Embed Size (px)
Citation preview

BRIEF COMMUNICATION
Mowat–Wilson syndrome: the first report of an associationwith central nervous system tumors
Elvis Terci Valera & Sabrine Teixeira Ferraz & María Sol Brassesco & Xiumei Zhen &
Yiping Shen & Antonio Carlos dos Santos & Luciano Neder & Ricardo Santos Oliveira &
Carlos Alberto Scrideli & Luiz Gonzaga Tone
Received: 14 June 2013 /Accepted: 17 September 2013 /Published online: 3 October 2013# Springer-Verlag Berlin Heidelberg 2013
Abstract Mowat–Wilson syndrome (MWS) is a rare geneticcondition where variable and multiple congenital anomaliesincluding Hirschsprung's disease, intellectual disability, andprominent facial features are present. At molecular level, MWSis characterized by many different described mutations in thezinc finger E-box protein 2 (ZEB2) gene, ultimately leading to
loss of gene function. This report is the first to describe theassociation of MWS with two different asynchronous malignantbrain tumors (medulloblastoma and glioblastoma) occurringin a child.
Keywords Mowat–Wilson syndrome . Cancer genetics .
Brain cancer . Hirschsprung's disease . Children
Introduction
Mowat–Wilson syndrome (MWS; OMIM 235730) is a par-ticularly rare genetic condition described by Mowat et al. in1998, who reported a series of six children with intellectualdisability, striking facial features, and variable multiple con-genital anomalies, including Hirschsprung's disease (HD) [9].All molecularly confirmed cases with typical MWS have aheterozygous loss of function mutation in the zinc finger E-box protein 2 (ZEB2 ) gene also called Smad-interacting pro-tein 1 (SIP) or ZFHX1B . To date, about 200 molecularlyproven MWS cases with over 100 different ZEB2 mutationshave been reported [3].
Although HD may also occur as an isolated phenotype in70 % of cases, between 5 and 30 % of patients with HD haveother associated congenital defects with central nervous sys-tem (CNS) abnormalities making up about 7 % of these cases[1, 7, 8]. These associations are of significance due to twomain reasons: firstly, they may be attributed to abnormalgenetic development signaling, yielding clues as to the geneticbackground of HD and its pathogenesis, and secondly, theymay have various influences on long-term prognosis [7].Essentially, HD appears at a molecular level to result due todisruption of normal signaling during development. As aresult, the cues controlling the migration of the neural crestcells go awry resulting in aganglionosis of the distal bowel.
E. T. Valera : S. T. Ferraz : C. A. Scrideli : L. G. ToneDivision of Pediatric Oncology, Department of Pediatrics;Faculty of Medicine of Ribeirão Preto, University of São Paulo,São Paulo, Brazil
M. S. BrassescoFaculty of Philosophy, Sciences and Letters at Ribeirão Preto,University of São Paulo, São Paulo, Brazil
X. Zhen :Y. ShenGenetic Diagnostic Laboratory, Department of Laboratory Medicine,Children’s Hospital, Boston, USA
A. C. dos SantosDivision of Radiology, Faculty of Medicine of Ribeirão Preto,University of São Paulo, São Paulo, Brazil
L. NederDepartment of Pathology, Faculty of Medicine of Ribeirão Preto,University of São Paulo, São Paulo, Brazil
X. ZhenDepartment of Obstetrics and Gynecology, Peking University,Third Hospital, Beijing, China
R. S. OliveiraDivision of Pediatric Neurosurgery of the Department of Surgeryand Anatomy, Faculty of Medicine of Ribeirão Preto,University of São Paulo, São Paulo, Brazil
E. T. Valera (*)Departamento de Pediatria, Hospital das Clínicas da Faculdade deMedicina de Ribeirão Preto—USP, 7 andar. Av. Bandeirantes, 3900.Bairro Monte Alegre, 14048-900 Ribeirão Preto, SP, Brazile-mail: [email protected]
Childs Nerv Syst (2013) 29:2151–2155DOI 10.1007/s00381-013-2283-5

The disorder is complex, and at least 11 genes are implicatedin its pathogenesis [1].
