Embed Size (px)
Citation preview

International Journal of
Molecular Sciences
Review
Multifaceted Interpretation of Colon CancerStem Cells
Yuichiro Hatano 1, Shinya Fukuda 1, Kenji Hisamatsu 1, Akihiro Hirata 2, Akira Hara 1 andHiroyuki Tomita 1,*
1 Department of Tumor Pathology, Gifu University Graduate School of Medicine, Gifu 501-1194, Japan;[email protected] (Y.H.); [email protected] (S.F.); [email protected] (K.H.);[email protected] (A.H.)
2 Division of Animal Experiment, Life Science Research Center, Gifu University, 1-1 Yanagido, Gifu 501-1194,Japan; [email protected]
* Correspondence: [email protected]; Tel.: +81-58-230-6225; Fax: +81-58-230-6226
Received: 7 June 2017; Accepted: 3 July 2017; Published: 5 July 2017
Abstract: Colon cancer is one of the leading causes of cancer-related deaths worldwide, despite recentadvances in clinical oncology. Accumulating evidence sheds light on the existence of cancer stemcells and their role in conferring therapeutic resistance. Cancer stem cells are a minor fraction ofcancer cells, which enable tumor heterogeneity and initiate tumor formation. In addition, these cellsare resistant to various cytotoxic factors. Therefore, elimination of cancer stem cells is difficult butessential to cure the malignant foci completely. Herein, we review the recent evidence for intestinalstem cells and colon cancer stem cells, methods to detect the tumor-initiating cells, and clinicalsignificance of cancer stem cell markers. We also describe the emerging problems of cancer stem celltheory, including bidirectional conversion and intertumoral heterogeneity of stem cell phenotype.
Keywords: colon cancer; cancer stem cell; intestinal stem cell; genetics; epigenetics; bidirectionalconversion; tumor heterogeneity
1. Cancer Stem Cells (CSCs) and Colon Cancer
Cancer stem cell (CSC) theory is the concept that cancer tissue contains a minor population ofcells with stem cell properties [1]. This minor fraction is believed to contribute to the development andexpansion of cancerous tissues, similar to tissue stem cells that generate normal functional histologicalunits, tissues, and organs. Therefore, the minimal qualifications for CSCs include self-renewal andtumor formation ability. Self-renewal is essential to maintain their stemness, which is the potentialfor both cellular proliferation and differentiation. By asymmetric cell division, CSCs are long-lived,have a low proliferative nature, and simultaneously produce actively proliferating cancer progenitorcells. The long-lived, low proliferative CSCs are resistant to cytotoxic conditions, whereas theactively proliferating cancer progenitor cells have an advantage of tumor propagation. Together,these heterogeneous components lead to tumor formation, which results in multiple and recurrentlesions in the clinical course of the disease. The concept of CSCs is a sophisticated interpretation ofintratumoral heterogeneity.
Although the idea of CSCs originally occurred about 160 years ago [2], the first demonstration wasmade in 1997. Bonnet and Dick reported that CD44+/CD38− leukemia cells possessed CSC properties,i.e., self-renewal, potential for proliferation and differentiation, and tumor formation ability, in nudemice [3]. After the first report, tumor-initiating cells with a stem cell phenotype were identified inseveral types of solid tumor, including colon cancer [4]. Currently, CSC theory provides a universalbasis to understand tumor cell biology.
Int. J. Mol. Sci. 2017, 18, 1446; doi:10.3390/ijms18071446 www.mdpi.com/journal/ijms

Int. J. Mol. Sci. 2017, 18, 1446 2 of 14
Colon cancer is the fourth most deadly cancer in the world [5]. The incidence is rising in manycountries, potentially because of widespread adoption of the Western diet and lifestyle. Worldwidemortality of colon cancer is approximately 50%, which varies according to the available therapeuticoptions. Interestingly, a systematic review reveals that surgical debulking of liver metastasis improvesthe prognosis of patients with colorectal cancer [6]. Although this macroscopic intervention isefficacious in advanced stage colon cancer, new clinical approaches to target CSCs are desired toeliminate viable cancer cells completely. The following sections describe a strategy to detect coloncancer cells with a stem cell-like/tumor-initiating phenotype (Figure 1).
Int. J. Mol. Sci. 2017, 18, 1446 2 of 14
Colon cancer is the fourth most deadly cancer in the world [5]. The incidence is rising in many
countries, potentially because of widespread adoption of the Western diet and lifestyle. Worldwide
mortality of colon cancer is approximately 50%, which varies according to the available therapeutic
options. Interestingly, a systematic review reveals that surgical debulking of liver metastasis
improves the prognosis of patients with colorectal cancer [6]. Although this macroscopic
intervention is efficacious in advanced stage colon cancer, new clinical approaches to target CSCs are
desired to eliminate viable cancer cells completely. The following sections describe a strategy to
detect colon cancer cells with a stem cell-like/tumor-initiating phenotype (Figure 1).
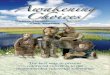
Figure 1. Various methods to detect colon cancer stem cells. Colon cancer stem cells are detectable on
the basis of common cancer stem cell markers (Section 2.1), intestinal stem cell markers (Section 2.2–
2.3), side population (Section 2.5), aldehyde dehydrogenase (ALDH1) activity (Section 2.6), and
hormone regulators (Section 2.7). Considering the multifaceted nature of cancer stem cells, there
must be unknown factors that mark cancer stem cells (for example, epithelial–mesenchymal
transition (EMT) inducers, Section 2.4).
2. Methods to Detect Colon Cancer Stem Cells
2.1. Cell Surface CSC Markers
Cell surface proteins have contributed to the isolation and identification of tumor-initiating
cancer cells [7]. Based on the presence of specific cell surface proteins, flow cytometric analysis
divides cancer cells into two populations. The isolated populations are often tested for their stem cell
properties using in vitro assays, and injected into nude mice to investigate their tumor forming
ability. These experiments are often attempted to demonstrate whether the cell surface protein of
interest is a CSC marker. Not surprisingly, the surface CSC markers identified in past studies are
concomitantly expressed in the CSC population. Therefore, dual color flow cytometric analysis with
combined CSC cell markers yields a highly precise CSC population. The following sections
introduce selected cell surface proteins that function as candidate CSC markers in colon cancer.
2.1.1. CD44
Of the first CSC phenotype, CD44+/CD38− [3], CD44 positivity in CSCs is found not only in
leukemia but also other solid tumors [8]. CD44 is a multifunctional cell surface adhesion protein that
reacts with extracellular matrix components, i.e., hyaluronan. The CD44 protein family consists of
various isoforms created by alternative splicing of ten different variant exons. One CD44 variant
Figure 1. Various methods to detect colon cancer stem cells. Colon cancer stem cells are detectable onthe basis of common cancer stem cell markers (Section 2.1), intestinal stem cell markers (Sections 2.2and 2.3), side population (Section 2.5), aldehyde dehydrogenase (ALDH1) activity (Section 2.6), andhormone regulators (Section 2.7). Considering the multifaceted nature of cancer stem cells, there mustbe unknown factors that mark cancer stem cells (for example, epithelial–mesenchymal transition (EMT)inducers, Section 2.4).
2. Methods to Detect Colon Cancer Stem Cells
2.1. Cell Surface CSC Markers
Cell surface proteins have contributed to the isolation and identification of tumor-initiating cancercells [7]. Based on the presence of specific cell surface proteins, flow cytometric analysis divides cancercells into two populations. The isolated populations are often tested for their stem cell propertiesusing in vitro assays, and injected into nude mice to investigate their tumor forming ability. Theseexperiments are often attempted to demonstrate whether the cell surface protein of interest is aCSC marker. Not surprisingly, the surface CSC markers identified in past studies are concomitantlyexpressed in the CSC population. Therefore, dual color flow cytometric analysis with combined CSCcell markers yields a highly precise CSC population. The following sections introduce selected cellsurface proteins that function as candidate CSC markers in colon cancer.
2.1.1. CD44
Of the first CSC phenotype, CD44+/CD38− [3], CD44 positivity in CSCs is found not only inleukemia but also other solid tumors [8]. CD44 is a multifunctional cell surface adhesion proteinthat reacts with extracellular matrix components, i.e., hyaluronan. The CD44 protein family consistsof various isoforms created by alternative splicing of ten different variant exons. One CD44 variant

Int. J. Mol. Sci. 2017, 18, 1446 3 of 14
associated with cancer metastasis was first discovered in a rat carcinoma cell line [9]. Subsequently,CD44 expression in colon cancer was reported [10] before the demonstration of leukemia stem cells.Expression of CD44 v6 is frequently found in advanced stages of colon cancer [11] and is associatedwith poorer prognosis [12].
