Embed Size (px)
Citation preview
MULLIGAN’SMobilisation with
Movement:
The science, theevidence and
the art.
Bill VicenzinoProfessor in Sports Physiotherapy
Head of Division of Physiotherapy
The science, the evidenceand the art .
MULLIGAN’SMobilisation with
Movement:
Mobilisation With Movement =
sustained force (accessory glide)while a previously painful
(problematic) movement is performed
or ?
Mobilisation With Movement =
discern and measure problem movement
apply glide &repeat problem movement
repeat iteration (max 4 times) &observe outcome
or ?
Mobilisation With Movement =
only used in treatment plan if thepreviously painful (problematic)movement is much/substantially
improved
& !
Sunday: 1:00 – 1:30 Dr Darren Rivett: MWM and clinical reasoning
…so what is the evidence?
THIS CONFERENCE!!!
Next … Hewitt - MWM: A systematic, critical narrative review.
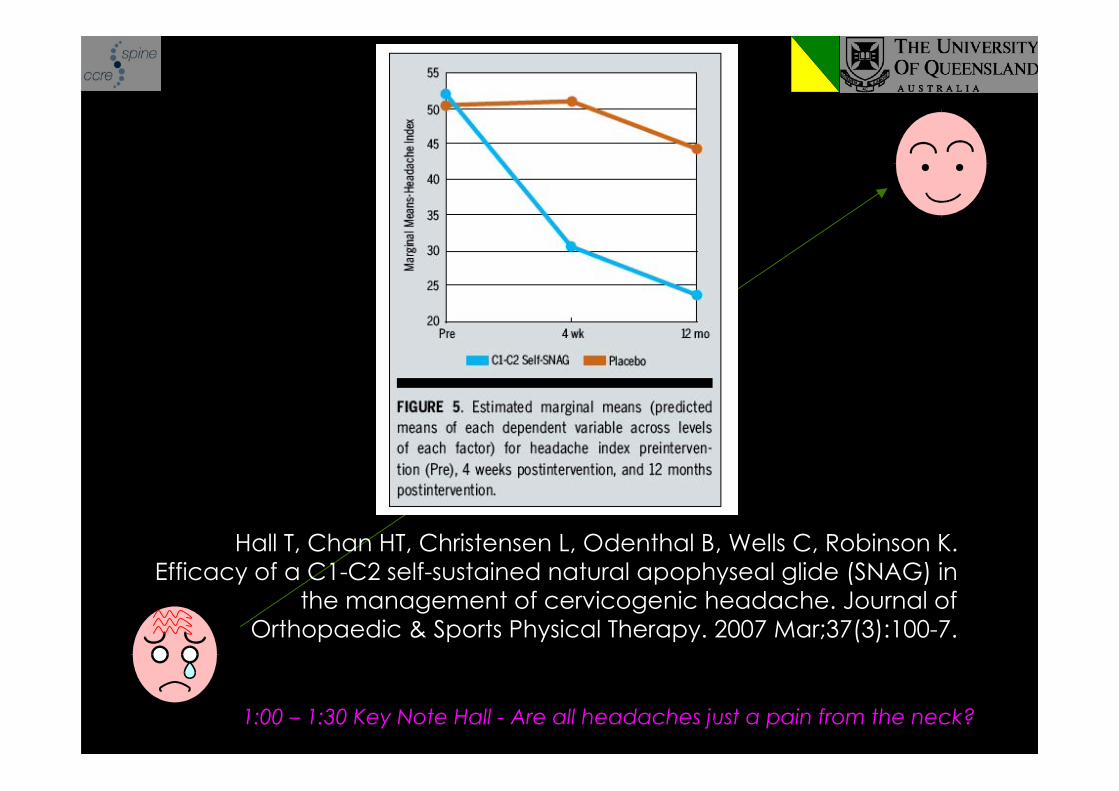
Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K.Efficacy of a C1-C2 self-sustained natural apophyseal glide (SNAG) in
the management of cervicogenic headache. Journal ofOrthopaedic & Sports Physical Therapy. 2007 Mar;37(3):100-7.
1:00 – 1:30 Key Note Hall - Are all headaches just a pain from the neck?
Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. MWM andexercise, corticosteroid injection, or wait & see for tennis elbow:
randomised trial. BMJ 2006, doi:10.1136/bmj.38961.584653.AE
MWM + exercise speeds up recoveryReduces need for other therapiesFewer recurrences than steroid injections in long term
2:00 - 2:30 MWM for soft tissue injuries such as tennis elbow
MWM works!
THIS CONFERENCE!!!
Next … Hewitt - MWM: A systematic, critical narrative review.
How does it work?
or
What do you tell your patients?
Biomechanical
Boney luxations
Reversing luxations
• Straighten spine (Pare 1958)
• Unlocking locked joint(Twomey 1992)
• Shift an IVD fragment (Cyriax1975)
• Reduce annular distortion(Farfan 1973)
• Stretching, tearing or rupturingadhesions that limit joint ornerve range (Zusman 1986,Chrisman et al 1964)
• Remove blockage orinterference of blood flow (Still1899), nerve compression(Palmer 1910), sympatheticchain (Kunert 1965), andcerebrospinal fluid circulation(DeJanette 1967)
Biomechanical
Neurophysiological
Paradigms in practice/research
• Correct abnormalsomatovisceral reflexes andvisceral organ dysfunction(Dhami & DeBoer 1992)
• Stretch contracted muscles,causing relaxation (Perl 1975)
• Remove ‘irrtable’ spinal lesions(Korr 1976)
• Intense reflex effects (mainlymusculature, Lewit 1985)
• Modulate peripheralnociceptors (Zusman 1987)
• Inhibition of reflex musclecontraction (Zusman 1987)
• Activates gating mechanism,neurotransmitters, opioidepeptides (Dhami and DeBoer1992)
Neurophysiological
Biomechanical
Neurophysiological
MWM
Paradigms in practice/research
Biomechanical
MWM
Positional fault hypothesis
Sunday:10.30 – 11:00 Key Note Wayne Hing - Positional Fault – Fact or Fiction
O’Brien & Vicenzino (1998) A study of effectsof a MWM for lateral ankle pain using a casestudy design. Manual Therapy 3: 78-84.
4.5 cm PVAS reduction following 1 treatment
7.4 units/day on Kaikkonen scale withtreatment over 5 weeks compared to 1.4units/day with natural resolution
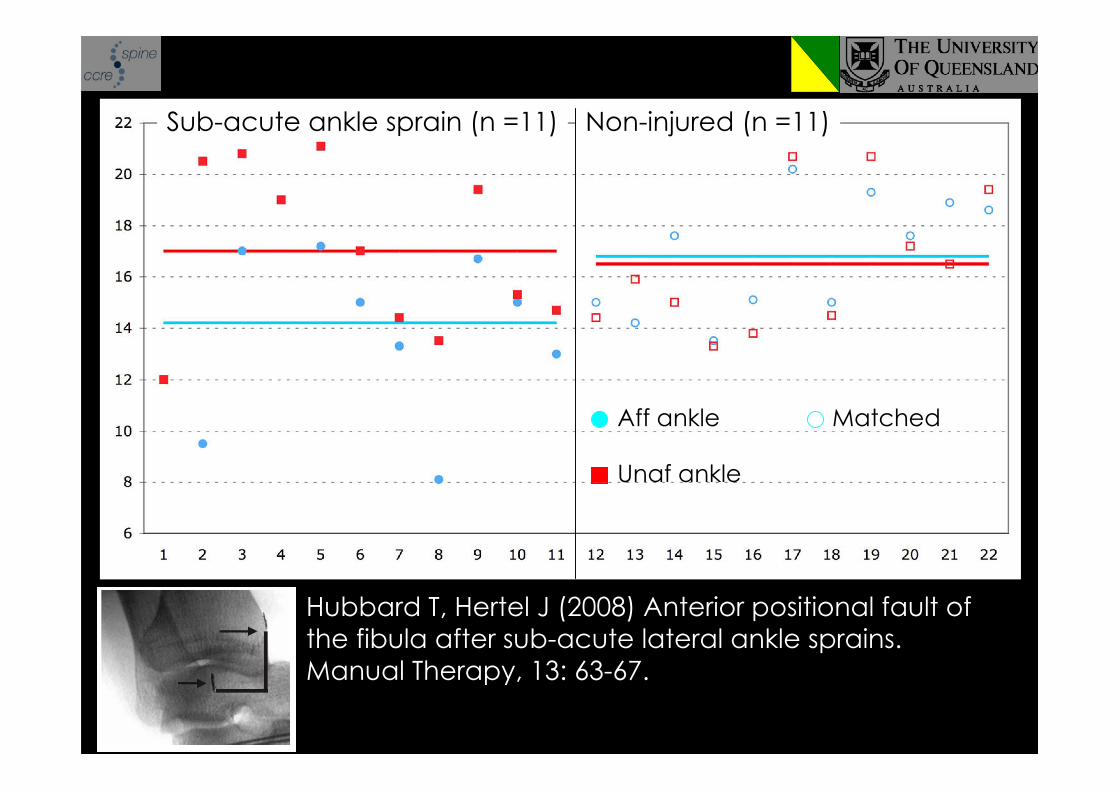
Hubbard T, Hertel J (2008) Anterior positional fault ofthe fibula after sub-acute lateral ankle sprains.Manual Therapy, 13: 63-67.
Sub-acute ankle sprain (n =11) Non-injured (n =11)
Aff ankle Matched
Unaf ankle
Biomechanical
MWM
Positional faults: may well occur butdifficult to measure?
Does the MWM reverse positional fault?
