Embed Size (px)
Citation preview
Inside this issue
Incidence/Severity ......................... 1
Breeds involved ............................. 2
Treatment of facial wounds........... 3
When to transfer……………..….…...3
Antibiotic Use…………………….......4
Tetanus & rabies prophylaxis.........5
Actual case review………..….……….5
Prevention……...……………………….6
Introduction
Dogs make great additions to families. They offer companionship, fun, and can teach children respon‐sibilities. We also must remember that dogs are animals and deserve respect. Dog bite injuries to the face can be devastating and have lasting effects on a child both physically and psychologically. Injury prevention through education is a vital role of healthcare providers, and this includes safe behavior around dogs.
Caring for the Pediatric Dog Bite
Incidence. The American Pet Products Association estimated in a 2011 to 2012 National Pet Owners Survey that there were 78.2 million owned dogs in the United States. The average number of dogs per household was 1.7. While most of these dogs may never cause harm, many of these family pets can inflict significant injury. According to Centers for Disease Control and Prevention data, approxi‐mately 4.5 million people in the United States are bitten by dogs annually, and approximately one in five of these victims receive some form of medical attention for their injuries. Many of these are treat‐ed in emergency departments. Injuries from dog bites account for approximately 1% of all emergency visits to hospitals in the United States.
Severity. The vast majority of dog bites result in nonfatal injuries that are most frequently encountered in the head and neck region and the extrem‐ities. According to the statistical data from the American Society of Plastic Surgeons, although the number of dog bite injuries has decreased over the last decade, there were still 27, 752 dog bite cases that required surgical repair by a facial surgeon in 2012 alone. Between 1979 and 1996 however, there were more than 300 human dog bite‐related fatalities in the United States. Most victims were children.
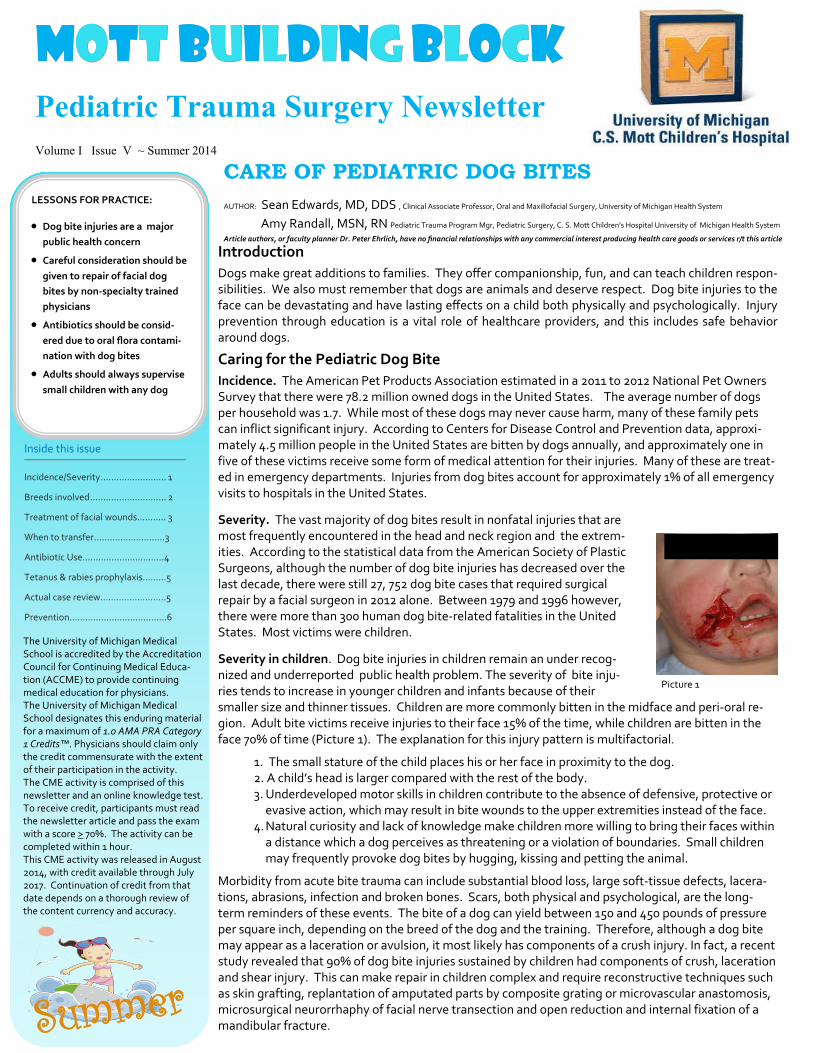
Severity in children. Dog bite injuries in children remain an under recog‐nized and underreported public health problem. The severity of bite inju‐ries tends to increase in younger children and infants because of their smaller size and thinner tissues. Children are more commonly bitten in the midface and peri‐oral re‐gion. Adult bite victims receive injuries to their face 15% of the time, while children are bitten in the face 70% of time (Picture 1). The explanation for this injury pattern is multifactorial.
