-
INVITED REVIEW
Contributions of cardiomyocytecardiac fibroblastimmunecell
interactions in heart failure development
Katsuhito Fujiu Ryozo Nagai
Received: 22 February 2013 / Revised: 13 March 2013 / Accepted:
21 March 2013 / Published online: 6 June 2013
Springer-Verlag Berlin Heidelberg 2013
Abstract The heart contains various types of cells,
including cardiomyocytes, cardiac fibroblasts, many kinds of
immune cells and vascular cells. Initial studies mainly
focused on cardiomyocytes, which directly reflect the con-
tractile function of the heart. Recently, pivotal functions
of
cardiac fibroblasts have been revealed in the maintenance of
cardiac function, physiological cardiac remodeling after
heart
stress and pathological remodeling using genetically engi-
neered mouse models, like the fibroblast-specific gene
knockout mouse, bone marrow transplantation and immune
cell-specific gene knockout. Moreover, chronic inflammation
is considered to be a basic pathological mechanism that
underlies various diseases, including heart failure. In the
development of heart failure, the contributions of immune
cells like T lymphocytes and monocyte/macrophage lineage
cells have been also reported. Immune cells have diverse and
multiple functions in regulating both pro-inflammatory
effects and the resolution of heart failure. On the one
hand,
immune cells have protective effects to compensate for and
overcome heart stresses. On the other hand, they also con-
tribute to sustained inflammation and result in the develop-
ment of heart failure. These observations prompted a shift
in
the heart-related studies to include the complex communi-
cations between cardiomyocytes and other kinds of cardiac
cells, including inflammatory cells residing in or recruited
to
the heart. This review will summarize the current knowledge
regarding cellcell interactions during cardiac remodeling
and the development of heart failure. We will especially
focus on the interactions among cardiomyocytes, cardiac
fibroblasts and immune cells.
Keywords Cardiac fibroblast Cardiomyocyte Cellcellinteraction
Heart failure Immune cell
Introduction
In the heart, cardiac fibroblasts, immune cells and vascular
cells, including vascular endothelial cells and vascular
smooth muscle cells, are all present. Under steady-state
conditions, non-myocytes may exhibit a quiescent pheno-
type, whereas cardiomyocytes are always beating. After the
exposure to heart stress, such as myocardial infarction,
pressure overload, myocarditis, volume overload and so on,
the cardiac fibroblasts change their phenotype to become
activated fibroblasts, which produce growth factors, cyto-
kines, chemokines and extracellular matrix [46]. Simulta-
neously, a variety of immune cells, such as T lymphocytes
and monocyte/macrophage lineage cells infiltrate into the
heart. These T lymphocytes and monocytes/macrophages
have diverse functions, which are regulated in a spatial and
This article is part of the Topical Collection Novel
Perspectives on
Heart Failure.
K. Fujiu (&) R. Nagai (&)Department of Cardiovascular
Medicine, University of Tokyo,
7-3-1, Hongo, Bunkyo, Tokyo 113-8655, Japan
e-mail: [email protected]
R. Nagai
e-mail: [email protected]
K. Fujiu
Translational Systems Biology and Medicine Initiative
(TSBMI), the University of Tokyo Graduate School of
Medicine,
Tokyo, Japan
R. Nagai
Funding Program for World-Leading Innovative R&D on
Science and Technology (FIRST Program), Tokyo, Japan
R. Nagai
Jichi Medical University, Tochigi, Japan
123
Basic Res Cardiol (2013) 108:357
DOI 10.1007/s00395-013-0357-x
-
temporal manner [93, 106]. The cellcell interactions
among cardiomyocytes and non-myocytes within the
interstitium of the heart have become an increasingly
popular focus of research on heart failure. These interac-
tions promote adaptive responses against heart stress, and
compensate or overcome these stresses. On the other hand,
these interactions can also provoke pathological remodel-
ing associated with heart diseases, and can thereby result
in
heart failure and cardiac death. In this review, we will
present the current knowledge regarding cellcell interac-
tions in the heart after heart stress, such as myocardial
infarction and pressure overload. We will especially focus
on the contribution of cellcell interactions among
cardiomyocytes, cardiac fibroblasts and immune cells to
heart failure.
Cellular components of the heart
Cardiomyocytes, cardiac fibroblasts, endothelial cells,
vascular smooth muscle cells and immune cells are all
major cellular components of the heart. In the 1970s,
efforts to establish the cellular populations of the adult
heart in rats were reported, based on a morphological
analysis using electron microscopy or gradient centrifuga-
tion. Recently, several common cardiac fibroblast markers
have been reported. Discoidin domain receptor 2 (DDR2)
[8] and CD90/thymus cell antigen-1 (Thy1) [42] are cell-
surface markers that can be used for fluorescence-activated
cell sorting (FACS). These discoveries showed that the
adult murine myocardium is composed of 56 % myocytes,
27 % fibroblasts, 7 % endothelial cells and 10 % vascular
smooth muscle cells [8]. Moreover, in the adult rat heart,
the number of cardiomyocytes was 30 %, that of fibroblasts
was 64 % and non-myocyte and non-fibroblast cell popu-
lations made up the remaining 6 %, which includes
immune cells and vascular cells [8]. The approaches using
FACS enabled the analysis of the relative percentages of
distinct, definable cell types present in the developing and
adult heart, as well as the elucidation of the cellcell
communications among various cells within the heart
during the homeostatic state, adaptive response state and
during the development of heart disease.
Cardiomyocytecardiac fibroblast interaction
The important role of cellcell communication between
cardiomyocytes and cardiac fibroblasts in both develop-
ment and/or cardiovascular diseases was implied by an
initial in vitro study using conditioned media or a simpli-
fied co-culture system [25]. For example, murine cardio-
myocytes developed a hypertrophied phenotype when they
were co-cultured with cardiac fibroblasts or their condi-
tioned media supplemented with interleukin (IL)-6. In that
report, the IL-6 signaling in cardiomyocytes in co-culture
with cardiac fibroblasts was suggested to be key in pro-
moting cardiomyocyte hypertrophy [31]. In addition to
IL-6, the tumor necrosis factor (TNF)a production was
alsoupregulated by cardiomyocytes when they were co-cul-
tured with cardiac fibroblasts [9]. These results from co-
culture systems suggested that paracrine factors are one of
the method by which cardiomyocytes and cardiac fibro-
blasts communicate. However, forced physical disconnec-
tion between cardiomyocytes and cardiac fibroblast using
an antibody for a cardiac fibroblast plasma membrane
protein or connexin 43 inhibited cell adhesion and
decreased the IL-6 production, but did not decrease the
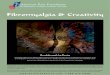
TNFa production [9]. These results highlighted theimportance of
direct cellcell interactions between
cardiomyocytes and cardiac fibroblasts, in addition to the
existence of multiple non-physical communication path-
ways mediated by cytokine production, during the devel-
opment of cardiac hypertrophy (Fig. 1). In addition to
cardiomyocyte hypertrophy, a recent in vitro study sug-
gested that cardiac fibroblasts also affected the
contractile
activity [59] and electrophysiological conditions of the
cardiomyocytes [77]. These results suggested that cardiac
fibroblasts may have pivotal pathological roles via their
interactions with cardiomyocytes in vivo. Many studies
have shown that cardiac fibroblasts were activated by heart
stresses and that they became proliferative and secreted
cytokines and growth factors and eventually differentiated
into cardiac myofibroblasts, which expressed smooth
muscle a-actin. There are a wide variety of heart
stresses,including mechanical stress, hypoxia [76], immune
cell-
derived inflammatory cytokines [107] and augmented
neurohormonal stimulation [64].
Among these stresses, the reninangiotensin system and
b-adrenergic stimulation have been extensively investi-gated.
Cardiac fibroblasts were found to express the
angiotensin II receptor [99] and b-adrenergic receptors[100] and
these receptors were involved in the pathological
process of heart diseases due to enhanced reninangioten-
sinaldosterone signaling [35, 82, 84] and chronic
b-adrenergic overstimulation [73]. These two signalingpathways
have been established as standard targets for the
treatment of heart failure. Recently, the interdependence
between angiotensin II receptor 1 and the serotonin
receptor [5-HT(2B)] in cardiac fibroblasts was reported
[44]. These two receptors in cardiac fibroblasts affected
the
sympathetic overstimulation-dependent heart failure, thus
suggesting that 5-HT(2B) might be a novel therapeutic
target for adrenergic overstimulation-dependent heart fail-
ure [44]. In addition to these signaling pathways, nuclear
factor kappa-light-chain-enhancer of activated B cells
Page 2 of 15 Basic Res Cardiol (2013) 108:357
123
-
(NF-jB) [5, 53], the Smad signaling pathway[38],
mitogenactivated protein kinase [72] and phosphoinositide
3-kinase
(PI3K) [15] were also suggested to be involved in cardiac
fibroblast activation during the development of heart fail-
ure, and might also be candidate therapeutic targets.
Cyclic nucleotide phosphodiesterase 1A (PDE1A) is a
key regulator of cardiac fibroblast activation induced by
angiotensin II and TGF-b through the Ca2?/calmodulinpathway both
in vitro and in vivo [71].
The extracellular heterodimeric protein S100A8/A9 is
produced in fibroblasts and macrophages in the heart fol-
lowing myocardial ischemia [104]. The production of
S100A8/A9 leads to increases in the activity of nuclear
factor (NF)-jB and the expression of proinflammatorycytokines in
cardiac fibroblasts and macrophages [104].
S100A8/A9 recruits macrophages into the heart by acti-
vating the receptor of advanced glycation end-products
(RAGE) on macrophage [104]. Secreted S100A8/A9
affects cardiomyocytes by activating MAP kinases JNK,
ERK1/2 and NF-jB, which mediates signals downstreamof RAGE
following ischemic heart failure and results in a
reduced cardiac function [104].
The TNF receptor superfamily member fibroblast
growth factor-inducible molecule 14 (Fn14) is produced
from cardiac fibroblasts in response to endothelin-1 stim-
ulated by right ventricular pressure overload [74]. Fn14
activates and leads to the proliferation of cardiac
fibroblast
cells autonomously, results in collagen synthesis via RhoA-
dependent nuclear translocation of myocardin-related
transcription factor-A (MRTF-A)/MAL [74].
In just the past decade, more details about the cellcell
interactions between cardiomyocytes and cardiac fibro-
blasts have been revealed by genetically manipulated mice
using the Cre-loxP system and estrogen receptor-inducible
system. This technique enabled the generation of cardio-
myocyte-specific [4, 39] and fibroblast-specific [45]
IL-6 family IL-6 family
GP130 GP130
cardiomyocyte cardiac fibroblast
JAK MAPK PI3K
hypertrophy cell death
iNOS
SERCAPLBRYR
contraction
extracellularmatrix
production
migrationproliferation
XONADPH
superoxideNO
peroxynitrite
Connexin43
IL-6 production
Stressinduced AngIIproduction
AngIIAT1
Fibroblast activation
AngIIIL-6 family
Fig. 1 Interleukin-6 family regulates the heart remodeling
bymodulating cardiomyocytes and cardiac fibroblasts. Current
knowl-
edge of cellular molecular mechanisms is shown. In
cardiomyocytes,
IL-6 induces cardiac hypertrophy via JAK signaling,
cardiomyocyte
death via MAPK and inducible nitric oxide synthase, xanthine
oxidase and NADPH oxidase expression through their receptor
GP130. Induced superoxide and nitric oxide produce
peroxynitrite.