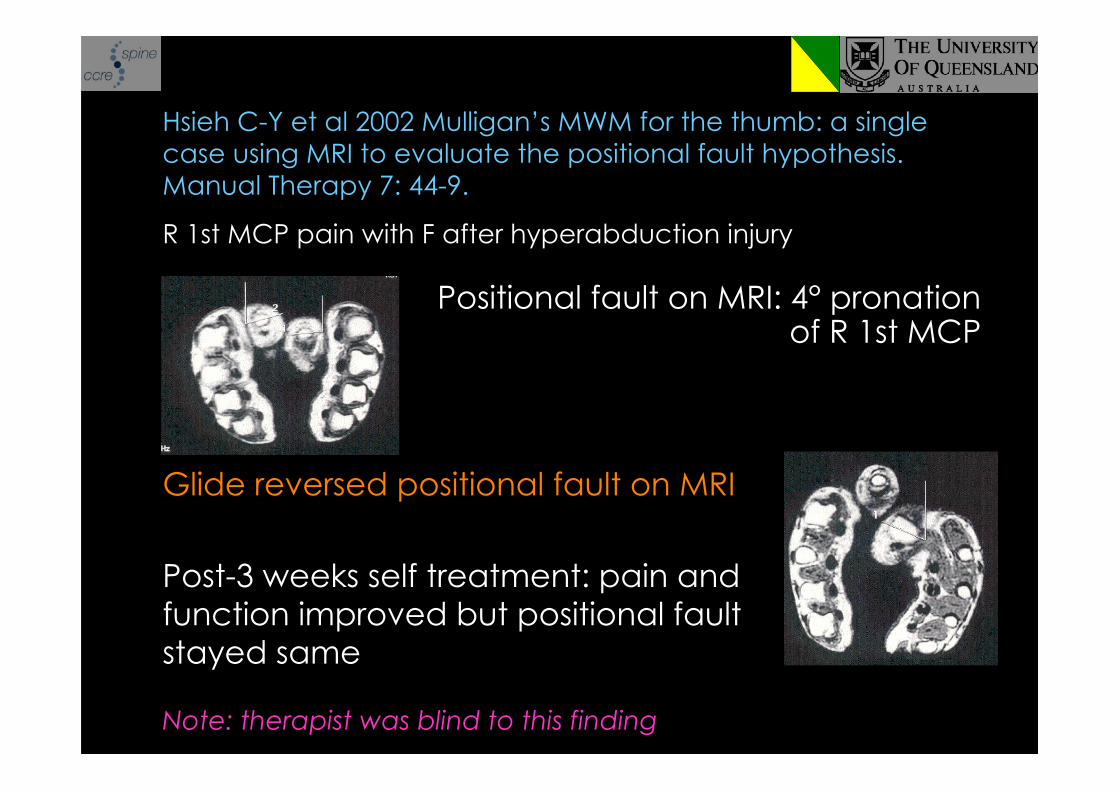
R 1st MCP pain with F after hyperabduction injury
Positional fault on MRI: 4° pronationof R 1st MCP
Hsieh C-Y et al 2002 Mulligan’s MWM for the thumb: a singlecase using MRI to evaluate the positional fault hypothesis.Manual Therapy 7: 44-9.
Glide reversed positional fault on MRI
Post-3 weeks self treatment: pain andfunction improved but positional faultstayed same
Note: therapist was blind to this finding
MWM
BIOMECHANICS
Human studies
Transient changein bone position
Teys P, Bisset L, Vicenzino B. The initial effects of a Mulliganmobilization with movement technique on ROM ad pressurepain threshold in pain-limited shoulders. Manual Therapy(2008) 13: 37-42.
• MWM versus Sham versus Control• 11 male & 13 female• mean age 46.1 ± SD 9.86 yrs

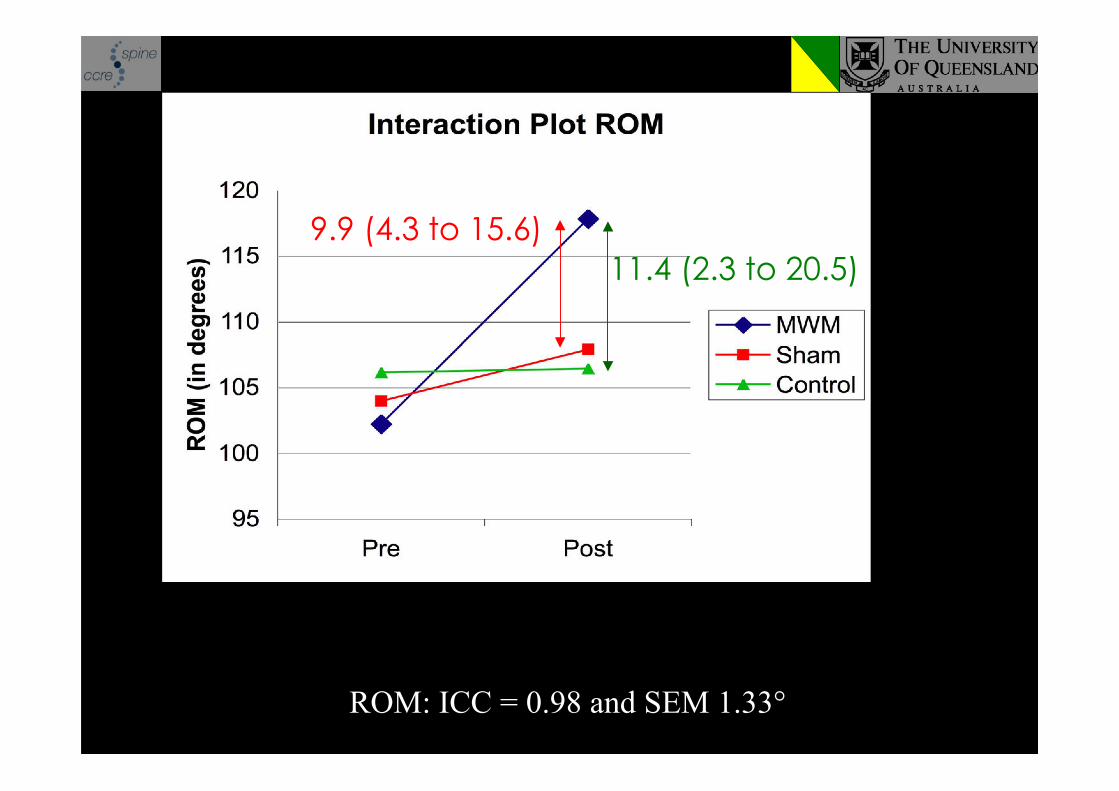
Results - ROM
ROM: ICC = 0.98 and SEM 1.33°
* 15.6°
11.4 (2.3 to 20.5)9.9 (4.3 to 15.6)
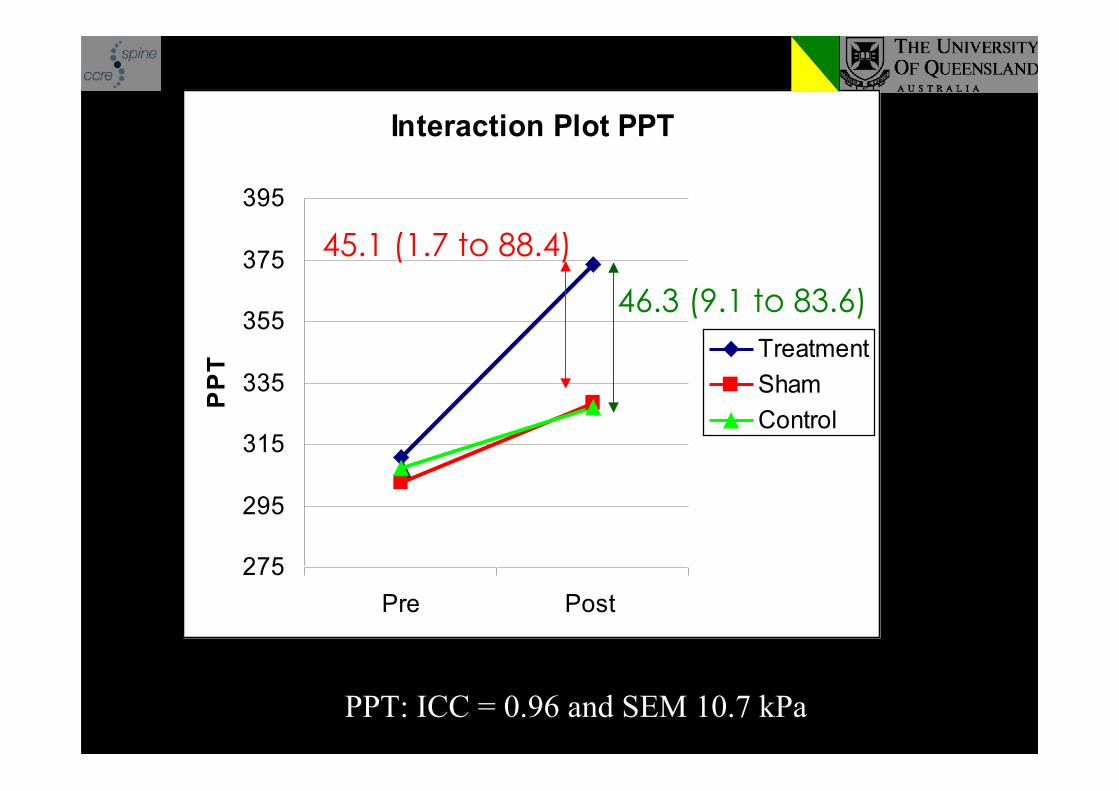
PPT: ICC = 0.96 and SEM 10.7 kPa
Interaction Plot PPT
275
295
315
335
355
375
395
Pre Post
PP
T
Treatment
Sham
Control
* 62.5 kPa
45.1 (1.7 to 88.4)
46.3 (9.1 to 83.6)
MWM
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
MWM
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
Pain effects human
animal
Associated systems & modeling
NEUROPHYSIOLOGIC
Transient changein bone position
&Increase ROM
Pain effects human
NEUROPHYSIOLOGIC
MWM produces an initial hypoalgesia
Treatment effect > placebo/control procedures
Initial hypoalgesia = non-opioid mechanisms
(e.g., Vicenzino et al (2001) Paungmali et al (2003a,b and 2004))
