Embed Size (px)
Citation preview

Multiple Sclerosis
Disease Overview & Current Management Strategies

Epidemiology

Demographics of MS
Age at onset 15 to 45 years1
Gender 70% women2
US incidence 8,500 to 10,000 new cases per year1
US prevalence 350,0002
1. Jacobsen DL et al. Clin Immunol Immunopathol. 1997;84:223-243.2. Anderson DW et al. Ann Neurol. 1992;31:333-336.

Worldwide Prevalence of MS
Worldwide distribution varies
High prevalence 30+/100,000– Northern United States and Canada
– Most of Europe
– Southern Australia
– New Zealand
– Northern Russia
Kurtzke JF. Neuroepidemiology. 1991;10:1-8.

Pathophysiologyand Diagnosis

Pathology of MS
An immune-mediated disease in genetically susceptible individuals
Demyelination leads to slower nerve conduction
Axonal injury and destruction are associated with permanent neurological dysfunction
Lesions occur in optic nerves, periventricular white matter, cerebral cortex, brain stem, cerebellum, and spinal cord
Trapp BD et al. N Engl J Med. 1998;338:278-285.

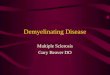
Axonal Transection in Acute MS Lesions
64m 45m A BReprinted with permission from Trapp BD et al. N Engl J Med. 1998;338:278-285. Copyright 1998 Massachusetts Medical Society. All rights reserved.

What Causes Demyelinationand Axonal Loss in MS?
Activation of autoreactive CD4+ T cells in peripheral immune system
Migration of autoreactive Th1 cells into CNS
In situ reactivation by myelin autoantigens
Activation of macrophages, B cells
Secretion of proinflammatory cytokines, antibodies
Inflammation, demyelination, axonal transection, and degeneration

Immunopathogenesis of MS
Th1+
RestingT cell
MMP
Activated (+)T cells
Th1+
Th1+
MMP
MMP
BBBBlood CNS
Th1+
TNF- IFN-
Bcell
IL-2
Th1APC APC

Immunopathogenesis of MS
Th1+MMP
Activated (+)T cells
Th1+
Th1+
MMP
MMP
Blood
RestingT cell
APC
CNS
TNF- IFN-
Bcell
IL-2
Th1 APC
BBB
Th1+

Disability Progression and Disease Type
Lublin FD, Reingold SC. Neurology. 1996;46:907-911.
Relapsing-remitting
Primary-progressive
Dis
abil
ity
Time
Time
Dis
abil
ity
Secondary-progressive
Progressive-relapsing
Time
Time
Dis
abil
ity
Dis
abil
ity

Adapted from Weinshenker BG et al. Brain. 1989;112:133-146.
Relapsing-remittingPrimary-progressive
Disease Type at Diagnosis Disease Type at 11-15 Years After Diagnosis (Among Those
With RRMS at Diagnosis)
Natural History Over Time
Secondary-progressiveRelapsing-remitting
42%
58%
15%
85%

Progression to Disability: EDSS
Expanded Disability Status Scale (EDSS)
Ordinal scale (range 0-10) measuring disability in increments of 0.5
Most widely accepted measure of disability in patients with MS
Reflects impact of disease on neurological function
Kurtzke JF. Neurology. 1983;33:1444-1452.

0 Normal neurological exam1.0–1.5 No disability2.0–2.5 Minimal disability3.0–3.5 Mild to moderate disability4.0–4.5 Moderate disability5.0–5.5 Increasing limitations in ability to walk6.0–6.5 Walking assistance is needed7.0–7.5 Confined to wheelchair8.0–8.5 Confined to bed/chair; self-care with assistance9.0–9.5 Completely dependent
10.0 Death due to MS
Progression to Disability: EDSS

Natural History
Average is 1 relapse per year, fewer over time1
25% of patients never lose ability to perform activities of daily living1
15% become severely disabled within short time1
Median time to reach EDSS of 6 is 15 years; to reach EDSS of 8 is 46 years2
Mortality from MS as primary cause is low1
1. Compston A, Coles A. Lancet. 2002;359:1221-1231. 2. Weinshenker BG et al. Brain. 1989;112:133-146.

