Embed Size (px)
Citation preview

1
14th Northern Cleft Foundation (NCF) Annual Trip to Nagpur, India, 2014 Dr Alex Bonner ST7 NW Deanery 1.0 Introduction 2.0 Northern Cleft Foundation (NCF) 3.0 Location 4.0 Clinical Aspects 5.0 Audit & Education 6.0 Social Aspects 7.0 Conclusion 8.0 Acknowledgements 1.0 Introduction I am an Anaesthetic ST7 trainee and was fortunate enough to join the Northern Cleft Foundation (NCF) on a trip to Nagpur, India in January 2014 with the aim of supporting an intensive 2-‐week surgical ‘camp’ treating patients with cleft lip and / or palate deformity. 2.0 Northern Cleft Foundation (NCF) The NCF was founded 2001 by Dr George Teturswamy, a Consultant Anaesthetist from the North West of England after identifying that a high proportion of children with cleft deformities in India had not had them repaired. This results in poor feeding, poor speech and has wider social implications e.g. children being excluded from education, or not able to marry. NCF has gone from strength to strength since its inception, and this was the 14th year that it has run. Camps have been held in Mysore, Hyderabad, Kerala and Nagpur, and over 850 patients have benefited. 3.0 Location 3.1 Nagpur, Maharashtra This trip was to Nagpur, which is in Maharashtra. Maharashtra is a large state in west central India, and includes the cities of Mumbai and Pune. Nagpur is the next biggest metropolis, with a population of approximately 2.5 million. Nagpur is known as the ‘Orange City’ as it is a major trading city for oranges which grown plentifully in the surrounding area. There are also several tiger reserves which are a short drive away. Nagpur itself is a typical bustling Indian city, and again is typical in that there is a vast rich-‐poor divide. It is usual to see
2
families asleep underneath the sections of elevated roads, and on the first run to the hospital (7am) they would be lighting fires to prepare food and drink.
Fig 1. Typical Nagpur scene. India is the second most populous country in the world, with a population of approximately 1.2 billion people. Modern India is characterised by a vast discrepancy between its rich and its poor. Healthcare provision reflects this – it is possible to find state of the art private, modern hospitals in the large urban areas that deliver a standard of care that the NHS would be envious of. In contrast, conditions in the state hospitals (particularly the mission hospitals) are antiquated and significantly below the standards we are used to in the UK. I have been fortunate enough to also work in Uganda during my anaesthetic training programme – conditions in Ugandan hospitals are poor, but are more commensurate with the economic situation of the country. Conditions in Mure Memorial Hospital were not much better than those in Mbarara, Uganda, yet the GDP per capita in India is $4209 compared to $1414 in Uganda. 3.2 Mure Memorial Hospital Mure Memorial Hospital (MMH) was created by Dr Agnes Henderson, who hailed from Aberdeen, in 1896. I can’t begin to imagine how challenging that must have been – I am sure Dr Henderson was a formidable woman! MMH is a Christian-‐mission hospital who offer multiple medical and surgical specialties to those members of the population who can’t afford to pay for their medical care. NCF has worked alongside several different hospitals and some of these have been more successful than others. It is not uncommon for a local hospital to try to capitalise on the workload and prestige that the NCF brings, but there have been no such issues with MMH. 3.3 Our hosts: Rotary Club of Nagpur West

3
We were warmly received and welcomed by the Rotary Club of Nagpur West. This group consisted of some local doctors and who had worked very hard to ensure that the camp ran smoothly. This required a considerable amount of hard work to find, review and assist patients from the surrounding area to come to the camp during the period of time NCF were operating. In total, a 400 km radius was scoured; 12 500 postal leaflets were distributed, often to areas where cars could not reach. One of the local doctors recounted a story whereby he had driven for most of the day, parked his car, and then walked for 8 hours to a village where he knew there was a child with a cleft deformity. When he got there, the parents were very reluctant to let him organise the surgery because their child was somewhat of a local celebrity! Eventually he managed to purport the benefits of surgery and the child was treated during our camp.