The prevalence of MWS is currently unknown, but it islikely that the syndrome is underdiagnosed, particularly inpatients without HD. Patients with clinically typical MWSalmost always have whole gene deletions or truncating muta-tions (nonsense or frameshift) of ZEB2 , suggesting thathaploinsufficiency is the basis of MWS pathology. No obviousgenotype–phenotype correlation could be identified so far [2].
To our knowledge, there are no descriptions of an associ-ation between Hirschsprung's disease or Mowat–Wilson Syn-drome and central nervous system tumors, although CNSanomalies are commonly associated to MWS. We present amolecularly confirmed MWS patient with two different CNStumors, which occurred within a 10-year interval.
Clinical report
A 5-year–11-month-old Brazilian male, born at term of a non-consanguineous marriage, with a birth weight of 2.5 kg via anuneventful spontaneous vaginal delivery was referred to thePediatric Gastroenterology Service for evaluation due a
diagnosis of Hirschsprung's disease. The patient had severeconstipation since neonatal period and had already performedabout six surgical interventions, including excision of a largeaganglionic segment of the colon and a part of the smallintestine. He was still very symptomatic at admission untilan ileostomy was performed.
The patient was observed to be hypotonic, globally de-layed, and dysmorphic. His weight was below third percentile,his height was below tenth percentile, and the head circum-ference was below the third percentile. He had sparse, coarsehair, hypertelorism, thick eyebrows, a saddle nose with prom-inent rounded nasal tip, prominent columella, telecanthicfolds, posterior low set ears with uplifted ear lobes, longtapered fingers, and a prominent pointed chin. He also showeddelayed developmental milestones, mainly significant speechdelay. Additionally, the patient presented a hyperactive behav-ior. Heart auscultation was normal, and an echocardiogramshowed no structural heart defects. Cytogenetic analysis withG-banding showed a normal karyotype.
At 3 years of age, he developed afebrile seizures and wascommenced on phenobarbital, which brought his epilepsy undercontrol. Cranial magnetic resonance imaging (MRI) did notshow structural anomalies like callosal agenesis, but revealed
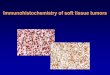
Fig. 1 BrainMRI from July 1, 2002 showing posterior fossa neoplasm inthe forth ventricle related with the cerebellar vermis. The lesion washeterogeneous, highly cellular with intense and heterogeneous enhance-ment following the intravenous administration of gadolinium-based con-trast material. The histopathology diagnosis was medulloblastoma. At the
top are one sagittal pre-contrast T1-weighted image (a) and two axialslices, a T2-weighted (b) and a T2-FLAIR imaging (c). At the bottom, d ,e , and f are T1-weighted images after gadolinium injection acquired witha whole brain volumetric MPRAGE sequence with reconstruction in thesagittal, axial, and coronal planes
2152 Childs Nerv Syst (2013) 29:2151–2155

an expansive mass in forth ventricle, isointense in T1 ponderedsequences and hyperintense in T2 sequences with heterogeneousenhancement (Fig. 1). A radical resection was performed, andthe anatomopathological results depicted a medulloblastomagrade IV according to World Health Organization (WHO)
classification. The patient was submitted to radiotherapy (3,600 cGy in the craniospinal region and a boost of 1,800 cGyin the posterior fossa) and chemotherapy (8 cycles of cisplatin,CCNU, and vincristine). After treatment, he was followed by7 years with no evidences of relapse and then he lost follow-up.
