Embed Size (px)
Citation preview
ORAL CAVITY, OESOPHAGUS & STOMACH
Amr Mahmoud
Outlines
Learn basics of 3 tumours
A. Oral cancer is associated with people who smoke and drink alcohol. Dentists are campaigning for early detection
B. 2 cancer with dismal prognosis: oesophageal cancer and gastric cancer
Oesophageal cancer is associated with Barrett’s oesphagus. Patients with Barrett’s oesphagus are under endoscopic surveillance
Gastric cancer presents late and is common in Japan
Learn a very common inflammatory disease, peptic ulcer, associated with infection with helicobacter pylori
Oral Cavity
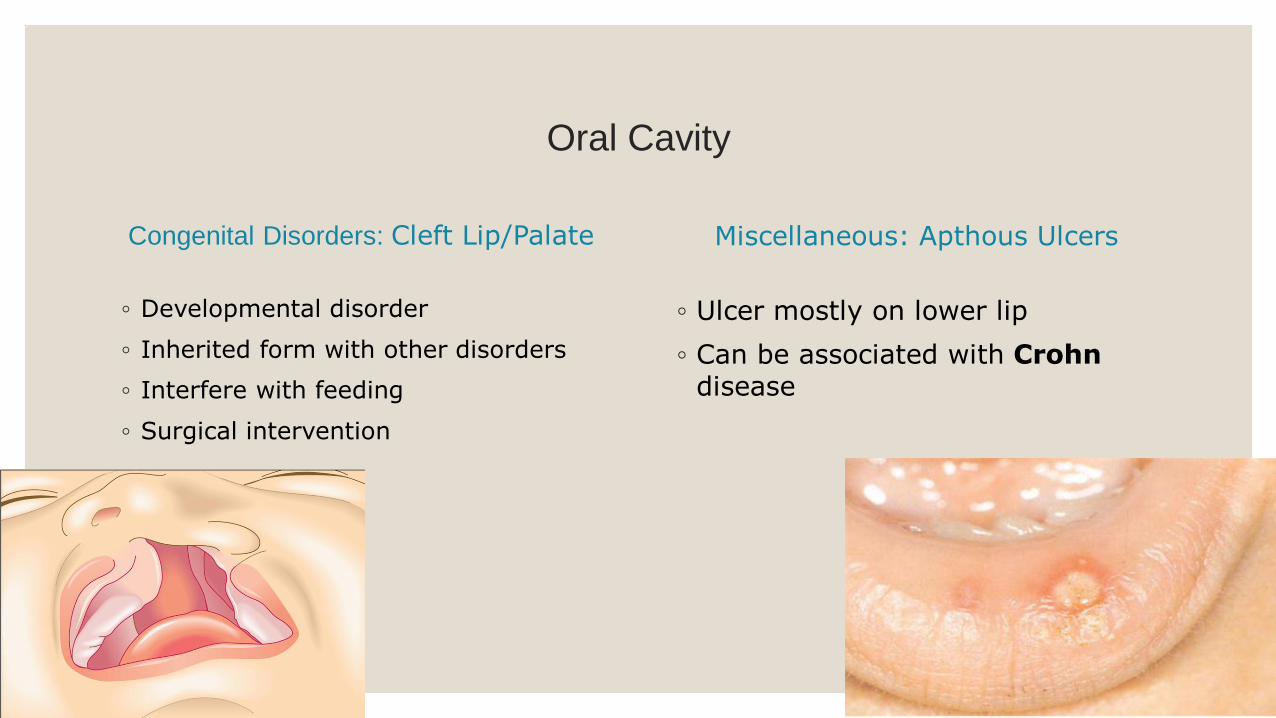
Congenital Disorders: Cleft Lip/Palate
◦ Developmental disorder
◦ Inherited form with other disorders
◦ Interfere with feeding
◦ Surgical intervention
Miscellaneous: Apthous Ulcers
◦ Ulcer mostly on lower lip
◦ Can be associated with Crohndisease
Oral Cavity: Inflammatory Conditions
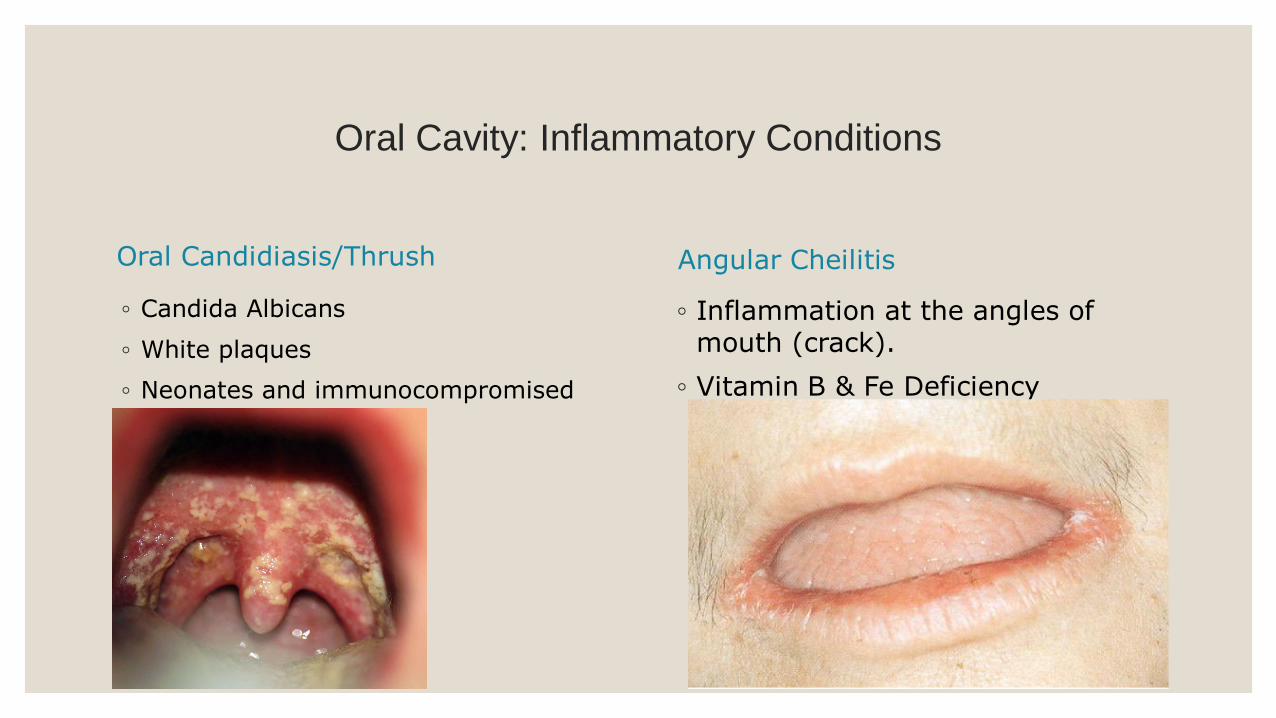
Oral Candidiasis/Thrush
◦ Candida Albicans
◦ White plaques
◦ Neonates and immunocompromised
Angular Cheilitis
◦ Inflammation at the angles of mouth (crack).
◦ Vitamin B & Fe Deficiency
Oral Cancer
Epidemiology:
◦ 3% malignancies
◦ 50 – 80 males
◦ 50% cases attributed smoking, drinking
Types:
◦ 90% Squamous carcinoma
OTHERS:
◦ Nasopharyngeal carcinoma: China, associated with EBV
◦ Malignant lymphoma of tonsils
◦ Malignant Melanoma
Oral Cancer: Predisposing FactorsTOBACCO
◦ Initiator of carcinogenesis – alter cell (DNA damage) permanently, but not sufficient to cause tumour
◦ Promoter of carcinogenesis – induce tumours in initiated cells, but non-carcinogenic themselves (reversible).
◦ Risk increases with duration, quantity
ALCOHOL:
◦ Increase the risk and decrease lag time to develop tumour.
