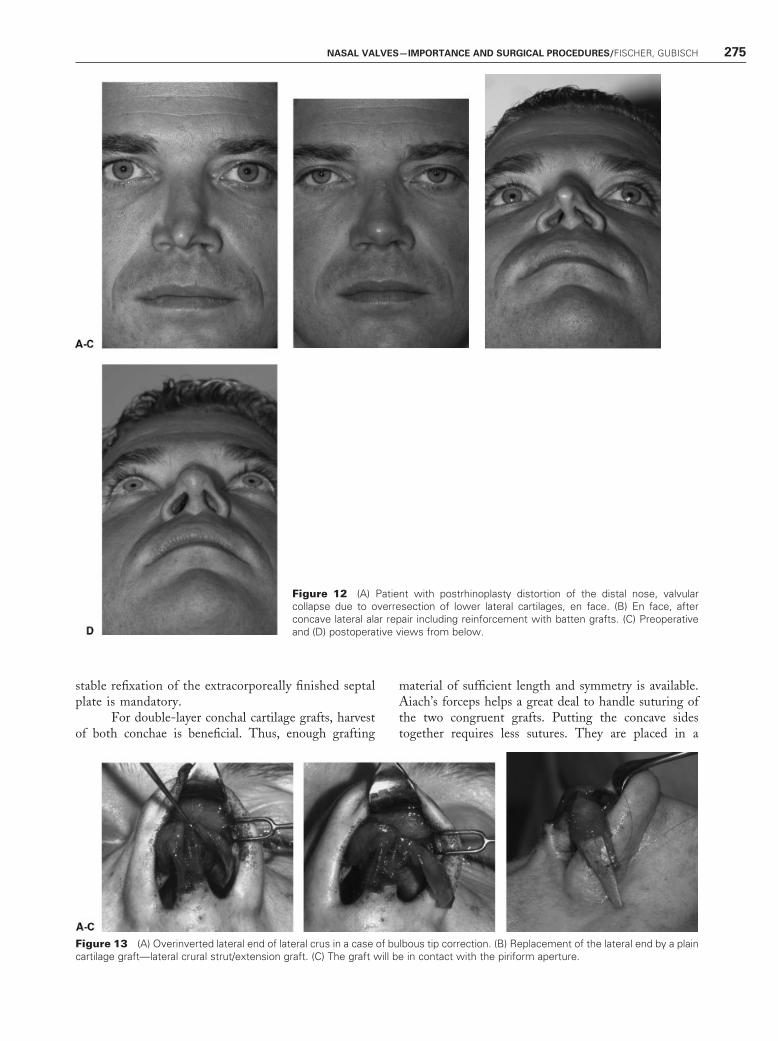
More often there is an indication for internalvalvular reinforcement by batten grafts (Fig. 12). Thesame approach as for external valve repair exposes thesite of implantation. Transnasal sutures can fix the graftsin position and are anchored on silicon sheets to preventsmall pressure sores. Wound care is essential. Silicontubes (e.g., Nasivent1) (Fig. 2) for several weeks help tostabilize the result during consolidation.