CD44 v6 binds hepatocyte growth factor (HGF) and vascular endothelial growth factor(VEGF) [13,14]. These interactions are important to Ras activation and angiogenesis in cancer [15,16].Subsequent alterations of cellular signaling and the microenvironment contribute to the tumor initiatingability of cancer cells. Interestingly, the expression of CD44 v6 is inducible in colon cancer cells byRho kinase (ROCK) inhibitors or a myosin II inhibitor [17]. Increased CD44 expression leads toenhancement of CSC properties in colon cancer cells. These findings support the interconversion ofcancer stemness: CSCs differentiate into non-CSCs while non-CSCs give rise to CSCs through thereactivation of stem cell markers.
2.1.2. CD133
CD133, also known as prominin-1, is a 120 kDa five transmembrane cell surface protein that affectsmulticellular functions including stemness, tumorigenesis, chemo-/radio-resistance, metabolism,autophagy, and apoptosis [18]. The expression of CD133 in colon cancer is one of the most importantfeatures of colon cancer stem cells. CD133+ human colon cancer cells are able to initiate tumorformation in immunodeficient mice [4]. Todaro et al. reported that CD133+ cells, approximately2% of human colon cancer cells, are treatable by an interleukin-4 inhibitor [19]. In addition, flowcytometric analysis revealed that CD133+ colon cancer cells overlap the cell fractions expressingCD44, CD29, CD24, and CD166 [20]. Isolated single CD133+ colon cancer cells show self-renewaland multi-lineage differentiation. Consistent with this evidence, transgenic mice demonstrate thatCD133 marks intestinal stem cells, which transform into neoplastic cells by expression of mutatedβ-catenin [21]. Recent evidence suggests that CD133 is expressed in both colon CSCs and non-CSCs [22].However, the AC133 epitope reacts with the most frequently used anti-CD133 antibody and is detectedin CSCs, probably due to differential glycosylation [23]. The most precise marker of CSCs is the AC133epitope, not the CD133 protein. Thus, there are considerable discrepancies in available research results,based on the difference between these markers.
2.1.3. CD24
CD24, also known as heat stable antigen, is a B cell-related short glycoprotein whose expression isassociated with several types of cancer. The first report described this surface protein as a CSC markerin breast cancer [24]. CD24−/low cancer cell subpopulations with the CD44+ and/or ESA+ phenotypehave higher tumorigenic abilities compared to the CD24 positive counterpart. In contrast, positivity forCD24 is a CSC marker of ovarian and pancreatic cancer [25,26]. In colon cancer, clinical research studiesreport that expression of CD24 is associated with differentiation. Using immunohistochemical analysisof CD24 in colon cancer, two papers described contradictory significance of CD24 expression [27,28].These results suggest that CD24 plays a different role in each cancer type. To unveil the detailedmechanism of CD24 function in cancer, further investigation is necessary.
2.1.4. CD29
CD29, also known as integrin β1, is the most plentiful β subunit of integrin, a cell surface receptorthat assists adherence to the extracellular matrix, i.e., collagen, fibronectin, and laminin [29]. Integrin,which is an αβ heterodimer, is a structural linker between the cytoskeleton and extracellular matrix,as well as a mediator of transmembrane signaling. Various integrins are involved in diverse cellularprocesses such as adhesion, development, inflammation, and hemostasis.
High expression of CD29 is observed in normal stem cells in various organs. In colon, CD29 ishighly expressed in the lower part of the crypt, where stem and progenitor cells reside [30]. Conditionaldeletion of CD29 leads to hyperplasia and dysplasia in the intestinal epithelium, which is associated

Int. J. Mol. Sci. 2017, 18, 1446 4 of 14
with increased TCF4 signaling and decreased hedgehog signaling [31]. This suggests that CD29 is akey regulator of intestinal proliferation and maintenance by modulating specific signal transductionpathways. In addition, CD29 is gathering attention as a CSC marker that is related to chemoresistanceand metastasis, especially in breast cancer [32]. However, the significance of CD29 in colon cancer hasyet to be elucidated.
2.1.5. CD26
CD26, also known as dipeptidyl peptidase IV, is a multifunctional transmembrane protein withserine protease activity [33] that is a new drug target for type 2 diabetes [34]. Recently, Pang et al.demonstrated that the CD26+ subpopulation of colon cancer cells was able to both initiate tumorformation and metastasize to liver [35]. CD26 knockdown in CD26+ cells weakened their invasive,adherence, migration, and tumor formation abilities. This alteration was associated with the decreasedexpression of epithelial–mesenchymal transition (EMT)-related factors and phosphorylated integrinβ1(CD29), and was consistent with a previous report [36]. Of note, administration of chemotherapeuticagents reduced the tumor volume and enrichment of the CD26+ subpopulation in SCID mice. Takentogether, CD26 is a possible CSC marker to induce the EMT, and may collaborate with another CSCmarker, CD29. Consistent with these findings, clinical research has reported that expression of CD26 isrelated to a poor prognosis in colon cancer [37–39].
2.1.6. CD166
CD166, also known as activated leukocyte cell adhesion molecule, is an immunoglobulinsuperfamily member that is a ligand of CD6, a marker of T cells and thymocytes [40]. This surfaceprotein is associated with T cell activation as its name suggests, but its potential usefulness as a CSCmarker is also attracting interest. Dalerba et al. found that CD166 was an additional differentiallyexpressed marker for CSC isolation in colon cancer [41]. Further investigation revealed that CD166was expressed in mouse and human intestinal stem cells, and human colon adenocarcinoma [42].Interestingly, some colon cancer cells showed not only cytomembranous but also cytoplasmic positivityof CD166. Although meta-analyses of CD166 expression in colon cancer studies resulted in little clinicalsignificance [43,44], further study is needed to consider these distinctive expression patterns.
2.1.7. CD326
CD326, also known as an epithelial cell adhesion molecule, was first discovered as a specificantigen for human colon carcinoma [45]. This transmembrane protein affects multiple cellularprocesses, including proliferation, differentiation, and cell death, and is widely expressed in severaltypes of normal/benign and malignant epithelial cells [46].
Immunohistochemical analyses clarified that the expression of CD326 was associated with normalintestinal epithelium [47], and enhanced in malignancy [48]. Another immunohistochemical analysisestimated that CD326 expression in colon cancer occurred at a strong (>70% of tumor cells) and highfrequency (almost all cases of conventional human colon cancer) [49], suggesting that the single markerof CD326 in colon cancer is inappropriate to capture the “minor” population of tumor-initiating cells.However, recent evidence suggests that CD326 is a marker of the CSC phenotype [50]. In hepatocellularcarcinoma, CD326 is activated by canonical Wnt signaling and vice versa [51]. Considering theimportance of canonical Wnt signaling in both intestinal stemness and colon carcinogenesis, thefunctional significance of CD326 in colon cancer should be investigated.
2.2. An Active Intestinal Stem Cell Marker, Leucine-Rich Repeat-Containing G-Protein-CoupledReceptor 5 (Lgr5)
Examination of intestinal crypts is one of the most active research subjects of stem cell biology.Intestinal stem cells are thought to be active tissue stem cells that promote rapid turnover of intestinalepithelia to wash out cytotoxic factors from the daily diet. Cheng and Leblond identified intestinal

Int. J. Mol. Sci. 2017, 18, 1446 5 of 14
epithelial stem cells, which are also known as crypt base columnar cells (CBCs), in the bottom of mousesmall intestinal crypts by injecting 3H-thymidine [52]. This radiolabel pulse-chase experiment clearlydemonstrated that CBCs give rise to multiple types of differentiated cells by asymmetric cell division.
Lgr5 is the most established marker of active intestinal stem cells. Barkers and colleagues selectedLgr5 for analysis [53]. Lgr5 is a downstream target of the canonical Wnt pathway and appears to playan important role in maintaining stemness in the intestinal crypt. Consistent with the hypothesis,a transgenic mouse study demonstrated that expression of Lgr5 was confined to CBCs, which haveabilities of self-renewal and multipotency to differentiate. Although LGR5 was previously recognizedas an orphan receptor, it is now recognized as a Wnt enhancer that binds R-spondins [54]. Based onthe function of Lgr5 to enhance the canonical Wnt pathway, it is reasonable that LGR5 expressionin intestinal stem cells leads to the formation of an automatic amplification circuit to maintain theirstemness. Additional studies reported that isolated intestinal cells expressing Lgr5 show stem cellproperties, and a single cell was able to build intestinal organoids in 3D culture conditions [55].Collectively, Lgr5 is a definitive intestinal stem cell marker that governs the canonical Wnt pathway.
A relationship between Lgr5 expression and intestinal tumorigenesis has been reported. Wntactivation by an APC/β-catenin mutation is the initial step for intestinal tumorigenesis, which isalso known as the adenoma-carcinoma sequence [56]. Conditional deletion of Apc leads to cellulartransformation of not only stem cells but also progenitor cells in mice [57]. However, Ah-Cre expressingnon-stem intestinal cells are able to transform into dysplastic cells, but most of the lesions fail todevelop into intestinal neoplasia. In contrast, LGR5-GFP+ stem cells efficiently form adenomatouslesions with high expression of β-catenin and LGR5-GFP. This lineage tracing study suggests thatactive intestinal stem cells are suitable for originating intestinal tumor cells.