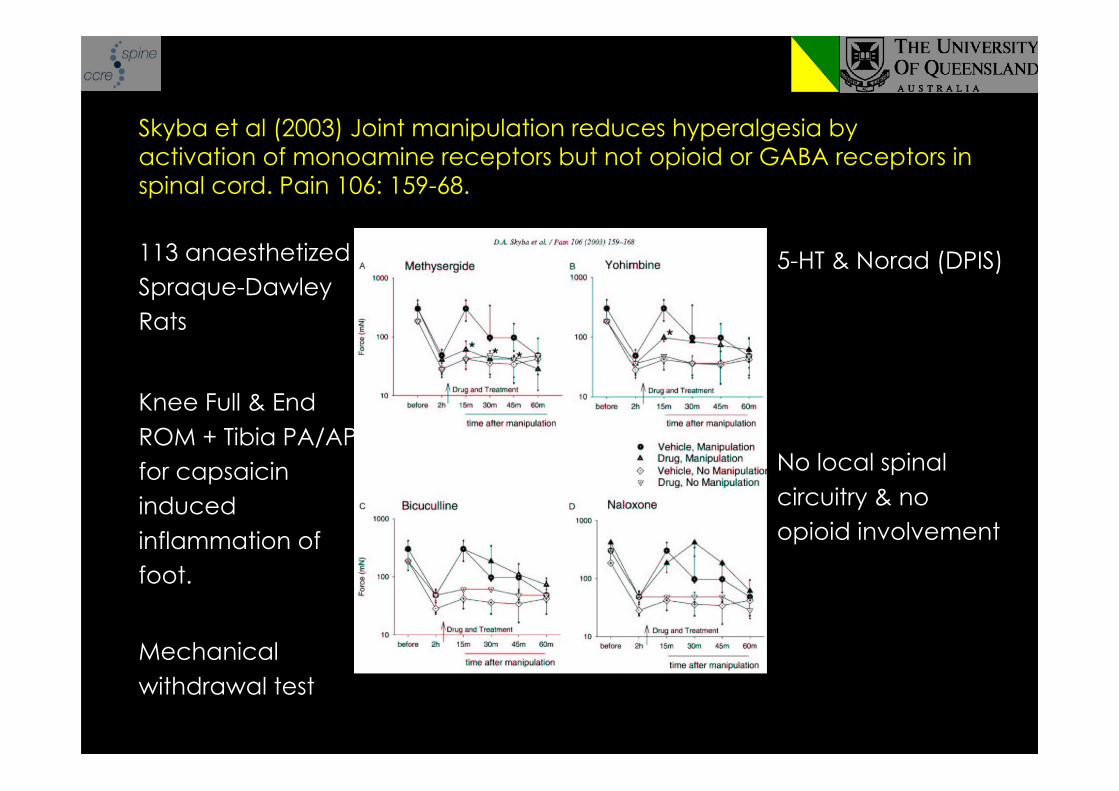
113 anaesthetizedSpraque-DawleyRats
Knee Full & EndROM + Tibia PA/APfor capsaicininducedinflammation offoot.
Mechanicalwithdrawal test
Skyba et al (2003) Joint manipulation reduces hyperalgesia byactivation of monoamine receptors but not opioid or GABA receptors inspinal cord. Pain 106: 159-68.
5-HT & Norad (DPIS)
No local spinalcircuitry & noopioid involvement
MWM
Pain effects human
animal
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
MWM
Pain effects human
animal
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
Associated systems & modeling
Transient changein bone position
&Increase ROM
animalPain effects human
NEUROPHYSIOLOGIC
Initial sympatho-excitation
(e.g., McGuiness et al 1997, Paungmali et al (2003), Simon et al 1997,Slater et al 1994, Vicenzino et al 1994, Vicenzino et al 1998)
Associated systems & modeling
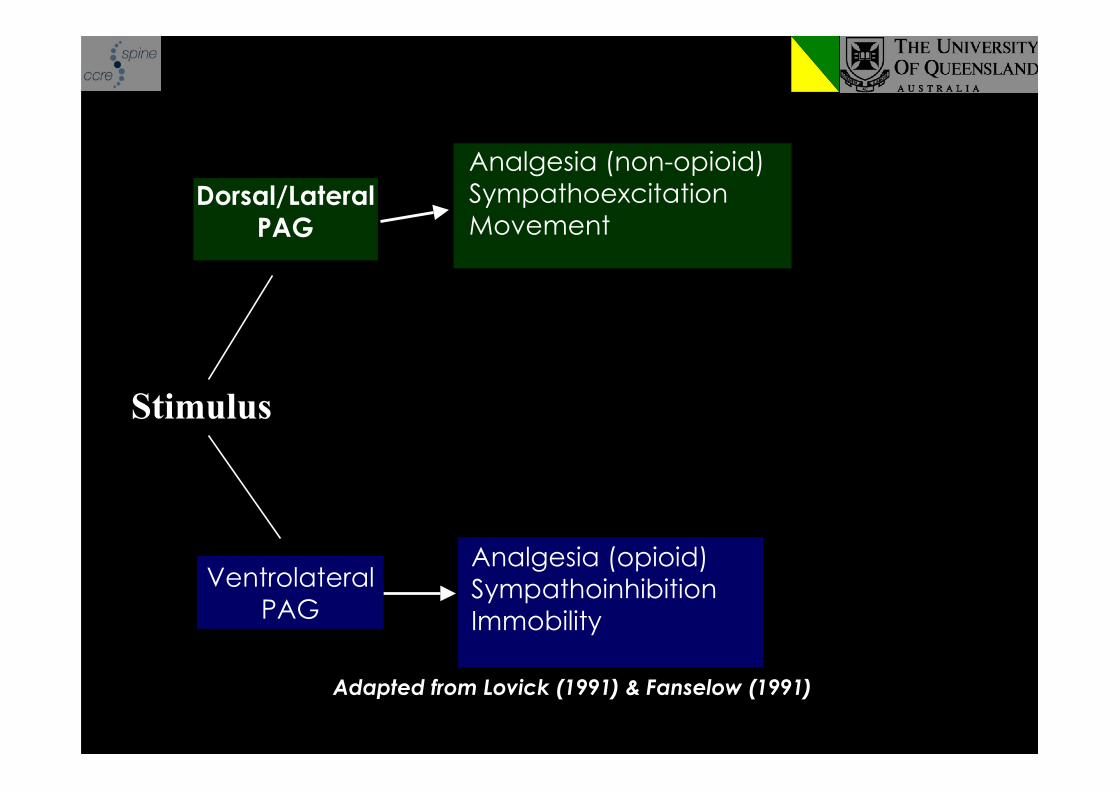
Adapted from Lovick (1991) & Fanselow (1991)
Stimulus
Dorsal/LateralPAG
Analgesia (non-opioid)SympathoexcitationMovement
Analgesia (opioid)SympathoinhibitionImmobility
VentrolateralPAG
Characteristics of pain relief:
Mechanical hypoalgesia associated withchanges in sympathetic and motor systemfunction
Mimics findings from spinal manipulationinferring involvement of descending paininhibitory systems
Preliminary animal studies confirming role ofendogenous non-opioid mechanisms in manual
therapy
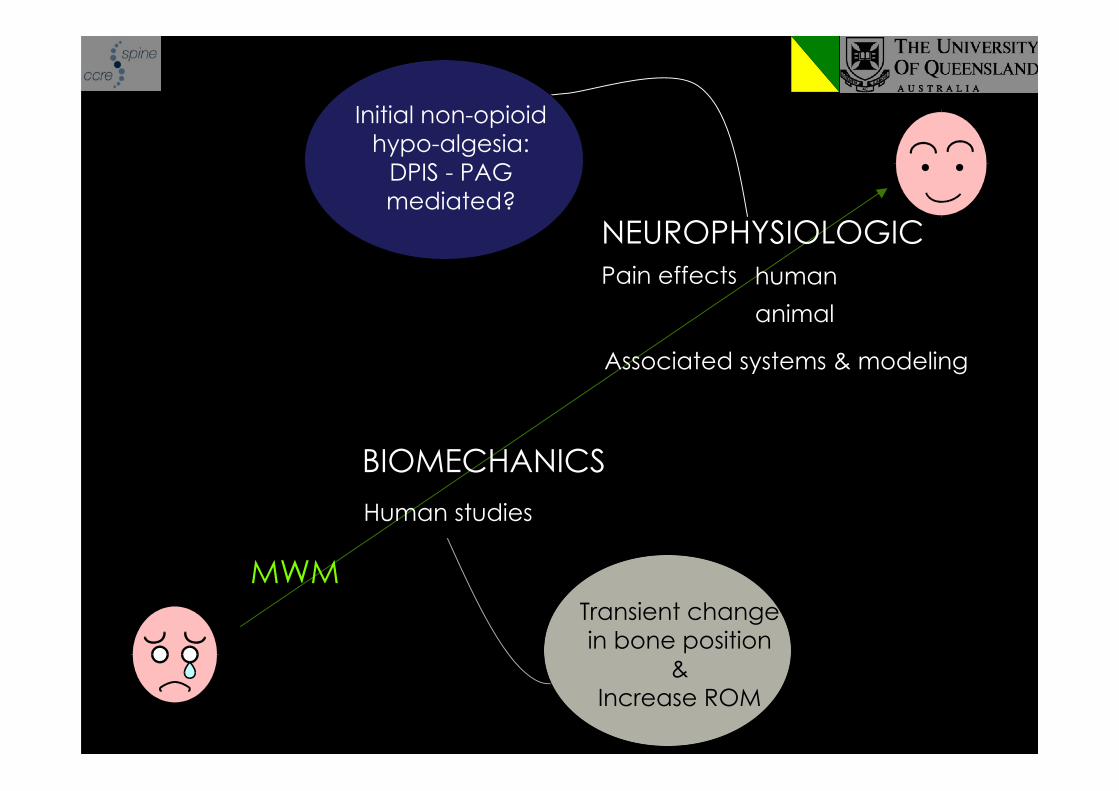
MWM
Pain effects human
animal
Associated systems & modeling
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS - PAGmediated?
