Embed Size (px)
Citation preview

Journal of the Korean Radiological Society, 1994: 31(4) : 627-632
MR Findings of Carebral Venous Sinus Thrombosis1
Myung Kwan lim, M.D. , Kee-Hyun Chang, M.D. ,
Moon Hee Han, M.D. , Choong Gon Choi. M.D.
Purpose: To describe MR findings of cerebral venoussinusthrombosis Meterials and Methods: We reviewed 11 MR images of six patients with cer
ebral venous sinus thrombosis. The MR images were retrospectively analyzed in terms of location and signal intensity of thethrombi. parenchymallesions such as hemorrhage and edema, and changes in follow-up study obtained in 4 patients.
Results: The thrombus in venous sinus was visualized on MRI in 허 1 six patients. The most frequently involved sites were superior sagittal sinus(n=4) and left transvere sinus(n=4). Signal intensity of the thrombus was isointense or hyperintense on both T1- and T2-weighted images with loss of normal signal void of the sinus on all sequences in all patients. Parenchymal lesion was present in five of six cases, manifested as local hemorrhage in three and edema in three cases(one case overlapped). Local edema seen in three patients was completely resolved on follow-up study of seven to 29 days intervals.
Conclusion: It is concluded that iso- or high signal intensity with loss of signal void in venous sinus is virtually diagnostic of venous sinus thromosis. If there are local parenchymallesions such as hemorrhage and/or edema of unknown causes, cerebral venoussinus thrombosis should be included in differential diagnosis.
Index Words: Brain , MR Brain , infarction Cerebral blood vessels , thrombosis Sinuses, superior sagittal Thrombosis, venous
Thrombosis of the c.erebral venous si nus and cortical vein , in the past, had been associated with high mortality rate. Only the prompt and appropriate treatment can save the life and decrease the morbidity(1-6). However, diagnosis of the cerebral venous thrombosis is not easy and often delayed because of non -specific clinical and radiological findings. The role of computed tomography(CT) and cerebral arteriography in establishing the diagnosis has been well described(7-1 이. Even though MR imaging is the best imaging method in demonstration of the patency of the vascular lumen as well as in detecting parenchymal alterations, MR findings of cerebral venous sinus thrombosis have been reported in only a few literature(1 , 3-6).
In this report, we describe MR findings of the cerebral venous sinus thrombosis in six patients.
'Oepartment 01 Diagnostic Radiology, Seoul National University College 01 Medicine ReceivedJune30, 1994 ; AcceptedAugust8, 1994 Address reprint requests to : Myung Kwan Lim, M. 0. , Oepartment 01 Oiagnostic Radiology, Seoul National University Hospital , 28 Yongon-dong, Chongno-gu ,
Seoul , 100-744 Korea. TeL 82- 2- 760- 3338 Fax. 82-2-743- 6385
METERIALS and METHODS
Eleven brain MR images of six patients with cerebral venous sinus thrombosis were reviewed retrospectively. The diagnosis was confirmed by angiography in four patients, and by both clinical and follow-up MR imaging in two patients. The patients , five females and a male, ranged in age from 18 to 49 years. Four patients had follow-up MR examinations 3 days to 6 weeks after the initial MR study. One patient had two follow-up MR studies. The predisposing factors to venous sinus thrombosis were found in three patients ; two had history of administration of oral contraceptives, and one was in pregnancy. In two patients , dural AV fistula was associated
In all patients , MR images were obtained using a 2.0 T superconducting magnet(Spectro 20000, Goldstar, Korea). Axial proton -density -weighted(2500/30/1 , TRI TE/exitation number) and T2 -weighted(2500/90/1) images and sagittal T1 -weighted(450 -500/25 -3012 -4) images were obtained in all patients. In 5 patients , cor-
긴
ι 0

chyma on T1 -weighted images. T2 -weighted images of the three patients showed that thrombi were hyperintense, isointense and hypointense , respectively. Contrast - enhanced T1 -weighted images of four pati ensts showed dense enhancement of dura adjacent to affected sinuses and the sinuses were filled with material predominantly isointense to brain , producing the delta or empty triangle signs previously described in the CT literature(7 -9) in two of four patients. These MR findings were well correlated with angiographic findigns.
Parenchymal lesion was present in five of six cases (83 %). Localized area of high signal intensity on both T1 - and T2 -weighted images representing hemorrhage was seen in temporallobes of three patients with thrombi in transverse sinus (case 1, 2, 6). There was localized area of slight low intensity on T1-weighted images and of high intensity on T2 -weighted images associated with mass effect, suggesting local edema, in three patients(case 1, 4, 5). It was seen in thalamus in two and in temporallobe in one patien t. On follow - up MR studies obtained in four patients , all edematous lesions were completely resolved. AII hemorrhagic lesions and venous sinus thrombi were partly resolved.