◦ Synergistic effect of cigarettes and C2H5
HPV: Types 16&18 (high risks)- Tonsils
Rare: betel Nut Chewing; Plummer Vinson syndrome
Premalignant conditions: Leukoplakia & Erythroplakia
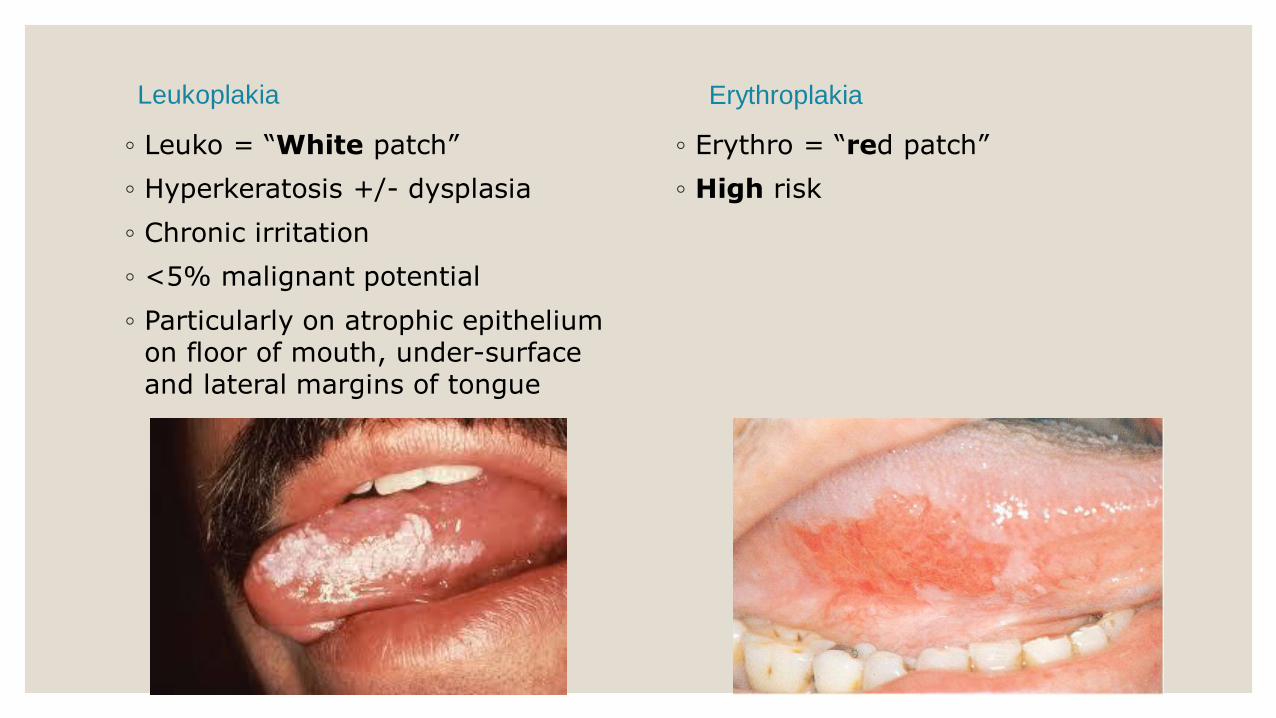
Leukoplakia
◦ Leuko = “White patch”
◦ Hyperkeratosis +/- dysplasia
◦ Chronic irritation
◦ <5% malignant potential
◦ Particularly on atrophic epithelium on floor of mouth, under-surface and lateral margins of tongue
Erythroplakia
◦ Erythro = “red patch”
◦ High risk

Squamous Cell Carcinoma (SCC)
Commonest site
◦ Lower Lip & lateral border of tongue
Presentation:
◦ Painless hard mass or ulcer with raised edges
Spread:
◦ Submaxillary and cervical lymph nodes
Staging: TNM
Prognosis:
◦ Good: mouth and anterior 2/3 of tongue
◦ Worse: posterior 2/3 of tongue and pharynx
(late presentation)
Salivary Glands: Inflammatory conditions
Salivary Calculi
◦ Usually CaCo3/CaPo4
◦ Submandibular & parotid
◦ Clinical presentation: unilateral pain & swelling on eating
◦ Duct obstruction---dilatation of ducts------sialadenitis----- atrophy and fibrosis
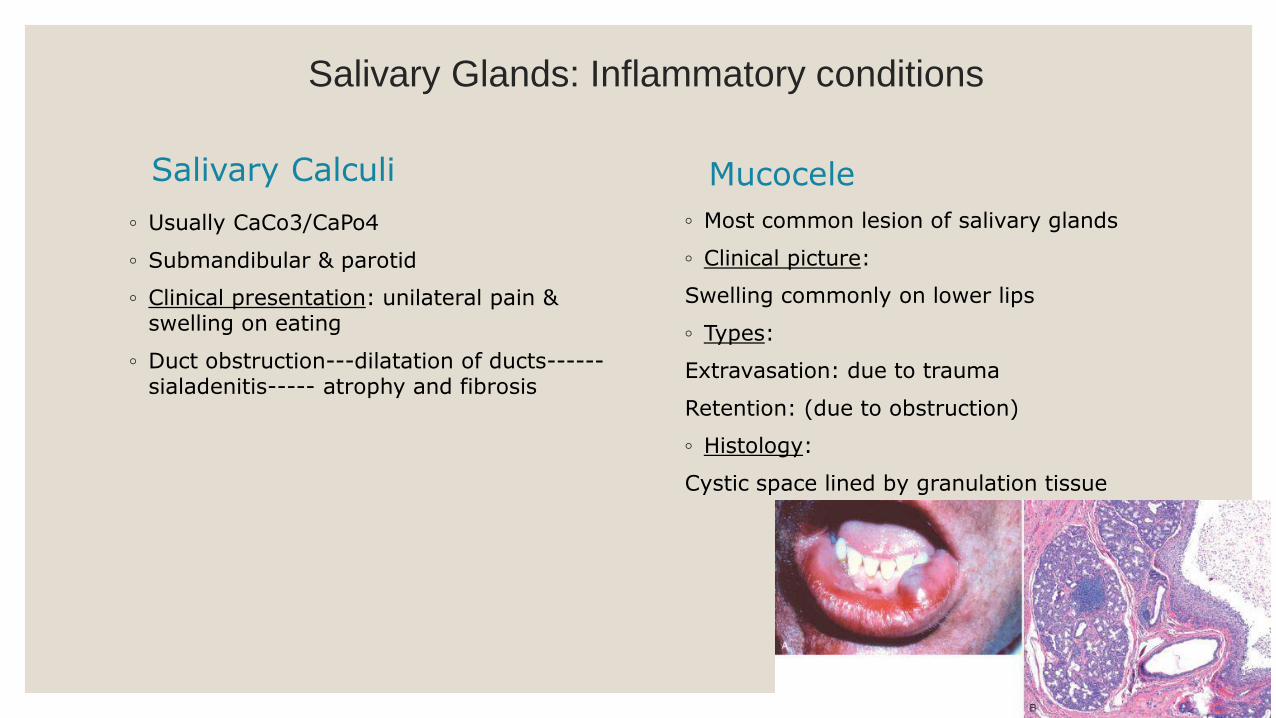
Mucocele
◦ Most common lesion of salivary glands
◦ Clinical picture:
Swelling commonly on lower lips
◦ Types:
Extravasation: due to trauma
Retention: (due to obstruction)
◦ Histology:
Cystic space lined by granulation tissue
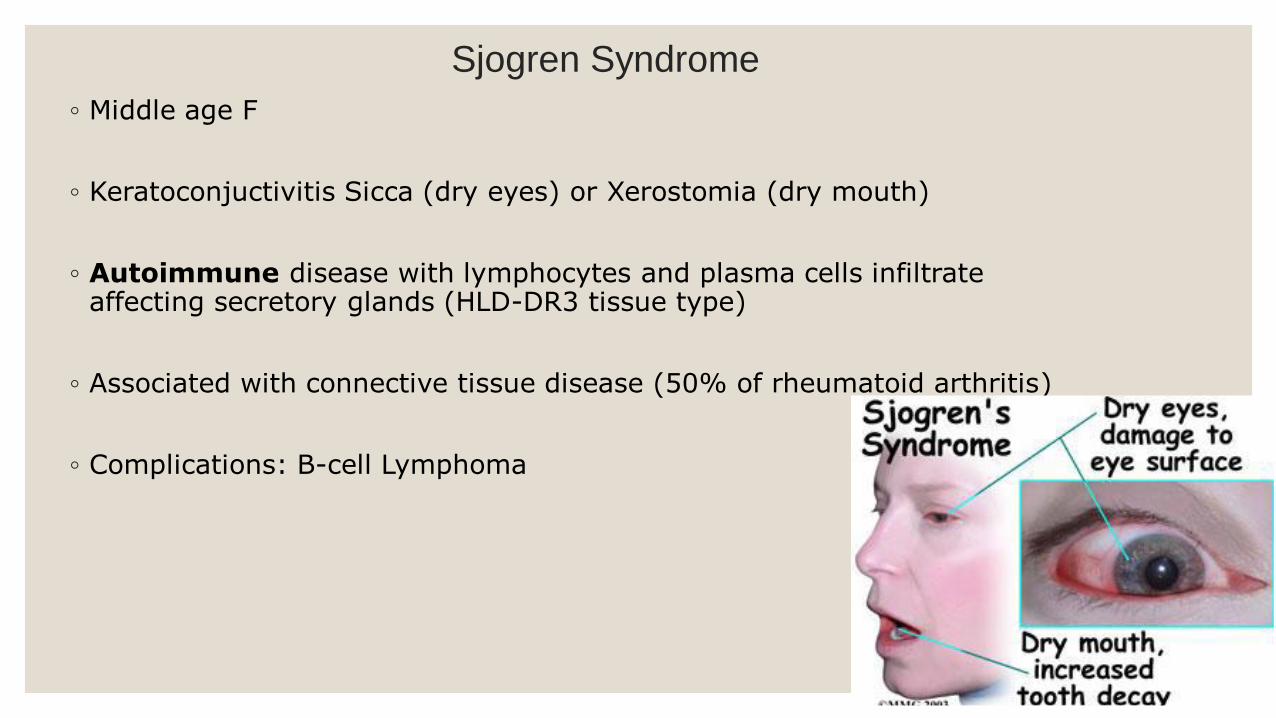
Sjogren Syndrome
◦ Middle age F
◦ Keratoconjuctivitis Sicca (dry eyes) or Xerostomia (dry mouth)
◦ Autoimmune disease with lymphocytes and plasma cells infiltrate affecting secretory glands (HLD-DR3 tissue type)
◦ Associated with connective tissue disease (50% of rheumatoid arthritis)
◦ Complications: B-cell Lymphoma