Further analysis of microadenomas elucidated that LGR5-expressing cells are mixed with Panethcells which are a stem cell niche in intestinal crypts. This suggests that a microenvironment likenormal intestinal crypts is necessary in the early stage of intestinal tumorigenesis [58]. In addition, amodel simulating an adenoma-carcinoma sequence has been reported using cell culture of intestinalorganoids [59,60]. These findings support a “bottom-up” model of intestinal carcinogenesis [61].However, counterevidence that indicates a “top-down” model also exists [62]. Schwitalla andcollaborators suggested that LGR5− intestinal cells have cell plasticity, which enabled them todedifferentiate into LGR5+ stem cells and give rise to tumor-initiating cells through Wnt activationmediated by NF-κB signaling [63].
2.3. Quiescent Intestinal Stem Cell Markers
Another fraction of intestinal stem cells is located at the +4 position counting Paneth cell nucleifrom the crypt bottom. The +4 position, which occurs directly above Paneth cells, contains DNAlabel-retaining cells, suggesting that these minor cells are long-lived and quiescent in nature [64].Buczacki et al. concluded that the intestinal label-retaining cells are secretory precursor cells arisingfrom LGR5-expressing stem cells, and give rise to LGR5-expressing cells for crypt regeneration andhomeostasis after severe injury [65].
Bmi1 (B lymphoma Mo-MLV insertion region 1, also known as polycomb group RING fingerprotein 4 or RING finger protein 51) was first identified in mouse lymphomagenesis [66]. Bmi1,a member of the polycomb group of genes, regulates proliferative activity in normal and cancerstem cells [67], and the multipotency of hematopoietic stem cells and multipotent progenitor cells, tosuppress transcriptional regulators for lineage differentiation [68]. In the intestine, expression of Bmi1corresponds to the +4 position of crypt cells. A study with transgenic mice demonstrated that Bmi1+
cells play a pivotal role in intestinal homeostasis and tumorigenesis [69]. Of note, Bmi1+ cells, as wellas label-retaining cells, give rise to Lgr5+ cells and maintain intestinal crypts after artificial ablation ofLgr5-expressing cells [70]. This suggests that BMI1+ cells are a stem cell source held in reserve in caseof critical damage of intestinal crypts.

Int. J. Mol. Sci. 2017, 18, 1446 6 of 14
Similarly, expression of BMI1 is important for the tumor-initiating and self-renewal abilities ofhuman colon cancer cells. Downregulation of BMI1 inhibits tumor cell growth, which is associatedwith a reduced fraction of tumor-initiating cells [71]. This suggests that the functional significance ofBMI1 is maintenance of stem cell properties in colon cancer cells. Consistent with this notion, clinicalstudies report that BMI1 expression is a negative predictor in colon cancer [72–75].
Other quiescent stem cell markers such as homeodomain-only protein (HOPX) [76],doublecortin-like kinase 1 (DCLK1) [77], telomerase reverse transcriptase (TERT) [78], and leucine-richrepeats and immunoglobulin-like domains protein 1 (LRIG1) [79] are associated with colontumorigenesis, but their detailed function and clinical significance remain unclear.
2.4. CSC Markers of Migration
Brabletz et al. proposed the migrating cancer stem cell (MCSC) concept that describes metastasis,which is the final step in the malignant process and the major cause of cancer patient mortality [80].MCSCs have not only stem cell characteristics but also a migratory phenotype that is induced by theEMT [81]. The EMT, and the reverse conversion, mesenchymal-epithelial transition, play essential rolesin embryonic development, tissue homeostasis, tissue recovery, and carcinogenesis. In cancer, the EMTis observed at the boundary between tumor and non-neoplastic tissues, indicating that acquisition ofmetastatic ability requires a specific microenvironment in addition to internal aberrant cell signaling.Cancer cells in the invasive front show strong nuclear β-catenin expression which activates EMT-relatedgenes through Wnt signaling [82]. Furthermore, extracellular matrix and secreted microenvironmentfactors also induce the EMT in these cancer cells [83,84].
Probable candidate markers for MCSCs include EMT inducers in addition to some of the cellsurface CSC markers. EMT inducers prompt the loss of E-cadherin, which is the initial step intransformation from the epithelial to mesenchymal phenotype [85]. However, it is difficult todifferentiate MCSC markers from EMT inducers because of the complex mechanism underlyingthe EMT. Further investigation is needed before clinical application of these EMT-related factors incolon cancer, as a previous systematic review recommended [86].
2.5. Side Population (SP) Cells
One method to identify CSCs is detection of the side population (SP), which is a minor populationof cells with the ability to extrude the DNA binding dye, Hoechst 33342. This exporting ability is dueto ATP-binding cassette (ABC) transporters that contribute to resistance to cytotoxic agents. Indeed,these transporters are found in many kinds of stem cells. Similarly, SP cells, which are detected inseveral types of human malignant tumors, generate both SP and non-SP cells and expel cytotoxicagents [87]. In human colon cancer cell lines, SP cells constitute 0.4% of total cancer cells [88] andexhibit resistance to chemotherapeutic agents [89].
An alternative method to identify the SP cell-like phenotype is the detection of ABC transporters.Some ABC transporters are induced in the hypoxic condition and play an important role in the survivalof cancer cells exposed to such an unfavorable microenvironment. Hypoxic cancer cells show resistanceto not only low oxygen concentrations, but also radiation and chemotherapy [90]. In addition to theirdrug efflux ability, ABC transporters are associated with other CSC properties including apoptosis,proliferation, differentiation, and cell migration [91]. Therefore, the microenvironment is a potentmodifier of the cancer cell phenotype, which leads to intratumoral heterogeneity.
In the ABC transporter family, ABCG2 (also known as BCRP or MXR), ABCC1 (also known asMRP1), and ABCB1 (also known as MDR1 or P-glycoprotein) are important in the efflux of anticancerdrugs. Immunohistochemical analysis revealed that expression of ABCC1 and ABCB1 is increased incolonic adenomas [92]. This suggests that the increased expression induces contradictory oncogeniceffects in adenoma cells, i.e., both increasing their survival activity and decreasing the potential foradditional mutations that would augment tumor progression. In colon cancer, expression of theABC transporters is related to drug resistance, which can be overcome by small interfering RNAs or

Int. J. Mol. Sci. 2017, 18, 1446 7 of 14
inhibitors of these pumps. Although many ABC transporter inhibitors are known to sensitize cancercells to chemotherapeutic agents in vitro, most clinical trials have failed to demonstrate any clinicalbenefit [93].
2.6. Aldehyde Dehydrogenase (ALDH) 1
ALDH1 is a member of the ALDH gene family that catalyzes the oxidation of aldehydes,including acetaldehyde and retinal (retinaldehyde) (detailed in [94]). Briefly, ALDH1, which isexpressed in various normal stem and/or progenitor cells, contributes to cell proliferation anddifferentiation through activation of retinoid signaling. In addition, ALDH1 has antioxidant propertiesto reduce reactive oxygen species arising from aldehydes. This detoxifying ability also applies to othercytotoxic factors.
High activity of ALDH1 has been identified as a CSC marker in various types of cancer, includingcolon cancer [41,95]. The expression of ALDH1 is detectable by an enzymatic assay [96] in additionto the conventional antibody-mediated method. However, this enzymatic assay is problematic interms of its specificity for different ALDH isoforms and misidentification of similar fluorescent signals.Nevertheless, understanding the functional role of ALDH1 in cancer is essential to develop newdiagnostic and therapeutic methods in clinical oncology.
2.7. Type III Deiodinase (D3)
Previous reports suggested that thyroid status influences the malignant process. An activeform of thyroid hormones, T3, is a transcription factor that controls cell metabolism, proliferation,differentiation, and apoptosis in several tissues [97]. Catalano and coworkers clarified the effect ofthyroid hormones in colon CSCs [98]. D3, which is a chief thyroid hormone inactivating enzyme,is strongly expressed in CD133+ Wnthigh colon cancer cells. In these cells, T3 signaling results inBMP4-mediated cellular differentiation while knockdown of D3 inhibits tumor formation. In addition,T3 treatment removes the chemoresistance of CSCs. These finding suggest that cancer progression isdue to not only local mutational events but also the general physiological state of the patient.
3. Stem Cell Phenotype in Colon Cancer: Emerging Evidence for Intertumoral Heterogeneity
Recent evidence has indicated that the stem cell phenotype in cancer applies not only tointratumoral heterogeneity but also intertumoral heterogeneity. Indeed, a comprehensive analysisrevealed that genomic and epigenetic alterations of colon cancer are both common and diverse [99].Moreover, the process of these alterations is not always accountable by the adenoma-carcinomasequence, suggesting that there must be intertumoral heterogeneity in colon cancer [100]. Because thedegree of stem cell marker expression varies with each colon cancer, this variation affects the biologicalbehavior of cancer cells.