Peroxynitrite decreases contractility through its effects on
SERCA2a,
ryanodine receptor and phospholamban. In cardiac fibroblasts,
IL-6
induces activation of extracellular matrix production and
migration
and proliferation of cardiac fibroblasts. Cardiac stresses
induce
angiotensin II production from cardiac fibroblasts and
secreted
angiotensin II induces IL-6 production of cardiomyocytes. IL
interleukin, JAK Janus Kinase, MAPK mitogen activated
protein
kinase, PI3K Phosphoinositide 3 kinase, SERCA Sarcoplasmic
reticulum calcium ATPase, XO xanthine oxidase, PLB
phospholam-
ban, iNOS inducible nitric oxide synthase, RYR ryanodine
receptor,
AngII angiotensin II, AT1 angiotensin II receptor type 1, IL-6
family
IL-6 leukemia inhibitory factor and cardiotropin-1
Basic Res Cardiol (2013) 108:357 Page 3 of 15
123
-
knockout or overexpression mice, and allowed the analysis
of cell type-specific functions in vivo. Haploinsufficiency
of a transcription factor, Klf5, inhibited cardiac hypertro-
phy and cardiac fibrosis after angiotensin II infusion or
pressure overload [86, 94]. However, cardiomyocyte-spe-
cific Klf5 knockout mice did not show any reduction of the
cardiac hypertrophy and fibrosis after left ventricular
pressure overload. On the other hand, fibroblast-specific
Klf5 knockout mice showed significantly suppressed car-
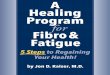
diac hypertrophy and fibrosis [94]. However, the fibroblast-
specific Klf5 knockout mice subsequently developed severe
heart failure, because of a truncation of the adaptive car-
diac response against pressure overload, including cardiac
hypertrophy and fibrosis, which resulted in heart failure
and cardiac death (Fig. 2).
Placental growth factor (Pgf) is another key regulator
of the interaction between cardiomyocytes and cardiac
fibroblasts. Pgf knockout mice died of severe heart failure
within a week after pressure overload [1]. Reductions of
fibroblast activation and angiogenesis after pressure
overload were observed. In contrast, the overexpression
PGF in cardiomyocytes augmented the cardiac hypertro-
phy in response to pressure overload [1]. Because the PGF
receptor is expressed in cardiac fibroblasts, but not in
cardiomyocytes, the PGF secreted from cardiomyocytes
only affects non-cardiomyocytes (mainly cardiac fibro-
blasts) and promoted cardiac adaptive responses after
pressure overload. Ras-associated domain family 1 iso-
form A (Rassf1a), a tumor suppressor gene, was reported
to enhance the secretion of TNFa by cardiac fibroblasts,and this
secreted TNFa facilitates the increases of thecardiac hypertrophy
and cardiac fibroblast proliferation
[20]. These reports also suggested that cardiac hypertro-
phy and cardiac fibrosis are part of an appropriate adap-
tive response, and that the loss of these adaptive responses
clearly resulted in a poor prognosis. Although cardiac
hypertrophy and cardiac fibrosis can be both a positive
and negative response to the physiological conditions, the
differences in the survival rates after heart stress in
genetically manipulated mice strongly support the
importance of these responses in the protection against
heart stress.
KLF5
IGF-1PDGF-A
KLF5 KLF5
Wild type cardiac fibroblast specific Klf5knockout mouse
a
b
pressure overloadangiotensin II infusion
cardiac hypertrophycardiac fibrosis
adaptive responsetruncation of adaptive responseby Klf5
deficiency in cardiac fibroblasts
htaeddnaeruliaftraehevila
pressure overload
Fig. 2 Cardiac fibroblasts facilitate adaptive responses
againstcardiac pressure overload. a In cardiac fibroblasts,
transcriptionfactor Kruppel-like factor 5 induces insulin-like
growth factor 1 and
platelet-derived growth factor A chain after pressure overload.
IGF1
is required for induced cardiac remodeling including cardiac
hyper-
trophy and cardiac fibrosis after pressure overload and
angiotensin II
infusion. b Although in wild-type mice, cardiac hypertrophy
and
cardiac fibrosis are observed after pressure overload, this
stress is
compensated by these appropriate responses and all mice can
survive.
Cardiac fibroblast-specific Kruppel-like factor 5 knock mice
develop
heart failure and show high mortality by lack of these
adaptive
responses. KLF5 Kruppel-like factor 5, IGF1 insulin-like
growth
factor 1, PDGF-A platelet-derived growth factor A chain
Page 4 of 15 Basic Res Cardiol (2013) 108:357
123
-
Cardiomyocytes and neuronal/vascular cell interactions
The sympathetic nervous system controls cardiac contrac-
tility, heart rate and cardiac hypertrophy through interac-
tion of neurons and cardiomyocytes by norepinephrine
secretion [109]. In neurons, angiotensin II induces and
nitric oxide inhibits sympathetic activation and norepi-
nephrine release [119]. In experimental models, ablation of
sympathetic nerves results in reduced cardiomyocytes size
[113]. These effects are mediated by the ubiquitin protea-
some followed by activation of autophagy. This atrophic
remodeling is caused by the reduction of basal stimulation
of adrenergic b2-receptors [113] and can be mimicked
byneuron-specific angiotensin converting enzyme 2 overex-
pression in mice which have lower norepinephrine levels.
The reduction of sympathetic activity protects against
cardiac hypertrophy induced by angiotensin II infusion
[27]. These results suggest that sympathetic neuroncar-
diomyocyte interactions induced by norepinephrine pro-
duction are required for the regulation of the
cardiomyocyte volume in maintenance and pathological
remodeling.
In terms of inflammation, vascular endothelial cells also
contribute to heart failure development by expressing cell
adhesion molecules. Cell adhesion molecules, including
selectins, integrins and the immunoglobulin gene super-
family of adhesion receptors, provoke leukocyte migration
from blood vessels into the cardiac interstitium [34].
Endothelial cell dysfunction via reduction of nitric oxide
production induces the expression of intercellular adhesion
molecule-1 (ICAM-1) and vascular cell adhesion mole-
cules-1 (VCAM-1). These cell adhesion molecules induce
the interaction of leukocytes with endothelial cells and
result in the accumulation of leukocytes; infiltrating leu-
kocytes provoke the interaction of immune cells, cardio-
myocytes and fibroblast via the actions of proinflammatory
cytokines.
Blood vessels supply oxygen for cardiac contraction. In
response to pressure overload, cardiomyocytes produce
VEGF and induce angiogenesis, thus adapting supply to the
increased oxygen demand of hypertrophic cardiomyocytes.
In later stages, p53 inhibits VEGF production from
cardiomyocytes and reduced oxygen supply contributes to
reduced contractile function and heart failure [83].
Contribution of inflammation in heart failure
development
The levels of many cytokines, chemokines and growth
factors were observed to be augmented during the adaptive
responses against heart stress and the development of heart
failure. These factors induce phenotypic changes in steady-
state cardiomyocytes and quiescent cardiac fibroblasts to
generate the active form of these cells, i.e. abundant
cytokine-producing cardiomyocytes and cardiac fibro-
blasts. Consequently, the increased paracrine factors from
these two kinds of cells can recruit immune cells and
provoke acute inflammatory changes. Recruited inflam-
matory cells from the bone marrow and spleen interact with
cardiomyocytes and cardiac fibroblasts, and make more
complex inflammatory statuses [46]. An acute response
that includes the infiltration of immune cells, like granu-
locytes and inflammatory monocytes/macrophages, into the
heart and the increased vascular permeability mainly exerts
favorable effects on the heart suffering from stresses and
injury, and enhances the cardiac repair, wound healing,
adaptive cardiac hypertrophy, etc. Supporting this idea, the
inhibition of acute inflammatory cell infiltration into the
heart by depletion of CC chemokine receptor 5 or intra-
venous injections of clodronate-containing liposomes
worsened the cardiac remodeling and healing after myo-
cardial infarction in model mice [102, 114]. However,
chronic inflammation has recently been reported to be a
common mechanism underlying many kinds of lifestyle-
related diseases, including coronary heart disease, diabetes
mellitus and cancer. Serum markers of inflammation, such
as the sustained elevation of inflammatory cytokines and
growth factors, in heart failure patients also augmented and
reflected the severity of their heart failure and clinical
outcomes [81, 97].
In chronic inflammation, macrophages undergo polari-
zation and contribute to tissue injury. In myocardial
infarction, classically activated macrophages produce pro-
inflammatory cytokines (M1 macrophages), and alterna-
tively activated macrophages (M2) anti-inflammatory
cytokines; both, are increased in the heart. Class A scav-
enger receptor (SRA) knockout mice have a reduction of
infiltrated M2 macrophages and increased M1 macro-
phages that result in exacerbation of the cardiac dysfunc-
tion and fibrosis following myocardial infarction [41]. A
particular importance of SRA for the M2 phenotype
polarization has been reported [41].
Bone marrow cells-derived mesenchymal stromal cells
(MSCs) also contribute to repair through their anti-
inflammatory effects. MSCs infiltrate into the heart fol-
lowing myocardial infarction and secrete interleukin-10,
which mediates a switch from an inflammatory monocyte/
macrophage lineage to anti-inflammatory lineages [41].
Regulatory T-cells are also suggested to contribute to
M2 polarization following myocardial infarction via IL-10
production [95].
In this context, the communication among immune cells,
cardiomyocytes and cardiac fibroblasts in the interstitium
of the heart leads to the formation of an immunoregulatory
network, and chronic inflammation might occur if these
Basic Res Cardiol (2013) 108:357 Page 5 of 15
123
-
cells fail to switch off their inflammatory programs, which
might lead to the inappropriate survival and retention of
leukocytes [11].
Intercellular mediators control cellcell interactions
Intercellular mediators produced by immune cells, cardio-
myocytes and cardiac fibroblasts are key factors in the
complex mechanism of connection among the different
types of cells, and have provided new therapeutic targets
for heart failure. In fact, during the development of heart
failure, large numbers of pro-inflammatory mediators are
secreted and contribute to the cellular dysfunction, modu-
late cellcell interactions, affect numerous signaling path-
ways and the cross-talk among signaling pathways [65].
Below, we describe the best-characterized mediators by
which immune cells, cardiomyocytes and cardiac fibro-
blasts interact during the development of heart failure and/
or the progression of other heart diseases.