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
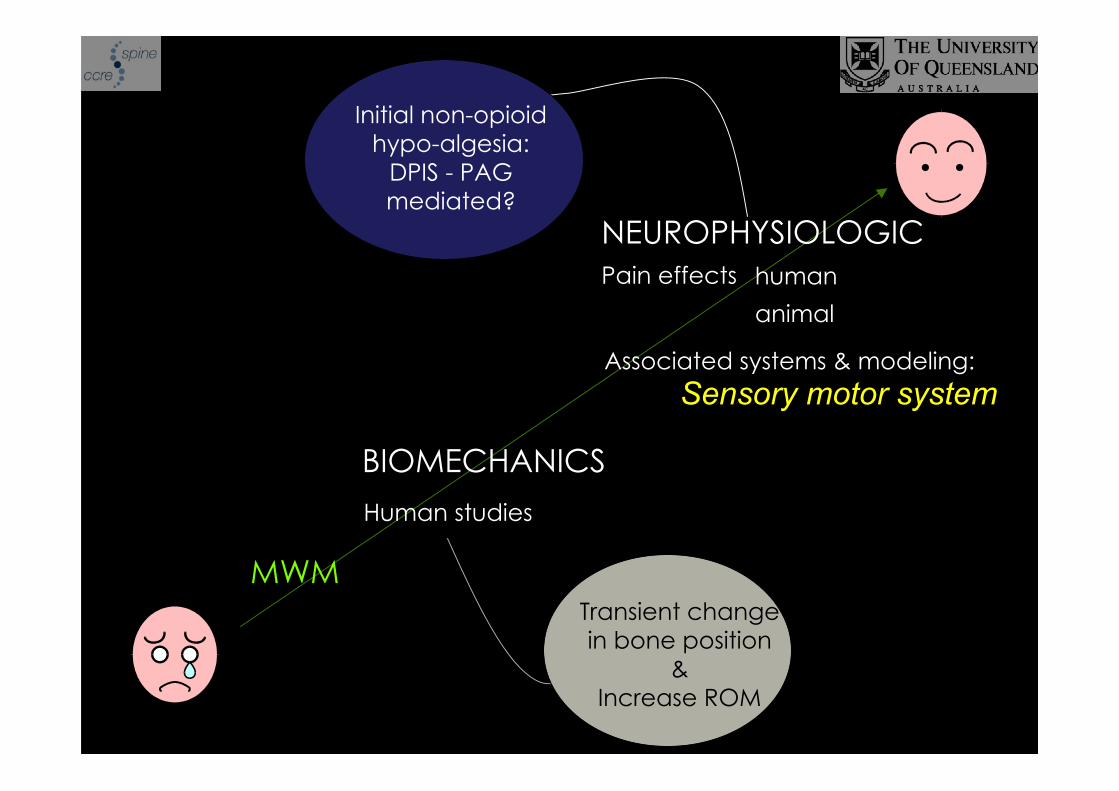
MWM
Pain effects human
animal
Associated systems & modeling:Sensory motor system
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS - PAGmediated?
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
Mobilisation With MovementEffects on Joint Position Sense:Preliminary Studies

Saturday: 9.00 - 9:30 The role of MWM in ankle injuries
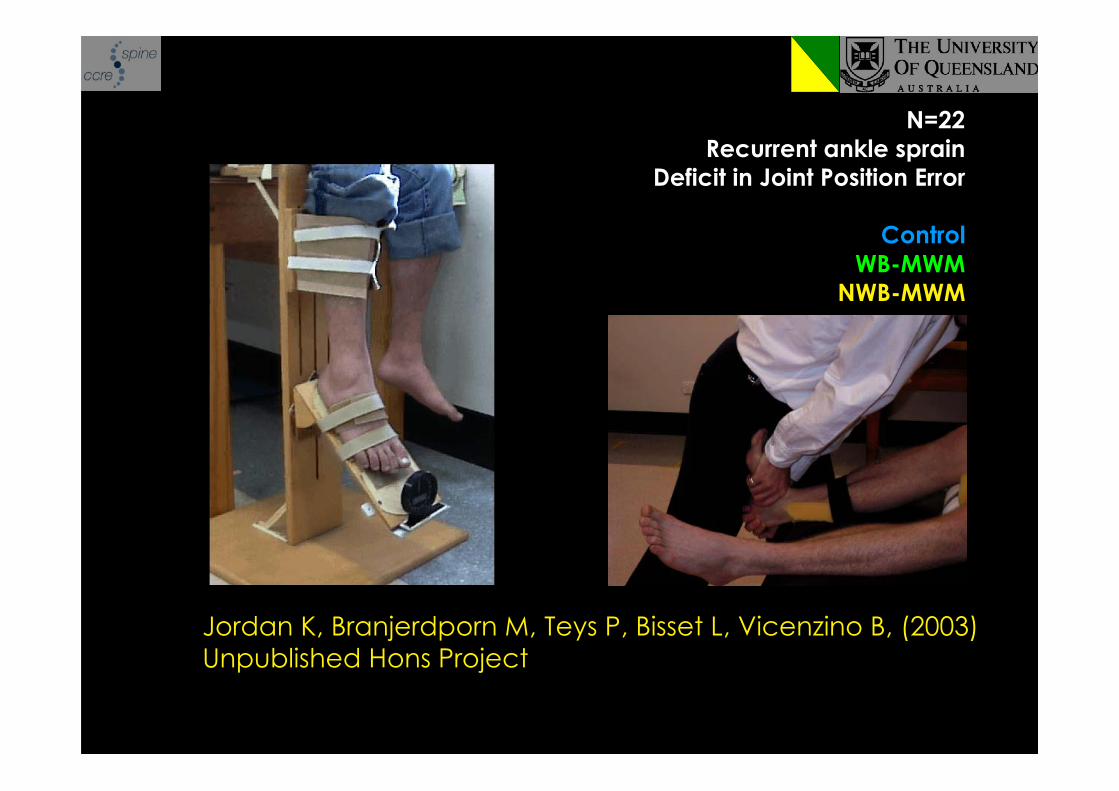
Jordan K, Branjerdporn M, Teys P, Bisset L, Vicenzino B, (2003)Unpublished Hons Project
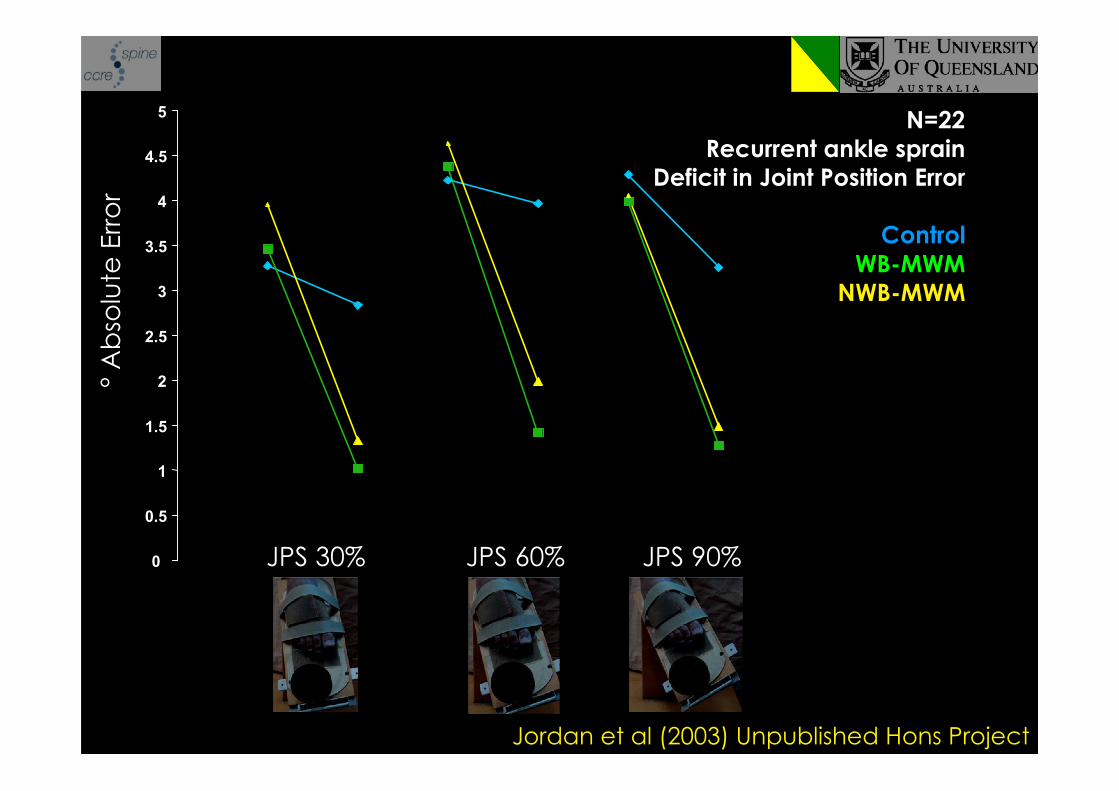
N=22Recurrent ankle sprain
Deficit in Joint Position Error
ControlWB-MWM
NWB-MWM
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
JPS 30% JPS 60% JPS 90%
Pre Post Pre Post Pre Post
° A
bso
lute
Err
or
Jordan et al (2003) Unpublished Hons Project
N=22Recurrent ankle sprain
Deficit in Joint Position Error
ControlWB-MWM
NWB-MWM
Are these findings an expression ofthe ‘restoration of joint memory’
explanation provided by Mulligan?