Diagnosis of MS: Basic Principles
Ultimately a clinical diagnosis; no definitive laboratory test
Clinical profile
Laboratory evaluation
Evidence of dissemination of lesions in space and time
Exclusion of other diagnoses
Coyle P. In: Burks J, Johnson K, eds. Multiple Sclerosis, Diagnosis, Medical Management and Rehabilitation. New York: Demos; 2000:81-97.

Most Common Presenting Symptoms
Sensory symptoms in arms/legs1 33% Unilateral vision loss1 16% Multiple symptoms at onset1 14% Slowly progressive motor deficit1 9% Diplopia (double vision)1 7% Acute motor deficit1 5% Others1 16% Rarely seen1
(eg, bladder dysfunction, heat intolerance,pain, movement disorders, dementia)2 <5%
1. Paty DW. In: Burks J, Johnson K, eds. Multiple Sclerosis, Diagnosis, Medical Management and Rehabilitation. New York: Demos; 2000:75-76. 2. Paty DW, Ebers GC (eds.). Multiple Sclerosis. Philadelphia: FA Davis; 1998.

Diagnoses That Mimic MS
Infection– Lyme disease
– Neurosyphilis
– PML, HIV, HTLV-1
Inflammatory– SLE
– Sjögren’s
– Other CNS vasculitis
– Sarcoidosis
– Behçet’s disease
Cohen J, Rensel M. In: Burks J, Johnson K, eds. Multiple Sclerosis Diagnosis, Medical Management and Rehabilitation. New York: Demos; 2000:127-138.
Metabolic
– Vitamin B12 and E deficiencies
CADASIL, other rare familial diseases
CNS lymphoma
Cervical spondylosis
Motor neuron disease
Myasthenia gravis

Use of MRI in Diagnosis
MRI is used to improve confidence in a clinical diagnosis of MS or to make a diagnosis of MS in clinically isolated syndromes1
May show dissemination in space and time(eg, new lesions on follow-up MRI)1
Total lesion load at diagnosis tends to be predictive of future disability2
1. McDonald WI et al. Ann Neurol. 2001;50:121-127.2. Brex PA et al. N Engl J Med. 2002;346:158-164.

MRI Basics in Diagnosing MS
T1-weighted scan– Shows hypointense lesions (black holes)
T2-weighted scan– Indicates total burden of disease– May show new lesions
FLAIR image– Suppresses CSF– Useful for subcortical and cortical lesion
identification
Gadolinium enhancement– Highlights new or active lesions
Costello K et al. American Journal for Nurse Practitioners. October 2000:9-26.Noseworthy JH. N Engl J Med. 2000;343:938-952.

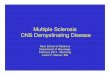
MS Lesions on MRI
T2 BOD
T1/Gd postcontrast
disease activity
T1precontrastblack holes
A B
C
T2-FLAIR
D

McDonald WI et al. Ann Neurol. 2001;50:121-127.
McDonald Diagnostic Criteria
Preserve traditional diagnostic criteria of 2 attacks of disease separated in space and time– Must be no better explanation– Add specific MRI criteria, CSF findings, and
analysis of evoked potentials as means of identifying the second “attack”
Conclude that the outcome of the diagnostic workup should yield 1 of 3 outcomes:– MS – Possible MS – Not MS

McDonald MRI Criteria
Abnormal MRI consistent with MS
– Must have at least 3 of the following:
• 1 Gd-enhancing lesion or 9 hyperintense lesions if no Gd-enhancing lesion
• 1 or more infratentorial lesions
• 1 or more juxtacortical lesions
• 3 or more periventricular lesions
– 1 cord lesion = 1 brain lesion
McDonald WI et al. Ann Neurol. 2001;50:121-127.