Journal of the Korean Radiological Society, 1994 ; 31(4) : 627- 632
RESULTS
The clinical and MR findings are summarized in Table 1 and 2, respectively. The most frequently involved sinuses were superior sagittal sinus(Fig. 1) and left transverse sinus (Fig. 1, 2)(four patients, respectively) . Straight and sigmoid sinuses were also involved in one patient each. Loss of normal signal void of the sinuses was seen in all MR sequences in all patients. Signal intensity of the thrombi was isointense relative to brain parenchyma on both T1 - and T2 -weighted images in three patients. In the remaining three patients , the thrombi were hyperintense relative to brain paren-
onal T1 - or T2 -weighted images were additionally obtained. Contrast - enhanced T1 - weighted images were obtained after intravenous injection of gadopentetate dimeglumine(O.1 mmole/1 kg) (Magnevist , SChering , Germany) in 4 patients. The section thickness and gap were 5 mm and 2 mm , respectively ; the matrix was 256 X 192-256 ; FOVwas20-25cm
The MR images were analyzed with attention to the location of the venous sinus thrombosis, signal intensity of parenchymallesions and thrombosed sinus, and changes of lesions on f이 low-up MR studies.
Table 1. Summary 01 Clinical Data
Angiography Location olvenous
sinus thrombosis
Predisposing
lactors
Chiel
complaint Age/Sex Case
perlormed
perlormed
perlormed
perlormed
NP
NP
SSS, TS(L)
TS( L)
SSS, TS(L)
VG , STS
SSS, Sig S
SSS, TS (L)
oral contraceptives
pregnancy id이iopat야thic
idiopathic
。ral contracetives
idiopathic
headache
headache
headache hemiparesis
headache
headache
22 I F
38 I F
49 / F
18 / F
43 / F
30 1M
1
2
3
4
5
6
STS : straight si nus SSS : superior sagittal sinus TS (L) : left transverse sinus VG: vein 01 Galen SigS: signoid sinus M ’ Male F: Female NP : not perlormed
Table 2. Summary 01 MR Fingings
F/U MRI
(i nterval*)
Parenchymal
edema
a e
m m) 빼
뼈
p’ h”
S101 thrombosed sinus
T1WI T2WI
Case number
disappeared edema(4wk)
decreased hemorrhage and thrombi(6wk)
NP
NP disappeared edema
decreased thrombi(4wk) disappeared edema
decreased thrombi(9d) decreased hemorrhage(3d)
right thalamus high high
left thalamus
right temporallobe
lefttemporallobe
left temporallobe lefttemporallobe
’so 150
low
IS。
ISO
ISO
high
ISO
끼/」 q니 A약
5
lefttemporallobe
SI : signal intensity NP : not performed
ISO
T1WI : T1-weighted image T2WI: T2-weighted image F/U : follow-up interval * : interval between initial and follow-up MRs
- 628
high 6

Myung Kwan Li m, et al : MR Findings of Carebral Venous Sinus Thrombosls
a b
c d
DISCUSION
The predisposing factors ofvenous sinus thrombosis are numerous. They include pregnancy and postpartum periods , use of oral contraceptives , dehydration , rapid diuresis , polycythemia vera , sickl cell disease, leukemia, thromobocytopenia, disseminated intravascular coagulation , malnutrition , acquired and congenital heart diseases, head truma, diabetes mellitus , and collagen vascular disease. However, many cases are idiopathic(1 -2). In our series, known predisposing factors were oral contraceptive in two patients , and pregnancy in one patien t.
The clinical manifestations are usually nonspecific and include headache, increased intracranial pressure , stroke, seizures , personality change, hallucinations , decreased mental function , and coma(1 -2). In our study , the most frequent clinical symptom was headache of sudden onset(five cases)
The CT diagnosis of cerebral sinus thrombosis is not easy , even though CT findings including intense tentorial and falcine enhancement and the delta sign have been well described in the postcontrast scans(7 -1 이.