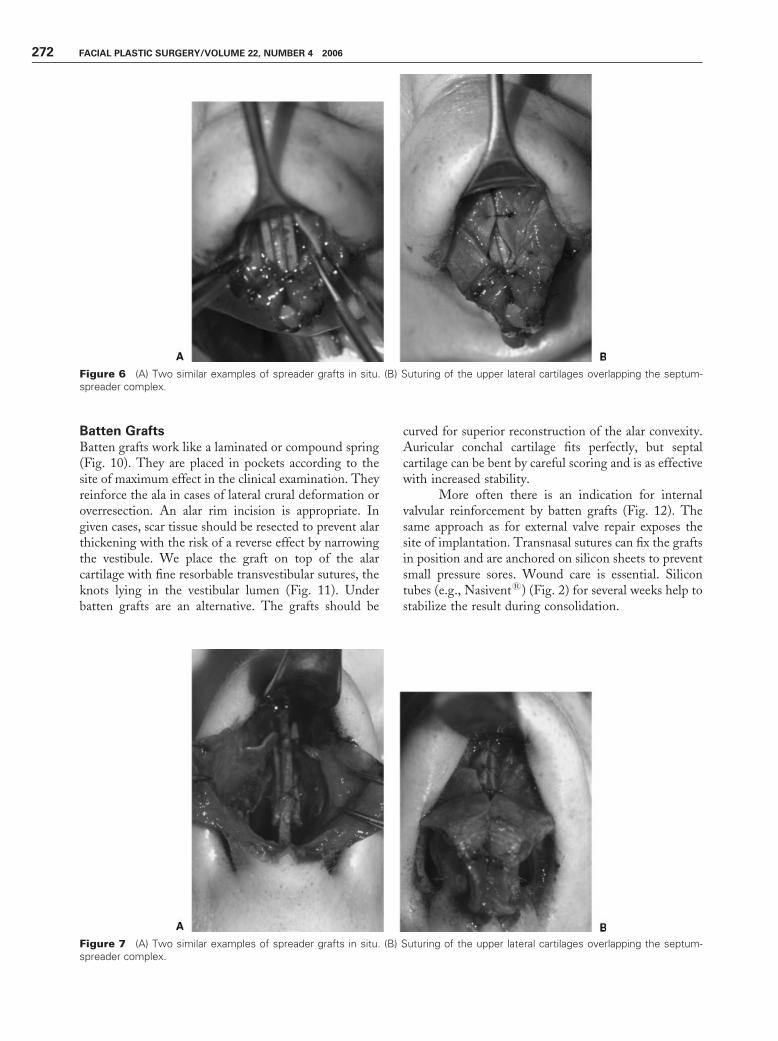
Figure 6 (A) Two similar examples of spreader grafts in situ. (B) Suturing of the upper lateral cartilages overlapping the septum-spreader complex.
Figure 7 (A) Two similar examples of spreader grafts in situ. (B) Suturing of the upper lateral cartilages overlapping the septum-spreader complex.
272 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006
Lateral Crural Strut GraftsThe indication for these grafts is the need for bettercartilaginous support of the lateral alar segment at thepiriform aperture, also vestibular impairment by thecurved lateral end of the lateral crus when worsened by
tip reshaping with intradomal sutures. They are shapedand implanted like batten grafts with special position asstrut grafts and functioning as lateral crural extensiongrafts (Fig. 13). Appropriate suturing is essential in theway described earlier.
Figure 9 (A) Patient with bilateral valvular collapse, at rest. (B) At forced inspira-tion. (C) His individual device for valvular stabilization overnight. (D) Same patient,postoperatively, with no external distortion and no more premature valvular collapse.
Figure 8 (A) Splay graft riding on the septum, a groove on the undersurface facilitating positioning and fixation. (B) Lowering thedorsal septal border for placement of the splay graft without parrot beak formation. (C) Example of an auricular cartilage splay graft withthe more patent configuration compared with septal cartilage grafts.
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 273
Reconstruction of Tip Supportby Septal ReplacementSevere tip depression requires reconstruction of tipsupport by one of the techniques of septal extensiongrafts, repositioning of septal remnants with intranasalor extracorporeal reshaping, double-layer conchal carti-lage grafts, or rib grafts. We use them in the listed orderfor reasons of biological quality.
Extension grafts are harvested from the septum(Fig. 14) or auricle. Unilateral or bilateral splints of
cartilage stabilize the central graft to give support tothe medial crura, which are also fixed by sutures. Theopen approach facilitates the procedures but is notmandatory.
