Embed Size (px)
Citation preview

11
ABSTRACT
OBJECTIVE: To see the outcome of treatment of small perforations of tympanic membranes in outpatient clinic.STUDY DESIGN: A Retrospective interventional study.
st st PLACE AND DURATION: ENT Department of Jaber Al-Ahmed Armed Forces Hospital Kuwait from 1 January 2007 to 31 December 2012. METHODOLOGY: Selected 63 cases of dry/ wet central perforation of tympanic membranes were treated in outpatient clinic with the help of filter paper and Argyrols. Actively discharging, diabetic, hypetensive and patients with marginal perforation were excluded from this study. Under microscope, margins of perforations were refreshed with the help of ear needle. Filter paper soaked in Argyrols were placed over perforations. After seven to ten days, filter papers were removed to see the results. Data was analysed on SPSS versiion 17.RESULTS: Out of 63 cases, 42 (66.6%) cases were dry and 21 (33.3%) cases were associated with active discharge. These 21(33.3%) cases were treated with oral antibiotic to settle the infection. After myringoplasty, 55 (87.3%) cases were healed, 6 (09.5%) cases showed residual perforation because of big size of perforation. 2 (03.1%) cases showed no response and that was due to slipping of filter paper from its place.CONCLUSION: In Chronic Suppurative Otitis Media, Perforations of tympanic membrane can be tackled in outpatient clinic by Myringoplasty with the use of filter paper and Argyrols chemical under microscope without any local or general anesthesia.KEYWORDS: Dry perforation, filter paper, argyrols, outpatient clinic, microscope
ORIGINAL ARTICLE ISRA MEDICAL JOURNAL | Volume 8 - Issue 1 | Jan - Mar 2016
INTRODUCTION
History of myrigoplasty is interesting and delightful. Mostly german otolgist attempted different techniques. This controversial discussion is spreaded over a long area from 1878
1to 1956 . �Small and medium size perforations can be handle in outpatient clinic with good results. Patients with dry perforations are selected from the clinic. They are discussed in detail about the procedure. Once they will get the message that this will save their time and money without disturbing their daily routine life, they prefer to go for this technique. Historically, various techniques and graft materials have been tried with