1. The small stature of the child places his or her face in proximity to the dog. 2. A child’s head is larger compared with the rest of the body. 3. Underdeveloped motor skills in children contribute to the absence of defensive, protective or evasive action, which may result in bite wounds to the upper extremities instead of the face. 4. Natural curiosity and lack of knowledge make children more willing to bring their faces within a distance which a dog perceives as threatening or a violation of boundaries. Small children may frequently provoke dog bites by hugging, kissing and petting the animal.
Morbidity from acute bite trauma can include substantial blood loss, large soft‐tissue defects, lacera‐tions, abrasions, infection and broken bones. Scars, both physical and psychological, are the long‐term reminders of these events. The bite of a dog can yield between 150 and 450 pounds of pressure per square inch, depending on the breed of the dog and the training. Therefore, although a dog bite may appear as a laceration or avulsion, it most likely has components of a crush injury. In fact, a recent study revealed that 90% of dog bite injuries sustained by children had components of crush, laceration and shear injury. This can make repair in children complex and require reconstructive techniques such as skin grafting, replantation of amputated parts by composite grating or microvascular anastomosis, microsurgical neurorrhaphy of facial nerve transection and open reduction and internal fixation of a mandibular fracture.
MMMOOOTTTTTT BBBUUUIIILLLDDDIIINNNG G G BBBLLLOOOCCCK K K Pediatric Trauma Surgery Newsletter Volume I Issue V ~ Summer 2014
CARE OF PEDIATRIC DOG BITES AUTHOR: Sean Edwards, MD, DDS , Clinical Associate Professor, Oral and Maxillofacial Surgery, University of Michigan Health System
Amy Randall, MSN, RN Pediatric Trauma Program Mgr, Pediatric Surgery, C. S. Mott Children’s Hospital University of Michigan Health System
Article authors, or faculty planner Dr. Peter Ehrlich, have no financial relationships with any commercial interest producing health care goods or services r/t this article
The University of Michigan Medical School is accredited by the Accreditation Council for Continuing Medical Educa‐tion (ACCME) to provide continuing medical education for physicians. The University of Michigan Medical School designates this enduring material for a maximum of 1.0 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. The CME activity is comprised of this newsletter and an online knowledge test. To receive credit, participants must read the newsletter article and pass the exam with a score > 70%. The activity can be completed within 1 hour. This CME activity was released in August 2014, with credit available through July 2017. Continuation of credit from that date depends on a thorough review of the content currency and accuracy.
LESSONS FOR PRACTICE:
Dog bite injuries are a major
public health concern
Careful consideration should be given to repair of facial dog
bites by non‐specialty trained
physicians
Antibiotics should be consid‐ered due to oral flora contami‐
nation with dog bites
Adults should always supervise
small children with any dog
Summer
Picture 1
2
“There shall be eternal summer in the grateful heart” Celia Thaxter
Breeds most commonly involved. Although it is difficult to predict which breed of dogs will bite, recent studies have focused on bite
type and breed to assess if some dog breeds are more likely to bite than others. One such study was performed at the Children’s Hospi‐
tal of Philadelphia who studied the nature of dog bite injuries over a 5 year period in order to identify relevant critical parameters for
public education and injury prevention. They identified 551 patients that were injured from 2001 to 2005, aged 5 months to 18 years.