Repositioning of septal remnants we performmostly by extracorporeal septoplasty if the remainingseptum is deviated. The technique is also advantageousif there is a straight remnant that ideally fits in theanterior position in a different orientation, either up-side down or rotated by 90 to 180 degrees. Again,
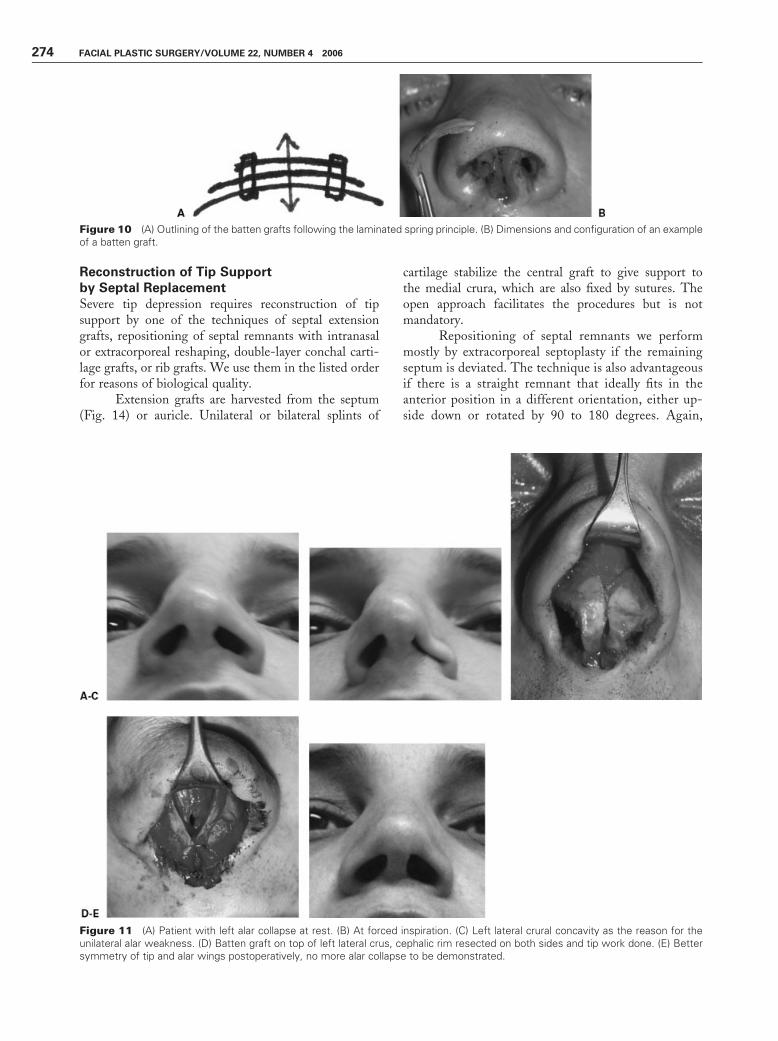
Figure 10 (A) Outlining of the batten grafts following the laminated spring principle. (B) Dimensions and configuration of an exampleof a batten graft.
Figure 11 (A) Patient with left alar collapse at rest. (B) At forced inspiration. (C) Left lateral crural concavity as the reason for theunilateral alar weakness. (D) Batten graft on top of left lateral crus, cephalic rim resected on both sides and tip work done. (E) Bettersymmetry of tip and alar wings postoperatively, no more alar collapse to be demonstrated.
274 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006
stable refixation of the extracorporeally finished septalplate is mandatory.
For double-layer conchal cartilage grafts, harvestof both conchae is beneficial. Thus, enough grafting
material of sufficient length and symmetry is available.Aiach’s forceps helps a great deal to handle suturing ofthe two congruent grafts. Putting the concave sidestogether requires less sutures. They are placed in a
Figure 12 (A) Patient with postrhinoplasty distortion of the distal nose, valvularcollapse due to overresection of lower lateral cartilages, en face. (B) En face, afterconcave lateral alar repair including reinforcement with batten grafts. (C) Preoperativeand (D) postoperative views from below.
Figure 13 (A) Overinverted lateral end of lateral crus in a case of bulbous tip correction. (B) Replacement of the lateral end by a plaincartilage graft—lateral crural strut/extension graft. (C) The graft will be in contact with the piriform aperture.
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 275

central line, keeping the ends free of sutures for ease offurther trimming and diverging the ends to ride on theanterior nasal spine or maxillary crest for reliable midlinefixation (Fig. 15).