2controversial effectiveness .These dry perforations are usually treated by myringoplasty under general anesthesia. This need prior admission of patient, need GA fitness, surgical procedure in operating room and post operative stay of patient in hospital. Stiches of incision are required to be removed and frequent changing of ear bandages is included in this package. In our study, we evaluated the outcome of treatment of small perforations of lymparic
membrance in out patient clinic.
METHODOLOGY
This retrospective interventional study was conducted at ENT Department of Jaber of Al-Ahmed Armed Forces Hospital
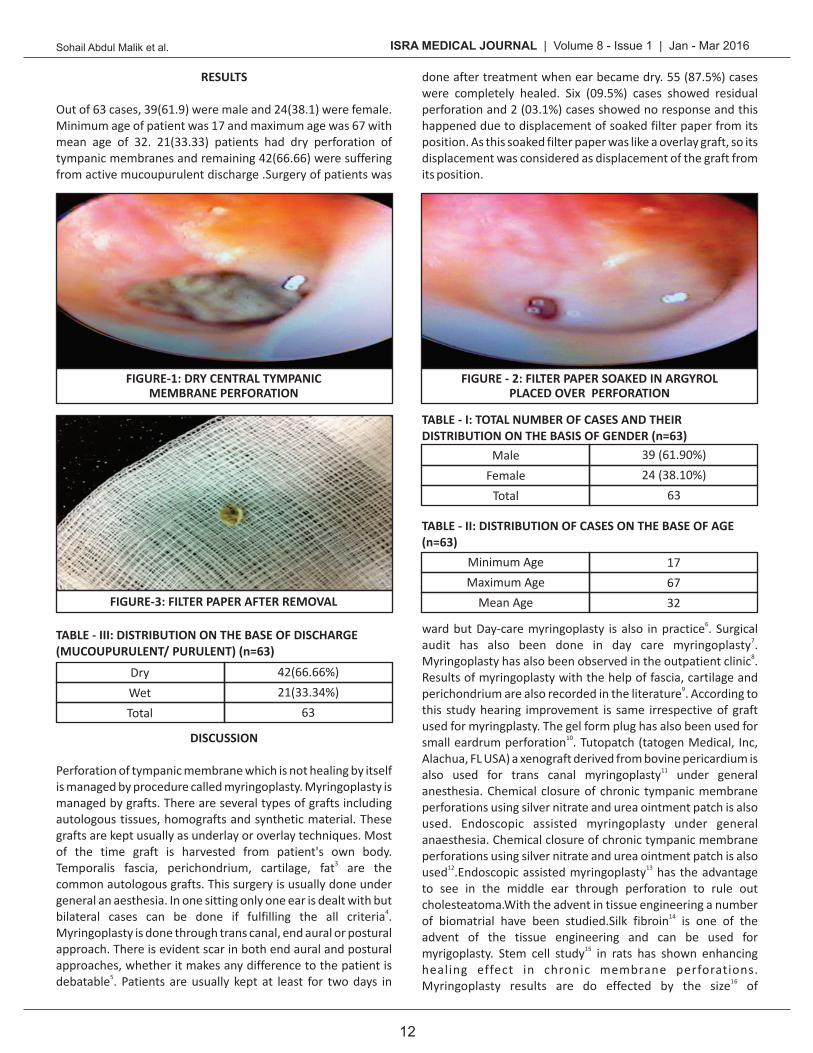
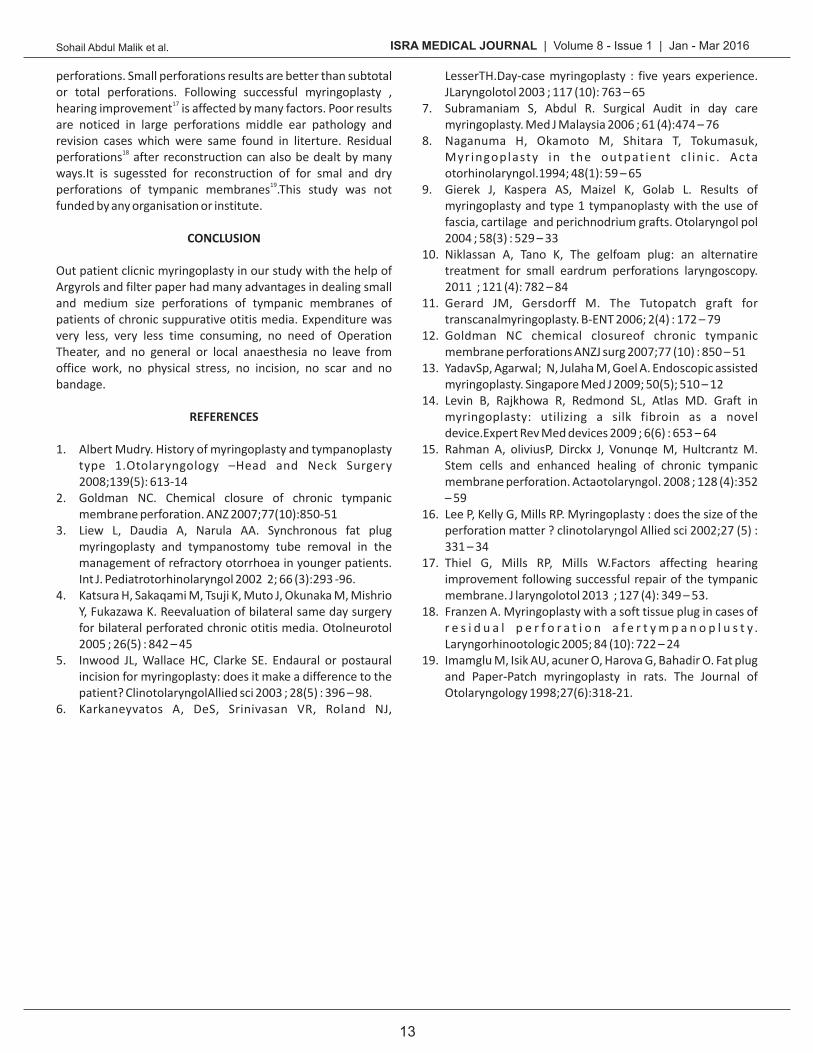
st st Kuwait from 1 January 2007 to 31 December 2012. Sixty three patients were selected from outpatient clinic. 39(61.90 s %) were male and 24 (38.10%) were female (Table - I). Maximum age was 67 and minimum age was 17 (Table - II). 42 (66.6 %) cases were dry (Figure - 1) right from the beginning and 21 (33.3 5) were actively discharging (mucoupurulent discharge) (Table - III). After 10-14 days of oral antibiotic therapy these perforations turned to dry. Filter paper which is easily available in market or in its place cigrattefilter paper is taken after removing the tobacco from it. This filter paper is made circular by the help of punch machine. The margins of perforations are injured with the help of needle used in tympanoplasty. Instead of injuring in few cases margins were refreshened. Circular patch of filter paper soaked in argyrols and with help of crocodile forcep tucked over the perforation (Figure - 2).Injuring or refreshing of perforation margins and tucking the patch of filter paper was done under microscope using the ONLAY TECHNIQUE. After one week in small perforations and after 10 days in medium size perforations filter paper was removed under microscope (Figure -2).We adopted following exclusion criteria.Actively discharging ears which failed to respond to antibiotics, diabetic, hypertension, patients with respiratory tract infections. Large central perforation/ marginal perforation were also excluded from this study.