Interleukins
Interleukins are a group of cytokines which are mainly
produced by immune cells, like T cells and monocyte/
macrophage lineage cells, as well as cardiomyocytes, car-
diac fibroblasts and vascular endothelial cells. IL-6 and
its
signal transducer, a 130-kDa glycoprotein (gp130; CD130)
is expressed in cardiomyocytes and cardiac fibroblasts, and
is associated with cardiac hypertrophy and cardiac fibrosis
[30] (Fig. 1). IL-6 is upregulated in the heart after myo-
cardial infarction [14, 22, 47]. The angiotensin II secreted
from cardiac fibroblasts also induced IL-6 production from
the cardiomyocytes, and an AT-1 receptor antagonist
inhibited cardiomyocyte hypertrophy and fibroblast pro-
liferation [30]. These results suggested that the IL-6 pro-
duction in cardiomyocytes contributes significantly to
cardiomyocyte hypertrophy by an autocrine pathway and to
cardiac fibroblast proliferation by a paracrine pathway.
Angiotensin II can induce various members of the IL-6
family, including IL-6, leukemia inhibitory factor and
cardiotropin-1, in cardiac fibroblasts [82]. These IL-6
family members induce significant hypertrophy of cardio-
myocytes through gp130 [82]. The administration of a
neutralizing antibody against IL-6 or gp130 (CD130)
resulted in the reduction of hypertrophic gene expression.
IL-6 blockade also led to reduced cardiac fibroblast pro-
liferation. Signal transducer and activator of transcription
3
(STAT3) is a key signal transducer that acts downstream of
gp130 in both cardiomyocytes and cardiac fibroblasts [28,
118]. Gp130 and STAT3 phosphorylation are altered in
end-stage dilated cardiomyopathy patients [79]. The
induction of signaling via the gp130STAT3 axis provoked
unfavorable downstream activation of this critical pathway
during heart failure [40]. The IL-6 family and gp130 axis is
the most extensively analyzed signal transduction pathway
between cardiomyocytes and cardiac fibroblasts in terms of
the effects on cardiac hypertrophy and cardiac fibrosis.
IL-1b and its receptor, the type I IL-1 receptor (IL-1RI), are
also markedly induced in the infarcted heart,
and this signaling is essential for the activation of the
fibrogenic pathways in the healing heart [12]. IL-1bleads to
extra cellular matrix remodeling by inducing the
migration of cardiac fibroblasts [72] and matrix
metalloproteinase production [87], which promotes car-
diac dilatation and cardiac rupture. IL-1b also inducescardiac
dysfunction through nitric oxide production [85],
modifying b-adrenergic signaling [37] and via a reduc-tion of
phospholamban [70]. On the other hand, IL-1RI
knockout mice showed decreased infiltration of neutro-
phils and macrophages into the myocardium after
ischemia/reperfusion injury [12]. Mice lacking the IL-1
receptor also showed a reduction of myofibroblast acti-
vation and collagen deposition, but no reduction of the
infarct size [12]. These results suggest that IL-1 signal-
ing regulates pathogenic cardiac remodeling in both
cardiomyocytes and cardiac fibroblasts.
IL-17, a recently identified cytokine, is released from
Th17 cells, which are a subset of CD4 effector T cells. IL-
17 is also induced in the infarct area after myocardial
infarction, and depletion of IL-17 by genetic deficiency or
a neutralizing antibody resulted in a reduction of the
infarct
size and preserved cardiac function [7, 63]. The mecha-
nisms underlying these effects of IL-17 are suggested to be
due to the fact that IL-17 provokes the apoptosis of
cardiomyocytes and induces chemokines that mediate
neutrophil migration [63]. In addition to Th17 cells, recent
in vitro studies suggested that cardiac fibroblasts can pro-
duce IL-17 and provoke collagen and metalloproteinase 1
production through the IL-17 receptor expressed on the
cardiac fibroblasts [16, 103]. These results imply that
IL-17
is a key mediator linking Th17 cells, cardiac fibroblasts
and
cardiomyocytes that contributes to pathological
remodeling.
IL-10 is a general anti-inflammatory cytokine that is
also induced after cardiac reperfusion injury or heart
failure in a canine model [29] and in humans [108].
Elevated IL-10 is considered to antagonize the effects of
pro-inflammatory cytokines like TNFa [51]. A studydemonstrated
that IL-10 reduced the oxidative stress and
TNFa-induced apoptosis of cardiomyocytes in vitro, andthe
administration of IL-10 after myocardial infarction led
to a reduction of the inflammatory cell invasion and
inflammatory cytokine production and resulted in an
ameliorated infarct area and cardiac remodeling [23].
These results suggest that IL-10 has important roles in the
Page 6 of 15 Basic Res Cardiol (2013) 108:357
123
-
adaptive response during myocardial infarction and heart
failure by affecting both cardiomyocytes and cardiac
fibroblasts.
TNFa
Tumor necrosis factor is a cytokine involved in inflam-
mation that is recognized by its receptors, TNF receptor
type I (TNF-R1) and TNF-R2 [53]. The serum level of
TNFa is elevated in heart failure patients in a
mannercorresponding to the severity of the heart failure [60].
TNFa provokes various effects on TNF-R expressing tis-sues,
including the myocardium [98], through the MAPK
and/or NF-jB pathways. Pathological conditions likehemodynamic
pressure overloading or myocardial infarc-
tion induce TNFa production in both cardiomyocytes
andnon-cardiomyocytes [18, 43, 49]. TNFa induced the pro-liferation
of cardiac fibroblasts and collagen deposition,
increasing the matrix metalloproteinase activity and
inflammatory cytokine production from cardiac fibroblasts,
and also induced the apoptosis of cardiomyocytes and
resulted in cardiac dysfunction and heart failure [91]. As
expected based on these findings, Tnf knockout mice
showed a reduction of cardiac death, infarct size, myo-
cardial apoptosis, inflammatory cell infiltration, inflam-
matory cytokine production, MMP activity and deposition
of extracellular matrix after myocardial infarction [91].
Phosphatase and tensin homolog deleted on chromo-
some ten (PTEN) inactivates protein kinase Akt and pro-
motes cell death in the heart [75]. PTEN is also induced in
the heart following myocardial infarction, while PTEN
heterozygous knockout mice show a reduction of the
number of infiltrated immune cells in the heart and a pre-
served cardiac function following myocardial infarction
[75]. In PTEN heterozygous knockout mice, the production
of TNFa and MMP-2 is decreased and the production ofIL-10 is
increased in the heart following myocardial
infarction [75]. In addition, inhibition of IL-10 receptors
increases TNFa and MMP-2 production following myo-cardial
infarction [75]. PTEN is also important in remote
ischemic preconditioning (RIPC) [13]. PTEN is inactivated
in limb muscles following lower limb RIPC. The inacti-
vation of PTEN promotes STAT3 phosphorylation and
induces IL-10 production in limb muscles. The IL-10
released from ischemic skeletal muscles activates protec-
tive signaling pathways in the heart [13]. These results
suggest that PTEN is critically involved in the post-myo-
cardial infarction remodeling induced by TNFa via theAkt/IL-10
signaling pathway.
TNFa directly impairs the contractility of cardiomyo-cytes
through sphingosine, a metabolite stimulated by
TNFa binding, by decreasing the intracellular calciumrelease and
inotropic activity [32, 96], inhibiting the
cardiac L-type calcium channel current and contractile
calcium transients [55], reducing the SERCA2A expression
and activity [48] and reducing the b-adrenergic respon-siveness
[37]. In addition, TNFa can directly induce car-diomyocyte
hypertrophy [110] and apoptosis [56]. These
findings indicate that TNFa might be a key to the devel-opment
of heart failure and could be a therapeutic target for
heart failure. Indeed, several preclinical studies showed
promising data that indicated favorable results for a
TNFablocking strategy against heart failure. In an animal model
of myocardial infarction, TNFa also had ambivalentfunctions
[88]. Indeed, clinical trials of anti-TNFa therapyusing the soluble
TNFa selective antagonist, etanercept, forNew York Heart
Association class II to IV chronic heart
failure patients (ejection fraction B 30 %) were terminated
prematurely due to a lack of benefit. A subanalysis of these
studies concluded that the outcome of patients after the
administration of etanercept was worsened compared to
patients who did not receive the drug [66]. These results
implied that the TNFa signaling in cardiomyocytes
andnon-cardiomyocytes in patients with heart failure is more
complex than was previously thought. Moreover, the
intervention targeting this single molecule associated with
inflammation and heart failure did not bring about favor-
able effects, thus suggesting that chronic inflammation
after heart stress may actually be a favorable adaptive
response, and that excessive blockade of the inflammatory
responses during heart failure might lead to decompensa-
tion. More cell type-specific analyses of this signaling
pathway under different conditions will be required.
Transforming growth factor-b
Transforming growth factor b (TGF-b) is expressed incardiac
fibroblasts, cardiomyocytes and vascular cells, and
is induced in the myocardium by myocardial infarction and
heart failure [19, 21]. Classical TGF-b signaling occurs
viabinding to the TGF-b type 2 receptor and activation of theTGF-b
type I receptor. Thereafter, both a Smad-dependentpathway and
non-canonical pathway (Smad-independent)
are activated. In the non-canonical pathway, PDE1A-
mediated cardiac fibroblast activation and cardiac fibrosis
in response to TGFb have recently been reported [71]. Inthis
report, PDE1A has a pivotal function in the develop-
ment of fibrosis induced by both TGFb and angiotensin II[71].
Blockade of the classical TGF-b signaling usingsystemic Smad3
knockout in mice led to their development
of severe hypertrophy and less fibrosis after left
ventricular
pressure overload [24]. On the other hand, cardiomyocyte-
specific forced non-canonical TGF-b activation by
over-expression of TGF-b activated kinase 1 (TAK1) alsoinduced
cardiac hypertrophy and heart failure in mice
[117]. A left ventricular pressure overload mouse model
Basic Res Cardiol (2013) 108:357 Page 7 of 15
123
-
treated with a TGF-b signal neutralizing antibody resultedin
suppression of the classical pathway (Smad) activation
in the interstitium (non-cardiomyocytes), but not in
cardiomyocytes, and the non-canonical activation (TAK1
activation) was also not affected. Although the cardiac
fibrosis was markedly suppressed, the cardiac dysfunction
was not ameliorated in this mouse model [54]. These
results based on systemic knockout mice and systemic
protein blockade methods have limitations for analyzing
the mechanism(s) underlying complex cellcell interac-
tions, because the same gene may work differentially in
different kinds of cells. A cell type-specific analysis of
TGF-b signaling will be necessary to better understand therole
of the molecule in heart failure.
In response to this need, cardiomyocyte-specific TGF-breceptor
knockout mice were recently reported [54]. These
mice showed reduced cardiac hypertrophy and cardiac
fibrosis as a result of the inhibited cardiomyocyte and
interstitial Smad and TAK1 activation [54] (Fig. 3). Inter-
estingly, the non-Smad pathways in cardiomyocytes,
including the Ras-MEK, Rho GTP-ase, phosphoinositide-3-
kinase and TAK1 pathways, might be the predominant
pathways leading to cardiac hypertrophy and cardiac dys-
function, because cardiomyocyte-specific Smad4 knockout
mice exhibit hypertrophy and heart failure [105] and Smad3
knockout worsens the hypertrophic response to pressure
overload [24]. Among the non-Smad pathways, TAK1 can
phosphorylate P38-MAPK, which promotes cardiac dys-
function [62]. In cardiomyocytes, connective tissue growth
factor and bone morphogenetic protein 7 are key paracrine
factors connecting these cells to cardiac fibroblasts in
response to TGF-b signaling [54]. Connecting tissue growthfactor
is thought to promote myofibroblast activation and to
affect cardiomyocyte dysfunction, in addition to Smad
signaling in the development of cardiac fibrosis, hypertro-
phy and myocarditis [36, 54, 68, 111]. Bone morphogenetic
protein 7 was also shown to suppress TGF-b-mediatedcardiac
fibrosis and the epithelial mesenchymal transition
[116]. TGF-b1 stimulation can suppress bone morphoge-netic
protein 7 by a TAK1-dependent pathway [54]. The
non-Smad pathway in cardiomyocytes is becoming gradu-
ally recognized to have a major role in TGF-b
signaling,especially in the communication between
cardiomyocytes
and cardiac fibroblasts, in terms of heart failure.