Fig 2. Rotary Club Nagpur West Closing Ceremony, Nagpur Cricket Ground Another component of the pre-‐camp work is iron supplementation. Last year, a considerable number of patients had to be cancelled due to pre-‐operative iron-‐deficient anaemia. Iron supplementation was routinely offered to all patients for 3 months prior to the camp and this meant that far fewer patients were cancelled due to anaemia. Our average pre-‐op Hb was 10.77 g/dL. 4.0 Clinical Aspects 4.1 Logistics and the team We ran 5 operating tables across 3 theatres. Each table was staffed with a consultant cleft lip & palate surgeon (and a registrar), an anaesthetic consultant (and a registrar), an ODP and scrub nurse. We were fortunate to have a floating consultant anaesthetist to trouble-‐shoot and help ensure everything ran smoothly. A room which was known as the ICU was morphed into our recovery area, and staffed with 2 nurses and usually an anaesthetic registrar. A single
4
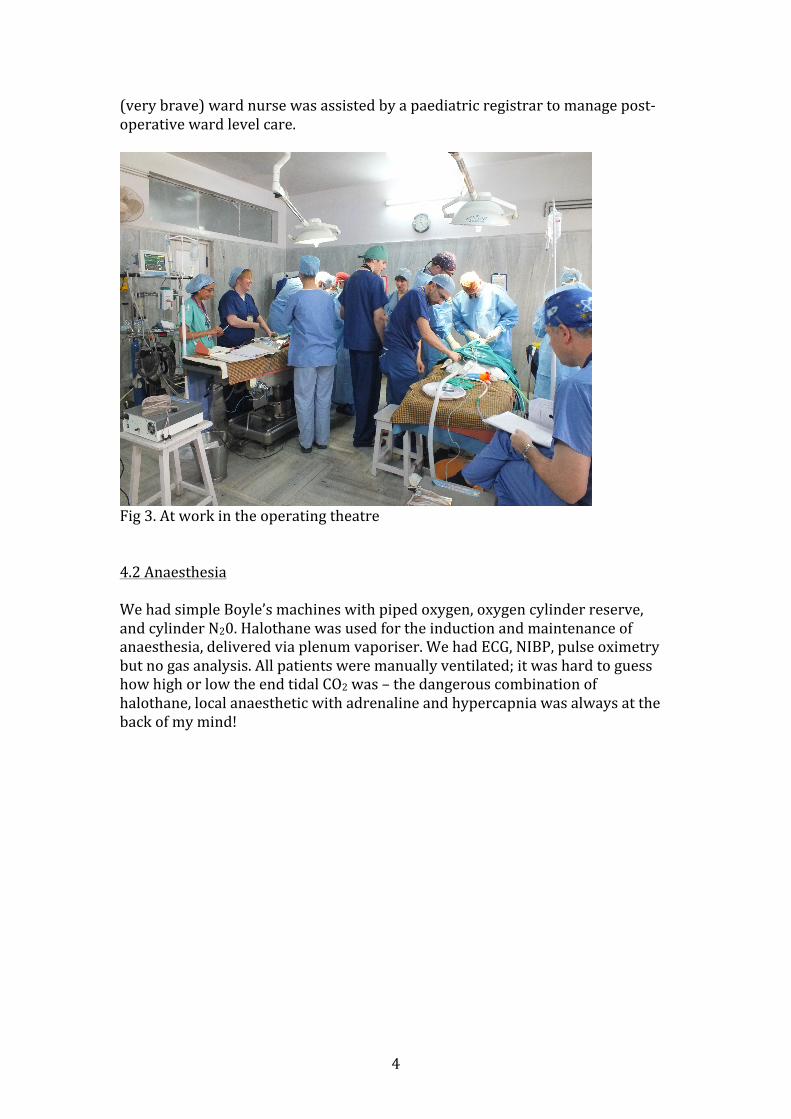
(very brave) ward nurse was assisted by a paediatric registrar to manage post-‐operative ward level care.
Fig 3. At work in the operating theatre 4.2 Anaesthesia We had simple Boyle’s machines with piped oxygen, oxygen cylinder reserve, and cylinder N20. Halothane was used for the induction and maintenance of anaesthesia, delivered via plenum vaporiser. We had ECG, NIBP, pulse oximetry but no gas analysis. All patients were manually ventilated; it was hard to guess how high or low the end tidal CO2 was – the dangerous combination of halothane, local anaesthetic with adrenaline and hypercapnia was always at the back of my mind!