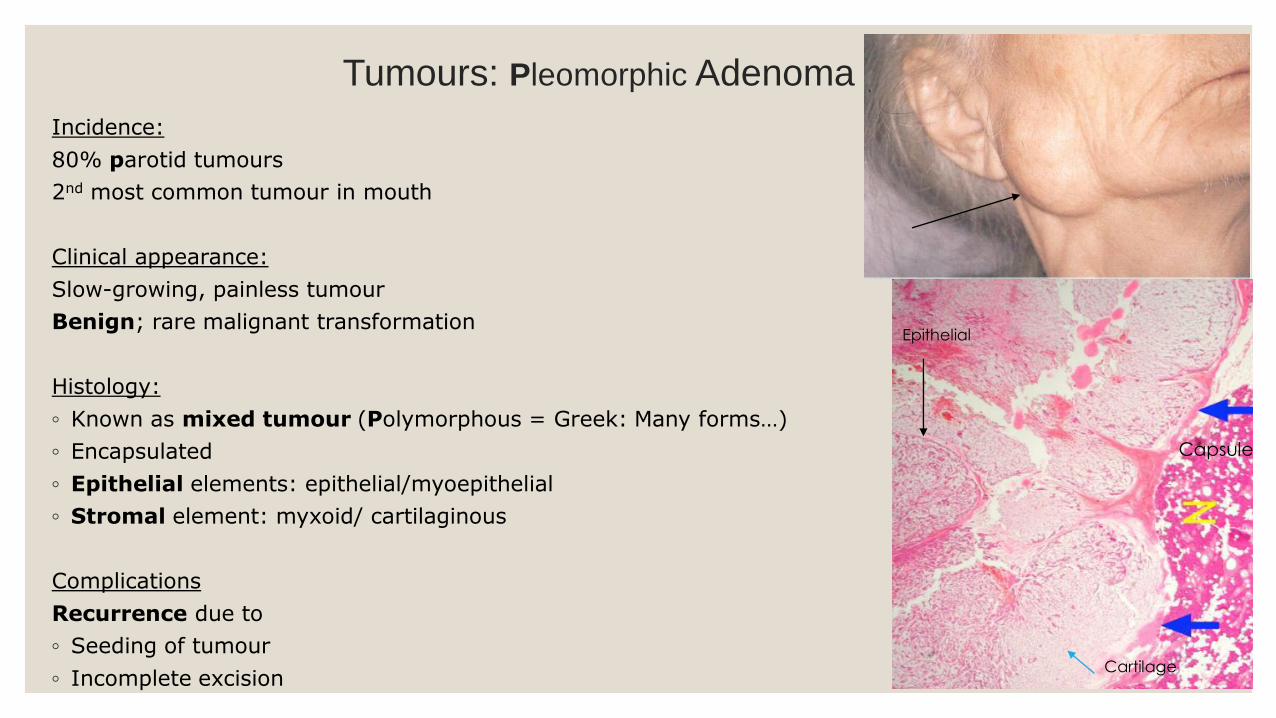
Tumours: Pleomorphic Adenoma
Incidence:
80% parotid tumours
2nd most common tumour in mouth
Clinical appearance:
Slow-growing, painless tumour
Benign; rare malignant transformation
Histology:
◦ Known as mixed tumour (Polymorphous = Greek: Many forms…)
◦ Encapsulated
◦ Epithelial elements: epithelial/myoepithelial
◦ Stromal element: myxoid/ cartilaginous
Complications
Recurrence due to
◦ Seeding of tumour
◦ Incomplete excision
Epithelial
Cartilage
Capsule
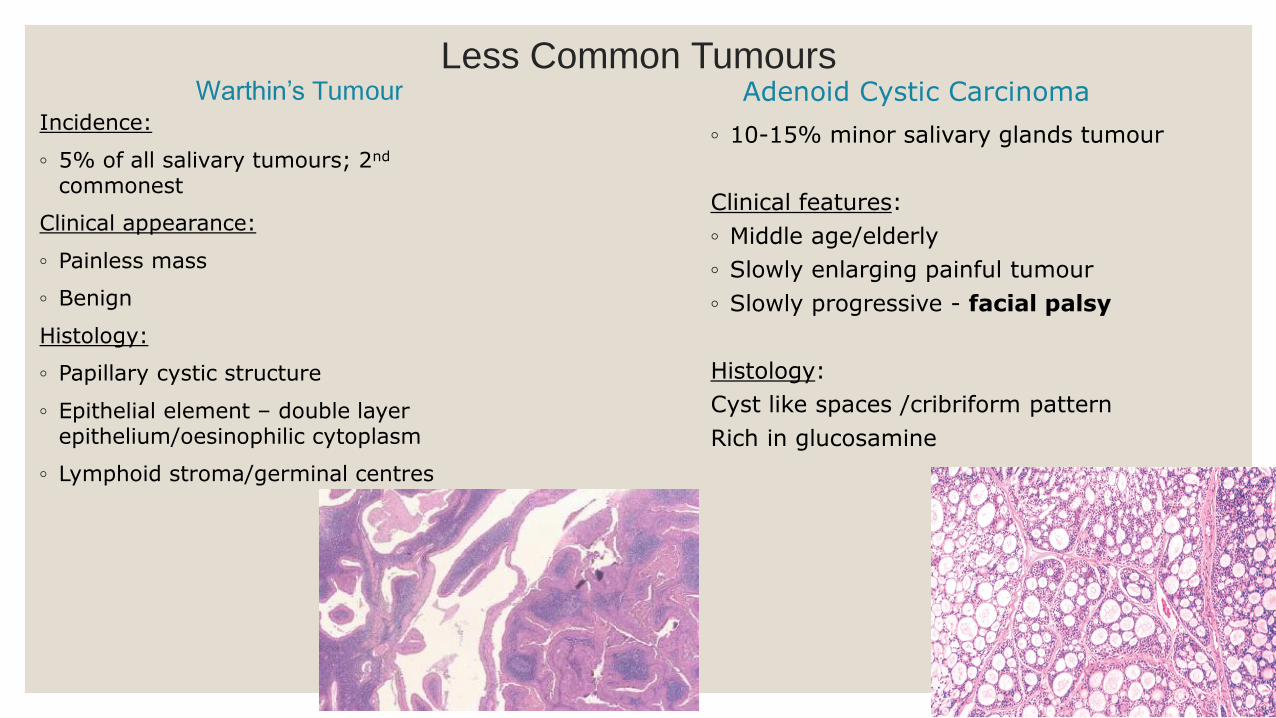
Less Common TumoursWarthin’s Tumour
Incidence:
◦ 5% of all salivary tumours; 2nd
commonest
Clinical appearance:
◦ Painless mass
◦ Benign
Histology:
◦ Papillary cystic structure
◦ Epithelial element – double layer epithelium/oesinophilic cytoplasm
◦ Lymphoid stroma/germinal centres
Adenoid Cystic Carcinoma
◦ 10-15% minor salivary glands tumour
Clinical features:
◦ Middle age/elderly
◦ Slowly enlarging painful tumour
◦ Slowly progressive - facial palsy
Histology:
Cyst like spaces /cribriform pattern
Rich in glucosamine

Oesophagus: Normal function, Anatomy and Histology
25cm muscular cylindrical structure
Upper sphincter: controls swallowing
Lower sphincter (LES): control entry to stomach and protect against regurgitation of gastric content
Histology:
◦ Stratified squamous epithelium
◦ Transition to columnar epithelium at the oesophago-gastric junction (OGJ)
Congenital Disorders
Atresia
◦ Failure or embryological canalisation
◦ Several types:
Fistula between oesophagus and trachea (commonest)
Clinically:
Aspiration
Treatment:
Urgent surgical intervention
Diverticula
◦ Out-pouching of the oesophageal wall
Complications:
Dysphagia (difficult swallowing)
Regurgitation
Aspiration pneumonia

Miscellaneous Conditions
Oesophageal Haemorrhage
Causes:
◦ Reflux Oesophgitis
◦ Varices: distended veins of porto-systemic anastomosis most commonly due to cirrhosis
◦ Ulcerating cancer
◦ Foreign body
◦ Mallory Weiss Syndrome / Boerhaavesyndrome due to rupture of oesophageal mucosa due to repeated vomiting or trauma
Achalasia
◦ Failure of relaxation of lower oesophageal sphincter - dilatation of oesophagus
◦ Also caused by Chagas disease
Histology:
◦ Reduction of ganglion cells
Clinically:
◦ Dysphagia

Reflux oesophagitis“Heart Burn”
Prevalence:
Very common: up to 36% of western population! but not all present with symptoms!
Definition:
Chronic inflammation due to regurgitation of gastric contents (chronic oesophagitis)
Causes:
◦ Life style: smoking, alcohol, caffeine
◦ Increased intra-abdominal pressure: pregnancy
◦ Defect in lower oesophageal sphincter
◦ Hiatus hernia
Protrusion of stomach into thorax
Very common
a) Sliding 90%
b) Para-oesophageal 10%
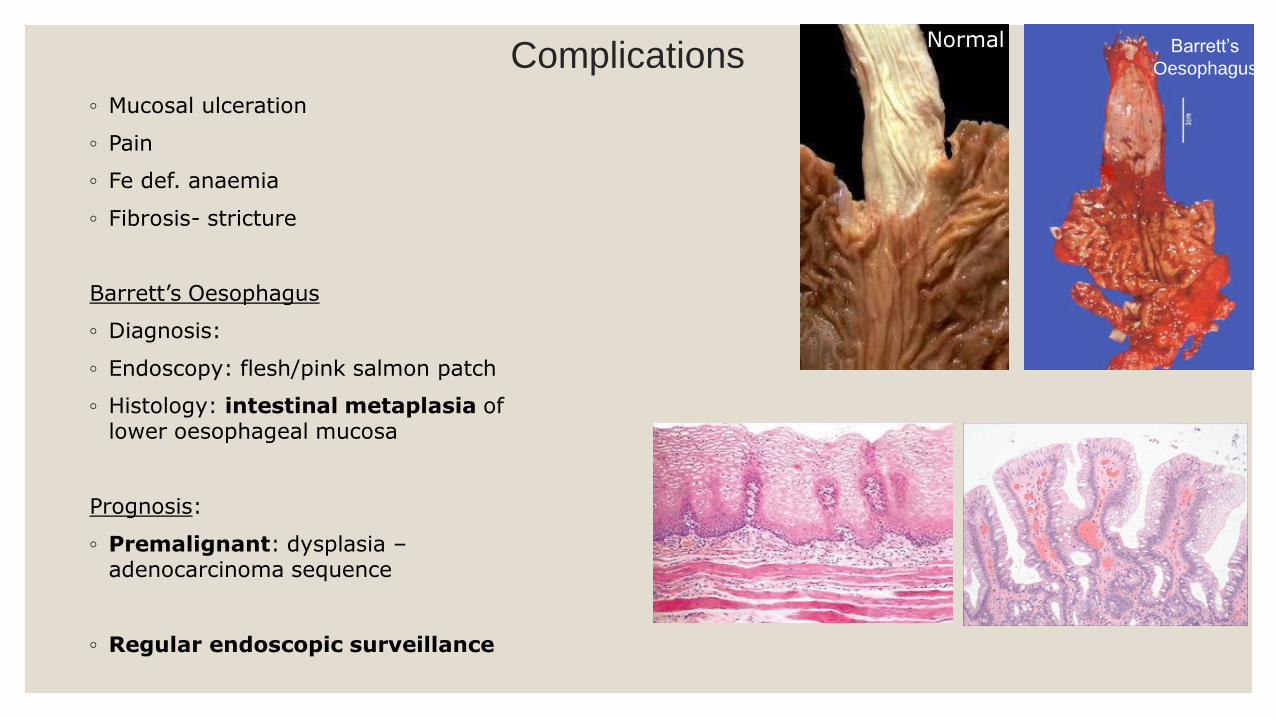
Complications
◦ Mucosal ulceration
◦ Pain
◦ Fe def. anaemia
◦ Fibrosis- stricture
Barrett’s Oesophagus
◦ Diagnosis:
◦ Endoscopy: flesh/pink salmon patch
◦ Histology: intestinal metaplasia of lower oesophageal mucosa
Prognosis:
◦ Premalignant: dysplasia –adenocarcinoma sequence
◦ Regular endoscopic surveillance
Barrett’s
Oesophagus
Normal
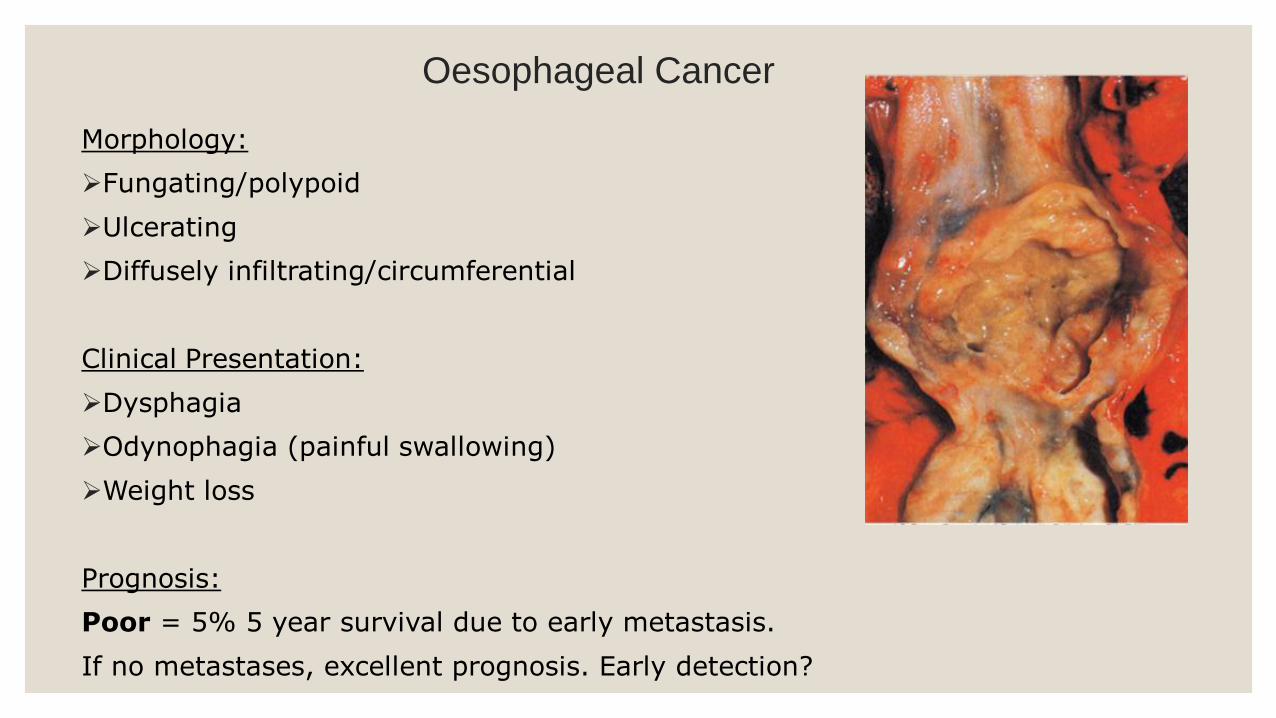
Oesophageal Cancer
Morphology:
Fungating/polypoid
Ulcerating
Diffusely infiltrating/circumferential
Clinical Presentation:
Dysphagia
Odynophagia (painful swallowing)
Weight loss
Prognosis:
Poor = 5% 5 year survival due to early metastasis.
