Embed Size (px)
Citation preview

Moving to the Futureor the past decade, the University ofTennessee, Public Health NutritionProgram faculty have used Moving to
the Future as one of the guidingdocuments to train graduate students inthe areas of community assessment,program planning, and evaluation. It notonly provides the didactic foundationabout how to complete these essentialpublic health nutrition services, but also
includes forms, practical tips andguidelines that allow students to modifydocuments to conduct specific andtargeted community assessments, developprogram plans, and develop goals andobjectives for evaluation. Studentsenrolled in a Public Health Nutritiongraduate course, Nutrition Interventions inthe Community, have completedcommunity nutrition needs assessments inconjunction with the Knox CountyTennessee Health Department, using theweb-based document and downloadableforms. Although these assessments canvary in focus, Moving to the Future allowsstudents to produce in-depth, qualityassessments that subsequently have beenused by health department andcommunity groups to advocate for policychanges and secure funding for improvedaccess to healthful foods in impoverishedcommunities in the county.
Marsha Spence, PhD, MS-MPH, RD, LDNAssistant Professor (Research),Department of Nutrition, Universityof Tennessee.
Community Health Assessments:A Tool for Successful Planning Karen L. Probert, MS, RD
or many years, a community healthassessment was an obscure functionoften relegated to a student or an
intern. Now we find ourselves asking,“Who isn’t doing a community healthassessment?” The topic made it onto theagenda of the American Health LawyersAssociation Annual Meeting in 2011,1 andnow we can find a news story about alocal hospital’s community health needs
assessment results along side anannouncement to close the hospital’smaternity ward.2 For those who haveadvocated for the need to conductcommunity health assessments for manyyears these are exciting times.
Community health assessment is a hot topicCommunity assessment is a principlefoundation of dietetics, communitynutrition, and public health nutrition.3
WINTER 2013Inside this issue:
1 Moving to the Future1 Community Health
Assessments: A Tool forSuccessful Planning
5 Online Peer Counseling (OPC)-A Cutting Edge Approach toLactation Support
7 Using Assessment to GuidePolicy and Make PracticeChanges in the Nutrition andPhysical Activity Environmentsof Family Child Care Homes
9 Diabetes Assessment inMilwaukee’s American IndianCommunity
11 Listeria Monocytogenes andPregnancy
12 Student Spotlight13 The Phillips Neighborhood
Clinic: Addressing HealthDisparities in CentralMinneapolis
14 National Nutrition Month®March 2013
15 In My Opinion18 Community Assessment Tools
and Resources19 Message from the Chair19 2012-2013 Executive
Committee
Ten Essential Public Health Services.http://www.cdc.gov/nphpsp/essentialServices.html.

2 The Digest—Winter 2013
Facts and other information must first begathered before deciding what to do.When conducting a communityassessment, information is gathered tounderstand what is going on in thecommunity. That information is thenused to make changes that will improvethe community’s health.
Currently, there is no standardized,prescriptive process in conducting acommunity health assessment. Eachresource on community assessmentdescribes a process slightly differentthan another resource. This article willprovide information on three entitiesrequiring a community healthassessment in addition to a review ofone resource that describes acommunity assessment that is entirelyfocused on planning community-basednutrition and physical activity programsand services.
Public Health AgenciesThe 2002 Institute of Medicine report The Future of the Public’s Health in the 21stCentury called for an examination of thebenefits of accrediting governmentalpublic health departments.4 The thinkingwas that by accrediting public healthdepartments, the quality andperformance of the public healthinfrastructure would improve. Starting in2004, examination began and includedstakeholder meetings, exploration teams,reports, and beta tests. The end result is avoluntary national public health agencyaccreditation program that has been inplace since September 2011. The PublicHealth Accreditation Board (PHAB) is thenonprofit organization that overseespublic health department accreditation.5
Tribal health departments, state andterritorial health departments, and localhealth departments are eligible to applyfor accreditation.6
One of the prerequisites to seekingaccreditation is completing a communityhealth assessment.7 Further, a communityhealth assessment is one of theaccreditation standards against which ahealth department is measured todetermine accreditation status.8 Ingeneral, conducting a communityassessment, per PHAB guidelines,includes gathering data and information,writing a narrative description, writing ananalysis of the information, anddistributing the community assessmentto partners and the population served.9
The PHAB Standards & Measuresdocument includes a list of models thatcould be used when conducting acomprehensive health assessment.10
The PHAB Standards & Measuresdocument is not prescriptive. Rather itprovides guidance and describes thelevel of documentation required inconducting a comprehensive communityhealth assessment.
Nonprofit HospitalsThrough the Patient Protection andAffordable Care Act of 2010, allnonprofit hospitals are now required toconduct a community health needsassessment every three years. If acommunity health needs assessment isnot conducted the hospital will beassigned a tax of $50,000 per year thatthe hospital is not compliant with thenew requirement. Hospitals are toconsult public health and othercommunity partners with informationrelevant to the health needs of thecommunity served by the hospital.11
Neither the law nor the subsequentregulations have provided much detailon what is included in the communityhealth needs assessment.
Title V, Maternal and Child HealthBlock Grants to StatesFor almost 80 years, the Title V Maternaland Child Health Program has providedfederal funding to states to ensure thehealth of our Nation’s mothers, women,children, and youth.12 And since the1980s, state Maternal and Child Healthprograms have been required to conducta state-wide, comprehensive needsassessment every five years.13 Theintended outcomes of the state-wideneeds assessments are to improve healthoutcomes for the maternal and childpopulations, and to strengthenpartnerships with the Federal Maternaland Child Health Bureau (MCHB), thestate department of health, and otheragencies and organizations with aninterest in the maternal and childpopulations.14
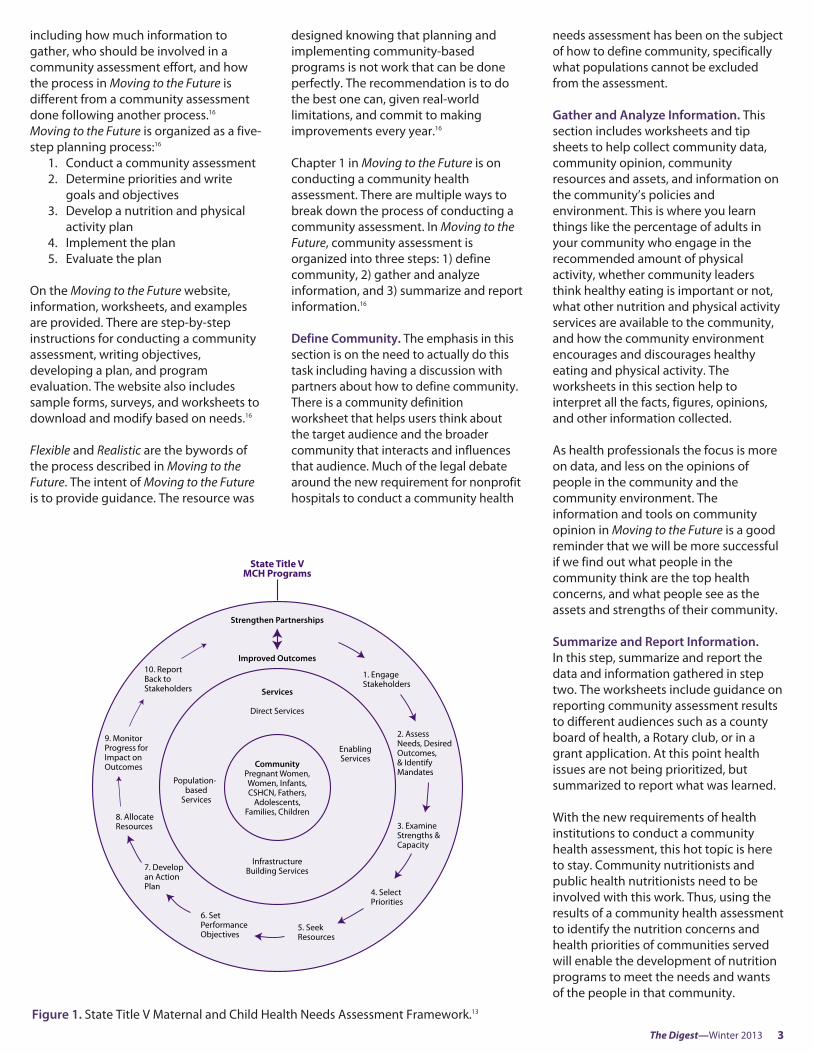
The MCHB is the federal agency thatoversees the Title V, Maternal and ChildHealth Block Grants to States. Theconceptual framework for the Title VNeeds Assessment process is shown inFigure 1 on the following page.13 It liststen steps that states are encouraged tofollow when conducting the Title V NeedsAssessment:
Step 1: Engage stakeholdersStep 2: Assess needs and identify desired
outcomes and mandatesStep 3: Examine strengths and capacityStep 4: Select prioritiesStep 5: Seek resourcesStep 6: Set performance objectivesStep 7: Develop an action planStep 8: Allocate resourcesStep 9: Monitor progress for impacts on
outcomesStep 10: Report back to stakeholders15
This quick review of three entitiesrequiring community assessmentdocuments the importance of knowinghow to conduct a community healthassessment. There are several resourcesthat outline how to conduct a communityhealth assessment (see the CommunityAssessment Resource List). Every resourceavailable on conducting a communityhealth assessment will describe theprocess differently. While the globalprocess is essentially the same, eachresource may organize the details a littledifferently. However, every resource hasthe same end goal—a plan of action toimprove the community’s health status.In general, most resources on how toconduct a community health assessmentwill include these three steps: gatherinformation, analyze information, andreport information. Some resources willadd steps such as form a team, or stepsthat are based on the informationgathered such as determine priorities,write goals and objectives, or develop aplan.
Community assessment resource:Moving to the FutureThe rest of this article will elaborate on aprogram-planning resource entirelyfocused on nutrition and physical activity.The resource, Moving to the Future:Nutrition and Physical Activity ProgramPlanning (Moving to the Future),16
includes specific guidance on how toconduct a community health assessment.
Moving to the Future includes the howand why of conducting a communityassessment. It is an online resourcedesigned to help health professionalsdevelop successful nutrition and physicalactivity programs. It provides tip sheetson specific topics, worksheets, exampleworksheets, and a frequently askedquestions section about conducting acommunity health assessment. Thequestions and answers cover topics
The Digest—Winter 2013 3
including how much information togather, who should be involved in acommunity assessment effort, and howthe process in Moving to the Future isdifferent from a community assessmentdone following another process.16
Moving to the Future is organized as a five-step planning process:16
1. Conduct a community assessment2. Determine priorities and write
goals and objectives3. Develop a nutrition and physical
activity plan4. Implement the plan5. Evaluate the plan
On the Moving to the Future website,information, worksheets, and examplesare provided. There are step-by-stepinstructions for conducting a communityassessment, writing objectives,developing a plan, and programevaluation. The website also includessample forms, surveys, and worksheets todownload and modify based on needs.16
Flexible and Realistic are the bywords ofthe process described in Moving to theFuture. The intent of Moving to the Futureis to provide guidance. The resource was
designed knowing that planning andimplementing community-basedprograms is not work that can be doneperfectly. The recommendation is to dothe best one can, given real-worldlimitations, and commit to makingimprovements every year.16
Chapter 1 in Moving to the Future is onconducting a community healthassessment. There are multiple ways tobreak down the process of conducting acommunity assessment. In Moving to theFuture, community assessment isorganized into three steps: 1) definecommunity, 2) gather and analyzeinformation, and 3) summarize and reportinformation.16
Define Community. The emphasis in thissection is on the need to actually do thistask including having a discussion withpartners about how to define community.There is a community definitionworksheet that helps users think aboutthe target audience and the broadercommunity that interacts and influencesthat audience. Much of the legal debatearound the new requirement for nonprofithospitals to conduct a community health
needs assessment has been on the subjectof how to define community, specificallywhat populations cannot be excludedfrom the assessment.
Gather and Analyze Information. Thissection includes worksheets and tipsheets to help collect community data,community opinion, communityresources and assets, and information onthe community’s policies andenvironment. This is where you learnthings like the percentage of adults inyour community who engage in therecommended amount of physicalactivity, whether community leadersthink healthy eating is important or not,what other nutrition and physical activityservices are available to the community,and how the community environmentencourages and discourages healthyeating and physical activity. Theworksheets in this section help tointerpret all the facts, figures, opinions,and other information collected.
As health professionals the focus is moreon data, and less on the opinions ofpeople in the community and thecommunity environment. Theinformation and tools on communityopinion in Moving to the Future is a goodreminder that we will be more successfulif we find out what people in thecommunity think are the top healthconcerns, and what people see as theassets and strengths of their community.
Summarize and Report Information.In this step, summarize and report thedata and information gathered in steptwo. The worksheets include guidance onreporting community assessment resultsto different audiences such as a countyboard of health, a Rotary club, or in agrant application. At this point healthissues are not being prioritized, butsummarized to report what was learned.
With the new requirements of healthinstitutions to conduct a communityhealth assessment, this hot topic is hereto stay. Community nutritionists andpublic health nutritionists need to beinvolved with this work. Thus, using theresults of a community health assessmentto identify the nutrition concerns andhealth priorities of communities servedwill enable the development of nutritionprograms to meet the needs and wantsof the people in that community.
1. EngageStakeholders
2. Assess Needs, Desired Outcomes,& IdentifyMandates
3. Examine Strengths &Capacity
4. SelectPriorities
6. Set PerformanceObjectives
7. Developan ActionPlan
9. MonitorProgress forImpact on Outcomes
Enabling Services
Direct Services
InfrastructureBuilding Services
Services
State Title VMCH Programs
Population-based
Services
8. AllocateResources
10. Report Back toStakeholders
Strengthen Partnerships
Improved Outcomes
CommunityPregnant Women,Women, Infants,CSHCN, Fathers,
Adolescents,Families, Children
5. SeekResources
Figure 1. State Title V Maternal and Child Health Needs Assessment Framework.13