Consistent with this notion, the intestinal stem cell signature predicts disease relapse of coloncancer [101]. However, low expression of Wnt target genes, including Lgr5 and Ascl2, indicates a moreimmature phenotype and worse prognosis in colon cancer compared with high Wnt groups [102].Interestingly, DNA methylation in these immature cells was found in the promoter of these genes. Thisfinding suggests that silencing of intestinal stem cell markers is an important step in colon carcinogenesisand that some intestinal stem cell markers maybe inappropriate as definitive CSC markers. It is alsonoted that colon cancer stem cells occur in a different context from normal intestinal epithelial cells.
Recently, a new colorectal cancer classification system was proposed based on the cellularphenotype analyzed by gene expression profiling [103]. Of the six classification subtypes, the stem-likesubgroup exhibited a good response to chemotherapy, whereas the goblet cell subgroup showed a poorresponse. Consistent with the evidence, our in vitro experiment clarified that a demethylating agentwas efficacious against colon cancer cell lines, especially in the stem-like subgroup [104]. This treatmentinduced goblet cell differentiation and reduced cell proliferation, suggesting that forced reduction ofDNA methylation diminishes stemness in cancer cells. Although the cancer phenotype is determined

Int. J. Mol. Sci. 2017, 18, 1446 8 of 14
by genetic and epigenetic alternations, epigenetic changes have a possible role in regulating cellulardifferentiation in cancer [105,106].
Thus, epigenetic alteration contributes to define the cancer cell phenotype, and detailed targets forthe alteration include the genes that regulate cellular differentiation. Our study found that CDX1, whichis considered a key transcriptional factor in intestinal differentiation, is silenced by hypermethylationin its promoter region [104]. However, knockdown of CDX1 failed to block the induction of gobletcell differentiation in colon cancer cell lines treated with a hypomethylating agent. On the other hand,Ordonez-Moran et al. demonstrated that retinoid therapy leads to cellular differentiation and tumorregression in colonic tumor through the reactivation of HOXA5 [95], which is a candidate target ofDNA hypermethylation in colon tumorigenesis [104]. Interestingly, knockdown of HOXA5 inhibitscellular differentiation in retinal-treated colon tumors, suggesting that HOXA5 is a candidate masterregulator of intestinal differentiation in colon cancer.
4. Conclusions
To date, many colorectal CSC marker candidates have been identified. It is reasonable thatthe various markers reflect the versatile nature of CSCs. Simultaneously, accumulating evidenceindicates that both normal and neoplastic cells show bidirectional conversion induced by internaland/or external signals. Currently, stem cells remain at the top of the hierarchy, but some are thoughtto originate from more highly differentiated subgroups. The bidirectional convertibility of cancerstemness explains why cancer is resistant to therapy, and raises questions about how to detect thetrue CSC population. Taking intertumoral heterogeneity into account, it is important to find the bestcombination of CSC and CSC-candidate markers rather than to search for a definitive single CSCmarker. In addition, identifying the master regulator of intestinal differentiation in colon cancer isessential for in vivo manipulation of colon cancer phenotype by epigenome editing techniques [107].
In vivo, genetic mutations are not currently correctable, whereas epigenetic changes are treatable.As mentioned above, epigenetic editing is a possible cancer treatment to block the restoration of cancerstemness. In the future, therapeutic targets may be extended to include not only cancer cells butalso their microenvironments and endocrine organs that affect the general condition of the patient(Figure 2). Therefore, further research is needed to understand the multifaceted traits of CSCs.
Int. J. Mol. Sci. 2017, 18, 1446 8 of 14
suggesting that forced reduction of DNA methylation diminishes stemness in cancer cells. Although the cancer phenotype is determined by genetic and epigenetic alternations, epigenetic changes have a possible role in regulating cellular differentiation in cancer [105,106].
Thus, epigenetic alteration contributes to define the cancer cell phenotype, and detailed targets for the alteration include the genes that regulate cellular differentiation. Our study found that CDX1, which is considered a key transcriptional factor in intestinal differentiation, is silenced by hypermethylation in its promoter region [104]. However, knockdown of CDX1 failed to block the induction of goblet cell differentiation in colon cancer cell lines treated with a hypomethylating agent. On the other hand, Ordonez-Moran et al. demonstrated that retinoid therapy leads to cellular differentiation and tumor regression in colonic tumor through the reactivation of HOXA5 [95], which is a candidate target of DNA hypermethylation in colon tumorigenesis [104]. Interestingly, knockdown of HOXA5 inhibits cellular differentiation in retinal-treated colon tumors, suggesting that HOXA5 is a candidate master regulator of intestinal differentiation in colon cancer.
4. Conclusions
To date, many colorectal CSC marker candidates have been identified. It is reasonable that the various markers reflect the versatile nature of CSCs. Simultaneously, accumulating evidence indicates that both normal and neoplastic cells show bidirectional conversion induced by internal and/or external signals. Currently, stem cells remain at the top of the hierarchy, but some are thought to originate from more highly differentiated subgroups. The bidirectional convertibility of cancer stemness explains why cancer is resistant to therapy, and raises questions about how to detect the true CSC population. Taking intertumoral heterogeneity into account, it is important to find the best combination of CSC and CSC-candidate markers rather than to search for a definitive single CSC marker. In addition, identifying the master regulator of intestinal differentiation in colon cancer is essential for in vivo manipulation of colon cancer phenotype by epigenome editing techniques [107].
In vivo, genetic mutations are not currently correctable, whereas epigenetic changes are treatable. As mentioned above, epigenetic editing is a possible cancer treatment to block the restoration of cancer stemness. In the future, therapeutic targets may be extended to include not only cancer cells but also their microenvironments and endocrine organs that affect the general condition of the patient (Figure 2). Therefore, further research is needed to understand the multifaceted traits of CSCs.
Figure 2. Cont.

Int. J. Mol. Sci. 2017, 18, 1446 9 of 14Int. J. Mol. Sci. 2017, 18, 1446 9 of 14
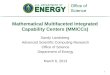
1 Figure 2. Conventional and prospective targets in cancer therapy: (A) Conventional therapy targets exclusively cancer cells without any distinction of cancer stemness. (B) On the other hand, prospective therapy involves microenvironment and endocrine status, which induce cancer stemness. Forced shrinking of cancer stem cell population by alteration of external signals is a possible approach for achieving complete response.
Acknowledgments: This study was supported by grants from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (Grant No. 15K11289 and 26430111).
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Kreso, A.; Dick, J.E. Evolution of the cancer stem cell model. Cell Stem Cell 2014, 14, 275–291. 2. Wicha, M.S.; Liu, S.; Dontu, G. Cancer stem cells: An old idea—A paradigm shift. Cancer Res. 2006, 66,
1883–1890. 3. Bonnet, D.; Dick, J.E. Human acute myeloid leukemia is organized as a hierarchy that originates from a
primitive hematopoietic cell. Nat. Med. 1997, 3, 730–737. 4. Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; de Maria, R.
Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. 5. World Cancer Report 2014; International Agency for Research on Cancer (IARC): Lyon, France, 2014. 6. Simmonds, P.C.; Primrose, J.N.; Colquitt, J.L.; Garden, O.J.; Poston, G.J.; Rees, M. Surgical resection of
hepatic metastases from colorectal cancer: A systematic review of published studies. Br. J. Cancer 2006, 94, 982–999.
7. Tirino, V.; Desiderio, V.; Paino, F.; Papaccio, G.; de Rosa, M. Methods for cancer stem cell detection and isolation. Methods Mol. Biol. 2012, 879, 513–529.
8. Yan, Y.; Zuo, X.; Wei, D. Concise review: Emerging role of CD44 in cancer stem cells: A promising biomarker and therapeutic target. Stem Cells Transl. Med. 2015, 4, 1033–1043.
9. Gunthert, U.; Hofmann, M.; Rudy, W.; Reber, S.; Zoller, M.; Haussmann, I.; Matzku, S.; Wenzel, A.; Ponta, H.; Herrlich, P. A new variant of glycoprotein CD44 confers metastatic potential to rat carcinoma cells. Cell 1991, 65, 13–24.
10. Herrlich, P.; Pals, S.; Ponta, H. CD44 in colon cancer. Eur. J. Cancer 1995, 31A, 1110–1112. 11. Wielenga, V.J.; Heider, K.H.; Offerhaus, G.J.; Adolf, G.R.; van den Berg, F.M.; Ponta, H.; Herrlich, P.; Pals,
S.T. Expression of CD44 variant proteins in human colorectal cancer is related to tumor progression. Cancer Res. 1993, 53, 4754–4756.