Gd-enhancing T2-hyperintense
Juxtacortical Periventricular Spinal Cord
Infratentorial
McDonald MRI Criteria

Reprinted with permission from Rudick RA et al. Neurology. 1999;53:1698-1704.
Brain Atrophy

Secondary-progressiveSecondary-progressive
Relapsing-remittingRelapsing-remittingPreclinicalPreclinical
Disease Progression
Time
Adapted with permission from JS Wolinsky.
Dis
a bi l
i ty
Measures of brain volumeRelapses and impairmentMRI burden of diseaseMRI activity

Disease Management

Goals of Disease Management
Treating relapses
Managing symptoms
Modifying or reducing relapses and delaying progression to disability
Facilitating an acceptable quality of life

Acute MS Relapses
Relapses– Focal disturbances of function >24 hours
– Occur about once a year in untreated patients
– In absence of environmental, metabolic, or infectious processes
Management: high-dose steroids– Common option: methylprednisolone IV for
5 days followed by short course of prednisone
– Oral prednisone, oral methylprednisolone, or dexamethasone

Common MS Symptoms
Fatigue
Depression
Focal muscle weakness
Visual changes
Bowel/bladder/sexual dysfunction
Gait problems/spasticity
Paresthesias

Less Common MS Symptoms
Dysarthria, scanning speech, dysphagia
Lhermitte’s phenomenon
Neuritic pain
Vertigo/ataxia
Cognitive dysfunction
Tremor/incoordination

Rare MS Symptoms
Decreased hearing
Seizures
Tinnitus
Mental disturbance
Paralysis

Sources of Symptoms
Symptoms vary widely in incidence and severity
Sensory symptoms,Lhermitte’sPainProprioception
Optic neuritis
DiplopiaVertigoDysarthriaINO
Tremor,Ataxia
Cognitive loss
Emotional disinhibition
Bladder dysfunction

Symptom Management: Fatigue
75% to 95% of patients with MS have fatigue, which is often debilitating
Rule out possible other causes, such as hypothyroidism, depression, anemia, heat exposure, sleep disorders, pulmonary dysfunction
Shapiro RT, Schneider DM. Fatigue. In: Multiple Sclerosis in Clinical Practice; 1999. MS Council for Clinical Practice Guidelines. Fatigue and Multiple Sclerosis; 1998.

Symptom Management: Fatigue
Management includes:– Lifestyle changes
– Effective energy expenditure
– Pharmacologic interventions• CNS stimulants, eg, amantadine and modafinil• Antidepressants, eg, fluoxetine
Shapiro RT, Schneider DM. Fatigue. In: Multiple Sclerosis in Clinical Practice; 1999. MS Council for Clinical Practice Guidelines. Fatigue and Multiple Sclerosis; 1998.

Symptom Management: Pain
Pain is a complex sensory phenomenon
Multiple causes and types– Neuropathic
– Musculoskeletal
– Optic neuritis
– Spasticity
– Dystonia
Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.

Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.
Symptom Management: Pain
Nonpharmacologic– Seating
– Posture improvement
– Physical therapy• Gait training• Assistive devices• Muscle strengthening/stretching

Pharmacologic options– Tricyclic antidepressants
• Amitriptyline (Elavil®), nortriptyline (Pamelor®)
– Antiepileptic medications• Carbamazepine (Tegretol®), gabapentin
(Neurontin®), phenytoin (Dilantin®)
– Antispasticity medications• Baclofen, tizanidine (Zanaflex®)• Benzodiazepines, eg, clonazepam (Klonopin®)
Symptom Management: Pain
Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.

Symptom Management: Spasticity
Spasticity can – Limit mobility
– Expend excessive energy
– Cause discomfort
Described as– Tightness
– Pulling
– Tugging
– Aching

Symptom Management: Spasticity
Nonpharmacologic interventions – Stretching
– Positioning
– Seating
– Physical therapy
Surgical Interventions– Baclofen pump
– Rhizotomy
Pharmacologic interventions– Baclofen
– Tizanidine
– Diazepam
– Dantrolene
– Nerve blocks
– Botulinum toxin

Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.
Symptom Management: Bladder Dysfunction
Failure to store urine, empty bladder, or both
Symptoms include double voiding, hesitancy, frequency, urgency, incontinence, UTIs
Evaluation: rule out UTI, check post-void residual (ie, amount of urine remaining after voiding bladder)
Management– Antispasmodics – Tricyclic antidepressants– DDAVP (an antidiuretic hormone)– Alpha blockers– Intermittent self-catheterization– Indwelling catheter

Symptom Management: Bowel Dysfunction
Caused by lesions in spinal cord
Symptoms– Constipation is most common– Involuntary bowel – Diarrhea is uncommon
Management– Constipation: fiber, fluids, activity, bowel
training, laxatives, dietary modification– Involuntary bowel: fiber, anticholinergics,
dietary modification
Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.

1. Prosiegel M, Michael C. J Neurol Sci. 1993;115:S51-S54.2. Rao SM. Curr Opin Neurol. 1995;8:216-220.
Symptom Management: Cognitive Impairment
Occurs in 45% to 60% of patients1 but results in significant changes in only 15%2
Manifests as short-term memory loss or impaired judgment, learning, word finding, or executive functioning
Management– Neuropsychiatric testing– Compensatory techniques– Cognitive retraining– Disease-modifying therapies

Sexual Dysfunction/Intimacy
Men and women can experience difficulties
Libido
Erection
Frequency of orgasms
Lubrication
Bladder spasticity
Depression
Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.

Sexual Dysfunction/Intimacy
Management strategies include– Pharmacologic management
– Treat underlying symptoms
– Adjust medications
– Positioning
– Lifestyle changes
Key to successful management is open communication
Costello K et al, eds. Nursing Practice in Multiple Sclerosis: A Core Curriculum. New York: Demos; 2003.

Disease-Modifying Therapies

Disease Modification
Aim to alter the natural course of the disease– Decrease relapses
– Delay disability
Two classes of disease-modifying medications:– Immunomodulators
– Immunosuppressants
Noseworthy JH et al. N Engl J Med. 2000;343:938-952.

MS Immunotherapy
Nonspecific immunomodulation– Interferon beta-1b (Betaseron®), Interferon
beta-1a (Avonex®, Rebif®)
Selective immunomodulation– Glatiramer acetate (Copaxone®)
Nonspecific immunosuppression– Corticosteroids– Mitoxantrone (Novantrone®)– Cyclophosphamide (Cytoxan®)*
Experimental therapies*
*These drugs do not have FDA approval for use in MS.

Type Recombinant protein Polypeptide mixture
Indication Reduce relapse frequency in RRMS
Slow Slowaccumulation accumulationof disability of disability
How given 30 g IM 22 or 44 g SC 250 g SC 20 mg SCweekly every other day 3x/week daily
Relapse rate 18% 27%-33% 30% 32%(annualized) (2 years) (5 years) (long-term)
Published data 2 years 4 years 5 years 8+ years
IFN -1a(Rebif®)
Nonselective and Selective Immunomodulatory Treatments
IFN -1a(Avonex®)
IFN -1b(Betaseron®)
GlatiramerAcetate
(Copaxone®)

IFN -1a(Rebif®)
Nonselective and Selective Immunomodulatory Treatments
MRI findings Reduces Reduces Reduces rate Reduces lesions active lesions of new lesions lesions
Reduces risk for Reduces Reduces rate Reduces lossprogression disability of severe of brain tissue
of disability relapses
Common side Mild flulike symptoms, No flulike effects muscle aches, anemia symptoms
No Injection-site reactionsinjection-site
reactions Menstrual Systemicdisorders; mild post-neutropenia and injection
thrombocytopenia; reactionabnormal liver
function
IFN -1a(Avonex®)
IFN -1b(Betaseron®)
GlatiramerAcetate
(Copaxone®)

Mechanisms of Action

Cytokine Imbalance in MS
Normal MS
InflammatoryIFN-IL-12TNF
InflammatoryIFN- IL-12TNF
Anti-inflammatory
IL-4IL-10TGF-
Anti-inflammatory
IL-4IL-10TGF-
Th1 Th2
Th1
Th2