Author InformationKaren Probert, MS, RD is the ExecutiveDirector of the Association of State &Territorial Public Health NutritionDirectors (ASTPHND) and author ofMoving to the Future: Nutrition andPhysical Activity Program Planning.
References1. American Health Lawyers Association.2011 Annual Meeting Schedule.Healthlawyers.org Web site.http://www.healthlawyers.org/EVENTS/ANNUALMEETING/IHC_AM11/Pages/AM11Schedule.aspx. Accessed February 8,2013.2. Journal Review Online. A Place to Start:Community Health Needs Assessmentreleased. Journal Review Online.http://www.journalreview.com/news/article_b8ea3aee-676a-11e2-9dae-0019bb2963f4.html. Published January26, 2013. Accessed February 8, 2013.3. Dodds J, ed. Personnel in Public HealthNutrition in the 2000s. 2009; 3.http://www.astphnd.org/resource_files/105/105_resource_file1.pdf. AccessedFebruary 8, 2013.4. Institute of Medicine. Committee onAssuring the Health of the Public in the21st Century. The Future of the Public’sHealth in the 21st Century. Washington,DC: The National Academies Press; 2002.5. Public Health Accreditation Board.Public Health Department AccreditationBackground. PHABoard.org Web site.http://www.phaboard.org/about-phab/public-health-accreditation-background/. Accessed February 9, 2013.6. Public Health Accreditation Board.Overview, Who is Eligible. PHABoard.org.Web site. http://www.phaboard.org/accreditation-overview/getting-started/.Accessed February 9, 2013.7. Public Health Accreditation Board.Overview, Getting Started. Public Health Accreditation Board.http://www.phaboard.org/accreditation-overview/getting-started/. AccessedFebruary 9, 2013.8. The Public Health Accreditation BoardStandards & Measures. Volume 1.0.Alexandria, VA: PHAB; 2011:9.9. The Public Health Accreditation BoardStandards & Measures. Volume 1.0.Alexandria, VA: PHAB; 2011:10-19.10. The Public Health Accreditation BoardStandards & Measures. Volume 1.0.
Alexandria, VA: PHAB; 2011:12 and 14.11. The Network for Public Health Law.Issue Brief: New Requirements forNonprofit Hospitals ProvideOpportunities for Health DepartmentCollaboration. The Network for PublicHealth Law.org Web site.http://www.networkforphl.org/_asset/fqmqxr/CHNAFINAL.pdf. Accessed February 9, 2013.12. Health Resources and ServicesAdministration/Maternal and ChildHealth Bureau. Title V Maternal & ChildHealth Services Block Grant Programpage. Health Resources and ServicesAdministration.gov Web site. http://mchb.hrsa.gov/programs/titlevgrants/index.html. Accessed December 20, 2012.13. Health Resources and ServicesAdministration/Maternal and ChildHealth Bureau. Title V Maternal & ChildHealth Block Grant Program NeedsAssessment page. Health Resources andServices Administration.gov Web site.http://mchb.hrsa.gov/programs/needsassessment/index.html. AccessedDecember 20, 2012.14. Health Resources and ServicesAdministration/Maternal and ChildHealth Bureau. Title V Maternal & ChildHealth Block Grant Program NeedsAssessment page. Health Resources andServices Administration.gov Web site.http://mchb.hrsa.gov/programs/needsassessment/index.html. Accessed December 20, 2012.15. Health Resources and ServicesAdministration/Maternal and ChildHealth Bureau. Title V Maternal & ChildHealth Block Grant Program NeedsAssessment page. Health Resources andServices Administration Web site.http://mchb.hrsa.gov/programs/needsassessment/index.html. Accessed December 20, 2012.16. Probert, KL. Moving to the Future:Nutrition and Physical Activity ProgramPlanning. Johnstown, PA: Association of State and Territorial Public HealthNutrition Directors; 2006.http://www.movingtothefuture.org/.Accessed December 15, 2012.
4 The Digest—Winter 2013
Share your expertiseand success!
Let other Public Health/Community Nutrition PracticeGroup members know what youare doing, how well it works,and how it is done. Considerwriting an article or a shortdescription of a program,community or school-basedintervention or curriculum thatyou are involved in.
Please include the followinginformation with yoursubmission: written permissionto print the article in thenewsletter that is signed by all authors; names, credentials,affiliations, and preferredaddresses for all authors;copyright permission for anymaterials that have beenpreviously published or are the work of a person whois not listed as an author;references written according tothe Journal of The Academy ofNutrition and Dieteticsguidelines; and the name,telephone number, fax number,and e-mail address for thecorresponding author.Submissions can be sent to Jessica Barron,Newsletter Editor [email protected].

The Digest—Winter 2013 5
Phyllis S. Crowley, MS, RD, IBCLC; Kierstin Holmgren, Dietetic Intern, Utah State University
mproving the health of mothers andtheir children is a goal of the Centersfor Disease Control and Prevention
(CDC).1 Protecting, promoting, andsupporting breastfeeding, with its manyknown benefits for infants, children, andmothers, are key strategies toward thisgoal. Support for breastfeeding has alsobeen a priority of the SpecialSupplemental Nutrition Program forWomen, Infants and Children (WIC)—which provides 9.2 million individuals inthe United States with nutritious food,nutrition education, support, andhealthcare referrals—since the programbegan in the 1970s.2 Throughout theyears breastfeeding rates have gone up,with increases of about 2 percentagepoints. When comparing the 2008 to2009 rates, breastfeeding initiationincreased from 74.6% to 76.9% andbreastfeeding at 6 months increasedfrom 44.3 % to 47.2%, whilebreastfeeding at 12 months increasedfrom 23.8% to 25.5%.1 This increase ininitiation represents the largest increaseover the previous decade from 1990-1999. This may be due, in part, toincreased awareness of the importance ofbreastfeeding, health benefits, andeducation-based programs.3
Breastfeeding rates among low-incomewomen, however, are much lower thanthose in higher socioeconomic groups.4
These statistics indicate the importanceof increased education opportunities formothers and families which are beneficialfor the promotion and maintenance ofbreastfeeding.
Breastfeeding peer counselors are a greatway of increasing and encouragingwomen to breastfeed while alsoproviding essential education formothers.4 Breastfeeding peer counselorsare not professionals, rather they arepeers with breastfeeding experience whohave been selected from a targetbreastfeeding population to providemom-to-mom support in a non-threatening, informal manner.Breastfeeding peer counselors help
women before, during, and afterpregnancy to increase the number ofmothers who decide to breastfeed andcontinue to breastfeed for a longerperiod of time than mothers who do notreceive peer counseling.
Numerous studies have shown that ratesof breastfeeding initiation andmaintenance have increased among allpopulation sectors over the past decade,including low-income groups.5-7 Providingwomen with adequate information aboutcommon breastfeeding obstacles such assore nipples, low milk supply, illness, andreturning to work/school whilecontinuing to breastfeed, in addition toaccess to a lactation consultant duringthe early postpartum period may helpthem to overcome barriers that stopthem from breastfeeding their child.5 Arecent review of breastfeeding strategiesshowed that a greater proportion oflactating women, who receivedprofessional support, continued tobreastfeed at 6 months compared tothose who did not receive professionalsupport.6 A study in the United Statesreported that peer counselors cansignificantly improve breastfeedinginitiation rates and have an impact onbreastfeeding rates at 1 and 3 monthspostpartum.5 Another study comparedinfant feeding practices of women whoplanned to breastfeed and receivedsupport from counselors to women whodid not receive support from counselors.7
Women in the counselor group hadsignificantly greater breastfeedinginitiation (93% vs. 70%), exclusivity (77%vs. 40%), and duration mean of 15 weeksvs. mean of 8 weeks than women in theno-counselor group.7 Mother-to-mothersupport has also been proven to be oneof the most successful approaches toencourage mothers to breastfeed theirbabies. WIC estimates that women whoattend breastfeeding support groups aretwice as likely to plan to breastfeed asthose who do not.8
A Cutting Edge ApproachThe United States Department ofAgriculture (USDA) Loving Support©Makes Breastfeeding Work campaignbegan in 1997 and was enhanced in later
years for the purpose of implementing astandardized campaign that was nationalin scope, but with implementation at thestate level.9 The USDA Loving Support©campaign included public awarenessmaterials, print materials, promotionalliterature, training, counseling skillsdevelopment, as well as technicalsupport with the goals of encouragingWIC participants to initiate and continuebreastfeeding. This campaign alsoincreased the public’s acceptance andsupport of breastfeeding, while providingtechnical assistance to state and localWIC staff who are promoting andsupporting breastfeeding.10 The SurgeonGeneral’s Call to Action also recommendsadopting new strategies that useelectronic communication such as socialnetworking sites and mobile messagingto communicate health information tofamilies.
Consistent with this recommendation,the Utah WIC Program partnered withwichealth.org (an online nutritioneducation service for state WIC agenciesacross the nation) in 2010. Thispartnership resulted in the submission ofa proposal to USDA for the developmentof a cutting edge approach using anonline application. The online applicationallows Utah WIC Breastfeeding PeerCounselors to connect with Utah WICparticipants who are breastfeeding andneed lactation support with theirquestions and lactation problems, viawichealth.org. Two years later, USDAapproved the Utah WIC Program PolicyGuidance for piloting this new OnlinePeer Counseling (OPC) application in twolocal Utah WIC Agencies (Salt LakeCounty and Tooele County). Crucial toobtaining USDA approval for piloting theOPC application was the ability to ensurethat it was highly secure, thus reducingthe possibility of data breaches, whichcould compromise WIC participantconfidentiality. The Utah WIC Programand wichealth.org decided to use thehighly secure and HIPPA compliantGoToMeeting™ service for connecting thepeer counselors with breastfeedingmothers. It was also important to marketthis OPC service as an expansion of thetraditional Utah WIC Peer Counseling
Online Peer Counseling (OPC)—A CuttingEdge Approach to Lactation Support