12. Mulder, J.W.; Kruyt, P.M.; Sewnath, M.; Oosting, J.; Seldenrijk, C.A.; Weidema, W.F.; Offerhaus, G.J.; Pals, S.T. Colorectal cancer prognosis and expression of exon-v6-containing CD44 proteins. Lancet 1994, 344, 1470–1472.
13. Orian-Rousseau, V.; Chen, L.; Sleeman, J.P.; Herrlich, P.; Ponta, H. CD44 is required for two consecutive steps in HGF/c-Met signaling. Genes Dev. 2002, 16, 3074–3086.
Figure 2. Conventional and prospective targets in cancer therapy: (A) Conventional therapy targetsexclusively cancer cells without any distinction of cancer stemness. (B) On the other hand, prospectivetherapy involves microenvironment and endocrine status, which induce cancer stemness. Forcedshrinking of cancer stem cell population by alteration of external signals is a possible approach forachieving complete response.
Acknowledgments: This study was supported by grants from the Ministry of Education, Culture, Sports, Science,and Technology of Japan (Grant No. 15K11289 and 26430111).
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Kreso, A.; Dick, J.E. Evolution of the cancer stem cell model. Cell Stem Cell 2014, 14, 275–291. [CrossRef][PubMed]
2. Wicha, M.S.; Liu, S.; Dontu, G. Cancer stem cells: An old idea—A paradigm shift. Cancer Res. 2006, 66,1883–1890. [CrossRef] [PubMed]
3. Bonnet, D.; Dick, J.E. Human acute myeloid leukemia is organized as a hierarchy that originates from aprimitive hematopoietic cell. Nat. Med. 1997, 3, 730–737. [CrossRef] [PubMed]
4. Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; de Maria, R. Identificationand expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [CrossRef] [PubMed]
5. World Cancer Report 2014; International Agency for Research on Cancer (IARC): Lyon, France, 2014.6. Simmonds, P.C.; Primrose, J.N.; Colquitt, J.L.; Garden, O.J.; Poston, G.J.; Rees, M. Surgical resection of hepatic
metastases from colorectal cancer: A systematic review of published studies. Br. J. Cancer 2006, 94, 982–999.[CrossRef] [PubMed]
7. Tirino, V.; Desiderio, V.; Paino, F.; Papaccio, G.; de Rosa, M. Methods for cancer stem cell detection andisolation. Methods Mol. Biol. 2012, 879, 513–529. [PubMed]
8. Yan, Y.; Zuo, X.; Wei, D. Concise review: Emerging role of CD44 in cancer stem cells: A promising biomarkerand therapeutic target. Stem Cells Transl. Med. 2015, 4, 1033–1043. [CrossRef] [PubMed]
9. Gunthert, U.; Hofmann, M.; Rudy, W.; Reber, S.; Zoller, M.; Haussmann, I.; Matzku, S.; Wenzel, A.; Ponta, H.;Herrlich, P. A new variant of glycoprotein CD44 confers metastatic potential to rat carcinoma cells. Cell 1991,65, 13–24. [CrossRef]
10. Herrlich, P.; Pals, S.; Ponta, H. CD44 in colon cancer. Eur. J. Cancer 1995, 31A, 1110–1112. [CrossRef]11. Wielenga, V.J.; Heider, K.H.; Offerhaus, G.J.; Adolf, G.R.; van den Berg, F.M.; Ponta, H.; Herrlich, P.; Pals, S.T.
Expression of CD44 variant proteins in human colorectal cancer is related to tumor progression. Cancer Res.1993, 53, 4754–4756. [PubMed]
12. Mulder, J.W.; Kruyt, P.M.; Sewnath, M.; Oosting, J.; Seldenrijk, C.A.; Weidema, W.F.; Offerhaus, G.J.; Pals, S.T.Colorectal cancer prognosis and expression of exon-v6-containing CD44 proteins. Lancet 1994, 344, 1470–1472.[CrossRef]

Int. J. Mol. Sci. 2017, 18, 1446 10 of 14
13. Orian-Rousseau, V.; Chen, L.; Sleeman, J.P.; Herrlich, P.; Ponta, H. CD44 is required for two consecutive stepsin HGF/c-Met signaling. Genes Dev. 2002, 16, 3074–3086. [CrossRef] [PubMed]
14. Tremmel, M.; Matzke, A.; Albrecht, I.; Laib, A.M.; Olaku, V.; Ballmer-Hofer, K.; Christofori, G.; Heroult, M.;Augustin, H.G.; Ponta, H.; et al. A CD44v6 peptide reveals a role of CD44 in VEGFR-2 signaling andangiogenesis. Blood 2009, 114, 5236–5244. [CrossRef] [PubMed]
15. Michieli, P.; Mazzone, M.; Basilico, C.; Cavassa, S.; Sottile, A.; Naldini, L.; Comoglio, P.M. Targeting the tumorand its microenvironment by a dual-function decoy met receptor. Cancer Cell 2004, 6, 61–73. [CrossRef][PubMed]
16. Cheng, C.; Yaffe, M.B.; Sharp, P.A. A positive feedback loop couples ras activation and CD44 alternativesplicing. Genes Dev. 2006, 20, 1715–1720. [CrossRef] [PubMed]
17. Ohata, H.; Ishiguro, T.; Aihara, Y.; Sato, A.; Sakai, H.; Sekine, S.; Taniguchi, H.; Akasu, T.; Fujita, S.;Nakagama, H.; et al. Induction of the stem-like cell regulator CD44 by rho kinase inhibition contributes tothe maintenance of colon cancer-initiating cells. Cancer Res. 2012, 72, 5101–5110. [CrossRef] [PubMed]
18. Li, Z. CD133: A stem cell biomarker and beyond. Exp. Hematol. Oncol. 2013, 2, 17. [CrossRef] [PubMed]19. Todaro, M.; Alea, M.P.; Di Stefano, A.B.; Cammareri, P.; Vermeulen, L.; Iovino, F.; Tripodo, C.; Russo, A.;
Gulotta, G.; Medema, J.P.; et al. Colon cancer stem cells dictate tumor growth and resist cell death byproduction of interleukin-4. Cell Stem Cell 2007, 1, 389–402. [CrossRef] [PubMed]
20. Vermeulen, L.; Todaro, M.; de Sousa Mello, F.; Sprick, M.R.; Kemper, K.; Perez Alea, M.; Richel, D.J.; Stassi, G.;Medema, J.P. Single-cell cloning of colon cancer stem cells reveals a multi-lineage differentiation capacity.Proc. Natl. Acad. Sci. USA 2008, 105, 13427–13432. [CrossRef] [PubMed]
21. Zhu, L.; Gibson, P.; Currle, D.S.; Tong, Y.; Richardson, R.J.; Bayazitov, I.T.; Poppleton, H.; Zakharenko, S.;Ellison, D.W.; Gilbertson, R.J. Prominin 1 marks intestinal stem cells that are susceptible to neoplastictransformation. Nature 2009, 457, 603–607. [CrossRef] [PubMed]
22. Shmelkov, S.V.; Butler, J.M.; Hooper, A.T.; Hormigo, A.; Kushner, J.; Milde, T.; St Clair, R.; Baljevic, M.;White, I.; Jin, D.K.; et al. CD133 expression is not restricted to stem cells, and both CD133+ and CD133−
metastatic colon cancer cells initiate tumors. J. Clin. Investig. 2008, 118, 2111–2120. [CrossRef] [PubMed]23. Kemper, K.; Sprick, M.R.; de Bree, M.; Scopelliti, A.; Vermeulen, L.; Hoek, M.; Zeilstra, J.; Pals, S.T.;
Mehmet, H.; Stassi, G.; et al. The AC133 epitope, but not the CD133 protein, is lost upon cancer stem celldifferentiation. Cancer Res. 2010, 70, 719–729. [CrossRef] [PubMed]
24. Al-Hajj, M.; Wicha, M.S.; Benito-Hernandez, A.; Morrison, S.J.; Clarke, M.F. Prospective identification oftumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 2003, 100, 3983–3988. [CrossRef] [PubMed]
25. Li, C.; Heidt, D.G.; Dalerba, P.; Burant, C.F.; Zhang, L.; Adsay, V.; Wicha, M.; Clarke, M.F.; Simeone, D.M.Identification of pancreatic cancer stem cells. Cancer Res. 2007, 67, 1030–1037. [CrossRef] [PubMed]
26. Gao, M.Q.; Choi, Y.P.; Kang, S.; Youn, J.H.; Cho, N.H. CD24+ cells from hierarchically organized ovariancancer are enriched in cancer stem cells. Oncogene 2010, 29, 2672–2680. [CrossRef] [PubMed]