Potential Mechanisms ofAction of IFN- in MS
Antiproliferative effect
Blocking T-cell activation
Apoptosis of autoreactive T cells
IFN- antagonism
Cytokine shifts
Antiviral effect
Does not cross blood-brain barrier
Indirect effects on CNS

IFN-β
MS
InflammatoryTh1 cytokines
Anti-inflammatoryTh2 cytokines
IL-10
IL-12
IFN-β–Induced Cytokine Shift

Th1+
RestingT cell
MMP
Activated (+)T cells
Th1+
Th1+
MMP
BBBBlood CNS
Th1+
TNF-α
IFN-γ
IL-2
Th1APC APC
IFN-β
IFN-β
MyelinproteinAntigen
Adapted from Yong VW. Neurology. 2002;59:802-808.
Effects of IFN- at Blood-Brain Barrier

Glatiramer Acetate: Possible Mechanisms of Action
Blocking autoimmune T cells
Induction of anergy
Induction of anti-inflammatory Th2 cells
Bystander suppression
Neuroprotection
Neuhaus O et al. Neurology. 2001;56:702-708.

Th2+
Adapted from Yong VW. Neurology. 2002;59:802-808.
Th2+
GA-inducedT cell
MMP
Activated (+)T cells
Th2+
Th2+
MMP
MMP
BBBBlood CNS
IL-4 TGF-β
Bcell
IL-10
Th2APC APC
Glatiramer acetate (GA)
Myelinprotein
• Bystander suppression
Effects of Glatiramer Acetateat Blood-Brain Barrier

Relapse Rates

0.25
0.50
0.75
1.00
1.25
1.50
1 2 3 4 5
PlaceboInterferon -1b, 8 MIU
Mea
n N
um
ber
of
Rel
apse
s 33%*
Study Year
28%†
28%‡
30%‡24%‡
Adapted from IFNB Multiple Sclerosis Study Group. Neurology. 1995;45:1277-1285.
*P < 0.001; †P < 0.05; ‡P = NS.
IFN -1b: Annual Relapse Rates Over 5 Years

Adapted from Jacobs LD et al. Ann Neurol. 1996;39:285-294.
Mea
n N
um
ber
of
Rel
apse
s
00.10.20.30.40.50.60.70.80.91.0
All Patients Patients Treated
2 Years
PlaceboInterferon -1a18%*
32%†
*P < 0.04; †P < 0.002.
Interferon β-1a IM: Annual Relapse Rate

PRISMS Study Group. Neurology. 2001;56:1628-1636.
Placebo/Active
22 g 3/wk
44 g3/wk
Placebo Both IFN -1a Arms
0.720.801.02
1.5 1.5
52%47%32%
P < 0.0001
P < 0.0001
0.0
0.5
1.0
1.5
2.0
Prior to Study Entry
Mea
n N
um
ber
of
Rel
apse
s/P
atie
nt/
Yea
r
At 4 Years
Annual Mean Number of Relapses for IFN -1a SC

Placebo
Glatiramer Acetate: Mean Relapse Rate
Adapted from Johnson KP et al. Neurology. 1998;50:701-708.
Glatiramer Acetate
0.00.20.40.60.81.01.21.41.61.82.0
Mea
n N
um
ber
of
Rel
apse
s
24 Months 24 Months + Extension
29%*
32%†
*P < 0.007; †P < 0.002.

Glatiramer Acetate: 8-Year DataAnnualized Relapse Rate
P = 0.05P = 0.01
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Re
lap
se
Rat
e (
me
an
s)
Entry Placebo-ControlledPhase and Extension
Placebo-ControlledPhase Through
Open-Label Phase
Glatiramer AcetatePlaceboPlacebo/Active
Johnson KP et al. Neurology. 2002;58(suppl 3):A458. P06.079.