Insulin-like growth factor
Insulin-like growth factor-1 (IGF1) is expressed in cardiac
fibroblasts and promotes cardiac cardiomyocyte hypertro-
phy through phosphoinositide 3-kinase signaling [69].
IGF1 is a downstream target of KLF5 that is activated by
KLF5 after pressure overload [94] (Fig. 2). The adminis-
tration of an IGF-1 inhibitor to wild-type mice with
pressure overload also led to the development of severe
heart failure [94]. These results clearly show that KLF5-
IGF-1 signaling in cardiac fibroblasts, but not in cardio-
myocytes, is required for adaptive responses, like cardiac
hypertrophy and cardiac fibrosis, during pressure overload.
Natriuretic peptide
The serum levels of atrial natriuretic peptide (ANP) and
brain natriuretic peptide (BNP) are clinically used as
diagnostic markers which reflect volume overload in heart
failure and the therapeutic index of heart failure
treatment.
Mice that were genetically deficient in the common
receptor for these two peptides, guanylyl cyclase-A,
showed marked cardiac hypertrophy and fibrosis, suggest-
ing that ANP and BNP have protective effects against
cardiac hypertrophy and fibrosis [52]. ANP and BNP are
produced by cardiomyocytes, and BNP directly affects and
protects cardiomyocytes following myocardial infarction
by opening ATP-sensitive potassium (KATP) channel [17].
BNP also directly affects cardiac fibroblasts and limits
TGF-b-mediated gene expression associated with cardiacfibrosis
and cardiac fibroblast proliferation [50]. In addi-
tion, ANP reduces the endothelin-1 expression, which can
exert proliferative effects on cardiac fibroblasts in vitro
[33]. These data suggest that these two peptides from
cardiomyocytes antagonize the fibrogenic activity of car-
diac fibroblasts in a paracrine fashion.
Immune cells and cardiomyocytes/cardiac fibroblasts
interactions
Several kinds of immune cells proliferate or infiltrate into
the heart after cardiac stress, and are considered to
promote
cardiac remodeling. Monocytes (Ly-6Chigh at acute phase
and Ly-6Clow at late phage) and macrophages are one of
the major immune cell types that accumulate in the heart
during stress, such as myocardial infarction or heart
failure.
The origin of cardiac macrophages is believed to be from
bone marrow-derived monocytes, which differentiate into
macrophages in the heart, or may be the result of the
proliferation of resident macrophages within the heart.
Recently, splenic monocytes were reported to function as a
reservoir of Ly-6C high-inflammatory monocytes that
participate in the repair of heart disease in the acute
phase
[92]. In addition, this rapid deployment of inflammatory
monocytes from the spleen depends on angiotensin sig-
naling [92].
Monocyte chemotactic protein-1 (MCP-1) is a major
chemokine that recruits inflammatory monocytes into var-
ious tissues. In a pressure overload model, MCP-1 was
upregulated in the early stage of heart remodeling. Chronic
Page 8 of 15 Basic Res Cardiol (2013) 108:357
123
-
treatment using a neutralizing antibody against MCP-1
inhibited the inflammatory monocyte/macrophage infiltra-
tion and cardiac fibroblast proliferation. This treatment
attenuated cardiac fibrosis through the inhibition of
TGF-binduction, and ameliorated the left ventricular diastolic
dysfunction, but not the cardiomyocyte hypertrophy [57].
These results suggest that MCP-1 mediates the accumula-
tion of monocyte/macrophage lineage cells into the heart,
and that this promotes myocardial fibrosis and diastolic
dysfunction in the pressure overloaded heart through a
TGF-b-mediated process.The reninangiotensinaldosterone system is
associated
with cardiac remodeling, and a competitive antagonist of
aldosterone (spironolactone) or a mineral corticoid-specific
inhibitor (eplerenone) has been indicated for reducing the
risk of cardiac death in patients with heart failure and
myocardial infarction. Myeloid cell-specific mineralocor-
ticoid receptor knockout mice showed a lack of classical
activation of infiltrated macrophages into the heart after
angiotensin II infusion, and the infiltrated macrophages
exhibited alternative activation profiles [101]. These mice
exhibited reduced cardiac hypertrophy and fibrosis, sug-
gesting that the mineralocorticoid receptor in cardiac
macrophages is critical for cardiac macrophage polarity
(pro-classical activation), cardiac hypertrophy and cardiac
fibrosis [101].
On the other hand, monocyte/macrophage depletion by
clodronate liposome administration, which can damage or
deplete monocytes and macrophages via their phagocytic
activity, resulted in exacerbated left ventricular ejection
function in a hypertensive heart disease model [115].
Monocyte/macrophage lineage cell depletion in hyperten-
sive hearts led to the abundant infiltration of inflammatory
cells within areas of cardiomyocyte loss, predominantly
CD4? T lymphocytes [115]. These results imply that
monocytes/macrophages have protective effects on adap-
tive stress through inhibiting T cell infiltration into the
heart. Monocytes/macrophages have diverse and bivalent
TGF-TGF- type I receptor
cardiomyocyte cardiac fibroblast
Smad dependentpathway
non Smad pathway
hypertrophy contraction
extracellularmatrix
production
myofibroblast activation
dominant
Smad3, Smad4
suppressor
no effect
TAK1Ras-MEKRho GTPasePI3K
P38MAPK
CTGF
BMP7
TGF- type I receptor
TGF-
fibrosis
suppress
Fig. 3 TGF-b signaling in cardiomyocytes and cardiac
fibroblasts.TGF-b signaling is associated with hypertrophy of
cardiomyocyte andcardiac fibrosis revealed by recent works are
shown. In cardiomyo-
cytes, TGF-b induces hypertrophy through TGF-b type I
receptor.TGF-b type I receptor transduces its signals after cardiac
stressesmainly through non-Smad pathways. For example, TGF-beta
acti-
vated kinase 1 (TAK1) induces hypertrophy of cardiomyocytes
and
reduces cardiac contractility via P38MAPK. In addition, TAK1
activation inhibits bone morphogenetic protein 7 (BMP7)
production
that can inhibit myofibroblast activation. Smad 4 might inhibit
cardiac
hypertrophy under TGF-b signaling. In cardiac fibroblasts,
TGF-bsignaling provokes myofibroblast activation through TGF-b type
Ireceptor and promotes cardiac fibrosis. TAK1 activation in
cardio-
myocytes also produced connective tissue growth factor
(CTGF).
CTGF reduces contractility of cardiomyocytes and inhibits
myofi-
broblast activation. TGF-b transforming growth factor beta,
TAK1TGF-beta activated kinase 1, MEK MAPK/ERK kinase, Rho
GTPase
Rho guanosine triphosphate, PI3K phosphoinositide-3-kinase,
BMP7
bone morphogenetic protein 7, CTGF connective tissue growth
factor
Basic Res Cardiol (2013) 108:357 Page 9 of 15
123
-
effects on tissue remodeling after heart stress. More sub-
type analyses of monocytes/macrophages should be per-
formed in the future to better understand their roles. The
balances of pro-inflammatory monocytes/macrophages
versus alternatively activated monocytes/macrophages in
the heart at every time point after heart stress might have
complex effects on cardiomyocyte and cardiac fibroblast
phenotypic modulation and activation.
Mast cells are also key effector cells during allergic
reactions, and show immune responses resulting from the
degranulation of synthesized bioactive agents, like
growth factors, cytokines and other molecules. Mast cells
are also increased during cardiac hypertrophy and heart
failure in humans [90]. These cells secrete platelet-
derived growth factor A, TGF-b, TNF-a and histamine,and affect
the cardiac function. Mast cell stabilizing
drugs ameliorated heart failure via reduced cardiac
remodeling in a volume overload model [10]. In addi-
tion, after pressure overload in a mouse model, the
infiltrated mast cells induced platelet-derived growth
factor A chain synthesis and promoted the proliferation
and collagen synthesis of cardiac fibroblasts. This mast
cellcardiac fibroblast interaction is required for atrial
fibrosis and affects the susceptibility to atrial
fibrillation,
which is the most common type of arrhythmia occurring
in heart failure [61]. These results suggest that cardiac
mast cells have a key role in the regulation of atrial
myocardial remodeling and in the communication
between cardiomyocytes and cardiac fibroblasts. In
addition to platelet-derived growth factor A chain, it has
recently been reported that angiotensin II-induced Rac 1
activation leads to atrial remodeling and atrial
fibrillation
via the CTGF and lysyl oxidase-mediated miR-21
expression [2].
To date, several T cell subsets have been reported.
CD4? T cells are divided into four subtypes, including
helper T cells (Th1, Th2), Th17 cells and regulatory T
cells (Tregs). T cells are also suggested to contribute to
cardiac remodeling via cellcell interactions, as well as
the production of cytokines and growth factors. In gen-
eral, Th1 cells secrete Th1 cytokines like interferon-c,and
promote an anti-fibrogenic response, while Th2
cytokines, like IL-4,-5 and -13, promote fibrosis [67]. In
the early stage of inflammation, Th1 cytokines are
secreted to eradicate intracellular pathogens. In the late
phase of inflammation, Th2 cytokines enhance chronic
inflammation, leading to the elimination of extracellular
organisms and contributing to the development of
chronic inflammatory diseases. The administration of
N(G)-nitro-L-arginine methyl ester (L-NAME: NO syn-
thesis inhibitor) to mice can induce hypertension. Dif-
ferent strains of mice, including C57BL/6 SCID mice,
which lack T and B lymphocytes, C57BL/6 wild-type
mice and BALB/c mice subjected to L-NAME-induced
hypertension showed different Th1/Th2 polarity, i.e. null,
Th1 polarity and Th2 polarity, respectively, whereas all
of the strains showed the same degree of hypertension.
The hypertension-induced cardiac fibrosis is decreased in
SCID mice, unchanged in C57BL/6 wild-type mice and
significantly increased in BALB/c mice [112]. Another
hypertension model (an angiotensin II continuous infu-
sion model) showed severe left ventricular dilatation,
thinning and fibrosis in BALB/c mice, but not in C57BL/
6 mice, whereas the same degree of hypertrophied
cardiomyocytes was observed in both BALB/c and
C57BL/6 mice [78]. These results suggest that Th1 cells
and cytokines might initiate fibroblastic activity, and that
Th2 cells and cytokines might contribute to the late or
chronic stage of fibrosis.