6 The Digest—Winter 2013
Program, rather than a replacement ofthe current program which allows peercounselors and WIC participants toconnect face-to-face in WIC clinicappointments, in the home, in thehospital, or via phone contacts.Expanding access to Utah WIC PeerCounselors by going online will openaccess to the provision of lactationsupport outside the standard WIC clinichours, with the intention of providingmore real time support at the moment itis needed to support continuation ofbreastfeeding and prevention ofcessation.
Utah WIC Program OPC PolicyGuidance FrameworkThe Utah WIC Program OPC PolicyGuidance, approved by USDA, wasessential in providing a framework ofpolicies and procedures for the Salt LakeCounty and Tooele County WIC staffs topilot the OPC application with confidence.This guidance was incorporated into theUtah WIC Program Policy and ProcedureManual, Section K.6 entitled BreastfeedingPositive Peer Influence. This policyintroduction states: “An additional optioninvolves participation in the Utah WICOnline Peer Counselor (OPC) programwhich is voluntary.” This additionalresource to an online peer counselor willadd a new dimension for expanding peercounselor services to all Utah WICparticipants, especially in more ruralareas. This is important because access toa peer counselor is often limited by eitherthe lack of peer counselor availability orthe inability to drive 50 miles or more to aWIC clinic to meet directly with a peercounselor. It will also allow for socialsupport and networking in which theOnline Peer Counselors can meet withtheir WIC participants in one-on-one orgroup settings using private and secure
video conference rooms viaGoToMeeting.™ The video conferenceroom calls will be used for demonstratingbreastfeeding techniques, sharing ideasand providing valuable peer counselingservices to Utah WIC participants whochoose to participate. This expansion, viaan OPC, closes certain gaps in the UtahWIC Peer Counselor Program and meetsthe USDA goal of making peer counselorservices broadly available and within apermanent infrastructure framework.9 It isrequired that local WIC staff educate WICparticipants who are interested in theUtah WIC OPC program about usingprofessional language at all times whencommunicating within the videoconference rooms.”12 The Utah WICProgram and wichealth.org anticipate thecompletion of the OPC pilot by thesummer of 2013, with subsequentimplementation in all interested localUtah WIC agencies shortly thereafter.Evaluation data and reports will begenerated to assess the efficacy of thiscutting edge approach for lactationsupport.
For more information about the Utah WICProgram OPC Policy Guidance, pleasecontact Phyllis Crowley at:[email protected].
Author InformationPhyllis Crowley, MS, RD, IBCLC is the statenutrition coordinator for the Utah WICProgram. She has been working inCommunity/Public Health Nutrition since 1986.
References1. CDC. Breastfeeding Report Card—United States, 2012. CDC.gov Web site.http://www.cdc.gov/breastfeeding/pdf/2012BreastfeedingReportCard.pdf.Accessed January 4, 2013.
2. Institute of Medicine. “Front Matter.”Updating the USDA NationalBreastfeeding Campaign: WorkshopSummary. Health Report: Updating theUSDA National Breastfeeding Campaign -Workshop Summary. IOM.edu Web site.http://www.iom.edu/Reports/2011/Updating-the-USDA-National-Breastfeeding-Campaign-Workshop-Summary.aspx.Published 2011. Accessed January 4,2013.3. Sikorski J, Renfrew MJ, Pindorai S, WadeA. Support for breastfeeding mothers: asystematic review. Paediatr PerinatEpidemiol. 2003;17:407-4174. Weimer J Breastfeeding: health andeconomic issues. Food Rev. 1999;2231-35.5. Merewood A, Philipp B. Peer counselorsfor breastfeeding mothers in the hospitalsetting: trials, tributes and tribulations. J Hum Lact. 2003;1972-76.6. Healthy People. Educational andcommunity based programs. HealthyPeople.gov Web site.http://www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=11. Accessed January 4, 2013.7. Kistin N, Abramson R, Dublin P. Effect of peer counselors on breastfeedinginitiation, exclusivity, and durationamong low-income urban women. J Hum Lact. 1994; 10(1): 11-15.8. Central Texas Healthy Mothers, HealthyBabies Coalition. Action Alert! WICBreastfeeding Peer Counselor ProgramMay Be Defunded. CTHMHBC.net Website. http://www.hmhbcentx.net/2012/06/16/action-alert-wic-breastfeeding-peer-counselor-program-may-be-defunded. Accessed January 4,2013.9. USDA. Breastfeeding Promotion andSupport in WIC. USDA.gov Website.http://www.fns.usda.gov/wic/Breastfeeding/mainpage.HTM. Accessed January 4,2013.10. US Department of Health and HumanServices, Office of the Surgeon General. TheSurgeon General’s Call to Action to SupportBreastfeeding. http://www.surgeongeneral.gov. Published 2011. AccessedJanuary 4, 2013.11. Pérez-Escamilla, R. Breastfeedingsocial marketing: lessons learned fromUSDA’s “Loving Support” campaign.Breastfeed Med. 2012, 7(5): 358-63. 12. Approved Utah WIC Program OnlinePeer Counselor Policy Guidance for Pilot,6/12/2012, USDA Mountain PlainsRegional Office.
Save the Dates
Please mark your calendar:
❖ Public Policy Workshop (PPW): March 10-12, 2013, Omni ShorehamHotel,Washington, DC. www.eatright.org/ppw
❖ Academy Food & Nutrition Conference & Expo (FNCE): Houston Texas,October 19-22, 2013. www.eatright.org/fnce
Calendar of Events

The Digest—Winter 2013 7
Doris Fredericks, MEd, RD, FADA
ecent research has focused on theimportant community role thatchild care plays in obesity
prevention.1 In 2010, the State ofCalifornia published a report providingkey recommendations titled KeepingChildren Healthy in California’s Child CareEnvironments: Recommendations toImprove Nutrition and Increase PhysicalActivity.2 The report states: "Children’searly years are critical in shaping theirphysical, emotional, and social well-being. One-third of California’slow-income children enter schooloverweight or obese. Interventions tocurb this obesity epidemic must beginbefore children enter school and beforethey develop poor health habits that leadto overweight and obesity. Child caresettings are ideal environments forpromoting healthy eating habits andphysical activity.”
Behaviors that lead to obesity oftenbegin in preschool and many childrenreach an unhealthy weight even beforethey begin kindergarten.3 Nutrition,physical activity, and screen mediapolicies and practices in the child careenvironment may greatly influence whatchildren eat and do, and can play a keyrole in preventing childhood obesity.4
Establishing policy and improvingnutrition and physical activity practicescan influence and benefit young childrenand families as new children are enrolledfor child care.
The strategies in the report address theneeds of family child care providers tohave guided information and support bythe staff of community agencies withwhom they are familiar in order to makesuccessful changes in their environments.Family child care providers who care forsix to twelve children in their own home,may have less knowledge of nutrition andphysical activity best practices and littleorganizational support for changes intheir home environment.5 Family childcare providers can also be influenced by
organizations that sponsor them on theUnited States Department of Agriculture(USDA) Child and Adult Care FoodProgram (CACFP). With technicalassistance and oversight by the sponsor,a family child care home receivesreimbursement for meals served tochildren in care based upon eligibilitywhich targets higher levels ofreimbursement to low-income areas,providers, or children.6 Research showsthat child care providers in the CACFPalready provide children with morenutritious meals. Additional guidancefrom sponsors can create healthierenvironments for young children infamily child care homes.7
Communities Putting Prevention to WorkIn August 2011, ContinuingDevelopment Incorporated/Choices ForChildren (CDI/CFC), a child care servicesorganization, recieved a 13 month,$90,000 grant from the Santa ClaraCounty California Department of PublicHealth, Communities Putting Preventionto Work, funded by the Centers forDisease Control and Prevention (CDC). Incollaboration with the 4C Council ofSanta Clara County, Inc. (4Cs) the projectaims to support assessment, and makepolicy development and practicechanges in the nutrition and physicalactivity environments of 300 LicensedFamily Child Care Providers, servingapproximately 2500 children, who aresponsored on and participate in theCACFP.
Together CDI/CFC and 4C’s leveraged astaff of six CACFP program monitors,who monitor each of the family childcare home operations three or moretimes per year, one registered dietitian,and three staff with bachelor of artdegree in nutrition. The family child carehomes participating in the CACFP, aresponsored by ether CDI/CFC or 4C’s, andmust follow food pattern andoperational regulations includingattendance at one training provided bythe sponsor per year. This project also
leverages agency resources and existingSanta Clara County obesity initiativeswhich include: Be Sugar Savvy: ReThinkYour Drink Campaign,8 5 Keys to Raising aHealthy Happy Eater parenting class,9
Share Our Strength’s—Cooking Mattersfor Child Care Professionals class,10 andChildhood Feeding Collaborative.11
The PopulationOf the 300 participating family child carehomes, 73% were at the Tier 1reimbursement rates, meaning the sitesare in the geographical areas of schoolswith 50% or more free and reduced pricemeals. An additional 7% qualified for Tier1 reimbursement with familiesparticipating who are below the 185thpercentile for poverty. Based onrace/ethnicity data collected throughagency CACFP enrollment forms, 44% areHispanic, 19% Asian, 5% AmericanIndian/Pacific Islander, and 29%Caucasian. Data from the Santa ClaraCounty, Early Childhood ObesityPrevention Strategic Plan, 2008-2013,indicated that children under the age of 6years who were overweight by ethnicityincluded 16.2% African American, and13.5% Hispanic.12 Some factorscontributing to overweight among thesechildren are foods high in calories, sugarand fat, the number of hours watching TV,and physical inactivity. These factorshighlight the need for early preventionactivities where children spend most oftheir waking hours with caregivers.
Child Care Assessment Tool Project staff used the Self-AssessmentQuestionnaire (SAQ), a list of 35 bestpractices for child care nutrition andphysical activity environments, and BestPractices for Child Care Nutrition andPhysical Activity Environment, a guide forself-assessment and policydevelopment.13 The SAQ and BestPractices Manual were designed to beused by child care center directors, staff,and family child care providers to helpplan, implement, and assure consistentnutrition and physical activity practices.13
The SAQ is divided into four categories:
Using Assessment to Guide Policy and MakePractice Changes in the Nutrition and PhysicalActivity Environments of Family Child Care Homes