Mean Annual Relapse Rates of DMTsNonrandomized, Open-Label Study
Haas J et al. Presented at: AAN, 2003.
INF β-1a IMINF β-1b SCGAINF β-1a 22 μg SC
1.4
1.2
1.0
0.8
0.4
0.6
0.2
0.0Before Study 6 Months 12 Months 24 Months
Mea
n N
um
ber
of
Rel
apse
s

Effects on Disability

ITT progression-free patients: all crossover vs 3 44 g:
P = 0.07
Adapted with permission from PRISMS-4 Study Group. Neurology. 2001;56:1628-1636.
Time (months)0 6 12 18 24 30 36 42 48
1.0
0.8
0.6
0.4
Placebo/44Placebo/22
3 443 22
Pro
po
rtio
n o
f P
ati
ents
IFN -1a SC: Proportion of Patients Free From Progression Over 4 Years

Time to progression:P = 0.096
Patients With Sustained Progression 1 EDSS Step
Placebo 46% (56/122)
IFN -1b 8 MIU 35% (43/122)
Adapted with permission from the IFNB MS Study Group. Neurology. 1995;45:1277-1285.
Pro
bab
ilit
y (%
)
Days
0 180 360 540 720 900 1080 1260 1440 1620 1800
100
90
80
70
60
50
40
30
20
10
0
8 MIUPlacebo1.6 MIU
IFN -1b: Probability of Avoiding Progression Over 5 Years

Johnson KP et al. Mult Scler. 2000;6:255-266.
0 1 2 3 4 5 6 7
Placebo/Active (n = 107)Glatiramer Acetate (n = 101)Time to worsening: P = 0.048
Open-Label PhasePlacebo-Controlled
Phase
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Su
rviv
al D
istr
ibu
tio
n E
stim
ate
Years
Glatiramer Acetate: Time to Worsening by 1.5 EDSS Steps Over 6 Years (Open-Label Cohort)

Glatiramer Acetate: 8-Year DataYearly EDSS Change From Baseline
Ch
ang
e in
ED
SS
Sco
re
Entry 1 2*
3*
4*
5 6 7 8
Year*P < 0.05.
Glatiramer AcetatePlacebo/Active
P = 0.0279 (RMA)
0.8
0.4
0.7
0.6
0.5
0.2
0.3
0.0
0.1
–0.1
Johnson KP et al. Neurology. 2002;58(suppl 3):A458.

Glatiramer Acetate: 8-Year DataCategorical EDSS Change From Randomization
to Last Observation
65.3
50.4
34.7
49.5
0
5
15
25
35
45
55
65
75
Improved/No Change Worsened
Glatiramer AcetatePlacebo/Active
Pat
ien
ts (
%) P = 0.0263
Johnson KP et al. Neurology. 2002;58(suppl 3):A458.

MRI Findings

MRI Endpoints in RRMS TrialsT2 Lesion Burden (Median % Change)*
*Weekly doses reported.1. Paty DW, Li DK. Neurology. 1993;43:662-667.2. Comi G et al. Ann Neurol. 2001;49:290-297.
66 μg
–15 –10 –5 0 5 10 15 20
P < 0.001
P = 0.36
P < 0.0001
IFN β-1b 1
IFN β-1a IM
Placebo
175 μg
875 μg
Placebo
132 μg
30 μg
Placebo
Glatiramer acetate 2
25
PlaceboP = 0.001
140 mg
IFN β-1a SC

IFN -1a IM: Change in Volumeof Black Holes (Total Lesion Load)
0
25
50
75
100
125
150
Placebo IFN β-1a IM
To
tal L
esio
n L
oad
(m
m3),
M
ed
ian
Ch
an
ge
Fro
m B
ase
line
P = 0.065, NS
n = 80 n = 80
Simon JH et al. Neurology. 2000;55:185-192.