23 subjects with LE and reduced shoulder externalrotation pre-intervention.
MWM for LE reversed the deficit in shoulderrotation.
Interpreted as MWM induced changes in shouldermuscle tone
implying neurophysiological effect
Abbott JH (2001) MWM applied to the elbow affects shoulderROM in subjects with LE. Manual Therapy 6(3): 170-7
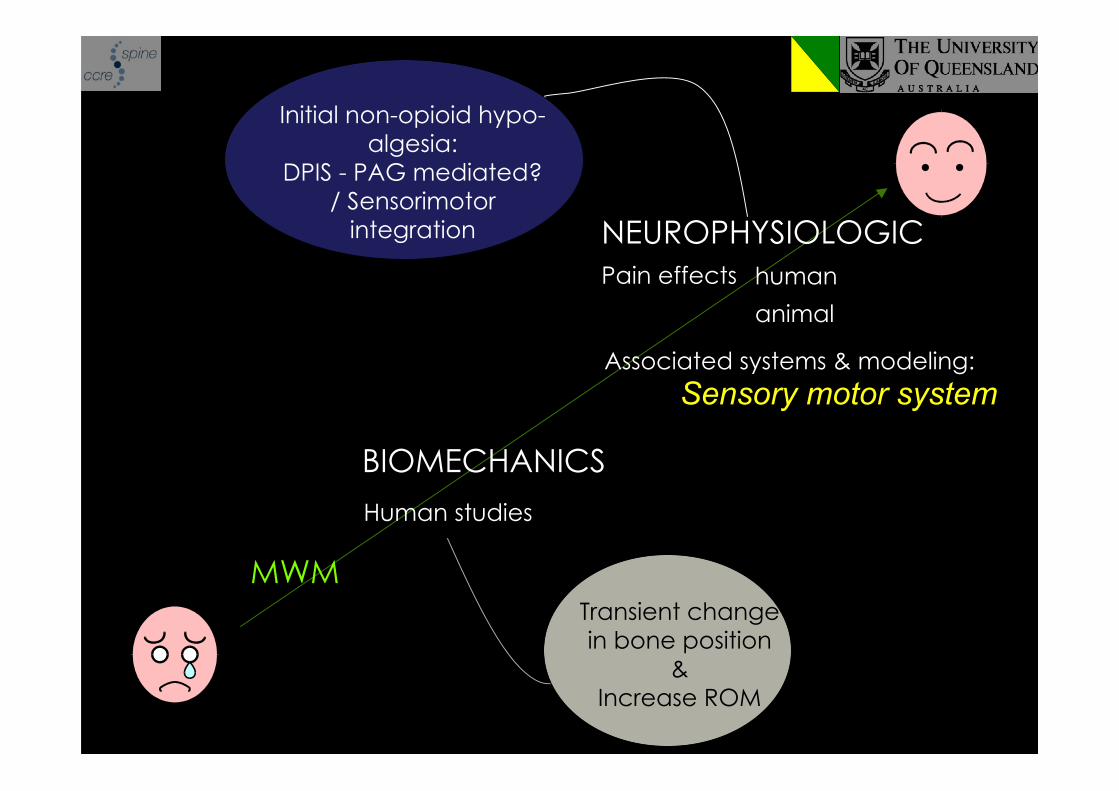
MWM
Pain effects human
animal
Associated systems & modeling:Sensory motor system
NEUROPHYSIOLOGIC
Initial non-opioid hypo-algesia:
DPIS - PAG mediated?/ Sensorimotor
integration
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
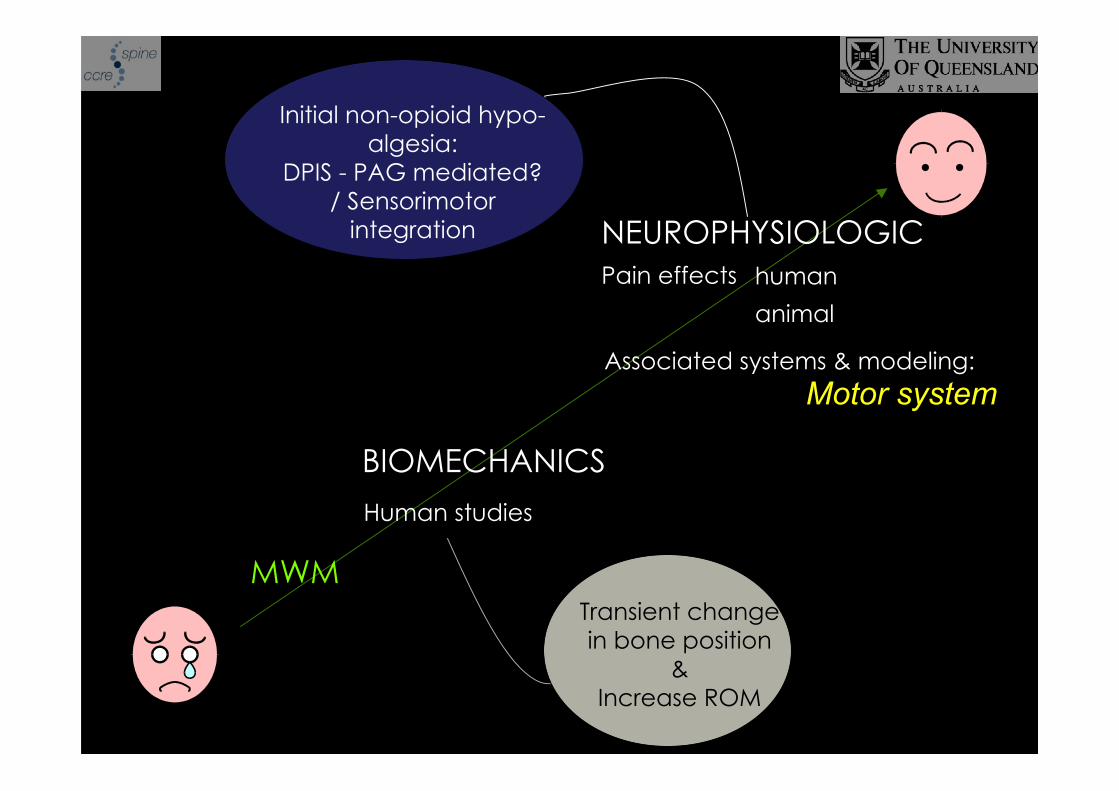
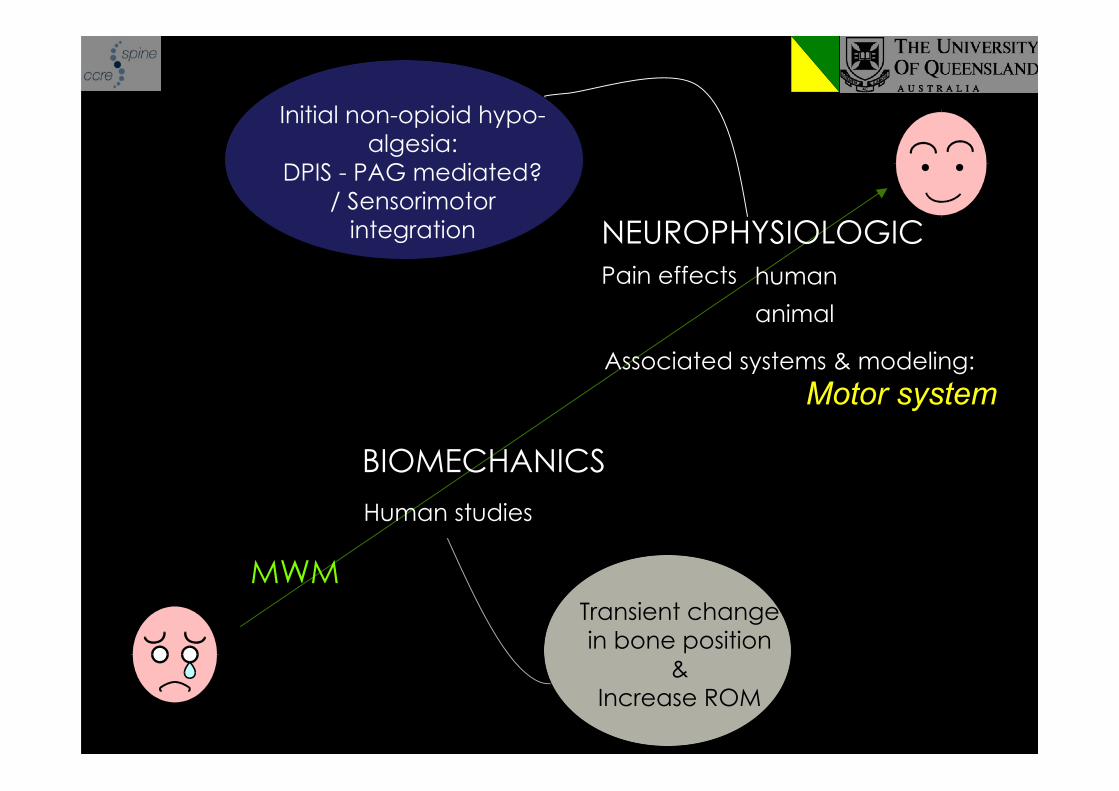
MWM
Pain effects human
animal
Associated systems & modeling:Motor system
NEUROPHYSIOLOGIC
Initial non-opioid hypo-algesia:
DPIS - PAG mediated?/ Sensorimotor
integration
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
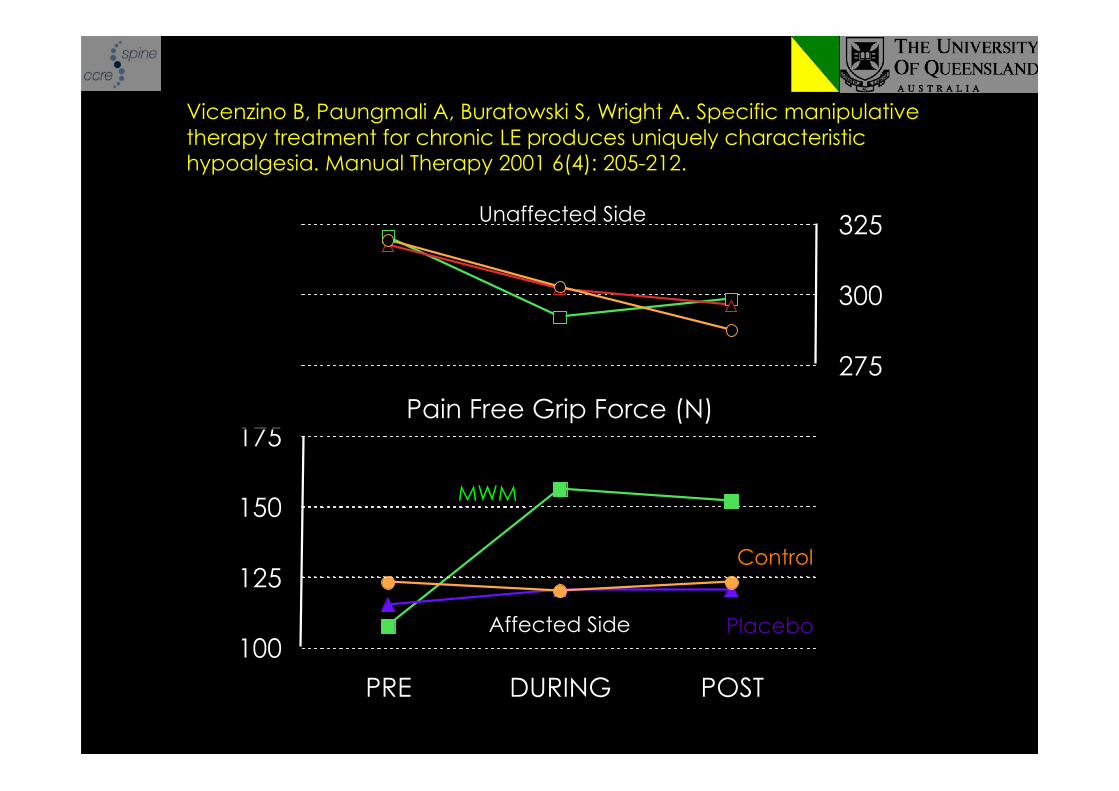
100
125
150
175
PRE DURING POST
275
300
325
Pain Free Grip Force (N)