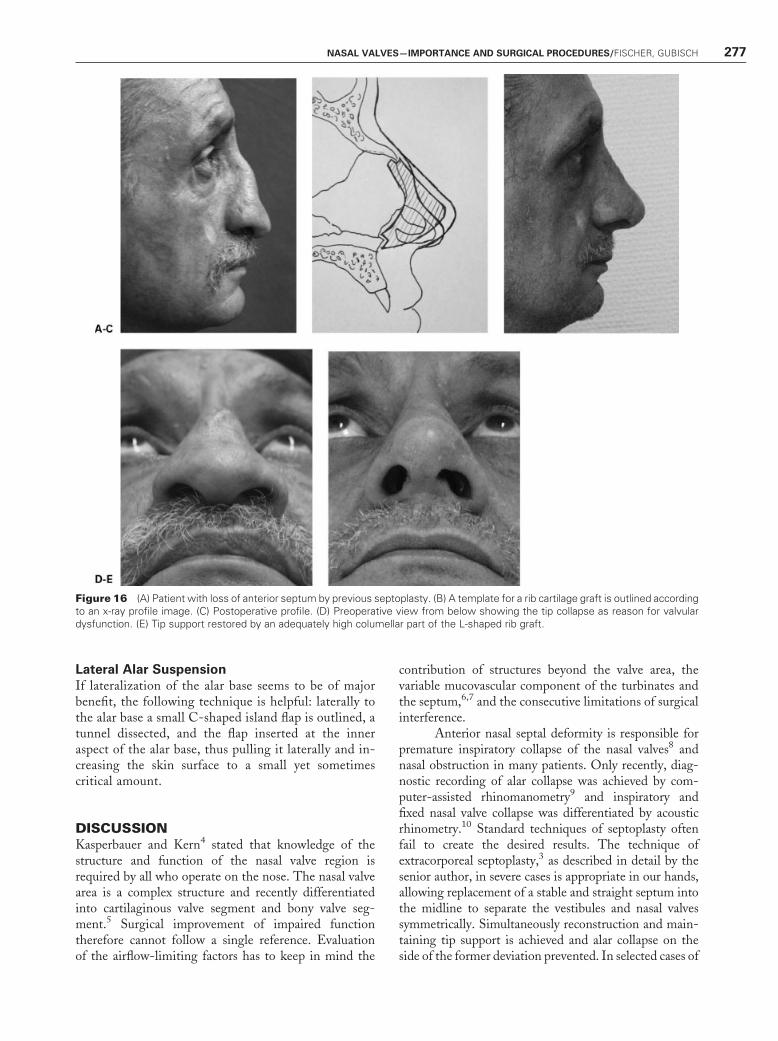
In severe saddle nose deformities, there is nobetter material than rib cartilage grafts, especially if tipand dorsum support is required (Fig. 16). Many detailsimprove the success rate. An anterior septocolumellarstrut should be harvested from the center of a plainsegment of a wide rib. An L-shaped graft for simulta-neous dorsum support can be harvested from the area ofa synchondrosis. Unfortunately, the rib contour there isoften curved so that the graft of sufficient dimensionshas to be fabricated out of two straight parts. Tailoringthe columellar strut grossly by a no. 11 blade and thenfurther thinning with a bur is advantageous to preventobjectionable cuts into the cartilage followed by de-flection. Stable fixation at the anterior nasal spinerequires subtle fabrication in a W-shaped fashion tofit on the spine or alternatively V-shaped fitting into agroove if the spine is missing. An adequate suturetechnique is necessary and a transoral approach bene-
ficial in selected cases. Bilateral fixation at the bony rimof the nasal floor through drill holes improves stabilitywhere appropriate. If the alar cartilages are preserved,the rib graft can be short to give support to the medialcrura like the former septum; otherwise, it can beconstructed as high as the tip projection to supportthe nasal tip directly. Then a nicely rounded and wideapical shape is required like an umbrella graft to supportthe skin smoothly. Lateral crural remnants can be fixedto the graft appropriately. In addition, spreader graftscan keep the rib graft straight in the midline in con-tinuity with the residual septum.
Reduction of Columellar WidthIf columellar width contributes significantly to vestibularobstruction, the depressor septi muscle can be partiallyresected and mattress sutures bring the footplates in firmcontact with the anterior septal border, so that scarringkeeps the result long lasting. In addition, footplatedivergence can be reduced by medial crural transsection(Fig. 17).
Figure 14 (A) Outline of a septal extension graft, sutured onto the anterior septal border, stabilized by overlong spreader grafts,working as bilateral splints to prevent dislocation. (B) Another example of a septal extension graft fixed side by side on the anteriorseptum.
Figure 15 (A) Defect of anterior septum. Template to measure the required extension/replacement graft. (B) Double-layer earcartilage graft, fixed in place by cartilage splints like spreader grafts.
276 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006
Lateral Alar SuspensionIf lateralization of the alar base seems to be of majorbenefit, the following technique is helpful: laterally tothe alar base a small C-shaped island flap is outlined, atunnel dissected, and the flap inserted at the inneraspect of the alar base, thus pulling it laterally and in-creasing the skin surface to a small yet sometimescritical amount.