8 The Digest—Winter 2013
1) nutrition: feeding practices includingdivision of responsibility; 2) nutrition: foodserved; 3) physical activity and active playpractices; and 4) caregiver and parenttraining. Statements in the nutrition:feeding practices including division ofresponsibility, physical activity and activeplay practices, and caregiver and parenttraining categories, can be answered bychoos ing one of the four options: alreadydoing, making progress in doing,planning to do, and not planning to do.Statements in the category, nutrition:food served, reflect common foods servedin child care that are of particular concernor significance, for example, quantity ofjuice and whole grains. The answers tothese statements reflect frequency oftimes served, or types of products, suchas milk, served to children two-years andolder. After each family child careprovider completed the SAQ, programstaff brought together groups for a one-hour session to discuss strengths and weaknesses of the existing nutritionand physical activity environment asidentified in the assessments.
Nutrition staff conducted an additionalone hour individualized support sessionat each family child care home to provideguidance in reviewing their individualassessment, identifying best practices toadopt, and writing policies to enforcethose changes. The assessment providedthe data for each family child careprovider to determine which new policieswould be written and implemented toimprove the nutrition and physicalactivity environment. Written andimplemented policy is a measurement ofquality in child care.
Using results of the assessment, providersselected at least two physical activity bestpractices, and included 60 minutes ofstructured physical activity per day. Inaddition, they selected a minimum of twonutrition feeding practices and wererequired to include two items under thebest practices for food served, providinglow-fat/non-fat milk at meals/snacks andwater available throughout the day.During the remainder of the year, staffdocumented and reviewed progress ofeach family child care provider when theywere on a CACFP monitor visit. Projectstaff developed and provided ongoingtargeted technical assistance to eachfamily child care provider. Resources,training and technical assistance tosupport the identified changes were
provided by both project nutritionistsand CACFP monitors to help supportsuccess.
AccomplishmentsA total of 278 family child care providers,serving 2,870 children, finished the oneyear project. Each provider completed anidentical follow-up assessment (SAQ)which allowed the project to evaluatechanges and improvements in all fourdomains. Based on the mandatory bestpractices, the important health relatedgoals the project accomplished included:child consumption of 1% or non-fat milkas the served beverage at child caremeals and snacks, child increasedconsumption of water during the day,and child increased structured physicalactivity to one hour per day in care.
Additional analysis of changes in the bestpractices implementation, identified thatin the nutrition: feeding practicesincluding division of responsibilitycategory, a majority number of providers(53%), were implementing family styledining, and 33% selected the response,“making progress doing.” In the categorynutrition: food served, a decrease from20% to 5% reported serving juice twicedaily. In a post analysis, data revealedthat 40% of providers limited juice alltogether. Under the physical activity andactive play practices category; there was a9% increase in the providers whorestricted screen time. An overall majorityof providers indicated that they usedmedia time for educational purposes.This information is consistent with one ofthe Let’s Move Child Care goals todecrease screen time.
Beginning with assessment, this projectincreased healthy eating and physicalactivity by improving the feedingmessages and role modeling for childrenand their families, encouraged healthierfoods served, and created healthierfeeding and physical activityenvironments. The combined strategy, ofsupporting policy development andenvironmental changes establishedsystemic changes in family child carepractices and in the operation of theCACFP. The extensive hours that childcare providers spend with young childrenin care make their example and theenvironment they provide, crucial to thehealth and well-being of children.
Author Information Doris Fredericks, MEd, RD, FADA is theExecutive Director for CDI/Choices ForChildren and co-founder of the SantaClara County, CA, Childhood FeedingCollaborative. She is the developer of the“5 Keys to Raising a Healthy Happy Eater”class and has implemented that parenteducation in the county.
References1. Larson N, Ward DS, Neelon SB, Story M.What role can child-care settings play inobesity prevention? A review of theevidence and call for research efforts. J Am Diet Assoc. 2011;111(9):1343-1362.2. California Department of Education,California Health and Human ServicesAgency. Keeping children healthy inCalifornia’s child care environments:recommendations to improve nutritionand increase physical activity. CDE.govWeb site. http://www.cde.ca.gov/ls/nu/he/documents/keepchildhealexecsumm.pdf. Accessed February 13, 2013.3. University of Washington. Child Care &Obesity Prevention. Washington.eduWeb site. http://depts.washington.edu/uwcphn/work/cfs/childcare.shtml.Accessed February 13, 2013.4. Erinosho T, Hales D, McWilliams C,Emunah J, Stanton Ward D. Nutritionpolicies at child-care centers and impacton role modeling of healthy eatingbehaviors of caregivers. J Acad Nutr Diet.2012;112(1):119-124.5. Nahikian-Nelms M. Influential factors ofcaregiver behavior at mealtime: a studyof 24 child care programs. J Am Diet Assoc.1997;97(5):505-509.6. United States Department ofAgriculture. Child & Adult Care FoodProgram. USDA.gov Web site.http://www.fns.usda.gov/cnd/care/.Accessed February 13, 2012.7. Monsivais P, Kirkpatrick S, Johnson DB.More nutritious food is served in child-care homes receiving higher federal foodsubsidies. J Am Diet Assoc. 2011;111(5):721-726.8. Santa Clara County Public Health. BeSugar Savvy Initiative. SSCGOV.org Website. http://www.sccgov.org/sites/sccphd/en-us/Partners/cdip/Pages/Be-Sugar-Savvy-Initiative.aspx. Accessed February 13, 2013.9. Santa Clara County Public Health. “5 Keys to Raising and Healthy HappyEater” Parenting Classes. SSCGOB.orgWeb site http://www.sccgov.org/sites/sccphd/en-us/Residents/HealthyActive/Pages/5-Keys-to-Raising-a-Healthy-

Jennifer Casey, RD, CD
iabetes is becoming moreprevalent among American Indian(AI) and Alaskan Natives (AN) in
the United States and in Wisconsin.1 Inthe United States AI/AN’s are over twiceas likely as non-Hispanic white adults tobe diagnosed with diabetes (16.1% vs.7.1%; 2009).1 In Wisconsin, about 31.5% ofthe AI/AN population has beendiagnosed with diabetes, almost twicethat of the general AI/AN population inthe United States.1 Diabetes is a major riskfactor for heart disease and stroke.1 It isalso the leading cause of kidney failure,nontraumatic lower-limb amputations,and blindness.1
Due to the high rates of diabetes, in 1999,the Gerald L Ignace Indian Health Center,Inc. (GLIIHC), one of 32 urban IndianHealth Service (IHS) clinics across thenation, was established to improve thehealth, peace, and welfare of Milwaukee’surban Indian community through medical,social, mental health, education andoutreach services.2 As part of theseservices, individual and group nutritioneducation classes are provided by thediabetes program coordinator who is alsoa registered dietitian. The diabetesprogram coordinator works with thediabetes team, which is comprised of aregistered nurse, fitness coordinator, andmedical providers. This team is chargedwith improving patient care, teachingcooking classes for diabetes preventionand control, and working with thecommunity on health initiatives. TheGLIIHC’s diabetes program is administeredthrough the IHS Special Diabetes Program
for Indians (SDPI)—a congressionallyfunded grant program to treat andprevent diabetes with over 400participating sites nationwide.3
To better understand the impact diabeteshas in this population, the GLIIHCDiabetes Team adopted the Indian HealthDiabetes Best Practice CommunityAdvocacy for Diabetes Prevention andControl6 (CABP) in mid-2012. Communityadvocacy is one of the 20 IHS bestpractices. The IHS best practices provideevidence-based recommendations andresources that have been “…developedby IHS professionals, that anyone inclinical and community settings can useto implement or improve diabetestreatment and prevention.”4 The CABPincludes five key recommendations fordiabetes prevention and control:
1. Conduct community needsassessments to determine resources,interests, and requirements fordiabetes efforts in the community.
2. Develop partnerships and communityadvocacy groups where people canwork together to improve theircommunity and effectively addressdiabetes prevention and care.
3. Provide community education toincrease awareness of the risk factorsfor diabetes and inform thecommunity that diabetes and itscomplications can be prevented ordelayed through sustained lifestylechanges that result in modest weightloss.
4. Develop a strategic plan. 5. Involve community partners in
participatory evaluation.
GLIIHC’s Community AssessmentAfter adopting the CABP, a CommunityDiabetes Advocacy group was formed toconduct the first ever community needsassessment in the Milwaukee AIpopulation. To better understand theMilwaukee AI community, a scan ofavailable data sets and past assessmentdata was done. This involved reviewingthe Wisconsin Department of Healthstatistics,5 the US Census Bureau6 andAmerican Community Survey data,7
GLIIHC patient demographics, theBemidji Urban Needs Assessment,8
Supplemental Nutrition AssistanceProgram usage information,9 and healthyfood accessibility in Milwaukee County.10
After reviewing data, the CommunityDiabetes Advocacy group beganplanning a community assessment toidentify the interests, resources (e.g.,services, networks, health classes, etc.,)and the perceived barriers, knowledge,and beliefs within the AI community. Dueto limited financial and personnelresources, the group needed to capitalizeon existing relationships, networks,communication channels, and low or nocost survey methods. The diabetesprogram coordinator and the fitnessinstructor began by first talking with theelders who attended the weekly elders’fitness, nutrition, and cooking class. Thisgroup was chosen first because many ofthe elders have diabetes and are alsorespected leaders in the community.Using a talking circle style,* the eldersshared their thoughts on the problemsand solutions to diabetes in the local AIpopulation. Staff members andvolunteers of area AI organizations were
The Digest—Winter 2013 9
Happy-Eater-parenting-classes.aspx.Accessed February 13, 2013.10. Share Our Strength. CookingMatters.org Web site. http://cookingmatters.org/. Accessed February 13, 2013.11. Santa Clara County Public Health.Childhood Feeding Collaborative OnlineTraining. SCCGOV.org Web site.http://www.sccgov.org/sites/sccphd/en-us/healthproviders/cfc/Pages/default.aspx.Accessed February 13, 2013.
12. First 5 Santa Clara County. Earlychildhood obesity prevention: Strategicplan 2008-2013. First 5 kids.http://samuelsandassociates.com/samuels/upload/obesity/5ECOP.pdf. AccessedJanuary 4, 2013.13. California Department of PublicHealth’s Network for a Healthy California,Contra Costa Child Care Council. Bestpractices for child care nutrition andphysical activity environments: a guide
for self-assessment and policydevelopment. http://www.healthybeveragesinchildcare.org/bestpractices/BestPracticesHandbook.pdf. AccessedFebruary 13, 2013.
Diabetes Assessment in Milwaukee’sAmerican Indian Community