IL-17- and IL-22-producing CD4? cells, called Th17
cells, play an important role in promoting inflammation
during tissue remodeling. IL-17 can induce or functionally
augment inflammatory cytokines, including IL-6, IL-1band TNFa,
and can promote extracellular matrix remod-eling by producing
matrix metalloproteinases or inhibiting
repair components, like proteoglycans [3]. IL-17 is a
pleiotropic cytokine that can modulate other cytokine
functions in multiple ways. Among them, the post-tran-
scriptional modification of IL-17 can stabilize the mRNA
of many cytokines through AU-rich elements in the 30UTR,a common
feature of inflammatory cytokine genes [80]. IL-
17 blockade using an anti-IL-17 antibody resulted in
decreased cardiac fibrosis in an isoproterenol-infusion rat
heart failure model [26]. In this model, the MMP-1 and
receptor activator of nuclear factor-rB ligand (RANKL)expression
and collagen synthesis were inhibited, and the
levels of tissue inhibitor of metalloproteinases and osteo-
protegerin (OPG) were increased in cardiac fibroblasts
[26]. These results indicate that Th17 cells control cardiac
fibrosis by the IL-17-RANKL/OPG system and MMP
production in cardiac fibroblasts, or via the stabilization
of
pro-inflammatory cytokines mRNA in various cardiac
cells and immune cells.
Tregs are an anti-inflammatory lineage of CD4? T
lymphocytes that express FoxP3 and produce anti-
inflammatory cytokines/growth factors, such as IL-10
and/or TGF-b. In a heart disease model, CD4?CD25?
Tregs were increased by angiotensin II infusion and
myocardial infarction, and adoptive transfer of Tregs led
to a reduction of cardiac hypertrophy, anti-inflammatory
and anti-fibrotic effects and resulted in a preserved car-
diac function via IL-10 production and a direct cellcell
interaction [58, 95]. These results suggested that there is
a close relationship among Tregs, cardiomyocytes and
cardiac fibroblasts, and confirms their importance in
cardiac remodeling.
Page 10 of 15 Basic Res Cardiol (2013) 108:357
123
-
Natural killer T cells (NKT cells)
NKT cells have been shown to be involved in inflammation
and tissue remodeling. The infiltration of NKT cells was
increased in the non-infarct area of the left ventricle
after
myocardial infarction in mice [89]. Moreover, the admin-
istration of a NKT cell activator, a-galactosylceramide(aGC) in
a mouse myocardial infarction model, led toenhanced infiltration of
NKT cells in the non-infarcted
area. The left ventricular dilatation and mortality due to
heart failure were significantly attenuated in the
aGCadministration group [89]. It was suggested that these
effects are dependent on NKT cells, because NKT deficient
mice did not show these effects, and because IL-10 is the
most potent effector cytokine for this process [89]. NKT
cells play a protective role after myocardial infarction and
heart failure via IL-10 production.
Dendritic cells
Dendritic cells infiltrate in the infarct heart. Depletion
of
bone marrow-derived dendritic cell using CD11c-diphteria
toxin receptor transgenic mice showed deteriorated left
ventricular function and remodeling after myocardial
infarction model. The dendritic cells ablation group
exhibited long-lasting inflammatory cytokines like IL-1b,IL-18
and TNFa. In addition, anti-inflammatory cellsincluding Ly-6Clow
monocytes and alternatively activated
macrophages were significantly infiltrated in the hearts of
dendritic cell depleted group [6]. These results suggest
that
cardiac dendritic cells have a potent immunoprotective
function after myocardial infarction.
Concluding remarks
Recent heart failure research has been focused not only on
cardiomyocytes, but also on non-myocytes, which have
been recognized as quiescent and structural cells under
normal conditions. Unveiling the pivotal functions of non-
myocytes has demonstrated that they have dynamic and
diverse functions during tissue remodeling as an adaptive
response and during the development of heart failure. In
this review, we summarized the recent reports of the cell
cell interactions in the heart. However, there is room for
further research into the cellcell interactions under both
physiological and pathological conditions in the heart.
Importantly, immune cells are mainly derived from non-
heart organs, like the bone marrow, spleen, thymus and
intestinal organs. Moreover, the recruitment of these
immune cells is at least partly controlled by the brain via
neurotransmitters or humoral proteins. In the next decade,
research should focus on further elucidating the mecha-
nisms of heart failure in terms of cellcell interactions and
organorgan communication.
Acknowledgments This study was supported by the FundingProgram
for World-Leading Innovative R&D on Science and Tech-
nology (FIRST Program) (to R.N.), Grants-in-Aid for
Scientific
Research (S) and (B), and Grants-in-Aid for Young Scientists
(B) from JSPS (23390203, 22229006, 23790835) (to R.N., K.F.);
a
grant for Translational Systems Biology and Medicine Initiative
(to
R.N.) from JST.
Conflict of interest On behalf of all authors, the
correspondingauthor states that there is no conflict of
interest.
References
1. Accornero F, van Berlo JH, Benard MJ, Lorenz JN, Carmeliet
P,
Molkentin JD (2011) Placental growth factor regulates
cardiac
adaptation and hypertrophy through a paracrine mechanism.
Circ Res 109:272280. doi:10.1161/CIRCRESAHA.111.240820
2. Adam O, Lohfelm B, Thum T, Gupta SK, Puhl SL, Schafers
HJ,
Bohm M, Laufs U (2012) Role of miR-21 in the pathogenesis of
atrial fibrosis. Basic Res Cardiol 107:278.
doi:10.1007/s00395-
012-0278-0
3. Afzali B, Lombardi G, Lechler RI, Lord GM (2007) The role
of
T helper 17 (Th17) and regulatory T cells (Treg) in human
organ
transplantation and autoimmune disease. Clin Exp Immunol
148:3246. doi:10.1111/j.1365-2249.2007.03356.x
4. Agah R, Frenkel PA, French BA, Michael LH, Overbeek PA,
Schneider MD (1997) Gene recombination in postmitotic cells.
Targeted expression of Cre recombinase provokes cardiac-
restricted, site-specific rearrangement in adult ventricular
mus-
cle in vivo. J Clin Invest 100:169179. doi:10.1172/jci119509
5. Aggarwal BB (2003) Signalling pathways of the TNF super-
family: a double-edged sword. Nat Rev Immunol 3:745756.
doi:10.1038/nri1184
6. Anzai A, Anzai T, Nagai S, Maekawa Y, Naito K, Kaneko H,
Sugano Y, Takahashi T, Abe H, Mochizuki S, Sano M, Yos-
hikawa T, Okada Y, Koyasu S, Ogawa S, Fukuda K (2012)
Regulatory role of dendritic cells in postinfarction healing
and
left ventricular remodeling. Circulation 125:12341245.
doi:10.1161/circulationaha.111.052126
7. Avalos AM, Apablaza FA, Quiroz M, Toledo V, Pena JP, Mi-
chea L, Irarrazabal CE, Carrion FA, Figueroa FE (2012)
IL-17A
levels increase in the infarcted region of the left ventricle in
a rat
model of myocardial infarction. Biol Res 45:193200.
doi:10.1590/S0716-97602012000200012
8. Banerjee I, Fuseler JW, Price RL, Borg TK, Baudino TA
(2007)
Determination of cell types and numbers during cardiac
devel-
opment in the neonatal and adult rat and mouse. Am J Physiol
Heart Circ Physiol 293:H1883H1891. doi:10.1152/ajpheart.
00514.2007
9. Bowers SL, Borg TK, Baudino TA (2010) The dynamics of
fibroblast-myocyte-capillary interactions in the heart. Ann
NY
Acad Sci 1188:143152. doi:10.1111/j.1749-6632.2009.05094.x
10. Brower GL, Janicki JS (2005) Pharmacologic inhibition of
mast
cell degranulation prevents left ventricular remodeling
induced
by chronic volume overload in rats. J Card Fail 11:548556.
doi:10.1016/j.cardfail.2005.05.005
11. Buckley CD, Pilling D, Lord JM, Akbar AN, Scheel-Toellner
D,
Salmon M (2001) Fibroblasts regulate the switch from acute
Basic Res Cardiol (2013) 108:357 Page 11 of 15
123
-
resolving to chronic persistent inflammation. Trends Immunol
22:199204. doi:10.1016/S1471-4906(01)01863-4
12. Bujak M, Dobaczewski M, Chatila K, Mendoza LH, Li N,
Reddy A, Frangogiannis NG (2008) Interleukin-1 receptor type
I
signaling critically regulates infarct healing and cardiac
remodeling. Am J Pathol 173:5767. doi:10.2353/ajpath.
2008.070974
13. Cai ZP, Parajuli N, Zheng X, Becker L (2012) Remote
ischemic
preconditioning confers late protection against myocardial
ischemiareperfusion injury in mice by upregulating
interleukin-
10. Basic Res Cardiol 107:277. doi:10.1007/s00395-012-0277-1
14. Chandrasekar B, Mitchell DH, Colston JT, Freeman GL
(1999)
Regulation of CCAAT/enhancer binding protein, interleukin-6,
interleukin-6 receptor, and gp130 expression during
myocardial
ischemia/reperfusion. Circulation 99:427433. doi:10.1161/
01.CIR.99.3.427
15. Colombo F, Gosselin H, El-Helou V, Calderone A (2003)
Beta-
adrenergic receptor-mediated DNA synthesis in neonatal rat
cardiac fibroblasts proceeds via a phosphatidylinositol
3-kinase
dependent pathway refractory to the antiproliferative action
of
cyclic AMP. J Cell Physiol 195:322330. doi:10.1002/jcp.10251
16. Cortez DM, Feldman MD, Mummidi S, Valente AJ, Steffensen
B, Vincenti M, Barnes JL, Chandrasekar B (2007) IL-17 stim-
ulates MMP-1 expression in primary human cardiac fibroblasts
via p38 MAPK- and ERK1/2-dependent C/EBP-beta, NF-kap-
paB, and AP-1 activation. Am J Physiol Heart Circ Physiol
293:H3356H3365. doi:10.1152/ajpheart.00928.2007
17. DSouza SP, Yellon DM, Martin C, Schulz R, Heusch G,
Onody
A, Ferdinandy P, Baxter GF (2003) B-type natriuretic peptide
limits infarct size in rat isolated hearts via KATP channel
opening. Am J Physiol Heart Circ Physiol 284:H1592H1600.
doi:10.1152/ajpheart.00902.2002
18. Dorge H, Schulz R, Belosjorow S, Post H, van de Sand A,
Konietzka I, Frede S, Hartung T, Vinten-Johansen J, Youker
KA, Entman ML, Erbel R, Heusch G (2002) Coronary micro-
embolization: the role of TNF-a in contractile dysfunction.J Mol
Cell Cardiol 34:5162. doi:10.1006/jmcc.2001.1489
19. Dean RG, Balding LC, Candido R, Burns WC, Cao Z, Twigg
SM, Burrell LM (2005) Connective tissue growth factor and
cardiac fibrosis after myocardial infarction. J Histochem
Cyto-
chem 53:12451256. doi:10.1369/jhc.4A6560.2005
20. Del Re DP, Matsuda T, Zhai P, Gao S, Clark GJ, Van Der
Weyden L, Sadoshima J (2010) Proapoptotic Rassf1A/Mst1
signaling in cardiac fibroblasts is protective against
pressure
overload in mice. J Clin Invest 120:35553567. doi:10.1172/
JCI43569
21. Deten A, Holzl A, Leicht M, Barth W, Zimmer HG (2001)
Changes in extracellular matrix and in transforming growth
factor beta isoforms after coronary artery ligation in rats. J
Mol
Cell Cardiol 33:11911207. doi:10.1006/jmcc.2001.1383
22. Deten A, Volz HC, Briest W, Zimmer HG (2002) Cardiac
cytokine expression is upregulated in the acute phase after
myocardial infarction. Experimental studies in rats.