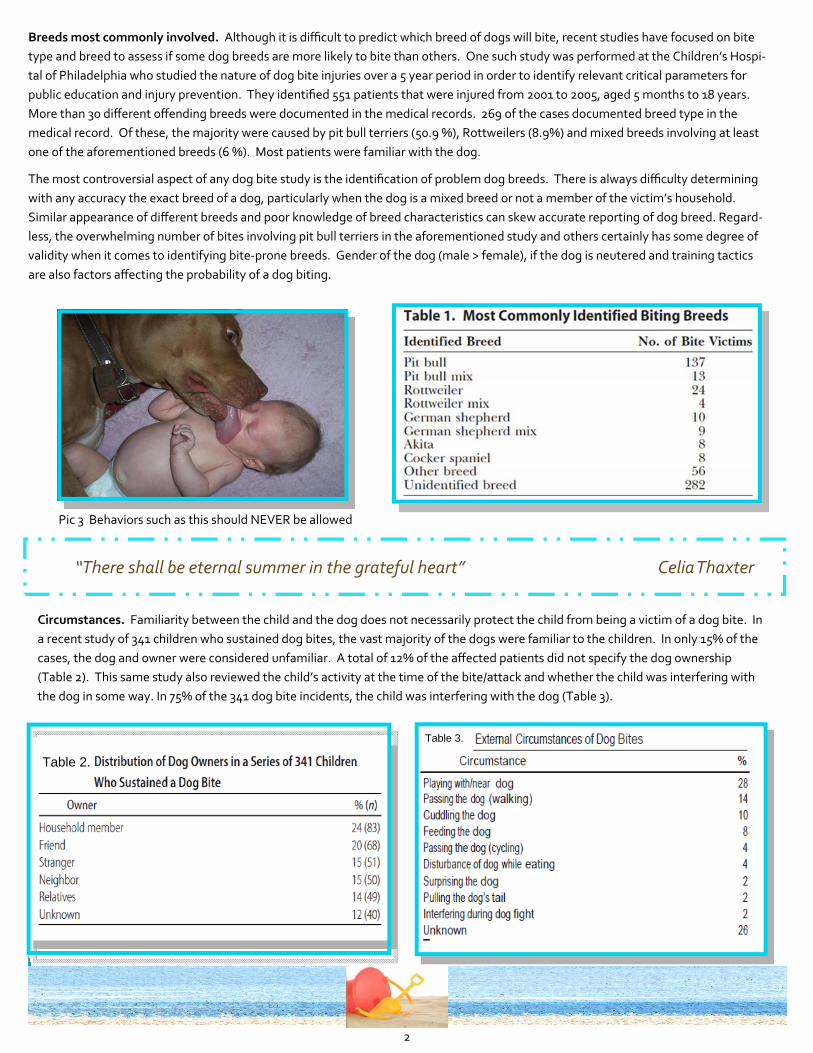
More than 30 different offending breeds were documented in the medical records. 269 of the cases documented breed type in the
medical record. Of these, the majority were caused by pit bull terriers (50.9 %), Rottweilers (8.9%) and mixed breeds involving at least
one of the aforementioned breeds (6 %). Most patients were familiar with the dog.
The most controversial aspect of any dog bite study is the identification of problem dog breeds. There is always difficulty determining
with any accuracy the exact breed of a dog, particularly when the dog is a mixed breed or not a member of the victim’s household.
Similar appearance of different breeds and poor knowledge of breed characteristics can skew accurate reporting of dog breed. Regard‐
less, the overwhelming number of bites involving pit bull terriers in the aforementioned study and others certainly has some degree of
validity when it comes to identifying bite‐prone breeds. Gender of the dog (male > female), if the dog is neutered and training tactics
are also factors affecting the probability of a dog biting.
Circumstances. Familiarity between the child and the dog does not necessarily protect the child from being a victim of a dog bite. In
a recent study of 341 children who sustained dog bites, the vast majority of the dogs were familiar to the children. In only 15% of the
cases, the dog and owner were considered unfamiliar. A total of 12% of the affected patients did not specify the dog ownership
(Table 2). This same study also reviewed the child’s activity at the time of the bite/attack and whether the child was interfering with
the dog in some way. In 75% of the 341 dog bite incidents, the child was interfering with the dog (Table 3).