10 The Digest—Winter 2013
also interviewed. The following findingswere revealed from the analysis ofinterviews and focus groups: 1) healthdisparities in general and diabetes areserious concerns for individuals in thecommunity; 2) several AI communityorganizations are ready to beginparticipating in diabetes advocacy; 3) barriers such as time, staff, funding,exist; and 4) opportunities are available to strengthen existing partnerships.
Milwaukee AI Diabetes SurveyThe next step of the assessment was todevelop and conduct a survey of the AIcommunity. The Milwaukee AI DiabetesSurvey was developed based on guidancefrom community health experts at theUniversity of Colorado Denver’s Centersfor AI and AN Health. The target group tobe surveyed included GLIIHC and SouthEastern Oneida Tribal Services clients. Thesurvey was used to collect informationabout knowledge, beliefs, interests, andfood access, which includes both physicaland economic access to sufficient food,including traditional native foods. A totalof 56 individuals completed theMilwaukee AI Diabetes Survey. Selectdata from the Milwaukee AI DiabetesSurveysurvey are below:
• 89% responded knowing that Type 2Diabetes can be prevented andcontrolled.
• 91% responded being aware thatNative Americans have the highestrate of diabetes.
• 55.3% either strongly agree orsomewhat agreed that in the past yearthey had trouble affording food.
• 82% responded that they have accessto fruits and vegetables.
• When asked, “What would helpMilwaukee’s AI Community fight Type 2 Diabetes?” Some responsesincluded education and/or outreach,access to traditional native or healthyfoods, youth targeted programs,community collaboration, and accessto transportation.
Lessons LearnedThe GLIIHC Diabetes Program plans tobuild upon this initial assessment. Theassessment yielded some interestingfindings, including, that while the surveyrespondents reported higher use of foodassistance program than the general AIpopulation in Milwaukee (39% comparedto 28.6%)9, they also reported higher thanexpected access to fruits and vegetables(82%).10 Due to the low survey responserate, and the inability to distribute itrandomly, the survey results cannot begeneralized. However, the data providedthe Diabetes team and the communitywith a starting place to design futureinitiative to help prevention and controldiabetes. Future plans include a policyscan as well as a community resourceinventory with asset mapping. Feedbackon this Community Assessment fromCommunity Diabetes Advocacy Groupand individual community members willguide the program planning, includingdesigning key messages for a publichealth information campaign on diabetesprevention and control.
* A talking circle is a method used by agroup to discuss a topic in an egalitarianmanner where every member of thecircle has a chance to speak and isgenerally accepted by native cultures.
Author InformationJennifer Casey, RD, CD oversees theGerald L Ignace Indian Health Center’scommunity-directed Diabetes Program.She provides nutrition education, workswith elders, facilitates a garden program,conducts healthy cooking classes, andworks with community partners to createpositive changes.
References1. Centers for Disease Control andPrevention. National diabetes fact sheet:national estimates and generalinformation on diabetes and prediabetesin the United States, 2011. CDC.gov Website. http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf. AccessedFebruary 8, 2013.2. Gerald L. Ignace Indian Health Center,Inc. Diabetes Program. GLIIHC.net Website. http://www.gliihc.net/Pages/Outreach.aspx. Accessed Feb 8,2013.3. US Department of Health and HumanServices, IHS Special Diabetes Programfor Indians. 2011 Report to Congress:Making Progress Toward a HealthierFuture. http://www.ihs.gov/MedicalPrograms/Diabetes/HomeDocs/Programs/SDPI/2011RTC_Layout_10102012_508c.pdf. Accessed February 8, 2013. 4. Indian Health Services. Indian HealthDiabetes Best Practice CommunityAdvocacy for Diabetes Prevention andControl. IHS.gov Web site.http://www.ihs.gov/MedicalPrograms/Diabetes/HomeDocs/Tools/BestPractices/2011_BP_CommAdvocacy_508c.pdf.Accessed January 30, 2013.5. Wisconsin Department of Health.American Indians in Wisconsin.dhs.wisconsin.gov. Web site.http://www.dhs.wisconsin.gov/health/minorityhealth/mhpop/amindpophlthfact.htm. Accessed January 9, 2013.6. US Census Bureau. Profile of GeneralPopulation and Housing Characteristics:2010. Census.gov Web site. http://factfinder2.census.gov. Accessed Jan 9, 2013.7. US Census Bureau. Selected EconomicCharacteristics:2006-2010. Census.govWeb site. http://factfinder2.census.gov.Accessed January 9, 2013.8. The Urban Indian Health Institute.Bemidji Area Urban AmericanIndian/Alaska Native Needs Assessment,Final Report, March 2009. Urban IndianHealth Institute, Seattle Indian HealthBoard.9. US Department of Agriculture. SNAP.USDA.gov Web site. http://www.fns.usda.gov/snap/. Accessed Jan 9, 2013.10. Hunger Task Force. Twinkies,Tomatoes, and Tomatillos. A QualitativeAssessment of Healthy Food Accessibilityin Milwaukee County.Hungertaskforce.org Web site.http://www.hungercenter.org/wp-content/uploads/2012/08/Twinkies-Tomatoes-and-Tomatillos1.pdfAccessed January 9, 2013.
The views and statementsappearing in The Digest do notnecessarily reflect policies and/orofficial positions of the Academy ofNutrition and Dietetics (Academy) orPublic Health/Community NutritionPractice Group (PHCNPG). Productnames mentioned in thispublication do not constituteendorsement by Academy orPHCNPG. © 2013 PublicHealth/Community NutritionPractice Group, a dietetic practicegroup of the Academy.
The PHCNPG welcomes corporaterelationships that support ourstrategic plans and activities;however, these relationships do notnecessarily indicate endorsement byour membership.
The Digest

Angela Brekken, RD, LD, CLEC
ood safety is an important aspect ofnutrition counseling duringpregnancy. Due to a decreased
immune system during pregnancy,women are 18-20 times more likely tosuffer from food borne illnesses.1-3
However, it is an often overlooked aspectof nutrition counseling duringpregnancy. There is one bacterium that isparticularly dangerous to pregnantwomen and their fetus called Listeriamonocytogenes (L. Monocytogenes).1-9
Listeremia has been found to be moreprevalent in first-time pregnancies due todecreased food safety measures.4
Furthermore, pregnant women carryingmultiple fetuses have an increased risk oftransmission to the fetuses.5
L. monocytogenes is a facultativeanaerobic, small, gram positive, rodshaped, and flagellated bacterium.1-3
It can survive refrigeration, freezing, andcan tolerate high-sodium environments.1-3
It is found naturally in soil and water.2
Food sources that commonly carry the L. monocytogenes bacterium includeunpasteurized milk, soft cheeses, delimeats, hot dogs, pates, meat spreads,smoked seafood, jerky, melons, as well ascommercially prepared hummus, fruitand vegetable spreads.1-3,5, 6
It is estimated that 13% of all L. monocytogenes cases occur in thepregnant population.7 L. monocytogenesinfection can present in the pregnantwoman within 2 to 70 days of ingesting acontaminated food with onset usuallyoccurring by 4 weeks post ingestion.2,5
The manifestations of listeriosis includesepticemia, meningitis, encephalitis, flu-like symptoms, fatigue, muscle pain,and intrauterine or cervical infections inpregnant women.1-3,5,6,8 The latter mayresult in spontaneous abortion duringthe second or third trimester or astillbirth.2,3,9 In infants that survive birth,common manifestations include skinrash, lethargy, meningitis, septicemia,bacteremia, listlessness, fever, andpneumonia.1-3,5,6, 8,9 Successful treatmentinclude parenteral penicillin orampicillin.2,3,9 For patients allergic topenicillin, trimethoprim-sulfamethoxazole has also been reportedto be effective.3
One of the Healthy People 2020 FoodSafety objectives is to decrease theprevalence of listeremia from a baselineof 0.3 infections per 100,000 populationto a goal of 0.2 per 100,000.10 Thishighlights the importance of prenatalnutrition education, especially within theprimipara and multigestationalpopulations. There are various settings inwhich prenatal nutrition education cantake place, such as WIC clinics, inpatientand outpatient medical settings, privatepractice, childbirth education classes,grocery stores, and social media.Registered Dietitians (RDs) can play alarge role in reducing maternal and fetalmortality rates related to L. monocytogensas well as make strides towards meetingthe Healthy People 2020 goals. RD’s canhelp by discussing food safety duringevery pregnancy counseling session orgroup class. This can include educatingmothers about the hazards of thecommon foods that could becontaminated with L. monocytogens andproviding preventive tips such as heatingprocessed meats before consumption,washing fruit, such as melon beforepreparation, and drinking pasteurizeddairy products.1-3,5,6
References1. Harris J. Listeria monocytogenes –which of your patients is not at risk. Aust Nurs J. 2008;16:26-28.2. Bortolussi R. Listeriosis: a primer. Can Med Assoc J. 2008;179(8):795-797.
3. Lamont RF, Sobel J, Mazaki-Tovi S, et al.Listeriosis in human pregnancy: asystemic review. J Perinat Med.2011;39:227-236.4. Trepka MJ, Newman FL, Dixon Z,Huffman FG. Food safety practices amongpregnant women and mothers in thewomen, infants, and children program,Miami, Florida. J Food Prot. 2007;70:1230-1237.5. Jackson KA, Iwamoto M, Swerdlow D.Pregnancy-associated listeriosis.Epidemiol Infect. 2010;138:1503-1509.6. Voetsch AC, Angulo FJ, Jones TF, et al.Reduction in the incidence of invasivelisteriosis in foodborne diseases activesurveillance network sites, 1996-2003.Clin Infect Dis. 2007;44:513-520.7. National enteric disease surveillance:Listeria annual summary, 2010. CDC.govWeb site. http://www.cdc.gov/listeria/pdf/listeria-annual-summary-2010-508c.pdf. Accessed February 11, 2013.8. Bennion JR, Sorvillo F, Wise ME, KrishnaS, Macola L. Decreasing listeriosis mortalityin the United States, 1990-2005. ClinicalInfectious Diseases. 2008;47:867-874.9. Cheung VYT, Sirkin WL. Listeriosiscomplicating pregnancy. Can Med Assoc J.2009;181(18):821-822.10. Food Safety – Listeria Monocytogenes.HealthyPeople.gov Web site.http://healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=14. Accessed February 11, 2013.
Listeria Monocytogenes and Pregnancy
The Digest—Winter 2013 11
PHCNPG is looking for real success stories frommembers with a recent accomplishment.
Community Champions will be featured in The Digest.Share a success story and in so doing, motivate and create enthusiasmamong the PHCNPG membership. Submissions are limited to 300 wordsand can include a photo of the member. Please send submissions to:[email protected]. The time from submission to publicationcan take 3 to 4 months.
Community Championsof PHCNPG