Cardiovasc
Res 55:329340. doi:10.1016/S0008-6363(02)00413-3
23. Dhingra S, Sharma AK, Arora RC, Slezak J, Singal PK
(2009)
IL-10 attenuates TNF-alpha-induced NF kappaB pathway acti-
vation and cardiomyocyte apoptosis. Cardiovasc Res 82:5966.
doi:10.1093/cvr/cvp040
24. Divakaran V, Adrogue J, Ishiyama M, Entman ML, Haudek S,
Sivasubramanian N, Mann DL (2009) Adaptive and maladaptive
effects of SMAD3 signaling in the adult heart after hemody-
namic pressure overloading. Circ Heart Fail 2:633642.
doi:10.1161/CIRCHEARTFAILURE.108.823070
25. Erlich JH, Boyle EM, Labriola J, Kovacich JC, Santucci
RA,
Fearns C, Morgan EN, Yun W, Luther T, Kojikawa O, Martin
TR, Pohlman TH, Verrier ED, Mackman N (2000) Inhibition of
the tissue factor-thrombin pathway limits infarct size after
myocardial ischemiareperfusion injury by reducing inflamma-
tion. Am J Pathol 157:18491862. doi:10.1016/S0002-9440
(10)64824-9
26. Feng W, Li W, Liu W, Wang F, Li Y, Yan W (2009) IL-17
induces myocardial fibrosis and enhances RANKL/OPG and
MMP/TIMP signaling in isoproterenol-induced heart failure.
Exp Mol Pathol 87:212218. doi:10.1016/j.yexmp.2009.06.001
27. Feng Y, Hans C, McIlwain E, Varner KJ, Lazartigues E
(2012)
Angiotensin-converting enzyme 2 over-expression in the
central
nervous system reduces angiotensin-II-mediated cardiac
hyper-
trophy. PLoS One 7:e48910. doi:10.1371/journal.pone.0048910
28. Fischer P, Hilfiker-Kleiner D (2007) Survival pathways
in
hypertrophy and heart failure: the gp130STAT axis. Basic Res
Cardiol 102:393411. doi:10.1007/s00395-007-0674-z
29. Frangogiannis NG, Mendoza LH, Lindsey ML, Ballantyne CM,
Michael LH, Smith CW, Entman ML (2000) IL-10 is induced in
the reperfused myocardium and may modulate the reaction to
injury. J Immunol 165:27982808
30. Fredj S, Bescond J, Louault C, Delwail A, Lecron JC, Potreau
D
(2005) Role of interleukin-6 in cardiomyocyte/cardiac
fibroblast
interactions during myocyte hypertrophy and fibroblast
prolif-
eration. J Cell Physiol 204:428436. doi:10.1002/jcp.20307
31. Fredj S, Bescond J, Louault C, Potreau D (2005)
Interactions
between cardiac cells enhance cardiomyocyte hypertrophy and
increase fibroblast proliferation. J Cell Physiol
202:891899.
doi:10.1002/Jcp.20197
32. Friedrichs GS, Swillo RE, Jow B, Bridal T, Numann R,
Warner
LM, Killar LM, Sidek K (2002) Sphingosine modulates myocyte
electrophysiology, induces negative inotropy, and decreases
survival after myocardial ischemia. J Cardiovasc Pharmacol
39:1828. doi:10.1097/00005344-200201000-00003
33. Glenn DJ, Rahmutula D, Nishimoto M, Liang F, Gardner DG
(2009) Atrial natriuretic peptide suppresses endothelin gene
expression and proliferation in cardiac fibroblasts through
a
GATA4-dependent mechanism. Cardiovasc Res 84:209217.
doi:10.1093/cvr/cvp208
34. Golias C, Tsoutsi E, Matziridis A, Makridis P, Batistatou
A,
Charalabopoulos K (2007) Review. Leukocyte and endothelial
cell adhesion molecules in inflammation focusing on inflam-
matory heart disease. In Vivo 21:757769
35. Gray MO, Long CS, Kalinyak JE, Li HT, Karliner JS (1998)
Angiotensin II stimulates cardiac myocyte hypertrophy via
paracrine release of TGF-beta 1 and endothelin-1 from fibro-
blasts. Cardiovasc Res 40:352363. doi:10.1161/01.CIR.101.
20.2338
36. Gruhle S, Sauter M, Szalay G, Ettischer N, Kandolf R,
Klingel
K (2012) The prostacyclin agonist iloprost aggravates
fibrosis
and enhances viral replication in enteroviral myocarditis by
modulation of ERK signaling and increase of iNOS expression.
Basic Res Cardiol 107:287. doi:10.1007/s00395-012-0287-z
37. Gulick T, Chung MK, Pieper SJ, Lange LG, Schreiner GF
(1989) Interleukin 1 and tumor necrosis factor inhibit
cardiac
myocyte beta-adrenergic responsiveness. Proc Natl Acad Sci
USA 86:67536757. doi:10.1073/pnas.86.17.6753
38. Hao J, Wang B, Jones SC, Jassal DS, Dixon IMC (2000)
Interaction between angiotensin II and Smad proteins in
fibro-
blasts in failing heart and in vitro. Am J Physiol Heart
Circ
Physiol 279:H3020H3030
39. Heine HL, Leong HS, Rossi FM, McManus BM, Podor TJ
(2005) Strategies of conditional gene expression in
myocardium:
an overview. Methods Mol Med 112:109154. doi:10.1007/978-
1-59259-879-3_8
40. Hilfiker-Kleiner D, Kaminski K, Podewski E, Bonda T,
Schaefer
A, Sliwa K, Forster O, Quint A, Landmesser U, Doerries C,
Luchtefeld M, Poli V, Schneider MD, Balligand JL, Desjardins
Page 12 of 15 Basic Res Cardiol (2013) 108:357
123
-
F, Ansari A, Struman I, Nguyen NQ, Zschemisch NH, Klein G,
Heusch G, Schulz R, Hilfiker A, Drexler H (2007) A cathepsin
D-cleaved 16 kDa form of prolactin mediates postpartum car-
diomyopathy. Cell 128:589600. doi:10.1016/j.cell.2006.12.036
41. Hu Y, Zhang H, Lu Y, Bai H, Xu Y, Zhu X, Zhou R, Ben J,
Xu
Y, Chen Q (2011) Class A scavenger receptor attenuates myo-
cardial infarction-induced cardiomyocyte necrosis through
sup-
pressing M1 macrophage subset polarization. Basic Res
Cardiol
106:13111328. doi:10.1007/s00395-011-0204-x
42. Ieda M, Tsuchihashi T, Ivey KN, Ross RS, Hong TT, Shaw
RM,
Srivastava D (2009) Cardiac fibroblasts regulate myocardial
proliferation through beta1 integrin signaling. Dev Cell
16:233244. doi:10.1016/j.devcel.2008.12.007
43. Jacobs M, Staufenberger S, Gergs U, Meuter K, Brandstatter
K,
Hafner M, Ertl G, Schorb W (1999) Tumor necrosis
factor-alpha
at acute myocardial infarction in rats and effects on
cardiac
fibroblasts. J Mol Cell Cardiol 31:19491959. doi:10.1006/
jmcc.1999.1007
44. Jaffre F, Bonnin P, Callebert J, Debbabi H, Setola V, Doly
S,
Monassier L, Mettauer B, Blaxall BC, Launay JM, Maroteaux L
(2009) Serotonin and angiotensin receptors in cardiac
fibroblasts
coregulate adrenergic-dependent cardiac hypertrophy. Circ
Res
104:113123. doi:10.1161/CIRCRESAHA.108.180976
45. Joseph NM, Mosher JT, Buchstaller J, Snider P, McKeever
PE,
Lim M, Conway SJ, Parada LF, Zhu Y, Morrison SJ (2008) The
loss of Nf1 transiently promotes self-renewal but not
tumori-
genesis by neural crest stem cells. Cancer Cell 13:129140.
doi:10.1016/j.ccr.2008.01.003
46. Kakkar R, Lee RT (2010) Intramyocardial fibroblast
myocyte
communication. Circ Res 106:4757. doi:10.1161/circresaha.
109.207456
47. Kaneko K, Kanda T, Yokoyama T, Nakazato Y, Iwasaki T,
Kobayashi I, Nagai R (1997) Expression of interleukin-6 in
the
ventricles and coronary arteries of patients with myocardial
infarction. Res Commun Mol Pathol Pharmacol 97:312
48. Kao YH, Chen YC, Cheng CC, Lee TI, Chen YJ, Chen SA
(2010) Tumor necrosis factor-alpha decreases sarcoplasmic
reticulum Ca2?-ATPase expressions via the promoter methyla-
tion in cardiomyocytes. Crit Care Med 38:217222.
doi:10.1097/CCM.0b013e3181b4a854
49. Kapadia SR, Oral H, Lee J, Nakano M, Taffet GE, Mann DL
(1997) Hemodynamic regulation of tumor necrosis factor-alpha
gene and protein expression in adult feline myocardium. Circ
Res 81:187195. doi:10.1161/01.RES.81.2.187
50. Kapoun AM, Liang F, OYoung G, Damm DL, Quon D, White
RT, Munson K, Lam A, Schreiner GF, Protter AA (2004) B-type
natriuretic peptide exerts broad functional opposition to
trans-
forming growth factor-beta in primary human cardiac fibro-
blasts: fibrosis, myofibroblast conversion, proliferation,
and
inflammation. Circ Res 94:453461. doi:10.1161/01.RES.0000
117070.86556.9F
51. Kaur K, Sharma AK, Singal PK (2006) Significance of
changes
in TNF-alpha and IL-10 levels in the progression of heart
failure
subsequent to myocardial infarction. Am J Physiol Heart Circ
Physiol 291:H106H113. doi:10.1152/ajpheart.01327.2005
52. Kishimoto I, Rossi K, Garbers DL (2001) A genetic model
provides evidence that the receptor for atrial natriuretic
peptide
(guanylyl cyclase-A) inhibits cardiac ventricular myocyte
hyper-
trophy. Proc Natl Acad Sci USA 98:27032706. doi:10.1073/
pnas.051625598
53. Kleinbongard P, Heusch G, Schulz R (2010) TNFalpha in
ath-
erosclerosis, myocardial ischemia/reperfusion and heart
failure.
Pharmacol Ther 127:295314. doi:10.1016/j.pharmthera.