DISCUSSIONKasperbauer and Kern4 stated that knowledge of thestructure and function of the nasal valve region isrequired by all who operate on the nose. The nasal valvearea is a complex structure and recently differentiatedinto cartilaginous valve segment and bony valve seg-ment.5 Surgical improvement of impaired functiontherefore cannot follow a single reference. Evaluationof the airflow-limiting factors has to keep in mind the
contribution of structures beyond the valve area, thevariable mucovascular component of the turbinates andthe septum,6,7 and the consecutive limitations of surgicalinterference.
Anterior nasal septal deformity is responsible forpremature inspiratory collapse of the nasal valves8 andnasal obstruction in many patients. Only recently, diag-nostic recording of alar collapse was achieved by com-puter-assisted rhinomanometry9 and inspiratory andfixed nasal valve collapse was differentiated by acousticrhinometry.10 Standard techniques of septoplasty oftenfail to create the desired results. The technique ofextracorporeal septoplasty,3 as described in detail by thesenior author, in severe cases is appropriate in our hands,allowing replacement of a stable and straight septum intothe midline to separate the vestibules and nasal valvessymmetrically. Simultaneously reconstruction and main-taining tip support is achieved and alar collapse on theside of the former deviation prevented. In selected cases of
Figure 16 (A) Patient with loss of anterior septum by previous septoplasty. (B) A template for a rib cartilage graft is outlined accordingto an x-ray profile image. (C) Postoperative profile. (D) Preoperative view from below showing the tip collapse as reason for valvulardysfunction. (E) Tip support restored by an adequately high columellar part of the L-shaped rib graft.
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 277

sharply bent anterior septal deviation, the technique ofscoring, splinting, and suturing achieves stability as well.A straight septum is important for unimpaired nasal valvefunction,11 and if material is missing, replacement isrequired.12 In any case, the goal is creating bilateralsymmetrical cross sections in the nasal valve area. Accord-ing to Pirila and Tikanto,13 the subjective sensation ofnasal obstruction is decreased significantly by increase ofcross-sectional area on the side of the deviation, althoughon the opposite side the cross-sectional area is reducedand the bilateral parameters of acoustic rhinometry andrhinomanometry show only a slight increase or none.14
Adamson et al15 stated no objective nasal obstruc-tion measured by posterior rhinomanometry in 50 pa-tients before and after reduction rhinoplasty ‘‘despite thepotential for a decreased cross-sectional area of the valveregion’’ (not displayed by the applied posterior exami-nation technique; author’s comment), whereas 5 yearslater in a prospective study by acoustic rhinomanometryGrymer16 verified a 25% decrease in cross-sectional areaat the nasal valve versus 13% decrease at the piriformaperture after aesthetic reduction rhinoplasty comparedwith the preoperative values.
Also, Roithmann et al17 found a significant de-crease in cross-sectional area in the nasal valves byacoustic rhinometric assessment in postrhinoplasty nasalobstruction patients compared with a healthy popula-tion. A new classification of the internal nasal valvetypes18 according to the cross-sectional configurationmay help to select the appropriate technique of valvularimprovement.
In reduction rhinoplasty, specific measures areessential to prevent airway compromise. Suture tech-niques for cartilaginous vault reconstruction on top of areduced septal dorsum might be sufficient.19 A bend-ing suture technique for vault reconstruction in eachupper lateral cartilage was presented by Ozturan et al.20
In a series of 28 patients with tension nose, the angle ofthe internal nasal valves was measured preoperativelyand 12 months postoperatively, showing an increase
from 9.1 degrees preoperatively to 25.3 degrees post-operatively.
A combination of suture techniques and cartilagegrafts might be more reliable and was proposed by Meyeret al21 for correcting collapsed alae or posterior valvulardisturbance, placing a slightly convex septal or auricularslice cartilage over the involved cartilages modified bypreceding sutures to place them in a more convexposition. Park22 suggested flaring sutures to augmentthe repair of the dysfunctional nasal valve, and subse-quently these were combined with spreader grafts.23,24
For severe internal nasal valve dynamic incompetence,Sciuto and Bernardeschi25 presented a similar solution.The upper lateral cartilages are dissected off the septum.The dorsal septal border is widened by dorsal spreadergrafts and the dorsal margins of the upper lateral carti-lages are sutured together over the suspending septum.