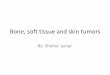
Fig. 2 BrainMRI fromMarch 6, 2012 showing posterior fossa neoplasmin the right cerebellar hemisphere. The lesion is heterogeneous withintense and heterogeneous enhancement following the intravenous ad-ministration of gadolinium-based contrast material. The histopathologydiagnosis was glioblastoma. At the top is shown three axial images (a) is
a T2-weighted, (b) is a pre-contrast T1-weighted, and (c) is a T2-weight-ed slice at the thalamus level. At the bottom, d , e , and f are T1-weightedimages after gadolinium injection acquired with a whole brain volumetricMPRAGE sequence with reconstruction in the axial, sagittal, and coronalplanes. The arrows point the neoplasm
Table 1 Primers used for ampli-fication and sequence of codingexons of Zeb2
For exons 2–7 and 9 and 10, usethe same amplification primers
Exon Primer forward Primer reverse
2 AAG TTT CGC TTT GGC GTT G CTCGGTTCCTTTTCCCTTTC
3 TTAGGGGTGGCTGATGTTTC ATTCTGCAAGGGCTCAATGG
4 TTCCTTGTTCCTGTGCTTGG TCACTGTTTCCTTCCCTGCC
5 TCTCACTGGCTATGATGGAG AACACCCAGGCATGTAGTGC
6 GCAGTGATTCCTGTCATACC ACACTCATTCGATCGTGAAC
7 GCAACTCTGAAAGACTGAGC TCAGGCACACAGAGTTGATG
8 GAGGTACCCCATTGTGTTCC AGTGATCCACTGTTTCATCC
8-seq1 ATGAATGGTGGGCTTGGAGC TGACTCACTACCGGAAGACC
8-seq2 CCTAATATTCCGCCTGTCGG CAGCAGTTCATCGGAGTTGG
8-seq3 ATGACAAGCCCCATCAACCC AGTCCTGGGTATGGTCGTAG
8-seq4 CCCAGTGTTCAGCATGAACC AGTGATCCACTGTTTCATCC
9 TGAGGTTCTCCAAATGTCCC CTTATGTTGCACAAGTGTGC
10 ACGCTTATGCCTGAGTCTGG CATCCTCGCCTTCTTTCTCG
Childs Nerv Syst (2013) 29:2151–2155 2153

Ten years after MB treatment, he presented with difficultiesto swallow and walking and uncontrolled seizures. A newMRI showed a mass in posterior fossa and a new tumor inleft temporal lobe (Fig. 2). A biopsy revealed a glioblastoma(GBM) grade IV (WHO). Due to large tumor extension, nosurgical resection was performed. The child started withtemozolomide. He died 10 months from GBM diagnosis dueto infectious complications.
Genetic testing
This study was approved by the Research Ethics Committeeof the Clinical Hospital of the Faculty ofMedicine of RibeirãoPreto—USP (proc: 6591/2007). Genomic DNAwas extractedfrom whole blood and tumor samples. The complete codingregions of ZEB2 were amplified by polymerase chain reactionusing specific primers (primers used for amplification andsequence are shown in Table 1). Ampliconwere purified usingexonuclease 1 and alkaline phosphatase and sequenced on anABI 3370 automated sequencer. The results of sequence werecompared with the standard sequence from Genbank(NM_014795.3). In exon 8, a heterozygous nonsense muta-tion (c.1381C>T/p.Gln461Stop) was detected both in bloodDNA and tumor DNA (nomenclature according to the HGVSguidelines; http://www.hgvs.org/mutnomen/, Fig. 3). To ourknowledge, this mutation has not been previously reported.
Discussion
In the present report, we describe a pediatric patient withMWS that developed asynchronous CNS tumors of two dif-ferent histologies. MWS is a relatively new clinical entity andmay be an underdiagnosed syndrome. It is characterized bytypical facial features, moderate-to-severe mental retardation,epilepsy, and variable congenital malformations includingHD. However, a meticulous search for previous reports didnot show any case of MWS in association with CNS tumors.
Although nonsense mutations account for more than 40 %of known ZEB2 mutations and approximately 50 % of these
are localized in exon 8 [5–7], the particular mutation detected inthe patient described in this paper has not been reported before.The ZEB2 gene encodes for SIP1 (Smad-interacting protein 1,SMADIP1), a zinc finger/homeodomain transcriptional repres-sor. ZEB2 mRNA is detected in nearly all human tissues, butclinical features suggest that the ZEB2 gene is involved in thedevelopment of neural crest-derived cells, central nervous sys-tem, heart septation, and midline development [2, 5]. Thesequence variant identified in both patients' constitutionalDNA and tumor DNAwas a heterozygous nonsense mutation(c.1381C>T/p.Gln461Stop) which is predicted to result in atruncated protein. This loss-of-function mutation is consistentwith the known molecular mechanism of MWS.