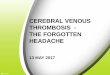
Fig. 1. A 22-year-old woman with history 01 oral contraceptives ingestion(case 1) a, b. There is an ill-delined area 01 low signal intensity(81) on T1-weighted image (T1WI) (a) , and 01 high 81 on T2WI (b) suggesting parenchymal edema in right thalamus c. Follow-up MR image obtained 4 weeks later shows new lesion 01 high 81 on both T1 WI and T2WI suggesting subacute hemorrhage in left temporal lobe. The edema in right thalamus had completely absorbed(not shown) d. There is thrombus 01 high 81 in superior sagittal sinus(arrows) on T1 WI. The thrombi were conli rmed with cerebral angiography
MR imaging is known to be very sensitive in detecting sinovenous thrombosis and parenchymal alterations. In the acute phase of dural sinus thrombosis , usually up to about 7 days, T1 -weighted images reveal an isointense signal within the venous sinus instead of the normal flow void. T2 -weighted images demonstrate marked hyp이 ntense signal within the venous sinus that simulates that of normal flow void , representing the presence of deoxyhemoglobin. Gradient echo flow images usually fail to demonstrate a flow enhancement, that is, a high - intensity signal within the sinus region . After about 7 days, both T1 - and T2 weighted images usually demonstrate hyperintense signal within the venous sinus which represents blood clot resulting from the formation of methemoglobin within the thrombus. The hemosiderin stage associated with chronic parenchymal hematomas does not 。ccur in sinus thrombus. The hemosiderin stage associated with chronic parenchymal hematomas does not occur in sinus thrombosis as the veins do not appear to accumulate hemosiderin - Iaden macrophages. Though the lack of a flow void may be due to thrombosis , it may also be seen with flow related enhancement, even echo rephasing , diastolic pseudogating , or flow compen-
없

Journal of the Korean Radiological Society, 1994 : 31(4) : 627- 632
a b
c d
sation techniques in normal subjects. The use of orthogonal imaging planes and differing repetition times (TRs) and avoidance of gradient moment nulling, e.g., the motion artifact suppression technique , can exclude these false -positive causes of increased signal Special flow images generated by gradient echos can be obtained and these demonstrate high signal of flowing blood within the patent vessels. Thrombosis will not show the high signal associated with flow(3 - 6, 11). In our study , the signal intensity of thrombi was either isointense or slightly hyperintense on both T1 -and T2 - weighted images except one case , which is generally well correlated with acute or subacute onset ofclinical symptoms.
In one case , the signal intensity of the thrombi in vein of Galen and straight sinus was high on T1 -weighted image and low on T2 -weighted image. This patient had sudden onset of severe headache, whose MR imaging was taken 3 days after ictus, probably representing acute stage ofthrombosis.
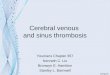
Fig. 2. A 38-year-old pregnant woman with 7 month pregnancy(case 2) a, b. There is a lesion of lightly high SI (arrows) on T1 WI (a) and isosignal (arrows) on T2WI (b) suggesting acute stage of hemorrhage in left temporallobe. c. T1-weighted sagittal i mage shows thrombi of iso-SI instead of normal flow void in lefttransverse sinus (arrows). d. Left external carotid arteriography shows dural arteriovenous malformation probably caused by left transverse sinus thrombosis (arrows).
As the complications of sinus thrombosis , parenchymal alterations such as venous infarct, intracerebral hemorrhage or dural arteriovenous fistula were reported(1 , 12-15). In our study, parenchymal abnormalities were found in five cases, localized hemorrhage in three cases and parenchymal edema in three cases(one case overlapped). The exact mechanism of parenchymal edema and hemorrhage is unknown. But, Yuh et al(16) explained the pathophysiological change with the concept of “Transependymal effusion". That is , the paUern of venous sinus thrombosis may be explained by the hypothetical model of the normal physiological shift of bulk interstitial fluid from the capillary bed toward the ventricle. The consequence of el evated venous pressure from venous occlusion can result in a spectrum ofchanges detectable by MR including a dilated venous and capillary bed , abnormal shift of bulk water, development of interstitial edema, increased CSF production , decreased CSF absorption , and rupture of venous structures(hematoma).
630-

Myung Kwan Li m, et a/ : MR Findings of Carebral Venous Sinus Thrombosis
jIÞ
..... ‘ -a b c Fig. 3. A 18-year-old woman with a venous thrombosis of unknown cause(case 4)
a. On T1 WI , there is focallow intensity lesion in leftthalamus(open arrows) and high signallesion suggesting thrombi in vein of Galen
and straight sinus (black arrows). The thrombi of the straight sinus show low intensity in venous sinus lesion suggesting acute stage
。f thrombosis (white arrows).
c. Venous phase ofvertebral angiography shows multiple filling defects in vein of Galen and straight sinus(arrows)
It is concluded that iso- or high signal intensity with
loss of signal void in venous sinus in association with a
local parenchymal hemorrhage and/or edema is
charateristic ofcerebral venous sinus thrombosis.
