Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 66 ■ October 201888
Multiple Cerebral Venous Sinus Thrombosis as Fist Manifestation of Primary Anti-Phospholipid Antibody SyndromeRathindranath Sarkar1, Rudrajit Paul2, Indranil Thakur2, Tanmay Jyoti Sau3, Debaditya Roy4, Rajesh Pandey4, Avinash Mani4, Aditya Vikram Ruia4
1Professor and HOD, 2Assistant Professor, 3Professor, 4Resident, Dept. of Medicine, Medical College, Kolkata, West BengalReceived: 23.07.2016; Accepted: 22.02.2018
AbstractAntiphospholipid antibody syndrome (APS) is an autoimmune disorder, mainly found in young females, presenting with vascular thrombosis and/or obstetric complications. Thrombosis at anatomically significant sites may lead to considerable morbidity and/or mortality. We here present a case of primary APS presenting with sudden onset bilateral multiple cerebral venous sinus thrombosis. The patient, a 17 year old female with no prior rheumatological history, presented with sudden onset bilateral painful blindness and massive proptosis. MRI venography was instrumental in diagnosis. She also had significant thrombocytopenia. Except for the visual dimness, the other symptoms responded to therapy. Such massive cerebral venous thrombosis is extremely rare in primary APS.
Introduction
An t i p h o s p h o l i p i d a n t i b o d y syndrome (APS) is a thrombophilic
disorder , mainly found in young women, characterized by the persistent presence of ant ibodies to certa in phosphol ip id or the i r assoc ia ted proteins in blood.1 This syndrome may remain asymptomatic or may present with arterial or venous thrombosis or obstetric complications.1 Sometimes catastrophic complicat ions of the syndrome may occur, mainly due to
blood vessel thrombosis at anatomically significant sites. We here report such a life threatening presentation of APS due to multiple cerebral venous sinus thrombosis.
Case Report
A 17 year old girl presented to the emergency with sudden onset severe headache and swelling of both eyes for one day. She had profound nausea but no history of seizures. She had no history of trauma to the head or any surgical intervention. There was no
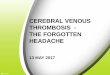
fever, arthritis or skin rash. She was not receiving any drugs. At presentation, the eyes were massively swollen (Figure 1) with complete ophthalmoplegia, chemosis and no light perception. Pupils were bilaterally dilated and non-reactive to light. Blood pressure was 150/97 mm of Hg. In view of this presentation, as a medical emergency, a provisional diagnosis of cavernous sinus thrombosis (CST) was made and she was started on intravenous vancomycin and meropenem. She was also started on intravenous heparin. An initial MRI scan of the brain was normal.
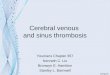
After three days, as the patient stabilized, an MRI venography of the brain was done which revealed (Figure 2) thrombosis of mult iple venous sinuses including superior sagittal sinus, inferior sagittal sinus, cavernous sinus and bilateral transverse sinuses. In addition to the heparin and antibiotics, oral acenocoumarol was also started to attain an INR of 3. The imaging revealed diffuse cerebral edema. Hence, a CSF study was decided against.
Other laboratory tests revealed a hemoglobin of 6.6 gm/dl, total leukocyte count of 9790/cmm (Neutrophil 81%; lymphocyte 16%) and platelet count of 60000/cmm. ESR was 90 mm in the 1st hour and C reactive protein was 15 mg/l (N<6). Peripheral blood smear did not reveal any abnormality. Direct Coomb’s test was negative. Urea/creatinine were 23 and 0.7 mg/dl respectively and liver function test was normal. Routine urine examination was normal. Blood and urine culture were negative. Urine pregnancy test was negative. D-dimer level was 862.1 ng/ml (N<400). INR was 2.6 and aPTT was 47 seconds (control: 28), even after stopping heparin 8 hours before the test. Anti-nuclear factor was negative.
Fig. 1: Marked proptosis at presentation
Fig. 2: MRI venography of the patient showing thrombosis and obliteration of superior sagittal sinus (A), inferior sagittal sinus (B), transverse sinuses (C) straight sinus (D) and sigmoid sinus (E)

Journal of The Association of Physicians of India ■ Vol. 66 ■ October 2018 89
But anti-phospholipid antibody (IgG) level was very high (204 .6 U/ml) (normal <12; done by ELISA). The other test for anti-cardiolipin antibody came as 148.8 U/L (N<12). ANCA was also negative. Both lower limb venous Doppler study was done; it was normal. Serum homocysteine level and viral serologies were also normal.
The patient was thus diagnosed provisionally as a case of primary APS.