Lindsay Miesel, Dietetic Intern, University of Tennessee, Knoxville
ecently, I had the opportunity to intern in the nutritiondivision at the Boling Center for Developmental Disabilities(BCDD) in Memphis, Tennessee. BCDD is one of more than
60 University Centers for Excellence in Developmental Disabilities(UCEDD) which serves children, youth, and adults withdevelopmental disabilities through training, service, appliedresearch, and policy development. During my internship, mymain project was to conduct a needs assessment to determinegaps in nutrition information and services provided to BCDD’schildren and their families. Conducting an assessment wasimportant to identify the health status of Children With SpecialHealth Care Needs (CSHCN), as well as the types of resources thatwere available to them and their families. Therefore, I used theNational Survey of Children with Special Health Care Needs (NS-CSHCN) and the National Survey of Children’s Health (NSCH) todescribe characteristics of CSHCN in the state of Tennessee. Thisincluded demographic and economic information, as well ashealth status. To assess resources available in the localcommunity, I used Tennessee Department of Health and ShelbyCounty Health Department resources to collect informationrelated to available health programs and services for children andtheir families.
Key FindingsAfter analyzing the data, I learned that according to the 2001,2005-2006, and 2009-2010 NS-CSHCN, there have been statewideand nationwide increases in the prevalence of CSHCN. Betweenthe years of 2001 and 2009-2010, prevalence of CSHCN increasedfrom 14% to 17% in Tennessee, and 13% to 15% nationwide.1
Further, according to the Academy of Nutrition and Dieteticposition paper on nutrition services for people withdevelopmental disabilities and special health care needs, up to90% of CSHCN experience associated nutrition-related needs,including but not limited to failure to thrive, overweight/obesity,and metabolic or digestive issues that complicate nutrientabsorption and utilization.2
Once the assessment was complete, I transitioned to the nextstep of my project, which was to identify gaps in resources forCSHCN. Based on the data, I identified that there was a need todevelop and offer programs and services that address theindividualized physical limitations and nutrition concerns ofCSHCN in a way that is supportive and interdisciplinary. Specificneeds that were identified included the recognition of nutritionas a core health concern for CSHCN, the prioritization of nutritionwithin the provision of health care services for CSHCN, increased
reimbursement of nutrition services for CSHCN by mainstreaminsurance providers, and avenues to increase parent interest andknowledge regarding nutrition for CSHCN. This information waspresented to administration and staff at BCDD and will be usedto raise awareness and hopefully affect future programs andservices in order to improve nutrition among CSHCN.
This community nutrition assessment was invaluable because ittaught me the importance of understanding the population I wastrying to reach. Conducting community assessments allowsregistered dietitians (RDs), dietetic technicians (DTRs), anddietetic interns the opportunity to gather, collect, andaccumulate data in order to determine appropriate and culturallyrelevant nutrition programs and services for the populationbeing served. By assisting agencies, organizations, and clinicswith identifying community resources and identifying needs, ourprofession can better equip these facilities with the knowledgeand tools needed to improve programs and services to thepopulation of interest.
I would like to thank Lee Wallace, MS, RD, LDN, FADA (Chief ofNutrition) and Sarah Sullivan, MS, RD, LDN, for giving me theopportunity to work with them at the Boling Center forDevelopmental Disabilities (BCDD) in Memphis, Tennessee.
Author InformationLindsay is pursuing a dual Master’s degrees in Public HealthNutrition and Public Health with a concentration in CommunityHealth Nutrition at the University of Tennessee, Knoxville. She isalso completing her Dietetic Internship. Her research interestsinclude school nutrition interventions and socio-ecologicalapproaches to combat childhood obesity.
References1. Data Resource Center for Child & Adolescent Health. 2001,2005-2006, 2009-2010 National Survey of Children with Special Health Care Needs. Child health data.org Web site.http://www.childhealthdata.org/browse/survey. AccessedFebruary 2, 2013.2. Van Riper CL, Wallace LS. Position of the American DieteticAssociation: Providing nutrition services for people withdevelopmental disabilities and special health care needs. J Am Diet Assoc. 2010;110(2):296-307.
Student Spotlight
12 The Digest—Winter 2013
Community Assessment: Boling Centerfor Developmental Disabilities

The Digest—Winter 2013 13
Julie Arndt, Carrie Dent, Mikaela Robertson. Graduate students in theCoordinated Masters Program in Public Health Nutrition, University ofMinnesota, Minneapolis
he Phillips neighborhood in the Twin Cities metropolitanarea of Minnesota is home to many recent immigrants andethnic minorities. More than 68% of the community's
residents are non-white compared to 35% citywide.1 Manyresidents of the Phillips neighborhood struggle financially;approximately 38% of all families live below the federal povertyline.2 Since 2003, a student-run free clinic called the PhillipsNeighborhood Clinic (PNC) has provided medical services to arearesidents. In this article, we describe the Phillips neighborhoodand the PNC, with an emphasis on the role of public healthnutrition (PHN) students and preceptors in providing nutritioncounseling services for the clinic.
Food access is an issue for Phillips neighborhood residents;residents experience the second highest prevalence of foodinsecurity in the Twin Cities.3 More than 37% of residentsconsume one or fewer servings of fruit or vegetables in a givenday, and 61% of residents report eating at least one meal outsideof the home per day.4 The neighborhood contains numerouscorner stores and ethnic markets, but only one grocery store.Several grocery stores are located within a short drive of theneighborhood, but more than 60% of area residents do not havereliable access to a car, making it difficult for them to shop atthese stores.3
Residents of the Phillips neighborhood also experience healthdisparities; rates of overweight, obesity, diabetes, andcardiovascular disease are elevated relative to state-level data.More than one third of adult residents are overweight, and 17%are obese. However, nutrition-focused health education isinadequate. When surveyed, less than 25% of residents reportedthey had been told by a doctor that they should lose weight toimprove their health.4 The neighborhood-wide prevalence ofdiabetes is approximately 10%, and the prevalence ofhypertension is 22%, which is considerably higher than the city-wide rates of 5% and 15%, respectively.3, 4
To address the health disparities of the Phillips Neighborhood,Dr. John Song, an assistant professor of medicine and bioethicsat the University of Minnesota (UMN), created the PNC in 2003.6
Dr. Song started the clinic with the mission of providing“accessible, culturally appropriate, interdisciplinary health careservices and education in order to reduce the burdens of poormedical access and raise the quality of life for patients.” Theclinic also provides students in the health professions (publichealth nutrition, medicine, pharmacy, nursing, social work, andphysical therapy) with the opportunity to develop their patientcare skills and interact with a diverse patient population.
For the past five years, the free clinic has operated under thesupervision of Dr. Brian Sick and the student-led PNC board. Tobecome a clinic volunteer, students from each of the
participating health professions are required to apply. Acceptedstudents agree to volunteer at the clinic for a two-year term. Theclinic is open two evenings a week, but the clinic is staffed by arotating roster of students, so that each student works only oneclinic night per month. Students are joined by licensed cliniciansfrom each specialty who supervise the care they provide. Afterthe first year, students can run for positions on the PNC StudentBoard. The PNC Student Board coordinates every aspect of theclinic—managing clinic finances, community relations,operations, and human resources.
The PNC provides access to vital health services for uninsuredand underinsured patients. Services provided by the clinicinclude physical exams, laboratory testing, pharmaceuticalprescriptions and refills, nutrition education, physical therapy,mental health counseling, and assistance with medical assistanceapplication forms. The clinic does not charge for services, labwork, or medications, although those services cost an average of$105 per patient.7 Funds for the clinic come from fundraisingefforts such as concerts, races, auctions, and donations from thehealth profession’s schools participating at the clinic. FairviewHealth Services and UMN physicians are two communitypartners that also play a major role in financing the clinic.6
A defining aspect of the PNC is its multidisciplinary approach toproviding quality medical care to patients. After medical andpharmacy students and preceptors conduct an initial assessmentof each patient, students and preceptors from all participatinghealth professions meet to discuss an appropriate care plan forthe patient. For example, a patient who presents with depressionand hypertension might receive medication for their high bloodpressure, counseling from the mental health team, and nutritioncounseling from the nutrition team.
Nutrition counseling is one of the services provided at the PNC.During the initial consultation, patients are asked if they wouldlike to meet with the nutrition team, which includes a PHNstudent and a Registered Dietitian. Patients who agree to receivenutrition services often have hypertension or diabetes, or areoverweight or obese. Further, because many residents facechallenges that influence their dietary habits and nutritionalstatus (time, money, access to transportation and healthy foodvenues, cultural traditions and beliefs), they have limitedexposure to accurate nutrition information necessary to makehealthy lifestyle changes. These concerns are addressed duringthe preceptor-supervised nutrition counseling. This helps toensure that the nutrition advice is culturally competent, relevant,and appropriate for the clients. Spanish translators are usuallypresent to assist with communication. Students chart the visitusing EPIC medical record software. After the nutritionconsultation, preceptors give students feedback on theircounseling techniques and suggestions for improvement.
PHN students who are involved with the clinic tend to find theexperience informative and rewarding. Working with patients inthe community makes classroom learning more relevant. It
The Phillips Neighborhood Clinic: AddressingHealth Disparities in Central Minneapolis