1 2SOHAIL ABDUL MALIK , EHSAN-UL-HAQ
1.Professor of ENT Al-Tibri Medical College and Hospital Isra University Karachi Campus, Pakistan
2.Professor of ENT Multan Medical and Dental College, Multan Pakistan
Correspondence to:Sohail Abdul Malik Professor of ENT Tibri Medical College and Hospital Isra University Karachi Campus, PakistanEmail: [email protected]
MYRINGOPLASTY IN OUTPATIENT CLINIC WITH THE USEOF FILTER PAPER AND ARGYROLS CHEMICAL
ISRA MEDICAL JOURNAL | Volume 8 - Issue 1 | Jan - Mar 2016Sohail Abdul Malik et al.
12
done after treatment when ear became dry. 55 (87.5%) cases were completely healed. Six (09.5%) cases showed residual perforation and 2 (03.1%) cases showed no response and this happened due to displacement of soaked filter paper from its position. As this soaked filter paper was like a overlay graft, so its displacement was considered as displacement of the graft from its position.
6ward but Day-care myringoplasty is also in practice . Surgical 7audit has also been done in day care myringoplasty . 8Myringoplasty has also been observed in the outpatient clinic .
Results of myringoplasty with the help of fascia, cartilage and 9perichondrium are also recorded in the literature . According to
this study hearing improvement is same irrespective of graft used for myringplasty. The gel form plug has also been used for
10small eardrum perforation . Tutopatch (tatogen Medical, Inc, Alachua, FL USA) a xenograft derived from bovine pericardium is
11also used for trans canal myringoplasty under general anesthesia. Chemical closure of chronic tympanic membrane perforations using silver nitrate and urea ointment patch is also used. Endoscopic assisted myringoplasty under general anaesthesia. Chemical closure of chronic tympanic membrane perforations using silver nitrate and urea ointment patch is also
12 13used .Endoscopic assisted myringoplasty has the advantage to see in the middle ear through perforation to rule out cholesteatoma.With the advent in tissue engineering a number
14of biomatrial have been studied.Silk fibroin is one of the advent of the tissue engineering and can be used for
15myrigoplasty. Stem cell study in rats has shown enhancing healing effect in chronic membrane perforations.
16Myringoplasty results are do effected by the size of
RESULTS
Out of 63 cases, 39(61.9) were male and 24(38.1) were female. Minimum age of patient was 17 and maximum age was 67 with mean age of 32. 21(33.33) patients had dry perforation of tympanic membranes and remaining 42(66.66) were suffering from active mucoupurulent discharge .Surgery of patients was
DISCUSSION
Perforation of tympanic membrane which is not healing by itself is managed by procedure called myringoplasty. Myringoplasty is managed by grafts. There are several types of grafts including autologous tissues, homografts and synthetic material. These grafts are kept usually as underlay or overlay techniques. Most of the time graft is harvested from patient's own body.
3Temporalis fascia, perichondrium, cartilage, fat are the common autologous grafts. This surgery is usually done under general an aesthesia. In one sitting only one ear is dealt with but
4bilateral cases can be done if fulfilling the all criteria . Myringoplasty is done through trans canal, end aural or postural approach. There is evident scar in both end aural and postural approaches, whether it makes any difference to the patient is
5debatable . Patients are usually kept at least for two days in
FIGURE-1: DRY CENTRAL TYMPANICMEMBRANE PERFORATION
FIGURE-3: FILTER PAPER AFTER REMOVAL
FIGURE - 2: FILTER PAPER SOAKED IN ARGYROLPLACED OVER PERFORATION
MaleFemale
Total
TABLE - I: TOTAL NUMBER OF CASES AND THEIRDISTRIBUTION ON THE BASIS OF GENDER (n=63)
39 (61.90%)24 (38.10%)
63
DryWetTotal
TABLE - III: DISTRIBUTION ON THE BASE OF DISCHARGE(MUCOUPURULENT/ PURULENT) (n=63)
176732
TABLE - II: DISTRIBUTION OF CASES ON THE BASE OF AGE(n=63)
Minimum AgeMaximum Age
Mean Age
42(66.66%)21(33.34%)
63
ISRA MEDICAL JOURNAL | Volume 8 - Issue 1 | Jan - Mar 2016Sohail Abdul Malik et al.