Table 2.
Table 3.
Pic 3 Behaviors such as this should NEVER be allowed

3
Treatment. Since a large percentage of dog bites in children are located on the face, facial trauma surgical specialists such as oral and
maxillofacial surgeons, are frequently involved in the surgical care of these wounds. As with any injury, treatment priority is given to
any life‐threatening conditions according to advance trauma life support (ATLS) guidelines. Injuries that require advanced trauma
treatment are usually associated with penetrating neck trauma following mauling by large dogs. Even apparently minor wounds re‐
quire careful exploration, because seemingly superficial injuries may well overlie fractures, involve lacerated tendons or nerves or pene‐
trate into joint spaces.
Since all bite wounds are contaminated with the oral flora of the animal, prevention of local wound infection is the principal treatment
concern along with rabies and tetanus prophylaxis. Copious, surgical wound irrigation followed by careful debridement remains the
mainstay of treatment of all bite wounds as this will significantly reduce the incidence of infection. Typically puncture type wounds are
irrigated, cleansed and left open. Primary repair may be necessary with non‐puncture and avulsion type injuries. The historical appre‐
hension with primary closure is the concern for increased infection rates due to “bacteria trapping”. Investigational data regarding pri‐
mary closure of bite wounds, however, reveals that infection rates for sutured and unsutured wounds are equivalent.
Treatment of facial bite wounds. The face and scalp are among the sites most resistant to
posttraumatic infection, presumably due the rich blood supply of the area. Facial wounds,
even when sutured, are typically associated with low infection rates, which in most studies
was < 6%. Bite wounds to this area, however, may be both severe and disfiguring, especially
in children (Pic 3) and the cosmetic result may be further compromised by inadequate surgi‐
cal management. Appropriate surgical management is vital (Pic 4).
Surgical management of facial bite injuries generally follow the standard principles of lacera‐
tion management. Current practice emphasizes the importance of high‐pressure irrigation in
reducing infection rates of contaminated wounds by decreasing the bacterial load and
removing particulate matter. Use of pulsatile jet lavage at pressures of 50‐70 psi may be
effective, but it may cause soft tissue disruption and should be limited in facial injuries. Manu‐
al irrigation is typically preferred for facial wounds. Although normal saline lacks bactericidal
activity, it remains the preferred irrigant because it does not interfere with normal wound
healing as most antiseptic solutions may. Following irrigation, debridement of devitalized
tissue further decreases the likelihood of infection. Minimal trimming of wound edges is indi‐
cated because facial tissue can survive on small pedicles. Sharp debridement near landmarks
such as the vermillion border of the lip and the eyebrows should also be avoided. Prior to the
suturing of the facial wound, exploration of the depth of the wound is important in order to de‐
tect and subsequently repair any damage to the facial nerve or parotid duct system. Because of the high risk of injury to the facial nerve
with bite injuries, testing facial nerve function is mandatory. This is done by having the patient perform facial expressions (grimace,
eyebrow raise, etc). If the patient is unable to symmetrically perform the facial expressions, facial nerve damage is likely. Location of
the bite injuries is also critical in determining the likelihood of facial nerve or parotid gland injury. Any bite that occurs between the can‐
thus of the eye and the earlobe (Pic 5) has a high probability of facial nerve injury while any bite between the tragus of the ear and the
midline of the upper lip is concerning for parotid injury (Pic 6).
When to transfer. When deciding to transfer a pediatric patient that has suffered a dog
bite to a definitive care facility (preferably a pediatric hospital with extensive pediatric surgical
specialist support) the severity of the injury should be considered. A high severity injury re‐
quiring transfer would be any bite that involves major structures of the face such as the eyes ,
nose, ears, mouth/lips or deep wounds affecting vital structures (facial nerve or parotid gland).