If no metastases, excellent prognosis. Early detection?
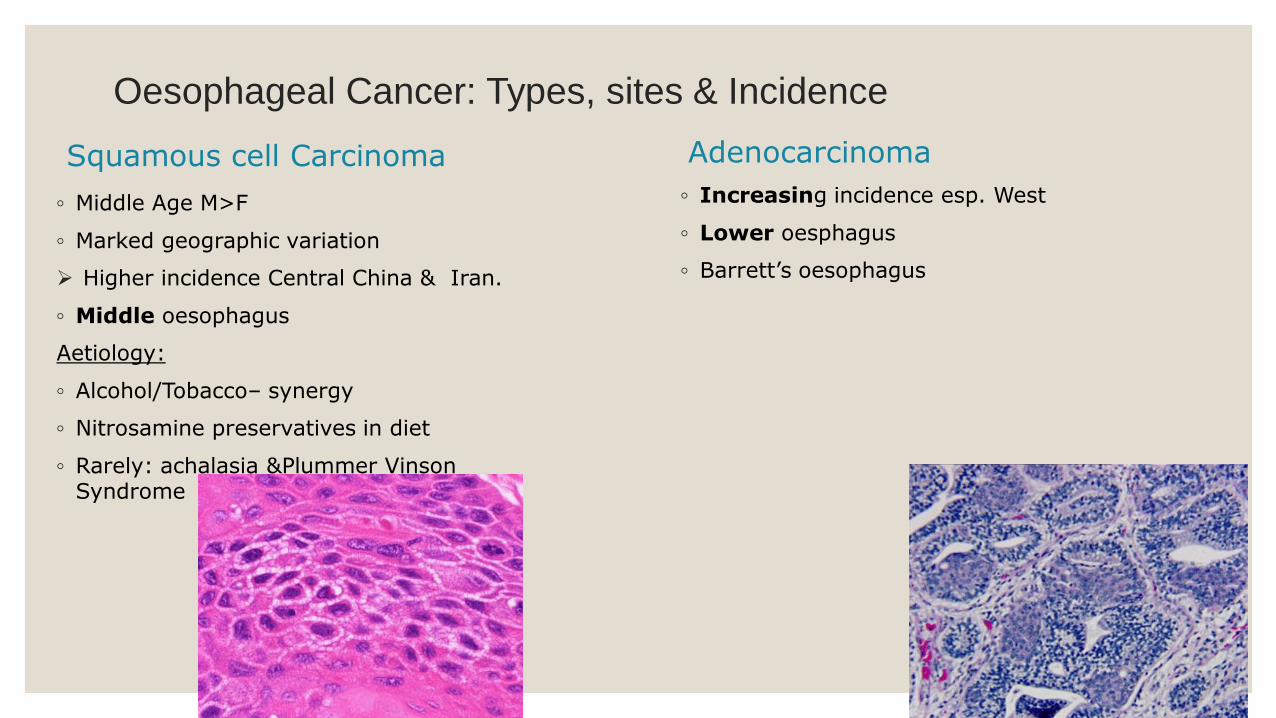
Oesophageal Cancer: Types, sites & Incidence
Squamous cell Carcinoma
◦ Middle Age M>F
◦ Marked geographic variation
Higher incidence Central China & Iran.
◦ Middle oesophagus
Aetiology:
◦ Alcohol/Tobacco– synergy
◦ Nitrosamine preservatives in diet
◦ Rarely: achalasia &Plummer Vinson Syndrome
Adenocarcinoma
◦ Increasing incidence esp. West
◦ Lower oesphagus
◦ Barrett’s oesophagus
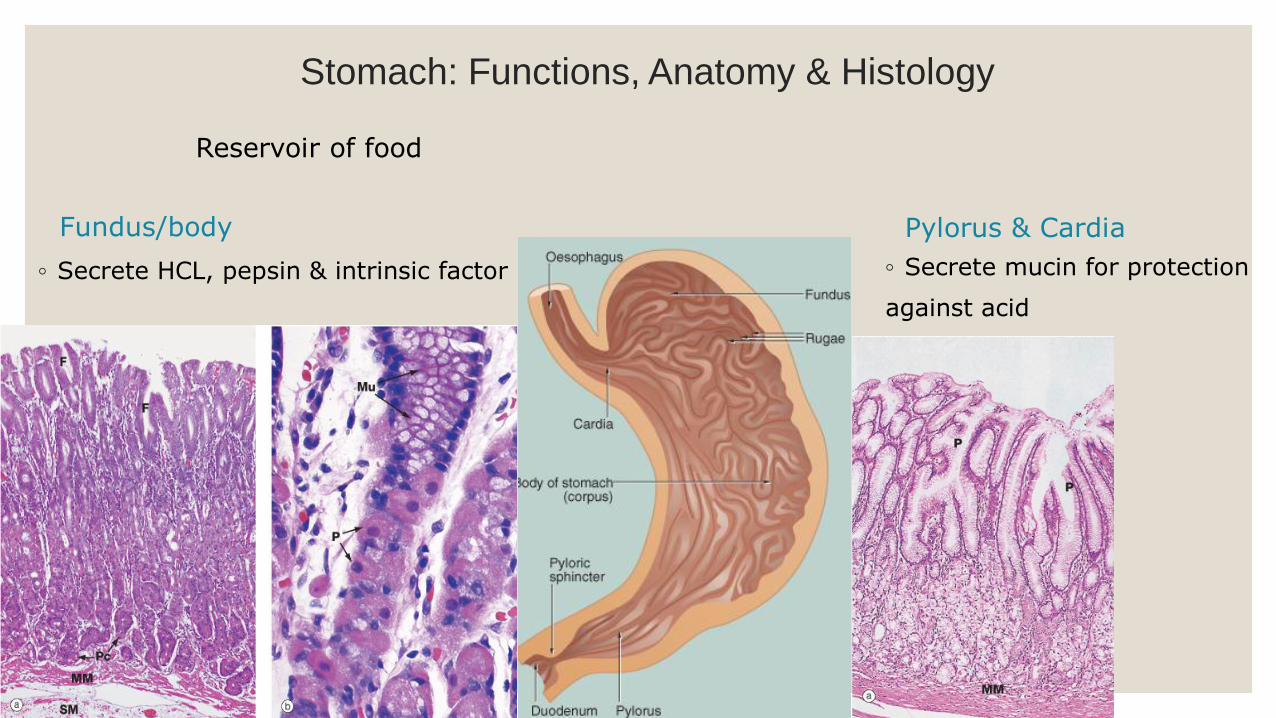
Stomach: Functions, Anatomy & Histology
Fundus/body Pylorus & Cardia
◦ Secrete HCL, pepsin & intrinsic factor ◦ Secrete mucin for protection
against acid
Reservoir of food
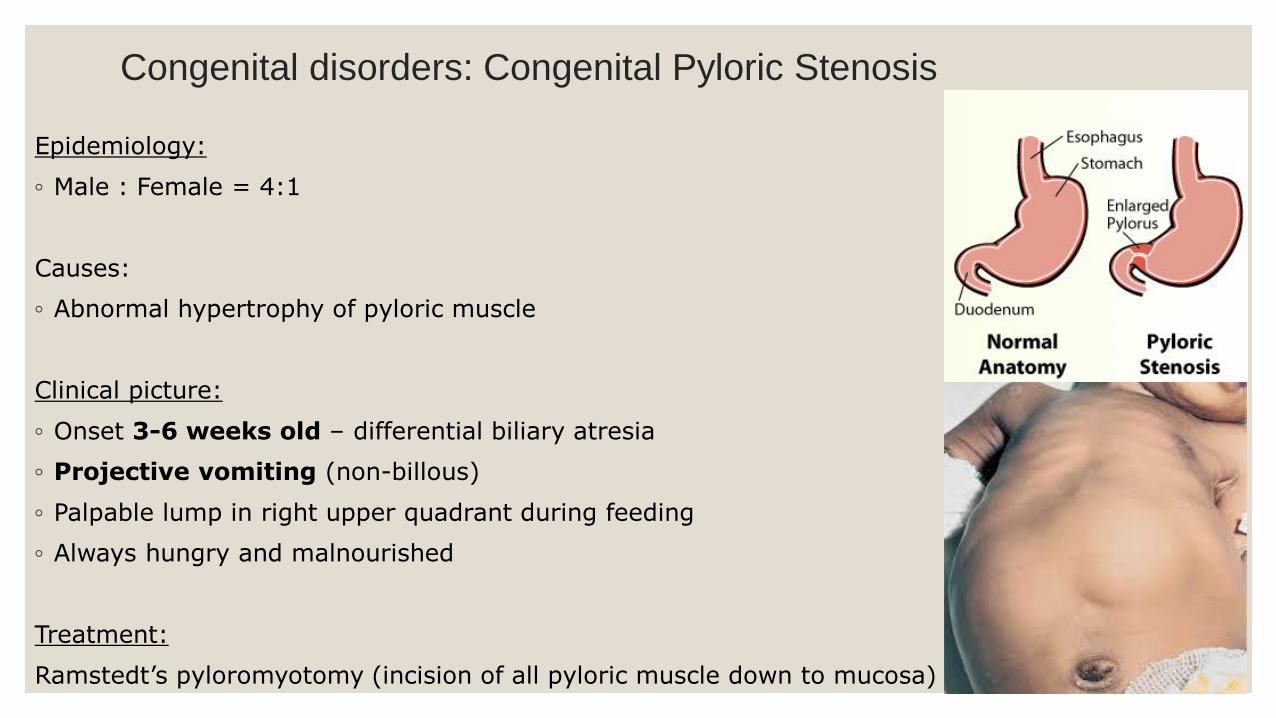
Congenital disorders: Congenital Pyloric Stenosis
Epidemiology:
◦ Male : Female = 4:1
Causes:
◦ Abnormal hypertrophy of pyloric muscle
Clinical picture:
◦ Onset 3-6 weeks old – differential biliary atresia
◦ Projective vomiting (non-billous)
◦ Palpable lump in right upper quadrant during feeding
◦ Always hungry and malnourished
Treatment:
Ramstedt’s pyloromyotomy (incision of all pyloric muscle down to mucosa)
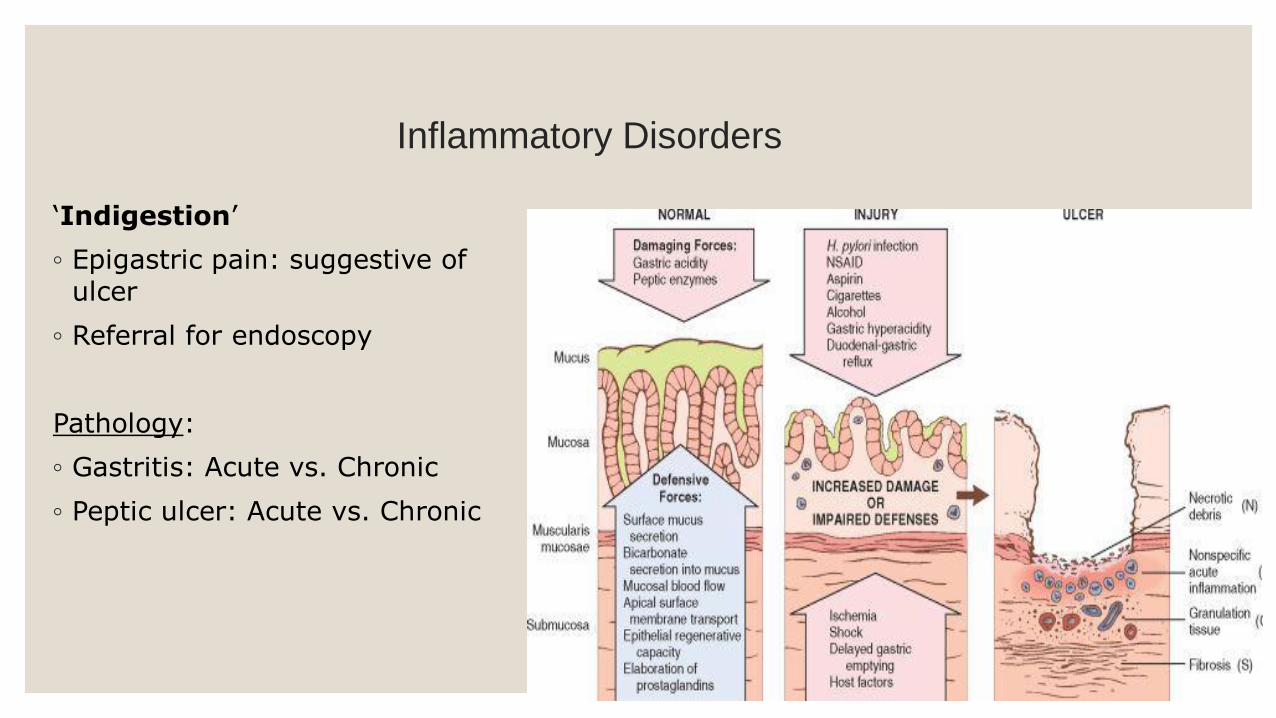
Inflammatory Disorders
‘Indigestion’
◦ Epigastric pain: suggestive of ulcer
◦ Referral for endoscopy
Pathology:
◦ Gastritis: Acute vs. Chronic