5
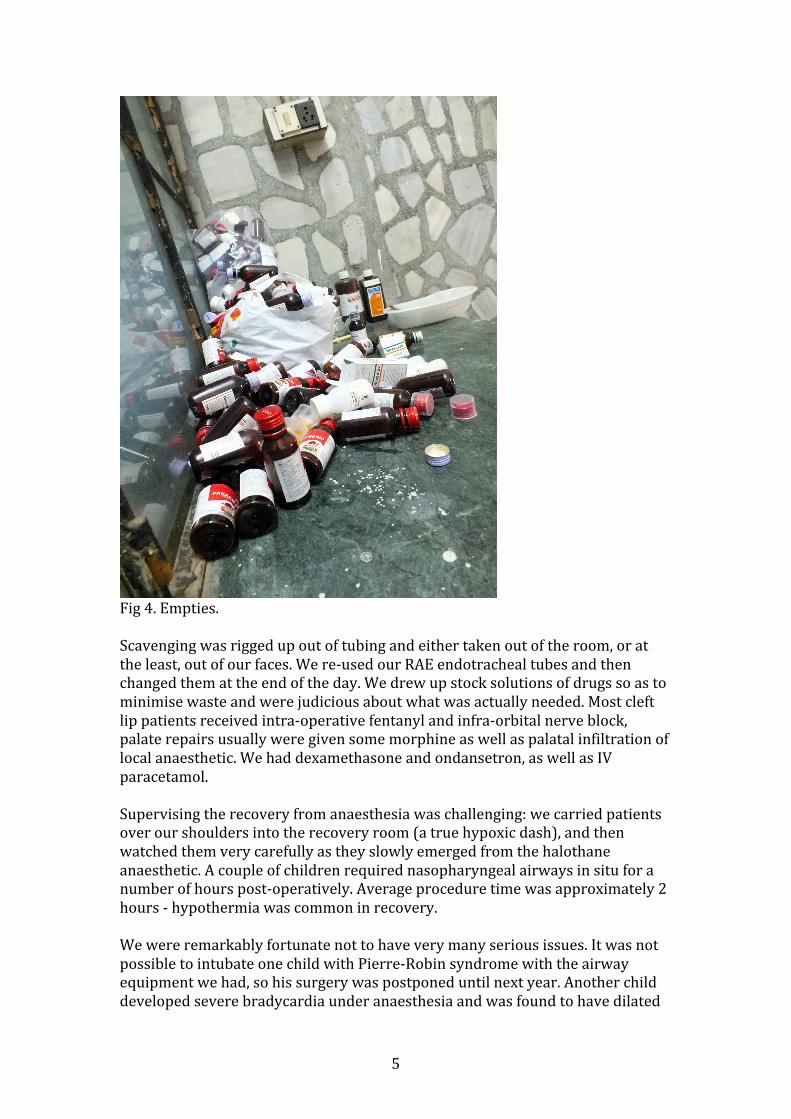
Fig 4. Empties. Scavenging was rigged up out of tubing and either taken out of the room, or at the least, out of our faces. We re-‐used our RAE endotracheal tubes and then changed them at the end of the day. We drew up stock solutions of drugs so as to minimise waste and were judicious about what was actually needed. Most cleft lip patients received intra-‐operative fentanyl and infra-‐orbital nerve block, palate repairs usually were given some morphine as well as palatal infiltration of local anaesthetic. We had dexamethasone and ondansetron, as well as IV paracetamol. Supervising the recovery from anaesthesia was challenging: we carried patients over our shoulders into the recovery room (a true hypoxic dash), and then watched them very carefully as they slowly emerged from the halothane anaesthetic. A couple of children required nasopharyngeal airways in situ for a number of hours post-‐operatively. Average procedure time was approximately 2 hours -‐ hypothermia was common in recovery. We were remarkably fortunate not to have very many serious issues. It was not possible to intubate one child with Pierre-‐Robin syndrome with the airway equipment we had, so his surgery was postponed until next year. Another child developed severe bradycardia under anaesthesia and was found to have dilated

6
cardiomyopathy post-‐operatively. Fortunately she made a good recovery and was transferred to a nearby hospital where paediatric high dependency level care could be offered.
Fig 5. Complete heart block captured on ECG 4.3 Surgery Cleft deformity has an incidence of 1:700 in the UK, and 1:650 in India i.e. it is not significantly more prevalent. The difference is that surgery is not offered to children within their first year of life, as would be the case in the UK.