With superficial skin or soft tissue injuries that do not affect these structures, or are not in an
area of concern for nerve or parotid gland injury primary closure may be done by trained pro‐
viders. When transferring a patient who has suffered an avulsion and/or amputation, care in‐
cludes keeping tissue moist and positioned so as to not strangulate blood supply. Avulsed/amputated tissues should be kept cool and
transported with the patient whenever possible.
Pic 4 Post‐surgical repair
Pic 3 Pre‐surgical repair
Pic 5: Area of concern for facial nerve injury
Pic 6: Area of concern for parotid gland injury

4
Treatment
Prophylactic antibiotic use. Whereas antimicrobial therapy is clearly indicated for bite wound in‐
fections, the role of antibiotics in the treatment of uninfected dog bite wounds is another major con‐
troversial issues. When antimicrobial prophylaxis is judged to be worthwhile, the empiric regimen
should be active primarily against Staphylococcus aureus, streptococci, Haemophilus species, anaer‐
obes and P. multocida. The high isolation frequency of β‐lactamase producing strains of S. aureus
renders penicillin inadequate therapy for bite wound prophylaxis; also, many anaerobic isolates
from animal bites. Although no single agent eradicates all pathogens responsible for bite wound
infections, several studies of the in vitro susceptibility of a wide spectrum of clinical isolates suggest
that amoxicillin‐clavulanate is the gold standard for empiric antimicrobial prophylaxis, not only for
dog bites, but cat and human bites as well (Table 4). Antibiotics typically used for skin and soft tis‐
sue infections, such as oral cephalosporins and clindamycin are less than optimal for bite wounds.
In the penicillin allergic patient, optimal prophylaxis is not well established. Clindamycin is currently recommended, but only in combi‐
nation with either ciprofloxacin or (for children) trimethoprim‐sulfamethoxazole to compensate for its poor activity against E. corrodens
and almost all Pasteurella isolates.
Antibiotic therapy for bite wound infection. Infected bite wounds are usually manifested by pain, edema localized at the site of the
injury frequently associated with a purulent discharge and possibly local lymphadenitis. When examining neglected bites of any kind,
the clinician must determine if the presentation is that of a normal inflammatory response or the erythema and swelling of infection.
Antibiotic therapy for established bite wound infection is initially the same as for prophylaxis. In case of infection despite proper empir‐
ic treatment, transitioning to a broader spectrum antibiotic is required, although definitive therapy ideally should be guided by cultures.
When parenteral therapy is indicated, treatment options include ampicillin‐sulbactam, cefoxitin and ticarcillin‐clavulanate pending cul‐
ture results. For the penicillin allergic patient, clindamycin plus ciprofloxacin is an appropriate combination. Duration of antibiotic ther‐
apy for established bite wound infection should be customized based on the site involved and the response to treatment (Table 5).