Affected Side
Unaffected Side
MWM
Placebo
Control
Vicenzino B, Paungmali A, Buratowski S, Wright A. Specific manipulativetherapy treatment for chronic LE produces uniquely characteristichypoalgesia. Manual Therapy 2001 6(4): 205-212.
Abbott J, Patla C, Jensen R 2001 The initial effects of anelbow MWM technique on grip strength in subjects with LE.Manual Therapy 6: 163-169
N=25 (17 male; age: 46 years, range: 29-60) withunilateral LE (16 months: range 2-96)
Mean deficit in PFGS: 38.4 pounds of force
Mean difference pre to post application of MWM:• Affected = 10.4 pounds• Unaffected = -2.7 pounds
MWM
Pain effects human
animal
Associated systems & modeling:Motor system
NEUROPHYSIOLOGIC
Initial non-opioid hypo-algesia:
DPIS - PAG mediated?/ Sensorimotor
integration
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
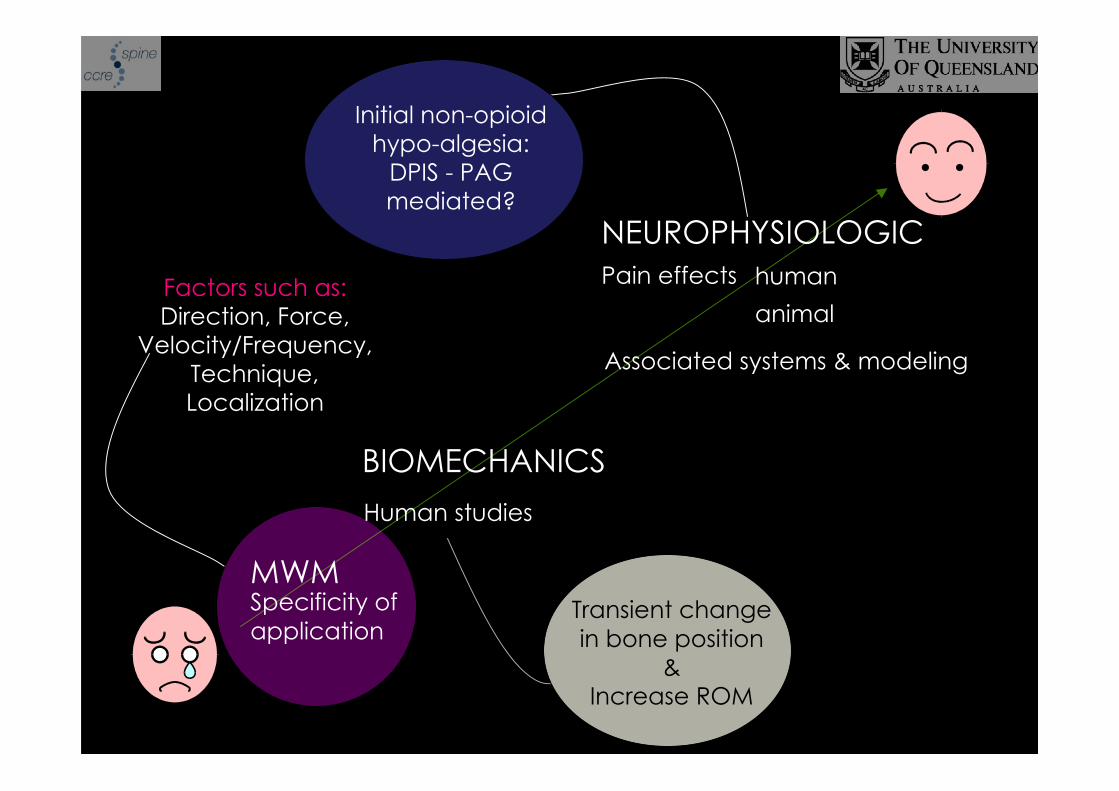
MWMSpecificity ofapplication
Pain effects human
animal
Associated systems & modeling
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS - PAGmediated?