7
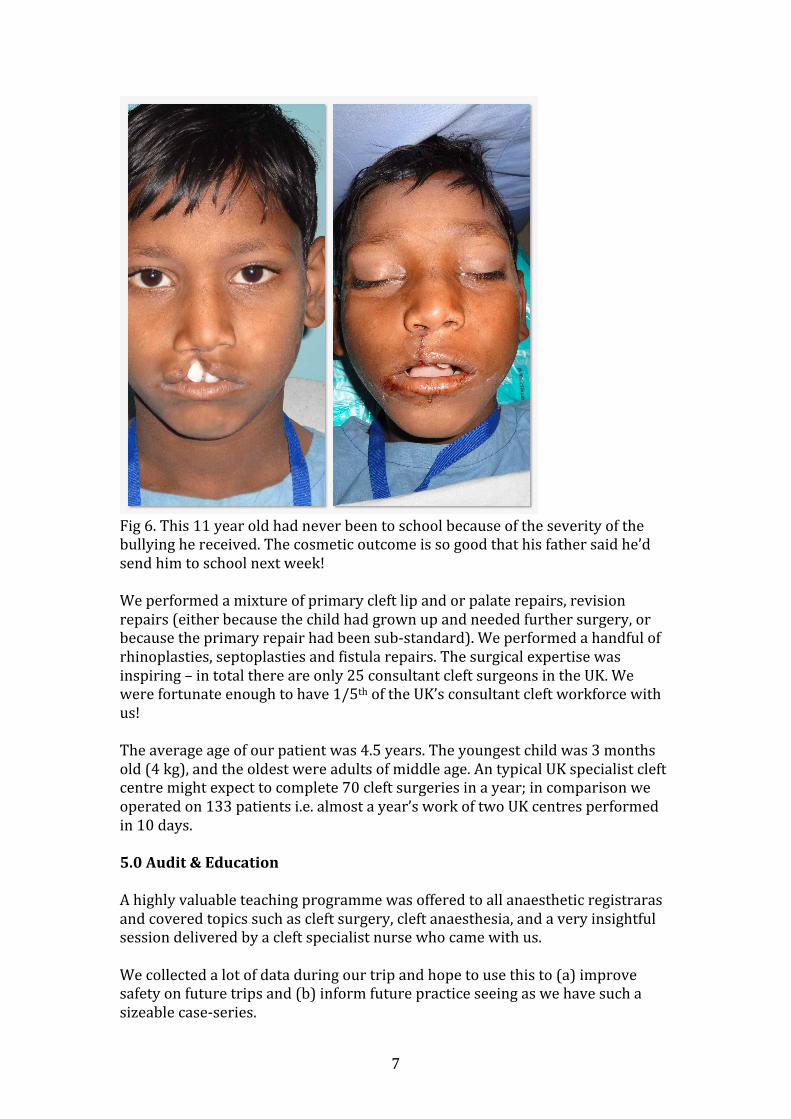
Fig 6. This 11 year old had never been to school because of the severity of the bullying he received. The cosmetic outcome is so good that his father said he’d send him to school next week! We performed a mixture of primary cleft lip and or palate repairs, revision repairs (either because the child had grown up and needed further surgery, or because the primary repair had been sub-‐standard). We performed a handful of rhinoplasties, septoplasties and fistula repairs. The surgical expertise was inspiring – in total there are only 25 consultant cleft surgeons in the UK. We were fortunate enough to have 1/5th of the UK’s consultant cleft workforce with us! The average age of our patient was 4.5 years. The youngest child was 3 months old (4 kg), and the oldest were adults of middle age. An typical UK specialist cleft centre might expect to complete 70 cleft surgeries in a year; in comparison we operated on 133 patients i.e. almost a year’s work of two UK centres performed in 10 days. 5.0 Audit & Education A highly valuable teaching programme was offered to all anaesthetic registraras and covered topics such as cleft surgery, cleft anaesthesia, and a very insightful session delivered by a cleft specialist nurse who came with us. We collected a lot of data during our trip and hope to use this to (a) improve safety on future trips and (b) inform future practice seeing as we have such a sizeable case-‐series.
8
Fig 7. The anaesthetic registrars 6.0 Social aspects By its very nature, this was a highly sociable trip. We numbered over 40 in total, and got to know one other pretty well – aided by a long journey via Dubai and Mumbai. Despite the long working hours, we found time to make the gym (sometimes at 5-‐something a.m.) and to equally unwind with a beer at the end of the day. A few of us made a trip to Pench Tiger Reserve, where we had a great trip into the jungle despite not seeing any tigers! I am told that it was 30°C during the day whilst we were there, but all I can say was that the average temperature in the OT was 24.6°C!

9
Fig 8. A chance to unwind 7.0 Conclusion It felt incredibly humbling to be part of such a well-‐oiled machine. I asked Dr Teturswarmy how he selected his team, and he answered “the team selects itself”. This is a testament to the commitment of everyone involved, many of whom return year after year to work 12 hours per day during their annual leave. To be able to literally put a smile on these children’s’ faces makes this an incredibly rewarding project to be involved with, and I can see why NCF goes from strength to strength. 8.0 Acknowledgements I would like to take this opportunity to thank everyone who was generous enough to offer financial support for this trip. Thanks to Dr Teturswarmy for inviting me. Thanks also to our generous hosts for all the ground work.





