A 7‐14 day course is typically adequate for soft tissue infections whereas a minimum of 3 weeks of therapy is recommended for infec‐
tions involving joints or bones.
“A life without love is like a year without summer” Swedish Proverb
Table 4
Table 5
5
ACTUAL CASE REVIEW A pictorial review of an actual dog bite case treated by the
Department of Oral & Maxillofacial Surgery at C. S. Mott Children’s Hospital
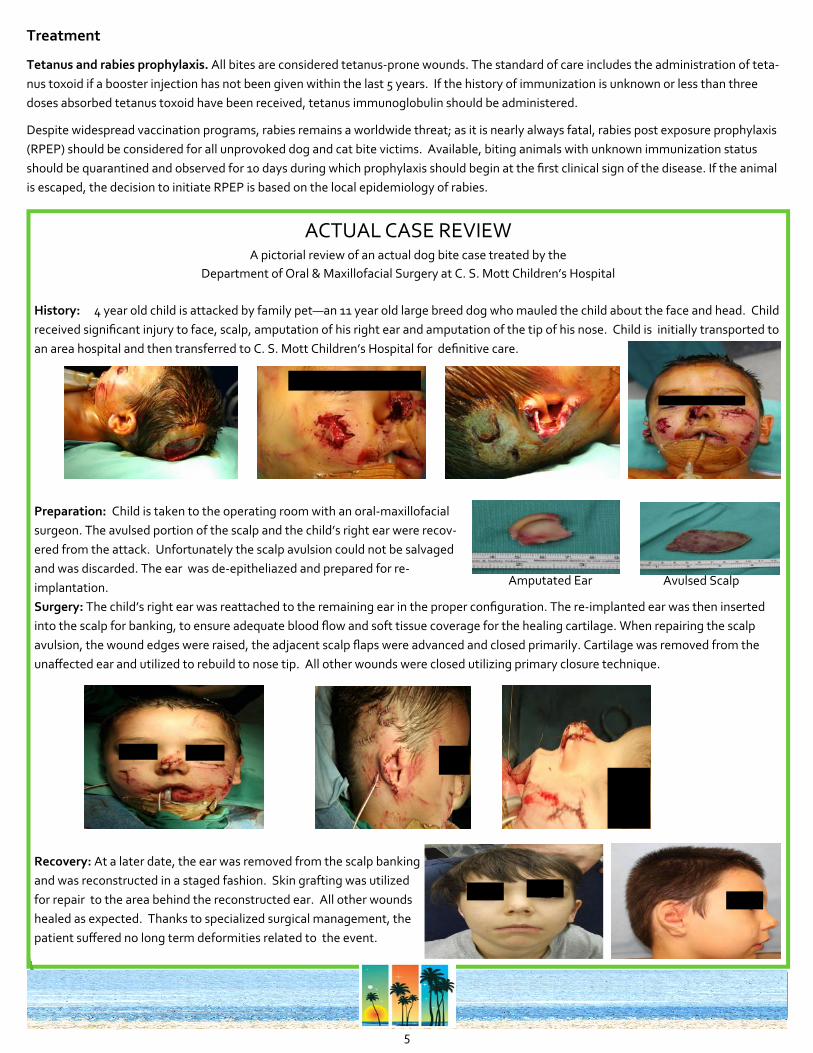
History: 4 year old child is attacked by family pet—an 11 year old large breed dog who mauled the child about the face and head. Child
received significant injury to face, scalp, amputation of his right ear and amputation of the tip of his nose. Child is initially transported to
an area hospital and then transferred to C. S. Mott Children’s Hospital for definitive care.
Preparation: Child is taken to the operating room with an oral‐maxillofacial
surgeon. The avulsed portion of the scalp and the child’s right ear were recov‐
ered from the attack. Unfortunately the scalp avulsion could not be salvaged
and was discarded. The ear was de‐epitheliazed and prepared for re‐
implantation.
Surgery: The child’s right ear was reattached to the remaining ear in the proper configuration. The re‐implanted ear was then inserted
into the scalp for banking, to ensure adequate blood flow and soft tissue coverage for the healing cartilage. When repairing the scalp
avulsion, the wound edges were raised, the adjacent scalp flaps were advanced and closed primarily. Cartilage was removed from the
unaffected ear and utilized to rebuild to nose tip. All other wounds were closed utilizing primary closure technique.
Recovery: At a later date, the ear was removed from the scalp banking
and was reconstructed in a staged fashion. Skin grafting was utilized
for repair to the area behind the reconstructed ear. All other wounds
healed as expected. Thanks to specialized surgical management, the
patient suffered no long term deformities related to the event.
Treatment
Tetanus and rabies prophylaxis. All bites are considered tetanus‐prone wounds. The standard of care includes the administration of teta‐
nus toxoid if a booster injection has not been given within the last 5 years. If the history of immunization is unknown or less than three
doses absorbed tetanus toxoid have been received, tetanus immunoglobulin should be administered.
Despite widespread vaccination programs, rabies remains a worldwide threat; as it is nearly always fatal, rabies post exposure prophylaxis
(RPEP) should be considered for all unprovoked dog and cat bite victims. Available, biting animals with unknown immunization status
should be quarantined and observed for 10 days during which prophylaxis should begin at the first clinical sign of the disease. If the animal
is escaped, the decision to initiate RPEP is based on the local epidemiology of rabies.
Amputated Ear Avulsed Scalp

6
CONTACT US
EDITOR: AMY RANDALL, MSN, RN Pediatric Trauma Program Manager
EMAIL: Mott‐Pediatric‐[email protected]
C. S. Mott Children’s Hospital 1500 E. Medical Center Drive Ann Arbor, MI 48109‐5231
TAKE THE QUIZ!