27. Weichert, W.; Denkert, C.; Burkhardt, M.; Gansukh, T.; Bellach, J.; Altevogt, P.; Dietel, M.; Kristiansen, G.Cytoplasmic CD24 expression in colorectal cancer independently correlates with shortened patient survival.Clin. Cancer Res. 2005, 11, 6574–6581. [CrossRef] [PubMed]
28. Choi, D.; Lee, H.W.; Hur, K.Y.; Kim, J.J.; Park, G.S.; Jang, S.H.; Song, Y.S.; Jang, K.S.; Paik, S.S. Cancer stemcell markers CD133 and CD24 correlate with invasiveness and differentiation in colorectal adenocarcinoma.World J. Gastroenterol. 2009, 15, 2258–2264. [CrossRef] [PubMed]
29. Hynes, R.O. Integrins: Bidirectional, allosteric signaling machines. Cell 2002, 110, 673–687. [CrossRef]30. Fujimoto, K.; Beauchamp, R.D.; Whitehead, R.H. Identification and isolation of candidate human colonic
clonogenic cells based on cell surface integrin expression. Gastroenterology 2002, 123, 1941–1948. [CrossRef][PubMed]
31. Jones, R.G.; Li, X.; Gray, P.D.; Kuang, J.; Clayton, F.; Samowitz, W.S.; Madison, B.B.; Gumucio, D.L.;Kuwada, S.K. Conditional deletion of β1 integrins in the intestinal epithelium causes a loss of hedgehogexpression, intestinal hyperplasia, and early postnatal lethality. J. Cell Biol. 2006, 175, 505–514. [CrossRef][PubMed]
32. Hamidi, H.; Pietila, M.; Ivaska, J. The complexity of integrins in cancer and new scopes for therapeutictargeting. Br. J. Cancer 2016, 115, 1017–1023. [CrossRef] [PubMed]

Int. J. Mol. Sci. 2017, 18, 1446 11 of 14
33. Misumi, Y.; Hayashi, Y.; Arakawa, F.; Ikehara, Y. Molecular cloning and sequence analysis of humandipeptidyl peptidase iv, a serine proteinase on the cell surface. Biochim. Biophys. Acta 1992, 1131, 333–336.[CrossRef]
34. Drucker, D.J.; Nauck, M.A. The incretin system: Glucagon-like peptide-1 receptor agonists and dipeptidylpeptidase-4 inhibitors in type 2 diabetes. Lancet 2006, 368, 1696–1705. [CrossRef]
35. Pang, R.; Law, W.L.; Chu, A.C.; Poon, J.T.; Lam, C.S.; Chow, A.K.; Ng, L.; Cheung, L.W.; Lan, X.R.; Lan, H.Y.;et al. A subpopulation of CD26+ cancer stem cells with metastatic capacity in human colorectal cancer.Cell Stem Cell 2010, 6, 603–615. [CrossRef] [PubMed]
36. Sato, T.; Yamochi, T.; Yamochi, T.; Aytac, U.; Ohnuma, K.; McKee, K.S.; Morimoto, C.; Dang, N.H. CD26regulates p38 mitogen-activated protein kinase-dependent phosphorylation of integrin β1, adhesion toextracellular matrix, and tumorigenicity of T-anaplastic large cell lymphoma Karpas 299. Cancer Res. 2005,65, 6950–6956. [CrossRef] [PubMed]
37. de la Haba-Rodriguez, J.; Macho, A.; Calzado, M.A.; Blazquez, M.V.; Gomez, M.A.; Munoz, E.E.; Aranda, E.Soluble dipeptidyl peptidase IV (CD-26) in serum of patients with colorectal carcinoma. Neoplasma 2002, 49,307–311. [PubMed]
38. Lam, C.S.; Cheung, A.H.; Wong, S.K.; Wan, T.M.; Ng, L.; Chow, A.K.; Cheng, N.S.; Pak, R.C.; Li, H.S.;Man, J.H.; et al. Prognostic significance of CD26 in patients with colorectal cancer. PLoS ONE 2014, 9, e98582.[CrossRef] [PubMed]
39. Lieto, E.; Galizia, G.; Orditura, M.; Romano, C.; Zamboli, A.; Castellano, P.; Mabilia, A.; Auricchio, A.;F, D.E.V.; Gemei, M. CD26-positive/CD326-negative circulating cancer cells as prognostic markers forcolorectal cancer recurrence. Oncol. Lett. 2015, 9, 542–550. [CrossRef] [PubMed]
40. Bowen, M.A.; Patel, D.D.; Li, X.; Modrell, B.; Malacko, A.R.; Wang, W.C.; Marquardt, H.; Neubauer, M.;Pesando, J.M.; Francke, U.; et al. Cloning, mapping, and characterization of activated leukocyte-cell adhesionmolecule (ALCAM), a CD6 ligand. J. Exp. Med. 1995, 181, 2213–2220. [CrossRef] [PubMed]
41. Dalerba, P.; Dylla, S.J.; Park, I.K.; Liu, R.; Wang, X.; Cho, R.W.; Hoey, T.; Gurney, A.; Huang, E.H.;Simeone, D.M.; et al. Phenotypic characterization of human colorectal cancer stem cells. Proc. Natl.Acad. Sci. USA 2007, 104, 10158–10163. [CrossRef] [PubMed]
42. Levin, T.G.; Powell, A.E.; Davies, P.S.; Silk, A.D.; Dismuke, A.D.; Anderson, E.C.; Swain, J.R.; Wong, M.H.Characterization of the intestinal cancer stem cell marker CD166 in the human and mouse gastrointestinaltract. Gastroenterology 2010, 139, 2072–2082. [CrossRef] [PubMed]
43. Ni, C.; Zhang, Z.; Zhu, X.; Liu, Y.; Qu, D.; Wu, P.; Huang, J.; Xu, A.X. Prognostic value of CD166 expressionin cancers of the digestive system: A systematic review and meta-analysis. PLoS ONE 2013, 8, e70958.[CrossRef] [PubMed]
44. Han, S.; Yang, W.; Zong, S.; Li, H.; Liu, S.; Li, W.; Shi, Q.; Hou, F. Clinicopathological, prognostic andpredictive value of CD166 expression in colorectal cancer: A meta-analysis. Oncotarget 2017. [CrossRef][PubMed]
45. Litvinov, S.V.; Velders, M.P.; Bakker, H.A.; Fleuren, G.J.; Warnaar, S.O. Ep-CAM: A human epithelial antigenis a homophilic cell-cell adhesion molecule. J. Cell Biol. 1994, 125, 437–446. [CrossRef] [PubMed]
46. Winter, M.J.; Nagtegaal, I.D.; van Krieken, J.H.; Litvinov, S.V. The epithelial cell adhesion molecule (Ep-CAM)as a morphoregulatory molecule is a tool in surgical pathology. Am. J. Pathol. 2003, 163, 2139–2148. [CrossRef]
47. Balzar, M.; Prins, F.A.; Bakker, H.A.; Fleuren, G.J.; Warnaar, S.O.; Litvinov, S.V. The structural analysis ofadhesions mediated by Ep-CAM. Exp. Cell. Res. 1999, 246, 108–121. [CrossRef] [PubMed]
48. Salem, R.R.; Wolf, B.C.; Sears, H.F.; Lavin, P.T.; Ravikumar, T.S.; DeCoste, D.; D’Emilia, J.C.; Herlyn, M.;Schlom, J.; Gottlieb, L.S.; et al. Expression of colorectal carcinoma-associated antigens in colonic polyps.J. Surg. Res. 1993, 55, 249–255. [CrossRef] [PubMed]
49. Went, P.; Vasei, M.; Bubendorf, L.; Terracciano, L.; Tornillo, L.; Riede, U.; Kononen, J.; Simon, R.; Sauter, G.;Baeuerle, P.A. Frequent high-level expression of the immunotherapeutic target Ep-CAM in colon, stomach,prostate and lung cancers. Br. J. Cancer 2006, 94, 128–135. [CrossRef] [PubMed]
50. Munz, M.; Baeuerle, P.A.; Gires, O. The emerging role of epcam in cancer and stem cell signaling. Cancer Res.2009, 69, 5627–5629. [CrossRef] [PubMed]
51. Yamashita, T.; Budhu, A.; Forgues, M.; Wang, X.W. Activation of hepatic stem cell marker epcam byWnt-β-catenin signaling in hepatocellular carcinoma. Cancer Res. 2007, 67, 10831–10839. [CrossRef][PubMed]

Int. J. Mol. Sci. 2017, 18, 1446 12 of 14
52. Cheng, H.; Leblond, C.P. Origin, differentiation and renewal of the four main epithelial cell types in themouse small intestine. V. Unitarian theory of the origin of the four epithelial cell types. Am. J. Anat. 1974,141, 537–561. [CrossRef] [PubMed]
53. Barker, N.; van Es, J.H.; Kuipers, J.; Kujala, P.; van den Born, M.; Cozijnsen, M.; Haegebarth, A.; Korving, J.;Begthel, H.; Peters, P.J.; et al. Identification of stem cells in small intestine and colon by marker gene Lgr5.Nature 2007, 449, 1003–1007. [CrossRef] [PubMed]