◦ Peptic ulcer: Acute vs. Chronic
Acute gastritis
◦ Acute inflammation
Causes:
◦ Damage by Chemicals: binge drinking, NSAIDS
Histology:
◦ Depend on severity: acute inflammation, ulcerations and erosions
◦ Heals by resolution and re-epithelialization
◦ Can cause massive haemorrhage
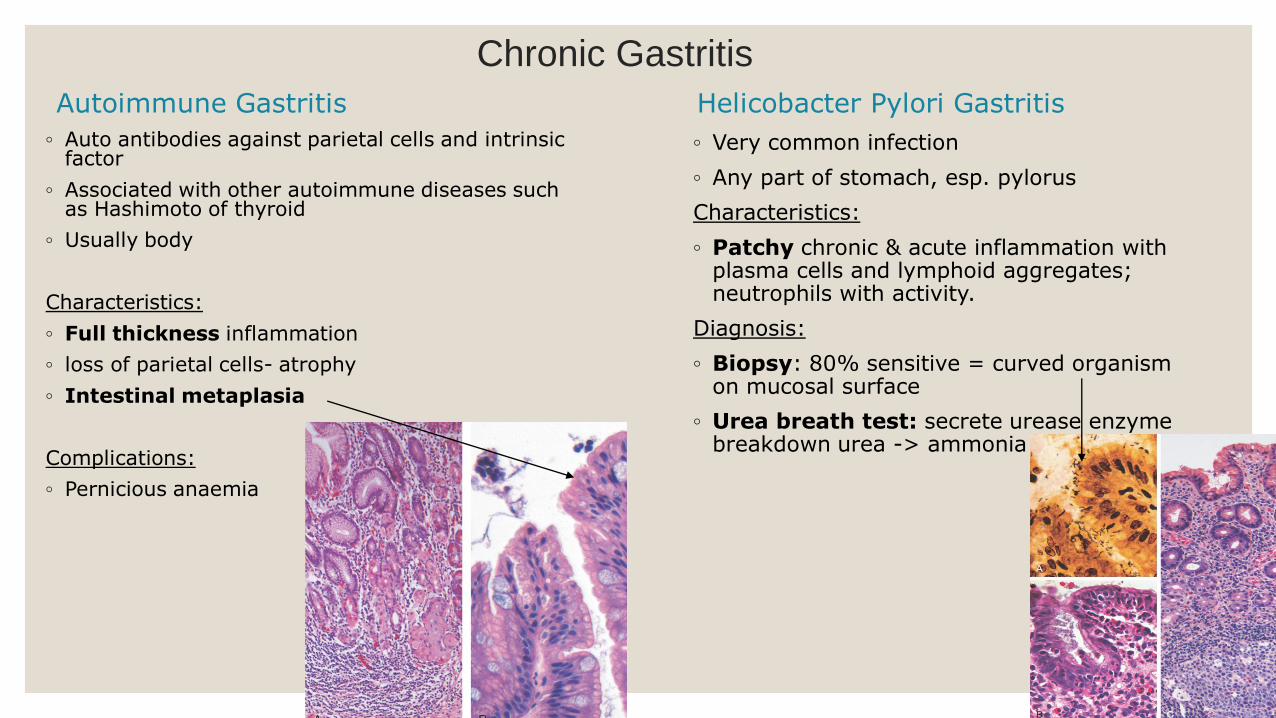
Chronic Gastritis
Autoimmune Gastritis
◦ Auto antibodies against parietal cells and intrinsic factor
◦ Associated with other autoimmune diseases such as Hashimoto of thyroid
◦ Usually body
Characteristics:
◦ Full thickness inflammation
◦ loss of parietal cells- atrophy
◦ Intestinal metaplasia
Complications:
◦ Pernicious anaemia
Helicobacter Pylori Gastritis
◦ Very common infection
◦ Any part of stomach, esp. pylorus
Characteristics:
◦ Patchy chronic & acute inflammation with plasma cells and lymphoid aggregates; neutrophils with activity.
Diagnosis:
◦ Biopsy: 80% sensitive = curved organism on mucosal surface
◦ Urea breath test: secrete urease enzyme breakdown urea -> ammonia
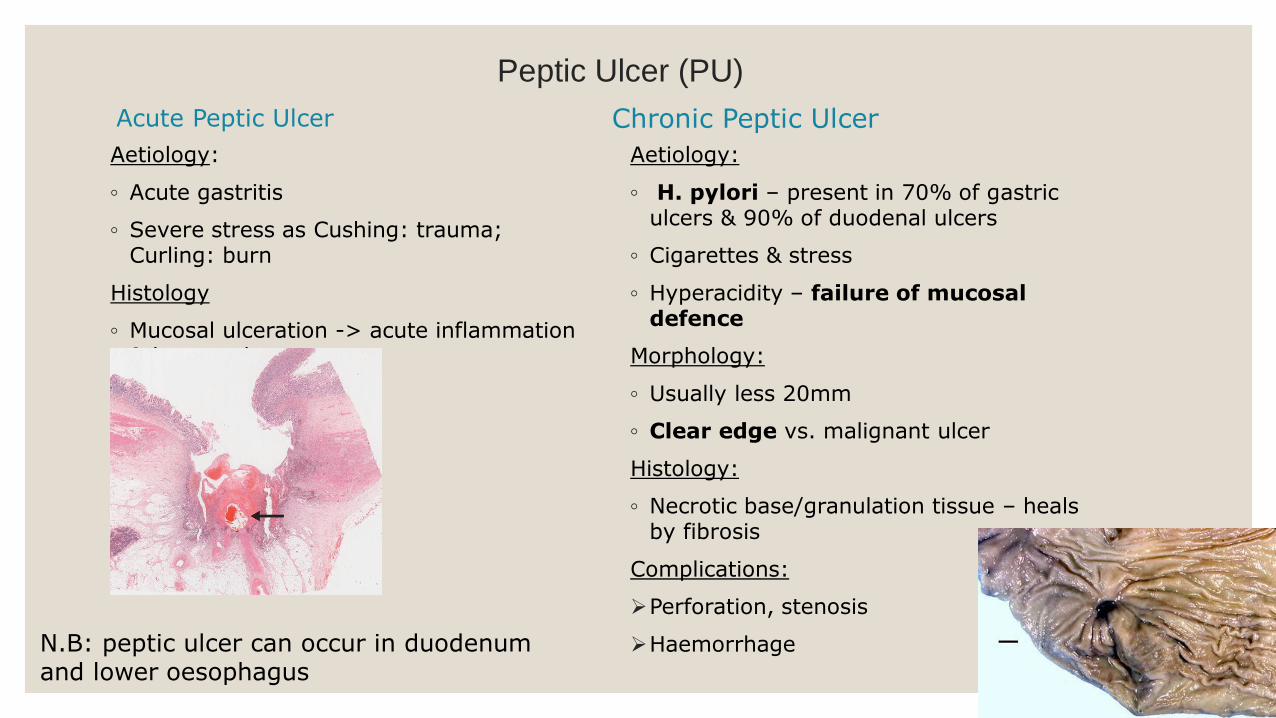
Peptic Ulcer (PU)
Acute Peptic Ulcer
Aetiology:
◦ Acute gastritis
◦ Severe stress as Cushing: trauma; Curling: burn
Histology
◦ Mucosal ulceration -> acute inflammation & haemorrhage
Chronic Peptic Ulcer
Aetiology:
◦ H. pylori – present in 70% of gastric ulcers & 90% of duodenal ulcers