2010.05.002
54. Koitabashi N, Danner T, Zaiman AL, Pinto YM, Rowell J,
Mankowski J, Zhang D, Nakamura T, Takimoto E, Kass DA
(2011) Pivotal role of cardiomyocyte TGF-beta signaling in
the
murine pathological response to sustained pressure overload.
J Clin Invest 121:23012312. doi:10.1172/JCI44824
55. Krown KA, Yasui K, Brooker MJ, Dubin AE, Nguyen C,
Harris
GL, McDonough PM, Glembotski CC, Palade PT, Sabbadini RA
(1995) TNF alpha receptor expression in rat cardiac
myocytes:
TNF alpha inhibition of L-type Ca2? current and Ca2?
transients.
FEBS Lett 376:2430. doi:10.1016/0014-5793(95)01238-5
56. Krown KA, Page MT, Nguyen C, Zechner D, Gutierrez V,
Comstock KL, Glembotski CC, Quintana PJ, Sabbadini RA
(1996) Tumor necrosis factor alpha-induced apoptosis in
cardiac
myocytes. Involvement of the sphingolipid signaling cascade
in
cardiac cell death. J Clin Invest 98:28542865. doi:10.1172/
JCI119114
57. Kuwahara F, Kai H, Tokuda K, Takeya M, Takeshita A,
Egashira
K, Imaizumi T (2004) Hypertensive myocardial fibrosis and
diastolic dysfunction: another model of inflammation? Hyper-
tension 43:739745. doi:10.1161/01.HYP.0000118584.33350.7d
58. Kvakan H, Kleinewietfeld M, Qadri F, Park JK, Fischer R,
Schwarz I, Rahn HP, Plehm R, Wellner M, Elitok S, Gratze P,
Dechend R, Luft FC, Muller DN (2009) Regulatory T cells
ameliorate angiotensin II-induced cardiac damage.
Circulation
119:29042912. doi:10.1161/CIRCULATIONAHA.108.832782
59. LaFramboise WA, Scalise D, Stoodley P, Graner SR,
Guthrie
RD, Magovern JA, Becich MJ (2007) Cardiac fibroblasts
influence cardiomyocyte phenotype in vitro. Am J Physiol
Cell
Physiol 292:C1799C1808. doi:10.1152/ajpcell.00166.2006
60. Levine B, Kalman J, Mayer L, Fillit HM, Packer M (1990)
Elevated circulating levels of tumor necrosis factor in
severe
chronic heart failure. N Engl J Med 323:236241. doi:10.1056/
NEJM199007263230405
61. Liao CH, Akazawa H, Tamagawa M, Ito K, Yasuda N, Kudo Y,
Yamamoto R, Ozasa Y, Fujimoto M, Wang P, Nakauchi H,
Nakaya H, Komuro I (2010) Cardiac mast cells cause atrial
fibrillation through PDGF-A-mediated fibrosis in pressure-
overloaded mouse hearts. J Clin Invest 120:242253.
doi:10.1172/JCI39942
62. Liao P, Georgakopoulos D, Kovacs A, Zheng M, Lerner D,
Pu
H, Saffitz J, Chien K, Xiao RP, Kass DA, Wang Y (2001) The
in vivo role of p38 MAP kinases in cardiac remodeling and
restrictive cardiomyopathy. Proc Natl Acad Sci USA
98:1228312288. doi:10.1073/pnas.211086598
63. Liao YH, Xia N, Zhou SF, Tang TT, Yan XX, Lv BJ, Nie SF,
Wang J, Iwakura Y, Xiao H, Yuan J, Jevallee H, Wei F, Shi
GP,
Cheng X (2012) Interleukin-17A contributes to myocardial
ischemia/reperfusion injury by regulating cardiomyocyte
apop-
tosis and neutrophil infiltration. J Am Coll Cardiol
59:420429.
doi:10.1016/j.jacc.2011.10.863
64. Long CS, Hartogensis WE, Simpson PC (1993)
Beta-adrenergic
stimulation of cardiac non-myocytes augments the growth-pro-
moting activity of non-myocyte conditioned medium. J Mol
Cell
Cardiol 25:915925. doi:10.1006/jmcc.1993.1104
65. Mann DL (2002) Inflammatory mediators and the failing
heart:
past, present, and the foreseeable future. Circ Res
91:988998.
doi:10.1161/01.RES.0000043825.01705.1B
66. Mann DL, McMurray JJ, Packer M, Swedberg K, Borer JS,
Colucci WS, Djian J, Drexler H, Feldman A, Kober L, Krum H,
Liu P, Nieminen M, Tavazzi L, van Veldhuisen DJ, Walden-
strom A, Warren M, Westheim A, Zannad F, Fleming T (2004)
Targeted anticytokine therapy in patients with chronic heart
failure: results of the Randomized Etanercept Worldwide
Evaluation (RENEWAL). Circulation 109:15941602.
doi:10.1161/01.CIR.0000124490.27666.B2
67. Marra F, Aleffi S, Galastri S, Provenzano A (2009)
Mononuclear
cells in liver fibrosis. Semin Immunopathol 31:345358.
doi:10.1007/s00281-009-0169-0
Basic Res Cardiol (2013) 108:357 Page 13 of 15
123
-
68. Matsui Y, Sadoshima J (2004) Rapid upregulation of CTGF
in
cardiac myocytes by hypertrophic stimuli: implication for
car-
diac fibrosis and hypertrophy. J Mol Cell Cardiol 37:477481.
doi:10.1016/j.yjmcc.2004.05.012
69. McMullen JR (2008) Role of insulin-like growth factor 1
and
phosphoinositide 3-kinase in a setting of heart disease. Clin
Exp
Pharmacol Physiol 35:349354. doi:10.1111/j.1440-
1681.2007.04873.x
70. McTiernan CF, Lemster BH, Frye C, Brooks S, Combes A,
Feldman AM (1997) Interleukin-1 beta inhibits phospholamban
gene expression in cultured cardiomyocytes. Circ Res
81:493503. doi:10.1161/01.RES.81.4.493
71. Miller C, Cai Y, Oikawa M, Thomas T, Dostmann W, Zaccolo
M, Fujiwara K, Yan C (2011) Cyclic nucleotide phosphodies-
terase 1A: a key regulator of cardiac fibroblast activation
and
extracellular matrix remodeling in the heart. Basic Res
Cardiol
106:10231039. doi:10.1007/s00395-011-0228-2
72. Mitchell MD, Laird RE, Brown RD, Long CS (2007) IL-1beta
stimulates rat cardiac fibroblast migration via MAP kinase
pathways. Am J Physiol Heart Circ Physiol 292:H1139H1147.
doi:10.1152/ajpheart.00881.2005
73. Murray DR, Prabhu SD, Chandrasekar B (2000) Chronic
beta-
adrenergic stimulation induces myocardial proinflammatory
cytokine expression. Circulation 101:23382341. doi:10.1161/
01.CIR.101.20.2338
74. Novoyatleva T, Schymura Y, Janssen W, Strobl F, Swiercz
JM,
Patra C, Posern G, Wietelmann A, Zheng TS, Schermuly RT,
Engel FB (2013) Deletion of Fn14 receptor protects from
right
heart fibrosis and dysfunction. Basic Res Cardiol 108:325.
doi:10.1007/s00395-012-0325-x
75. Parajuli N, Yuan Y, Zheng X, Bedja D, Cai Z (2012) Phos-
phatase PTEN is critically involved in post-myocardial
infarc-
tion remodeling through the Akt/interleukin-10 signaling
pathway. Basic Res Cardiol 107:248. doi:10.1007/s00395-012-
0248-6
76. Pawlinski R, Tencati M, Hampton CR, Shishido T, Bullard
TA,
Casey LM, Andrade-Gordon P, Kotzsch M, Spring D, Luther T,
Abe J, Pohlman TH, Verrier ED, Blaxall BC, Mackman N
(2007) Protease-activated receptor-1 contributes to cardiac
remodeling and hypertrophy. Circulation 116:22982306.
doi:10.1161/CIRCULATIONAHA.107.692764
77. Pedrotty DM, Klinger RY, Kirkton RD, Bursac N (2009)
Car-
diac fibroblast paracrine factors alter impulse conduction
and
ion channel expression of neonatal rat cardiomyocytes. Car-
diovasc Res 83:688697. doi:10.1093/Cvr/Cvp164
78. Peng H, Yang X-P, Carretero OA, Nakagawa P, DAmbrosio M,
Leung P, Xu J, Peterson EL, Gonzalez GE, Harding P, Rhaleb
N-E (2011) Angiotensin II-induced dilated cardiomyopathy in
Balb/c but not C57BL/6J mice. Exp Physiol 96:756764.
doi:10.1113/expphysiol.2011.057612
79. Podewski EK, Hilfiker-Kleiner D, Hilfiker A, Morawietz
H,
Lichtenberg A, Wollert KC, Drexler H (2003) Alterations in
Janus kinase (JAK)-signal transducers and activators of
tran-
scription (STAT) signaling in patients with end-stage
dilated
cardiomyopathy. Circulation 107:798802. doi:10.1161/
01.CIR.0000057545.82749.FF
80. Qian Y, Liu C, Hartupee J, Altuntas CZ, Gulen MF, Jane-Wit
D,
Xiao J, Lu Y, Giltiay N, Liu J, Kordula T, Zhang QW,
Vallance
B, Swaidani S, Aronica M, Tuohy VK, Hamilton T, Li X (2007)
The adaptor Act1 is required for interleukin 17-dependent
sig-
naling associated with autoimmune and inflammatory disease.
Nat Immunol 8:247256. doi:10.1038/ni1439
81. Rauchhaus M, Doehner W, Francis DP, Davos C, Kemp M,
Liebenthal C, Niebauer J, Hooper J, Volk HD, Coats AJ, Anker
SD (2000) Plasma cytokine parameters and mortality in
patients
with chronic heart failure. Circulation 102:30603067.
doi:10.1161/01.CIR.102.25.3060
82. Sano M, Fukuda K, Kodama H, Pan J, Saito M, Matsuzaki J,
Takahashi T, Makino S, Kato T, Ogawa S (2000) Interleukin-6
family of cytokines mediate angiotensin II-induced cardiac
hypertrophy in rodent cardiomyocytes. J Biol Chem
275:2971729723. doi:10.1074/jbc.M003128200
83. Sano M, Minamino T, Toko H, Miyauchi H, Orimo M, Qin Y,
Akazawa H, Tateno K, Kayama Y, Harada M, Shimizu I,
Asahara T, Hamada H, Tomita S, Molkentin JD, Zou Y,
Komuro I (2007) p53-Induced inhibition of Hif-1 causes
cardiac
dysfunction during pressure overload. Nature 446:444448.
doi:10.1038/nature05602
84. Schultz Jel J, Witt SA, Glascock BJ, Nieman ML, Reiser PJ,
Nix
SL, Kimball TR, Doetschman T (2002) TGF-beta1 mediates the
hypertrophic cardiomyocyte growth induced by angiotensin II.