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
Factors such as:Direction, Force,
Velocity/Frequency,Technique,Localization
Lateral glide with0 or 5° posterior inclination
NOT 5° anterior to direct lateral
Direction of force:
Abbott et al, 2001, The initial effects of an elbow MWM techniqueon grip strength in subjects with LE. Manual Therapy 6: 163-9
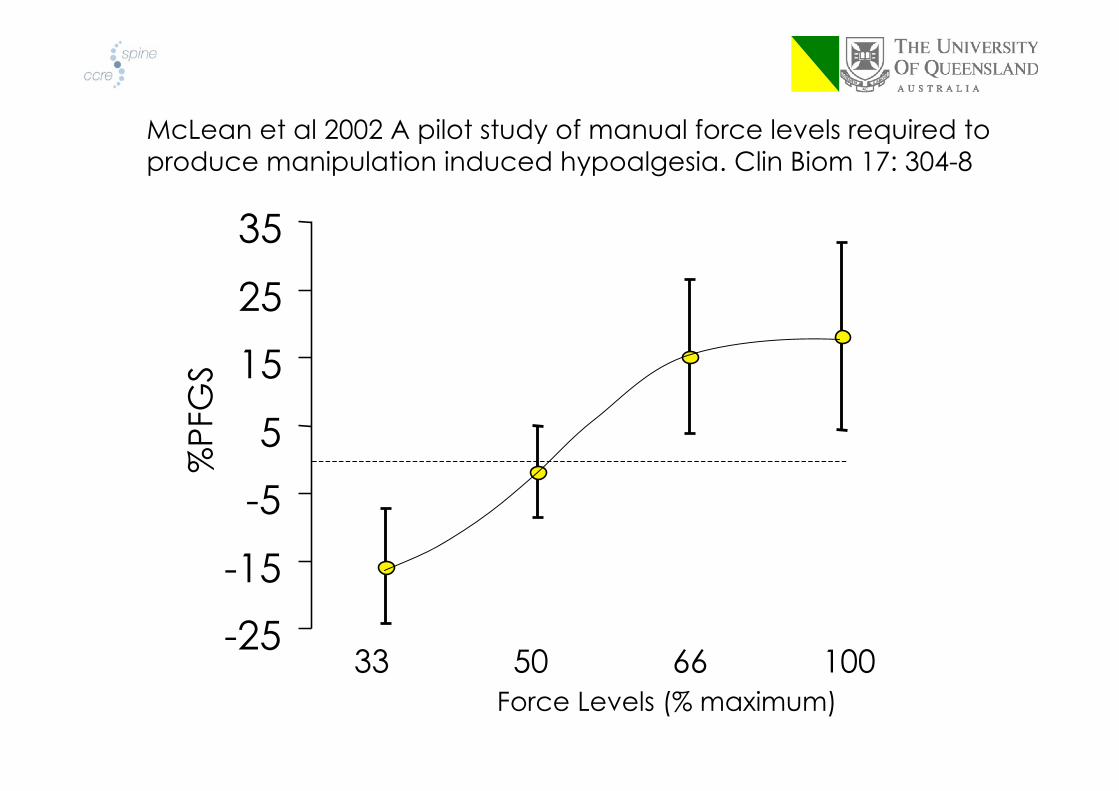
McLean et al 2002 A pilot study of manual force levels required toproduce manipulation induced hypoalgesia. Clin Biom 17: 304-8
-25
-15
-5
5
15
25
35%
PFG
S
33 50 66 100 Force Levels (% maximum)
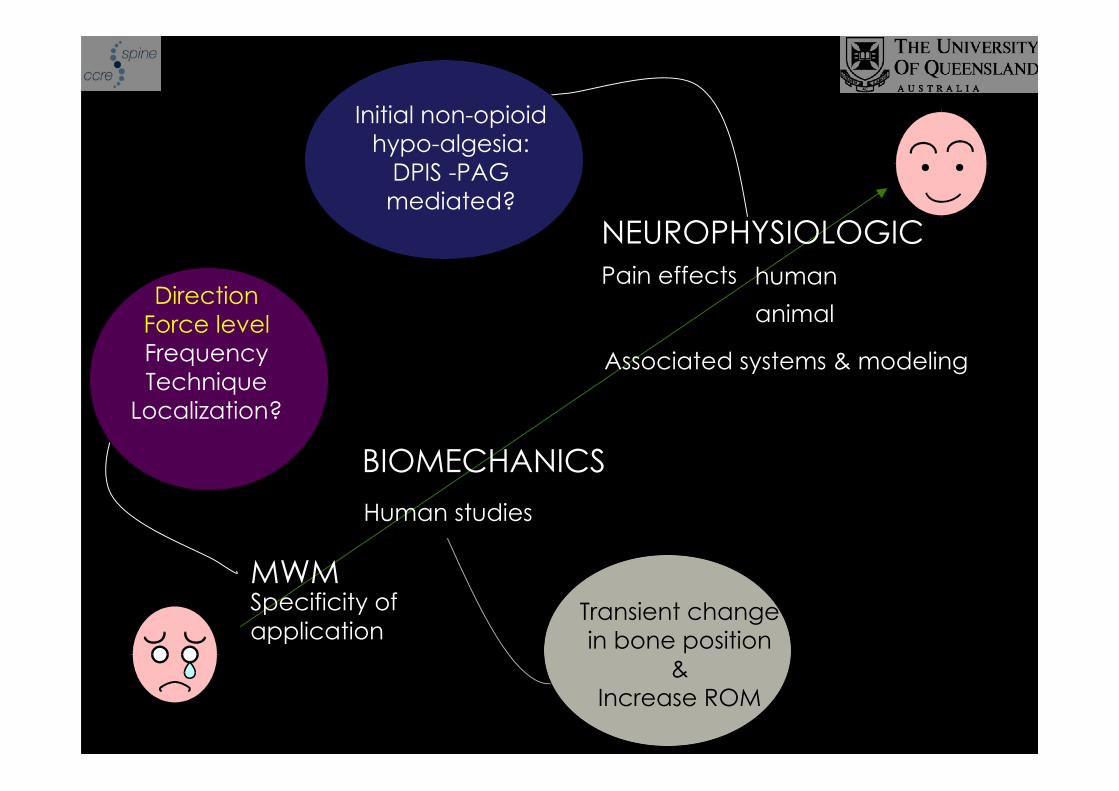
MWMSpecificity ofapplication
Pain effects human
animal
Associated systems & modeling
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS -PAGmediated?
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
DirectionForce levelFrequencyTechnique
Localization?
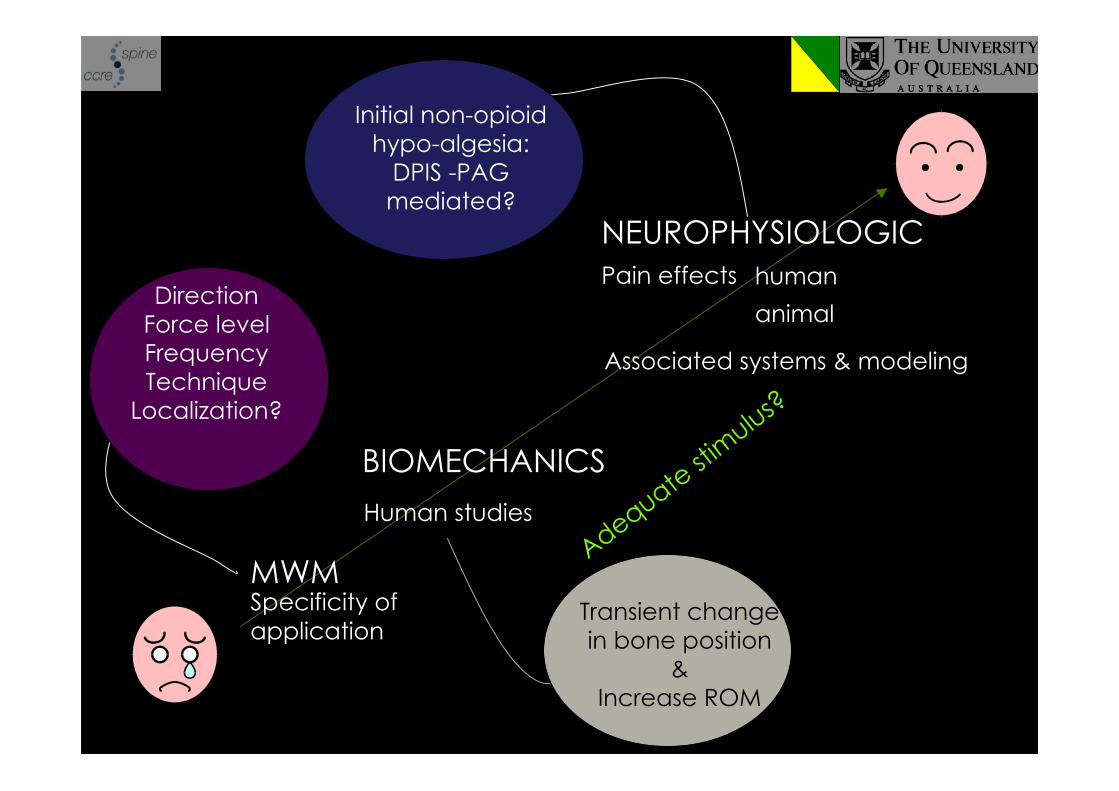
MWMSpecificity ofapplication
Pain effects human
animal
Associated systems & modeling
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS -PAGmediated?
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
DirectionForce levelFrequencyTechnique
Localization?
Adequate st
imulus?