13
perforations. Small perforations results are better than subtotal or total perforations. Following successful myringoplasty ,
17hearing improvement is affected by many factors. Poor results are noticed in large perforations middle ear pathology and revision cases which were same found in literture. Residual
18perforations after reconstruction can also be dealt by many ways.It is sugessted for reconstruction of for smal and dry
19perforations of tympanic membranes .This study was not funded by any organisation or institute.
CONCLUSION
Out patient clicnic myringoplasty in our study with the help of Argyrols and filter paper had many advantages in dealing small and medium size perforations of tympanic membranes of patients of chronic suppurative otitis media. Expenditure was very less, very less time consuming, no need of Operation Theater, and no general or local anaesthesia no leave from office work, no physical stress, no incision, no scar and no bandage.
REFERENCES
1. Albert Mudry. History of myringoplasty and tympanoplasty type 1.Otolaryngology –Head and Neck Surgery 2008;139(5): 613-14
2. Goldman NC. Chemical closure of chronic tympanic membrane perforation. ANZ 2007;77(10):850-51
3. Liew L, Daudia A, Narula AA. Synchronous fat plug myringoplasty and tympanostomy tube removal in the management of refractory otorrhoea in younger patients. Int J. Pediatrotorhinolaryngol 2002 2; 66 (3):293 -96.
4. Katsura H, Sakaqami M, Tsuji K, Muto J, Okunaka M, Mishrio Y, Fukazawa K. Reevaluation of bilateral same day surgery for bilateral perforated chronic otitis media. Otolneurotol 2005 ; 26(5) : 842 – 45
5. Inwood JL, Wallace HC, Clarke SE. Endaural or postaural incision for myringoplasty: does it make a difference to the patient? ClinotolaryngolAllied sci 2003 ; 28(5) : 396 – 98.
6. Karkaneyvatos A, DeS, Srinivasan VR, Roland NJ,
LesserTH.Day-case myringoplasty : five years experience. JLaryngolotol 2003 ; 117 (10): 763 – 65
7. Subramaniam S, Abdul R. Surgical Audit in day care myringoplasty. Med J Malaysia 2006 ; 61 (4):474 – 76
8. Naganuma H, Okamoto M, Shitara T, Tokumasuk, Myr ingoplasty in the outpat ient c l in ic . Acta otorhinolaryngol.1994; 48(1): 59 – 65
9. Gierek J, Kaspera AS, Maizel K, Golab L. Results of myringoplasty and type 1 tympanoplasty with the use of fascia, cartilage and perichnodrium grafts. Otolaryngol pol 2004 ; 58(3) : 529 – 33
10. Niklassan A, Tano K, The gelfoam plug: an alternatire treatment for small eardrum perforations laryngoscopy. 2011 ; 121 (4): 782 – 84
11. Gerard JM, Gersdorff M. The Tutopatch graft for transcanalmyringoplasty. B-ENT 2006; 2(4) : 172 – 79
12. Goldman NC chemical closureof chronic tympanic membrane perforations ANZJ surg 2007;77 (10) : 850 – 51
13. YadavSp, Agarwal; N, Julaha M, Goel A. Endoscopic assisted myringoplasty. Singapore Med J 2009; 50(5); 510 – 12
14. Levin B, Rajkhowa R, Redmond SL, Atlas MD. Graft in myringoplasty: utilizing a silk fibroin as a novel device.Expert Rev Med devices 2009 ; 6(6) : 653 – 64
15. Rahman A, oliviusP, Dirckx J, Vonunqe M, Hultcrantz M. Stem cells and enhanced healing of chronic tympanic membrane perforation. Actaotolaryngol. 2008 ; 128 (4):352 – 59
16. Lee P, Kelly G, Mills RP. Myringoplasty : does the size of the perforation matter ? clinotolaryngol Allied sci 2002;27 (5) : 331 – 34
17. Thiel G, Mills RP, Mills W.Factors affecting hearing improvement following successful repair of the tympanic membrane. J laryngolotol 2013 ; 127 (4): 349 – 53.
18. Franzen A. Myringoplasty with a soft tissue plug in cases of r e s i d u a l p e r f o r a t i o n a f e r t y m p a n o p l u s t y . Laryngorhinootologic 2005; 84 (10): 722 – 24
19. Imamglu M, Isik AU, acuner O, Harova G, Bahadir O. Fat plug and Paper-Patch myringoplasty in rats. The Journal of Otolaryngology 1998;27(6):318-21.





