KNOWLEDGE TEST AND AMA/PRA
CATEGORY 1 CREDIT
After reading the article, continue the educational activity by
taking the online CME quiz at:
h ps://cme.med.umich.edu/assessment/ques ons.asp?gid=167 After you initially take the test, the test will be immediately electronically scored.
If fewer than 70% of the questions are answered correctly, the questions that were not answered correctly will be
noted in red. Review the CME content related to those topics and retake the test.
If 70% or more of the questions are answered correctly, the correct and incorrect answers for all questions will be
shown along with explanations of the basis for the correct answer. The link to register and receive credit is shown
at the end of the items and explanations. Complete the electronic credit request and activity evaluation. An elec‐
tronic certificate of participation will be provided immediately. Print the certificate of participation for your per‐
sonal records.
NURSES: Remember 1 CME = 1 CEU credit for nursing! This activity WILL count toward your 25 hours/2yrs of required CEU for licensure
“It’s a good idea to begin at the bottom in everything except in learning to swim” Author Unknown
Article references:
Eppley, B, Schleich, A. Facial dog bite injuries in children: treatment and outcome assessment. The Journal of Craniofacial Surgery. 2013; 24(2): 384‐386
Gurunluoglu, R, Glasgow, M, Arton, J, Bronsert, M. Retrospective analysis of facial dog bite injuries at a level I trauma center in the Denver metro area. Journal of Trauma and Acute Care Surgery.
2014; 76(5): 1294‐1300
Kaye, A, Belz, J, Kirschner, R. Pediatric dog bite injuries: a 5‐year review of the experience at the Children’s Hospital of Philadelphia. Plastic and Reconstructive Surgery. 2009; 124(2): 551‐558
Reisner, I, Nance, M, et al. Behavioral characteristics associated with dog bites to children presenting to an urban trauma centre. Injury Prevention. 2011; 17: 348‐353
Sacks, J, Sinclair, L, et al. Breeds of dogs involved in fatal human attacks in the United States between 1979 and 1998. Journal of the American Veterinary Medical Association. 2006; 217(6): 836‐840
Schalamon, J, Ainoedhofer, H, et al. Analysis of dog bites in children who are younger than 17 years. Journal of the American Academy of Pediatrics. 2006; 117(3): e374‐e379
Stefanopoulos, P, Tarantzopoulou, A. Facial bite wounds: management update. International Journal of Oral and Maxillofacial Surgeons. 2005; 34: 464‐472
http://www.cdc.gov/HomeandRecreationalSafety/Dog‐Bites/
Jackler, RK anatomic picture retrieved from http://med.stanford.edu/ohns/atlas_sb/atlas_21.1.html
Prevention
Pet owner. Any dog of any breed has the potential to bite. If you have a dog in your home, there are several things that can be done
to reduce aggressive tendencies:
• Spay/neuter your dog • Never leave infants or young children alone with a dog
• Don’t play aggressive games with your dog • Properly socialize and train dogs. Teach submissive behaviors
• Immediately seek professional advice if the dog begins to display aggressive or undesirable behaviors
What to teach children. Even young children can be taught techniques to reduce their susceptibility to being bitten by a dog. The
best prevention, however, is close observation of children while in the presence of any dog. Teach children basic safety tips and re‐
view them regularly. Those tips are:
• Do not approach an unfamiliar dog • Remain motionless when approached by an unfamiliar dog
• Do not run from a dog or scream • If knocked over by a dog, roll into a ball and be still
• Do not play with a dog unless with an adult • Immediately report stray dogs or dogs showing unusual behavior
• Avoid direct eye contact with a dog
• Do not disturb a dog that is sleeping, eating or caring for puppies
• If bitten, immediately report the bite to an adult
• Do not pet a dog without allowing it to see and sniff you first
• Do not hug or kiss a dog























![] 1 Mott - epawebapp.epa.ie](https://img.pdfslide.us/doc/110x75/619a4404f1d852760143f744/-1-mott-.jpg)