54. Carmon, K.S.; Gong, X.; Lin, Q.; Thomas, A.; Liu, Q. R-spondins function as ligands of the orphan receptorsLgr4 and Lgr5 to regulate Wnt/β-catenin signaling. Proc. Natl. Acad. Sci. USA 2011, 108, 11452–11457.[CrossRef] [PubMed]
55. Sato, T.; Vries, R.G.; Snippert, H.J.; van de Wetering, M.; Barker, N.; Stange, D.E.; van Es, J.H.; Abo, A.;Kujala, P.; Peters, P.J.; et al. Single Lgr5 stem cells build crypt-villus structures in vitro without a mesenchymalniche. Nature 2009, 459, 262–265. [CrossRef] [PubMed]
56. Fearon, E.R.; Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell 1990, 61, 759–767. [CrossRef]57. Barker, N.; Ridgway, R.A.; van Es, J.H.; van de Wetering, M.; Begthel, H.; van den Born, M.; Danenberg, E.;
Clarke, A.R.; Sansom, O.J.; Clevers, H. Crypt stem cells as the cells-of-origin of intestinal cancer. Nature 2009,457, 608–611. [CrossRef] [PubMed]
58. Schepers, A.G.; Snippert, H.J.; Stange, D.E.; van den Born, M.; van Es, J.H.; van de Wetering, M.; Clevers, H.Lineage tracing reveals lgr5+ stem cell activity in mouse intestinal adenomas. Science 2012, 337, 730–735.[CrossRef] [PubMed]
59. Drost, J.; van Jaarsveld, R.H.; Ponsioen, B.; Zimberlin, C.; van Boxtel, R.; Buijs, A.; Sachs, N.; Overmeer, R.M.;Offerhaus, G.J.; Begthel, H.; et al. Sequential cancer mutations in cultured human intestinal stem cells. Nature2015, 521, 43–47. [CrossRef] [PubMed]
60. Matano, M.; Date, S.; Shimokawa, M.; Takano, A.; Fujii, M.; Ohta, Y.; Watanabe, T.; Kanai, T.; Sato, T. Modelingcolorectal cancer using CRISPR-Cas9-mediated engineering of human intestinal organoids. Nat. Med. 2015,21, 256–262. [CrossRef] [PubMed]
61. Preston, S.L.; Wong, W.M.; Chan, A.O.; Poulsom, R.; Jeffery, R.; Goodlad, R.A.; Mandir, N.; Elia, G.;Novelli, M.; Bodmer, W.F.; et al. Bottom-up histogenesis of colorectal adenomas: Origin in the monocryptaladenoma and initial expansion by crypt fission. Cancer Res. 2003, 63, 3819–3825. [PubMed]
62. Shih, I.M.; Wang, T.L.; Traverso, G.; Romans, K.; Hamilton, S.R.; Ben-Sasson, S.; Kinzler, K.W.; Vogelstein, B.Top-down morphogenesis of colorectal tumors. Proc. Natl. Acad. Sci. USA 2001, 98, 2640–2645. [CrossRef][PubMed]
63. Schwitalla, S.; Fingerle, A.A.; Cammareri, P.; Nebelsiek, T.; Goktuna, S.I.; Ziegler, P.K.; Canli, O.; Heijmans, J.;Huels, D.J.; Moreaux, G.; et al. Intestinal tumorigenesis initiated by dedifferentiation and acquisition ofstem-cell-like properties. Cell 2013, 152, 25–38. [CrossRef] [PubMed]
64. Potten, C.S. Extreme sensitivity of some intestinal crypt cells to X and γ irradiation. Nature 1977, 269, 518–521.[CrossRef] [PubMed]
65. Buczacki, S.J.; Zecchini, H.I.; Nicholson, A.M.; Russell, R.; Vermeulen, L.; Kemp, R.; Winton, D.J. Intestinallabel-retaining cells are secretory precursors expressing Lgr5. Nature 2013, 495, 65–69. [CrossRef] [PubMed]
66. Haupt, Y.; Alexander, W.S.; Barri, G.; Klinken, S.P.; Adams, J.M. Novel zinc finger gene implicated as myccollaborator by retrovirally accelerated lymphomagenesis in Eµ-myc transgenic mice. Cell 1991, 65, 753–763.[CrossRef]
67. Lessard, J.; Sauvageau, G. Bmi-1 determines the proliferative capacity of normal and leukaemic stem cells.Nature 2003, 423, 255–260. [CrossRef] [PubMed]
68. Oguro, H.; Yuan, J.; Ichikawa, H.; Ikawa, T.; Yamazaki, S.; Kawamoto, H.; Nakauchi, H.; Iwama, A. Poisedlineage specification in multipotential hematopoietic stem and progenitor cells by the polycomb proteinBmi1. Cell Stem Cell 2010, 6, 279–286. [CrossRef] [PubMed]
69. Sangiorgi, E.; Capecchi, M.R. Bmi1 is expressed in vivo in intestinal stem cells. Nat. Genet. 2008, 40, 915–920.[CrossRef] [PubMed]
70. Tian, H.; Biehs, B.; Warming, S.; Leong, K.G.; Rangell, L.; Klein, O.D.; de Sauvage, F.J. A reserve stem cellpopulation in small intestine renders Lgr5-positive cells dispensable. Nature 2011, 478, 255–259. [CrossRef][PubMed]

Int. J. Mol. Sci. 2017, 18, 1446 13 of 14
71. Kreso, A.; van Galen, P.; Pedley, N.M.; Lima-Fernandes, E.; Frelin, C.; Davis, T.; Cao, L.; Baiazitov, R.; Du, W.;Sydorenko, N.; et al. Self-renewal as a therapeutic target in human colorectal cancer. Nat. Med. 2014, 20,29–36. [CrossRef] [PubMed]
72. Tateishi, K.; Ohta, M.; Kanai, F.; Guleng, B.; Tanaka, Y.; Asaoka, Y.; Tada, M.; Seto, M.; Jazag, A.; Lianjie, L.;et al. Dysregulated expression of stem cell factor bmi1 in precancerous lesions of the gastrointestinal tract.Clin. Cancer Res. 2006, 12, 6960–6966. [CrossRef] [PubMed]
73. Du, J.; Li, Y.; Li, J.; Zheng, J. Polycomb group protein Bmi1 expression in colon cancers predicts the survival.Med. Oncol. 2010, 27, 1273–1276. [CrossRef] [PubMed]
74. Li, D.W.; Tang, H.M.; Fan, J.W.; Yan, D.W.; Zhou, C.Z.; Li, S.X.; Wang, X.L.; Peng, Z.H. Expression level ofBmi-1 oncoprotein is associated with progression and prognosis in colon cancer. J. Cancer Res. Clin. Oncol.2010, 136, 997–1006. [CrossRef] [PubMed]
75. Pun, J.C.; Chan, J.Y.; Chun, B.K.; Ng, K.W.; Tsui, S.Y.; Wan, T.M.; Lo, O.; Poon, J.T.; Ng, L.; Pang, R.Plasma Bmi1 mRNA as a potential prognostic biomarker for distant metastasis in colorectal cancer patients.Mol. Clin. Oncol. 2014, 2, 817–820. [CrossRef] [PubMed]
76. Yamashita, K.; Katoh, H.; Watanabe, M. The homeobox only protein homeobox (HOPX) and colorectal cancer.Int. J. Mol. Sci. 2013, 14, 23231–23243. [CrossRef] [PubMed]
77. May, R.; Riehl, T.E.; Hunt, C.; Sureban, S.M.; Anant, S.; Houchen, C.W. Identification of a novel putativegastrointestinal stem cell and adenoma stem cell marker, doublecortin and CaM kinase-like-1, followingradiation injury and in adenomatous polyposis coli/multiple intestinal neoplasia mice. Stem Cells 2008, 26,630–637. [CrossRef] [PubMed]
78. Montgomery, R.K.; Carlone, D.L.; Richmond, C.A.; Farilla, L.; Kranendonk, M.E.; Henderson, D.E.;Baffour-Awuah, N.Y.; Ambruzs, D.M.; Fogli, L.K.; Algra, S.; et al. Mouse telomerase reverse transcriptase(mTert) expression marks slowly cycling intestinal stem cells. Proc. Natl. Acad. Sci. USA 2011, 108, 179–184.[CrossRef] [PubMed]
79. Powell, A.E.; Wang, Y.; Li, Y.; Poulin, E.J.; Means, A.L.; Washington, M.K.; Higginbotham, J.N.; Juchheim, A.;Prasad, N.; Levy, S.E.; et al. The Pan-ErbB negative regulator Lrig1 is an intestinal stem cell marker thatfunctions as a tumor suppressor. Cell 2012, 149, 146–158. [CrossRef] [PubMed]
80. Brabletz, T.; Jung, A.; Spaderna, S.; Hlubek, F.; Kirchner, T. Opinion: Migrating cancer stem cells — Anintegrated concept of malignant tumour progression. Nat. Rev. Cancer 2005, 5, 744–749. [CrossRef] [PubMed]