Active lesion—new or enlarging T2, new or persistently Gd-enhancing, avoiding double counting. The exact relation between MRI findings and the clinical status of patients is unknown.
Panitch H et al. Neurology. 2002;59:1496-1506.
0
1
2
3
4
5
6
7
8
Week (4-Week MRI Scans)
0 4 8 12 16 20 24
Mea
n C
um
ula
tive
C
U A
ctiv
e L
esio
ns
*P < 0.001 at Week 24
EVIDENCE Trial CU Lesions
IFN β-1a 30 μg qw IM
IFN β-1a 44 μg tiw SC

9.7
7.2
3.4
–6.2
–10
–5
0
5
10
Placebo/22 μgtiw SC(n = 57)
Placebo/44 μgtiw SC(n = 49)
IFN β-1a 22 μgtiw SC
(n = 117)
IFN β-1a 44 μgtiw SC
(n = 111)
IFN β-1a 44 tiw SC vs placebo/44 tiw SCIFN β-1a 22 tiw SC vs placebo/22 tiw SCIFN β-1a 44 tiw SC vs IFN β-1a 22 tiw SC
Med
ian
Per
cen
t C
han
ge
in T
ota
l T2
Les
ion
Are
a
The exact relation between MRI findings and the clinical status of patients is unknown.
PRISMS Study Group. Neurology. 2001;56:1628–1636 [correction in 57:1146].
P = 0.11 P = 0.003 P = 0.009
IFN β-1a SC Long-term Data: MRI T2 Lesions

Adapted with permission from the IFNβ MS Study Group. Neurology. 1995;45:1277-1285.
6.7
21.0
30.2
11.9
18.7
3.6
–0.8–3.8–4.9 –5.6
1 2 3 4 5
Placebo8 MIU
Med
ian
Ch
ang
e A
fter
Bas
elin
e
P = 0.0363
Study Year
P = 0.0012
P = 0.0015
P = 0.0002 P = 0.0055
35
–10
–5
0
5
10
15
20
25
30
IFN -1b: Median Change in MRI-Measured BOD217 Patients Having at Least a Fourth-Year Annual Scan

Stone LA et al. Neurology. 1997;49:862-869.
Months on Study (27 Subjects)
1 2 3 4 5 6 7 8 9 10 11 120
20406080
100120140160
To
tal E
nh
ance
men
ts
80%–90% response
Interferon β-1b initiated
Effect of IFN -1b on Enhancements

Months
Placebo
0
5
Vo
lum
e %
Ch
ang
e (m
edia
n)
1 2 3 4 5 6 7 8 9
Comi G et al. Neurology. 2001;56(suppl 3):A255.
Glatiramer Acetate 9-Month Data:MRI T2 Lesions
25
20
15
10
Glatiramer Acetate

Adapted with permission from Comi G et al. Ann Neurol. 2001;49:290-297. This material is used by permission of John Wiley & Sons, Inc.
Primary Endpoint: Cumulative Numberof Enhancing Lesions (9 Months)
36.8
26.0
0
5
10
15
20
25
30
35
40
45
Les
ion
Nu
mb
er (
mea
n +
SE
)
–29%P = 0.0032
LOCF
PlaceboGlatiramer Acetate

Glatiramer acetate had significant effects on:
Reduction P Value
Total number of enhancing lesions (LOCF) 29% 0.003
Total number of enhancing lesions (as is) 35% 0.001
Total number of new enhancing lesions 33% 0.003
Total number of new T2 lesions 30% 0.003
T2 lesion volume (median, from baseline) 40% 0.001
Relapse rate (9 months) 33% 0.01
Comi G et al. Ann Neurol. 2001;49:290-297.
European/Canadian MRI Trial: Summary

Glatiramer Acetate: Evolution to Black Holes
0
5
10
15
20
25
30
35
7 8
Lesion Age (months)
Les
ion
s E
volv
ing
Into
B
lack
Ho
les
(%)
P = 0.002
P = 0.04 31.4%
15.6%
Filippi M et al. Neurology. 2001;57:731-733.
PlaceboGlatiramer Acetate
50%

Safety and Tolerability

Long-term Safety and Tolerability Issues: IFNs
Flulike syndrome (fever, chills, fatigue) – Experienced by up to 75% of patients taking
an IFN-β
Injection-site reaction and necrosis
Depression
Liver function and bone marrow abnormalities
Neutralizing antibodies
PRISMS Study Group. Lancet. 1998;352:1498-1504.Freedman M. Presented at: The American Academy of Neurology 52nd Annual Meeting; April 29-May 6, 2000; San Diego, Calif.The IFNB MS Study Group. Neurology. 1995;45:1277-1285.