Our patient developed two different brain tumors in a 10-year interval. The first neoplasia (MB) was treated with aregimen that contained craniospinal radiotherapy. The secondtumor was an aggressive high-grade glioma (GBM) that oc-curred 10 years later. One of the most serious consequences oftherapy for childhood cancer is the development of secondmalignant neoplasms, particularly following radiotherapy [4].In order to define if a second tumor is actually a radiation-induced second malignancy, some criteria needs to be fulfilled:(1) the second tumor must occur within the field of radiother-apy, (2) tumor must not be present prior to irradiation, (3)histological differences between tumors must be evident, and(4) the child must not have a genetic disease (such as neurofi-bromatosis type II or others) or a predisposing condition tosecondary malignancy. Although criteria from one to three areall fulfilled in this index case, the phenotypically and molecu-larly diagnosis of MWS precludes a definite diagnosis of aradio-induced secondary malignancy in this setting.
There is no specific treatment for MWS, and the frequentpresence of serious congenital malformations requires preco-cious clinical investigation and intervention by many differentspecialists [5]. This case report raises a putative association ofMWS with childhood brain cancer. Whether MWS may beper se a genetic condition predisposing to brain cancer in thepediatric population needs further appraisal.
Acknowledgments This study was financially supported by FAPESPprocess number 2010/15717-0.
Fig. 3 Heterozygous C to T transversion in blood DNA and tumor DNA
2154 Childs Nerv Syst (2013) 29:2151–2155

Conflict of interest All authors have no conflict of interest to declare.
References
1. Amiel J, Lyonnet S (2001) Hirschsprung disease, associated syn-dromes, and genetics: a review. J Med Genet 38(11):729–739
2. Balasubramaniam S, Keng WT, Ngu LH, Michel LG, Irina G (2010)Mowat-Wilson syndrome: the first two Malaysian cases. Singap Med51(3):e54–e57
3. Evans E, Einfeld S, Mowat D, Taffe J, Tonge B,Wilson M (2012) Thebehavioral phenotype of Mowat-Wilson syndrome. Am J Med GenetA 158A(2):358–366
4. Galloway TJ, Indelicato DJ, Amdur RJ, Swanson EL, Morris CG,Marcus RB (2011) Favorable outcomes of pediatric patients treatedwith radiotherapy to the central nervous system who developradiation-induced meningiomas. Int J Radiat Oncol Biol Phys 79(1):117–120
5. Garavelli L, Mainardi PC (2007) Mowat-Wilson syndrome. OrphanetJ Rare Dis 2:42
6. Ishihara N, YamadaK, YamadaY,Miura K, Kato J, Kuwabara N, HaraY, Kobayashi Y, Hoshino K, Nomura Y, Mimaki M, Ohya K,Matsushima M, Nitta H, Tanaka K, Segawa M, Ohki T, Ezoe T,Kumagai T, Onuma A, Kuroda T, Yoneda M, Yamanaka T, Saeki M,Segawa M, Saji T, Nagaya M, Wakamatsu N (2004) Clinical andmolecular analysis of Mowat-Wilson syndrome associated withZFHX1B mutations and deletions at 2q22 q24.1. J Med Genet 41(5):387–393
7. Moore SW (2006) The contribution of associated congenital anoma-lies in understanding Hirschsprung's disease. Pediatr Surg Int 22(4):305–315
8. Moore SW (2011) Hirschsprung's disease and the brain. Pediatr SurgInt 27(4):347–352
9. Mowat DR, Croaker GD, Cass DT, Kerr BA, Chaitow J, Adès LC,Chia NL, Wilson MJ (1998) Hirschsprung disease, microcephaly,mental retardation, and characteristic facial features: delineation of anew syndrome and identification of a locus at chromosome 2q22-q23.J Med Genet 35(8):617–623
Childs Nerv Syst (2013) 29:2151–2155 2155