81. Thiery, J.P.; Acloque, H.; Huang, R.Y.; Nieto, M.A. Epithelial-mesenchymal transitions in development anddisease. Cell 2009, 139, 871–890. [CrossRef] [PubMed]
82. Conacci-Sorrell, M.; Simcha, I.; Ben-Yedidia, T.; Blechman, J.; Savagner, P.; Ben-Ze’ev, A. Autoregulation ofE-cadherin expression by cadherin-cadherin interactions: The roles of β-catenin signaling, slug, and mapk.J. Cell Biol. 2003, 163, 847–857. [CrossRef] [PubMed]
83. Muller, T.; Bain, G.; Wang, X.; Papkoff, J. Regulation of epithelial cell migration and tumor formation byβ-catenin signaling. Exp. Cell Res. 2002, 280, 119–133. [CrossRef] [PubMed]
84. Eger, A.; Stockinger, A.; Park, J.; Langkopf, E.; Mikula, M.; Gotzmann, J.; Mikulits, W.; Beug, H.; Foisner, R.β-catenin and TGFβ signalling cooperate to maintain a mesenchymal phenotype after foser-inducedepithelial to mesenchymal transition. Oncogene 2004, 23, 2672–2680. [CrossRef] [PubMed]
85. De Craene, B.; Berx, G. Regulatory networks defining EMT during cancer initiation and progression.Nat. Rev. Cancer 2013, 13, 97–110. [CrossRef] [PubMed]
86. Busch, E.L.; McGraw, K.A.; Sandler, R.S. The potential for markers of epithelial-mesenchymal transitionto improve colorectal cancer outcomes: A systematic review. Cancer Epidemiol. Biomark. Prev. 2014, 23,1164–1175. [CrossRef] [PubMed]
87. Hirschmann-Jax, C.; Foster, A.E.; Wulf, G.G.; Nuchtern, J.G.; Jax, T.W.; Gobel, U.; Goodell, M.A.; Brenner, M.K.A distinct “side population” of cells with high drug efflux capacity in human tumor cells. Proc. Natl. Acad.Sci. USA 2004, 101, 14228–14233. [CrossRef] [PubMed]
88. Haraguchi, N.; Utsunomiya, T.; Inoue, H.; Tanaka, F.; Mimori, K.; Barnard, G.F.; Mori, M. Characterization ofa side population of cancer cells from human gastrointestinal system. Stem Cells 2006, 24, 506–513. [CrossRef][PubMed]
89. Xiong, B.; Ma, L.; Hu, X.; Zhang, C.; Cheng, Y. Characterization of side population cells isolated from thecolon cancer cell line SW480. Int J. Oncol. 2014, 45, 1175–1183. [CrossRef] [PubMed]

Int. J. Mol. Sci. 2017, 18, 1446 14 of 14
90. Brown, J.M. The hypoxic cell: A target for selective cancer therapy—Eighteenth Bruce F. Cain memorialaward lecture. Cancer Res. 1999, 59, 5863–5870. [PubMed]
91. Fletcher, J.I.; Haber, M.; Henderson, M.J.; Norris, M.D. Abc transporters in cancer: More than just drug effluxpumps. Nat. Rev. Cancer 2010, 10, 147–156. [CrossRef] [PubMed]
92. Meijer, G.A.; Schroeijers, A.B.; Flens, M.J.; Meuwissen, S.G.; van der Valk, P.; Baak, J.P.; Scheper, R.J. Increasedexpression of multidrug resistance related proteins Pgp, MRP1, and LRP/MVP occurs early in colorectalcarcinogenesis. J. Clin. Pathol. 1999, 52, 450–454. [CrossRef] [PubMed]
93. Yu, M.; Ocana, A.; Tannock, I.F. Reversal of ATP-binding cassette drug transporter activity to modulatechemoresistance: Why has it failed to provide clinical benefit? Cancer Metastasis Rev. 2013, 32, 211–227.[CrossRef] [PubMed]
94. Tomita, H.; Tanaka, K.; Tanaka, T.; Hara, A. Aldehyde dehydrogenase 1A1 in stem cells and cancer. Oncotarget2016, 7, 11018–11032. [PubMed]
95. Ordonez-Moran, P.; Dafflon, C.; Imajo, M.; Nishida, E.; Huelsken, J. HOXA5 counteracts stem cell traits byinhibiting Wnt signaling in colorectal cancer. Cancer Cell 2015, 28, 815–829. [CrossRef] [PubMed]
96. Dolle, L.; Boulter, L.; Leclercq, I.A.; van Grunsven, L.A. Next generation of aldh substrates and their potentialto study maturational lineage biology in stem and progenitor cells. Am. J. Physiol. Gastrointest. Liver Physiol.2015, 308, G573–G578. [CrossRef] [PubMed]
97. Sirakov, M.; Skah, S.; Nadjar, J.; Plateroti, M. Thyroid hormone’s action on progenitor/stem cell biology:New challenge for a classic hormone? Biochim. Biophys. Acta 2013, 1830, 3917–3927. [CrossRef] [PubMed]
98. Catalano, V.; Dentice, M.; Ambrosio, R.; Luongo, C.; Carollo, R.; Benfante, A.; Todaro, M.; Stassi, G.;Salvatore, D. Activated thyroid hormone promotes differentiation and chemotherapeutic sensitizationof colorectal cancer stem cells by regulating Wnt and Bmp4 signaling. Cancer Res. 2016, 76, 1237–1244.[CrossRef] [PubMed]
99. Cancer Genome Atlas, N. Comprehensive molecular characterization of human colon and rectal cancer.Nature 2012, 487, 330–337.
100. De Sousa, E.M.F.; Wang, X.; Jansen, M.; Fessler, E.; Trinh, A.; de Rooij, L.P.; de Jong, J.H.; de Boer, O.J.;van Leersum, R.; Bijlsma, M.F.; et al. Poor-prognosis colon cancer is defined by a molecularly distinctsubtype and develops from serrated precursor lesions. Nat. Med. 2013, 19, 614–618. [CrossRef] [PubMed]
101. Merlos-Suarez, A.; Barriga, F.M.; Jung, P.; Iglesias, M.; Cespedes, M.V.; Rossell, D.; Sevillano, M.;Hernando-Momblona, X.; da Silva-Diz, V.; Munoz, P.; et al. The intestinal stem cell signature identifiescolorectal cancer stem cells and predicts disease relapse. Cell Stem Cell 2011, 8, 511–524. [CrossRef] [PubMed]
102. de Sousa, E.M.F.; Colak, S.; Buikhuisen, J.; Koster, J.; Cameron, K.; de Jong, J.H.; Tuynman, J.B.;Prasetyanti, P.R.; Fessler, E.; van den Bergh, S.P.; et al. Methylation of cancer-stem-cell-associated Wnttarget genes predicts poor prognosis in colorectal cancer patients. Cell Stem Cell 2011, 9, 476–485.
103. Sadanandam, A.; Lyssiotis, C.A.; Homicsko, K.; Collisson, E.A.; Gibb, W.J.; Wullschleger, S.; Ostos, L.C.;Lannon, W.A.; Grotzinger, C.; del Rio, M.; et al. A colorectal cancer classification system that associatescellular phenotype and responses to therapy. Nat. Med. 2013, 19, 619–625. [CrossRef] [PubMed]
104. Hatano, Y.; Semi, K.; Hashimoto, K.; Lee, M.S.; Hirata, A.; Tomita, H.; Kuno, T.; Takamatsu, M.; Aoki, K.;Taketo, M.M.; et al. Reducing DNA methylation suppresses colon carcinogenesis by inducing tumor celldifferentiation. Carcinogenesis 2015, 36, 719–729. [CrossRef] [PubMed]
105. Matsuda, Y.; Semi, K.; Yamada, Y. Application of iPS cell technology to cancer epigenome study: Uncoveringthe mechanism of cell status conversion for drug resistance in tumor. Pathol. Int. 2014, 64, 299–308. [CrossRef][PubMed]
106. Hashimoto, K.; Yamada, Y.; Semi, K.; Yagi, M.; Tanaka, A.; Itakura, F.; Aoki, H.; Kunisada, T.; Woltjen, K.;Haga, H.; et al. Cellular context-dependent consequences of Apc mutations on gene regulation and cellularbehavior. Proc. Natl. Acad. Sci. USA 2017, 114, 758–763. [CrossRef] [PubMed]
107. Srivastava, D.; DeWitt, N. In vivo cellular reprogramming: The next generation. Cell 2016, 166, 1386–1396.[CrossRef] [PubMed]
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open accessarticle distributed under the terms and conditions of the Creative Commons Attribution(CC BY) license (http://creativecommons.org/licenses/by/4.0/).