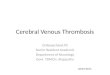
Whi le in hospi ta l , the pat ient received oral anticoagulants and i.v. antibiotics for three weeks. Although an etiology for the thrombosis was found, still antibiotics were given as infection was not completely ruled out. Anti hypertensives were also given. The swelling around her eyes decreased quickly (Figure 3). However, visual acuity was markedly decreased in both eyes. Fundus examination revealed normal retina with mild papilledema.
On follow up, after three months, the anti-phospholipid antibody (IgG) was st i l l posit ive. Thus, the anti -phospholipid antibody was persistent, supporting our init ial provisional diagnosis. To search for the etiology of the thrombosis, a protein C and protein S level was also done after two months (after stopping the acenocoumarol
for adequate per iod) , which was normal. Lipid profile was also normal. There were no new venous or arterial thrombosis. However, visual acuity was still decreased and bilateral ocular movement was partially restricted. Also, she required anti-hypertensives persistently.
Discussion
APS is characterized by thrombosis in both arteries and veins, although veins are more commonly affected1. It can be in the form of involvement of large veins like deep vein thrombosis in legs or involvement of small veins in the skin leading to livedo reticularis1. Paradoxically, the platelet count is often low although bleeding is rare. Our patient also had thrombocytopenia at presentation.
C e r e b r a l v e n o u s t h r o m b o s i s (CVT) can occur due to a variety of e t io logies l ike infect ion, post -neurosurgery, cerebral hypotension or hereditary thrombophilic states. Anti-phospholipid antibodies as a cause of CVT has been infrequently reported. Usually, previous published case reports have shown thrombosis of unilateral single cerebral venous sinus in APS2. But in our case, as the imaging shows, multiple venous sinuses were involved bilaterally. In single sinus involvement, the presenting symptoms may be subtle like prolonged headache or intermittent visual problems2. But in a case like ours with multiple sinus involvement, the presentation is acute with dramatic symptoms. In one of the reported cases, chronic hepatitis was associated with APS3. But in our case, no other system was involved. Some authors have reported associated other extra-cerebral sites of venous thrombosis in patients of CVT in APS4. However, in our case, no other site of venous thrombosis was evident.
However, the mere presence of anti-phospholipid antibody in a case of CVT does not indicate a cause-effect relationship. As a recent study shows, even in patients who were APLA+,
other etiologies like sickle cell trait or pregnancy also contributed to the CVT.5 Hence, even if APS is diagnosed, other common et iologies l ike use of oral contraceptives, infection or hereditary thrombophilias should still be searched.
A P S m a y h a v e o t h e r c e n t r a l nervous system (CNS) manifestations.6 Headache, epilepsy and chorea can occur in APS without any venous t h r o m b o s i s . 6 C e r e b r o v a s c u l a r accident, that is arterial thrombosis, may also occur. However, most CNS manifestations are found in secondary APS associated with SLE.6 Primary APS presenting with CVT is extremely rare.
Mult iple cerebral venous sinus thrombosis is very rare. In a recent study from India, out of a series of CVT cases, only 20% were multiple.7 The mortality in this group of patients was extremely high. Our patient survived the episode but had long term visual sequelae, as stated above.
We report this case to highlight this rare complication of APS. Such a m a n i f e s t a t i o n o f p r i m a r y A P S has not yet been reported from the subcontinent.
References1. Dhir V, Pinto B. Antiphospholipid syndrome: A review.
Journal of Mahatma Gandhi Institute of Medical Sciences 2014; 19:19-27.
2. Boggild MD, Sedhev RV, Fraser D, Heron JR. Cerebral venous sinus thrombosis and antiphospholipid antibodies. Postgrad Med J 1995; 71:487–9.
3. Kesler A, Pomeranz IS, Huberman M, Novis B, Kott E. Cerebral venous thrombosis and chronic active hepatitis as part of the antiphospholipid syndrome. Postgrad Med J 1996; 72:690-2.
4. Shlebak A. Antiphospholipid syndrome presenting as cerebral venous sinus thrombosis: a case series and a review. J Clin Pathol 2016; 69:337-43.
5. Carhuapoma JR, Mitsias P, Levine SR. Cerebral venous thrombosis and anticardiolipin antibodies. Stroke 1997; 28:2363-9.
6. Sanna G, Bertolaccini ML, Cuadrado MJ, Khamashta MA, Hughes GR. Central nervous system involvement in the antiphospholipid (Hughes) syndrome. Rheumatology (Oxford) 2003; 42:200-13.
7. Patil VC, Choraria K, Desai N, Agrawal S. Clinical profile and outcome of cerebral venous sinus thrombosis at tertiary care center. J Neurosci Rural Pract 2014; 5:218-24.
Fig. 3: Condition of the eyes on day 10