Spreader grafts alone sometimes fail to preventimpairment of breathing in our experience in reductionof a narrow nose with a high dorsum. But in many casesthey represent a great improvement for maintenance ofvalvular function in rhinoplasty compared with earliertechniques. Hurst26 described the placement of strips ofcartilage without dividing the upper lateral cartilages,preserving their continuity across the dorsum to straddlethem effectively, confirmed by Andre et al.27 As a singlemeasure, we apply this technique in revision casesimproving the sidewall tension and configuration incases of middle vault collapse. Described by Sheen inendonasal rhinoplasty, the spreader grafts became awidespread technique applied in the external approach.28
Constantinides et al29 reported the lasting objectiveimprovement on the nasal valve by spreader grafts inopen cosmetic septorhinoplasty. This technique resultedin an 89% improvement of internal valvular function bysubjective data from patients in a minimum of 12 monthsfollow-up,30 17% of the patients treated simultaneouslywith batten grafts. As a modification, minispreadergrafts taken from the cephalic border of the lower lateralcartilages were sutured to the septum, preserving a
Figure 17 (A) Patient with a wide columellar base—the only reason for a severe breathing impairment. (B) Small columellar shapeafter depressor muscle resection, cartilage transsection, and resorbable mattress sutures, 7 months postoperatively.
278 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006

fibromucous connection and simultaneously suspendingthe nasal tip, with rhinomanometric data demonstratingan improvement in total mean nasal airflow.31
Batten grafts are recommended in cases of dy-namic insufficiency of the nasal valves, contrary to stat-ically narrowed valves indicating spreader grafts.18,24,30
Toriumi et al32 precisely described the placement ofbatten grafts at the site of maximal lateral nasal wallcollapse, applying curved septal or auricular cartilagegrafts into pockets through limited endonasal incisionsor by open approach. Patients’ scoring and clinical testingconfirmed a high success rate in treatment of external orinternal nasal valve collapse except for cases of excessivenarrowing at the piriform aperture, loss of vestibular skin,or scarring. Other authors found the batten grafts aseffective33–36 with minimal side effects such as minoraesthetic fullness in the augmented area. They work like alaminated spring reinforcing weak alar or upper lateralcartilages or the junction of both, the scroll area especiallyin postsurgical weakness. Placement requires great carenot to protrude the wall internally and reducing the cross-sectional area.
In this context, the treatment of external nasalvalve (alar rim) collapse is focused on alar rim battengrafts or lateral crural struts placed as overlay or underlaygrafts.37–39
Related techniques of structural grafting for air-flow improvement are important in cases of loss of tipsupport and changes in nasal tissue resilience resultingfrom rhinoplasties or aging effects,40–43 varying fromseptal extension grafts to total reconstruction of the alarcartilages with a partially split septal cartilage graft. Inour hands, septal extension grafts stabilized withspreader grafts such as splints are most effective.
A significantly wide columellar base can be thepredominant cause for valvular dysfunction and has to becorrected by columelloplasty.44 In some cases, the truelocus and solution to the problem lies lateral to the nasalvalve angle in the fibroareolar tissue that connects thelateral aspect of the lateral crus to the bony pyriformaperture. Then trimming a lateral crural J flap forincreasing lateral and caudal tension is successful inopening the nasal valves.45 Other ancillary techniquessuch as lateral suture suspension are most effective inspecial cases of valvular dysfunction related to weakenedmuscular activity, narrow vestibular floor or medializedalar base, nasal valve stenosis, and facial palsy.46–49 Thefinding of airflow improvement following face lifts50
confirms these proposals. Some cases of severe valvularstenosis following rhinoplasty require revision osteoto-mies with outfracture of the nasal bones.51
CONCLUSIONWe state with Croce et al52: The rhinosurgeon should beable to locate precisely the cartilaginous and/or osseus
structural deformity impairing nasal airflow. The rhino-surgeon has to realize the functional drawbacks associ-ated with a planned rhinoplasty procedure, employ aproper approach to the region, and apply prophylactictechniques not to endanger nasal valve function to satisfyaesthetics.