◦ Cigarettes & stress
◦ Hyperacidity – failure of mucosal defence
Morphology:
◦ Usually less 20mm
◦ Clear edge vs. malignant ulcer
Histology:
◦ Necrotic base/granulation tissue – heals by fibrosis
Complications:
Perforation, stenosis
HaemorrhageN.B: peptic ulcer can occur in duodenumand lower oesophagus

Tumours: Benign Neoplasms
Epithelial Polyps
◦ Hyperplastic, fundic gland polyps
◦ Hamartomatous polyp – Peutz-Jeghers polyp
◦ Adenomas:
Mostly in east (Japan)
Pre-malignant
Non-epithelial/mesenchymal
Leiomyoma – smooth muscle
Malignant Tumours
Majority Adenocarcinoma
Lymphoma: less common
Incidence:
◦ Age 50-70, M: F = 3: 2
◦ Geographical variation – high incidence Japan, China & Columbia
◦ Incidence declining elsewhere
Clinical presentation:
◦ Present when clinically advance (silent killer)
◦ Few non-specific symptoms/silent (anaemia)

Gastric Adenocarcinoma
Aetiology:
Familial
Diet:
Nitrates and nitrosamines in salty and smoked food and smoking
Fruits, vegetable & antioxidants: protective
Chronic inflammation:
Intestinal metaplasia associated with chronic gastritis
Helicobacter: linked to cancer, but no definite mechanism understood yet
EBV infection
Gastric adenoma (associated with dysplasia)
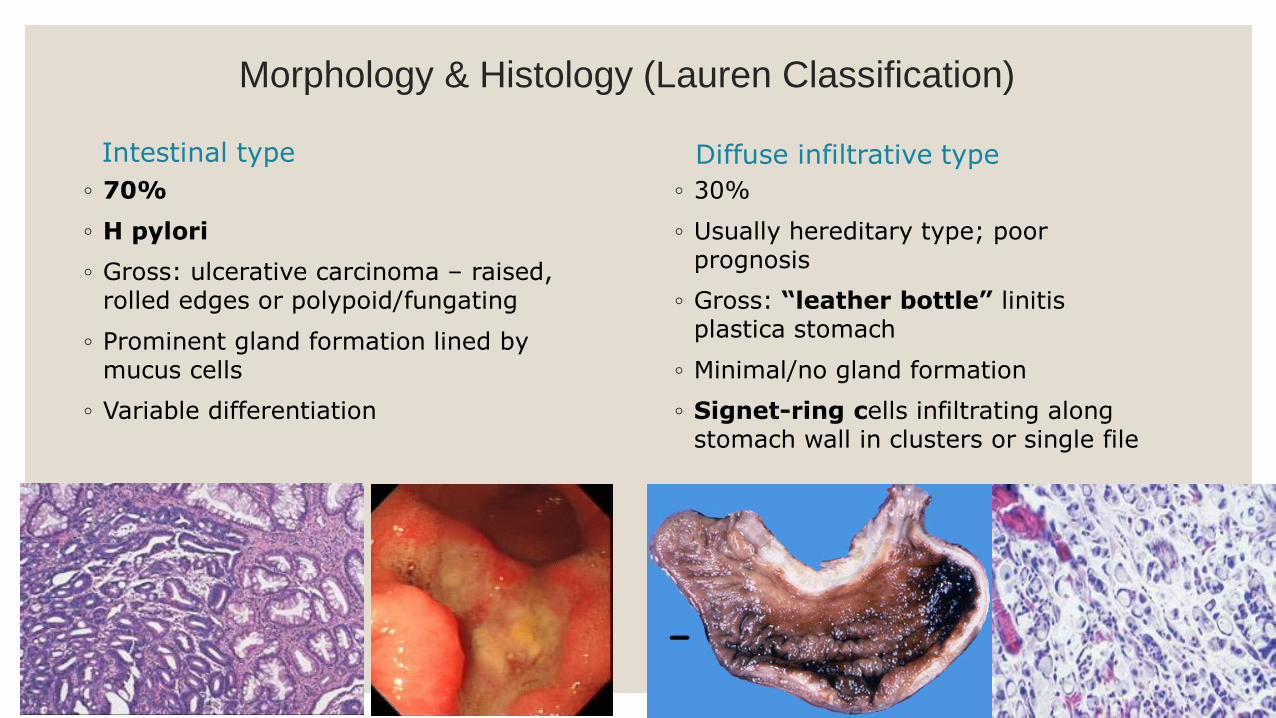
Morphology & Histology (Lauren Classification)