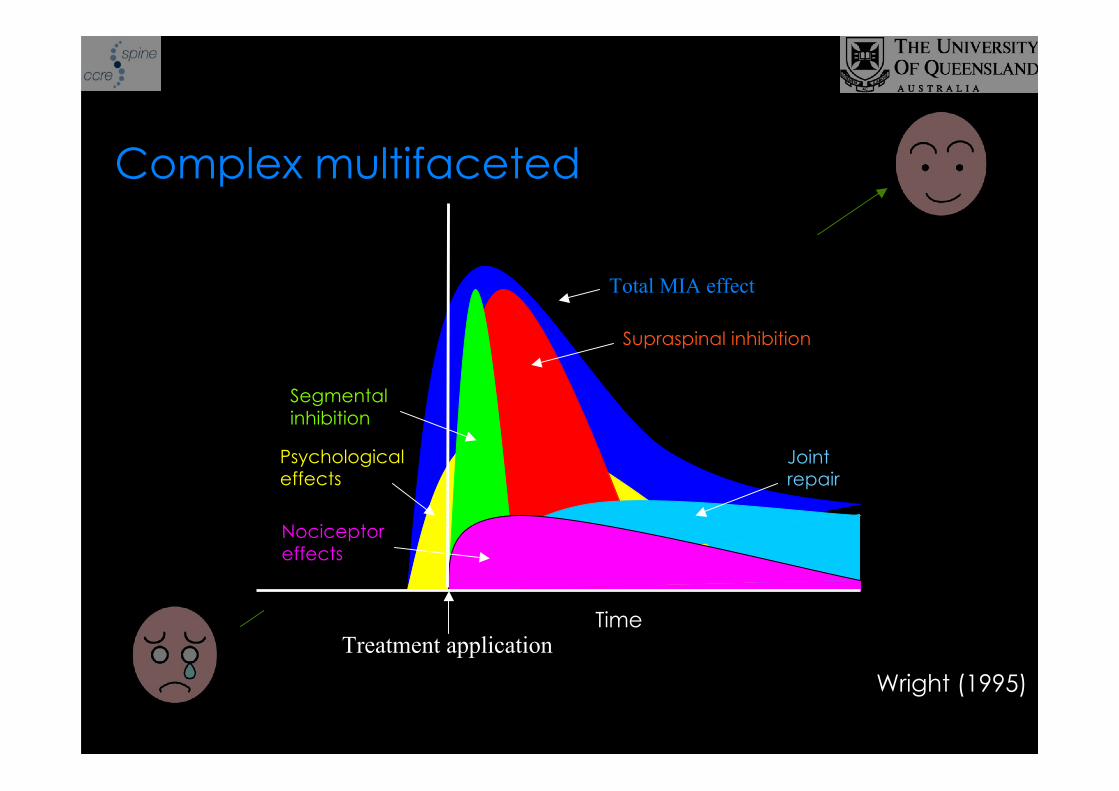
Complex multifaceted
Wright (1995)
Nociceptoreffects
Segmentalinhibition
Supraspinal inhibition
Psychologicaleffects
Total MIA effect
Treatment applicationTime
Jointrepair
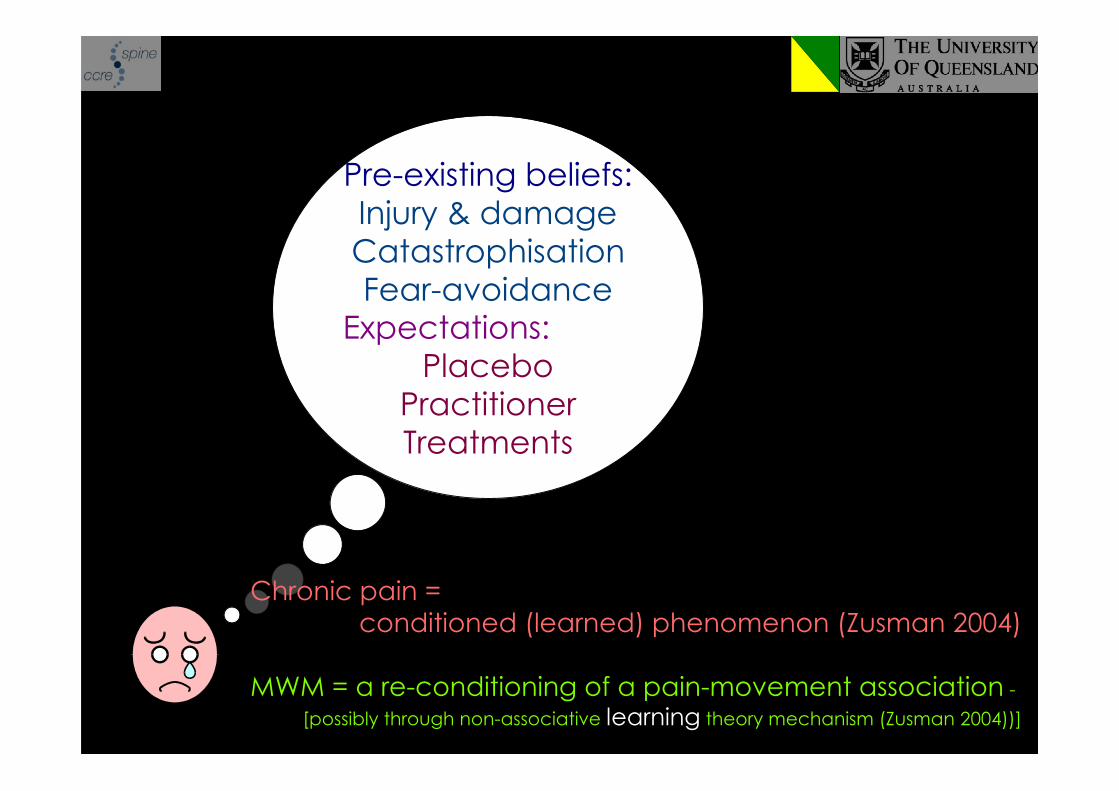
Pre-existing beliefs:Injury & damageCatastrophisationFear-avoidance
Expectations:Placebo
PractitionerTreatments
Chronic pain =conditioned (learned) phenomenon (Zusman 2004)
MWM = a re-conditioning of a pain-movement association -
[possibly through non-associative learning theory mechanism (Zusman 2004))]
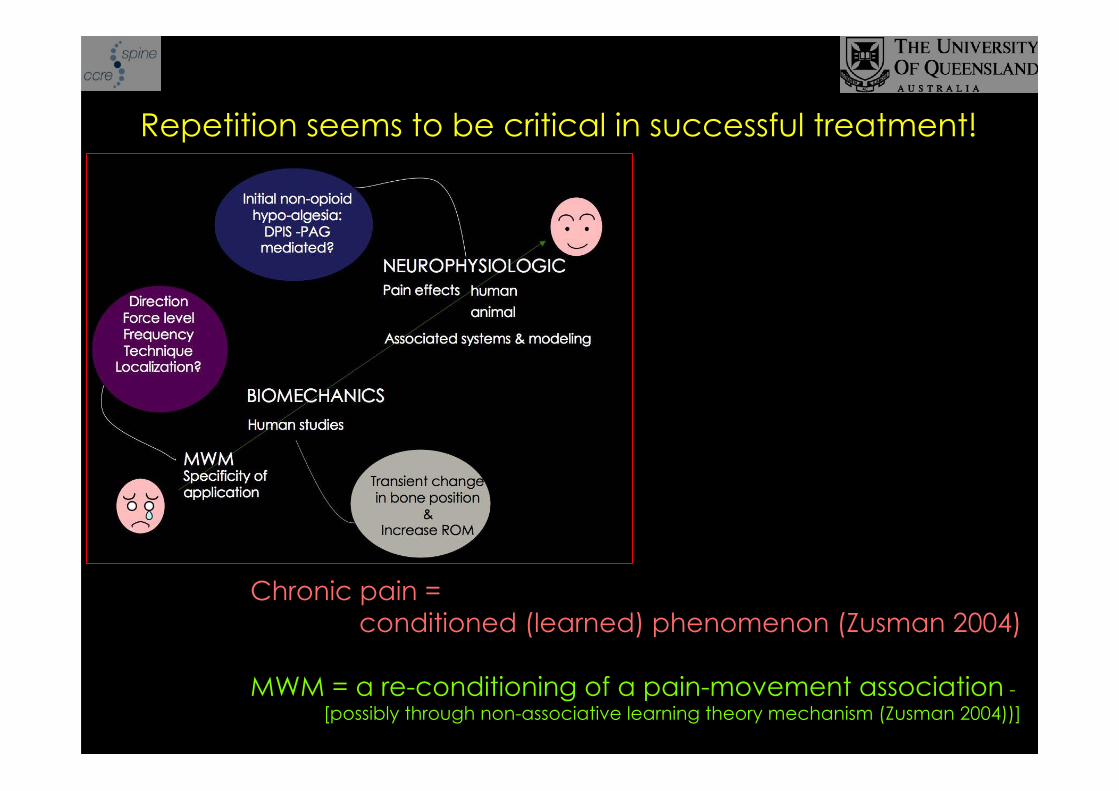
Repetition seems to be critical in successful treatment!
Chronic pain =conditioned (learned) phenomenon (Zusman 2004)
MWM = a re-conditioning of a pain-movement association -[possibly through non-associative learning theory mechanism (Zusman 2004))]
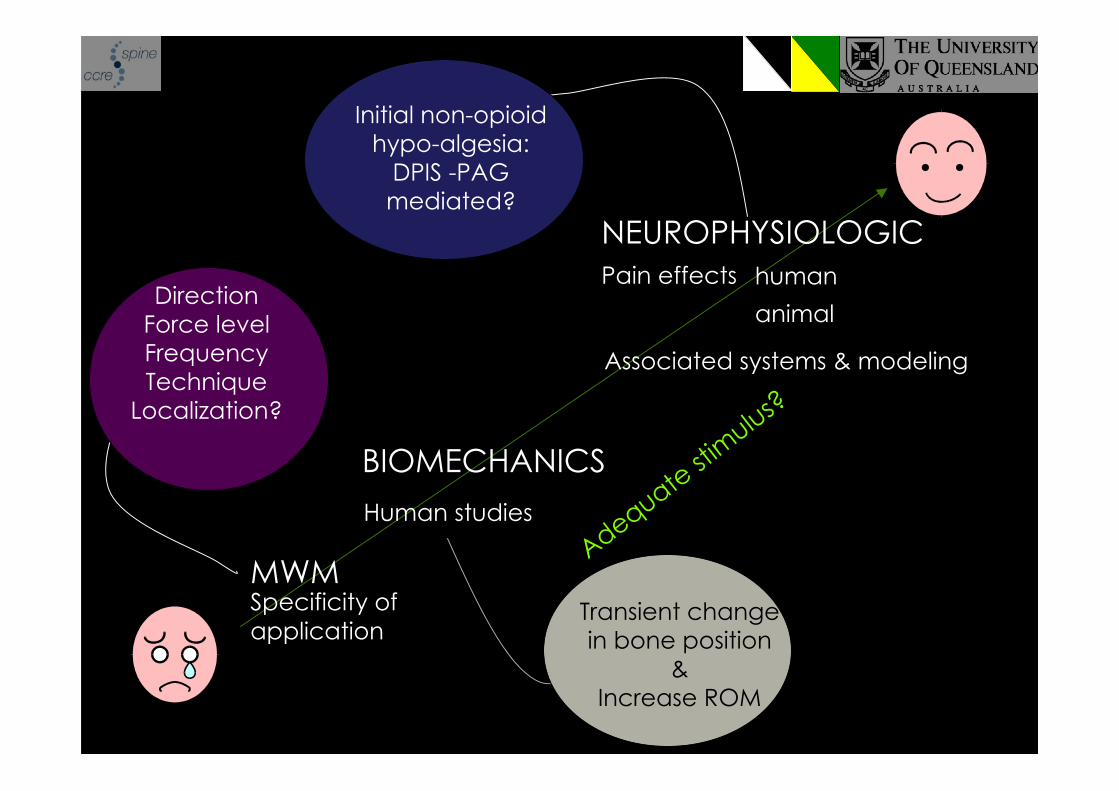
MWMSpecificity ofapplication
Pain effects human
animal
Associated systems & modeling
NEUROPHYSIOLOGIC
Initial non-opioidhypo-algesia:
DPIS -PAGmediated?
BIOMECHANICS
Human studies
Transient changein bone position
&Increase ROM
DirectionForce levelFrequencyTechnique
Localization?
Adequate st
imulus?