14 The Digest—Winter 2013
Food preferences, lifestyles, cultural and ethnic traditionsand health concerns all affect food choices. That is why, aspart of National Nutrition Month® 2013, the Academy ofNutrition and Dietetics is encouraging everyone to “EatRight, Your Way, Every Day.”
Each March, the Academy encourages Americans to returnto the basics of healthy eating through National NutritionMonth. This year’s theme emphasizes the advantages ofdeveloping a healthful eating plan that incorporatesindividual food choices and preferences.
Initiated in 1973 as a week-long event, “National NutritionWeek” became a month-long observance in 1980 inresponse to growing public interest in nutrition. This yearthe Academy is celebrating the 40th anniversary of NationalNutrition Month (NNM). For more NNM history, visit “AboutNNM” at www.eatright.org/NNM/content.aspx?id=7832.
To commemorate the dedication of registered dietitians asthe leading advocates for advancing the nutritional status ofAmericans and people around the world, the secondWednesday of each March is celebrated as “RegisteredDietitian Day.” This year marks the sixth annual RegisteredDietitian Day, which will be celebrated March 13.
As part of the campaign, the National Nutrition Monthwebsite, www.eatright.org/nnm, includes a variety ofnutrition tip sheets, recipes, games, a promotional toolkitand catalog, all designed to spread the message of goodnutrition based on the “Eat Right, Your Way, Every Day”theme.
If you have additional questions, please contact MaryUhrick, Project Manager, Academy of Nutrition and [email protected].
National Nutrition Month® March 2013
allows students to integrate and apply their public health,nutrition education, and clinical nutrition skills in one setting.Volunteering at the PNC is also a great way to meet otherdietitians and preceptors. The PNC has served as a model for thedevelopment of other free clinics throughout the United States,and serves as a model training opportunity for public health andcommunity nutrition dietitians.
Table 1. Phillips Neighborhood Demographics.1, 2, 6
References1. United States Census Bureau. 2000 Census. Informationaccessed at Phillips Neighborhood Network. Phillips at a glance.http://www.pnn.org/PNNwebsites/Census2000/home.htm.Accessed December 5, 2012. 2. City of Minneapolis. Phillips community: location and generalcharacteristics. Official Website of the City of Minneapolis.http://www.minneapolismn.gov/neighborhoods/phillips/neighborhoods_phillips_profile_home. Updated 2011.Accessed December 20, 2012. 3. Swingley S. The Northside healthy eating project: Transportationaccess to affordable fresh produce. NorthPoint Health andWellness Center Web site. http://northpointhealth.org/LinkClick.aspx?fileticket=AAw867 IPVrs%3D&tabid=135&mid=845.Updated 2011. Accessed December 20, 2012.4. United States Department of Agriculture. Economic ResearchService. Food security in the US. http://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us.aspx. AccessedFebruary 17, 2013. 5. Hennepin County Human Services and Public HealthDepartment. SHAPE 2010 Adult Data Book, Survey of the Healthof All the Population and the Environment, Minneapolis,Minnesota, March 2011. 6. Phillips Neighborhood Clinic. http://www.phillips.neighborhoodclinic.com/. Updated 2010. Accessed December 19, 2012. 7. Phillips Neighborhood Clinic. Orientation Presentation.University of Minnesota, Minneapolis, MN. Presented October 6,2012.
Population 19,805
Poverty: Percent of all residents withincomes below the federal poverty line
34% (compared to17% city-wide)
Poverty: Percent of all families withincomes below the federal poverty line
38%
Residents without health insurance 34%
Non-white residents 68% (compared to35% city-wide)
Median household income in 1999 $22,044 (comparedto $37,974 city-wide)

The Digest—Winter 2013 15
Implementing the Healthy Hunger Free Kids Act: The Importance of Assessment Maureen Pisanick, RD
The Healthy Hunger Free Kids Act (HHFKA)1, also known as thefirst sweeping changes for the National School Meals Program in15 years, has created a new opportunity for school food servicesnationwide. The new regulations include grade specific rangesfor the main food groups, including fruit, vegetable, grain ounceequivalents, protein equivalents, as well as fluid milk. Specificcalorie and saturated fat ranges capture a window of nutrientdensity that must be achieved while meeting these minimumand maximum requirements. The regulations also include limitson sodium that will be phased in over time.1
As a registered dietitian, how can you best meet the newrequirements while at the same time, keep the kids happy andhealthy? First, start by assessing the current food landscape,specifically focus on aspects required by HHFKA, such as signage,meal components, and student participation. Once assessed,develop a diagnostic plan to move operations forward.
Assessment: Signage, Meal Components, and Student ParticipationSignage. One area of assessment in school nutrition is meetingthe regulation for signage. The law states that all nutritionoperations must provide adequate signage to include whatmenu is being offered, and what components are beingsatisfied.1 MyPlate,2 developed by the United States Departmentof Agriculture (USDA), provides a ready-made and accessibleresource for the color and balance of foods that arerecommended based on the 2010 Dietary Guidelines forAmericans. It is a good first step to organizing, implementing,and communicating changes on the menus of schoolsparticipating in the National School Breakfast and Lunchprograms.
Meal Components. The second area of assessment in schoolnutrition is meeting the regulation for providing daily and weeklymeal components in the appropriate portion and variety.1 TheHealthierUS School Challenge (HUSSC) is an award supported bythe USDA.3 This award credits schools for not only meeting theminimum requirements, but also for setting goals to achieve acommitment to a school-based wellness policy. The applicationprocess comes with a ready-made checklist that includesassessment in the area of the school meals, wellness policy,competitive foods, nutrition curriculum, physical educationcurriculum, as well as physical activity opportunities in the schoolday. The website shares success stories from award-winningschools. Public health and community nutrition advocates canshare in the effort by assisting schools in applying for this award.Recipient schools receive national attention as well as a financialreward. Schools can highlight this award to the community,
which can help gain support, increased student participation andimproved perception about the nutritional quality of the schoolbreakfast and lunch program.
Student Participation. The third area of assessment in schoolnutrition is student participation—are students actuallyconsuming the foods in the new meal regulations. BehavioralEconomics (BE) is a psychological concept used to understandeating behaviors.4 In other words, BE can be used to help identifyways to meet the new guidelines while creating menus that kidswill actually eat. Cornell University has dedicated an entiredepartment known as the BEN Center (Behavioral Economics inChild Nutrition Programs). The BEN Center provides informationon best practice approaches to assessing the schoolenvironment. One resource is the “Smarter LunchroomMovement.”5 This Web site also includes a process improvementplanning tool called DPIE: diagnose, prescribe, implement, andevaluate. DPIE can help nutrition professionals determine thecurrent state of a lunchroom’s operation, provide guidingrecommendations to customize change, offer implementationstrategies to plan for these goals, and guide outcome research bymeasuring and analyzing how the changes influence eatingbehaviors in the K-12 environment.6
Managing HHFKA RegulationsMeeting the HHFKA regulations such as signage, offering specificmeal components, and having certain participation levels areimportant. However, an operational model must also be used toidentify key performance indicators that can help districtsunderstand how to manage a healthy plate while balancing ahealthy budget. For a good example of how key performanceindicator management is used in the K-12 environment read onat http://food-management.com/news-amp-trends/why-kpi.Keeping current and reviewing key indicators such as changes inthe menu and sales volume are important to improving thehealth and nutritional status of school aged children. School foodservices are essential. Using resources from other organizations,schools, and individuals, as well as sharing best practices andideas can help schools successfully implement the new HealthyHunger Free Kids Act regulations.
Author InformationMaureen Pisanick, RD has worked in many Cleveland basedschool nutrition programs including Chagrin Falls and HudsonCity School District. She is currently on the nutrition steeringcommittee for Ohio Action for Healthy Kids.
References1. US Department of Agriculture. Healthy Hungry Kids Act.USDA.gov Web site. http://www.fns.usda.gov/cnd/Governance/Legislation/CNR_2010.htm. Accessed February 14, 2013.

16 The Digest—Winter 2013
Margaret Tate, MS, RD
What can we, as public health nutritionists, do to gain a competitiveedge when seeking promotional opportunities?
The Commission on Dietetic Registration recently conducted astudy to examine the factors that influence the dietetic workforcesupply and demand.1 Results of the study, Projections andOpportunities for an Increasing Demand for DieteticPractitioners: 2011 Dietetic Workforce Demand Study Results andRecommendations were published in March 2012 as asupplement to the Journal of the Academy of Nutrition andDietetics.
The study results identified the need to change how we practicein order to remain on the cutting edge. This is particularlyimportant because it is anticipated that employers will makehiring decisions based on skills and not on credentials. Therefore,we will need to demonstrate that we possess those skills.2 Thestudy states that “the profession will have to be assertive andopportunistic to secure positions in a world where competenciesand credentials are less important than teaming and problem-solving.”3 Some of the characteristics and skills that are neededfor future positions are:
✓ Strong business skills. Develop strong business skills(includes management and administration), and learn how tobe more effective negotiators and communicators.
✓ Fast, fluid and flexible: As summarized in the study report,“dietetic practitioners will need to learn to move quickly thenreassess to determine if additional changes are needed.”2
✓ Risk taking: Act like a turtle. A turtle must stick its neck out tosee where to go. Likewise, we must also “stick our neck out”and move out of our comfort zone, and be willing to take risksto move forward.
✓ Interpersonal skills: Rhea and Bettles stated “emotionalintelligence and leadership are as critical as intellect andtechnical skills.”3 Learn how to work cooperatively and respectthe contributions made by others.
✓ Leadership, leadership, leadership: Aim high and strive fortop leadership positions.
✓ Accept ambiguity and uncertainty: Learn how to work withambiguity and uncertainty. Pritchett states “pinning down yourjob during change can be like trying to nail Jell-O to the wall.”4
Four Dimensions of Power: Self-Assessment ToolIn addition to enhancing our skills, we also need to become moreorganizationally savvy. As chair of the Public Health CommunityNutrition Practice Group (many years ago), one of my favoritereports highlighted a presentation by Janet Porter titledOrganization Political Analysis: How to Assure Support for You Plan.5
The report focused on the four dimensions of power—visibility,autonomy, relevance, and relationship—and how it relates to anindividual’s job. The report also provided a tool to assess thesedimensions. I invite you to sit down, and take the self-assessmenttool (Table 1, page 17). Based on your responses, develop a planto increase your power (some personal tips for success willfollow).
The commonality with the skills development and organizationsavvy is that they focus on what each of us, need to do, toposition ourselves for future opportunities. In addition the skillsmentioned above, below is a list of tips that I feel are essential forsecuring our future success.
1. Increase a sense of awareness, both personally and of theenvironment.
2. Focus on building new skills and not just rely on technicalexpertise.
3. Develop leadership skills. One useful tool Strength-finders 2.0by Tom Rath is a great book with strategies for applying yourstrengths.
4. Look at issues beyond the dietetic profession. Other issues,such as injury prevention or tobacco use, can also impactpublic health and community nutrition.
5. Become an influencer, defined as “the power to changeanything.”7 To be successful, learn how to influencepolicymakers, work administrators, and community leaders.
Gaining the Edge to Compete for Public Health Leadership Positions
2. United States Department of Agriculture. MyPlate. USDA.govWeb site. http://www.choosemyplate.gov/. Accessed February14, 2013.3. United States Department of Agriculture. Healthier US SchoolsChallenge. USDA.gov Web site. http://www.fns.usda.gov/tn/HealthierUS/index.html. Accessed January 31, 2013.4. Cornell University. Cornell Center for Behavioral Economics inChild Nutrition Programs Web site. http://ben.dyson.cornell.edu/Accessed January 31, 2013.
5. Cornell University. SmarterLunchrooms Movement Website. http://smarterlunchrooms.org/. Accessed January 31, 2013.6. Cornell University. Cornell Center for Behavioral Economics inChild Nutrition Programs Web site. http://ben.dyson.cornell.edu/grants-and-research.html. Accessed January 31, 2013.