Intestinal type
◦ 70%
◦ H pylori
◦ Gross: ulcerative carcinoma – raised, rolled edges or polypoid/fungating
◦ Prominent gland formation lined by mucus cells
◦ Variable differentiation
Diffuse infiltrative type
◦ 30%
◦ Usually hereditary type; poor prognosis
◦ Gross: “leather bottle” linitis plastica stomach
◦ Minimal/no gland formation
◦ Signet-ring cells infiltrating along stomach wall in clusters or single file
Spread:
◦ Direct – through stomach wall
◦ Transcoelomic – tumour cells may seed peritoneum or cross peritoneal cavity, e.g. ovary (Kruckenburg tumour)
◦ Lymphatic – local nodes, supraclavicular (Virchow’s) node
◦ Invade nearby organs
Prognosis:
1. Early: (intra mucosal or submucosa)
◦ Excellent prognosis up to 90%
◦ ? Early detection in Japan
2. Late:
◦ Poor – 5%
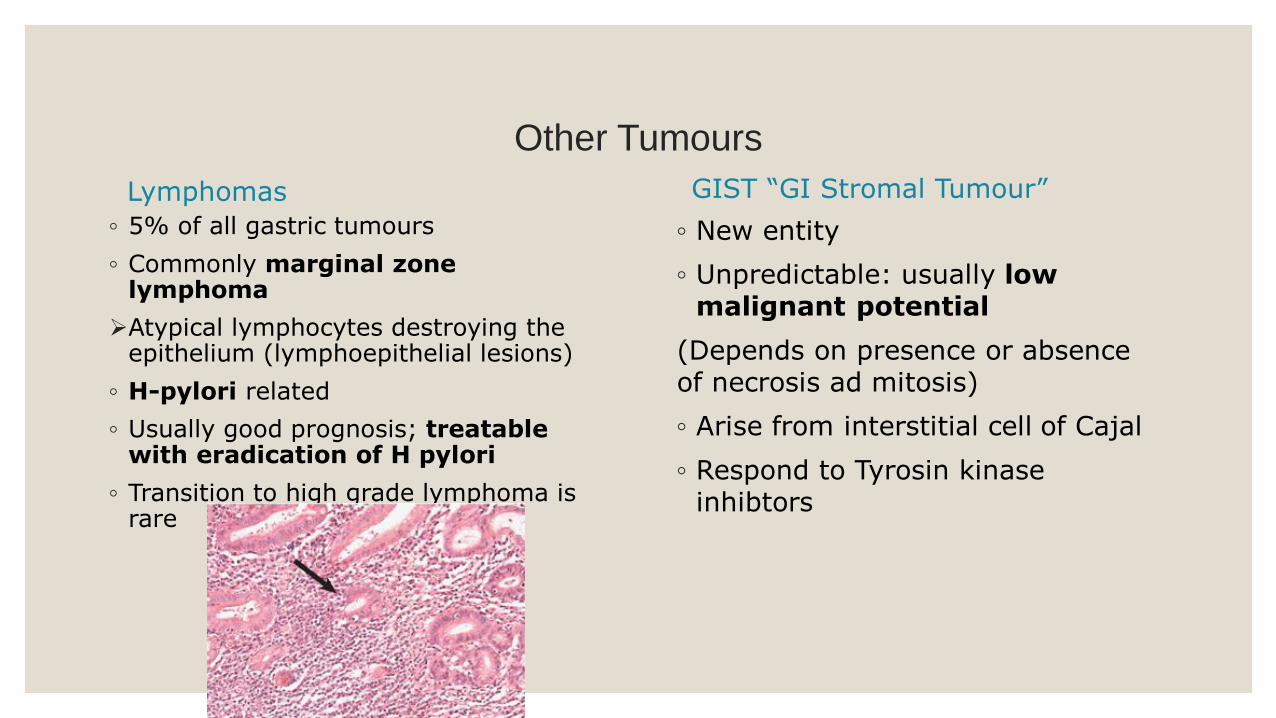
Other Tumours
Lymphomas
◦ 5% of all gastric tumours
◦ Commonly marginal zone lymphoma
Atypical lymphocytes destroying the epithelium (lymphoepithelial lesions)
◦ H-pylori related
◦ Usually good prognosis; treatable with eradication of H pylori
◦ Transition to high grade lymphoma is rare
GIST “GI Stromal Tumour”
◦ New entity
◦ Unpredictable: usually low malignant potential
(Depends on presence or absence of necrosis ad mitosis)
◦ Arise from interstitial cell of Cajal
◦ Respond to Tyrosin kinase inhibtors