REFERENCES
1. Ricci E, Palonta F, Preti G, et al. Role of nasal valve in thesurgically corrected nasal respiratory obstruction: evalua-tion through rhinomanometry. Am J Rhinol 2001;15:307–310
2. Eccles R. Nasal airflow in health and disease. Acta Otolaryngol2000;120:580–595
3. Gubisch W. Extracorporeal septoplasty for the markedlydeviated septum. Arch Facial Plast Surg 2005;7:218–226
4. Kasperbauer JL, Kern EB. Nasal valve physiology. Implica-tions in nasal surgery. Otolaryngol Clin North Am 1987;20:699–719
5. Wexler DB, Davidson TM. The nasal valve: a review of theanatomy, imaging, and physiology. Am J Rhinol 2004;18:143–150
6. Cole P. Biophysics of nasal airflow: a review. Am J Rhinol2000;14:245–249
7. Cole P. The four components of the nasal valve. Am J Rhinol2003;17:107–110
8. Santiago-Diez de Bonilla J, McCaffrey TV, Kern EB. Thenasal valve: a rhinomanometric evaluation of maximum nasalinspiratory flow and pressure curves. Ann Otol RhinolLaryngol 1986;95(3 Pt 1):229–232
9. Grutzenmacher S, Gunther M, Robinson DM, Mlynski G,Beule A. Investigations for the diagnostic recording of nasalwing collapse. Laryngoscope 2005;115:1763–1767
10. Vidyasagar R, Friedman M, Ibrahim H, Bliznikas D, JosephNJ. Inspiratory and fixed nasal valve collapse: clinical andrhinometric assessment. Am J Rhinol 2005;19:370–374
11. Urquhart AC, Bersalona F. Septoplasty: correcting the nasalvalve. Laryngoscope 1997;107:537–539
12. Boccieri A. Subtotal reconstruction of the nasal septum usinga conchal reshaped graft. Ann Plast Surg 2004;53:118–125
13. Pirila T, Tikanto J. Unilateral and bilateral effects of nasalseptum surgery demonstrated with acoustic rhinometry,rhinomanometry, and subjective assessment. Am J Rhinol2001;15:127–133
14. Roithmann R, Cole P, Chapnik J, Barreto SM, Szalai JP,Zamel N. Acoustic rhinometry, rhinomanometry, and thesensation of nasal patency: a correlative study. J Otolaryngol1994;23:454–458
15. Adamson P, Smith O, Cole P. The effect of cosmeticrhinoplasty on nasal patency. Laryngoscope 1990;100:357–359
16. Grymer LF. Reduction rhinoplasty and nasal patency: changein the cross-sectional area of the nose evaluated by acousticrhinometry. Laryngoscope 1995;105(4 Pt 1):429–431
17. Roithmann R, Chapnik J, Zamel N, Barreto SM, Cole P.Acoustic rhinometric assessment of the nasal valve. Am JRhinol 1997;11:379–385
18. Miman MC, Deliktas H, Ozturan O, Toplu Y, Akarcay M.Internal nasal valve: revisited with objective facts. Otolar-yngol Head Neck Surg 2006;134:41–47
NASAL VALVES—IMPORTANCE AND SURGICAL PROCEDURES/FISCHER, GUBISCH 279
19. Fayman MS, Potgieter E. Nasal middle vault support: a newtechnique. Aesthetic Plast Surg 2004;28:375–380; discussion381–382
20. Ozturan O, Miman MC, Kizilay A. Bending of the upperlateral cartilages for nasal valve collapse. Arch Facial PlastSurg 2002;4:258–261
21. Meyer R, Jovanovic B, Derder S. All about nasal valvecollapse. Aesthetic Plast Surg 1996;20:141–151
22. Park SS. The flaring suture to augment the repair of thedysfunctional nasal valve. Plast Reconstr Surg 1998;101:1120–1122
23. Schlosser RJ, Park SS. Functional nasal surgery. OtolaryngolClin North Am 1999;32:37–51
24. Schlosser RJ, Park SS. Surgery for the dysfunctional nasalvalve. Cadaveric analysis and clinical outcomes. Arch FacialPlast Surg 1999;1:105–110
25. Sciuto S, Bernardeschi D. Upper lateral cartilage suspensionover dorsal grafts: a treatment for internal nasal valvedynamic incompetence. Facial Plast Surg 1999;15:309–316
26. Hurst WB. Internal nasal implant to correct nasal valveobstruction. J Laryngol Otol 1978;92:47–50
27. Andre RF, Paun SH, Vuyk HD. Endonasal spreader graftplacement as treatment for internal nasal valve insufficiency:no need to divide the upper lateral cartilages from theseptum. Arch Facial Plast Surg 2004;6:36–40