Neutralizing Antibodies
Conflicting evidence regarding role of neutralizing antibodies in treatment failure
38% of patients in the IFN -1b trial developed neutralizing antibodies by the end of the third year1
5% of patients in a recent weekly IFN -1a IM trial who had received drug for at least 1 year developed neutralizing antibodies2
1. The IFNβ Multiple Sclerosis Study Group. Neurology. 1993;43:655-661.2. Avonex® [package insert]. Cambridge, Mass: Biogen, Inc; 2003.

Glatiramer Acetate–Reactive Antibodies
In clinical trials, patients treated with glatiramer acetate developed reactive antibodies that peaked at 3 months and decreased at 6 months1
Development of these antibodies did not correlate with side effects and did not affect therapeutic activity of glatiramer acetate1
Additional recent research confirms that reactive antibodies do not interfere with the biological functions of glatiramer acetate2
1. Brenner T et al. J Neuroimmunol. 2001;115:152-160.2. Teitelbaum D et al. Mult Scler. 2003;9(suppl 1):S37.

Long-term Safety and Tolerability Issues: Glatiramer Acetate
Injection-site reaction
Immediate postinjection reaction
Copaxone® [package insert]. Kansas City, Mo: Teva Marion Partners; 2000.

possibly
no
C
B
noyesyesyesIFN
yesnonoyesGA
Menstrual disorders
Pregnancy category
Post-injection reaction
Flulike symptoms
Lab changes
Injection- site
reaction
Safety and Tolerability Issues

Side Effect Management

Walther EU, Hohlfeld R. Neurology. 1999;53:1622-1627.
Side Effect Management: IFN Flulike Symptoms
Begin 3-6 hours after injection; last up to 24 hours
Management:– Injection at night
– NSAIDs or acetaminophen as comedications
– Dose titration
Not experienced with glatiramer acetate

1. Copaxone® [package insert]. Kansas City, Mo: Teva Marion Partners; 2000.
Side Effect Management:IFN Laboratory Test Abnormalities
Obtain baseline complete blood count and differential and liver function values before initiation of therapy
Monitor laboratory test values at regular intervals after initiation of therapy
Consider dose adjustment or discontinuation of treatment if abnormalities persist
Not indicated with glatiramer acetate1

Side Effect Management: IFN Injection-Site Reactions
Site rotation
Ice to injection site
Use of autoinjector
Local wound care for skin necrosis

Side Effect Management:Glatiramer Acetate Injection-Site Reactions
Site rotation
Ice to injection site
Use of autoinjector

Side Effect Management:Glatiramer Acetate Postinjection Reaction
Occurs immediately after injection and consists of facial flushing, chest tightness, palpitations, anxiety, and shortness of breath
Unrelated to serious sequelae
Treatment steps:– Educate patient about possible occurrence– Reassure patient if reaction occurs– Instruct patient to sit upright in a comfortable
chair– Refer for emergency care if no improvement
in symptom intensity after 15-20 minutes

Quality of Life andAdherence

Facilitating an Acceptable QOL
Quality of life (QOL) is the congruence between actual life conditions and one’s hopes and expectations
MS, with its range of symptoms and its progressive nature, has a profound effect on QOL
Maximizing QOL is an essential component of an optimal management strategy
Includes comprehensive approach

Promoting Adherence
Educate about the critical role of adherence in outcomes
Recognize and address barriers to adherence
Importance of clarifying realistic expectations
Advocacy– Assistance with reimbursement
– Identify resources
– Involve family

Burden of diseaseEnhancing lesions
Disease courseNumber of relapses
Medical PatientConsiderations Considerations
LifestyleExpectationsCapabilities
Support system
Factors That Influence Treatment Decisions

Summary

Summary: Goals of DiseaseManagement in MS
Modifying/reducing relapses and delaying progression to disability
Treating relapses
Managing symptoms
Facilitating an acceptable quality of life