REFERENCES
1. Lee SH , Rao KCV, Zimmerman RA. Cranial MRI and CT
McGraw-Hill , lnc. 3rd. ed. 1992 ; 677-683
2. Bousser MG, Chiras J, Bories J, Castaigne P. Cerebral venous
thrombus- a reviewol38cases. Stroke 1985 ; 16: 199-213
3. McMurdo SK , Zawadzki MB , Bradley WG , Chang GY, Berg BO
Dural sinus thrombosis : study using intermediate lield strength
MR imaging. Radiology 1986; 161 ‘ 83-86
4. Lee SK , Han CH , Lee MO, Park KJ , Lee JH. MR imaging 01 dural
sinus thrombosis: a case report. J Korean Radiol Soc 1993; 29
51-54
5. Bauer WM , Heywang SH , vogl T, Seiderer M, Clados D. MR olve
nous sinus thrombosis : a case report. AJNR 1987; 8 : 713-715
6. Harris TM , Smith RR , Koch KJ. Gadolinium-DTPA enhanced MR
imaging 01 septic dural sinus thrombosis. J Comput Assist
Tomogr 1989 ; 13 : 682-684
7. Goldberg AL , Rosenbaum AE, Wang H, Kim WS, Lewis VL , Hanley DF. Computed tomography 01 dural sinus thrombosis. J
Comput AssistTomogr1986 ; 1 0 : 16-20
- 631
8. Rao KCV, Knipp HC, Wagner EJ. Computed tomographic lindings
in cerebral sinus and venous thrombosis. Radiology 1981 ; 140
391 -398
9. Eick JJ, Miller KD, Bell KA , Tutton RH. Computed tomogrpahy 01
deep cerebral venous thrombosis in children. Radiology 1981 ;
140 : 399-402
10. Gabrielsen TO, Seeger JF, Knake JE, Stilwill EW. Radiology 01
cerebral vein occl usion without dural sinus occlusion. Radiology
1981 ; 140 : 403-408
11. Strother CM , Eldevik P, Kiduchi Y, Graves V, Partington C, Merlis
A. Thrombus lormation and structure and the evolution 01 mass
effect in intracranial aneurysms treated by balloon embolization
: emphasis on MR lindings. AJNR1989 ; 1 0: 787-796
12. Halbach VV, Higashida RT, Hieshima GB , Goto K, Norman D, Newton Th. Dural listulas involving the transverse and sigmoid
sinuses : results 01 treatment in 28 patients. Radiology 1987; 163
443-447
13. Marco JK , Dillon WP, Halbach VV, Tsuruda JS. Dural arteri
。venous listula ‘ evaluation with MR imaging. Radiololgy 1990 ;
175: 193-199
14. Halbach VV, Higashida RT, Hieshima GB , Reicher M, Norman D, Newton TH. Dural listulas involving the carvernous sinus: results
。Itreatment in 30 patients. Radiology 1987 ; 163 : 437-442
15. Chaudhary MY, Scahdev VP , Cho SH , Weitzner 1, Puljic S, Huang
YP. Dural arteriovenous mallormation 01 the major venous
sinuses : an acquired lesion. AJNR 1982 ; 3: 13-19
16. Yuh WTC, Simonson TM , Wang AM , etal. Venoussinus occlusive
disease: MR lindings. AJNR 1994 ; 15 : 309-316

Journal of the Korean Radiological Society, 1994: 31(4) : 627 -- 632
대한방사선의학회지 1994 ; 31(4) : 627-632
경막정맥동 혈전증의 자기 공명 영상
서울대학교 의과대학 진 단방사선과학교실
임명관·장기현·한문회·최충곤
목 적 : 비염증성 원인에 의한 두개내 경막정맥동 혈전증의 자기공명(MR)영상 소견을 기술하고자 하였다.
대상 및 방법 :혈관조영술과 추적 MR영상으로 확진된 6여| 환자으111 MR영상을 후향적으로 분석하였다.MR상에서 경막정
맥동 혈전의 위치와 신호강도, 뇌출혈이나 국소적 부종등의 뇌실질의 병변을 분석하였고 이러한 소견들을 4예에서 시행한
추적 MR영상소견과 비교하였다.
결 과 : 가장 흔한 경막정맥동 혈전증의 위치는 상시상정맥동(suprior sagittal sinus, 4예)과 좌측 경막횡정맥동( trans
verse sinus, 4예) 이었으며, 혈전의 신호강도는 5예에서 Tl 및 T2강조영상에서 돔등 혹은 고신호강도를 나타내었다. 국소적
인 뇌실질병변은 5여|에서 관찰되었는데, 뇌출혈 (3예)과 부종(3예)( 1예는 중복)을 보였으며, 부종은 추적 검사상 완전 소실
도|었다.
결 론 :MR영상에서 경막정맥돔내의 정상적인 무신호강도 대신에, Tl 및 T2강조영상 모두에서 중등도 내지 는 고신호강
도를 보일 때 경막정맥돔 혈전증을 진단할 수 있고, 원인이 뚜렷하지 않은 뇌출혈이나 부종등의 뇌실질의 병변이 있을 때, 경
막정 맥동 혈전증이 감별진 단에 포함되어야 한다고 생각한다.
? ‘
Q U