28. Rohrich RJ, Hollier LH. Use of spreader grafts in theexternal approach to rhinoplasty. Clin Plast Surg 1996;23:255–262
29. Constantinides MS, Adamson PA, Cole P. The long-termeffects of open cosmetic septorhinoplasty on nasal air flow.Arch Otolaryngol Head Neck Surg 1996;122:41–45
30. Khosh MM, Jen A, Honrado C, Pearlmann SJ. Nasal valvereconstruction: experience in 53 consecutive patients. ArchFacial Plast Surg 2004;6:167–171
31. Boccieri A. Mini spreader grafts: a new technique associatedwith reshaping of the nasal tip. Plast Reconstr Surg2005;116:1525–1534
32. Toriumi DM, Josen J, Weinberger M, Tardy MD Jr. Useof alar batten grafts for correction of nasal valve collapse.Arch Otolaryngol Head Neck Surg 1997;123:802–808
33. Millman B. Alar batten grafting for management of thecollapsed nasal valve. Laryngoscope 2002;112:574–579
34. Becker DG, Becker SS. Treatment of nasal obstruction fromnasal valve collapse with alar batten grafts. J Long Term EffMed Implants 2003;13:259–269
35. Constantian MB. The incompetent external nasal valve:pathophysiology and treatment in primary and secondaryrhinoplasty. Plast Reconstr Surg 1994;93:919–931; discussion932–933
36. Armengot M, Perez A, Izquierdo J, Campos A, Basterra J.Upper lateral cartilage transposition in the surgical manage-ment of nasal valve incompetence. Acta Otorrinolaringol Esp2001;52:373–378
37. Troell RJ, Powell NB, Riley RW, Li KK. Evaluation of anew procedure for nasal alar rim and valve collapse: nasal alarrim reconstruction. Otolaryngol Head Neck Surg 2000;122:204–211
38. Kalan A, Kenyon GS, Seemungal TA. Treatment of externalnasal valve (alar rim) collapse with an alar strut. J LaryngolOtol 2001;115:788–791
39. Rohrich RJ, Raniere J Jr, Ha RY. The alar contour graft:correction and prevention of alar rim deformities inrhinoplasty. Plast Reconstr Surg 2002;109:2495–2505;discussion 2506–2508
40. Ochi JW, deWerd DL. Surgery for bilateral nasal valvularcollapse. Rhinology 1988;26:105–110
41. Dyer WK II, Yune ME. Structural grafting in rhinoplasty.Facial Plast Surg 1997;13:269–277
42. Ishida LC, Ishida J, Henrique Ishida L, Passos AP, VieiraJC, Ferreira MC. Total reconstruction of the alar cartilageswith a partially split septal cartilage graft. Ann Plast Surg2000;45:481–484
43. Gassner HG, Remington WJ, Sherris DA. Quantitativestudy of nasal tip support and the effect of reconstructiverhinoplasty. Arch Facial Plast Surg 2001;3:178–184
44. Ghidini A, Dallari S, Marchioni D. Surgery of the nasalcolumella in external valve collapse. Ann Otol RhinolLaryngol 2002;111:701–703
45. O’Halloran LR. The lateral crural J-flap repair of nasal valvecollapse. Otolaryngol Head Neck Surg 2003;128:640–649
46. Paniello RC. Nasal valve suspension. An effective treatmentfor nasal valve collapse. Arch Otolaryngol Head Neck Surg1996;122:1342–1346
47. Lee DS, Glasgold AI. Correction of nasal valve stenosis withlateral suture suspension. Arch Facial Plast Surg 2001;3:237–240
48. Friedman M, Ibrahim H, Syed Z. Nasal valve suspension: animproved, simplified technique for nasal valve collapse.Laryngoscope 2003;113:381–385
49. Friedman M, Ibrahim H, Lee G, Joseph NJ. A simplifiedtechnique for airway correction at the nasal valve area.Otolaryngol Head Neck Surg 2004;131:519–524
50. Capone RB, Sykes JM. The effect of rhytidectomy on thenasal valve. Arch Facial Plast Surg 2005;7:45–50
51. Pontell J, Slavit DH, Kern EB. The role of outfracture incorrecting post-rhinoplasty nasal obstruction. Ear NoseThroat J 1998;77:106–108111–112
52. Croce G, Croce A, Neri G, Bianchedi M, Moretti A,Sacilotto C. The history of nasal valve surgery. ActaOtorhinolaryngol Ital 1996;16:189–201
280 FACIAL PLASTIC SURGERY/VOLUME 22, NUMBER 4 2006