The Digest—Winter 2013 17
6. Learn to respect yourself and the profession if you wantothers to do the same. One of the most significant pointsmade in the workforce demand study report was that“registered dietitians will have to shed self-limiting views oftheir identity to seize new opportunities.”3
The only constant in the future will be change. By proactivelyassuming responsibility for our professional growth, we will beable to successfully compete for the public health leadershippositions we deserve. The future is in our hands.
Author InformationMargaret J. Tate, MS, RD, serves as the House of Delegate (HOD)for the PHCNPG and was the chair of the Public Health NutritionTaskforce.
References1. 2011 CDR Forum: The Future is In Your Hands—Charts YourCareer in a Changing Workplace: Insights from the 2011 Dietetics
Workforce Demand Study,September, 2011.2. Laramee S, Tate M. DieteticWorkforce Demand Study Task Force Supplement: An Introduction. J Acad Nutr Diet.2012;112(3): S7-S9.3. Rhea M, Bettle C. Future Changes Driving Dietetic WorkforceSupply and Demand: Future Scan 2012—2022. J Acad Nutr Diet.2012;112(3):S10-S24. 4. Prithcett P. The Employee Handbook of New Work Habits for aRadically Changing World: 13 Ground Rules for Job Success in theInformation Age. Dallas, Tex. Pritchett and Associates. 1994.5. Tate, M, Chairman’s Report. The Digest (Fall, 1988).6. Parks S. "President's page: creating your future--careeropportunities in an era of change." J Am Diet Assoc.1994;94(4):451.7. Patterson K, Grenny J,Maxfield D, McMillan R, Switzler A.Influencer: The power to change anything. New York: McGraw-Hill;2008.
Visibility: The extent to which your work is known in theorganization.1. Who in the organization have I shared my ambitions, my
career goals? Who else could help if they had more suchinformation?
2. How is what I do in my job communicated to the largerorganization? How can I improve on this communication?
3. Who are the influential people inside and outside of mydepartment who know my work? What additionalinformation could be shared?
4. Which of my job activities bring me in contact withpeople beyond my department or organization? How canthese activities be expanded?
5. How often do I participate in committees, task forces, andother work groups that include people from across theorganization? What other activities can I participate in?
6. What non-work related groups and professionalassociations do I belong to?
Autonomy: The amount of discretion in your job.1. What types of decisions do I make where I can act on my
own authority (e.g. budget expenditures, hiring, staffing,etc.)? In what other areas could I expand my authority?
2. What parts of my job allow me to decide how I will dosomething, to act on my own initiative? How could Imake these areas more central to my job activities?
3. Are there new projects or activities in the organization orjob that would give me the opportunity to create anddevelop something? How could I get more involved?
Relevance: Your job’s involvement with a pressingorganization issue.1. What are two or four crucial issues that my organization
faces within the next three years? Which aspect of my job
plays a role in addressing these issues? How can I furtherdevelop my job to become more involved in theseissues?
2. What skills do I have that are of most value to theorganization? How Can I use these, or trade on them, toimprove my job situation?
3. What other skills could I develop or improve to make memore of an asset to the organization? How can I go aboutthis?
Relationship: Supports and alliance on the job.1. How often am I in contact with my peers? How could
I better utilize these interactions to help my jobperformance?
2. If you have subordinates, who are most promising? Whatcould I do to help them develop and advance in theircareers?
3. What responsibilities do I share with them? What otherresponsibilities could be shared with them?
4. Which senior person could best help me do my job moreeffectively? What can I do to develop this relationship(s)?How can I be of use to this person in his/her job?
5. Who is the most senior person with influence who hasshown an interest in my career? In what ways can I makemy skills and ambitions better known to this person?How can I be of help to this person in his/her job?
6. What contacts, both in and outside of the organization,do I have that are of most value to the organization? Howcan I use these, trade on them, to improve my jobsituation? What contacts could I develop that wouldmake me more of an asset to the organization?
Table 1. Organization Political Analysis.
18 The Digest—Winter 2013
he tools and resources listed below provide generalinformation about community assessments.
1. Association for Community Health Improvement CommunityHealth Assessment Toolkit is a guide for planning, leading andusing community health needs assessments to betterunderstand and improve the health of communities.
2. Baby-Friendly USA Self-Appraisal Tool allows hospitals,birthing centers, and other approved clinics to conduct an initialappraisal or assessment of its policies and practices related tobreastfeeding.
3. CDC Community Health Assessment and Group Evaluation(CHANGE) Tool assists community health and nutritionpractitioners and community team members through thecommunity assessment process and help identify and develop a priority list.
4. CDC National Public Health Performance Standards Program(NPHPSP) provides resources on National Public HealthPerformance Standards for state and local public health systemsand for public health governing bodies.
5. CDC School Health Index and Healthy Schools Builder are botha nationally recognized self-assessment and planning tool thatallows schools to identify the strengths and weaknesses of theschool wellness policies and programs, and develop an actionplan to improve health and safety.
6. Green LW, Kreuter MW. Health Program Planning anEducational and Ecological Approach. 4th Ed. Boston: TheMcGraw-Hill Companies, Inc., 2005. Print. This book describes indetail, the Precede-Proceed Model, a framework for planning.Applications to communities and a variety of other settings areincluded.
7. Healthy Communities Institute. Community Health NeedsAssessment System is a customizable web-based informationsystem that provides the data, tools and best practices to help
hospitals meet Healthcare Reform and IRS 990 requirements forconducting community health needs assessments.
8. Martin T. “Assess the Community’s Needs for NutritionServices.” Nutrition in Promoting the Public’s Health: Strategies,Principles, and Practices. Ed. Mildred Kaufman. Sudbury,Massachusetts: Jones and Barlett Publishers, 2007. 57-81. Print.This book chapter describes the purpose of communityassessments and provides several health-planning models.
9. Moving to the Future is an online assessment resource to helpdevelop successful nutrition and physical activity programs inyour community.
10. National Association of County and City Health Officials.Mobilizing for Action Through Planning and Partnerships(MAPP). MAPP is a health planning model used to informplanning and strategic plan development. It is commonly usedby local health departments to prioritize public health issues.
11. Self-Assessment Tool for Public Health/CommunityNutritionists provides public health and community nutritionpractitioners, dietetic interns, and dietetic technicians with anopportunity to identify strengths and weaknesses within thescope of public health and community nutrition practice.
12. The Community Tool Box provides more than 7,000 pages ofessential public health skills for assessing and building healthycommunities.
13. The Let’s Move! Child Care Checklist Quiz is an interactive self-assessment tool that asks about physical activity, screentime, food, beverages, and infant feeding at your child care orhome program. After completing the self-assessment, you cancreate a customized action plan to help you reach your goals.
14. USDA Community Food Security Assessment Toolkit providesa standardized set of measurement tools to assess variousindicators of community food security.
Community Assessment Tools and Resources
NEW! Pocket Supermarket Guide, 4th EditionMary Abbott Hess, MS, RD, FADA
In this fully updated edition, theauthor guides readers through thesupermarket and offers advice to makegrocery shopping a faster, healthier,and budget-friendly experience.
Academy Member Price: $7.00Nonmember Price: $9.00
Available at www.eatright.org/shop.
T hank youto the following PHCNPG members who
served as content reviewersfor the Winter 2013 issue of The Digest:
Margaret J. Tate, MS, RD
Leah A. Groppo, RD
The Digest—Winter 2013 19
ow are we doing? We have been active and movingforward. Below is a list of the key accomplishments andmember contributions from November 2012
to January 2013:
1. A workgroup for developing Standards of Practice (SOP)and Standards of Professional Performance (SOPP) in PublicHealth Nutrition was established and the proposal wasapproved by the Academy on January 28, 2013.“Congratulations!”
Members of the team are: • Meg Bruening, PhD, MPH, RD (Project Lead, co-chair)• Margaret Tate, MS, RD (co-chair)• Adrienne Udarbe, MS, RD• Doris C. Fredericks, MEd, RD, RYT• Gloria Stables, PhD, RD• Jamie Stang, PhD, MPH, RD• Leigh Ann Edwards, MPH, RD• Phyllis Crowley, MS, RD, CD, IBCLC • Rebecca Liebes, PhD, RD• Samia Hamdan, MPH, RD
2. The Academy’s Kids Eat Right Project has selected three of our members for thefollowing:
• Kay Dutram, MS, RD has been selected to serve on the Future of Food NutritionSolutions Working Group.
• Margaret Tate, MS, RD and Christina Ferroli, PhD, RD have been selected to serveas panelists on the July 2013 Kids Eat Right CPEU Future of Food webinar.
3. Networking relationship with the Association of State & Territorial Public HealthNutrition Directors (ASTPHND) has been formally established.
4. We have sponsored the CPUE webinar “Meatless Monday: The Science Behind theCampaign.” About 450 people from 34 DPG/MIG attended the webinar.
5. We received valuable input from members on our Strategic Plan and the 2012-2013PHCNPG Strategic Plan project team has been established. They will review and updatethe current Strategic Plan which was established in 2009.
6. A proposal for the 2013 FNCE Spotlight Program was developed by Nicole Larson, PhD,MPH, RD, Chair-elect and was submitted to the Academy.
7. The following nominations will be submitted to the Academy, Jamie Stang, PhD, MPH,RD for the 2013 Academy Medallion Award, and Margie Tate, MS, RD for the 2013Excellence in Community Dietetics Award.
8. The Gwendolyn Rossell Memorial Continuing Education Scholarship is being reviewedand revised to better meet members’ needs and increase the number of applications.
My sincere thanks to our members for volunteering for PHCNPG and Academy projects.Thank you to the Executive Committee members for their tireless work and our DPG/MIGManager, Mya Wilson for her guidance.
Thank you for your continued support in making PHCNPG active! If you have anysuggestions and/concerns, please feel free to contact me at [email protected].
A Message from the Chair
Takako Tagami, MS,MBA, RD, LD
2012-2013Executive Committee
ChairTakako Tagami, MBA, MS, RD, [email protected]
Chair-ElectNicole Larson, PhD, MPH, RD, [email protected]
Past ChairChristina E. Ferroli, PhD, [email protected]
SecretaryLauren M. Melnick, MS, RD, [email protected]
TreasurerLeslye L. Rauth, MPH, RD, CDE, [email protected]
AdvisorDoris C. Fredericks, MEd, RD, [email protected]
Website ChairLeah A. Groppo, [email protected]
Technology ChairKay A. Sisk, MS, RD, [email protected]
Membership ChairGloria Stables, PhD, MS, RD, [email protected]
Awards ChairJoanne Kouba, PhD, RD, [email protected]
Nominating Committee ChairBeth Foland, MS, [email protected]
Public Policy ChairElvira E. Souza, MPH, MS, [email protected]
House of DelegateMargaret J. Tate, MS, [email protected]
Newsletter EditorJessica Barron, MS, [email protected]
Assistant Newsletter EditorShannon Looney, MPH, [email protected]
DPG/MIG ManagerMya Wilson, MPH, [email protected]
Design and LayoutJoyce [email protected]