J Clin Invest 109:787796. doi:10.1172/JCI14190
85. Schulz R, Panas DL, Catena R, Moncada S, Olley PM,
Lopas-
chuk GD (1995) The role of nitric oxide in cardiac
depression
induced by interleukin-1 beta and tumour necrosis
factor-alpha.
Br J Pharmacol 114:2734. doi:10.1111/j.1476-
5381.1995.tb14901.x
86. Shindo T, Manabe I, Fukushima Y, Tobe K, Aizawa K, Mi-
yamoto S, Kawai-Kowase K, Moriyama N, Imai Y, Kawakami
H, Nishimatsu H, Ishikawa T, Suzuki T, Morita H, Maemura K,
Sata M, Hirata Y, Komukai M, Kagechika H, Kadowaki T,
Kurabayashi M, Nagai R (2002) Kruppel-like zinc-finger tran-
scription factor KLF5/BTEB2 is a target for angiotensin II
signaling and an essential regulator of cardiovascular
remodel-
ing. Nat Med 8:856863. doi:10.1038/nm738
87. Siwik DA, Chang DL, Colucci WS (2000) Interleukin-1beta
and
tumor necrosis factor-alpha decrease collagen synthesis and
increase matrix metalloproteinase activity in cardiac
fibroblasts
in vitro. Circ Res 86:12591265. doi:10.1161/01.RES.86.
12.1259
88. Skyschally A, Gres P, Hoffmann S, Haude M, Erbel R,
Schulz
R, Heusch G (2007) Bidirectional role of tumor necrosis
factor-
alpha in coronary microembolization: progressive contractile
dysfunction versus delayed protection against infarction.
Circ
Res 100:140146. doi:10.1161/01.RES.0000255031.15793.86
89. Sobirin MA, Kinugawa S, Takahashi M, Fukushima A, Homma
T, Ono T, Hirabayashi K, Suga T, Azalia P, Takada S, Tanig-
uchi M, Nakayama T, Ishimori N, Iwabuchi K, Tsutsui H (2012)
Activation of natural killer T cells ameliorates postinfarct
car-
diac remodeling and failure in mice. Circ Res 111:10371047.
doi:10.1161/CIRCRESAHA.112.270132
90. Sperr WR, Bankl HC, Mundigler G, Klappacher G, Grosssch-
midt K, Agis H, Simon P, Laufer P, Imhof M, Radaszkiewicz T,
Glogar D, Lechner K, Valent P (1994) The human cardiac mast
cell: localization, isolation, phenotype, and functional
charac-
terization. Blood 84:38763884
91. Sun M, Dawood F, Wen WH, Chen M, Dixon I, Kirshenbaum
LA,
Liu PP (2004) Excessive tumor necrosis factor activation
after
infarction contributes to susceptibility of myocardial rupture
and
left ventricular dysfunction. Circulation 110:32213228.
doi:10.1161/01.CIR.0000147233.10318.23
92. Swirski FK, Nahrendorf M, Etzrodt M, Wildgruber M,
Cortez-
Retamozo V, Panizzi P, Figueiredo J-L, Kohler RH, Chudnov-
skiy A, Waterman P, Aikawa E, Mempel TR, Libby P, Weiss-
leder R, Pittet MJ (2009) Identification of splenic
reservoir
monocytes and their deployment to inflammatory sites.
Science
325:612616. doi:10.1126/science.1175202
93. Swirski FK, Nahrendorf M (2013) Leukocyte behavior in
ath-
erosclerosis, myocardial infarction, and heart failure.
Science
339:161166. doi:10.1126/science.1230719
Page 14 of 15 Basic Res Cardiol (2013) 108:357
123
-
94. Takeda N, Manabe I, Uchino Y, Eguchi K, Matsumoto S, Ni-
shimura S, Shindo T, Sano M, Otsu K, Snider P, Conway SJ,
Nagai R (2010) Cardiac fibroblasts are essential for the
adaptive
response of the murine heart to pressure overload. J Clin
Invest
120:254265. doi:10.1172/Jci40295
95. Tang TT, Yuan J, Zhu ZF, Zhang WC, Xiao H, Xia N, Yan
XX,
Nie SF, Liu J, Zhou SF, Li JJ, Yao R, Liao MY, Tu X, Liao
YH,
Cheng X (2012) Regulatory T cells ameliorate cardiac remod-
eling after myocardial infarction. Basic Res Cardiol
107:232.
doi:10.1007/s00395-011-0232-6
96. Thielmann M, Dorge H, Martin C, Belosjorow S, Schwanke
U,
van de Sand A, Konietzka I, Buchert A, Kruger A, Schulz R,
Heusch G (2002) Myocardial dysfunction with coronary mi-
croembolization: signal transduction through a sequence of
nitric oxide, tumor necrosis factor-a, and sphingosine. Circ
Res90:807813. doi:10.1161/01.res.0000014451.75415.36
97. Torre-Amione G, Kapadia S, Benedict C, Oral H, Young JB,
Mann DL (1996) Proinflammatory cytokine levels in patients
with depressed left ventricular ejection fraction: a report
from
the Studies of Left Ventricular Dysfunction (SOLVD). J Am
Coll Cardiol 27:12011206. doi:10.1016/0735-1097(95)00589-7
98. Torre-Amione G, Kapadia S, Lee J, Durand JB, Bies RD,
Young
JB, Mann DL (1996) Tumor necrosis factor-alpha and tumor
necrosis factor receptors in the failing human heart.
Circulation
93:704711. doi:10.1161/01.CIR.93.4.704
99. Tsutsumi Y, Matsubara H, Ohkubo N, Mori Y, Nozawa Y,
Murasawa S, Kijima K, Maruyama K, Masaki H, Moriguchi Y,
Shibasaki Y, Kamihata H, Inada M, Iwasaka T (1998) Angio-
tensin II type 2 receptor is upregulated in human heart with
interstitial fibrosis, and cardiac fibroblasts are the major
cell type
for its expression. Circ Res 83:10351046. doi:10.1161/
01.RES.83.10.1035
100. Turner NA, Porter KE, Smith WH, White HL, Ball SG,
Balm-
forth AJ (2003) Chronic beta2-adrenergic receptor
stimulation
increases proliferation of human cardiac fibroblasts via an
autocrine mechanism. Cardiovasc Res 57:784792. doi:10.1016/
S0008-6363(02)00729-0
101. Usher MG, Duan SZ, Ivaschenko CY, Frieler RA, Berger S,
Schutz G, Lumeng CN, Mortensen RM (2010) Myeloid miner-
alocorticoid receptor controls macrophage polarization and
cardiovascular hypertrophy and remodeling in mice. J Clin
Invest 120:33503364. doi:10.1172/JCI41080
102. van Amerongen MJ, Harmsen MC, van Rooijen N, Petersen
AH,
van Luyn MJ (2007) Macrophage depletion impairs wound
healing and increases left ventricular remodeling after
myocar-
dial injury in mice. Am J Pathol 170:818829. doi:10.2353/
ajpath.2007.060547
103. Venkatachalam K, Mummidi S, Cortez DM, Prabhu SD,
Valente
AJ, Chandrasekar B (2008) Resveratrol inhibits high glucose-
induced PI3K/Akt/ERK-dependent interleukin-17 expression in
primary mouse cardiac fibroblasts. Am J Physiol Heart Circ
Physiol 294:H2078H2087. doi:10.1152/ajpheart.01363.2007
104. Volz HC, Laohachewin D, Seidel C, Lasitschka F, Keilbach
K,
Wienbrandt AR, Andrassy J, Bierhaus A, Kaya Z, Katus HA,
Andrassy M (2012) S100A8/A9 aggravates post-ischemic heart
failure through activation of RAGE-dependent NF-kappaB sig-
naling. Basic Res Cardiol 107:250. doi:10.1007/s00395-012-
0250-z
105. Wang J, Xu N, Feng X, Hou N, Zhang J, Cheng X, Chen Y,
Zhang Y, Yang X (2005) Targeted disruption of Smad4 in
cardiomyocytes results in cardiac hypertrophy and heart
failure.
Circ Res 97:821828. doi:10.1161/01.RES.0000185833.42544.06
106. Wei L (2011) Immunological aspect of cardiac remodeling:
T
lymphocyte subsets in inflammation-mediated cardiac
fibrosis.
Exp Mol Pathol 90:7478. doi:10.1016/j.yexmp.2010.10.004
107. Westermann D, Lindner D, Kasner M, Zietsch C, Savvatis
K,
Escher F, von Schlippenbach J, Skurk C, Steendijk P, Riad A,
Poller W, Schultheiss HP, Tschope C (2011) Cardiac inflam-
mation contributes to changes in the extracellular matrix in
patients with heart failure and normal ejection fraction.
Circ
Heart Fail 4:4452. doi:10.1161/CIRCHEARTFAILURE.
109.931451
108. Yamaoka M, Yamaguchi S, Okuyama M, Tomoike H (1999)
Anti-inflammatory cytokine profile in human heart failure:
behavior of interleukin-10 in association with tumor
necrosis
factor-alpha. Jpn Circ J 63:951956. doi:10.1253/jcj.63.951
109. Yamazaki T, Komuro I, Yazaki Y (1998) Signalling
pathways
for cardiac hypertrophy. Cell Signal 10:693698. doi:10.1016/
S0898-6568(98)00036-9
110. Yokoyama T, Nakano M, Bednarczyk JL, McIntyre BW, Ent-
man M, Mann DL (1997) Tumor necrosis factor-alpha provokes
a hypertrophic growth response in adult cardiac myocytes.
Circulation 95:12471252. doi:10.1161/01.CIR.95.5.1247
111. Yoon PO, Lee MA, Cha H, Jeong MH, Kim J, Jang SP, Choi
BY, Jeong D, Yang DK, Hajjar RJ, Park WJ (2010) The
opposing effects of CCN2 and CCN5 on the development of
cardiac hypertrophy and fibrosis. J Mol Cell Cardiol
49:294303. doi:10.1016/j.yjmcc.2010.04.010
112. Yu Q, Horak K, Larson DF (2006) Role of T lymphocytes
in
hypertension-induced cardiac extracellular matrix
remodeling.
Hypertension 48:98104. doi:10.1161/01.HYP.0000227247.
27111.b2
113. Zaglia T, Milan G, Franzoso M, Bertaggia E, Pianca N,
Pia-
sentini E, Voltarelli VA, Chiavegato D, Brum PC, Glass DJ,
Schiaffino S, Sandri M, Mongillo M (2013) Cardiac
sympathetic
neurons provide trophic signal to the heart via
beta2-adreno-
ceptor-dependent regulation of proteolysis. Cardiovasc Res
97:240250. doi:10.1093/cvr/cvs320
114. Zamilpa R, Kanakia R, Cigarroa J 4th, Dai Q, Escobar
GP,
Martinez H, Jimenez F, Ahuja SS, Lindsey ML (2011) CC
chemokine receptor 5 deletion impairs macrophage activation
and induces adverse remodeling following myocardial infarc-
tion. Am J Physiol Heart Circ Physiol 300:H1418H1426.
doi:10.1152/ajpheart.01002.2010
115. Zandbergen HR, Sharma UC, Gupta S, Verjans JW, van den
Borne S,